Back to Journals » Infection and Drug Resistance » Volume 19
Retrospective Analysis of Infection Characteristics and Prognostic Factors in ICU Sepsis Patients in Jiaxing Area
Authors Li H, Tan X, Wang S, Shen W, Yuan B
Received 25 October 2025
Accepted for publication 23 March 2026
Published 8 April 2026 Volume 2026:19 576517
DOI https://doi.org/10.2147/IDR.S576517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Hui Li, Xiaochun Tan, Siheng Wang, Weifeng Shen, Beibei Yuan
Department of Clinical Laboratory, the First Hospital of Jiaxing, the Affiliated Hospital of Jiaxing University, Jiaxing, Zhejiang, People’s Republic of China
Correspondence: Beibei Yuan, Email [email protected]
Background: Sepsis remains a leading cause of morbidity and mortality in intensive care units (ICUs), with antimicrobial resistance (AMR) complicating therapeutic decisions. This study aimed to characterize pathogen distribution, AMR patterns, and prognostic indicators in ICU patients with sepsis at Jiaxing First Hospital.
Methods: A retrospective analysis of 352 septic patients (2021– 2024) was conducted. Clinical outcomes, pathogen profiles, and antimicrobial susceptibility were evaluated. Multivariable logistic regression and ROC curve analysis identified predictors of non-recovery.
Results: Gram-negative bacteria predominated (67.31%), with Klebsiella pneumoniae (K. pneumoniae), Escherichia coli (E. coli), Acinetobacter baumannii (A. baumannii), and Pseudomonas aeruginosa (P. aeruginosa) as the most frequent isolates. Notably, A. baumannii exhibited extensive resistance (> 80% to ceftazidime, ciprofloxacin, and carbapenems) and the highest Non-recovery rate (60.98%). Among Gram-positive isolates, Enterococcus faecium (E. faecium), Staphylococcus aureus (S. aureus), and Enterococcus faecalis (E. faecalis) were prevalent, showing high susceptibility to vancomycin, tigecycline, and quinupristin-dalfopristin. Pulmonary infection was the predominant source (37.8%), primarily involving A. baumannii and K. pneumoniae, while intestinal translocation was twice as frequent in non-recovery patients. Independent predictors of non-recovery included age, pneumonia, shock, respiratory failure (RF), and lactate (LA). Their combination yielded a robust prognostic model (AUC 0.813), with RF as the strongest contributor.
Conclusion: This study highlights the epidemiological landscape of ICU sepsis and emerging AMR patterns, particularly for A. baumannii. A prognostic model using routine parameters enables early identification of high-risk patients. Targeted interventions—updated guidelines, enhanced infection control, and antimicrobial stewardship—may improve outcomes and warrant prospective validation.
Keywords: sepsis, antimicrobial resistance, prognostic biomarkers, ICU, bloodstream infections
Introduction
Sepsis is a life-threatening syndrome triggered by a dysregulated host response to infection, resulting in physiological, pathological, and biological abnormalities1 It poses a major global public health challenge due to its high mortality, significant morbidity, and considerable economic burden2 Bloodstream infections (BSI) are responsible for 40% of community- and hospital-acquired sepsis and septic shock cases, and approximately 20% of those acquired in the ICU. In critically ill patients, about 25% of hospital-acquired BSI cases are imported (identified at ICU admission), while 75% occur within the ICU.3 The use of invasive devices like intravascular catheters and endotracheal tubes compromises anatomical barriers, increasing the risk of healthcare-associated infections in these patients.4 Additionally, impaired immune defenses in some ICU patients heighten their susceptibility to infections.5
Antibiotics are the cornerstone of sepsis treatment. The 2021 sepsis guidelines recommend initiating antimicrobials within one hour for confirmed, highly suspected, or possible sepsis with shock. For possible sepsis without shock, antibiotics should be given within three hours if infection remains suspected after rapid assessment. Although early intervention improves outcomes, treatment delays persist due to the lack of standardized rapid assessment tools.6 Inappropriate antibiotic use in some regions has also contributed to the spread of drug-resistant bacteria in ICUs, complicating clinical management.7
To improve sepsis management in the ICU, there is a need to identify effective infection indicators and understand local pathogen resistance patterns. Easily accessible clinical indicators are commonly used to evaluate infection likelihood. Although some studies have linked certain indicators to sepsis incidence, regional variations in pathogen types, drug resistance, and patient characteristics necessitate location-specific screening of clinical markers. However, data specifically addressing the clinical characteristics, pathogen distribution, and antimicrobial resistance profiles of sepsis patients in the Jiaxing region remain scarce. This knowledge gap hinders the development of regionally tailored empirical treatment strategies and may compromise patient outcomes. Therefore, we analyzed blood samples from ICU sepsis patients in our hospital between 2021 and 2024, along with the drug resistance profiles of detected strains. This approach supports the selection of tailored treatment strategies for different pathogens and may aid in earlier identification of high-risk sepsis patients.
In selecting clinical indicators, we analyzed the routine tests after ICU admission for sepsis patients. Indicators such as C-reactive protein (CRP), procalcitonin (PCT), and lymphocyte percentage (LYM, %), previously shown to correlate with sepsis outcomes,8,9 were our key focuses. Additional variables—including AGE, time to positivity, hospital stay length, pre-hospital shock, underlying disease, concomitant disease, source of infection, and GCS at the time of diagnosis—were also evaluated. Using multivariate logistic regression, we found indicators to judge infection occurrence. This helps clinicians with early identification, severity assessment, timely treatment, and better prognosis for patients.
Materials and Methods
Study Population, Inclusion and Exclusion Criteria
This retrospective study enrolled patients admitted to the intensive care unit (ICU) of our hospital between January 2021 and December 2024 who developed sepsis secondary to bloodstream infection (BSI). Patients were selected based on the following inclusion criteria: (1) compliance with the healthcare-associated infection criteria established by the Ministry of Health; (2) confirmation of pathogenic bacteria through microbiological laboratory testing; and (3) availability of complete clinical records. Patients were excluded if any of the following conditions applied: (1) incomplete clinical documentation; (2) bacterial culture results suggestive of contamination or lacking accompanying antimicrobial susceptibility testing; (3) identification of pathogenic bacteria prior to admission with no new pathogens detected thereafter; or (4) positive culture results deemed to represent contamination after comprehensive assessment of inflammatory markers. Based on clinical outcomes, patients were categorized into the recovery group (n = 210), comprising patients who were cured or improved, and the non-recovery group (n = 142), which included patients who died or showed no remission during the study period.
