Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Real-World Evidence for Combination Sedation: Propofol Plus Dexmedetomidine and Clinical Outcomes in Mechanically Ventilated ICU Patients
Authors Qi J ![]() , Gao W
, Gao W ![]() , Ni Q, Liang Z, Wang W, Qiao T, Wang B
, Ni Q, Liang Z, Wang W, Qiao T, Wang B
Received 19 January 2026
Accepted for publication 11 May 2026
Published 27 May 2026 Volume 2026:22 597422
DOI https://doi.org/10.2147/TCRM.S597422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandeep Ajoy Saha
Jialin Qi,1,* Weihua Gao,2,* Qian Ni,1 Zishun Liang,1 Wei Wang,3 Tong Qiao,1,* Baoyan Wang4,*
1Department of Vascular Surgery, Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, Jiangsu, People’s Republic of China; 2School of Basic Medicine and Clinical Pharmacy, China Pharmaceutical University, Nanjing, Jiangsu, People’s Republic of China; 3Interventional Department, Qujing Second People’s Hospital of Yunnan Province, Qujing, Yunnan, People’s Republic of China; 4Department of Pharmacy, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baoyan Wang, Department of Pharmacy, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China, Tel +86-15161477178, Email [email protected]
Purpose: This retrospective multicenter cohort study evaluated the real-world effectiveness of propofol alone versus a propofol-plus-dexmedetomidine combination on clinical outcomes in mechanically ventilated ICU patients.
Methods: Adult mechanically ventilated ICU patients receiving long-term continuous infusion sedation (≥ 48 h) with either propofol alone or propofol plus dexmedetomidine were identified from the MIMIC-IV and eICU databases. An external validation cohort from Nanjing Drum Tower Hospital (2013– 2022) was assembled using the same eligibility criteria. Patients were categorized into a propofol monotherapy group (Pro) and a propofol plus dexmedetomidine group (Pro+Dex). Outcomes included 28–day all-cause mortality, incident delirium, ICU length of stay, duration of mechanical ventilation, and longitudinal changes in mean arterial pressure, heart rate, and oxygen saturation.
Results: Among 5495 patients (Pro: n=4730; Pro+Dex: n=765), the Pro+Dex regimen was associated with lower 28-day mortality (adjusted HR: 0.45, 95% CI: 0.36– 0.56; P < 0.001) and a markedly reduced incidence of delirium (adjusted OR: 0.28, 95% CI: 0.21– 0.37; P < 0.001), but with a modestly longer ICU stay (13.07 vs 10.60 days; adjusted ratio: 1.23, 95% CI: 1.18– 1.29). Mechanical ventilation duration did not differ significantly between groups (154.79 vs 157.64 hours; adjusted ratio: 0.98, 95% CI: 0.92– 1.05). Longitudinal mixed-effects models suggested a more stable MAP trajectory and lower HR with Pro+Dex, while SpO2 was slightly lower on average but remained stable over time. Subgroup analyses were broadly consistent with the overall cohort. In the external validation cohort, Pro+Dex was also associated with significantly lower 28-day mortality, whereas the reduction in delirium incidence did not reach statistical significance.
Conclusion: In this large real-world multicenter study, combination sedation with propofol and dexmedetomidine was associated with lower 28-day mortality and a lower risk of delirium, without a significant difference in mechanical ventilation duration, although ICU length of stay was modestly longer.
Keywords: sedation, propofol, dexmedetomidine, mechanical ventilation
Introduction
Mechanical ventilation (MV) is a cornerstone life-support intervention in the intensive care unit (ICU).1 By maintaining adequate gas exchange in patients with respiratory failure, severe infection, or multiple organ dysfunction, MV has become a cornerstone of modern critical care and has substantially improved survival.2 However, its implementation is often complicated by anxiety, agitation, discomfort, and patient-ventilator asynchrony, which can precipitate accidental extubation, hemodynamic instability, and treatment failure.3 To address these challenges, sedation is routinely administered to improve patient comfort, facilitate ventilator synchrony, and minimize adverse events, thereby ensuring the safe and effective delivery of MV.4
The choice of sedative agent can significantly influence patient outcomes, including the duration of mechanical ventilation, the incidence of delirium, and ICU length of stay.5 Propofol, one of the most commonly used sedatives in the ICU, provides rapid onset and easy titration, but its use may be limited by dose-dependent hypotension and myocardial depression.6 These effects are particularly concerning in mechanically ventilated patients with hemodynamic instability, such as those with septic shock, acute respiratory distress syndrome (ARDS), or decompensated heart failure.7,8 Dexmedetomidine, a selective α2-adrenergic agonist, offers light, arousable sedation with minimal respiratory depression.9 It has been associated with a reduced incidence of ICU delirium and may provide more favorable hemodynamic stability compared with γ-aminobutyric acid (GABA)-ergic agents.10 Because propofol and dexmedetomidine have distinct pharmacologic profiles, combining these agents may allow dose reduction of each drug while maintaining effective sedation.11 However, dexmedetomidine is also associated with adverse effects such as bradycardia and delayed recovery related to its context-sensitive half-life.12 In addition, prolonged or dual-agent sedation may be associated with longer ICU stays and greater resource utilization.13 Although several studies have evaluated dexmedetomidine-based sedation strategies in critically ill patients, direct comparative evidence between propofol monotherapy and a propofol-dexmedetomidine combination strategy in mechanically ventilated ICU populations remains limited. Existing studies have also been constrained by modest sample sizes, narrower comparator frameworks, or limited assessment of clinically relevant outcomes.
Therefore, we conducted a retrospective multicenter cohort study using two large public critical care databases and an independent hospital cohort to compare propofol monotherapy with propofol plus dexmedetomidine in mechanically ventilated ICU patients. We aimed to evaluate their associations with 28-day all-cause mortality, delirium, ICU length of stay, duration of mechanical ventilation, and longitudinal trajectories of hemodynamic and oxygenation parameters.
Methods
Study Design and Data Source
This retrospective multicenter cohort study utilized data from two large, publicly available critical care databases and an additional cohort from a large tertiary teaching hospital in China (Nanjing Drum Tower Hospital): MIMIC-IV (version 3.1, Beth Israel Deaconess Medical Center, 2008–2022) and the eICU Collaborative Research Database (eICU-CRD, version 2.0, 2014–2015). Access to both databases was granted after completion of the required National Institutes of Health (NIH) and Collaborative Institutional Training Initiative (CITI) courses on human research protection. The use of these de-identified public datasets was approved by the institutional review boards of the contributing institutions, with a waiver of individual informed consent owing to the retrospective and anonymized nature of the databases. The study utilizing data from Nanjing Drum Tower Hospital was approved by the Institutional Ethics Committee of Nanjing Drum Tower Hospital (Approval Number: 2023–488-02). Patient consent to review their medical records was not required by the Institutional Ethics Committees of Nanjing Drum Tower Hospital because this was a retrospective study using existing clinical records. Patient data confidentiality was strictly protected throughout the study. The study protocol complied with the Declaration of Helsinki.
