Back to Journals » Nature and Science of Sleep » Volume 14
Association of Delayed Sleep/Wake Rhythm with Depression During the First COVID-19 Lockdown in France
Authors Felician J, Galvao F, Lefebvre M, Nourredine M, Peter-Derex L ![]()
Received 11 May 2022
Accepted for publication 24 August 2022
Published 2 September 2022 Volume 2022:14 Pages 1545—1557
DOI https://doi.org/10.2147/NSS.S369859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Juliette Felician,1– 3 Filipe Galvao,3 Mylène Lefebvre,3 Mikail Nourredine,2,4– 6,* Laure Peter-Derex1,2,7,*
1Centre for Sleep Medicine and Respiratory Diseases, Hôpital de la Croix-Rousse, Hospices Civils de Lyon, Lyon, France; 2Medicine faculty, Lyon 1 University, Lyon, France; 3Unité Michel Jouvet – Pôle Est – Z19, Centre Hospitalier Le Vinatier, Bron, France; 4Biostatistics Unit, University Hospital Service of Pharmacotoxicology and Public Health Department, Hospices Civils de Lyon, Lyon, France; 5Research Department, Centre Hospitalier Le Vinatier, Bron, France; 6Biometry and Evolutionary Biology Laboratory, UMR CNRS 5558, Lyon, France; 7Lyon Neuroscience Research Centre, CNRS UMR 5292/INSERM U1028, Lyon, France
*These authors contributed equally to this work
Correspondence: Laure Peter-Derex, Centre for Sleep Medicine and Respiratory Diseases, Hôpital de la Croix-Rousse, Hospices Civils de Lyon, 103 Grande Rue de la Croix-Rousse, Lyon, 69004, France, Tel +33 4 72 07 17 69, Fax +33 4 72 07 28 08, Email [email protected]
Purpose: The containment of the population during the COVID-19 pandemic led to the emergence or recurrence of psychiatric conditions and sleep disorders. The influence of sleep/wake rhythm on mental health is well known. The objective of our study was to evaluate the link between the shift in sleep/wake rhythm and the presence of depressive symptoms during the March to May 2020 lockdown in the French population.
Participants and Methods: Participants (n = 2513) were recruited via newspapers and social networks in March 2020. We evaluated i) the chronotype before and during the lockdown, assessed by the change in mid-sleep time on work-free days corrected for sleep debt on workdays (delta MSFsc); ii) morningness-eveningness circadian preference (Horne & Ostberg questionnaire); iii) depressive symptoms (Patient Health Questionnaire-9, PHQ-9). The delta MSFsc and the PHQ-9 score were compared between circadian preference types. A multivariate model adjusted for age, sex, circadian preference, housing type, and marital status was used to assess the influence of delta MSFsc on the PHQ-9 score in the whole population.
Results: The population consisted of 77% women, of median (IQR) age 39 (30– 48) years. Compared with the pre-lockdown period, the median (IQR) MSFsc was shifted by 30 (0– 66) min during the lockdown, with a significant difference between evening [60 (15– 120) min], morning [15 (0– 46) min] and neutral [30 (0– 70) min] circadian type individuals, p < 0.001. One-third of all participants had moderate to severe depressive symptoms (PHQ-9 ≥ 10). A 1-hour shift in MSFsc was associated with a 0.50-point increase [95% CI (0.28; 0.72), p < 0.001] in the PHQ-9.
Conclusion: A phase delay in the chronotype was observed in the general population during lockdown. Such disruption was associated with depressive symptoms but the direction of the relationship remains hypothetical. The impact on mental health of preventive measures targeting the sleep/wake rhythm in this context needs further evaluation.
Keywords: phase delay, pandemic, containment, mental health, chronotype, circadian preference
Introduction
The COVID-19 pandemic emerged in late 2019 and spread fast across the world. The first cases were reported in China and subsequently in many other countries. A general population lockdown was declared on March 2020, 17th in France for a period of 2 months, aiming to reduce the number of cases and fatalities.1 However, containment was identified as an anxiety-provoking period2,3 due to various factors: isolation, boredom, lack of or overexposure to information, financial loss and fear of contamination.4 Such anxiety was worsened by limited autonomy, professional difficulties, stigma, loss of reference points and changes in physical activity.5
The first major national survey on psychological distress associated with lockdown in the general population was conducted in China.6 It showed that the containment measures were responsible for depressive and anxious symptoms likely to promote the development or recurrence of psychological disorders.6 In this study, nearly 35% of respondents reported experiencing psychological distress.6 Subsequently, several studies and systematic reviews have confirmed these findings, with a prevalence of depression in the general population during the COVID-19 pandemic ranging from 28% (95% CI [0.17–0.38])7 to 33.7% (95% CI [27.5–40.6]).8
In parallel, sleep disturbances associated with home confinement were reported in many countries.9,10 In France, the prevalence of insomnia increased by almost 50% compared to 2017.11 In the general population, rates of sleep disturbances reached 41% and proved to be more pronounced under lockdown conditions.10 Although the determinism of sleep disturbances appears to be multifactorial, insomnia was particularly associated with anxiety and mood disorders including suicidal ideation, presumably with a bidirectional relationship.9,12–15 Interestingly, changes in sleep-wake rhythm during confinement were one of the most prominent findings.16 Several patterns were consistently reported, including delayed bedtime with or without delayed wake-up time, as well as a decrease in “social jetlag” defined by the difference between weekday and weekend sleep times (ie, the mismatch between social and biological time),17 with an increase in sleep duration mitigated by a lower sleep quality.18–21 These changes in sleep-wake rhythms observed in a large part of the population during the lockdown were attributed to the reduced exposure of individuals to environmental cues such as outdoor daylight and daily social and occupational constraints, which are the main drivers of biological rhythms, but also to high levels of stress and anxiety linked to the pandemic.16,22–25
Circadian rhythms, including their phase, amplitude and period, play a key role not only in the regulation of sleep but also in mental health and cognitive functions.26,27 Some authors have shown that even a slight misalignment between the circadian phase and the timing of sleep period can disturb mood in healthy subjects.28 An association between an evening chronotype and the risk of depression, anxiety, and problematic substance use was also reported.29,30 The experimental advance shift of evening-type late timing with light exposure, behavioral measures and exercise leads to significant improvement in self-reported depression.31 Such modulation of brain physiology by circadian rhythms was recently shown to be underpinned by changes in cortical excitability, which is enhanced and associated with improved cognitive performance at the preferred time of the day.32 Interestingly, impaired cortical excitability and brain plasticity have also been reported in depression.33
Thus, the impact of lockdown on mood could be partly explained by sleep and circadian rhythm disturbances. However, it is not clear whether the changes in lifestyle and the decrease in schedule constraints, allowing individuals to bring their sleep-wake rhythm closer to their circadian preference, has a favorable or deleterious effect on mood. Whereas increased sleep problems and poorer mental health have been reported in evening-types during the pandemic, few studies have assessed the link between changes in sleep behavior (circadian rhythm shift, ie, change in chronotype) and depressive symptoms or negative emotions.34–36 Only one recent survey study performed on 1011 students in Bangladesh showed that participants shifted their chronotype according to their circadian preference, and that a shift toward earlier sleep-wake timing was related to better moods and well-being.35 We therefore aimed to extend these findings in the general population by exploring if delays in chronotype would be associated with lower mood and if this relationship would be modulated by circadian preference.
