Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 14
Psychosocial Problems Among Primary School Children in Thailand During the COVID-19 Pandemic, 2022
Authors Pudpong N ![]() , Julchoo S
, Julchoo S ![]() , Sinam P, Uansri S, Kunpeuk W
, Sinam P, Uansri S, Kunpeuk W ![]() , Suphanchaimat R
, Suphanchaimat R ![]()
Received 8 November 2022
Accepted for publication 17 April 2023
Published 20 May 2023 Volume 2023:14 Pages 159—168
DOI https://doi.org/10.2147/PHMT.S396706
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Nareerut Pudpong,1 Sataporn Julchoo,1 Pigunkaew Sinam,1 Sonvanee Uansri,1 Watinee Kunpeuk,1 Rapeepong Suphanchaimat1,2
1International Health Policy Program, Ministry of Public Health, Nonthaburi, Thailand; 2Division of Epidemiology, Department of Disease Control, Nonthaburi, Thailand
Correspondence: Rapeepong Suphanchaimat, International Health Policy Program, Ministry of Public Health, Nonthaburi, Thailand, Tel +66815446966, Email [email protected]
Background: During the COVID-19 pandemic, primary school children are particularly vulnerable as restriction measures have caused a huge impact on their health and well-being. This study aims to assess the prevalence of mental health among primary school children in Thailand during the COVID-19 pandemic and identify factors associated with psychosocial problems.
Methods: A survey was conducted among 701 Thai parents of primary school children from January to March 2022 – when teaching modalities between onsite and online learning were alternated. Parents were requested to assess the mental health of their youngest child at primary school age level. Psychosocial problems were measured by the Strengths and Difficulties Questionnaire (SDQ) with a total score of 40, based on 4 domains (emotion, behavior, hyperactivity, and relationship). Independent variables included (1) parental/household factors, (2) children characteristics, and (3) online learning-related issues. The dependent variable was the prevalence of children with a total score of 14– 40, which indicates at risk and/or having mental health problems. The analysis was performed using logistic regression model.
Results: Thai parents reported that 41.1% of children had psychosocial problems. Children in a single-parent family (adjusted odds ratio [AOR] = 1.7; 95% confidence interval (CI) = 1.1– 2.8), male children (AOR = 1.7, 95% CI = 1.2– 2.4), and children who did not receive adequate assistance for online learning from their parents (AOR = 2.1, 95% CI = 1.1– 4.0) significantly faced greater odds of mental health problems.
Conclusion: The prevalence of Thai primary school children confronting psychosocial difficulties during the COVID-19 pandemic increased, with significant concern. Public health interventions that aim to protect the mental health of primary school children during the pandemic should be introduced and targeted male children and those living with a single parent. Social support that facilitates online learning for children whose parents have limited capacity in supporting them should be implemented.
Keywords: mental, health, primary school, children, COVID-19, Thailand
Introduction
The COVID-19 pandemic has significantly impacted people’s living conditions all around the globe. To prevent and control the spread of the 2019 novel coronavirus (COVID-19), several public health measures have been implemented. School closure is one of the measures, with distance and/or online learning becoming the solution to support learners in continuing their education. It was estimated that over 1.5 billion learners in 165 countries are affected by COVID-19 school closures, particularly in accessing digital devices as well as internet connectivity challenges.1 Primary school children are particularly vulnerable as restriction measures during the pandemic have caused a huge impact on their health and well-being. Evidence has shown that the pandemic has negatively influenced children’s health in many forms, such as physical activities, sleep patterns, eating habits, and psychosocial responses; mental issues such as difficulty in concentrating, boredom, irritability, restlessness, nervousness, feelings of loneliness, uneasiness, and worries have also emerged.2–6
The Strength and Difficulties Questionnaire (SDQ) is commonly used for assessing children’s psychosocial behaviors in order to provide appropriate assistance to children.7,8 This questionnaire consists of 25 questions in five domains: 1) emotional symptoms (5 items); 2) conduct problems (5 items); 3) hyperactivity/inattention (5 items); 4) peer relationship problems (5 items); and 5) prosocial behaviour (5 items). The total difficulties score is based on the first four domains, while the fifth domain refers to the strengths. The assessment by the SDQ can be done by children, parents, or teachers, depending on the user; however, self-assessments may be more suitable for older children and adolescents.