Study Population and Eligibility Criteria
Patients were eligible for inclusion if they were adults aged 18 years or older at ICU admission and met all of the following criteria: (1) admission to an intensive care unit with receipt of invasive mechanical ventilation; (2) initiation of continuous intravenous sedation with propofol, either as monotherapy or in combination with dexmedetomidine; and (3) continuation of mechanical ventilation under the same sedation strategy for at least 48 consecutive hours after sedation initiation. A landmark design was applied, and cohort entry was defined as the 48-hour landmark time after sedation initiation to ensure stable classification of sedation strategy and appropriate temporal alignment between exposure and outcome follow-up. This approach is consistent with landmark analysis methodology for handling time-dependent treatment classification and reducing time-related bias.14
Patients were excluded if they met any of the following criteria: (1) age <18 years at ICU admission; (2) multiple ICU admissions during the same hospitalization (only the first ICU stay was included); or (3) discontinuation of invasive mechanical ventilation, ICU discharge, or death within the first 48 hours after sedation initiation, precluding assignment to a stable sedation strategy. Patients who did not survive to the predefined landmark time were not eligible for cohort entry, as outcome follow-up was initiated only after exposure classification was complete.
Exposure Definition and Covariate Collection
The primary exposure of interest was the ICU sedation strategy, defined according to the use of propofol either as monotherapy or in combination with dexmedetomidine during mechanical ventilation. In routine ICU practice, dexmedetomidine is commonly initiated as part of a planned multimodal sedation approach rather than exclusively as a rescue agent. Accordingly, this study aimed to compare two clinically meaningful sedation strategies instead of isolated drug exposure.
Sedation regimens were classified into two mutually exclusive groups. The propofol monotherapy group (Pro) consisted of patients who received continuous intravenous propofol infusion without any overlapping administration of dexmedetomidine during the exposure window. The combination sedation group (Pro+Dex) included patients who received concurrent continuous infusions of propofol and dexmedetomidine with a sustained overlap of at least 48 consecutive hours, ensuring stable exposure to the combination strategy and excluding transient or intermittent add-on use.
Consistent with the landmark design used for cohort entry, exposure classification was based on sedation administered during the first 48 hours after sedation initiation. Only patients who remained invasively mechanically ventilated and continued the same sedation strategy throughout this 48-hour window were eligible for exposure assignment. The index time for outcome follow-up was defined as the 48-hour landmark time after sedation initiation, thereby ensuring temporal alignment between exposure definition and subsequent outcome assessment.
Sedative medications were identified using medication administration and infusion records from the MIMIC-IV and eICU Collaborative Research Database, as well as electronic medical records from Nanjing Drum Tower Hospital. For each sedative agent, start and stop times of infusion episodes were extracted to determine exposure duration and overlap. Data extraction was performed using Structured Query Language (SQL) in PostgreSQL (version 8.2) and managed with Navicat Premium (version 17). The following variables were collected for each patient: (1) Demographic characteristics: age, sex, body mass index (BMI), and race; (2) Comorbidities: hypertension, sepsis, coronary artery disease (CAD), diabetes mellitus, chronic obstructive pulmonary disease (COPD), arrhythmia and ischemic stroke; (3) Medication exposure during the ICU stay: analgesics (eg, fentanyl, morphine), other sedatives (eg, midazolam, lorazepam), antihypertensive agents (eg, calcium channel blockers, angiotensin-converting enzyme inhibitors, and angiotensin II receptor blockers, diuretics), β-adrenoceptor antagonists (β-blockers), and vasoactive agents; (4) Severity of illness and comorbidity burden were evaluated using the Acute Physiology Score III (APS III) score and Charlson Comorbidity Index (CCI), respectively. In MIMIC-IV, both APS III score and CCI were available in dedicated tables and were extracted directly. APS III score was based on the first measurements recorded after ICU admission. In eICU-CRD, APS III score was derived from the severity scoring table using initial ICU data. Since eICU-CRD did not provide a predefined CCI, the CCI for each patient was calculated retrospectively from documented diagnostic codes and relevant laboratory findings according to the standard Charlson algorithm. For the Nanjing Drum Tower Hospital cohort, APS III and CCI were likewise computed in accordance with internationally accepted scoring standards; (5) Laboratory parameters: serum creatinine and creatinine clearance (CrCl). Renal function was estimated using the Cockcroft-Gault formula. This formula may overestimate or underestimate renal function in patients with extreme body composition; (6) Average propofol infusion rate: calculated as the total cumulative propofol dose divided by the duration of propofol infusion (hours) and body weight, yielding a weight-standardized average rate (mg/kg/h). Patients were categorized into quartiles (Q1–Q4) based on the interquartile range of infusion rates to form propofol dose groups. Duration of propofol administration (hours): defined as the total time interval during which continuous propofol infusion was recorded, from the initiation to the discontinuation of propofol administration; (7) Physiological data: baseline mean arterial pressure (MAP), oxygen saturation (SpO2), and heart rate (HR), defined as the first recorded measurements during ICU admission.
Clinical Endpoints
The primary outcome was 28-day all-cause mortality, defined as death from any cause occurring within 28 days after cohort entry (ie, the 48-hour landmark time after sedation initiation). Secondary outcomes included incident delirium, ICU length of stay, duration of mechanical ventilation, and longitudinal changes in physiological parameters. Incident delirium was defined as the first occurrence of delirium after cohort entry (the 48-hour landmark time) among patients without documented delirium before that time. In MIMIC-IV and eICU, delirium was identified using structured CAM-ICU assessments, whereas in the Nanjing Drum Tower Hospital cohorts, delirium was ascertained based on available clinician documentation. ICU length of stay (days) and duration of mechanical ventilation (hours) were assessed as post-exposure utilization outcomes and interpreted in the context of survival. To evaluate the temporal effects of sedation strategies on physiological stability, MAP, HR, and SpO2 were extracted at 4-hour intervals after cohort entry during ongoing sedation and mechanical ventilation. The average value within each interval was calculated for longitudinal modeling.
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate, and categorical variables were presented as counts and percentages. Baseline characteristics between sedation strategy groups were compared using the t test or Mann–Whitney U-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. Standardized mean differences (SMDs) were calculated to assess baseline balance, with an SMD < 0.1 considered indicative of acceptable balance.
All time-to-event and regression analyses were anchored at cohort entry, defined as the 48-hour landmark time after sedation initiation. This landmark approach ensured that sedation strategy classification was completed before follow-up began, thereby improving temporal alignment between exposure assignment and outcome assessment and reducing the risk of immortal time bias.
Missing values in baseline covariates and laboratory variables were handled using multiple imputation by chained equations (MICE) under the assumption of missing at random. Variables included in the imputation model comprised all baseline demographic characteristics, comorbidities, illness severity scores, laboratory measurements, physiological parameters, exposure indicators, and outcomes. Five imputed datasets were generated, and estimates were pooled using Rubin’s rules to obtain final effect estimates and standard errors.
The primary outcome, 28-day all-cause mortality, was analyzed using Kaplan–Meier survival curves and compared between groups using the Log rank test. Multivariable Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for the association between sedation strategy and mortality. Proportional hazards assumptions were assessed using Schoenfeld residuals and were not materially violated. Covariate adjustment was performed using a hierarchical modeling strategy: Model 1 adjusted for demographic variables; Model 2 additionally adjusted for comorbidities, renal function, and concomitant medications; and Model 3 further adjusted for illness severity (APS III), CCI, and baseline physiological parameters (MAP, HR, and SpO2). Multicollinearity among covariates was assessed using variance inflation factors (VIFs), with no evidence of problematic collinearity observed.