Clinical Sample Collection and Data Recording
All patient information obtained from medical records of all enrolled patients was used in this study. The following parameters were recorded from blood tests: white blood cell count (WBC), neutrophil percentage (NEUT, %), LYM, serum albumin (ALB) levels, LA, CRP, and PCT Levels. Pathogen information was obtained from blood culture records. In addition, the following clinical variables were documented: pre-hospital shock, GCS; underlying diseases (eg., hypertension, diabetes mellitus [DM], malignancy); comorbidities (eg., pneumonia, acute kidney injury [AKI], cerebrovascular disease [CVD], RF); and clinical interventions (eg., chemotherapy, cardiopulmonary resuscitation [CPR]). Patient outcomes were also documented.
Bacterial Isolation and Identification and and Antimicrobial Susceptibility Testing
For ICU-acquired BSI episodes, microbial identification was performed using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS, Bruker Daltonics) on colonies subcultured from positive blood culture bottles. Subsequent antimicrobial susceptibility testing (AST) was conducted on the same isolates following standardized microbiological protocols in accordance with the CLSI M100 (Performance Standards for Antimicrobial Susceptibility Testing) guidelines. Depending on the bacterial species, AST was performed using either the Kirby-Bauer disk diffusion method or the broth microdilution method to determine inhibition zone diameters or minimum inhibitory concentrations (MICs). All results were interpreted based on the clinical breakpoints and quality control criteria recommended by the CLSI. For Gram-negative bacteria, susceptibility testing included the following antibiotics: amoxicillin (AMC), amikacin (AMK), ampicillin (AMP), aztreonam (ATM), ceftazidime (CAZ), ciprofloxacin (CIP), ceftriaxone (CRO), cefoperazone (CSL), cefuroxime (CXM), cefazolin (CZO), ertapenem (ETP), cefepime (FEP), cefoxitin (FOX), gentamicin (GEN), imipenem (IPM), levofloxacin (LVX), meropenem (MEM), ampicillin sulbactam (SAM), trimethoprim-sulfamethoxazole (SXT), tigecycline (TGC), tobramycin (TOP), and piperacillin-tazobactam (TZP). For Acinetobacter baumannii, we also performed antimicrobial susceptibility testing using colistin (COL), minocycline (MNO), and tetracycline (TCY). For Gram-positive bacteria, susceptibility testing included the following antibiotics: ampicillin (AMP), ciprofloxacin (CIP), clindamycin (CLI), erythromycin (ERY), high concentration gentamicin (GEH), gentamicin (GEN), linezolid (LNZ), levofloxacin (LVX), moxifloxacin (MFX), oxacillin (OXA), penicillin (PEN), quinupristin-dalfopristin (QDA), rifampin (RIF), high-concentration streptomycin (STH), trimethoprim-sulfamethoxazole (SXT), tetracycline (TCY), tigecycline (TGC), and vancomycin (VAN).
Statistical Analysis
Statistical analysis was conducted using SPSS 26.0. Appropriate tests were selected based on data characteristics, and a p-value <0.05 (two-tailed) was considered statistically significant. Binary logistic regression analysis was used to identify factors associated with poor prognosis in patients with sepsis. Factors with significant differences identified in univariate logistic regression were further analyzed in multivariate logistic regression. The discriminative ability of the predictive model was evaluated using receiver operating characteristic (ROC) curve analysis, with the area under the curve (AUC) indicating discriminative performance. A significance level of p < 0.05 was used for all statistical tests.
Results
General Situation of Patients with Bacterial Infections in ICU
Among the 352 patients enrolled in the study, ages ranged from 19 to 96 years (mean 67.01 ± 15.87 years). The cohort included 117 females (33.24%) and 235 males (66.76%), yielding 410 bacterial isolates (141 from females [34.39%] and 269 from males [65.61%]). Overall, 142 patients (40.34%) experienced non-recovery, comprising 43 females (30.28%) and 99 males (69.72%); the remaining 210 patients (59.66%) recovered. Detailed analyses are provided in Table 1.
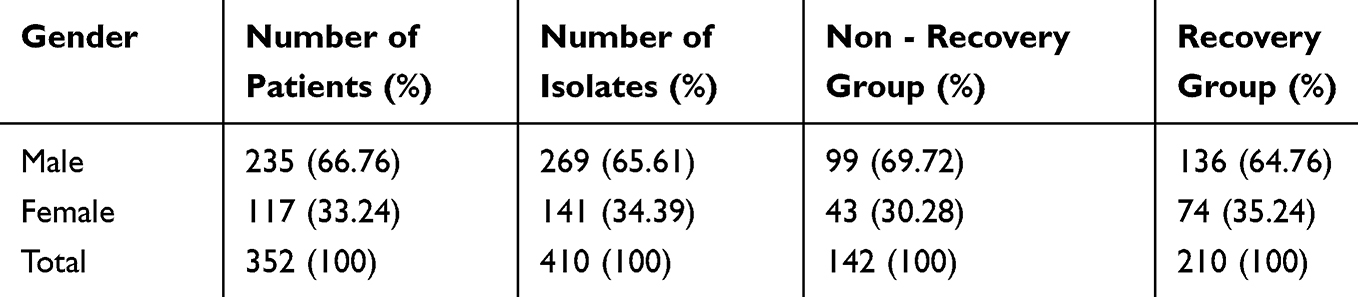 |
Table 1 Gender and Recovery Rates of Patients |
Analysis of the Sources of Acquired Infections in ICU
In this study, all clinical samples were collected during positive blood culture episodes from 352 patients, yielding 410 bacterial isolates. Among these, 121 (29.5%) were Gram-positive and 289 (70.5%) were Gram-negative. The predominant Gram-positive bacteria were E. faecium, E. faecalis, and S. aureus; the most frequent Gram-negative pathogens were K. pneumoniae, E. coli, A. baumannii, and P. aeruginosa. E. coli and K. pneumoniae counts were significantly higher in the recovery group than in the non-recovery group, with no significant differences in other bacteria. Notably, the proportion of non-recovery exceeded 50% for A. baumannii, E. faecium, E. faecalis, and S. aureus, with the highest proportion observed for A. baumannii at 60.98%. Pulmonary infection (LRTI) was the most common source (37.80%), followed by urinary tract (UTI), biliary tract (Biliary-tract Infection), and intestinal flora translocation (BT). Over 75% of biliary and urinary tract infections occurred in the recovery group, whereas intestinal translocation-related infections were twice as frequent in the non-recovery group. Other infection routes showed no significant intergroup differences. Among the top seven pathogens, A. baumannii and K. pneumoniae primarily entered the bloodstream via LRTI, E. coli through UTI, and Enterococci via BT. Isolate distribution and infection sources are summarized in Figure 1.