During the COVID-19 pandemic, the SDQ was employed to determine children’s psychosocial problems in several countries. In Europe, a study on primary school children’s emotional engagement with remote schooling during the 2020 lockdown in Ireland revealed that children (8–9 years) with higher scores in the hyperactivity had lower engagement with remote schooling both before and during the pandemic.9 Another study in Wales showed that 64.0% of children (5–10 years) were at high or very high risk of psychosocial problems,10 while a study in Lithuania showed that 44.7% of children (7–14 years) were at risk (13.1%) or showing psychosocial challenges (31.6%).11 A study in France explored the change of children’s SDQ scores (mean age = 9.5 years) and found that there was no significant difference before and during the lockdown; however, being a single child and being a boy were more likely to have a deterioration of the SDQ score.12 A German study that assessed the emotional symptoms in children showed that the SDQ score did not differ between the pandemic phases, and approximately 32.8–39.0% of children (6–13 years) were at risk of emotional problems.13
In the US, it was found that the lower total difficulties score was associated with park access, suggesting that children (6–17 years) required some outdoor activities to release their emotional stress during home confinements.14 Another study in the US revealed that older children (11–17 years) who attended school remotely had worse SDQ scores compared with those who attended school in-person, whereas younger children (6–10 years) who attended school remotely had slightly better SDQ scores than those who attended school in-person.15
In Asia, a study in Japan, which investigated the changes of children’s social relationships during and after quarantine, revealed that school closures and/or home confinements were not related to social behavior among elementary school children (4–9 years). However, hyperactivity and prosocial behavior scores were significantly higher than those in peer problems, conduct problems, and emotional symptoms.5 A study in Hong Kong showed that children (2–12 years) with special educational needs and/or acute or chronic disease, mothers with mental illness, single-parent families, and low-income families were at higher risk of psychosocial problems.16 Another study in China demonstrated the prevalence of children with abnormal total difficulties scores, including 7.16% for borderline, 3.34% for moderately abnormal, and 1.96% for prominently abnormal.17,18 One study in China showed that among 1771 adolescents ranging from junior high schools to universities suffered from mental health problems with the rates of occurrence of anxiety and depression at 28.3 and 30.8%, respectively.19
Like other countries, Thailand also dealt with the COVID-19 pandemic. From the initial outbreak in 2020 until mid-2022, school closures and online learning were implemented to minimise disruptions to learners’ education.20 Thai school children experienced school closures multiple times, depending on how severe the COVID-19 situation was, as well as how intense the government restriction measures were; most students ended up attending their classes online.
While there have been numerous research studies on the mental health of primary school children during the pandemic in developed countries, this topic has not yet been explored in the Thai context. Therefore, this study aims to assess the prevalence of psychosocial problems among primary school children in Thailand during the COVID-19 pandemic and to identify factors associated with those psychosocial challenges. The findings should provide helpful insights for public health responses if online education is ever required to temporarily replace onsite education again in certain emergencies.
Methods
Study Design and Participants
This cross-sectional survey was conducted from January to March 2022. Participants were parents and/or guardians of primary school children studying in 10 purposively selected schools in five Thailand’s major provinces (one public school and one private school in each province). The five provinces located in different regions, including Bangkok (Central), Chiang Rai (North), Udon Thani (Northeast), Chonburi (East), and Songkhla (South). The selection was based on the suggestion of local healthcare providers or local education officers and the willingness of school directors to participate in the research.
The sample size was calculated by using the formula—n = z2p (1−p)/d2, where “z”= 1.96 (reflecting the z-statistic for a two-tailed 95% confidence level), “p” reflects the prevalence of mental health among children, and “d” denotes acceptable error. Since no studies on children’s mental health during the pandemic in Thailand have been published yet, we used the prevalence of 13.7% of mental health among primary school children, assessed by the SDQ during a normal period in a normal period.21 We replaced “p” with 0.137 and replaced “d” with 0.04. After applying all parameters in the formula, 284 samples were needed. When accounting for a 20% non-response rate and incomplete information, the final sample size expanded to approximately 350 samples. We employed simple random sampling with probability proportional to size (PPS) for selecting parents from name lists in the participating schools.
Initially, we aimed to distribute the paper-based questionnaires to all parents. However, the COVID-19 situation was unstable due to the fluctuations in infected cases as well as the restriction measures enforced by the government. Hence, we could not physically visit certain schools and had to distribute the online questionnaires via Google forms instead. In the actual survey, we were able to acquire 730 participants, a relatively far larger number than the calculated sample size. To ensure the validity and reliability of the questionnaire, a pilot test was conducted prior to the online survey. Thirty students were given the questionnaire as a test, and their feedback was used to improve the questionnaire. School representatives were the primary point of contact, and they were informed about the objectives and details of the study.