In this cross-sectional study based on questionnaires administered online in the general French population between April 2020 and June 2020 among 2609 participants, we investigated (i) the effect of changes in sleep-wake rhythms on depression symptoms during the containment and (ii) the factors modulating this relationship, including the demographic characteristics and the chronotype. We hypothesized that a greater shift in sleep-wake rhythm would be associated with an increased risk of depression, with a particular vulnerability of individuals with extreme circadian preference.
Materials and Methods
Study Procedure and Participants
We conducted a web-based self-reported cross-sectional questionnaire survey to collect data about sleep schedules and depressive symptoms. The questionnaire was built by psychiatrists and sleep physicians. The web-platform Framaforms was used to distribute the online-survey which was delivered in French language from April 2020, 9th to June 2020, 11th. At the time of the survey’s distribution, a strict lockdown had been imposed in France. The population was required to stay at home, and all non-essential activities were prohibited since March 2020, 17th.
To recruit a large number of participants, the survey was promoted via the Vinatier Hospital communication systems, social networking (Facebook, Twitter) as well as traditional media (local newspapers and radio programs). It took about 15 min to fill the questionnaire online and submit it. No monetary compensation was provided for participating in the study. Data were exported in xls format.
The study was approved by the Centre Hospitalier Le Vinatier Institutional Review Board and was conducted in accordance with the Declaration of Helsinki (protocol number: #2021.09.E01). All participants completed the survey anonymously and gave informed consent electronically before participating. General data protection regulations were applied to ensure privacy and confidentiality.
Questionnaires
Several dimensions were assessed in the questionnaires:
- Socio-demographic information: gender, age, cohabitation/marital status, employment status, children and their ages, housing (number of people in the dwelling, type and size of the dwelling, presence of an outdoor space).
- Medical data: psychiatric and non-psychiatric medical history and current treatments.
- Sleep patterns: work schedule before and during the containment, bedtime and wake-up time on weekdays and weekends before and during the containment, sleep duration, presence and duration of naps.
- Circadian preference: the Horne and Ostberg self-questionnaire37 was used to determine the circadian preference of the participants. A total score above 70 indicates a “very morning” circadian type, a score between 59 and 69 a “rather morning” circadian type, a score between 42 and 58 a “neutral” circadian type, a score between 31 and 41 a “rather evening” circadian type and a total score below 30 a “very evening” circadian type.
- Symptoms of depression: the Patient Health Questionnaire (PHQ-9)38 which is also a self-administered questionnaire was used to screen for the presence and severity of depression during the 2 last weeks. Its questions rate each of the 9 DSM-IV criteria for Major Depressive Disorder (MDD) (the core criteria for MDD have not changed in the DSM-V) from “0” (not at all) to “3” (almost every day). A total score of 5 to 9, 10 to 14, 15 to 19 and 20 to 27 indicates ? mild, moderate, moderately severe, and severe levels of depression, respectively. It has been shown that a score ≥10 has good sensitivity (0.88) and specificity (0.88) for screening for an MDD.39 A contact link was also provided to the participants (emergency call number and hotline of the Centre Hospitalier Le Vinatier) that could be reached in case of psychological distress.
This was a one-off questionnaire performed during the lockdown, meaning that the sleep/wake schedule before the lockdown was assessed retrospectively and that the symptoms of depression were assessed once.
Midsleep Point
In order to assess the chronotype, we used the mid-sleep point, which is one of the most accurate behavioral markers of the circadian phase.40,41 As sleep-wake schedules are constrained during workdays, the midsleep point is calculated on work-free days (MSF, MidSleep point on Free days), when the circadian system is under less pressure to adapt. However, most people accumulate a sleep debt during work days, which is compensated for on free days by waking-up later: this is the “social jetlag”. This sleep debt during workdays inducing sleep compensation on free days leads to a later MSF.42 In order to account for this confounding homeostatic factor, MSF corrected for sleep debt has been proposed (midsleep point on work-free days sleep debt corrected, MSFsc).43 The MSFsc is calculated by subtracting from the MSF half of the difference between the average duration of sleep on work-free days (SDf) and the average duration of sleep over the whole week (SDw). This correction was only applied to participants who slept longer on rest days than on work days (SDf > SDw).43
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD) or median (Q1-Q3) depending on their distribution and categorical variables as N and %. Circadian preference types were merged in 3 groups: morning (rather and quite morning time), neutral, and evening (rather and quite evening) types. The variation of MSFsc between pre- and per-lockdown periods and the PHQ-9 score were compared between the 3 circadian types with the Kruskal–Wallis test. A linear model with PHQ-9 score as dependent variable, and delta MSFsc, age, sex, housing type, cohabitation/marital status and circadian rhythm type as independent variables was used to assess the influence of delta MSFsc on the PHQ-9 score in the whole population. As our analysis was exploratory, we did not control for alpha risk inflation, so caution should be exercised in interpreting the significance level of the p-value, which was set at 0.05%.
Results
Among the 2609 participants who responded to the survey, 96 individuals were excluded. Reasons for exclusions were 1) age below 18 (n = 18 participants); 2) shift in MSFsc >4 hours (n = 78 participants) as expected changes in MSFsc were estimated to be around 30 minutes with a SD between 1:15 and 1:45.44,45 This 4h value (>30 min + 2 SD) allowed to exclude outliers mainly due to misunderstandings (eg, we noticed that some participants had recorded bedtimes and wake-up times in 12-hour instead of 24-hour format), a table is provided with characteristics of these outliers (Supplementary Table 1); The final sample consisted of 2513 participants, among which 285 were excluded from the multivariate analysis because of missing data for the main outcome or at least one of the adjustment variables.
