Back to Journals » Open Access Emergency Medicine » Volume 15
The Clinical Value of Comprehensive Nursing Intervention in Preventing Severe Lymphopenia and Improving the Survival Rate Among Patients with Sepsis
Authors Zhang L, Xu C, Bai L, Li L, Guo J, Li Y
Received 4 August 2023
Accepted for publication 12 October 2023
Published 21 October 2023 Volume 2023:15 Pages 393—403
DOI https://doi.org/10.2147/OAEM.S433980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Lin Zhang, Chao Xu, Lin Bai, Lin Li, Jinyan Guo, Yanyi Li
Department of Intensive Care Unit, Heilongjiang Provincial Hospital, Harbin, Heilongjiang, 150036, People’s Republic of China
Correspondence: Yanyi Li, Tel +8615304513567, Email [email protected]
Background: Intensive care unit (ICU) patients with sepsis who experience severe lymphopenia are at a higher risk of mortality, and they serve as a more accurate indicator of bacteremia compared to traditional infection markers.
Aim: Our study aimed to examine the influence of severe lymphopenia on ICU mortality and outcomes in sepsis patients, while also evaluating the clinical significance of comprehensive nursing intervention in preventing severe lymphopenia.
Methods: Patients with sepsis in the ICU at our hospital between January 2015 and January 2021 were split into a control group and a test group.The control group received regular nursing care, while the test group was provided with comprehensive nursing care in addition to the control group. The results encompassed mortality rates of 28 days, mortality rates of 1 year, and lengths of stay in the ICU.
Results: Our attention was directed towards day 4 absolute lymphocyte counts, taking into account the receiver operating characteristic (ROC) outcome. Patients with severe lymphopenia were older, more patients with 2 above comorbidities, higher co-infection rates and SOFA score. In addition, patients with severe lymphopenia required longer days stay in ICU (P< 0.001), and presented with higher 28-day mortality (P=0.038) and 1-year mortality (P=0.004). Patients in control group have a higher incidence of severe lymphopenia (P=0.006), 28-day mortality (P=0.015) and 1-year mortality (P=0.019) compared with the test group.
Conclusion: Comprehensive nursing intervention can prevent the occurrence of severe lymphopenia, improve patients satisfaction and reduce mortality.
Keywords: sepsis, lymphopenia, comprehensive nursing, survival, intensive care unit, ICU
Introduction
Sepsis is a dysregulated host response to infection that causes life-threatening organ failure and has a significant global health cost.1–3 The mortality rate among sepsis patients in the ICU far exceeded that of the general ICU population.4,5 Sepsis is marked by intricate pathophysiology and diverse phenotypes that elicit both proinflammatory and antiinflammatory immune responses.2 Nevertheless, the established principle in sepsis care involves promptly diagnosing the condition, administering antibiotics, and controlling the source of infection prior to identifying any organ dysfunction.6,7
During sepsis, approximately 74% of patients present with lymphopenia,8,9 which can be identified as a potential indicator of ongoing immunosuppression in sepsis patients.Research has shown that the amount of lymphocytes in circulation decreases when sepsis begins and can stay low for as long as 28 days.Earlier research has also indicated a potential correlation between severe lymphopenia and the mortality rate of sepsis patients in the ICU, and they serve as a more accurate indicator of bacteremia compared to traditional infection indicators in the emergency care unit.9–12 Additionally, elderly individuals suffering from severe lymphopenia during severe sepsis exhibit a higher mortality rate.13 Therefore, it is imperative to assess the precise lymphocyte counts while providing regular medical attention.
Routine nursing for ICU patients does not yield positive results in clinical practice.Nurses in the intensive care unit offer intricate evaluations and treatments, intensive interventions, and unwavering nursing attention to critically ill individuals facing life-threatening health issues.14 If we can detect abnormal test indicators, it would improve the nursing level of sepsis in ICU patients.In this setting, nurses employ precise lymphocyte counts as a means of conveying patients’ health issues and susceptibility to sepsis. The utilization of conventional clinical nursing approaches, diverse examination techniques, medication interventions, interventions against patient cognition, psychological condition, and behavior, and even Emergency Medical Services are all included in the complete nurse intervention model.15 Our study aimed to examine the influence of severe lymphopenia on risk factors for ICU mortality and outcomes in sepsis patients, while also evaluating the clinical significance of comprehensive nursing intervention in preventing severe lymphopenia and offering recommendations for its prevention.
Methods
Data Collection
We conducted this research in the ICU at Heilongjiang Provincial Hospital. We registered sepsis patients who met the criteria and were admitted to the ICU during the period of January 2015 to January 2021. The medical ethics committee of Heilongjiang Provincial Hospital gave the green light to this study. The criteria for exclusion encompassed individuals below the age of 18, those diagnosed with immunological disease or receiving immunosuppressant medication within the preceding 30 days prior to admission, patients with a previous history of cerebrovascular epilepsy, mental illness, pregnancy; hematological malignancies; HIV infection; with COVID; and non-consent to the study. The flow chart of patient screening was shown in Figure 1.
