")
Back to Journals » International Journal of Women's Health » Volume 15
Factors Influencing the Antenatal Care Attendance of Pregnant Women During the First COVID-19 Wave Lockdown in Thailand
Authors Chalermpichai T, Subsomboon K, Kasak R, Pinitlertsakun O, Pangzup S
Received 27 February 2023
Accepted for publication 5 May 2023
Published 11 May 2023 Volume 2023:15 Pages 731—740
DOI https://doi.org/10.2147/IJWH.S409642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Thiwarphorn Chalermpichai, Kultida Subsomboon, Rungtip Kasak, Orrawan Pinitlertsakun, Saowaros Pangzup
Department of Obstetrics and Gynecological Nursing, Faculty of Nursing, Mahidol University, Bangkok, Thailand
Correspondence: Thiwarphorn Chalermpichai, 2 Faculty of Nursing, Mahidol University, Wang Lang Road, Bangkoknoi, Bangkok, 10700, Thailand, Tel +662-419-7466-80 Ext 1810, Fax +662-412-8415, Email [email protected]
Background: The coronavirus disease 2019 (COVID-19) outbreak impacted healthcare service management worldwide. Thailand had limited healthcare resources. During the pandemic, several medical supplies were in high demand and expensive. The Thai government needed to declare a lockdown to reduce the unnecessary use of medical supplies. Antenatal care (ANC) services have adapted to the outbreak situation. However, information about the potential impact of COVID-19 lockdown on pregnant women and the reduction of disease exposure risk in this population remains unclear. Thus, this study aimed to assess the percentage of ANC attendance and factors affecting the scheduled ANC attendance of pregnant women during the first COVID-19 wave lockdown in Thailand.
Methods: This retrospective cross-sectional study included Thai women who were pregnant between 1 March and 31 May 2020. An online survey was conducted among pregnant women who had first ever ANC attendance before 1 March 2020. A total of 266 completed responses were returned and analysed. Statistically, the sample size was representative of the population. The predictors of scheduled ANC attendance during the lockdown were identified through logistic regression analysis.
Results: Overall, 223 (83.8%) pregnant women had scheduled ANC attendance during the lockdown. The predictive factors of ANC attendance were non-relocation (adjusted odds ratio [AOR] = 2.91, 95% confidence interval [CI]: 1.009– 8.381) and access to health services (AOR = 2.234, 95% CI: 1.125– 4.436).
Conclusion: During the lockdown, ANC attendance slightly declined, and the extended duration of each ANC or reduced face-to-face interactions with healthcare professionals. For pregnant women with non-relocation, healthcare providers must provide opportunities to contact them directly if they had doubts. The limited number of pregnant women who access health services allowed the clinic to be less crowded and therefore easy to ANC attendance.
Keywords: access care, ANC, COVID-19, pandemic, pregnant women, Thailand
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has affected numerous countries worldwide, including Thailand. In Thailand, the pandemic started on December 2019, when a Chinese woman travelling from China was found to be infected with the disease. This case was the first to be detected outside the Chinese territory.1 Cumulative cases of COVID-19 have rapidly increased and spread out in many provinces. Currently, the country is on the third COVID-19 wave. By 5 March 2022, the statistics of the Centre for Disease Control reported that COVID-19 had affected 781,379 people.2 In this study, data collection began during the early stages of the pandemic (lockdown) wherein the health service provisions, such as emergency–chronic outpatient services and antenatal care (ANC), were not yet modified to provide care systematically. In 2019, the total number of Thai pregnant women was around 670,000.3 Based on the statistics from the World Bank, the rate of pregnant women receiving prenatal care tended to increase slightly since 2013 and 2019 with percentages being 98.1 and 98.6, respectively.4 Thai ANC guidelines recommend pregnant women attending ANC before 12 gestational ages. In 2nd to 3rd trimester of gestation, obstetricians should schedule ANC at 20, 26, 30, 34, 36, 38 and 40 weeks.5 Pregnant women will receive the following benefits: ultrasounds, toxoids, medical care screenings (ABO typing, thalassemia, Down’s syndrome and sexually transmitted disease), vitamin supplements, mental health and dental care and health education programmes (nutrition, exercise, sexual intercourse, fetal movement counting and breastfeeding).5