Incident delirium was analyzed using multivariable logistic regression models and reported as odds ratios (ORs) with 95% CIs. Delirium analyses were restricted to patients without documented delirium prior to cohort entry. Logistic regression was chosen because the exact timing of delirium onset was not uniformly available across datasets, particularly in the eICU-CRD and external validation cohort. The same hierarchical covariate adjustment strategy used for the mortality analyses was applied.
ICU length of stay (days) and duration of mechanical ventilation (hours) were analyzed as post-exposure healthcare utilization outcomes using generalized linear models (GLMs) with a Gamma distribution and log-link function, given their right-skewed distributions and strictly positive values. Adjusted predicted mean values and ratios comparing the Pro+Dex and Pro groups were estimated with corresponding 95% CIs. These outcomes were interpreted in the context of survival rather than as direct causal effects.
To evaluate longitudinal changes in physiological parameters, linear mixed-effects models (LMMs) were fitted for MAP, HR, and SpO2. Repeated measurements were extracted at 4-hour intervals after cohort entry during ongoing sedation and invasive mechanical ventilation. Time, sedation strategy, and their interaction were included as fixed effects, with random intercepts and random slopes for time specified at the patient level to account for within-subject correlation. Models were estimated using restricted maximum likelihood (REML), and model adequacy was assessed using residual diagnostics and Akaike Information Criterion (AIC). Model-based predicted trajectories and 95% CIs were generated for visualization.
Prespecified subgroup analyses were conducted to explore the consistency of associations across clinically relevant strata, including age (≤ 65 vs > 65 years), sex, renal function (CrCl ≥ 90, 30–89, < 30 mL/min), APS III score (≤ 70 vs > 70), CCI (≤ 4 vs > 4), presence of sepsis, and propofol infusion rate categories. Interaction terms between sedation strategy and subgroup variables were incorporated into regression models to assess effect modification.
Sensitivity analyses were performed to evaluate the robustness of the primary findings and included: (1) propensity score-matched analyses using 1:2 nearest-neighbor matching with a caliper of 0.05; (2) analyses stratified by data source (MIMIC-IV vs eICU-CRD); and (3) multivariable Cox regression models for ICU mortality. External validation was conducted using an independent cohort from Nanjing Drum Tower Hospital with harmonized eligibility criteria and variable definitions. These additional analyses were intended to assess the consistency and robustness of the observed associations rather than to generate independent causal estimates.
All statistical analyses were performed using R software (version 4.5.0). A two-sided P value <0.05 was considered statistically significant.
Results
Patient Characteristics
A total of 5495 mechanically ventilated ICU patients were included, comprising 4730 in the Pro group and 765 in the Pro+Dex group (Table 1). Among these patients, 1890 were from the MIMIC-IV database and 3605 were from the eICU database (Table S1). Additionally, an external validation cohort from Nanjing Drum Tower Hospital included 731 patients, with 224 in the Pro group and 507 in the Pro+Dex group (Table S2). Overall, patients in the Pro+Dex group were younger and had a lower proportion of females. The distribution of comorbidities was largely comparable between groups, except for a lower prevalence of diabetes mellitus in the Pro+Dex group. Notably, the Pro+Dex group showed higher use of concomitant medications, including analgesic, other sedatives, antihypertensives, β-blockers, and vasoactive agents. Patients in the Pro+Dex group had a longer duration of propofol infusion and were more frequently classified in the highest quartile of infusion rate (≥ 1.18 mg/kg/h). Better renal function (CrCl ≥ 90 mL/min) and a lower CCI were observed in the Pro+Dex group, whereas APS III scores were comparable between the two groups. Baseline physiological parameters were largely comparable, except for a slightly higher heart rate in the Pro+Dex group.
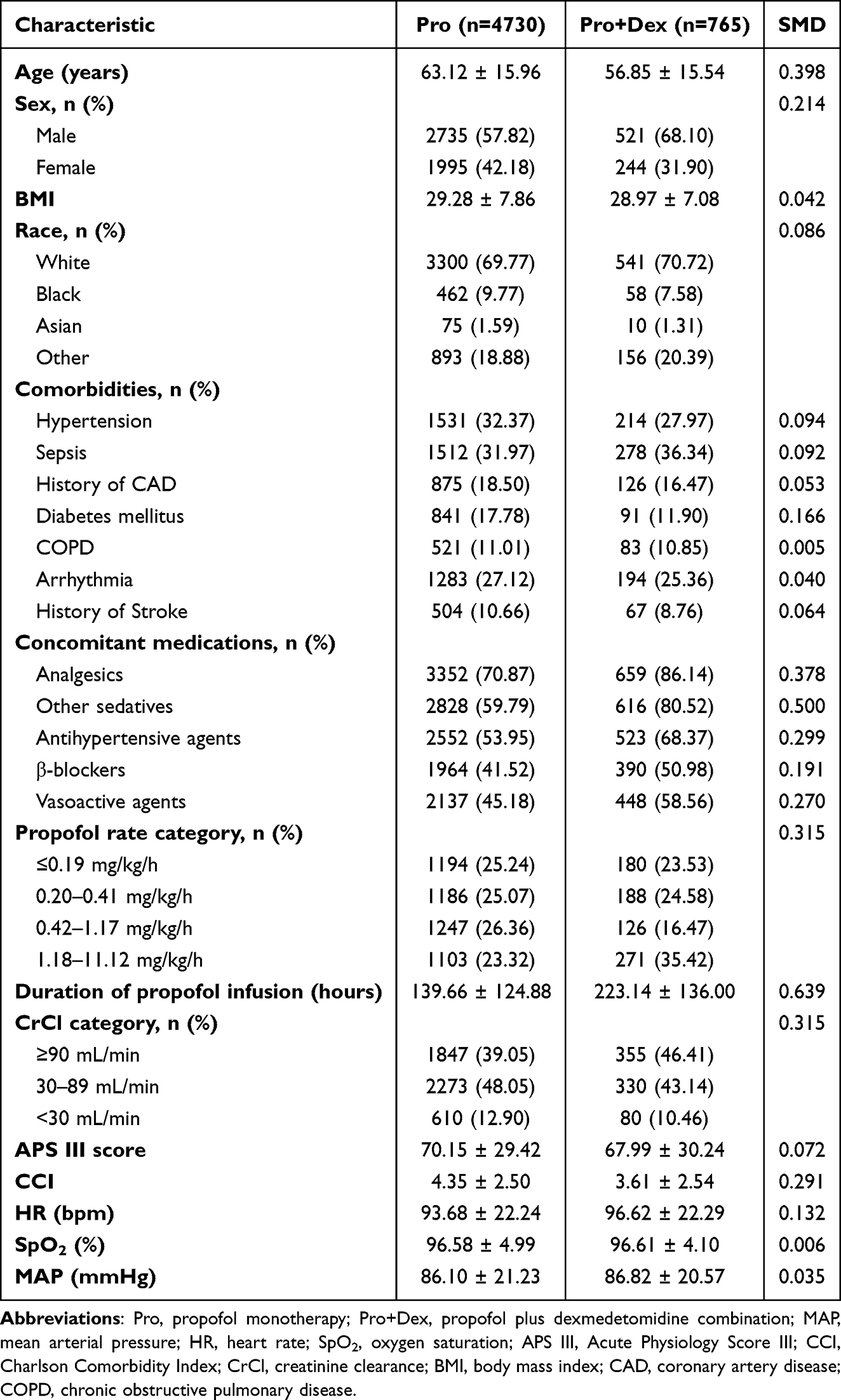 |
Table 1 Baseline Characteristics of the Study Population |
Study Outcomes
Figure 1A shows the Kaplan-Meier survival curves for 28-day mortality. Patients in the Pro+Dex group had significantly lower mortality than those in the Pro group (log-rank P < 0.001). In multivariable Cox proportional hazards models (Figure 1B), the Pro+Dex group was consistently associated with reduced 28-day mortality across all adjustment levels. The adjusted HRs for the Pro+Dex group versus the Pro group were 0.51 (95% CI: 0.41–0.62) in Model 1, 0.44 (95% CI: 0.35–0.54) in Model 2, and 0.45 (95% CI: 0.36–0.56) in Model 3, indicating a robust survival benefit. Similarly, in multivariable logistic regression analysis (Figure 1C), the Pro+Dex group was associated with a substantially lower risk of incident delirium. The adjusted ORs were 0.52 (95% CI: 0.40–0.66) in Model 1, 0.37 (95% CI: 0.28–0.47) in Model 2, and 0.28 (95% CI: 0.21–0.37) in Model 3.