 |
Figure 1 Patients screening flow diagram. |
We acquired the baseline patient profiles and infection diagnoses. The SOFA scores were computed for every patient upon admission. For those who were transferred from the ward, the baseline SOFA scores were calculated by comparing those obtained during the ward stay before ICU admission with those obtained during the most recent prior admission or in outpatient clinics for those whose ICU admission came directly from the emergency department.16 A lymphocyte count of less than 1.2 cells/μL × 103 was considered to be lymphopenia, representing the minimum threshold of normalcy within our establishment.Severe lymphopenia was characterized by a lymphocyte count below 0.6 cells/μL × 103, equivalent to half of the minimum threshold for normal.17 The definition of septic shock (Sepsis 3.0) was established based on a consensus of criteria.In this study, our attention was directed towards day 4 absolute lymphocyte counts, taking into account previously published evidence18 and the ROC curve that suggested lymphocyte counts on this particular day would serve as a distinguishing factor between survivors and nonsurvivors. If the patient died before day 4, we used day 2 absolute lymphocyte counts.
Nursing methods, Grouping and Following Up
At the preoperative outpatient clinic, patients who were scheduled to be admitted to the ICU were provided with an information letter and informed consent form. Once they had given their approval, they were requested to fill out the survey a few days prior to their admission to the ICU. Patients who were admitted to the ICU without prior planning were given the information letter and informed consent form either during their stay in the ICU or through their proxy. Once patients had given their informed consent, they were requested to fill out the questionnaire by retrospectively rating their health and recollecting their pre-ICU health status. A self-administered paper-based or online questionnaire was provided depending on patients’ or their proxies’ preferences. Weekly reminders were dispatched, followed by a two-week phone call. Patients who failed to exhibit a response within a 90-day period were disqualified from participating in the study. The patients were then divided into groups according to their willingness and financial situation. Patients were then grouped according to their willingness and financial situation. Enrolled patients were followed-up from ICU admission until hospital discharge, hospital death, or 1 year after hospital discharge. Physical, sequelae, cognitive and emotional problems were assessed and followed up every three months after discharge until 1 year.
Our database including 192 patients with lymphopenia, and the primary diagnosis of sepsis requiring ICU admission were reviewed. The 192 patients who were registered were categorized into a test group (n=98) and a control group (n=94).The control group (n=94) received routine nursing in ICU, while the test group (n=98) received comprehensive nursing intervention based on the general group. The patients in the control group received routine nursing in ICU, including disease monitoring (mainly vital signs observation), position nursing, health education and psychological nursing.19 Based on the approach taken in the control group, a thorough nursing intervention was delivered to the test group. The comprehensive nursing included the following aspects:19,20 (1) Position nursing in bed. Once the patients had regained their vital signs and consciousness, the bedside temperature was increased to 20° - 30° and they were provided with a passive massage. The upper limbs, muscles, and joints were guided in both active and passive activities, with the intensity of the activity determined by their tolerance.Based on the patient’s condition, they were aided in attaining a state of comfort where the head, neck, and shoulders were positioned equidistantly. (2) Nursing with a focus on psychological well-being. Nursing staff had to provide patients with detailed information about the disease, the purpose of the treatment, and any possible adverse reactions. Patients were motivated to confront the illness head-on and to build trust in their approach to treatment. (3) Increased airway maintenance. The airway temperature and humidity of the patients were maintained at a suitable level to guarantee their airway patency. The ventilator parameters were altered for patients with ventilators based on their individual circumstances. The patients were provided with a comprehensive explanation of the proper technique for spitting, and were aided in the process of flipping their bodies. (4) Complication nursing: Observe the wound closely for infection, redness, fever, and pain. Trauma patients should change dressings in time to reduce infection. Strengthen the links of fixed pipes to avert the pipeline from crumbling and air blockage. Drugs that are analgesic and sedative were used to relieve the pain of the patient, relax the patient, and prevent emotional agitation from affecting treatment. The presence of grave bleeding complications, including intracranial hematoma and systemic hemorrhage, was closely observed and promptly addressed. (5) Nutritional support. In light of the patients’ circumstances, appropriate dietary regimens were established; for those who were unable to consume food independently, nasal feeding was implemented.19–21
Outcomes
The main result indicated a mortality rate of 28 days.Additional consequences included a one-year mortality rate and the duration of hospitalization in the ICU. Nursing satisfaction was evaluated by the self-made questionnaire. There were covers service attitude, operation standards, and other items in total with 3 ranks from “satisfied” to “unsatisfied”. The satisfaction rate = (satisfied + generally satisfied)/number of cases ×100%.
Statistical Analysis
SPSS23 was applied to perform statistical analysis. The collected data was visualized using GraphPad Prism 7 and the “R” language. A two-sided t-test with a significance level of 5% is used to determine the power of the primary endpoint weight change.The usage (%) was used to represent the counting data, which was then analyzed using chi-square and expressed as χ2. Meas ± SD was used to represent the measurement data. The measurements were all in accordance with a normal distribution. The independent samples t-test was used to compare the measurement data between the two groups. The Kaplan-Meier method was employed to estimate survival curves, while the Log rank test was utilized to examine disparities among the groups. The creation of a receiver operating characteristic (ROC) plot aimed to demonstrate the predictive power of day 1 and day 4 absolute lymphocyte counts in determining 28-day mortality, with higher AUCs indicating a heightened ability to discriminate.Univariate and multivariate logistic regression analyses were employed to conduct risk factor analysis. The multivariate logistic regression analysis incorporated variables that exhibited statistical significance from the univariate analysis. The Cox regression model was utilized to compute hazard ratios and their corresponding 95% confidence intervals (CIs). P-value < 0.05 was deemed to have statistical significance.