Participants were given 15–20 minutes to complete each questionnaire. Incentives (500 THB or USD 13.8) were provided to all respondents who filled out the paper-based questionnaires. Participants were informed that their confidentiality would be ensured, and that their responses would be completely anonymous. The survey consisted of a total of 42 questions, covering five domains: participants’ demographic characteristics, online learning experiences during COVID-19, the physical health status of children and parents, mental health and psychosocial challenges among children and their parents, and family health and well-being. To ensure the quality of the data, we employed the instructional manipulation check (IMC) method by inserting one question to ask the participants “not to answer the question and leave it blank”. Therefore, we discarded 27 questionnaires where parents had still answered this IMC question by assuming that these questionnaires were not of good quality. We also discarded 2 questionnaires where the parents reported that they had no primary school children at home, thereby disqualifying their answers due to ineligibility. Finally, we acquired a total of 701 samples (paper-based = 231; online = 470). Supplementary File S1 shows the summary details of participants by school location (Table S1a) and type of questionnaires (Table S1b) included in the survey.
Data Collection
We began the data collection by coordinating with the designated teacher at each participating school. The questionnaires and survey methods were clearly explained to them. After that, the teachers were tasked with randomly distributing the questionnaires to parents. For schools that could be visited physically, paper-based questionnaires were used, whereas a Google Forms link or online questionnaires were sent to the designated teacher of each school that was contacted remotely. The designated teachers explained the purpose of the study to the participating parents and sent them the link to complete the questionnaire. Participants were given approximately one week to complete the paper-based form and two weeks for the online form. Upon completion of the paper-based form, participants returned the forms to the designated teacher and were subsequently passed on to the research team. Completed online questionnaires were received directly by the research team via the online application system. Characteristics of schools receiving either face-to-face or online surveys were shown in Supplementary File S1 (Table S1c).
Measurements
The Thai version of the 25-item SDQ was used in this study.8 We asked the parents/guardians to assess psychosocial problems of the family’s youngest child studying in primary school. Children’s mental health problems were measured by the total difficulties score (40), derived from the sum of 5 domains (emotion, behavior, hyperactivity, peer relationship, and prosocial behavior) that indicate the overall extent of a child’s psychosocial problems. According to the SDQ recommended cut‐off points and the analysis purpose, we categorized the scores into 2 groups: (i) normal mental condition (0–13), and (ii) at risk of and/or having problems (14–40).
Independent variables in this study were divided into 3 main groups: (1) parental/household factors, (2) children’s characteristics, and (3) online learning-related issues. Parental/household factors included gender, age (20–34, 35–44, and ≥45 years), education (none/primary school, high school/diploma, and bachelor’s degree or higher), monthly incomes (<=10,000, 10,001–30,000, and ≥30,001 Baht), parental status (with partner/single), family type (single/extended), and household size by number of people in the house (1–3, 4–5, and >5 people). Children’s characteristics comprised two variables: age and gender. Online learning-related factors included the number of digital devices, such as mobile phones/computers (0–1 and ≥2 devices), frequency of assisting the child during the learning time by parents (every day/not every day), and whether or not parents assisted the child by themselves (yes/no).
Data Analysis
Descriptive statistics (number and frequencies) were used to describe the characteristics of parents/guardians and of their children. The prevalence proportion of psychosocial problems among the studied children was calculated. A univariable analysis was employed to explore the association between the mental health outcomes and each independent variable. Only the variables that showed statistical significance in univariable analysis (p-value < 0.05) would be included in the multivariable analysis. A multivariable logistic regression was subsequently undertaken to account for independent variables all at once. Crude odds ratio (COR), adjusted odds ratio (AOR), and 95% confidence intervals (95% CI) were reported. All analyses were performed using STATA version 13.1 (license number: 401406358220).
Ethical Considerations
This study was approved by the Institute for the Development of Human Research Protections in Thailand (IHRP 1045/2021). All participants were asked to voluntarily sign a consent form. If interviewees felt uncomfortable responding to any questions at any point of time, they were free to stop the interview. Individual identification was kept anonymous. The ethics review followed the principles outlined in the Declaration of Helsinki.
Results
Characteristics of Parents, Children, and Online Learning-Related Issues
The characteristics of parents, children, and online learning-related issues are presented in Table 1. The majority of parents who answered the questionnaire was female (80.2%), and about half of them (54.4%) were at working age (35–45 years). Most parents (61.2%) were well educated as they had at least completed a bachelor’s degree. Almost half of them (49.5%) had monthly incomes of about 10,000–30,000 Baht, while about one-third of them (30.4%) received over 30,000 Baht/month. Most parents (79.0%) took care of the children with their partners. Participants from extended families slightly outnumbered those from single families (54.8% as opposed to 43.5%) and half of them had about 4–5 family members (50.9%). Children included in this assessment were relatively equal in number across age groups, with 42.7% for children aged 6–9 years and 45.2% for children aged 10–14 years. Male children (52.1%) slightly outnumbered female children (43.8%). Half of the parents reported having at most one electronic learning device at home (50.2%). Most of them reported that they assisted their children with learning at home every day (81.5%) and provided the assistance by themselves (89.0%).