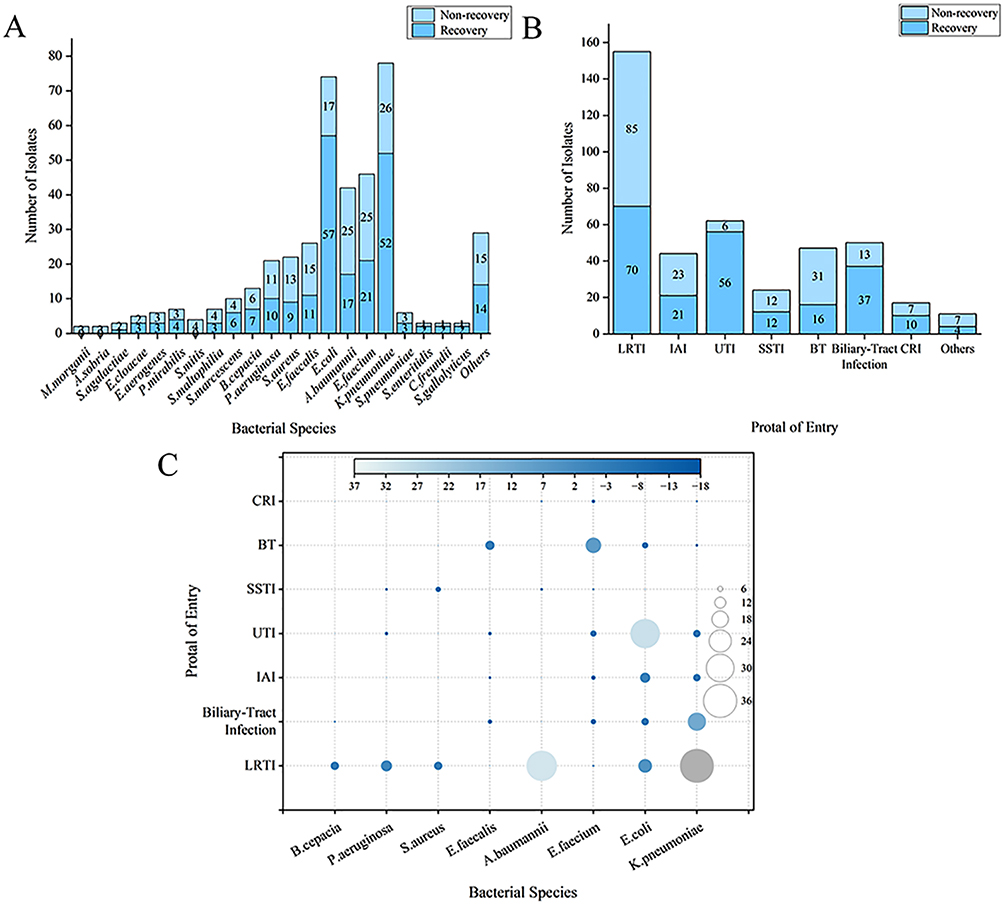 |
Figure 1 Distribution of Isolated Strains and BSI Sources by Bacterial Pathogen. (A) BSI species in the ICU patient population. (B) Bacterial sources of BSI in ICU patients; (C) The first 7 bacterial species by infection source. |
Bacterial Distribution of Different Specimen Types in ICU Acquired Infections
We further analyzed the annual bacterial detection counts and multidrug-resistant organisms (MDROs) rates for the predominant Gram-positive and Gram-negative species. From 2021 to 2024, detections of E. coli and K. pneumoniae declined steadily, while S. aureus detections decreased after 2022. In contrast, detections of E. faecalis and E. faecium rebounded in 2023, alongside a sharp rise in A. baumannii.
The total number of MDROs showed considerable fluctuation, reaching a peak of 55 strains in 2023 before dropping to 31 strains in 2024. Notably, while E. faecium remained relatively stable, E. faecalis—which had not exhibited resistance in previous years—developed new resistance. In 2021, 38 MDROs strains were isolated, comprising 10 carbapenem-resistant Enterobacteriaceae (CRE) strains, 4 carbapenem-resistant A. baumannii (CRAB) strains, 1 methicillin-resistant S. aureus strains (MRSA) strains, 1 carbapenem-resistant P. aeruginosa (CRPA) strains, and 22 other strains. The following year, 36 MDROs were isolated, including 4 CRE strains, 7 CRAB strains, 2 MRSA strains, 1 CRPA strains, and 22 other strains. In 2023, isolations rose to 55 MDROs strains, consisting of 4 CRE strains, 19 CRAB strains, 3 MRSA strains, 2 CRPA strains, and 27 other strains. By 2024, the total fell to 31 MDROs strains: 8 CRE strains, 6 CRAB strains, 4 MRSA strains, and 13 other strains.
Analysis of multidrug resistance rates revealed year-to-year fluctuations for most pathogens. CRAB demonstrated a marked upward trend: its proportion surged to 95% (19 strains) in 2023, and though detections fell to 6 strains in 2024, the resistance rate remained high at 86%. The proportion of CRE dropped to a low of 9% in 2022 but increased to 21% (8 strains) by 2024. MRSA rose consistently from 40% in 2021 to 100% in 2024. Meanwhile, the proportion of CRPA remained stable, ranging between 17% and 20% across the period. The annual bacterial detection numbers and MDROs rates are summarized in Figure 2 and Table S1.