Results
Comparison of Clinical Data of Patients with or Without Severe Lymphopenia
In the course of the study, 192 patients satisfied the criteria for inclusion and exclusion. A ROC plot was generated to demonstrate the capacity of absolute lymphocyte counts from day 1 to day 4 in forecasting 28-day mortality. The results showed that the AUC value of day 4 was the highest, and the difference was statistically significant compared with day 1 (day 1 vs day 4, 0.014) and Day 2 (day 1 vs day 4, 0.013). Although the AUC values of day 3 (AUC=0.656) and day 4 (AUC=0.667) were not statistically different, the AUC values of day 4 were higher (Figure 2). Consequently, we opted to concentrate on the fourth day’s total lymphocyte counts in light of the aforementioned outcome.The baseline characteristics of two groups for the entire patient cohort were reported in Table 1(with or without severe lymphopenia) (Table 1). Seventy-seven patients (40.1%) had severe lymphopenia. The results showed no significant disparities between the groups with and without severe lymphopenia in their general data such as gender, body mass index (BMI), septic shock, smoking, single comorbidity (P>0.05) (Table 1). The patients with severe lymphopenia were older, more patients with 2 above comorbidities, higher co-infection rates and SOFA score. In addition, patients with severe lymphopenia required longer days stay in ICU (P<0.001), and presented with higher 28-day mortality (P=0.038) and 1-year mortality (P=0.004) (Table 2). We also used Kaplan-Meier survival analysis to test the correlation between severe lymphopenia and 28-day mortality, which showed that patients with severe lymphopenia were related to the higher risk of 28-day mortality (P=0.034) (Figure 3).
 |
Table 1 General Clinical Characteristics of Sepsis Patients with Lymphopenia |
 |
Table 2 Comparison of Outcomes of Sepsis Patients with Lymphopenia |
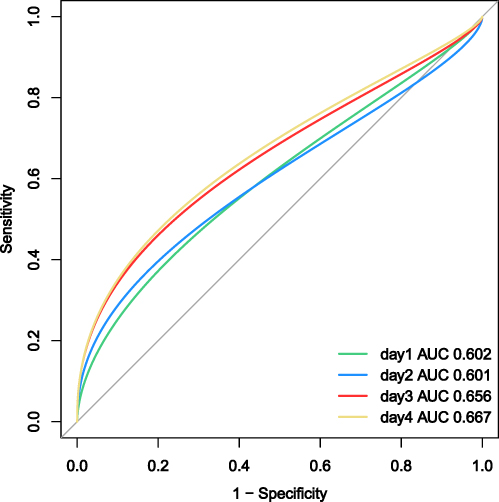 |
Figure 2 Receiver operator characteristic plot comparing the ability of absolute lymphocyte counts on the first 4 days after sepsis diagnosis to predict 28-day mortality. |
 |
Figure 3 Kaplan-Meier survival analysis of the patients with or without severe lymphopenia. |
Comparison of Clinical Data of the Two Nursing Groups
Table 3 reports baseline characteristics before the nursing of the two groups. By closely observing and analyzing the overall clinical data of both the control and test groups, we found no significant differences in terms of age, gender, BMI, comorbidities, septic shock, smoking, co-infection rates and SOFA score between two groups (all P value > 0.05), as shown in Table 3. In Table 4, we also found no significant differences in term of days stay in ICU (P=0.108). In addition, patients in control group have a higher 28-day mortality (P=0.015) and 1-year mortality (P=0.019) compared with the test group (Table 4). We used Kaplan-Meier analysis to test the correlation between nursing methods and 28-day mortality, which also showed that patients in control group have a higher 28-day mortality (P=0.013) (Figure 4).