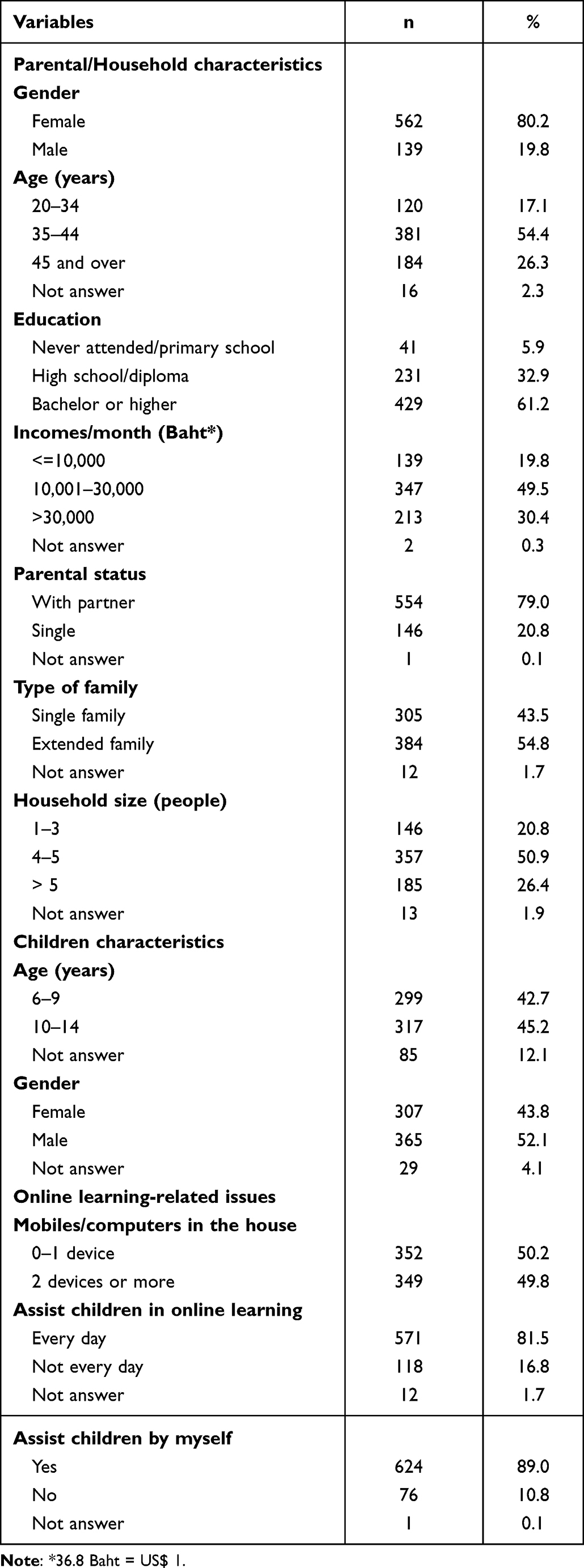 |
Table 1 Characteristics of Answering Parents, Children, and Online Learning-Related Issues (n = 701) |
Psychosocial Problems Among Thai Primary School Children
The prevalence of psychosocial problems among Thai primary school as determined by the SDQ is presented in Table 2. As shown in the table, just below half of the children (41.1%) were classified as at risk or having emotional and behavioral problems during the COVID-19 pandemic in 2022. When considering each domain of the SDQ, it was found that 68.9% of young children experienced peer relationship problems, followed by 37.4% with conduct problems and 30% with hyperactivity.
 |
Table 2 Psychological Problem Screening by Using the Strengths and Difficulties Questionnaire (SDQ) Among Thai Primary School Children Assessed by Parents (n = 701) During the COVID-19 Pandemic, 2022 |
Associated Factors on Psychosocial Problems
Results of the univariable and multivariable analyses are shown in Table 3. There was a significant association between psychosocial problems and being male children, living with parents completing up to high school/diploma level, living with a single parent, and those whose parents were unable to support online learning at home every day.
