Back to Journals » Clinical Ophthalmology » Volume 17
Successful Use of Low-Dose Combination Propofol and Fentanyl in Cataract Surgery Phacoemulsification
Authors Irawati D ![]() , Adli M, Yadi DF
, Adli M, Yadi DF
Received 22 April 2023
Accepted for publication 20 June 2023
Published 5 July 2023 Volume 2023:17 Pages 1929—1937
DOI https://doi.org/10.2147/OPTH.S415852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dian Irawati,1 Muhamad Adli,1 Dedi Fitri Yadi2
1Department of Anesthesiology, National Eye Center Cicendo Eye Hospital-Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Anesthesiology, Dr. Hasan Sadikin General Hospital- Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Dian Irawati, Department of Anesthesiology, National Eye Center Cicendo Eye Hospital-Universitas Padjadjaran, Tel +62 8138932261, Email [email protected]
Background: The combination between sedatives and opioids is one of the recommended anesthetic options in ophthalmic procedures and regimens are more advantageous as smaller amounts of each drug can be administered to reduce side effects and have proper outcomes due to the synergistic effects. This study aims to observe the use of low-dose propofol and fentanyl for patients undergoing phacoemulsification surgery.
Material and Methods: This observational study involves a sample of 125 adult patients who underwent elective cataract procedures using the phacoemulsification technique and had an American Society of Anesthesiologists (ASA) physical status of 1 to 3. Dose amount of fentanyl and propofol, Ramsay score, hemodynamic parameter, side effects, and patient satisfaction were evaluated, recorded, and analyzed using a 5-point Likert scale.
Results: The result showed the mean absolute dose of propofol was 12.46± 4.376 mg, with a range between 10 and 30 mg, while the mean per body weight was 0.21± 0.075 mg. Similarly, the mean absolute dose for fentanyl was 25.04± 3.012 mcg within the range of 10– 50 mcg, and the per-body weight dose was 0.43± 0.080 mcg. About 90.4% and 9.6% of the patients reached Ramsay 2 and 3, respectively. The analysis of systolic, diastolic blood pressure, mean arterial pressure, and pulse rate showed that the combination of low-dose fentanyl and propofol was significantly lower than before therapy administration in all four values (p < 0.05).
Conclusion: The combination of low-dose propofol and fentanyl in cataract surgery using phacoemulsification successfully reached the targeted sedation level and a significant decrease in blood pressure, MAP, pulse rate, minimal side effects, and high satisfaction rate.
Keywords: combination, propofol, fentanyl, low dose, phacoemulsification, sedation
Introduction
According to the 2010 Global Burden of Disease Study and other worldwide meta-analyses, 32.4 million individuals worldwide were blind. Globally, the leading overall cause of blindness was cataracts. The only treatment for cataracts is surgery. Phacoemulsification is the gold standard for cataract surgery in the developed world. The benefit of phacoemulsification over purely manual methods is the ability to extract the large nucleus through a small incision of ≤3.0mm1 There is no anesthesia gold standard for cataract surgery,2 however, having safe, painless, efficient, and effective anesthesia is the goal, regardless of the decision.3 The trend has shifted in cataract surgery from general anesthesia to the combination of sedation and topical anesthesia.4
Fear and anxiety directly related to the procedure are well-known preoperative feelings for patients scheduled to undergo cataract surgery.5 Counselling is not only to provide information and clarify the patient’s doubts but also to reassure them. Ophthalmologists and other health-care professionals can contribute to improving communication with patients.6 Catecholamine release induced by anxiety has a negative effect on comorbidities, which are present in many cataract patients. Anxiolysis can also reduce catecholamine secretion and subsequently tachycardia and hypertension.7 Meanwhile, the major predictors of lower patient satisfaction with ocular surgery include pain, fear, and anxiety.8
One of the recommended options in ophthalmic procedures, which could have proper outcomes due to the synergistic effects of these agents is the combination between sedatives and opioids. Several studies have demonstrated the effectiveness of different combination therapies to achieve conscious sedation during cataract surgery under local anesthesia. The combination of sedatives and opioids provides better sedation during phacoemulsification due to its favorable effects.9 Combined regimens are more advantageous as smaller amounts of each drug can be administered to reduce side effects.7
The ideal sedative agent is non-toxic, has a rapid onset and short duration of action, has a favorable therapeutic index and predictable effects, does not cumulate, and is cost-effective.2 Unfortunately, no drug is presently available that fulfills all these criteria.7 Fentanyl citrate is a narcotic analgesic that has been extensively used in ophthalmic procedures under topical anesthesia, which includes cataract surgery.10 It is 50 to 100 times more potent than morphine and has a quick onset of action and predictable short duration but less sedative effect.9 The effects of these drugs in excess doses besides sedation are nausea and vomiting.11 Fentanyl is the most commonly used opioid due to its ease of administration, but the time-to-peak effect is relatively slow.12
Sedative drugs are abundant, one of which is propofol, used for sedation and also for hypnosis. It is preferred for moderate-to-deep sedation due to its easy titration, allows a more rapid recovery of cognitive function, and has antiemetic properties.13 Its major side effects include respiratory depression and reduced blood pressure. However, administering this drug at a lower dose is suggested for safe medication. Meanwhile, propofol lacks analgesic properties,11 and must be combined with analgesics for painful procedures.12 A previous study compared the use of a combination of fentanyl with etomidate, propofol, and midazolam, which concluded that the patients’ mean score of satisfaction in the propofol group was significantly higher than the etomidate.14 Any increase in blood pressure during surgery can lead to ocular and systemic complications such as suprachoroidal hemorrhage, stroke, or myocardial ischemic events. The blood pressure changes in phacoemulsification surgery may require constant monitoring for achieving favorable ocular and systemic outcomes.15
Administering drug at a lower dose decreases the possibility of side effect to occur. This study aims to observe the use of low-dose propofol and fentanyl for patients undergoing phacoemulsification. It also analyzes the effect of the combination therapy on sedation level using the Ramsay scale, systolic and diastolic blood pressure, mean arterial pressure (MAP), heart rate, side effects, and patient satisfaction rate on a five-point Likert scale.