Characteristics of the Population
The population consisted of 77% women, of median (IQR) age 39 (30–48) years. Two-thirds of participants were employees with daytime working hours before the confinement and worked from home during the lockdown. The demographic characteristics of the population are presented Table 1. Most individuals had never been treated for a psychiatric condition (N = 1965, 78%). In participants with a current or past psychiatric medical condition, the most common disorder was depression (N = 391) (Table 2). The most common reported treatments were antidepressants (N = 202) and anxiolytics (N = 147). Data regarding medical past apart from psychiatric history are presented in Supplementary Table 2.
 |
Table 1 Demographic Characteristics of the Participants |
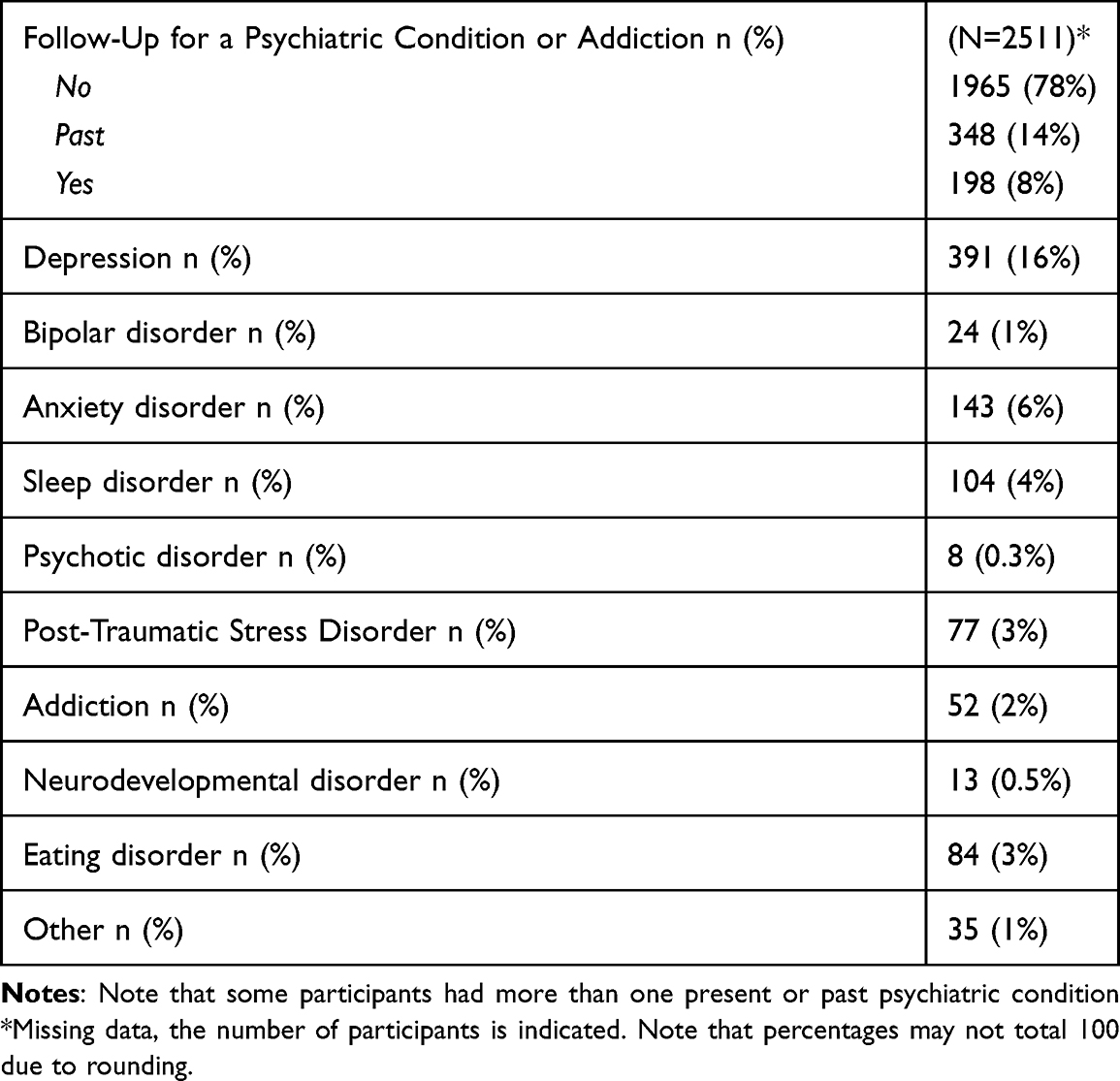 |
Table 2 Psychiatric Medical Past of the Participant |
The circadian preference evaluation with the Horne & Ostberg questionnaire showed a neutral type in 1325 (53%), a morning type in 892 (35%) and an evening type in 296 (12%) participants. The distribution of PHQ-9 severity scores is shown in Table 3. One-third of the population had a PHQ-9 score ≥10 (N = 730, 33%). The median PHQ-9 score was 7 (4, 11) in the whole population, but significant differences were observed between circadian preference groups (p < 0.001). Evening type individuals rated higher on PHQ-9 scale (9.0 [6.0, 15.0]) than neutral (7.0 [4.0, 11.0], p < 0.001) and morning (6.0 [2.0, 9.0], p < 0.001) types.
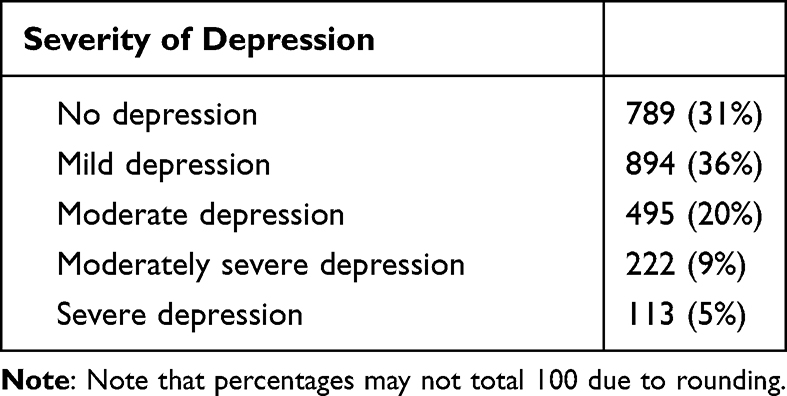 |
Table 3 Distribution of Phq-9 Scores Among Participants |
Sleep Schedule During Lockdown
The average (SD) reported total sleep time in the whole population before confinement was 7h29 (1h17) on weekdays and 8h43 (1h33) on weekends or days off. During the lockdown, the total sleep time was 7h36 (1h55) on weekdays and 8h26 (1h55) on weekends. A reduction in the difference in sleep habits between weekdays and weekends was also observed for napping. Before the lockdown, 42% of the participants took naps (33% on weekends or days off and 9% every day or almost every day) compared to 36% during the lockdown (18% on weekends and days off and 18% every day or almost every day).
The median (Q1, Q3) MSFsc increased from 3:30:00 (3:00:00, 04:19:00) before the lockdown to 4:00:00 (3:17:00, 5:00:00) during the lockdown (Figure 1 and Supplementary Table 3). The median change in MSFsc was 30 minutes (0, 66), with a significant difference between participants according to the circadian preference (p < 0.001). Evening type individuals shifted the MSFsc more (60.0 [15.0, 120.0]) than neutral (30.0 [0.0, 70.0], p < 0.001) and morning (15.0 [0.0, 46.0], p < 0.001) types.