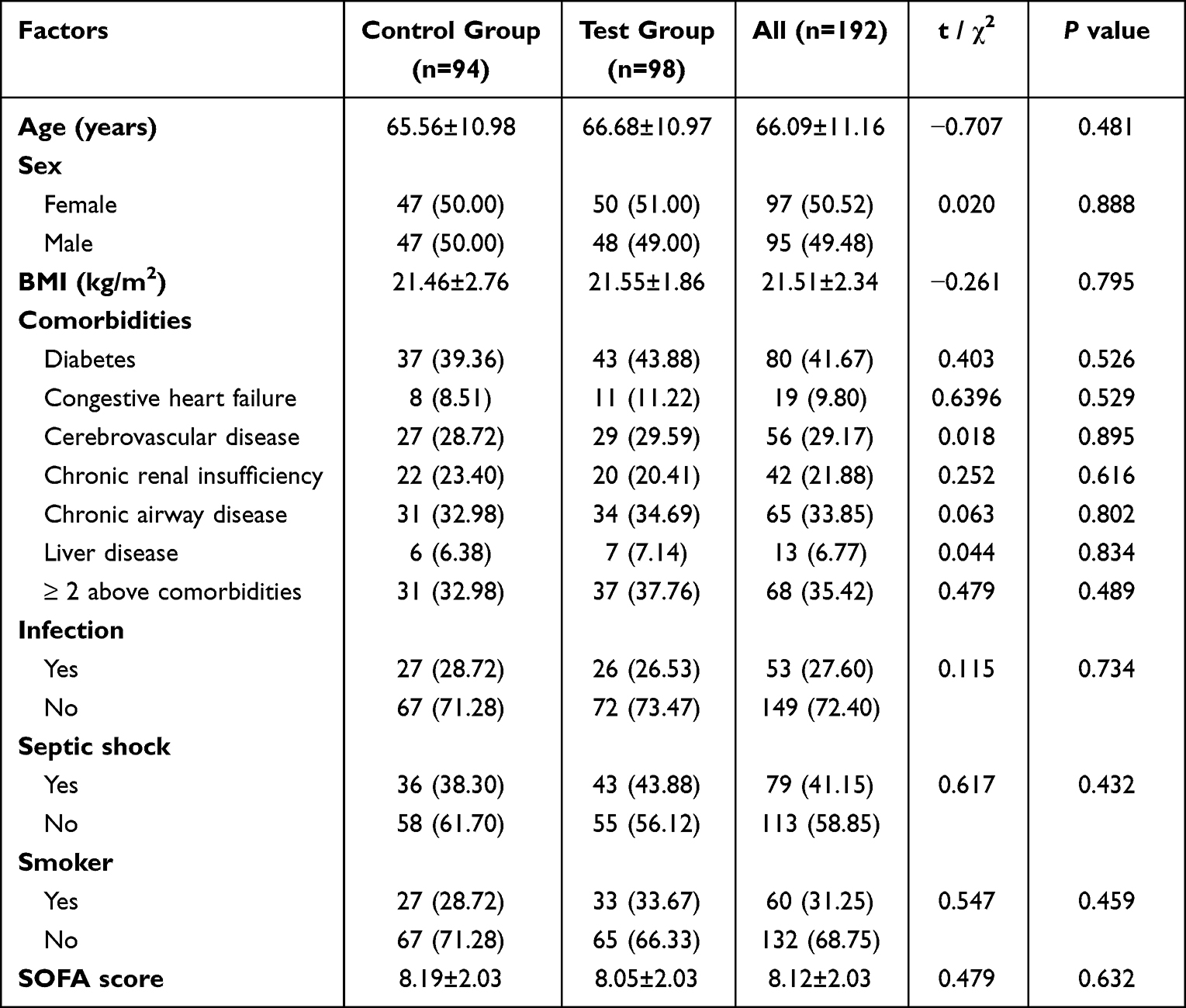 |
Table 3 Comparison of the General Information Between the Two Nursing Groups |
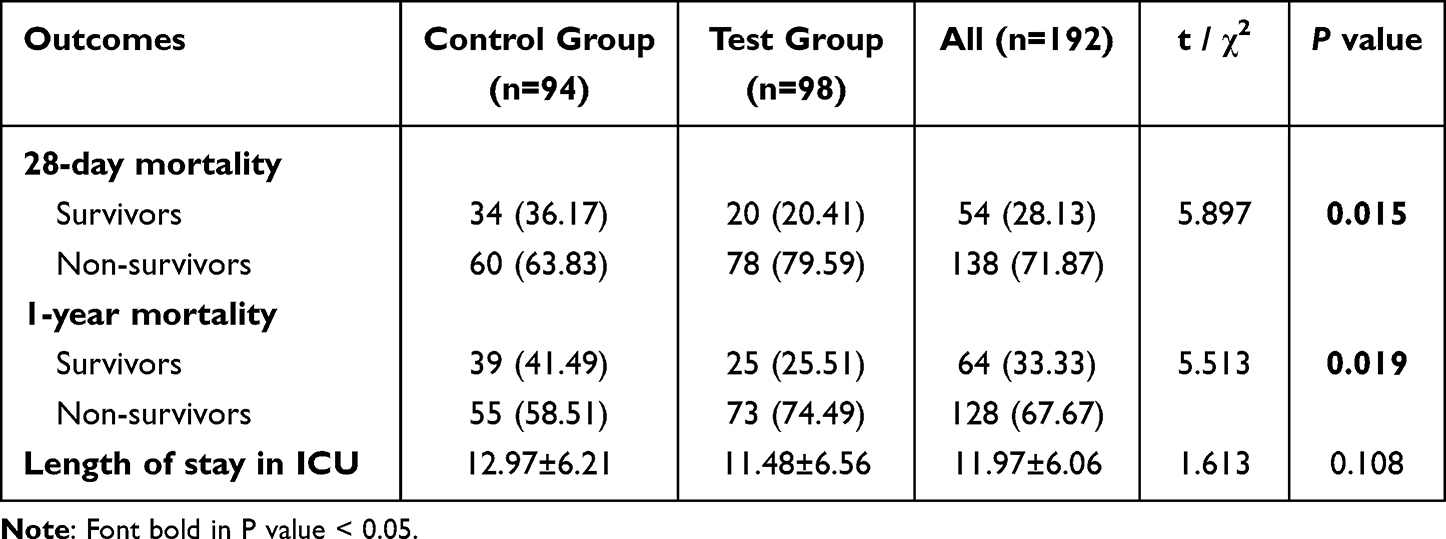 |
Table 4 Comparison of Outcomes of Sepsis Patients in the Two Nursing Groups |
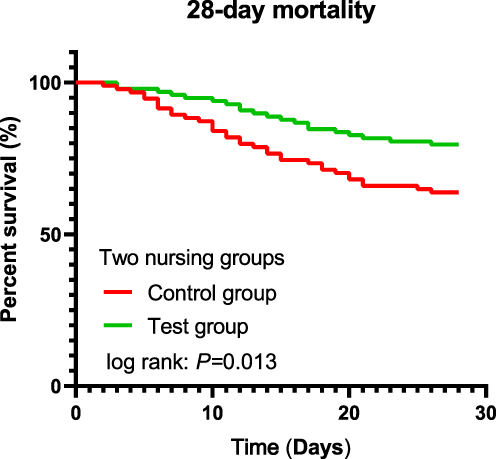 |
Figure 4 Kaplan-Meier survival analysis between the the two nursing groups. |
Severe Lymphopenia and Nursing Satisfaction in the Two Nursing Groups
Univariate and multivariate Cox proportional hazard regression model adjusted for severe lymphopenia was performed based on the terms of age, BMI, comorbidities, smoking, co-infection rates, SOFA score, length stay, and nursing methods in ICU. Comorbidities, nursing methods and co-infection rates were independently related to 28-day mortality (Table 5). In this part, we compared the impact of two nursing methods on lymphocyte count. The test group exhibited a significantly higher average lymphocyte count compared to the control group, as indicated by the results (t=3.401, P=0.0008), (Figure 5). The control group and the test group exhibited no notable disparity in the occurrence of severe lymphopenia upon admission. The control group had a significantly higher percentage of patients with severe lymphopenia than the test group after nursing intervention (50.00% vs 30.61%, P=0.006) (Table 6). The incidence of severe lymphopenia was changed before and after nursing in the control group, but the difference was not significant. And the incidence of severe lymphopenia in the test group after nursing was significantly reduced (P<0.001) (Table 6). The nursing satisfaction was investigated in both groups. The overall satisfaction of 192 patients was 90.63%. It was 94.90% in the test group, which was significantly higher than it was in the control group (86.17%) (P=0.031). More details are shown in Table 7. The above results indicated that the test group had better nursing satisfaction and lower proportion of severe lymphopenia.