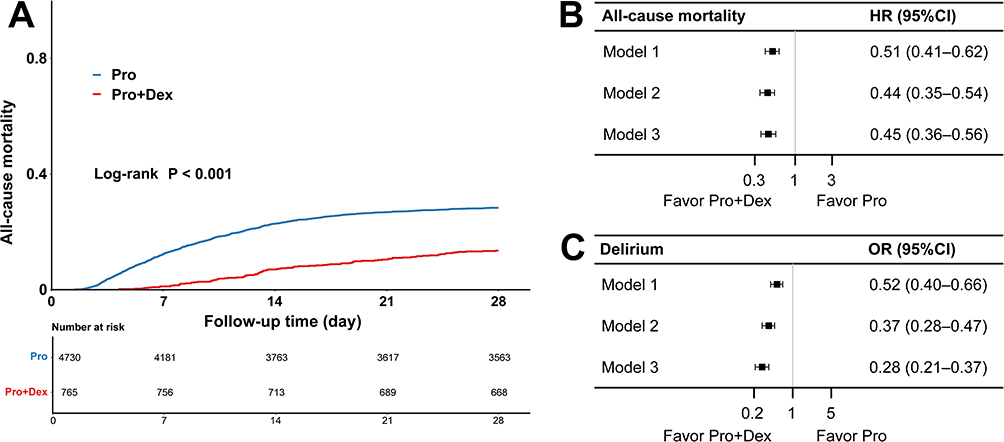 |
Figure 1 Kaplan-Meier survival curves and multivariable regression analyses comparing the Pro group and Pro+Dex group. (A) 28-day mortality; (B) Cox models for 28-day mortality; (C) Logistic regression models for delirium. |
As shown in Table 2, in the GLMs with a Gamma distribution and log-link function, patients in the Pro+Dex group had a significantly longer ICU length of stay than those in the Pro group (adjusted mean 13.07 vs 10.60 days, ratio: 1.23, 95% CI: 1.18–1.29, P < 0.001). In contrast, the duration of mechanical ventilation did not differ significantly between the two groups (adjusted mean 154.79 vs 157.64 hours, ratio: 0.98, 95% CI: 0.92–1.05, P = 0.614).
 |
Table 2 Generalized Linear Model Analysis of ICU Length of Stay and Mechanical Ventilation Duration According to Sedation Strategy |
Longitudinal analysis using LMMs revealed distinct temporal trajectories of MAP, HR, and SpO2 between the Pro and Pro+Dex groups (Figure 2). The detailed model outputs are provided in Tables S3–S5. MAP was significantly lower in the Pro+Dex group (Estimate = −5.520, P < 0.001), with a more stable trajectory over time, while the Pro group showed a gradual increase (group × time spline 1: Estimate = −2.962, P = 0.002). SpO2 was slightly lower overall in the Pro+Dex group (Estimate = −0.899, P < 0.001), but significant positive time interactions (all P < 0.05) indicated stable oxygenation compared with an early decline and recovery pattern in the Pro group. HR was also lower in the Pro+Dex group (Estimate = −4.398, P < 0.001), with significant group × time interactions (all P < 0.05) showing an early HR reduction followed by gradual convergence between groups.
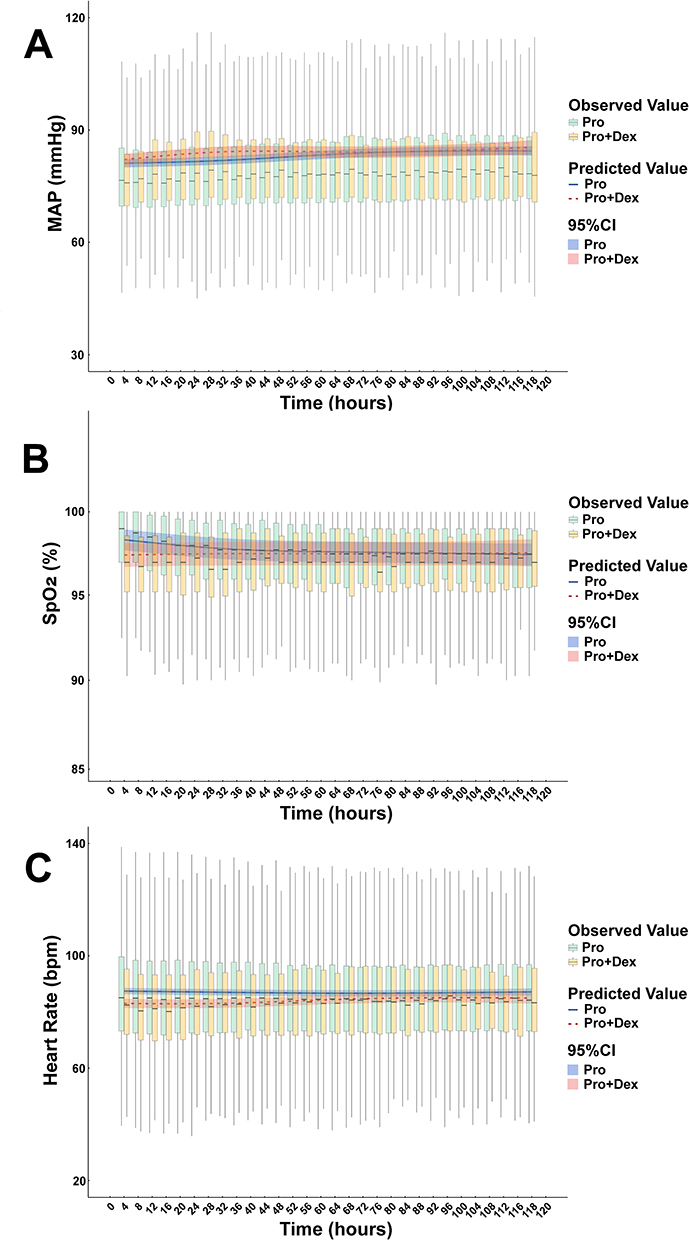 |
Figure 2 Longitudinal trajectories of (A) MAP, (B) SpO2 and (C) HR during sedation. Boxplots represent observed values, while solid lines and shaded areas indicate linear mixed model (LMM)–estimated trends and corresponding 95% confidence intervals. |
Subgroup Analysis
Subgroup analyses of 28-day mortality and delirium were conducted to evaluate the consistency of treatment effects across various clinical subgroups (Figure 3). For 28-day mortality (Figure 3A), the survival benefit associated with the Pro+Dex combination was consistent across all examined subgroups, including age, gender, renal function, APS III score, CCI, sepsis, and propofol infusion rate, with no significant interactions observed (all P for interaction > 0.05). For delirium (Figure 3B), subgroup interaction analysis revealed no significant effect modification by age, gender, renal function, or propofol infusion rate (all P for interaction > 0.05), except for the APS III score, where the preventive effect of Pro+Dex was more pronounced among patients with lower APS III score (P for interaction = 0.026). These results demonstrated that the beneficial effects of the Pro+Dex combination on 28-day mortality and delirium were generally robust and consistent across heterogeneous patient subgroups.