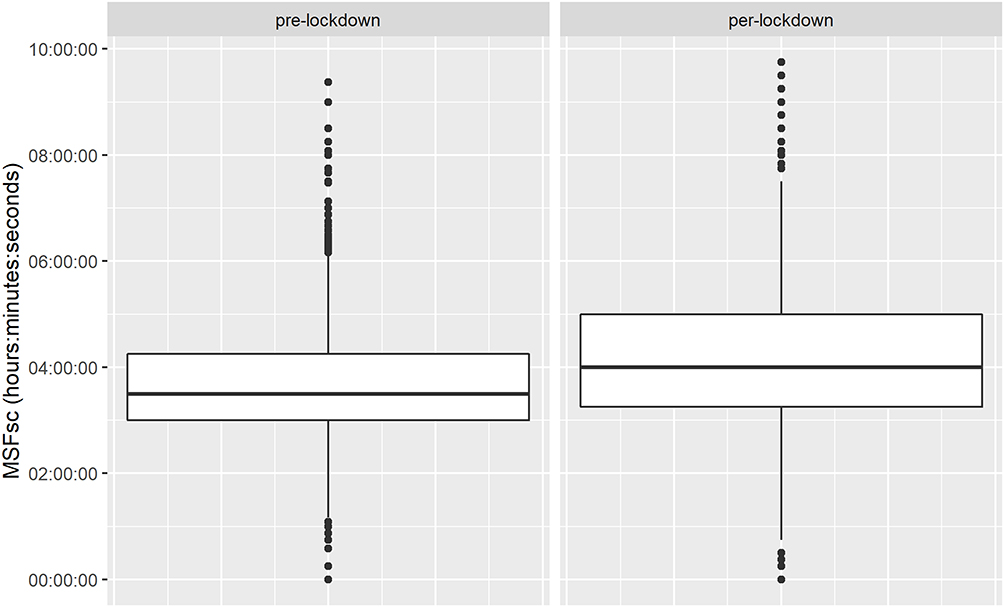 |
Figure 1 MSFsc change between pre- and per-lockdown. The median (Q1, Q3) MSFsc increased from 3:30:00 (3:00:00, 04:19:00) before the lockdown to 4:00:00 (03:17:00, 05:00:00) during the lockdown. |
Association Between Sleep Schedule and Depression During the Lockdown
The PHQ-9 score was significantly associated with sex, age, housing type, marital status, circadian preference and MSFsc shift; being a female, younger, living in an apartment (vs a house), being single, having a vesperal preference and showing a delay in MSFsc were associated with higher level of depression (Table 4). A multivariate analysis adjusted for sex, age, housing type, marital status and circadian preference showed that the shift in the MSFsc was associated with the PHQ-9 score (Table 5 and Figure 2). Including the presence of children aged up to 17 in the analysis did not improve the model (Supplementary Table 4). A one-hour increase in the MSFsc between pre- and per-lockdown was associated with a 0.50 [95% CI 0.28–0.72] increase in the PHQ-9 score (p < 0.001).
 |
Table 4 Univariate Analysis of the PHQ-9 Score |
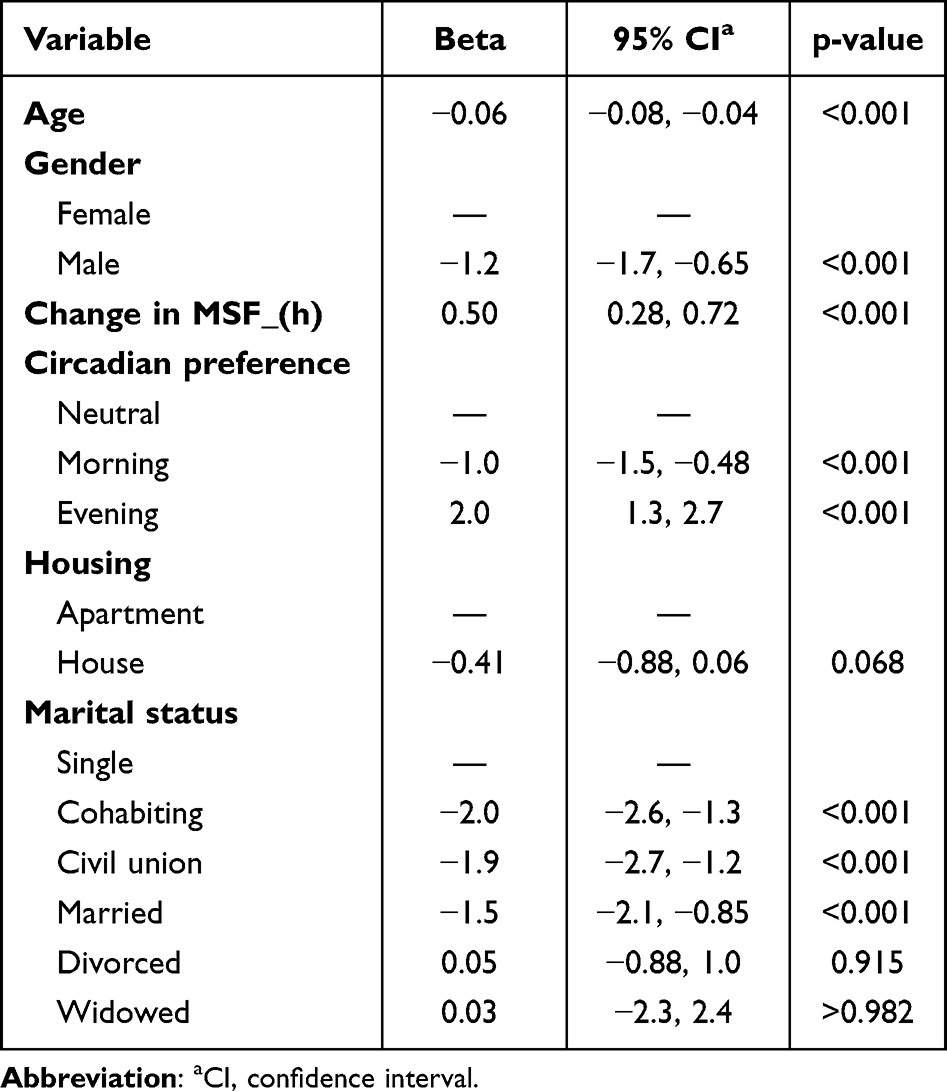 |
Table 5 Multivariate Analysis of PHQ-9 Score |
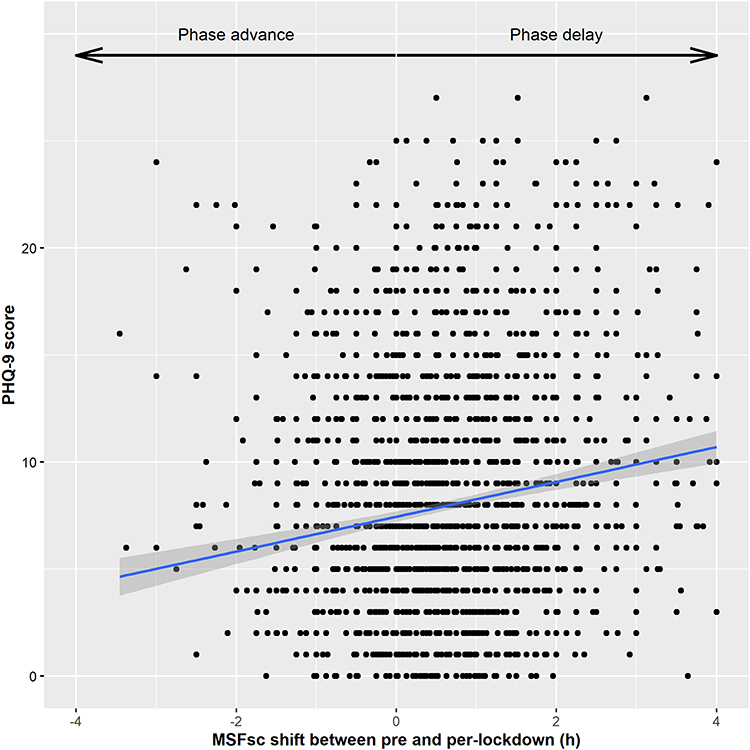 |
Figure 2 Correlation between change in MSFsc and depression symptoms. The depression severity score as assessed by the PHQ-9 scale is positively correlated with the change in MSFsc between pre- and per-lockdown period (expressed in hours, h). Note that a negative MSFsc shift indicates a phase advance and a positive MSFsc shift indicates a phase delay. |
Discussion
In this cross-sectional study performed during the first lockdown in France in 2158 participants we found i) a delay in the chronotype of about 30 min as estimated by the MSFsc as well as a reduction in the difference in total sleep time between weekdays and weekends; ii) a high rate of moderate to severe depressive symptoms, reported in over a third of the population; iii) an association between the amplitude of the sleep-wake rhythm shift and depressive symptoms.
The 30-minute delay in MSFsc during the lockdown can be explained by a shift in bedtime and wake-up time along with a decrease in sleep debt during the week. These findings of a later and longer sleep during weekdays, thus reducing social jetlag, corroborate previous studies performed during the lockdown: Leone et al found a 36-minute delay in MSFsc in the Argentina’s population44 and Smit et al reported a 30-minute delay in sleep schedule in Canadian students.45 Such change in sleep-wake rhythm during the week may be related to the fact that most participants of our study worked from home during the lockdown, with more flexible schedules and a decrease in exposure to external synchronizers such as outdoor daylight and social constraints.22 It may also result from the psychological distress linked to the pandemic.24 In our study, although most participants had a neutral circadian preference according to the Horne & Ostberg questionnaire, morning types (37%) were over-represented as compared to evening types (12%). This finding differs from the distribution of circadian preference in the general population, showing a slight overrepresentation of later types.46 This can be explained by the characteristics of our population, which was mostly composed of females, with a median age of 39 years. Indeed, the circadian preference is related to age and gender, morning type being more frequent in older and female individuals.46,47 It may also have resulted from the fact that almost one-fourth of the participants had a child younger than 18 years, given the association between childcare and earlier chronotype in women and men younger than 40 years.48 Interestingly, “evening” subjects shifted their sleep more, presumably because they had the opportunity to align with their physiological rhythm in the absence of constraints, in line with previous studies on the topic.34 It should be noted that the increase in sleep duration on workdays during confinement was modest, compared with previous studies in the field.21,44 This may be related to country-specific habits or to the characteristics of our population, which included more women and few participants working exclusively at home.
A high rate of depressive symptoms was observed in our study. The proportion of moderate to severe depression, according to the PHQ-9, reached one-third of patients which is within the range of values reported in other studies.7,8 The high level of psychological distress during the pandemic, and specifically the impact on mental well-being and mood of public health measures restraining daily life, was highlighted as early as 2020.49 Several factors have been identified as contributing to mental health issues related to confinement, including demographic characteristics such as female gender and young age, as confirmed by our study.50 We also showed that being single and living in an apartment (as opposed to a house, which is usually larger and more exposed to light) were associated with higher PHQ-9 scores. Bereavement, social isolation, uncertainty and socioeconomic distress, poor diet and low physical activity, as well as individual factors such as low resilience, were also reported to be involved in adverse mental health issues.51–55 Interestingly, we found that individuals with late circadian preference seemed to be more vulnerable and scored higher on depression scale. This finding echoes the literature about eveningness impact on general health including