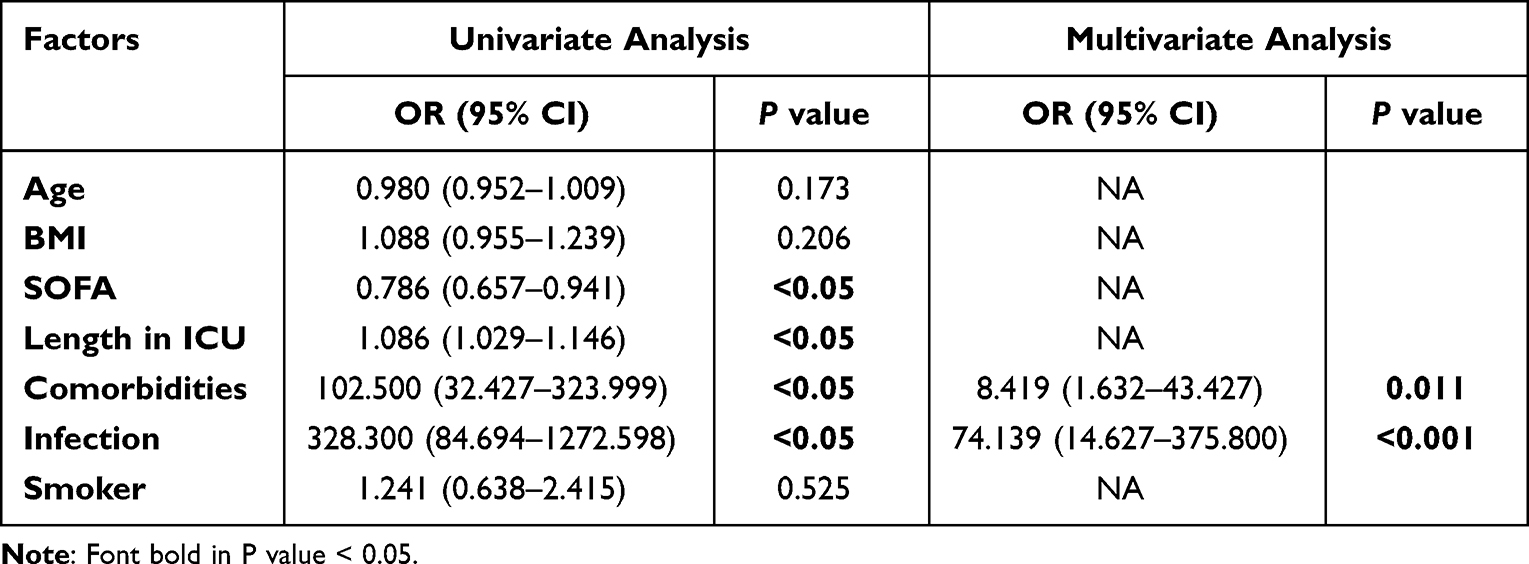 |
Table 5 Cox Proportional Hazard Regression Analysis for 28-Day Mortality |
 |
Table 6 Comparison of the Number of Severe Lymphopenia Between the Two Nursing Groups |
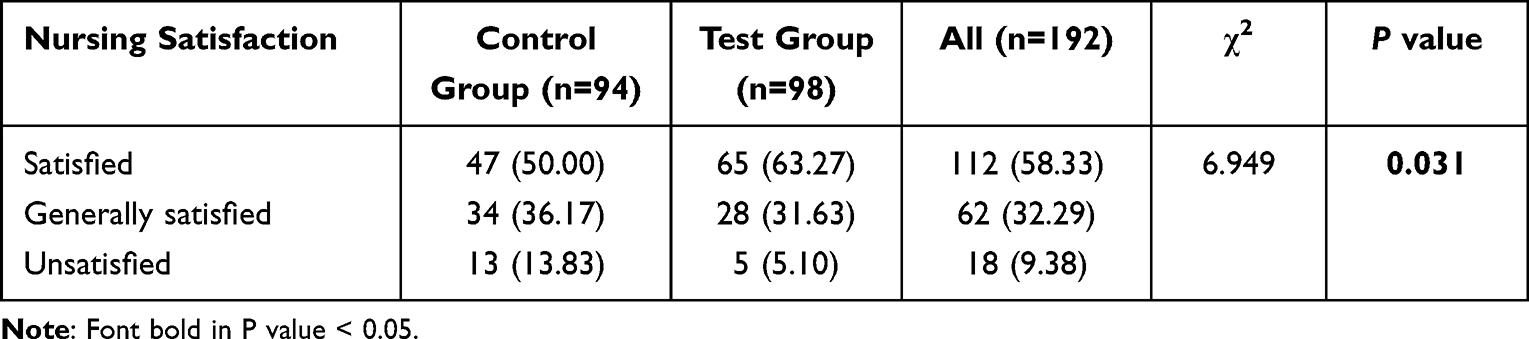 |
Table 7 Comparison of Nursing Satisfaction Between the Two Nursing Groups |
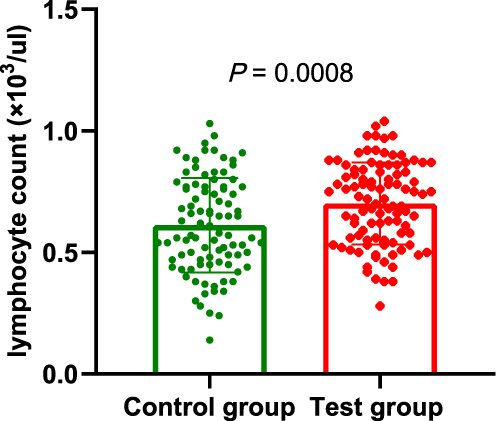 |
Figure 5 The lymphocyte count under the two nursing methods. |
Discussion
Patients with sepsis who experience persistent lymphopenia due to sepsis-induced immunosuppression are at a higher risk of mortality.9 Sepsis triggers both inflammatory and anti-inflammatory processes, which can result in prolonged immunosuppression. Sepsis-induced immunosuppression can lead to the death of immune cells, such as T and B cells, through apoptosis.The presence of persistent lymphopenia has been correlated with elevated chances of mortality and nosocomial infection.22,23 Despite the evidence of lymphopenia in patients treated with induced therapeutic hypothermia, there has been a lack of research on the potential correlation between spontaneous hypothermia and higher mortality rates in sepsis patients. According to a recent study, there was no significant alteration in the circulating lymphocyte counts within 48 hours following admission to the ICU.24 In this single-center retrospective study of 192 randomly selected patients met the inclusion and exclusion criteria with ICU length of stay more than 48 hours. In order to differentiate between survivors and non-survivors after 28 days, ROC curve was performed on lymphocyte