Method
This is an observational study with all samples that meet the inclusion criteria and signed informed consent to participate will be included as the subjects. The consecutive sampling method was used to collect data from all patients that underwent cataract surgery with the phacoemulsification technique from February to April 2021 and signed informed consent. The current study protocol was approved by the Ethics Committee of National Eye Center Cicendo Eye Hospital of Medical Sciences with ethical approval letter number LB.02.01/2.3/017/2021. Furthermore, written informed consent was obtained from each subject. The study was conducted on adult patients and it followed the tenets of the Declaration of Helsinki. All adult patients who underwent elective cataract procedures using the phacoemulsification technique had an American Society of Anesthesiologists (ASA) physical status of 1 to 3. The exclusion criteria include patients who had involuntary movements such as Parkinson’s disease, were mentally disabled, and had already received sedatives and analgesia preoperative. Drop-out criteria were intraoperative procedure complications such as lens nucleus or intraocular lens drop, and all patients who received additional sedatives other than fentanyl and propofol during the procedure.
The age, gender, weight, comorbidities, and ASA physical status of all subjects were recorded. Hemodynamic parameters before and during surgery, sedation level using the Ramsay scale summarized in Table 1, doses of fentanyl and propofol, side effects, and patient satisfaction after surgery, immediately after the patients entering the recovery room were evaluated and recorded using a five-point Likert scale.
 |
Table 1 Ramsay Sedation Scale |
The patients underwent noninvasive blood pressure monitoring, electrocardiography (ECG), and pulse oximetry and they also received oxygen of 3 liters per minute via nasal cannula before and during the procedure. Anesthesia with topical eye drops (tetracaine 2%) was given before surgery. Surgery is performed by an experienced surgeon or trainee. Subsequently, the subjects were given fentanyl, and after two minutes, the patients received propofol for sedation. Intraoperatively, the heart rate, blood pressure, mean arterial pressure, and saturation were monitored regularly. Subsequently, data were analyzed to determine the effect of fentanyl and propofol combination on systolic and diastolic pressure, MAP, and heart rate. For data analysis, the paired t-test is performed for normally distributed data; otherwise, the Wilcoxon test is performed. Results were considered statistically significant when p < 0.05.
After the procedure, patients were then shifted to recovery from the operative room. Complications during recovery were recorded, and all patients were asked for sedation satisfaction immediately after the patients entering recovery room using a five-point Likert scale namely 1 (Not Satisfied), 2 (Not too Satisfied), 3 (Average), 4 (Satisfied), 5 (Very Satisfied).17
Results
A total of 125 subjects were included in this study. Table 2 describes patient characteristics such as age, sex, weight, comorbidities, duration of operation, and the American Society of Anesthesiologists (ASA) score. The result showed that the use of propofol and fentanyl with a mean absolute dose of 12.46±4.376 mg and 25.04±3.012 mcg or mean per body weight dose of 0.21±0.075mg/kg and 43±0.080 mcg/kg, respectively, achieved Ramsay score of 2 in most patients (113 or 90.4%) as described in Table 3. The results of systolic blood pressure analysis using a paired t-test, and diastolic blood pressure, mean arterial pressure (MAP), and pulse rate using the Wilcoxon test showed that the four values after the use of the combination of fentanyl and propofol were significantly lower than before therapy administration (p < 0.05) as portrayed in Table 4. Most of the patients had no complications (113 or 90.4%), with a satisfaction rate of 4.136 based on the Likert scale as shown in Table 5.