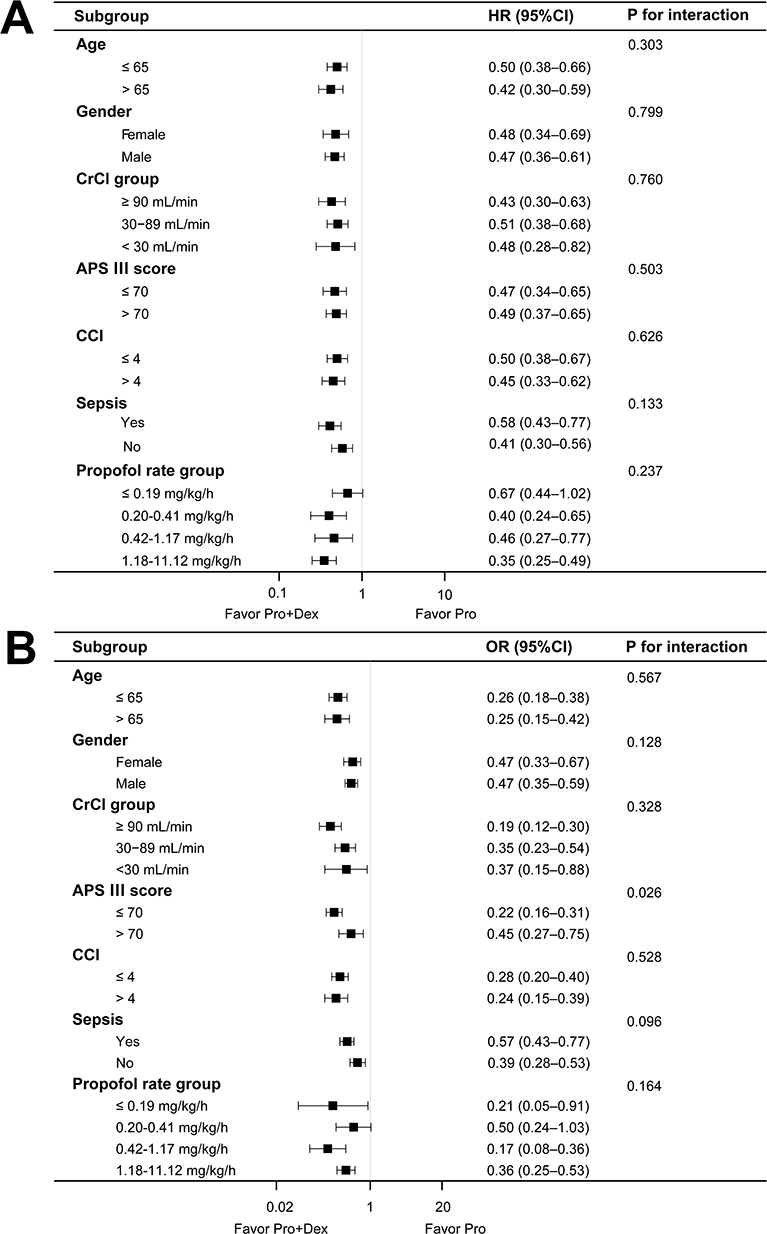 |
Figure 3 Subgroup analyses of 28-day mortality (A) and delirium (B). |
External Validation and Sensitivity Analysis
The robustness of these findings was supported by external validation and multiple sensitivity analyses. In the Nanjing Drum Tower Hospital cohort, the Pro+Dex strategy was associated with a lower 28-day mortality (HR 0.56, 95% CI 0.34–0.93), whereas the reduction in delirium was not statistically significant (OR 0.79, 95% CI 0.46–1.38). In the propensity score-matched cohort, the survival and delirium benefits associated with Pro+Dex remained significant (mortality: HR 0.47, 95% CI 0.38–0.60; delirium: OR 0.39, 95% CI 0.20–0.51); baseline characteristics after matching are shown in Table S6. Multivariable Cox regression for ICU mortality yielded similar results, and associations were consistent in analyses stratified by data source (MIMIC-IV vs eICU-CRD), further supporting the robustness and generalizability of the findings. All stratified, sensitivity, and external validation results are summarized in Table S7.
Discussion
In this large multicenter retrospective cohort study, the use of combined propofol and dexmedetomidine for continuous sedation in mechanically ventilated ICU patients was associated with significantly lower 28-day mortality and a reduced incidence of delirium compared with propofol monotherapy. These associations remained generally consistent across multivariable adjustment, subgroup analyses, and sensitivity analyses, supporting the robustness of the primary findings. Importantly, the survival benefit was also reproduced in the external validation cohort from Nanjing Drum Tower Hospital, supporting the generalizability of the mortality finding. However, patients in the Pro+Dex group had a modestly longer ICU length of stay, whereas the duration of mechanical ventilation was similar between groups. This finding may plausibly relate to the distinct pharmacologic and bedside management profile of dexmedetomidine-based sedation, which provides a more arousable sedation state and is associated with a higher risk of bradycardia, potentially influencing monitoring needs, sedation titration, and the trajectory of ICU recovery.15,16 At the same time, prior comparative studies have not shown a consistent increase in ICU length of stay with dexmedetomidine versus propofol, so this association should be interpreted cautiously as a management-related clinical finding rather than a direct harmful effect of the drug itself.16 Taken together, these findings support the conclusion that the propofol-plus-dexmedetomidine strategy was associated with lower 28-day mortality and lower delirium risk, while its association with ICU length of stay should be interpreted more cautiously.