mental diseases.56,57 Recently, a multinational cross-sectional study conducted on 19,267 adults examined the potential role of circadian preference in explaining sleep and mental health outcomes during the first wave of the COVID-19 pandemic.34 The investigators explored the circadian preference (assessed by a single question), as well as sleep-wake schedule and sleep quality before and during the pandemic, insomnia symptoms, anxiety (GAD-2), depression (PHQ-2), post-traumatic stress disorder symptoms, stress and quality of life. They found poorer outcomes among evening types regarding employment, financial status, mental health status and quality of life. They also observed increased sleep duration, later midpoint of sleep and decreased sleep quality in these participants. These findings were moderated by socio-economic status and confinement. However, in this study, the relationship between circadian rhythm shift and mental health was not assessed.34
The main result of our study is that the shift in sleep schedule was associated with more severe depressive symptoms as assessed by the PHQ-9 score. Although this effect was quantitatively limited (0.5 points on the PHQ-9 scale for 1-hour MSFsc shift) and the risk of depression appeared to be multifactorial (age, gender, circadian preference, social environment), this relationship suggests that chronotype and mood are closely linked. To our knowledge, only one recent study performed on university students reported the association between change in sleep patterns and risk of depression according to the circadian preference in the context of population containment.35 Our study is therefore an important step towards a better understanding of the impact of sleep-wake rhythms on the risk of depression when individuals are no longer exposed to the usual social environmental constraints. Our results may seem somewhat counter-intuitive. Indeed, social jetlag and sleep restriction during the week have been associated with negative health-related outcomes including metabolic and cardiovascular conditions, performances, and are also suspected to increase the risk of depression.58 Thus, one may have expected that the decrease in social jetlag during the pandemic, linked to increased flexibility in sleep-wake schedules, might have alleviated sleep disturbances and mental health disorders especially in evening-type individuals. Our results can be interpreted in several ways. One can hypothesize that the depressive symptoms may have led to sleep-wake rhythm disruption as circadian misalignment has been reported for several biological rhythms in MDD.27,59,60 Another explanation is that common underlying factors may explain both the depression and the shift in chronotype in the pandemic context (eg, unemployment or financial loss, which were reported to be more frequent during the pandemic in evening circadian types).34 However, the change in chronotype itself may exert an impact on depression.27 Such a relationship has been reported for shift work and social jetlag even if data in the latter case are less consistent.61,62 Experimental data obtained in animal models by manipulation of the suprachiasmatic nucleus activity strongly support the negative effect of circadian rhythm disruption on depressive symptoms.63,64 Mechanisms underlying the relationship between change in chronotype and depression may involve disturbances in cortical excitability and impaired synaptic plasticity.32,33 Only longitudinal and interventional studies will allow to disentangle the respective influence of these different factors. Interestingly, preliminary studies suggest that keeping stable routine including physical exercise and regular sleep hours during home confinement may have a positive impact on mood, suggesting a causal link between sleep-wake schedule and mental health.65
One of the strengths of this study was its rapid implementation and its large sample size. Indeed, although the lockdown containment was a sudden decision, we managed to set up the study and disseminate the questionnaire quickly using the virtual snowball sampling technique.66 We used Facebook because it is an effective approach for engaging the so-called “hard-to-reach” populations.66 In addition, we combined the social network dissemination with the use of traditional media, in order to reach other populations, especially those who do not have access to the internet. This may have balanced the results as we know that social media can be particularly attractive to people in distress, looking for answers or support, which can create bias.67
We acknowledge several limitations to our work. First, its cross-sectional design allowed us to highlight possible links but prevented us from drawing conclusion about causality. Additionally, as in most studies performed in this context, it is not possible to rule out a memory bias in the retrospective estimation of the sleep-wake rhythm before confinement. Second, depressive symptoms were assessed only once at the time of confinement, and several other factors may have contributed to the depressed mood; some were included in our model, such as age, gender, and marital status, but others may also have modulated well-being and sleep-wake rhythms, such as screen exposure and time spent outdoors.23,68 Third, it should be noted that our sample included a high proportion of middle-aged, employed women with a morning chronotype. As some of these characteristics may be related to better resources for coping with the pandemic, this may limit the generalizability of our results. Fourth, the