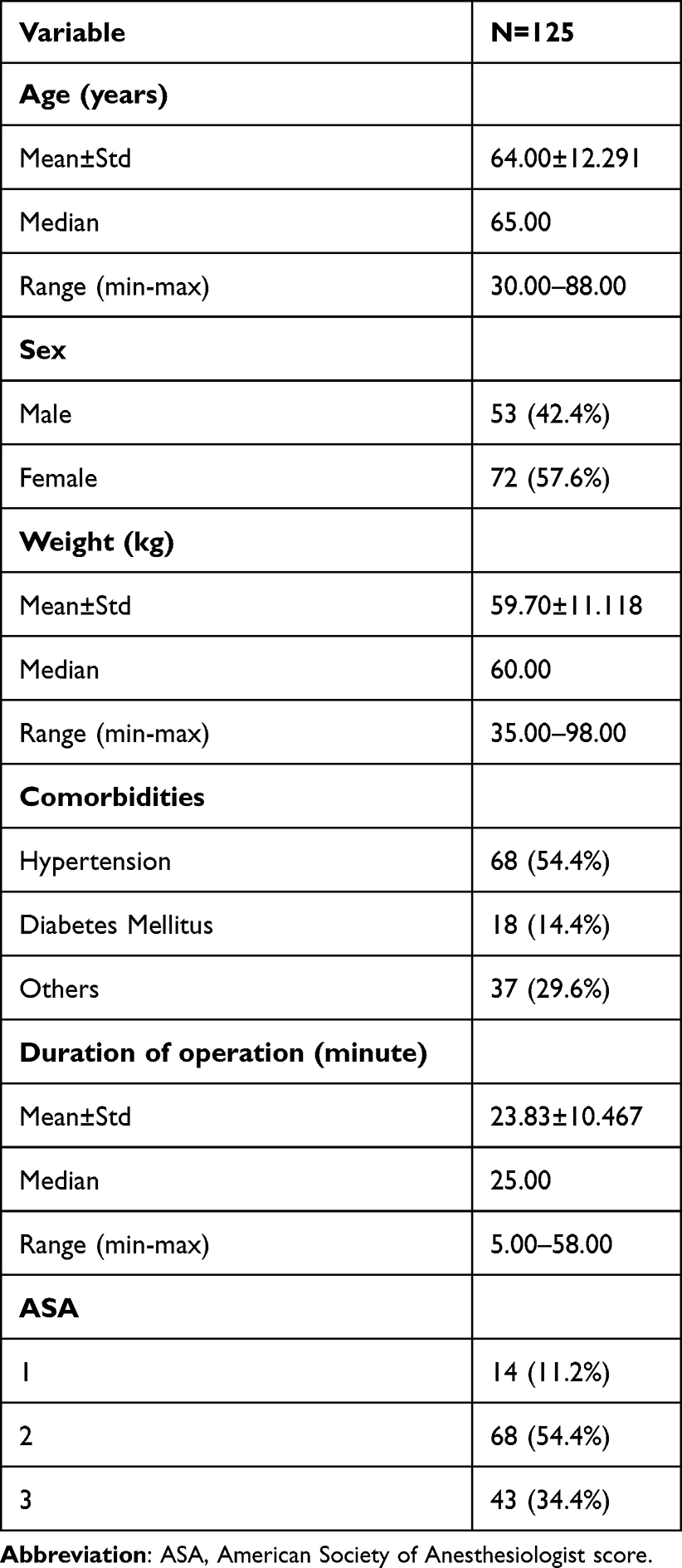 |
Table 2 Demographic Characteristics |
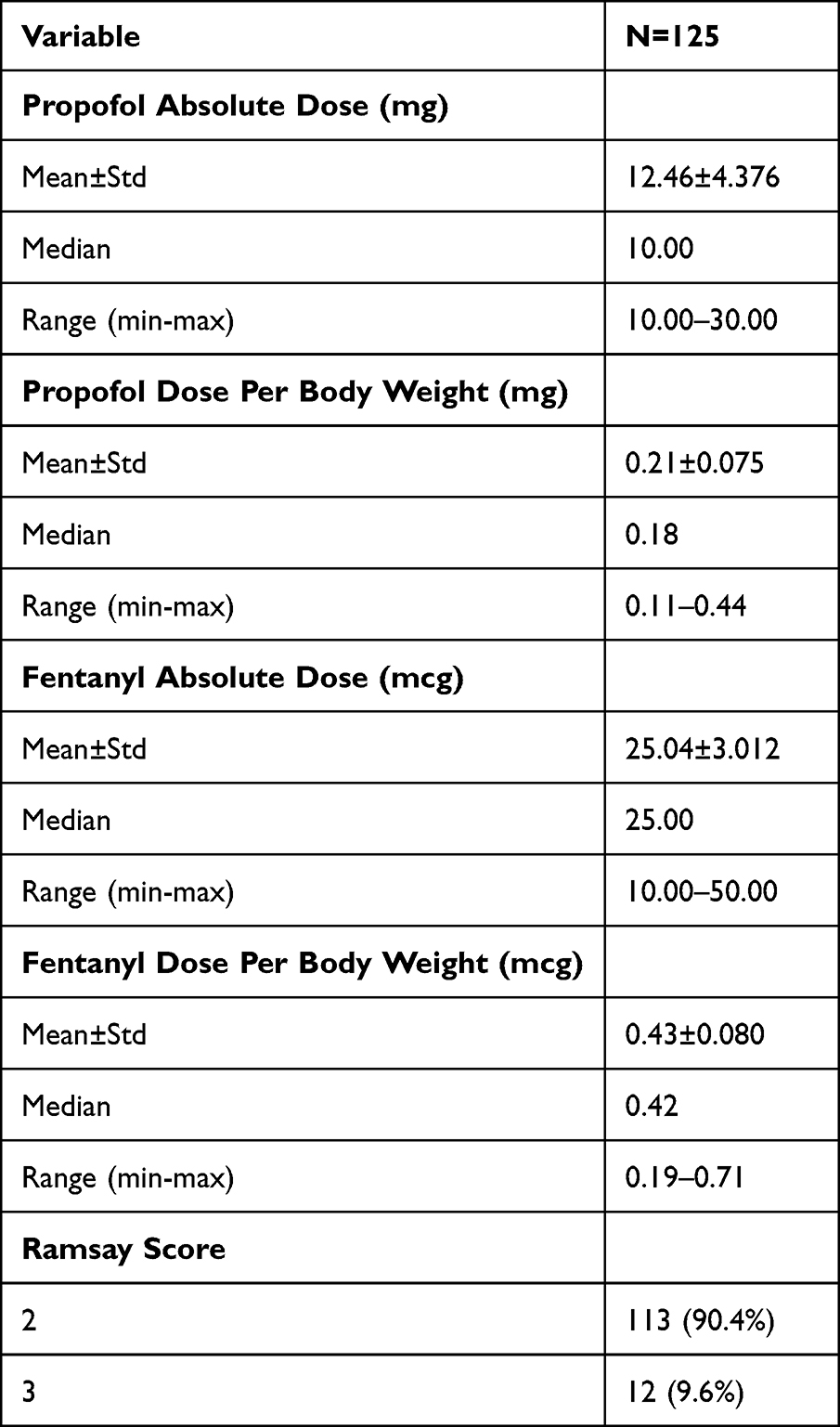 |
Table 3 Dose of Propofol, Fentanyl, and Ramsay Score |
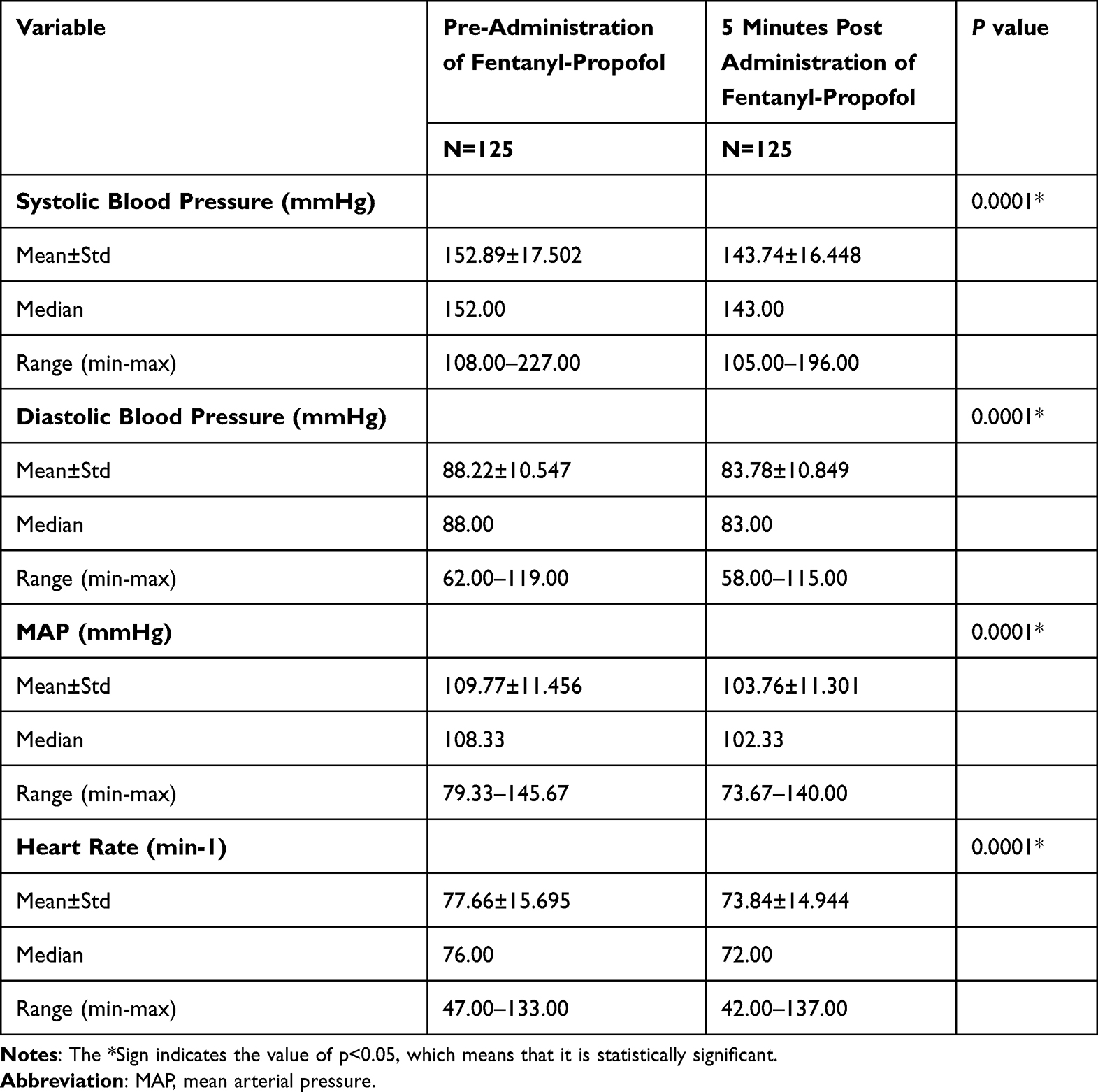 |
Table 4 Comparison Between Systolic Blood Pressure, Diastolic Blood Pressure, MAP, and Pulse Rate Before Administration of Fentanyl-Propofol with 5 Minutes Post-Administration of Fentanyl-Propofol |
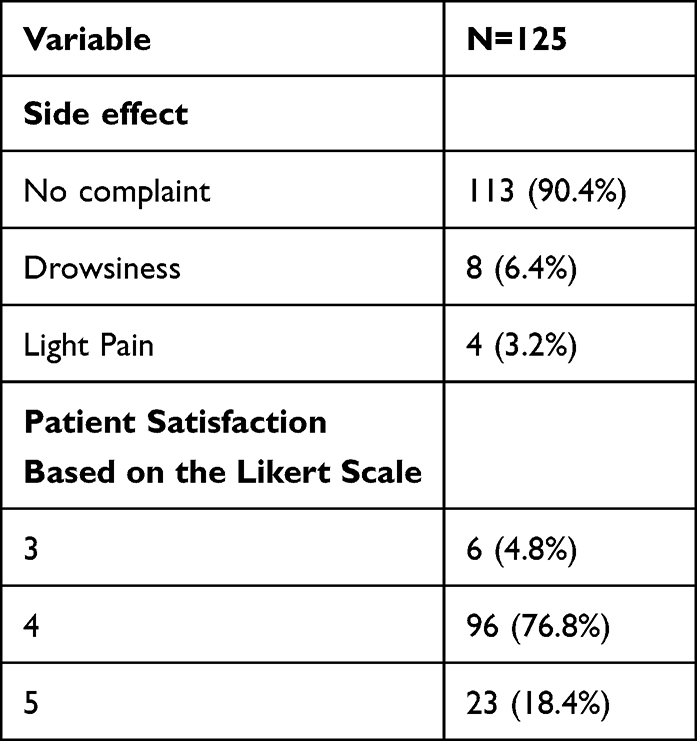 |
Table 5 Side Effects Dan Patient Satisfaction |
Discussion
Dose of Combination Therapy
Monitoring anesthetic care (MAC) or sedation can alleviate anxiety and analgesia, which will increase patients’ satisfaction. Furthermore, the patients who undergo cataract surgery are usually elderly and have comorbidities and painful stimuli during operations.18 The use of sedation for patients undergoing cataract