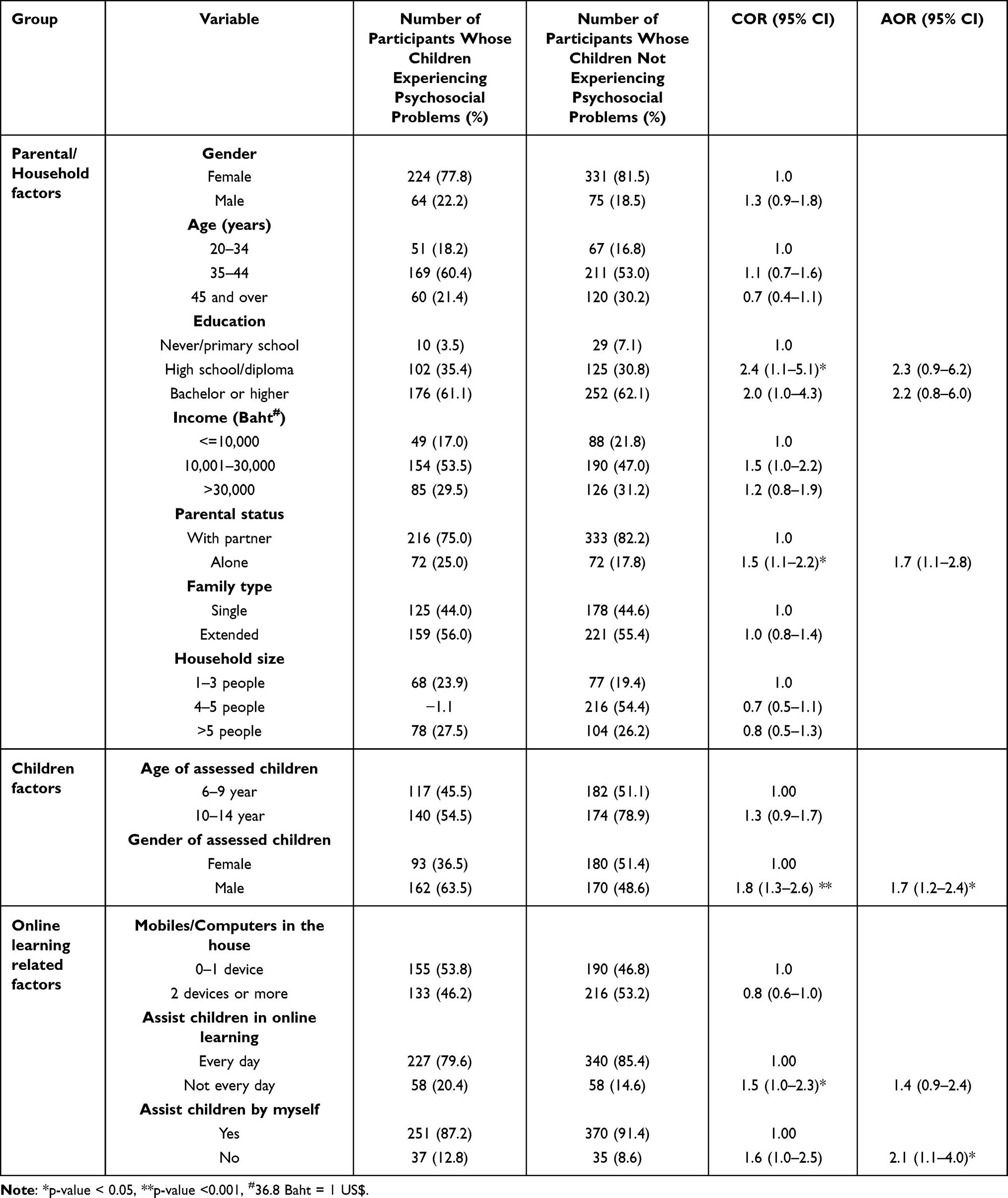 |
Table 3 Univariable and Multivariate Analyses on Psychosocial Problems Among Thai Primary School Children During the COVID-19 Pandemic, 2022 |
After adjusting for all significant variables, being male and living with a single parent remained statistically significant association with psychosocial problems (AOR = 1.7 [95% CI = 1.2–2.4] and AOR = 1.7 [95% CI = 1.1–2.8], respectively). Children whose parents did not provide daily assistance for online learning did not show a significant association with psychosocial challenges in the adjusted model. However, children whose parents reported that they helped their children with online learning by themselves revealed a significant association with psychosocial problems (AOR = 2.1, 95% CI = 1.1–4.0).
Since this study consisted of two different types of questionnaires (paper-based and online), we further explored whether there was a substantial difference between the questionnaire types; we found that both questionnaire types produced almost similar results (see Supplementary S2, Table S2).