use of self-report screening questionnaires without additional clinical assessment may have led us to overestimate the prevalence of the conditions explored.69 Finally, previous work focusing on the evolution of psychological distress during infectious disease outbreak has shown that, although initial reactions were characterized by high levels of anxiety, these symptoms tended to decrease over the course of the pandemic.70,71 Some studies suggest that the same findings may be observed for the COVID-19 pandemic.72 The change in chronotype might also prove to be temporary and recoverable, reflecting the variability of restrictions imposed to the population as the pandemic develops. Further studies will be needed to assess the long-term effect of the population containments as well as the COVID-19 pandemic on mental health and sleep.
Conclusion
In a containment situation, a phase delay in the chronotype was observed in the general population. Such disruption is associated with depressive symptoms, with a greater vulnerability in people with an evening circadian preference. The mechanisms underlying this association are still hypothetical because depression can also influence the sleep/wake rhythm. The impact on mental health of preventive measures targeting the sleep/wake rhythm in this context should be further evaluated.
Disclosure
The abstract of this paper was presented at the 16th World Sleep Congress in March 2022 as an abstract presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Sleep Medicine doi: 10.1016/j.sleep.2022.05.130.
The authors report no conflicts of interest in this work.
References
1. Fowler JH, Hill SJ, Levin R, Obradovich N, Barbarossa MV. Stay-at-home orders associate with subsequent decreases in COVID-19 cases and fatalities in the United States. PLoS One. 2021;16(6):e0248849. doi:10.1371/journal.pone.0248849
2. Pfefferbaum B, North CS. Mental health and the Covid-19 pandemic. N Engl J Med. 2020;383(6):510–512. doi:10.1056/NEJMp2008017
3. Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M. The psychological impact of COVID-19 on the mental health in the general population. QJM. 2020;113:531–537. doi:10.1093/qjmed/hcaa201
4. Leger D, Beck F, Fressard L, Verger P, Peretti-Watel P, Group C. Poor sleep associated with overuse of media during the COVID-19 lockdown. Sleep. 2020;43(10). doi:10.1093/sleep/zsaa125
5. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
6. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr. 2020;33(2):e100213. doi:10.1136/gpsych-2020-100213
7. Ren X, Huang W, Pan H, Huang T, Wang X, Ma Y. Mental health during the Covid-19 outbreak in China: a meta-analysis. Psychiatr Q. 2020;91(4):1033–1045. doi:10.1007/s11126-020-09796-5
8. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1):57. doi:10.1186/s12992-020-00589-w
9. Yuksel D, McKee GB, Perrin PB, et al. Sleeping when the world locks down: correlates of sleep health during the COVID-19 pandemic across 59 countries. Sleep Health. 2021;7(2):134–142. doi:10.1016/j.sleh.2020.12.008
10. Jahrami HA, Alhaj OA, Humood AM, et al. Sleep disturbances during the COVID-19 pandemic: a systematic review, meta-analysis, and meta-regression. Sleep Med Rev. 2022;62:101591. doi:10.1016/j.smrv.2022.101591
11. Beck F, Leger D, Fressard L, Peretti-Watel P, Verger P, Coconel G. Covid-19 health crisis and lockdown associated with high level of sleep complaints and hypnotic uptake at the population level. J Sleep Res. 2021;30(1):e13119. doi:10.1111/jsr.13119
12. Cellini N, Canale N, Mioni G, Costa S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in Italy. J Sleep Res. 2020;29(4):e13074. doi:10.1111/jsr.13074
13. Franceschini C, Musetti A, Zenesini C, et al. Poor sleep quality and its consequences on mental health during the COVID-19 lockdown in Italy. Front Psychol. 2020;11:574475. doi:10.3389/fpsyg.2020.574475
14. Killgore WDS, Cloonan SA, Taylor EC, Fernandez F, Grandner MA, Dailey NS. Suicidal ideation during the COVID-19 pandemic: the role of insomnia. Psychiatry Res. 2020;290:113134. doi:10.1016/j.psychres.2020.113134
15. Zhao X, Lan M, Li H, Yang J. Perceived stress and sleep quality among the non-diseased general public in China during the 2019 coronavirus disease: a moderated mediation model. Sleep Med. 2021;77:339–345. doi:10.1016/j.sleep.2020.05.021
16. Salehinejad MA, Azarkolah A, Ghanavati E, Nitsche MA. Circadian disturbances, sleep difficulties and the COVID-19 pandemic. Sleep Med. 2022;91:246–252. doi:10.1016/j.sleep.2021.07.011
17. Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: misalignment of biological and social time. Chronobiol Int. 2006;23(1–2):497–509. doi:10.1080/07420520500545979
18. Wright KP
19. Robillard R, Dion K, Pennestri MH, et al. Profiles of sleep changes during the COVID-19 pandemic: demographic, behavioural and psychological factors. J Sleep Res. 2021;30(1):e13231. doi:10.1111/jsr.13231
20. Blume C, Schmidt MH, Cajochen C. Effects of the COVID-19 lockdown on human sleep and rest-activity rhythms. Curr Biol. 2020;30(14):R795–R797. doi:10.1016/j.cub.2020.06.021
21. Korman M, Tkachev V, Reis C, et al. COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci Rep. 2020;10(1):22225. doi:10.1038/s41598-020-79299-7
22. Skeldon AC, Phillips AJ, Dijk DJ. The effects of self-selected light-dark cycles and social constraints on human sleep and circadian timing: a modeling approach. Sci Rep. 2017;7:45158. doi:10.1038/srep45158
23. Conroy DA, Hadler NL, Cho E, et al. The effects of COVID-19 stay-at-home order on sleep, health, and working patterns: a survey study of US health care workers. J Clin Sleep Med. 2021;17(2):185–191. doi:10.5664/jcsm.8808