surgical procedures during local/regional anesthesia strikes a balance between patient comfort, safety, and an optimal outcome.19 It is achieved through the use of sedatives and analgesics to induce drowsiness and alleviate fear, anxiety, and pain.7
A previous study found that the administration of fentanyl at 0.75 mcg/kg in patients over 65 years old in combination with 0.5 mg/kg propofol provided good quality sedation that was associated with quick recovery, hemodynamic evaluation, and sedation-related complications.14 In a different study showed that a combination of 1mcg/kg fentanyl and 1 mg/kg propofol in cataract surgery provides appropriate sedation and safe anesthesia with lower complications and acceptable satisfaction in patients and surgeons.20 According to Rewari et al, a minimal dose of opioid and propofol in sedation with a combination of 0.5 mcg/kg remifentanil and 0.5 mg/kg propofol as a bolus in cataract surgery provided excellent relief of pain and anxiety with the fewest adverse effects from ophthalmic block placement.21 Meanwhile, Ferrari et al reported that the administration of 0.47 mg/kg propofol has other advantages besides being amnestic and anxiolytic. These advantages include its ability to reduce the incidence of nausea and vomiting, decrease intraocular pressure, and fast recovery time.22 The result from this study showed that the mean dose of fentanyl and propofol was 0.43 mcg/kg and 0.21 mg/kg, respectively. According to Habib et al, the administration of a subanesthetic dose of propofol of 15–75 mg before peribulbar block injection was effective in reducing the patient’s memory during the procedure.23 Meanwhile, the dose range of propofol used in this study was 10–30 mg.