To reduce potential bias and strengthen the robustness of the observed associations, our primary analysis used hierarchical multivariable models incorporating baseline illness severity and physiologic parameters, and the findings were further supported by sensitivity analyses and external validation. Although dexmedetomidine is widely used for ICU sedation due to its favorable pharmacologic profile, its effect on mortality remains controversial. Several randomized controlled trials (RCTs) have examined its impact, yielding inconsistent results. Early studies such as the MENDS trial suggested a potential mortality benefit, particularly in septic patients, where dexmedetomidine was associated with a lower 28-day mortality compared to lorazepam.17 However, subsequent larger trials, including the MIDEX, PRODEX and SPICE III trials, found no significant differences in ICU or long-term mortality when comparing dexmedetomidine to standard agents like propofol or midazolam.16,18 Notably, SPICE III revealed age-related heterogeneity: older patients (>65 years) exhibited a trend toward improved survival with dexmedetomidine, whereas younger patients experienced slightly worse outcomes.15 Meta-analyses have further clarified these discrepancies. While dexmedetomidine appeared to reduce mortality compared to benzodiazepines, no such advantage was observed when compared with propofol.5,19 Additionally, dexmedetomidine may offer greater benefit in patients with lower illness severity, as reflected in studies showing improved outcomes in lower APACHE IV quartiles.20 Dexmedetomidine often showed benefit over benzodiazepines but not over propofol, a sedative with an already favorable safety profile.21 Trials such as SPICE III included broad ICU cohorts, including younger or postoperative patients requiring deep sedation, which dexmedetomidine alone may not adequately provide.18 This led to frequent crossover and adjunctive sedative use, diluting treatment effects. Moreover, illness severity further modified treatment response. Patients with preserved organ function may benefit more from sympatholytic and anti-inflammatory effects of dexmedetomidine, while sicker patients may see limited or no benefit.22 Importantly, our study did not compare dexmedetomidine monotherapy with propofol monotherapy. Rather, it evaluated a multimodal sedation strategy combining dexmedetomidine with propofol, which may offer complementary rather than isolated drug effects in routine ICU practice. Some prior studies have specifically examined propofol-dexmedetomidine combination strategies rather than dexmedetomidine monotherapy alone. In a propensity-matched cohort of mechanically ventilated ICU patients, adjunctive dexmedetomidine added to propofol did not significantly improve major clinical outcomes, suggesting that the benefits of combination sedation may not be uniform across settings. In addition, concomitant dexmedetomidine and propofol has been associated with a higher incidence of hypotensive events in mechanically ventilated ICU patients, indicating that combination therapy may involve both potential benefits and hemodynamic trade-offs.23,24 Taken together with the broader high-impact literature on dexmedetomidine-based ICU sedation, these findings suggest that the comparative effects of propofol-plus-dexmedetomidine strategies remain clinically important but incompletely defined.17 The observed association with lower mortality may plausibly relate to the complementary pharmacologic profiles of the two agents. Dexmedetomidine’s sympatholytic and anti-inflammatory properties can offset propofol-induced hypotension and myocardial depression, promoting hemodynamic stability.25,26 Dexmedetomidine may also exert neuroprotective effects that are relevant to vulnerable critically ill patients, although this interpretation remains hypothesis-generating in the context of our observational study.27,28
Delirium reduction was another important finding of this study. Dexmedetomidine promotes a sleep-like sedative state via locus coeruleus inhibition while preserving respiratory drive and circadian rhythms, which may protect against neurocognitive dysfunction.29 In addition, its anti-inflammatory and anti-oxidative actions have been shown to attenuate neuroinflammation, a key driver of ICU delirium.30 The greater delirium prevention observed among patients with lower APS III score suggested that the benefits of dexmedetomidine may be attenuated in severe systemic illness, where metabolic and inflammatory disturbances predominate.10 Recent clinical guidance supports the use of dexmedetomidine in mechanically ventilated adult ICU patients when delirium reduction is considered a key priority.31 Similarly, the SEDCOM study found a lower prevalence of delirium in patients receiving dexmedetomidine versus midazolam.32 Meta-analyses have further confirmed these findings, indicating that dexmedetomidine reduced both the incidence and duration of delirium, particularly in elderly and high-risk patients. Collectively, these data supported the use of dexmedetomidine as a delirium-sparing sedative strategy in critically ill patients.33
However, no significant difference in delirium incidence was observed between the two sedation groups in the eICU database. The unexpectedly low incidence of delirium observed in the eICU database likely reflects limitations in data capture rather than true clinical differences. Unlike the single-center MIMIC database with standardized and frequent CAM-ICU assessments, the multicenter eICU database includes hospitals with heterogeneous delirium screening practices and inconsistent documentation. Collectively, these factors likely led to attenuation of the observed association between the propofol-dexmedetomidine combination and delirium risk. Similarly, in the external validation cohort, although delirium incidence was directionally lower in the Pro+Dex group, the difference did not reach statistical significance.
Linear mixed-effects model analysis revealed distinct temporal patterns in physiologic parameters between groups. Although MAP differences varied over time, the Pro group showed an early upward trend, while the Pro+Dex group maintained greater stability, suggesting improved autonomic regulation with dexmedetomidine. SpO2 declined slightly in the Pro group but remained stable with Pro+Dex, likely reflecting dexmedetomidine’s minimal respiratory depression.34 Dexmedetomidine, via central α2-adrenergic agonism, modulates key physiologic parameters.35 In the SEDCOM trial, it reduced tachycardia and hypertension compared with midazolam while maintaining stable MAP and SpO2.31 Compared with propofol, it was associated with less hypotension requiring vasopressors and fewer respiratory complications. Jakob et al reported a smaller MAP drop with dexmedetomidine (−23 mmHg vs −29 mmHg for propofol).15 Notably, dexmedetomidine preserved spontaneous ventilation and airway tone, supporting stable oxygenation even during prolonged use. These features are particularly beneficial in elderly or frail patients with limited respiratory reserve.36 Overall, dexmedetomidine offers a favorable balance of hemodynamic and respiratory stability.37
Clinically, our findings suggest that the propofol-plus-dexmedetomidine strategy may provide a pragmatic balance between sedation adequacy, hemodynamic tolerance, and delirium risk in mechanically ventilated ICU patients. However, given the observational design, these findings should be interpreted as supportive of a clinically relevant association rather than definitive evidence of treatment superiority.
This study has several limitations that warrant consideration. First, as a retrospective observational study, it cannot establish causality. To reduce potential bias, we used hierarchical multivariable adjustment in the primary analysis, and further assessed the robustness of the findings through propensity score matching and external validation in an independent cohort, particularly given the substantial difference in sample size between the Pro and Pro+Dex groups. Furthermore, because this study compared propofol monotherapy with a propofol-plus-dexmedetomidine strategy and did not include a dexmedetomidine-only group, the present findings should not be interpreted as evidence of the isolated effect of dexmedetomidine itself. Second, differences in data structure and documentation between the MIMIC-IV and eICU databases may introduce heterogeneity. In particular, delirium assessments in the eICU database were inconsistently recorded across centers, often limited to admission or discharge evaluations, which likely led to underestimation of its true incidence and attenuation of the observed associations. Third, although the mortality association was externally validated using the Nanjing Drum Tower Hospital cohort, this validation was based on a single-center dataset with a relatively small sample size; moreover, delirium ascertainment relied primarily on physicians’ daily ward-round documentation with low assessment frequency, which may have resulted in under-detection and reduced power to detect group differences. Fourth, sedation depth, cumulative dexmedetomidine exposure, time-varying hemodynamic variables, and differences in nursing care strategies were not fully standardized, which may have affected comparability between groups. Finally, long-term cognitive and functional outcomes after ICU discharge were not captured, limiting the assessment of persistent neurocognitive benefits. Future prospective studies integrating continuous sedation depth monitoring and standardized delirium screening are needed to validate these findings and further clarify the comparative effects of different ICU sedation strategies.