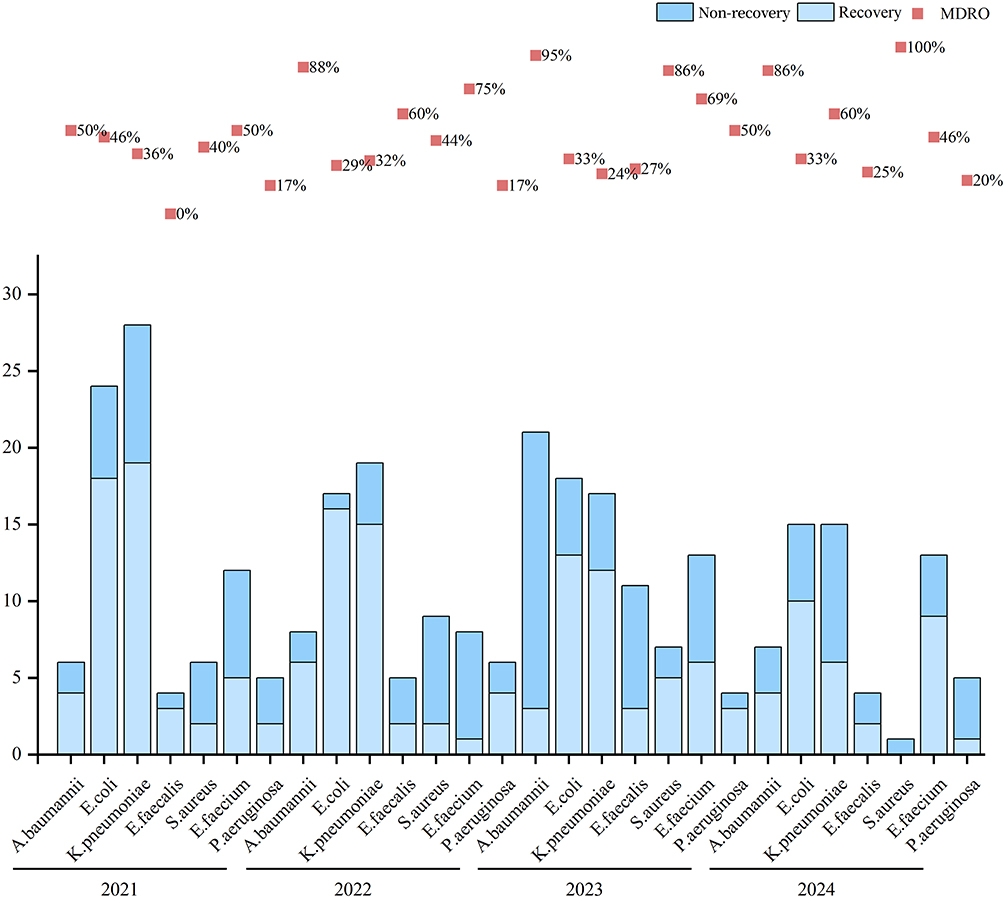 |
Figure 2 Trends in Predominant Bacterial Isolates and Their MDROs Rates. |
Antibiotic Resistance Rate of Common BSI Bacteria in ICU
From a total of 6,357 positive blood culture bottles screened, 410 ICU-acquired BSI episodes were identified. Drug resistance profiles were analyzed for the most frequently detected pathogens, including three Gram-positive species (E. faecium, S. aureus, and E. faecalis) and three Gram-negative species (K. pneumoniae, E. coli, and A. baumannii). Antimicrobial susceptibility testing revealed that all three species were susceptible to vancomycin. Tigecycline, tetracycline, and quinupristin-dalfopristin also demonstrated relatively good efficacy. However, significant resistance was observed for erythromycin and penicillin. The detailed resistance profiles are provided in Table 2.
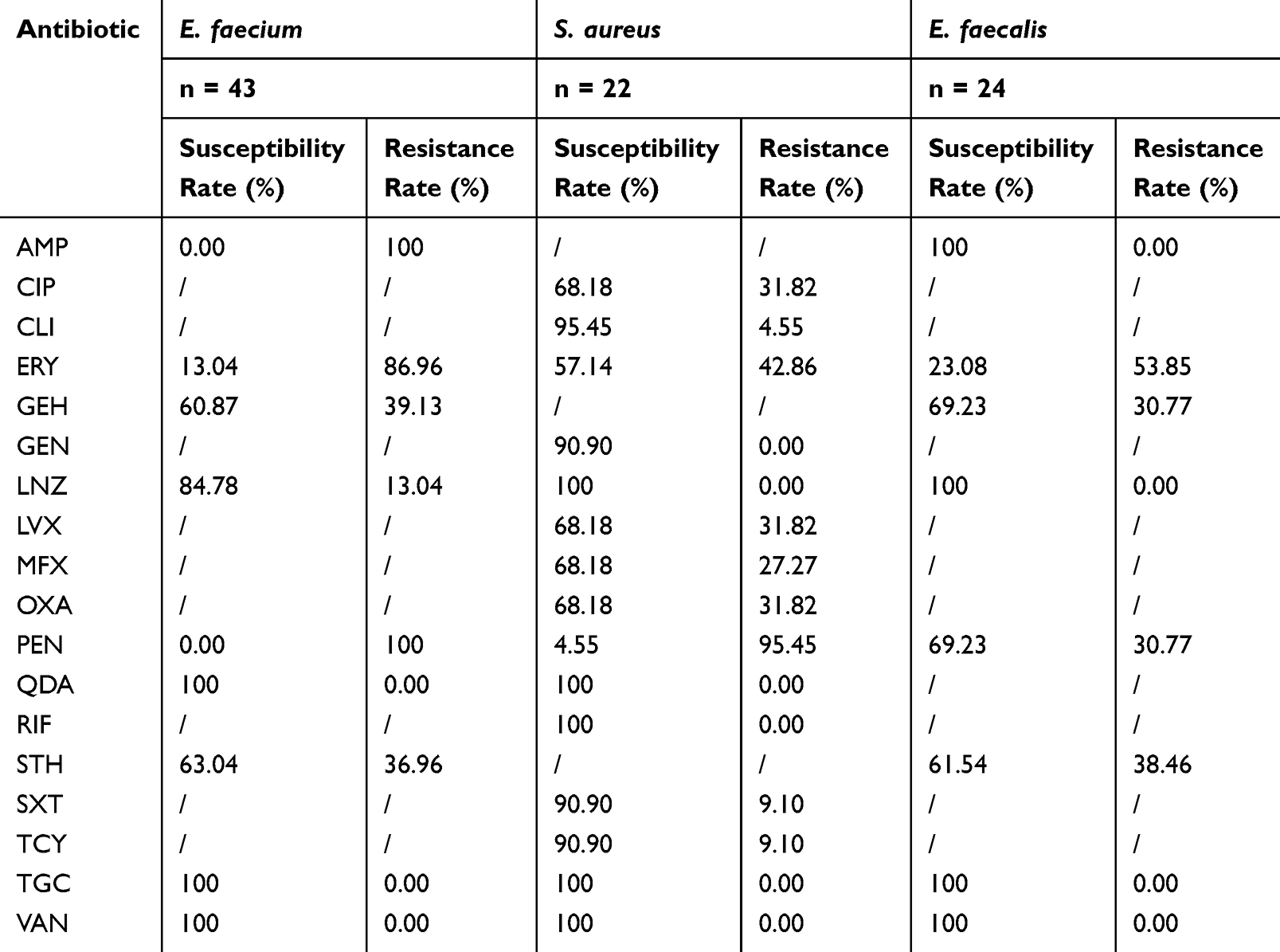 |
Table 2 Resistance Test Results of Three Gram Positive Bacterial Species |
Among Gram-negative bacteria, we focused on K. pneumoniae, E. coli, and A. baumannii. Our analysis showed that A. baumannii exhibited significant resistance to all antibiotics except colistin and amikacin, which had a sensitivity rate of over 50%. Amikacin and tigecycline were found to be highly effective against K. pneumoniae (sensitivity rate ≥75%). For E. coli, multiple antibiotics including amoxicillin, amikacin, cefoperazone, ertapenem, cefepime, cefoxitin, imipenem, meropenem, tigecycline, tobramycin, and piperacillin showed good efficacy. The specific drug-resistance profiles of these three bacterial species are detailed in Table 3.