counts of first 4 days to distinguish them. Our ROC analysis suggested that day 4 absolute lymphopenia could serve as a more precise discriminatory threshold for accurately predicting 28-day mortality. Although day 3 also showed well predicted results, its AUC value was still lower than day 4. In addition, previous studies have shown that day 4 absolute lymphocyte counts have the ability to differentiate between survivors and non-survivors.25 Our results also fully verified the accuracy of the previous studies. Consequently, we identified severe lymphopenia by analyzing the hemogram findings on the fourth day of ICU admission. The findings of this study demonstrated a correlation between severe lymphopenia and the elevated mortality rate of 28 days per year in sepsis, and the result was consistent with previous reports.26
Inadequate nourishment may be a factor in the emergence of lymphopenia in hospitalized individuals. Despite this, our patients with severe lymphopenia during sepsis did not experience a decline in their nutritional status. No significant difference in BMI was observed between patients with severe lymphopenia and those without in this study. There were no remarkable differences between the groups with and without severe lymphopenia in terms of general data such as gender, septic shock, smoking and single comorbidity. However, we also found that severe lymphopenia was associated with higher age, co-infection rates and SOFA score. Patients with severe lymphopenia are more prone to experiencing a decline in physiological function, reduced metabolic capacity, low drug tolerance, and poor psychological stress ability,27 so it is more likely to happen in the patients with severe lymphopenia, and it is also consistent with the results of our study.