Discussion
This study appears to be the first study to provide empirical evidence about psychosocial problems among primary school children during the COVID-19 pandemic in Thailand by using parent-reported SDQs. It was found that the prevalence of children’s psychosocial problems during the Covid pandemic in Thailand was 41.1%. This prevalence was much higher than that found in Bangkok children during normal period (13.7%).21
When comparing to other studies conducted elsewhere, the prevalence among Thai children was higher than German children (32.8–39.0%, although that study focused on the emotional domain only)13 and Chinese children (12.5% for borderline and abnormal scores combined).18 However, it was still lower than the prevalence among Lithuanian (44.7%)11 and Welsh (64.0%)10 children. The diverse findings might be due to several factors, such as differences in the period of assessment according to the COVID-19 situation (eg, comprehensive restriction phase versus relaxation phase), variation in the age of children assessed, and disparity in tradition or cultural difference. Nevertheless, all findings pointed to the fact that children around the world experienced some degrees of emotional and behavioral difficulties during the COVID-19 pandemic.
When exploring the effects of parents and household factors, we found that “living with a single parent” was significantly associated with psychosocial problems; both univariable and multivariable analyses indicated that this probability was 1.5–1.7 times greater than those living with both parents. This finding is consistent with the study in Germany, which found that children living with a single parent faced a 50% greater chance of having mental health problems (COR = 1.5 [95% CI = 0.71–3.16]), compared with those living with both parents, although no significant association was found in the adjusted model.13 However, it is important to note that the German study assessed only the emotional domain, not the total difficulties score. Nonetheless, the findings highlight that public health interventions to promote mental health among primary school children should target single-parent families, including parents with limited capacity in assisting their children with online learning. This is because, when considering online related factors, we also found that children were prone to have mental health problems when lacking assistance from their own parents (AOR = 2.1 [95% CI = 1.1–4.0]) or not receiving adequate assistance daily (COR = 1.5 [95% CI = 1.0–2.3]). This suggests that children require more support for their online education, and the support received from their caretakers is of utmost importance. A study in China also underpinned this point by revealing that a poor caregiver–child relationship was associated with both abnormal total difficulties scores and prosocial behavior scores.17 Moreover, evidence shows that during the lockdown period, art-based therapy including drawing-based interventions and music therapy could improve mental health and positive feelings among school children, and the impacts were likely to be greater with involvement of their parents.22–24
In addition, parental education seemed to be related to children’s psychosocial problems as we found a significant association in the crude model, but not in the adjusted model. This was in line with the German study, which reported the lack of a relationship between parental education and children’s mental health.13 However, this finding contrasted with a study in China, which reported that lower education levels of caregivers were associated with children’s abnormal total difficulties scores and abnormal prosocial behavior scores.18
In terms of children’s characteristics, we found that boys were more likely to have psychosocial problems than girls in both the crude (COR = 1.8 [95% CI = 1.3–2.6]) and the adjusted (AOR = 1.7 [95% CI = 1.2–2.4]) models. This finding contradicts studies in China18 and Lithuania,11 which did not find any gender effect on the SDQ scores. A study in New Zealand showed that there was inconclusive evidence regarding gender impact on children’s emotional and behavioral difficulties.25 It also suggested that boys identified as having more mental health problems than girls when reported by teachers; however, there was no difference in the SDQ scores between boys and girls when it was assessed by parents.25 It should also be noted that the New Zealand study was conducted during a non-pandemic period. Thus, the impact of gender differences on children’s mental health still requires further investigation.
This study contains some limitations. Firstly, since this is a cross-sectional survey during the COVID-19 pandemic in Thailand, public health implications from this study need to be approached cautiously as the country-specific context when the fieldwork was arranged may differ markedly from the present situation and causal relationship between cause (various independent variables) and outcome (psychosocial problems) cannot be firmly determined. Future research that employs a long-term and regular follow-up on mental health status changes in children will be very valuable. Secondly, we did not collect the data on children’s and/or parents’ medical conditions due to time limitations and difficulties in accessing personal illness data. As such, further psychiatric interviews will be useful to confirm evidence for psychopathologic processes. Physical health and illness may possibly be related to emotional and behavioral difficulties of children and therefore should be included as covariates in the regression model. Thirdly, this study relies on parents’ opinions, which may be susceptible to some degrees of social desirability bias. A comparison of the total difficulties score assessed by teachers and/or children themselves may be useful to confirm our findings. Fourthly, as this study mainly intended to estimate prevalence of children with psychological problems, the sample calculation was based on sample size calculation, not hypothesis testing from the outset. This means that in the assessment of statistical difference of psychological problems across each characteristic of the participants, one should be reminded that the statistical power might not suffice. For instance, we performed power analysis on some online learning-related factor and found that based on our data, the statistical power was less than 80% as mostly used in several studies. Finally, a comparison of the findings between our study and other studies should be made with caution as the characteristics of the study population always vary across studies. Although we recruited a vast range of primary schools from various regions all over Thailand, the findings still have limited generalisability. Moreover, the study was partially conducted online and therefore the data quality might need to be carefully interpreted when comparing with the data from the face-to-face questionnaire.