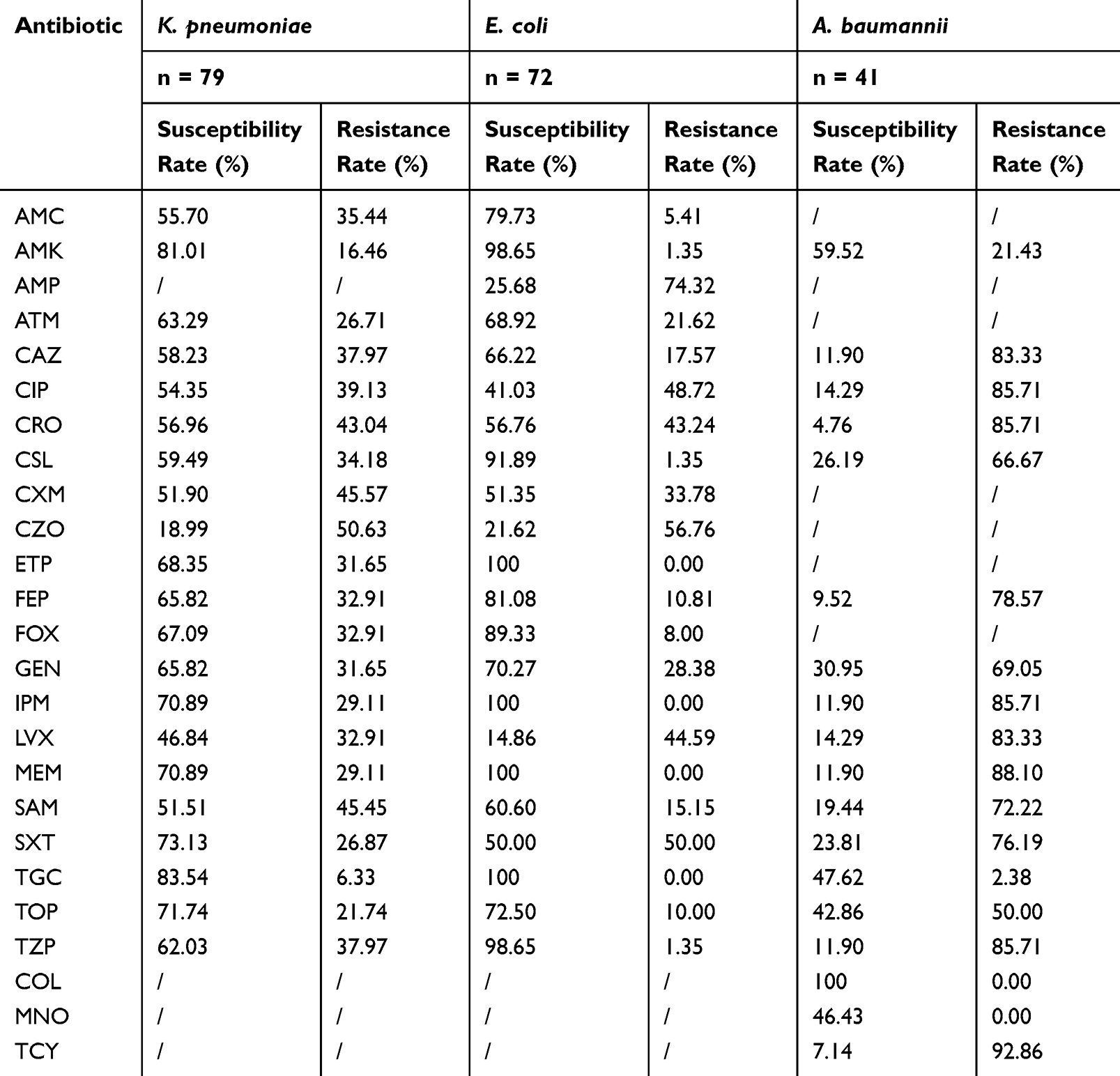 |
Table 3 Resistance Test Results of Three Gram Negative Bacterial Strains |
Analysis of Multiple Logistic Regression Results
We summarized the baseline characteristics of the cohort stratified by clinical outcomes. Univariate analysis revealed that patients in the non-recovery group presented with a more severe clinical profile. They were older, had lower GCS scores, and experienced higher rates of pre-hospital shock, in-hospital shock, CPR and RF. Pneumonia and malignancy were also significantly associated with non-recovery. In contrast, UTI was more frequent among patients who recovered. Regarding other infection sources, BT was significantly more common in non-recovered patients, whereas biliary tract infection was more prevalent in the recovery group. Lower respiratory tract infection and intra-abdominal infection did not significantly differ between groups. Laboratory findings further distinguished the two outcomes: non-recovered patients exhibited lower LYM percentages and elevated serum LA levels, suggesting greater metabolic stress and possible tissue hypoperfusion.
In multivariate logistic regression analysis, advanced age, pneumonia, and shock remained independent predictors of non-recovery. RF emerged as the strongest independent predictor, with the highest effect size. Elevated serum LA also retained a significant association with poor outcome, reinforcing its value as an objective biomarker of disease severity. Although factors such as GCS score, malignancy, UTI, LYM percentage, biliary-tract infection, and BT were significant in univariate analyses, their effects were not sustained after adjustment for stronger clinical determinants like shock and RF—suggesting that their prognostic influence may be confounded or superseded by these dominant factors. Detailed results are shown in Table 4.