In a previous study, 70 patients over 60 years old with cataract surgery who were given fentanyl and a bolus dose of 25–50 mcg provided analgesia with minimal sedation.24 The dose range of fentanyl given in this study was 10–50 mcg, which is lower than the previous studies.
Sedation Level
According to ASA guidelines, the preferred sedation level in ophthalmic surgery is either minimal or moderate.11 Furthermore, Ramsay’s sedation score of 2 or 3 is preferable during cataract surgery,25 because spontaneous ocular movement at this level is common and the procedures are frequently hindered at scores of 4 or 5. Park et al reported that deep sedation in cataract surgery is related to poor patient cooperation and lower surgeon satisfaction.26 Higher sedation score is also associated with lower recovery time.14 This study’s results showed that the use of a low-dose combination of propofol and fentanyl gives a Ramsay sedation score of 2 or 3 on all patients.
Blood Pressure
Several factors such as systemic absorption of an anesthetic drug, use of intracameral adrenaline for pupillary dilation, patient anxiety, and discomfort such as iris touch causing pain in topical anesthesia can cause blood pressure changes during cataract surgery. Any increase in blood pressure during surgery can lead to ocular and systemic complications such as suprachoroidal hemorrhage, stroke, or myocardial ischemic events. Furthermore, the blood pressure changes in phacoemulsification surgery may require constant monitoring to achieve favorable ocular and systemic outcomes. These changes need to be observed in order to make a timely intervention to achieve favorable postoperative outcomes. The result of a study conducted by Singh et al on cataract patients comparing topical anesthesia and peribulbar block showed that the increase in intraoperative systolic blood pressure in the topical group is due to the discomfort from microscopic light, iris manipulation, irrigation, and aspiration during surgery. Furthermore, the mean preoperative systolic blood pressure was higher in the topical group, which is probably due to anxiety or stress under topical anesthesia.15 It is a fundamental necessity to monitor anesthesia care to prevent such complications. The result of a study conducted by Shetabi et al on the use of propofol and fentanyl for cataract surgery found a significant reduction in heart rate, systolic, and diastolic blood pressure.20 Similarly, Adinnehmer conducted a study on cataract patients found that pulse rate, systolic and diastolic blood pressure, and mean arterial blood pressure decreased significantly in the three groups during the procedure until recovery time (P < 0.001).14 In this study, a significant decrease in systolic blood pressure, diastolic blood pressure, MAP, and heart rate was found after the administration of low-dose propofol and fentanyl (p < 0.001).
Side Effects
One study on 19.250 cataract surgeries at nine centers in the United States and Canada from June 1995 through June 1997 showed that the use of intravenous anesthetic agents significantly increases the incidence of the adverse event compared to topical or injection anesthesia.27 Combined regimens of intravenous sedatives and opioids can decrease the amounts of each drug administered which can reduce the side effects.7 Another study compared the use of sedation and analgesia using ketamine/propofol combination versus fentanyl/propofol in 60 patients undergoing colonoscopy. The result showed that the incidence of nausea and vomiting was 12.5% in both groups.28 In this study, the use of combination therapy of fentanyl and propofol at a low dose resulted in 4% pain during cataract surgery, as well as 8% postoperative side and 8% dizziness. No vomiting or nausea was found in all the patients receiving the low-dose anesthesia.
Satisfaction Rate
According to Adinnehmeir, propofol has a superior satisfaction rate compared to midazolam and etomidate, with each patient’s satisfaction rate being sequentially 4.88, 4.77, and 4.48, respectively. Furthermore, Aghadavoudi et al29 and Lee-Jayaram et al30 compared the efficacy of etomidate-fentanyl versus ketamine midazolam in procedural sedation for cataract surgery and pediatric orthopedic reductions, respectively. Both studies showed that the satisfaction score of patients was significantly higher.
Limitation
Blood pressure was not always evaluated during the surgery, but only during the first five minutes after drug administration due to the surgery length variability.
Conclusion
Based on the data, the combination of 10–30 mg propofol and 10–50 mcg fentanyl can be used in cataract phacoemulsification surgery because it can achieve an ideal Ramsay score, significant reduction in blood pressure, minimal side effects, and acceptable satisfaction rate.