A new patient-centered nursing model, known as comprehensive nursing intervention, has the potential to significantly enhance patient nursing services through the utilization of multiple resources.15 After position nursing, lower extremity venous thrombosis may be mostly prevented; psychological nursing interventions can increase patient confidence and treatment compliance and are better for the advancement of nursing practice. After enhanced airway nursing, the co-infection rate of respiratory tract and the utilization rate of ventilator were significantly reduced. As a result of long-term braking of patients, the sarcolysis in those receiving mechanical ventilation rises, leading to a decrease in muscle protein synthesis levels, therefore nutritional support is very important. The two nursing groups showed no significant difference in general information when we carried out comprehensive nursing interventions for people in the test group. A previous comparative study showed that additional nursing has a better nursing effect on ICU patients and can significantly improve the psychological state, satisfaction, and other indicators of ICU patients.28 In order to further clarify the influence of nursing methods on lymphocyte count, we compared the average value of lymphocyte count between two nursing methods through t test. The results showed that the lymphocyte count in patients with general nursing was significantly lower than that in the comprehensive nursing group, which firstly suggested that nursing methods played an important role in the prevention of lymphopenia. Then, compared with general nursing in our research, comprehensive nursing has been found to have a remarkable impact on improving the prognosis of ICU patients, leading to a decrease in severe lymphopenia and an increase in patient satisfaction with clinical nursing. Our results indicating the significant intervention effect of comprehensive nursing.
Our research is not without its drawbacks. The research was conducted at a solitary facility.The study group consisted of a diverse group of medical and surgical patients, varying in age and conditions, who necessitated intensive care in the intensive care unit. The selection bias could have an impact on the cohort size, which was restricted due to the 12-month follow-up period. The nursing methods for lymphopenia that have been validated in our center should be confirmed and validated in future studies to increase external validity.
Conclusions
To sum up, patients with severe lymphopenia counts during severe sepsis experienced higher mortality rates and longer stays in the ICU. The nursing effect of comprehensive nursing on ICU sepsis patients is significantly better than general nursing alone. The former yields a notably superior outcome in enhancing patient contentment and diminishing mortality rates.
Declaration
This study was approved by the medical ethics committee of Heilongjiang Provincial Hospital (ID: 2021088). Our study complies with the Declaration of Helsinki.
Data Sharing Statement
All data obtained and/or analyzed in this study were available from the corresponding authors in a reasonable request.
Acknowlegments
We extend our heartfelt appreciation to everyone who assisted us in the composition of this manuscript.
Author Contributions
All authors contributed significantly to the work that was published, whether it be in the ideation, study design, implementation, data collection, analysis, and interpretation, or in all of these areas. They also all participated in writing, revising, or critically evaluating the article, gave their final approval for the version that would be published, agreed on the journal to which the article would be submitted, and agreed to be responsible for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169–1176. doi:10.1097/CCM.0000000000003817
2. Cohen J, Vincent JL, Adhikari NK, et al. Sepsis: a roadmap for future research. Lancet Infect Dis. 2015;15(5):581–614. doi:10.1016/S1473-3099(15)70112-X
3. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45:486–552. doi:10.1097/CCM.0000000000002255
4. Vincent JL, Marshall JC, Namendys-Silva SA, et al. Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. 2014;2:380–386. doi:10.1016/S2213-2600(14)70061-X
5. Reinhart K, Daniels R, Kissoon N, Machado FR, Schachter RD, Finfer S. Recognizing sepsis as a global health priority-a WHO resolution. N Engl J Med. 2017;377(5):414–417. doi:10.1056/NEJMp1707170
6. Shankar-Hari M, Fear D, Lavender P, et al. Activation-associated accelerated apoptosis of memory B cells in critically Ill patients with sepsis. Crit Care Med. 2017;45:875–882. doi:10.1097/CCM.0000000000002380
7. Perner A, Rhodes A, Venkatesh B, et al. Sepsis: frontiers in supportive care, organisation and research. Intensive Care Med. 2017;43(4):496–508. doi:10.1007/s00134-017-4677-4
8. Castelino DJ, McNair P, Kay TW. Lymphocytopenia in a hospital population what does it signify? Aust N Z J Med. 1997;27(2):170–174. doi:10.1111/j.1445-5994.1997.tb00934.x
9. Drewry AM, Samra N, Skrupky LP, Fuller BM, Compton SM, Hotchkiss RS. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014;42(5):383–391. doi:10.1097/SHK.0000000000000234