Conclusion
In this retrospective multicenter cohort study, the propofol-plus-dexmedetomidine strategy was associated with lower 28-day mortality and lower delirium risk than propofol monotherapy, without a significant difference in mechanical ventilation duration, although ICU length of stay was longer and should be interpreted cautiously.
Abbreviations
MIMIC-IV, Medical Information Mart for Intensive Care IV; eICU-CRD, eICU Collaborative Research Database; ICU, Intensive Care Unit; Pro, propofol monotherapy; Pro+Dex, propofol plus dexmedetomidine combination; MAP, mean arterial pressure; HR, heart rate; SpO2, oxygen saturation; APS III, Acute Physiology Score III; CCI, Charlson Comorbidity Index; CrCl, creatinine clearance; CAM-ICU, Confusion Assessment Method for the ICU; GLM, generalized linear model; LMM, linear mixed-effects model; REML, restricted maximum likelihood; AIC, Akaike Information Criterion; SMD, standardized mean difference; VIF, variance inflation factor; MICE, multiple imputation by chained equations; NIH, National Institutes of Health; CITI, Collaborative Institutional Training Initiative; SQL, Structured Query Language; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease.
Data Sharing Statement
The datasets analyzed in this study are publicly available. MIMIC-IV is accessible via PhysioNet, and access to both databases requires completion of the required credentialing process. The analytic code and SQL queries used for data extraction can be made available by the corresponding author upon reasonable request. Data from the Nanjing Drum Tower Hospital validation cohort are available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Ethics Approval and Consent to Participate
This study was a retrospective analysis of two de-identified, publicly available critical care databases (MIMIC-IV and the eICU Collaborative Research Database). The creation of the MIMIC-IV database was approved by the Institutional Review Boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center, and studies using the database were granted a waiver of informed consent. The external validation study based on the Nanjing Drum Tower Hospital cohort was approved by the Institutional Ethics Committee of Nanjing Drum Tower Hospital (Approval Number: 2023-488-02). Patient consent to review their medical records was not required by the Institutional Ethics Committees of Nanjing Drum Tower Hospital because this was a retrospective study using existing clinical data. All patient data were handled in a de-identified and confidential manner, and all methods were performed in accordance with the relevant guidelines and regulations and the Declaration of Helsinki.
Acknowledgments
The authors would like to thank Nanjing Drum Tower Hospital, the MIMIC-IV database, and the eICU Collaborative Research Database for providing the research platforms and data resources. The authors also thank all individuals who participated in and contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hodgson CL, Bailey M, Bellomo R, et al. Early active mobilization during mechanical ventilation in the ICU. N Engl J Med. 2022;387(19):1747–14. doi:10.1056/NEJMoa2209083
2. Ayenew T, Gedfew M, Fetene MG, et al. Prevalence of mortality among mechanically ventilated patients in the intensive care units of Ethiopian hospitals and the associated factors: a systematic review and meta-analysis. PLoS One. 2024;19(7):e0306277. doi:10.1371/journal.pone.0306277
3. Chen Y, Zhang K, Zhou C, Chase JG, Hu Z. Automated evaluation of typical patient-ventilator asynchronies based on lung hysteretic responses. Biomed Eng Online. 2023;22(1):102. doi:10.1186/s12938-023-01165-0
4. García-Montoto F, Paz-Martín D, Pestaña D, et al. Guidelines for inhaled sedation in the ICU. Rev Esp Anestesiol Reanim. 2024;71(2):90–111. doi:10.1016/j.redare.2024.01.010
5. Wang C, Chen Q, Wang P, et al. The effect of dexmedetomidine as a sedative agent for mechanically ventilated patients with sepsis: a systematic review and meta-analysis. Front Med Lausanne. 2021;8:776882. doi:10.3389/fmed.2021.776882
6. Heybati K, Xie G, Deng J, Walkey AJ, Gajic O, Yadav H. Hemodynamic effects of guideline-based sedation in mechanically ventilated adults: a multicenter observational analysis. Crit Care Explor. 2025;7(9):e1313. doi:10.1097/CCE.0000000000001313
7. Martínez-Castro S, Monleón B, Puig J, et al. Sedation with sevoflurane versus propofol in COVID-19 patients with acute respiratory distress syndrome: results from a randomized clinical trial. J Pers Med. 2023;13(6):925. doi:10.3390/jpm13060925
8. Karan A, Maaliki N, Kogler WM, Esmail K. Acute decompensated heart failure and cardiogenic shock following propofol infusion: a report and review of pathophysiology. Cureus. 2023;15(7):e41815. doi:10.7759/cureus.41815
9. Spinazzola G, Spadaro S, Ferrone G, et al. Management of analgosedation during noninvasive respiratory support: an expert Delphi consensus document developed by the Italian society of anesthesia, analgesia, resuscitation and intensive care (SIAARTI). J Anesth Analg Crit Care. 2024;4(1):68. doi:10.1186/s44158-024-00203-0
10. Bateman RM, Sharpe MD, Jagger JE, et al. 36th international symposium on intensive care and emergency medicine: Brussels, Belgium, 15–18 March 2016. Crit Care. 2016;20(Suppl 2):94. doi:10.1186/s13054-016-1208-6
11. Xu HC, Ye Q, Wu L, et al. The EC50 of propofol with different doses of dexmedetomidine during gastrointestinal endoscopy: a double-blind, placebo-controlled trial. Medicine. 2024;103(23):e38421. doi:10.1097/MD.0000000000038421
12. Walsh TS, Parker RA, Aitken LM, et al. Dexmedetomidine- or clonidine-based sedation compared with propofol in critically ill patients: the A2B randomized clinical trial. JAMA. 2025;334(1):32–45. doi:10.1001/jama.2025.7200
13. Lewis K, Alshamsi F, Carayannopoulos KL, et al. Dexmedetomidine vs other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials. Intensive Care Med. 2022;48(7):811–840. doi:10.1007/s00134-022-06712-2
14. Dafni U. Landmark analysis at the 25-year landmark point. Circ Cardiovasc Qual Outcomes. 2011;4(3):363–371. doi:10.1161/CIRCOUTCOMES.110.957951
15. Shehabi Y, Serpa Neto A, Howe BD, et al. Early sedation with dexmedetomidine in ventilated critically ill patients and heterogeneity of treatment effect in the SPICE III randomised controlled trial. Intensive Care Med. 2021;47(4):455–466. doi:10.1007/s00134-021-06356-8