During the lockdown, the government announced that Thai people should stay at home or work from home. COVID-19 has affected the normal lifestyle of all people. For example, temporary cessation of various business sectors leads to income loss (ie daily wage, overtime), relocation back to their hometown and travel restriction within and outside the province.6 Regarding the effects on the health service system, the number of outpatient/inpatient department healthcare service users decreased, and the time for scheduled follow-up/ANC attendance was extended unless they had any urgent health problems. Some hospitals have changed healthcare services from a face-to-face setting to telemedicine or online consultation via mobile applications and delivered drugs by post.7,8 In ANC, pregnant women who sought for ANC visit for the first time could not walk in and might receive such care late. Meanwhile, the schedule for continued ANC attendance was extended or postponed further to reduce congestion in the clinic.8,9 Many routine services, such as antenatal educational programmes and after-hour clinics, were also cancelled. Moreover, the limited number of healthcare providers who would replace the team infected with COVID-19 might not be relevant to certain healthcare users, resulting in inconvenient service provision and increased waiting time. High-capacity hospitals also provided web-based health education for pregnant women for self-study and communication with healthcare providers.7 However, the availability of such services may vary from place to place. Having regular ANC services for pregnant women is essential because it allows these women and their unborn infants to receive timely health care and be evaluated in terms of risks, referred to suitable institutions and planned for appropriate health care according to each trimester. An infant who receives proper gestational care will most likely have good health.8,10
Based on the ANC arrangement mentioned above to prevent COVID-19 outbreak in pregnant women, the restrictions might affect ANC attendance in other trimesters, consistent with the studies conducted by Dynes et al11 and Luginaah et al.12 These previous studies reported that ANC and postnatal care attendance declined during the Ebola virus outbreak because pregnant women generally did not trust the physicians or the healthcare workers, fearing of contracting the Ebola virus from these healthcare providers as mediators of transmission. During the lockdown period, the people had refrained from travelling outside their homes or across provinces, except when seeing physicians, buying essential needs, working for healthcare services and other important tasks. Unfortunately, the health service provisions were limited. Pregnant women should be monitored closely to screen, diagnose, manage and control the risk factors and to reduce adverse effects and complications during the delivery and postpartum periods. Hence, this study aimed to assess the percentage of ANC attendance and factors affecting the scheduled ANC attendance of pregnant women during the COVID-19 lockdown in Thailand between 1 March and 31 May 2020. The results of this study would serve as preliminary data on readiness management for ANC during emerging disease outbreaks.
Materials and Methods
Study Design and Population
This retrospective cross-sectional study included 266 women living in Thailand who were pregnant between 1 March and 31 May 2020. These women had their first ever ANC attendance before 1 March 2020. During data collection, several women might already have deliveries, but they ever had ANC attendance during the lockdown. They had learned the normal ANC process and lockdown also. The researchers publicised the project via internet platforms (Facebook, Line application) and leaflets by attaching inclusion and exclusion criteria, QR code, and a short URL of an electronic survey questionnaire. To increase access to the electronic questionnaire, four regions (North, Central, South and North-East) were randomised to find two healthcare settings per each region. The researchers coordinated with the eight hospital-staff to introduce themselves, give research information and send out project leaflets to them. The coordinating research staff recommended the project and distributed the leaflets to pregnant women in every clinic. The target group might live in beyond eight provinces because the researchers also publicised via internet platform.
Sample Size Determination and Sampling Technique
The sample size was calculated using G*Power. The proportion of ANC was based on previous research studying the vulnerability of attending ANC in Southern Sudan wherein mother’s literacy was significantly associated with non-use of ANC (adjusted odds ratio [AOR] = 1.79; 95% confidence interval [CI]: 1.31–2.45, p = 0.001).13 Moreover, the significance criterion was 0.05 with a power of 80%, and the sample size was at least 266 cases. The inclusion criteria were as follows: 1) aged 18 years or more, 2) could read and write the Thai language, 3) had communication devices and could use an online platform, 4) attended the first ANC service in Thailand before 1 March 2020. An exclusion criterion was pregnant women did not live in Thailand from 1 March to 31 May 2020.
Study Tool
The survey questionnaire was designed using Google Forms, consisting of four parts as follows:
Part 1 Respondents’ personal data including age, education level, marital status, occupation, income, province of residence, relocation, planned pregnancy, parity, pregnancy-related complications, travel and scheduled ANC attendance were collected.