24. Innocenti P, Puzella A, Mogavero MP, Bruni O, Ferri R. Letter to editor: coVID-19 pandemic and sleep disorders-a web survey in Italy. Neurol Sci. 2020;41(8):2021–2022. doi:10.1007/s10072-020-04523-1
25. Sinha M, Pande B, Sinha R. Impact of COVID-19 lockdown on sleep-wake schedule and associated lifestyle related behavior: a national survey. J Public Health Res. 2020;9(3):1826. doi:10.4081/jphr.2020.1826
26. Wirz-Justice A. Chronobiology and psychiatry. Sleep Med Rev. 2007;11(6):423–427. doi:10.1016/j.smrv.2007.08.003
27. Walker WH 2nd, Walton JC, DeVries AC, Nelson RJ. Circadian rhythm disruption and mental health. Transl Psychiatry. 2020;10(1):28. doi:10.1038/s41398-020-0694-0
28. Danilenko KV, Cajochen C, Wirz-Justice A. Is sleep per se a zeitgeber in humans? J Biol Rhythms. 2003;18(2):170–178. doi:10.1177/0748730403251732
29. Merikanto I, Kronholm E, Peltonen M, Laatikainen T, Vartiainen E, Partonen T. Circadian preference links to depression in general adult population. J Affect Disord. 2015;188:143–148. doi:10.1016/j.jad.2015.08.061
30. Taylor BJ, Hasler BP. Chronotype and mental health: recent advances. Curr Psychiatry Rep. 2018;20(8):59. doi:10.1007/s11920-018-0925-8
31. Facer-Childs ER, Middleton B, Skene DJ, Bagshaw AP. Resetting the late timing of “night owls” has a positive impact on mental health and performance. Sleep Med. 2019;60:236–247. doi:10.1016/j.sleep.2019.05.001
32. Salehinejad MA, Wischnewski M, Ghanavati E, Mosayebi-Samani M, Kuo MF, Nitsche MA. Cognitive functions and underlying parameters of human brain physiology are associated with chronotype. Nat Commun. 2021;12(1):4672. doi:10.1038/s41467-021-24885-0
33. Cantone M, Bramanti A, Lanza G, et al. Cortical plasticity in depression. ASN Neuro. 2017;9(3):1759091417711512. doi:10.1177/1759091417711512
34. Merikanto I, Kortesoja L, Benedict C, et al. Evening-types show highest increase of sleep and mental health problems during the COVID-19 pandemic-multinational study on 19 267 adults. Sleep. 2022;45(2). doi:10.1093/sleep/zsab216
35. Hasan MM, Jankowski KS, Khan MHA. Morningness-eveningness preference and shift in chronotype during COVID-19 as predictors of mood and well-being in university students. Pers Individ Dif. 2022;191:111581. doi:10.1016/j.paid.2022.111581
36. Chen S, Huang T, Huang Y, et al. A population-level analysis of changes in circadian rhythms and sleep and their association with negative emotions during the outbreak of COVID-19 in China. COVID. 2022;2(4):450–463. doi:10.3390/covid2040032
37. Horne JA, Ostberg O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int J Chronobiol. 1976;4(2):97–110.
38. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
39. Levis B, Benedetti A, Thombs BD; Collaboration DESD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. doi:10.1136/bmj.l1476
40. Terman JS, Terman M, Lo ES, Cooper TB. Circadian time of morning light administration and therapeutic response in winter depression. Arch Gen Psychiatry. 2001;58(1):69–75. doi:10.1001/archpsyc.58.1.69
41. Kantermann T, Sung H, Burgess HJ. Comparing the morningness-eveningness questionnaire and Munich chronotype questionnaire to the dim light melatonin onset. J Biol Rhythms. 2015;30(5):449–453. doi:10.1177/0748730415597520
42. Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: daily temporal patterns of human chronotypes. J Biol Rhythms. 2003;18(1):80–90. doi:10.1177/0748730402239679
43. Roenneberg T, Pilz LK, Zerbini G, Winnebeck EC. Chronotype and social jetlag: a (Self-) critical review. Biology (Basel). 2019;8(3). doi:10.3390/biology8030054
44. Leone MJ, Sigman M, Golombek DA. Effects of lockdown on human sleep and chronotype during the COVID-19 pandemic. Curr Biol. 2020;30(16):R930–R931. doi:10.1016/j.cub.2020.07.015
45. Smit AN, Juda M, Livingstone A, Sr U, Mistlberger RE. Impact of COVID-19 social-distancing on sleep timing and duration during a university semester. PLoS One. 2021;16(4):e0250793. doi:10.1371/journal.pone.0250793
46. Roenneberg T, Kuehnle T, Juda M, et al. Epidemiology of the human circadian clock. Sleep Med Rev. 2007;11(6):429–438. doi:10.1016/j.smrv.2007.07.005
47. Baehr EK, Revelle W, Eastman CI. Individual differences in the phase and amplitude of the human circadian temperature rhythm: with an emphasis on morningness-eveningness. J Sleep Res. 2000;9(2):117–127. doi:10.1046/j.1365-2869.2000.00196.x
48. Sladek M, Kudrnacova Roschova M, Adamkova V, Hamplova D, Sumova A. Chronotype assessment via a large scale socio-demographic survey favours yearlong standard time over daylight saving time in central Europe. Sci Rep. 2020;10(1):1419. doi:10.1038/s41598-020-58413-9
49. Ammar A, Mueller P, Trabelsi K, et al. Psychological consequences of COVID-19 home confinement: the ECLB-COVID19 multicenter study. PLoS One. 2020;15(11):e0240204. doi:10.1371/journal.pone.0240204
50. Terry PC, Parsons-Smith RL, Terry VR. Mood responses associated with COVID-19 restrictions. Front Psychol. 2020;11:589598. doi:10.3389/fpsyg.2020.589598
51. Czeisler ME, Howard ME, Rajaratnam SMW. Mental health during the COVID-19 pandemic: challenges, populations at risk, implications, and opportunities. Am J Health Promot. 2021;35(2):301–311. doi:10.1177/0890117120983982b
52. Tsang S, Avery AR, Duncan GE. Do married and/or cohabiting individuals fare better during the COVID-19 pandemic? Satisfaction with life and depression among adult twins in the United States. Psychol Health Med. 2022;1–8. doi:10.1080/13548506.2022.2039397