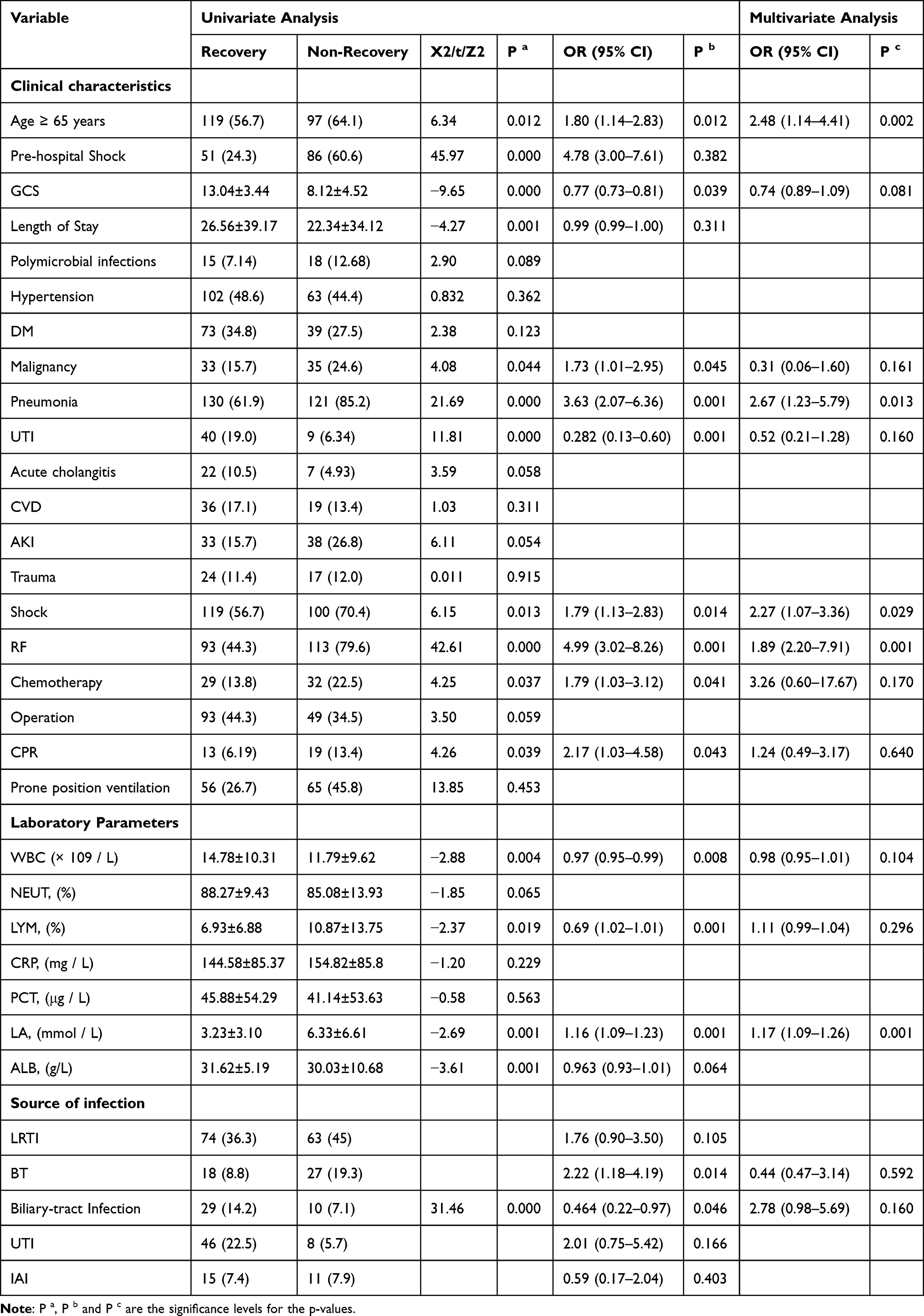 |
Table 4 Univariate and Multivariate Logistic Regression Analysis of Clinical Characteristics Associated with Recovery |
ROC Curve Analysis
The discriminatory ability of individual clinical variables and a combined model for predicting non-recovery was evaluated using ROC analysis. Among single predictors, RF yielded the highest AUC (0.676), followed by serum LA (0.661) and pneumonia (0.614). Age and shock exhibited limited predictive value, with AUCs of 0.567 and 0.565, respectively. The combined model, incorporating multiple significant variables, demonstrated substantially improved performance (AUC 0.813), indicating that an integrative approach enhances risk stratification beyond any single factor alone, as shown in Figure 3 and Table 5.
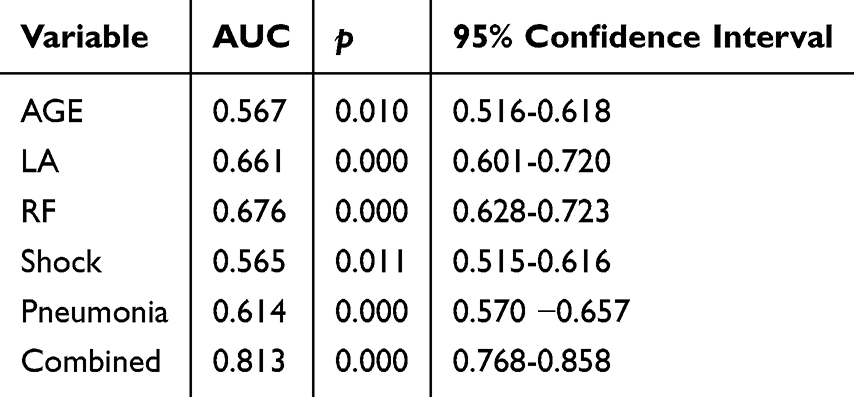 |
Table 5 ROC Analysis Results |
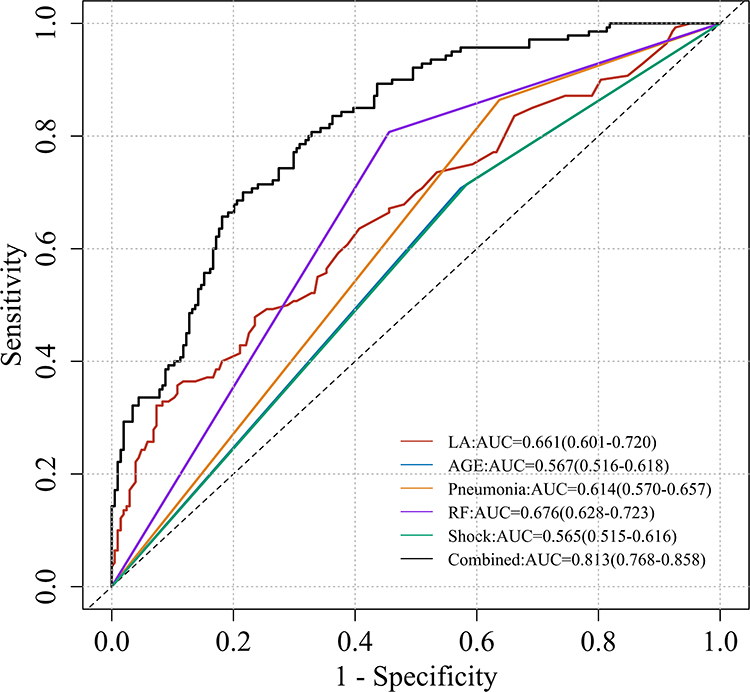 |
Figure 3 ROC curve analysis results. |
Association of Key Variables with Hospital Stay Duration
We assessed the correlation between several key clinical variables and the length of hospitalization. The analysis revealed that lower GCS (HR = 0.90, 95% CI: 0.85–0.94, p < 0.001) and decreased ALB levels (HR = 0.94, 95% CI: 0.91–0.97, p < 0.001) were associated with prolonged hospital stays. In contrast, elevated CRP (HR = 1.01, 95% CI: 1.01–1.02, p = 0.02) and LA (HR = 1.13, 95% CI: 1.10–1.16, p < 0.001) levels were positively correlated with longer hospitalization, as shown in Figure 4.