Conclusions
In conclusion, the prevalence of Thai primary school children confronting psychosocial challenges during the COVID-19 pandemic was relatively high, which should be one area of public health concern. Public health personnel as well as concerned stakeholders should urgently introduce interventions that aim to protect the mental health of primary school children during the pandemic, especially interventions targeted at male children and those living with a single parent. Social support that facilitates online learning for children whose parents had limited capacity in assisting with learning daily should be implemented. Our findings also highlight the importance of children’s mental health screening to monitor their problems and provide appropriate assistance during a period of public health emergencies when routine onsite education cannot be continued and is replaced by online education. In addition, to ensure that the problems have been addressed properly, further research that follows the changes of their mental health during the post-pandemic period should be undertaken.
Key Messages
- By using the parent-reported Strength and Difficulties Questionnaire (SDQ), it was found that the prevalence of children’s psychosocial problems during the COVID-19 pandemic in Thailand was 41.1%, which was much higher than that found in a normal period.
- Factors associated with children’s mental health included: being a boy, living with a single parent, lacking assistance from their own parents, and not receiving adequate assistance on a daily basis.
- During a public health emergency period, when onsite education cannot be continued and is replaced by online education, health interventions should be introduced and targeted at male children and those living with a single parent. Meanwhile, social support that facilitates online learning for children whose parents had limited capacity in assisting with learning daily should also be implemented.
- To ensure that children’s psychosocial problems have been addressed properly, follow-up of the changes of children’s mental health during the post-pandemic period should be undertaken.
Disclosure
The authors report no conflicts of interest in this work.
References
1. United Nations Educational SaCOU. UNESCO rallies international organizations, civil society and private sector partners in a broad Coalition to ensure #LearningNeverStops; 2020. Available from: https://en.unesco.org/news/unesco-rallies-international-organizations-civil-society-and-private-sector-partners-broad.
2. López-Bueno R, López-Sánchez G, Casajús J, et al. Health-related behaviors among school-aged children and adolescents during the Spanish Covid-19 confinement. Front Pediatr. 2020;8:573. doi:10.3389/fped.2020.00573
3. Lopez-Bueno R, Lopez-Sanchez G, Casajús J, Calatayud J, Tully M, Smith L. Potential health-related behaviors for pre-school and school-aged children during COVID-19 lockdown: a narrative review. Prev Med. 2021;143:106349. doi:10.1016/j.ypmed.2020.106349
4. Lehmann J, Lechner V, Scheithauer H. School closures during the COVID-19 pandemic: psychosocial outcomes in children - a systematic review. Int J Dev Sci. 2021;15:85–111. doi:10.3233/DEV-220322
5. Hagihara H, Yamamoto N, Meng X, et al. COVID‑19 school and kindergarten closure relates to children’s social relationships: a longitudinal study in Japan. Sci Rep. 2022;12:814. doi:10.1038/s41598-41022-04944-41592
6. Orgilés M, Morales A, Delvecchio E, Mazzeschi C, Espada J. Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Front Psychol. 2020;11:579038. doi:10.3389/fpsyg.2020.579038
7. Goodman R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry. 1997;38:581–586. doi:10.1111/j.1469-7610.1997.tb01545.x
8. Wongpiromsarn Y, Wipulakorn P, Nuanmanee S, Woener W, Mongkol A. Strengths and Difficulties Questionnaire (SDQ) Thai improved version: change and administration. J Ment Health Thai. 2011;19(2):128–134.
9. Chzhen Y, Symonds J, Devine D, et al. Learning in a pandemic: primary school children’s emotional engagement with remote schooling during the spring 2020 Covid-19 lockdown in Ireland. Child Indic Res. 2022;15:1517–1538. doi:10.1007/s12187-12022-09922-12188
10. Adegboye D, Williams F, Collishaw S, et al. Understanding why the COVID-19 pandemic-related lockdown increases mental health difficulties in vulnerable young children. JCCP Adv. 2021;1(1):e12005.
11. Jusienė R. Risk of behavioural and emotional disorders in Lithuanian school aged children as assessed with SDQ during the second lockdown due to COVID-19. Psichologija. 2021;64:77–85. doi:10.15388/Psichol.12021.15343
12. Pailhé A, Panico L, Solaz A. Children’s well-being and intra-household family relationships during the first COVID-19 lockdown in France. J Fam Res. 2021;2021:1–32.