53. Xiao H, Zhang Y, Kong D, Li S, Yang N. Social capital and sleep quality in individuals who self-isolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Med Sci Monit. 2020;26:e923921. doi:10.12659/MSM.923921
54. Ingram J, Maciejewski G, Hand CJ. Changes in diet, sleep, and physical activity are associated with differences in negative mood during COVID-19 lockdown. Front Psychol. 2020;11:588604. doi:10.3389/fpsyg.2020.588604
55. Lenzo V, Quattropani MC, Musetti A, et al. Resilience contributes to low emotional impact of the COVID-19 outbreak among the general population in Italy. Front Psychol. 2020;11:576485. doi:10.3389/fpsyg.2020.576485
56. Au J, Reece J. The relationship between chronotype and depressive symptoms: a meta-analysis. J Affect Disord. 2017;218:93–104. doi:10.1016/j.jad.2017.04.021
57. Fabbian F, Zucchi B, De Giorgi A, et al. Chronotype, gender and general health. Chronobiol Int. 2016;33(7):863–882. doi:10.1080/07420528.2016.1176927
58. Caliandro R, Streng AA, van Kerkhof LWM, van der Horst GTJ, Chaves I. Social jetlag and related risks for human health: a timely review. Nutrients. 2021;13(12):4543. doi:10.3390/nu13124543
59. Vadnie CA, McClung CA. Circadian rhythm disturbances in mood disorders: insights into the role of the suprachiasmatic nucleus. Neural Plast. 2017;2017:1504507. doi:10.1155/2017/1504507
60. Emens J, Lewy A, Kinzie JM, Arntz D, Rough J. Circadian misalignment in major depressive disorder. Psychiatry Res. 2009;168(3):259–261. doi:10.1016/j.psychres.2009.04.009
61. Lee A, Myung SK, Cho JJ, Jung YJ, Yoon JL, Kim MY. Night shift work and risk of depression: meta-analysis of observational studies. J Korean Med Sci. 2017;32(7):1091–1096. doi:10.3346/jkms.2017.32.7.1091
62. Levandovski R, Dantas G, Fernandes LC, et al. Depression scores associate with chronotype and social jetlag in a rural population. Chronobiol Int. 2011;28(9):771–778. doi:10.3109/07420528.2011.602445
63. Ben-Hamo M, Larson TA, Duge LS, et al. Circadian forced desynchrony of the master clock leads to phenotypic manifestation of depression in rats. eNeuro. 2016;3(6):
64. Landgraf D, Long JE, Proulx CD, Barandas R, Malinow R, Welsh DK. Genetic disruption of circadian rhythms in the suprachiasmatic nucleus causes helplessness, behavioral despair, and anxiety-like behavior in mice. Biol Psychiatry. 2016;80(11):827–835. doi:10.1016/j.biopsych.2016.03.1050
65. Zubek J, Ziembowicz K, Pokropski M, Gwiazdzinski P, Denkiewicz M, Boros A. Rhythms of the day: how electronic media and daily routines influence mood during COVID-19 pandemic. Appl Psychol Health Well Being. 2021;14:519–536. doi:10.1111/aphw.12317
66. Baltar F, Brunet I. Social research 2.0: virtual snowball sampling method using Facebook. Internet Research. 2012;22(1):57–74. doi:10.1108/10662241211199960
67. Gao J, Zheng P, Jia Y, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS One. 2020;15(4):e0231924. doi:10.1371/journal.pone.0231924
68. Korman M, Tkachev V, Reis C, et al. Outdoor daylight exposure and longer sleep promote wellbeing under COVID-19 mandated restrictions. J Sleep Res. 2022;31(2):e13471. doi:10.1111/jsr.13471
69. Thombs BD, Kwakkenbos L, Levis AW, Benedetti A. Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. CMAJ. 2018;190(2):E44–E49. doi:10.1503/cmaj.170691
70. Jones JH, Salathe M. Early assessment of anxiety and behavioral response to novel swine-origin influenza A(H1N1). PLoS One. 2009;4(12):e8032. doi:10.1371/journal.pone.0008032
71. Tausczik Y, Faasse K, Pennebaker JW, Petrie KJ. Public anxiety and information seeking following the H1N1 outbreak: blogs, newspaper articles, and Wikipedia visits. Health Commun. 2012;27(2):179–185. doi:10.1080/10410236.2011.571759
72. Liao YH, Fan BF, Zhang HM, et al. The impact of COVID-19 on subthreshold depressive symptoms: a longitudinal study. Epidemiol Psychiatr Sci. 2021;30:e20. doi:10.1017/S2045796021000044
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychosocial Problems Among Primary School Children in Thailand During the COVID-19 Pandemic, 2022
Pudpong N, Julchoo S, Sinam P, Uansri S, Kunpeuk W, Suphanchaimat R
Pediatric Health, Medicine and Therapeutics 2023, 14:159-168
Published Date: 20 May 2023
Loneliness Trajectories, Associated Factors and Subsequent Health in Children and Young People During the COVID-19 Pandemic: A National Matched Cohort Study
Schneider V, Norris T, Nugawela M, Dalrymple E, Hargreaves D, Käll A, McOwat K, Shafran R, Stephenson T, Xu L, Pinto Pereira SM
Psychology Research and Behavior Management 2023, 16:4461-4477
Published Date: 1 November 2023
Anxiety and Depression in Family Members of Critically Ill Covid-19 Inpatients: Brief Psychological Interventions via Telephone, an Exploratory Study
Caballero-Suárez NP, Barrientos-Casarrubias V, Gutiérrez-Velilla E, González Avilés LM, Pérez-López LD, Alvarado-De la Barrera C, Ávila-Ríos S, Mora-Gallegos J
Journal of Multidisciplinary Healthcare 2023, 16:3319-3331
Published Date: 7 November 2023
University Students’ Financial Situation During COVID-19 and Anxiety and Depressive Symptoms: Results of the COVID-19 German Student Well-Being Study (C19 GSWS)
Negash S, Horn J, Heumann E, Stock C, Zeeb H, Pischke CR, Matos Fialho PM, Helmer SM, Niephaus Y, Mikolajczyk R
Psychology Research and Behavior Management 2024, 17:2271-2285
Published Date: 4 June 2024
The Effects of Home Quarantine Duration, Parental Emotional Intelligence, and Family Socioeconomic Status on Children’s Anxiety During the Pandemic: A Survey of 29,550 Parents
Xiang J, Wu J, Lian C, Lin X
Psychology Research and Behavior Management 2025, 18:953-964
Published Date: 16 April 2025