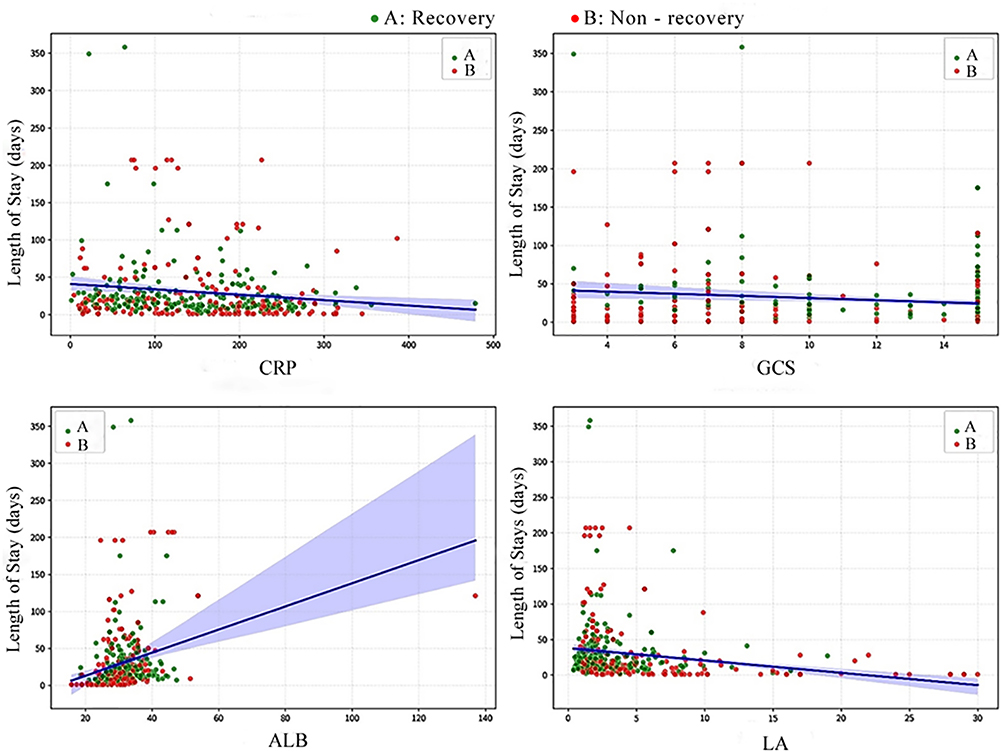 |
Figure 4 Association of Key Variables with Hospital Stay Duration. |
Discussion
This 4-year retrospective study of 352 ICU sepsis patients at Jiaxing First Hospital delineates the local epidemiological landscape, antimicrobial resistance patterns, and clinically relevant prognostic factors. Gram-negative pathogens predominated, with A. baumannii emerging as the most formidable challenge—exhibiting the highest non‑recovery rate and extensive resistance. Temporal trends reveal escalating threats: CRAB resistance reached 95% in 2023 and remained 86% in 2024, while CRE increased to 21% and MRSA to 100% over the study period. These findings demand urgent action.
Antimicrobial susceptibility data provide actionable guidance for empirical therapy: vancomycin remains reliable for Gram-positive coverage, although the increasing prevalence of MRSA warrants empirical anti-MRSA therapy in at-risk patients. For A. baumannii, limited therapeutic options necessitate combination regimens, and novel agents (eg., sulbactam-durlobactam, cefiderocol) should be considered for confirmed resistant cases.10,11 The sustained susceptibility of K. pneumoniae and E. coli to amikacin and tigecycline, particularly in the context of emerging CRE, supports the implementation of carbapenem-sparing regimens.
To ensure accurate attribution of true bacteraemia, a rigorous case-selection strategy was applied. Most patients with coagulase-negative staphylococci (CoNS) isolates were excluded due to their overall inflammatory marker profiles and the high likelihood of contamination (eg., from puncture sites or catheters); inclusion occurred only when typical sepsis symptoms were present. Conversely, patients with Enterococcus isolates were included even when inflammatory markers were not fully consistent with sepsis.12 This approach reflects that Enterococcus—primarily a gut colonizer—typically enters the bloodstream via mucosal barrier disruption or invasive procedures (eg., abdominal drainage). In the absence of such procedures, Enterococcus bacteraemia is attributed to transient bacteraemia, intra-abdominal infections, urinary tract infections, or endocarditis, rather than external contamination.
Building upon these microbiological and methodological foundations, we developed a pragmatic prognostic model integrating age, pneumonia, shock, RF, and serum LA—all routinely available parameters. The model achieved robust discriminatory performance, enabling early identification of high-risk patients who may benefit from intensified monitoring, aggressive source control, or adjunctive therapies. Notably, RF emerged as the strongest predictor, underscoring the critical importance of ventilator-associated pneumonia prevention and respiratory support optimisation in this vulnerable population.13,14
Based on these findings, we propose several targeted interventions for institutional implementation. First, empirical antibiotic protocols should be revised to reflect local resistance patterns, with consideration of combination therapy for high-risk patients while awaiting culture results. Second, integrating the prognostic model into electronic health records or daily checklists could facilitate systematic risk stratification at the point of care. Third, infection control measures should be strengthened, particularly environmental disinfection and contact precautions for patients colonized with CRAB. Fourth, given the altered pharmacokinetics in critically ill patients—attributable to clinical complexity, poor baseline status, and interference from organ support such as continuous renal replacement therapy (CRRT)—therapeutic drug monitoring for key antibiotics is warranted to ensure adequate plasma exposure and treatment efficacy.15 Finally, antimicrobial stewardship efforts should be reinforced, with a focus on carbapenem conservation. Translating these strategies into clinical practice may contribute to improved outcomes in this vulnerable population. Future directions include prospective validation of the prognostic model, evaluation of rapid diagnostic technologies, and ongoing surveillance to monitor the impact of these interventions on resistance trends and patient outcomes. We acknowledge the inherent limitations of this single-center study, including its sample size and the potential influence of institutional epidemiology and practice patterns on generalizability. Therefore, these findings should be regarded as preliminary, warranting further validation in larger, multicenter cohorts. Furthermore, due to the limited number of polymicrobial infection cases, we were unable to perform a comprehensive comparison of clinical characteristics and resistance patterns between monomicrobial and polymicrobial groups, underscoring the need for dedicated studies with larger cohorts to investigate this important subset of infections.