13. Rathgeb C, Schillok H, Voss S, et al. Emotional situation of children and adolescents during the COVID-19 pandemic in Germany: results from the COVID-19 Snapshot Monitoring Study (COSMO). Int J Environ Res Public Health. 2022;19(5):2698. doi:10.3390/ijerph19052698
14. Hazlehurst M, Muqueeth S, Wolf K, Simmons C, Kroshus E, Tandon P. Park access and mental health among parents and children during the COVID-19 pandemic. BMC Public Health. 2022;22:800. doi:10.1186/s12889-12022-13148-12882
15. Hawrilenko M, Kroshus E, Tandon P, Christakis D. The association between school closures and child mental health during COVID-19. JAMA Netw Open. 2021;4(9):e2124092. doi:10.1001/jamanetworkopen.2021.24092
16. Tso W, Wong R, Tung K, et al. Vulnerability and resilience in children during the COVID‑19 pandemic. Eur Child Adolesc Psychiatry. 2022;31:161–176. doi:10.1007/s00787-020-01680-8
17. Wang J, Chen Y, Guo X, et al. Impact of COVID-19 related knowledge and precautions on emotional and behavioral problems among children during the post-pandemic in China: the explanatory value of emotional problems among caregivers. Front Psychol. 2021;12:712529. doi:10.3389/fpsyg.2021.712529
18. Wang J, Wang Y, Lin H, et al. Mental health problems among school-aged children after school reopening: a cross-sectional study during the COVID-19 post-pandemic in East China. Front Psychol. 2021;12:773134. doi:10.3389/fpsyg.2021.773134
19. Ren Z, Xin Y, Wang Z, Liu D, Ho RCM, Ho CSH. What factors are most closely associated with mood disorders in adolescents during the COVID-19 pandemic? A cross-sectional study based on 1771 adolescents in Shandong Province, China. Front Psychiatry. 2021;12:728278. doi:10.3389/fpsyt.2021.728278
20. Bangkokbiznews. Update!! School reopening measure for onsite learning on May 17, what to do?; 2022. Available from: https://www.bangkokbiznews.com/social/1004269.
21. Wongtapitien J. Behavioral and Emotional Expression of Depression In Senior Primary School Students in The Bangkok Area [Master Thesis]. Bangkok: Department of Psychiatry, Faculty of Medicine, Chulalongkorn University; 2011:106.
22. Malboeuf-Hurtubise C, Léger-Goodes T, Mageau GA, et al. Online art therapy in elementary schools during COVID-19: results from a randomized cluster pilot and feasibility study and impact on mental health. Child Adolesc Psychiatry Ment Health. 2021;15(1):15. doi:10.1186/s13034-021-00367-5
23. Cho E, Ilari BS. Mothers as home DJs: recorded music and young children’s well-being during the COVID-19 pandemic. Front Psychol. 2021;12. doi:10.3389/fpsyg.2021.637569
24. Le Vu MN, Do AL, Boyer L, et al. A review of the effectiveness, feasibility, and acceptability of art therapy for children and adolescents during the COVID-19 pandemic. Int J Environ Res Public Health. 2022;19(18):11612. doi:10.3390/ijerph191811612
25. Sargisson R, Stanley P, Hayward A. Multi-informant scores and gender differences on the strengths and difficulties questionnaire for New Zealand children. NZ J Psychol. 2016;45(2):4–12.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Delayed Sleep/Wake Rhythm with Depression During the First COVID-19 Lockdown in France
Felician J, Galvao F, Lefebvre M, Nourredine M, Peter-Derex L
Nature and Science of Sleep 2022, 14:1545-1557
Published Date: 2 September 2022
Factors Influencing the Antenatal Care Attendance of Pregnant Women During the First COVID-19 Wave Lockdown in Thailand
Chalermpichai T, Subsomboon K, Kasak R, Pinitlertsakun O, Pangzup S
International Journal of Women's Health 2023, 15:731-740
Published Date: 11 May 2023
Loneliness Trajectories, Associated Factors and Subsequent Health in Children and Young People During the COVID-19 Pandemic: A National Matched Cohort Study
Schneider V, Norris T, Nugawela M, Dalrymple E, Hargreaves D, Käll A, McOwat K, Shafran R, Stephenson T, Xu L, Pinto Pereira SM
Psychology Research and Behavior Management 2023, 16:4461-4477
Published Date: 1 November 2023
Mindfulness Through Storytelling for Mental Health of Primary School Children: Impact on Acceptability and Its Associations with Personality
Matiz A, Fabbro F, Crescentini C
Psychology Research and Behavior Management 2024, 17:1757-1774
Published Date: 25 April 2024
University Students’ Financial Situation During COVID-19 and Anxiety and Depressive Symptoms: Results of the COVID-19 German Student Well-Being Study (C19 GSWS)
Negash S, Horn J, Heumann E, Stock C, Zeeb H, Pischke CR, Matos Fialho PM, Helmer SM, Niephaus Y, Mikolajczyk R
Psychology Research and Behavior Management 2024, 17:2271-2285
Published Date: 4 June 2024