Acknowledgments
The authors are grateful to the staff of the Department of Anesthesiology, Department of Cataract and Refractive Surgery Unit, Ophthalmology Department of National Eye Center Cicendo Eye Hospital-Universitas Padjadjaran, Bandung, West Java, Indonesia.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare having no conflicts of interest for this article.
References
1. Lam D, Rao SK, Ratra V, et al. Cataract. Nat Rev Dis Primers. 2015;2:25014. doi:10.1038/nrdp.2015.14
2. The Royal College of Anaesthetists and The Royal College of Ophthalmologists. Local anaesthesia for ophthalmic surgery; 2012. Available from: https://www.rcoa.ac.uk/document-store/local-anaesthesia-ophthalmic-surgery.
3. Hamilton RC, Gimbel HV, Strunin L. Regional anesthesia for 12,000 cataract extraction and intraocular lens implantation procedures. Can J Anaesth. 1988;35:615–623. doi:10.1007/bf03020350
4. Leaming DV. Practice styles and preferences of ASCRS members – 2003 survey. J Cataract Refract Surg. 2004;30:892–900. doi:10.1016/j.jcrs.2004.02.064
5. Ługowska D, Konopinska J, Mariak Z, Obuchowska I. Comparison of subjective preoperative experiences of patients before first- or second-eye cataract surgeries. Clin Ophthalmol. 2020;14:2883–2889. doi:10.2147/OPTH.S270196
6. Obuchowska I, Konopinska J. Fear and anxiety associated with cataract surgery under local anesthesia in adults: a systematic review. Psychol Res Behav Manag. 2021;14:781–793. doi:10.2147/PRBM.S314214
7. Greenhalgh DL, Kumar CM. Sedation during ophthalmic surgery. Eur J Anaesthesiol. 2008;25:701–707. doi:10.1017/s0265021508004389
8. Fung D, Cohen MM, Stewart S, et al. What determines patient satisfaction with cataract care under topical local anesthesia and monitored sedation in a community hospital setting? Anesth Analg. 2005;100:1644–1650. doi:10.1213/01.ane.0000154206.81132.b9
9. Woo JH, Au Eong KG, Kumar CM. Conscious sedation during ophthalmic surgery under local anesthesia. Minerva Anestesiol. 2009;75:211–219.
10. Balkan BK, Iyilikci L, Günenç F. Comparison of sedation requirements for cataract surgery under topical anesthesia or retrobulbar block. Eur J Ophthalmol. 2004;14:473–477. doi:10.1177/112067210401400605
11. Diwan R. Monitored anaesthesia care and sedation for eye surgery. In: Kumar J, Jagadesh JMV, editors. Principles and Practice of Ophthalmic Anesthesia. New Delhi: Jaypee Brothers medical publishers; 2017:174–186.
12. Kumar CM, Seet IE, Eke T, Irwin MG, Joshi GP. Peri-operative considerations for sedation-analgesia during cataract surgery: a narrative review. Anaesthesia. 2019;74:1601–1610. doi:10.1111/anae.14845
13. Eleveld DJ, Colin P, Absalom AR, Struys MMRF. Pharmacokinetic-pharmacodynamic model for propofol for broad application in anaesthesia and sedation. Br J Anaesth. 2018;120(5):942e959. doi:10.1016/j.bja.2018.01.018
14. Adinehmehr L, Shetabi H, Moradi Farsani D, Salehi A, Noorbakhsh M. Comparison of the Sedation quality of etomidate, propofol, and midazolam in combination with fentanyl during phacoemulsification cataract surgery: a double-blind, randomized, controlled, clinical trial. Anesth Pain Med. 2019;9(2):e87415. doi:10.5812/aapm.87415
15. Singh B, Kumar P, Moulick PS, et al. Comparison of changes in blood pressure in phacoemulsification cataract surgery performed via topical and peribulbar anaesthesia: a cohort study. Med J Armed Forces India. 2021;79:34–39. doi:10.1016/j.mjafi.2020.12.017
16. Ramsay MA, Savage TM, Simpson BR, et al. Controlled sedation with alphaxalone-alphadolone. Br Med J. 1974;22:656–659. doi:10.1136/bmj.2.5920.656
17. Roberts JS, Laughlin JE, Wedell DH. Validity issues in the Likert and Thurstone approaches to attitude measurement. Educ Psychol Meas. 1999;59(2):211–233. doi:10.1177/00131649921969811
18. Katz J, Feldman MA, Bass EB. Adverse intraoperative medical events and their association with anesthesia management strategies in cataract surgery. Ophthalmology. 2001;108:1721–1726. doi:10.1016/s0161-6420(01)00704-7
19. Krishnamurthy A. A prospective randomized study comparing ketamine - propofol vs midazolam - propofol sedation in elective cataract surgeries done under peribulbar block. Int J Contemp Med Res. 2018;5(3):C12–C16.