Conclusion
This study elucidates the epidemiological landscape, resistance patterns, and prognostic determinants of sepsis in the ICU setting at our institution. The findings carry direct translational value for clinical practice. They mandate a revision of empirical antibiotic strategies to address the predominance of XDR A. baumannii and the emergence of CRE. Furthermore, they support the adoption of a pragmatic bedside prognostic model to enable early risk stratification. Finally, they delineate specific infection sources and pathogen-resistance combinations that should be prioritized in prevention and treatment efforts. By translating these findings into clinical practice—through updated guidelines, enhanced infection control, and systematic risk assessment—we can potentially improve outcomes for this vulnerable patient population. Future investigations should prioritize prospective validation of the prognostic model, evaluation of novel antibiotic regimens tailored to our local epidemiology, and implementation science research to optimize the adoption of rapid diagnostic technologies and enhanced infection control strategies.
Ethics Approval
The study was approved by the ethics committee of the First Hospital of Jiaxing (No. 2025-LP-471). The ethics committee abandoned the requirement for participants to give formal informed permission because of the retrospective nature of this study. Patients’ anonymous information was provided from the microbiology hospital laboratory, which isolated the strains. The study completely followed the guiding principles in the Declaration of Helsinki.
Author Contributions
All authors contributed significantly to the work, including in the conception, study design, execution, data acquisition, analysis, and interpretation; participated in drafting or critically revising the manuscript; gave final approval of the version to be published; agreed on the journal for submission; and agreed to be accountable for all aspects of the work.
Funding
This study was supported by Jiaxing Key Discipline of Medcine–Clinical Diagnostics (2023-ZC-002 & 2023-ZC-02) and Talent Training of the First Hospital of Jiaxing of Zhejiang Province of China (2021-QMX-22).
Disclosure
The authors declare no conflicts of interest.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–13. doi:10.1001/jama.2016.0287
2. Reinhart K, Daniels R, Kissoon N, et al. Recognizing sepsis as a global health priority - A WHO resolution. N Engl J Med. 2017;377(5):414–417. doi:10.1056/NEJMp1707170
3. Timsit JF, Ruppé E, Barbier F, et al. Bloodstream infections in critically ill patients: an expert statement. Intensive Care Med. 2020;46(2):266–284. doi:10.1007/s00134-020-05950-6
4. Vincent J-L, Sakr Y, Singer M, et al. Prevalence and outcomes of infection among patients in intensive care units in 2017. JAMA. 2020;323(15):1478–1487. doi:10.1001/jama.2020.2717
5. Kreitmann L, Helms J, Martin-Loeches I, et al. ICU-acquired infections in immunocompromised patients. Intensive Care Med. 2024;50(3):332–349. doi:10.1007/s00134-023-07295-2
6. Tabah A, Buetti N, Staiquly Q, et al. Epidemiology and outcomes of hospital-acquired bloodstream infections in intensive care unit patients: the EUROBACT-2 international cohort study. Intensive Care Med. 2023;49(2):178–190. doi:10.1007/s00134-022-06944-2
7. De Waele JJ, Akova M, Antonelli M, et al. Antimicrobial resistance and antibiotic stewardship programs in the ICU: insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med. 2018;44(2):189–196. doi:10.1007/s00134-017-5036-1
8. Tocu G, Mihailov R, Serban C, et al. The contribution of procalcitonin, c-reactive protein and interleukin-6 in the diagnosis and prognosis of surgical sepsis: an observational and statistical study. J Multidiscip Healthc. 2023;16:2351–2359. doi:10.2147/JMDH.S422359
9. Denstaedt SJ, Cano J, Wang XQ, et al. Blood count derangements after sepsis and association with post-hospital outcomes. Front Immunol. 2023;14:1133351. doi:10.3389/fimmu.2023.1133351
10. Serapide F, Guastalegname M, Gullì SP, et al. Antibiotic treatment of carbapenem-resistant Acinetobacter baumannii infections in view of the newly developed β-lactams: a narrative review of the existing evidence. Antibiotics. 2024;13(6):506. doi:10.3390/antibiotics13060506
11. El-Ashry AH, Abdrabou AM, El-Tantawy N, et al. In vitro activity of meropenem-vaborbactam combinations and eravacycline against carbapenem-resistant Acinetobacter baumannii. Sci Rep. 2025;15(1):34109. doi:10.1038/s41598-025-19642-y
12. Asai N, Sakanashi D, Suematsu H, et al. Clinical characteristics and relevance of coagulase-negative Staphylococci other than S. epidermidis by positive blood culture. J Microbiol Immunol Infect. 2021;54(4):632–638. doi:10.1016/j.jmii.2020.03.001
13. Howroyd F, Chacko C, MacDuff A, et al. Ventilator-associated pneumonia: pathobiological heterogeneity and diagnostic challenges. Nat Commun. 2024;15(1):6447. doi:10.1038/s41467-024-50805-z
14. Guillamet CV, Kollef MH. Is zero ventilator-associated pneumonia achievable? Updated practical approaches to ventilator-associated pneumonia prevention. Infect Dis Clin North Am. 2024;38(1):65–86. doi:10.1016/j.idc.2023.11.001
15. Geng S, Tang Q, Shi N. Antibiotic-sparing strategies for multidrug-resistant organism (MDRO) infections. Front Pharmacol. 2025;16:1653424. doi:10.3389/fphar.2025.1653424
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Procalcitonin in Predicting Mortality and Organ Dysfunction at Intensive Care Admission
Suranadi IW, Sinardja CD, Suryadi IA
International Journal of General Medicine 2022, 15:4917-4923
Published Date: 12 May 2022
Epidemiological and Antimicrobial Resistant Patterns, and Molecular Mechanisms of Carbapenem-Resistant Klebsiella pneumoniae Infections in ICU Patients
Lu F, Zhang L, Ji J, Xu Y, Wang B, Xia J
Infection and Drug Resistance 2023, 16:2813-2827
Published Date: 9 May 2023
The Clinical Value of Comprehensive Nursing Intervention in Preventing Severe Lymphopenia and Improving the Survival Rate Among Patients with Sepsis
Zhang L, Xu C, Bai L, Li L, Guo J, Li Y
Open Access Emergency Medicine 2023, 15:393-403
Published Date: 21 October 2023
LASSO-Based Identification of Risk Factors and Development of a Prediction Model for Sepsis Patients
Hong C, Xiong Y, Xia J, Huang W, Xia A, Xu S, Chen Y, Xu Z, Chen H, Zhang Z
Therapeutics and Clinical Risk Management 2024, 20:47-58
Published Date: 7 February 2024
Epidemiology and Antimicrobial Resistance Trends of Bloodstream Infections During and After the Implementation of the National Action Plan on Antimicrobial Resistance in Mwanza, Tanzania: A Comparative Cross-Sectional Study
Silago V, Matthews L, Oravcova K, Mshana SE, Seni J, Claus H
Infection and Drug Resistance 2025, 18:4441-4453
Published Date: 29 August 2025