10. Hamilton F, Arnold D, Payne R. Association of prior lymphopenia with mortality in pneumonia: a cohort study in UK primary care. Br J Gen Pract. 2021;71:e148–56. doi:10.3399/bjgp20X713981
11. Lewis RT, Klein H. Risk factors in postoperative sepsis: significance of preoperative lymphocytopenia. J Surg Res. 1979;26(4):365–371. doi:10.1016/0022-4804(79)90021-0
12. de Jager C, van Wijk P, Mathoera RB, de Jongh-Leuvenink J, van der Poll T, Wever PC. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Critical Care. 2010;14(5):R192. doi:10.1186/cc9309
13. Inoue S, Suzuki-Utsunomiya K, Okada Y, et al. Reduction of immunocompetent T cells followed by prolonged lymphopenia in severe sepsis in the elderly. Crit Care Med. 2013;41(3):810–819. doi:10.1097/CCM.0b013e318274645f
14. Thoroddsen A, Ehnfors M, Nurs ED, Ehrenberg A. Nursing specialty knowledge as expressed by standardized nursing languages. Internat J Nurs Terminol Classif. 2010;21(2):69–79. doi:10.1111/j.1744-618X.2010.01148.x
15. Maurya S, Mishra SB, Azim A, Baronia AK, Gurjar M. Ventilator-associated complications: a study to evaluate the effectiveness of a planned teaching program for intensive care unit staff nurses-an Indian experience. Am J Infect Control. 2016;44:1422–1423. doi:10.1016/j.ajic.2016.03.008
16. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the european society of intensive care medicine. Intensive Care Med. 1996;22:707–710. doi:10.1007/BF01709751
17. Levy MM, Fink MP, Marshall JC, et al. International Sepsis Definitions Conference: 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 2003;29(4):530–538. doi:10.1007/s00134-003-1662-x
18. Thompson K, Venkatesh B, Finfer S, et al. Sepsis and septic shock: current approaches to management. Intern Med J. 2019;49(1):160–170. doi:10.1111/imj.14199
19. Jiang XL, Zhang PN. The role of nursing in the diagnosis and treatment of severe sepsis. Med J Qilu. 2005;6:559–560.
20. Yue CR, Lu P, Liu LZ. Analysis of nursing effect of comprehensive nursing intervention on patients with bronchial asthma. Cap Food Med. 2018;25:63.
21. Yuan LJ, Meng L. Effect of comprehensive nursing intervention on negative emotion and quality of life of elderly patients with stable chronic obstructive pulmonary disease. Shanxi Med J. 2020;49:359–361.
22. Kaya T, Açıkgöz SB, Yıldırım M, Nalbant A, Altaş AE, Cinemre H. Association between neutrophil-to-lymphocyte ratio and nutritional status in geriatric patients. J Clin Lab Anal. 2019;33(1):e22636. doi:10.1002/jcla.22636
23. Manzoli TF, Delgado AF, Troster EJ, et al. Lymphocyte count as a sign of immunoparalysis and its correlation with nutritional status in pediatric intensive care patients with sepsis: a pilot study. Clinics. 2016;71(11):644–649. doi:10.6061/clinics/2016(11)05
24. Venet F, Davin F, Guignant C, et al. Early assessment of leukocyte alterations at diagnosis of septic shock. Shock. 2010;34(4):358–363. doi:10.1097/SHK.0b013e3181dc0977
25. Chung KP, Chang HT, Lo SC, et al. Severe lymphopenia is associated with elevated plasma interleukin-15 levels and increased mortality during severe sepsis. Shock. 2015;43(6):569–575. doi:10.1097/SHK.0000000000000347
26. Von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. for the STROBE initiative: the strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Int Med. 2007;147(8):573–577. doi:10.7326/0003-4819-147-8-200710160-00010
27. Dai HL, Liu XL, Feng DJ, Li R, Shen HY. Evidence-based nursing combined with cognitive function training can reduce the incidence of delirium in ICU patients and improve their cognitive function. Am J Transl Res. 2021;13(4):3262–3269.
28. Song J, Liu D, Zhang M, Wang H, Tan S. Intermittent theta burst stimulation (Itbs) combined with working memory training to improve cognitive function in schizophrenia: study protocol for a randomized controlled trial. Trials. 2020;21:683. doi:10.1186/s13063-020-04563-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Role of Procalcitonin in Predicting Mortality and Organ Dysfunction at Intensive Care Admission
Suranadi IW, Sinardja CD, Suryadi IA
International Journal of General Medicine 2022, 15:4917-4923
Published Date: 12 May 2022
LASSO-Based Identification of Risk Factors and Development of a Prediction Model for Sepsis Patients
Hong C, Xiong Y, Xia J, Huang W, Xia A, Xu S, Chen Y, Xu Z, Chen H, Zhang Z
Therapeutics and Clinical Risk Management 2024, 20:47-58
Published Date: 7 February 2024
Correlation of Neutrophil-Lymphocyte Ratio and Critical Illness in Adults on Vancomycin: A Cross-Sectional Study
Alfhili MA, Alazmi SA, Alsughayyir JM
International Journal of General Medicine 2025, 18:4157-4167
Published Date: 31 July 2025
Retrospective Analysis of Infection Characteristics and Prognostic Factors in ICU Sepsis Patients in Jiaxing Area
Li H, Tan X, Wang S, Shen W, Yuan B
Infection and Drug Resistance 2026, 19:576517
Published Date: 8 April 2026
Development and Internal Validation of a Nomogram Model to Predict Invasive Pulmonary Aspergillosis Occurrence Risk in ICU Patients with Sepsis
Li H, Liang Y, Xiao W, Zheng Y, Hua T, Yang M
Infection and Drug Resistance 2026, 19:603823
Published Date: 25 May 2026