16. Jakob SM, Ruokonen E, Grounds RM, et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307(11):1151–1160. doi:10.1001/jama.2012.304
17. Pandharipande PP, Pun BT, Herr DL, et al. Effect of sedation with dexmedetomidine vs lorazepam on acute brain dysfunction in mechanically ventilated patients: the MENDS randomized controlled trial. JAMA. 2007;298(22):2644–2653. doi:10.1001/jama.298.22.2644
18. Shehabi Y, Howe BD, Bellomo R, et al. Early sedation with dexmedetomidine in critically ill patients. N Engl J Med. 2019;380(26):2506–2517. doi:10.1056/NEJMoa1904710
19. Zhang T, Mei Q, Dai S, Liu Y, Zhu H. Use of dexmedetomidine in patients with sepsis: a systematic review and meta-analysis of randomized-controlled trials. Ann Intensive Care. 2022;12(1):81. doi:10.1186/s13613-022-01052-2
20. Dai X, Wei H, Zou D, et al. Dexmedetomidine improves prognosis in septic patients with myocardial injury and lower APACHE IV scores: a retrospective cohort study. BMC Anesthesiol. 2025;25(1):145. doi:10.1186/s12871-025-02906-5
21. Wen J, Ding X, Liu C, et al. A comparison of dexmedetomidine and midazolam for sedation in patients with mechanical ventilation in ICU: a systematic review and meta-analysis. PLoS One. 2023;18(11):e0294292. doi:10.1371/journal.pone.0294292
22. Gao X, Li Z, Li Z, et al. Is dexmedetomidine superior to non-dexmedetomidine sedatives (particularly propofol) for sedation in critically ill patients with septic shock? A systematic review and meta-analysis of randomized controlled trials. Front Med Lausanne. 2025;12:1646256. doi:10.3389/fmed.2025.1646256
23. Louie JM, Lonardo NW, Mone MC, et al. Outcomes when using adjunct dexmedetomidine with propofol sedation in mechanically ventilated surgical intensive care patients. Pharmacy. 2018;6(3):93. doi:10.3390/pharmacy6030093
24. Buckley MS, Agarwal SK, MacLaren R, Kane-Gill SL. Adverse hemodynamic events associated with concomitant dexmedetomidine and propofol for sedation in mechanically ventilated ICU patients. J Intensive Care Med. 2020;35(12):1536–1545. doi:10.1177/0885066619884548
25. Yamazaki S, Yamaguchi K, Someya A, Nagaoka I, Hayashida M. Anti-inflammatory action of dexmedetomidine on human microglial cells. Int J Mol Sci. 2022;23(17):10096. doi:10.3390/ijms231710096
26. Tu K, Tian L, Zhu Q, et al. Intraoperative opioid-free anesthesia with dexmedetomidine and esketamine versus conventional general anesthesia in laparoscopic cholecystectomy at 3600 m: a randomized trial on hemodynamic stability and postoperative recovery. High Alt Med Biol. 2025;28:8–16. doi:10.1177/15578682251381135
27. Ye C, Shen J, Zhang C, Hu C. Impact of intraoperative dexmedetomidine on postoperative delirium and pro-inflammatory cytokine levels in elderly patients undergoing thoracolumbar compression fracture surgery: a prospective, randomized, placebo-controlled clinical trial. Medicine. 2024;103(18):e37931. doi:10.1097/MD.0000000000037931
28. Chen HY, Deng F, Tang SH, Liu W, Yang H, Song JC. Effect of different doses of dexmedetomidine on the median effective concentration of propofol during gastrointestinal endoscopy: a randomized controlled trial. Br J Clin Pharmacol. 2023;89(6):1799–1808. doi:10.1111/bcp.15647
29. Anuncibay Soto B, Ma Y, Nollet M, et al. The locus coeruleus maintains core body temperature and protects against hypothermia during dexmedetomidine-induced sedation. Proc Natl Acad Sci U S A. 2025;122(41):e2422878122. doi:10.1073/pnas.2422878122
30. Wang J, Sun JQ, Lu Y, et al. Delirium as a mediating factor in the survival benefits of dexmedetomidine in acute brain injury management. Sci Rep. 2025;15(1):30937. doi:10.1038/s41598-025-14180-z
31. Møller MH, Alhazzani W, Lewis K, et al. Use of dexmedetomidine for sedation in mechanically ventilated adult ICU patients: a rapid practice guideline. Intensive Care Med. 2022;48(7):801–810. doi:10.1007/s00134-022-06660-x
32. Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301(5):489–499. doi:10.1001/jama.2009.56
33. Caetano da Silva L, Tapioca V, Viana P, Pereira EM, Gibicoski T, Amaral S. Dexmedetomidine for delirium prevention after cardiac surgery: an updated systematic review and meta-analysis with trial sequential analysis. Anaesth Crit Care Pain Med. 2025;44(5):101578. doi:10.1016/j.accpm.2025.101578
34. Simioli F, Annunziata A, Coppola A, et al. The role of dexmedetomidine in ARDS: an approach to non-intensive care sedation. Front Med Lausanne. 2023;10:1224242. doi:10.3389/fmed.2023.1224242
35. Zhang XW, Chen L, Chen CF, Cheng J, Zhang PP, Wang LC. Dexmedetomidine modulates neuronal activity of horizontal limbs of diagonal band via α2 adrenergic receptor in mice. BMC Anesthesiol. 2023;23(1):327. doi:10.1186/s12871-023-02278-8
36. Santos Neto NCD. Dexmedetomidine- or clonidine-based sedation vs propofol in critically ill patients. JAMA. 2025;334(15):1394. doi:10.1001/jama.2025.12647
37. Heybati K, Zhou F, Ali S, et al. Outcomes of dexmedetomidine versus propofol sedation in critically ill adults requiring mechanical ventilation: a systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2022;129(4):515–526. doi:10.1016/j.bja.2022.06.020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low-Dose Esketamine as an Adjuvant to Propofol Sedation for Same-Visit Bidirectional Endoscopy: Protocol for a Multicenter Randomized Controlled Trial
Song N, Shan XS, Yang Y, Zheng Z, Shi WC, Yang XY, Li Y, Tan AP, Liu H, Peng K, Ji FH
International Journal of General Medicine 2022, 15:4733-4740
Published Date: 6 May 2022
Remimazolam Tosylate Combined with Low-Dose Propofol Improves Sedation and Safety in Hysteroscopy
Zhang F, Chang H, Qing W, Yu R, Liao Q, Tong J
Drug Design, Development and Therapy 2022, 16:4101-4108
Published Date: 29 November 2022
Efficacy and Safety of Ciprofol for Sedation/Anesthesia in Patients Undergoing Hysteroscopy: A Randomized, Parallel-Group, Controlled Trial
Lan H, Shan W, Wu Y, Xu Q, Dong X, Mei P, Duan G, You M, Jin L, Wu J
Drug Design, Development and Therapy 2023, 17:1707-1717
Published Date: 11 June 2023
Successful Use of Low-Dose Combination Propofol and Fentanyl in Cataract Surgery Phacoemulsification
Irawati D, Adli M, Yadi DF
Clinical Ophthalmology 2023, 17:1929-1937
Published Date: 5 July 2023
Intranasal Dexmedetomidine with Propofol Provides Superior Sedation for Pediatric Contrast-Enhanced CT: A Randomized Controlled Trial
Zhang SJ, Weng YJ, Lei Q, Lin MY, Chen HL, Fang TF, Lu GL
Drug Design, Development and Therapy 2025, 19:9523-9532
Published Date: 24 October 2025