20. Shetabi H, Hashemi SJ, Haghi F, Moradi Farsani D. Safety and efficacy of fentanyl versus pethidine in cataract surgery under propofol- based sedation: a double-blind randomized controlled clinical trial. J Res Med Sci. 2020;25:81. doi:10.4103/jrms.jrms_932_19
21. Rewari V, Madan R, Kaul HR, Kumar L. Remifentanil and propofol sedation for retrobulbar nerve block. Anaesth Intensive Care. 2002;30:433–437. doi:10.1177/0310057X0203000405
22. Ferrari LR, Donolon JV. A comparison of propofol, midazolam, and methohexital for sedation during retrobulbar and peribulbar block. J Clin Anesth. 1992;4:93. doi:10.1016/0952-8180(92)90021-r
23. Habib NE, Balmer HG, Hocking G. Efficacy and safety of sedation with propofol in peribulbar anaesthesia. Eye. 2002;16:60–62. doi:10.1038/sj.eye.6700062
24. Aydin ON, Ugur B, Kir E, Özkan SB. Effect of single-dose fentanyl on the cardiorespiratory system in elderly patients undergoing cataract surgery. J Clin Anest. 2004;16(2):98–103. doi:10.1016/j.jclinane.2003.05.008
25. Ryu JH, Hwang JW, Hwang J-W, Do S-H. Optimal target concentration of remifentanil during cataract surgery with monitored anesthesia care. J Clin Anesth. 2010;22:533–537. doi:10.1016/j.jclinane.2010.02.007
26. Park J, Kwo J. Remifentanil or dexmedetomidine for monitored anesthesia care during cataract surgery under topical anesthesia. Korean J Anesthesiol. 2012;63(1):92–93. doi:10.4097/kjae.2012.63.1.92
27. Katz J, Feldman M, Bass E. Injectable versus topical anesthesia for cataract surgery patient perceptions of pain and side effects. Ophthalmology. 2000;107:2054–2060. doi:10.1016/s0161-6420(00)00359-6
28. Khajavi M, Emami A, Etezadi F, Safari S, Sharifi A, Shariat Moharari R. Conscious sedation and analgesia in colonoscopy: ketamine/propofol combination has superior patient satisfaction versus fentanyl/ propofol. Anesth Pain Med. 2013;3(1):209–213. doi:10.5812/aapm.9653
29. Aghadavoudi O, Balaei P, Akbari M. مقايسهي كيفيت و عوارض آرامبخشي (Sedation (توسط اتوميديت- فنتانيل و كتامين- ميدازولام در جراحي كاتاراكت [The comparison of the efficacy and safety of sedation with etomidate-fentanyl versus ketaminemidazolam combinations in cataract surgery]. J Isfahan Med Sch. 2012;30(209):1. Persian.
30. Lee-Jayaram JJ, Green A, Siembieda J, et al. Ketamine/midazolam versus etomidate/fentanyl: procedural sedation for pediatric orthopedic reductions. Pediatr Emerg Care. 2010;26(6):408–412. doi:10.1097/PEC.0b013e3181e057cd
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Low-Dose Esketamine as an Adjuvant to Propofol Sedation for Same-Visit Bidirectional Endoscopy: Protocol for a Multicenter Randomized Controlled Trial
Song N, Shan XS, Yang Y, Zheng Z, Shi WC, Yang XY, Li Y, Tan AP, Liu H, Peng K, Ji FH
International Journal of General Medicine 2022, 15:4733-4740
Published Date: 6 May 2022
Remimazolam Tosylate Combined with Low-Dose Propofol Improves Sedation and Safety in Hysteroscopy
Zhang F, Chang H, Qing W, Yu R, Liao Q, Tong J
Drug Design, Development and Therapy 2022, 16:4101-4108
Published Date: 29 November 2022
Efficacy and Safety of Ciprofol for Sedation/Anesthesia in Patients Undergoing Hysteroscopy: A Randomized, Parallel-Group, Controlled Trial
Lan H, Shan W, Wu Y, Xu Q, Dong X, Mei P, Duan G, You M, Jin L, Wu J
Drug Design, Development and Therapy 2023, 17:1707-1717
Published Date: 11 June 2023
Comparing Remimazolam and Propofol for Postoperative Anesthesia Satisfaction in Outpatient Gynecological Surgery: A Randomized Clinical Trial
Wang XL, Dai LL, Li YN, Zhang JW, Qu MC, Zhou YY, Xing N
Drug Design, Development and Therapy 2024, 18:4615-4627
Published Date: 18 October 2024
Analgesic and Hemodynamic Effects of Dexmedetomidine–Ketamine vs Fentanyl–Ketamine in Healthy Volunteers: A Randomized Trial
Green M, Hayley AC, Downey LA, Keane M, Kenneally ME, Chakravarthy K, Shehabi Y
Journal of Pain Research 2025, 18:2483-2496
Published Date: 16 May 2025