Part 2 Knowledge, Attitudes, and Practices (KAP) towards COVID-19 questionnaire, which was developed by Zhong, Luo, Li, Zhang, Liu, Li and Li14 was used. Experts edited this questionnaire to investigate the equivalence of meaning between the English and Thai languages. This questionnaire has 14 items. Knowledge about COVID-19 is composed of three domains: Symptomatic and Symptom (4 items), Disease Transmission (3 items) and Prevention and Control (5 items). The attitudes towards COVID-19 have 2 items. Each item can be answered with either true, false, or unknown. A correct answer corresponds to 1 point, and an incorrect/unknown answer is 0 points. The scores range between 0 and 14 points, with higher scores indicating better knowledge of COVID-19. The Cronbach’s alpha coefficient of the questionnaire was acceptable both in China (α=0.71)14 and Paraguay (α=0.8)15 In this study, the Kuder–Richardson 20 (KR-20) test score was 0.64, consistent with that in Malaysia (α = 0.65).16
Part 3 Access to health services was measured using 22-questions developed by Manowwhan, Yusamran and Thananowan.17 These questions were based on the conceptual framework of Penchansky and Thomas18 and have subjective ratings of sufficiency (3 items), convenience (6 items), accessibility (3 items), acceptability (7 items) and healthcare and ANC use (3 items). Each item is rated on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). The total scores ranged from 22 to 88; the higher the score, the higher the level of access to health services. Cronbach’s alpha in this study was 0.86.
Part 4 Social support was measured using the 25-item Personal Resource Questionnaire, which was developed by Brandt and Weinert19 and translated in Thai by Choowattanapakorn.20 Each item is rated on a 7-point Likert scale and has both positive and negative questions. For positive items, the rating scores ranged from 1 (strongly disagree) to 7 (strongly agree), whereas for negative items, the scores ranged from 1 (strongly agree) to 7 (strongly disagree). The total scores ranged from 25 to 175, with a higher score indicating a higher level of social support. In this study, Cronbach’s alpha was 0.91.
Study Variables and Operational
Definition
The dependent variable was scheduled ANC attendance. Independent variables included age, education level, intended pregnancy, family income, relocation, transportation, risk level of the province of residence, KAP towards COVID-19, access to health services, social support, parity and pregnancy-related complications. Scheduled ANC attendance was defined as the on-time health check-up of pregnant women and their fetuses every ANC appointment or within a week before and after the appointed date from 1 March to 31 May 2020. Failure to follow this condition indicated non-ANC attendance.
Ethical Consideration
The institutional review board of the Faculty of Nursing in Mahidol University reviewed this study and waived the attainment of written informed consent (Protocol No. IRB-NS2020/37.0610). This study conformed to the Declaration of Helsinki. A QR code linked to an electronic survey questionnaire was forwarded to several social network platforms. Moreover, the dean of the Faculty of Nursing sent official letters to the medical directors, requesting to allow the coordinating research nurses to distribute leaflets with the QR code. A participant information sheet was attached to the first page of the electronic questionnaire. Selecting “Agree to participate in the study” and completing the questionnaires indicated women’s willingness to participate. Participants’ information was kept confidential to maintain anonymity. To express gratitude, the researchers sent souvenirs to the participants who were willing to leave their addresses.
Data Collection
Data were collected online from 1 December 2020 to 31 March 2021. The participants agreed to participate in the study that could scan QR code or access via short URL. The researchers attached the participant information sheet to describe in detail project on the first page of the questionnaire (Google form). If samples disagreed to participate, they could leave that page suddenly. Each participant completed the questionnaires for approximately 20–30 min. After the participants submitted their answers, the researchers monitored answer sheets by themselves everyday and deleted participants’ answers beyond the inclusion criteria until completely 266 participants. The researchers screened participants according to inclusion and exclusion criteria with two important questions from the electronic answer sheet; 1) “When did you attend the first ANC?” (dd/mm/yy) 2) which provinces did you live in between 1 March and 31 May 2020?
Data Management and Analysis
Data were analysed using descriptive statistics and logistic regression. Descriptive statistics, including frequencies, percentages, means and standard deviation (SD), were used to describe participants’ demographic data. Before logistic regression, the data of ordinal and nominal variables (age, education level, intended pregnancy, family income, relocation, transportation, risk level in the province of residence, parity, pregnancy-related complication and scheduled ANC attendance) were coded and categorised into two groups. The statistical level of significance was 0.05. Twelve factors potential influencing scheduled ANC attendance were examined by univariate logistic regression analyses. Variables with a p-value < 0.05 from the univariate analysis were chosen for the multivariable logistic regression analysis using the forward selection (likelihood ratio) method. In this analysis, the odds ratio and 95% confidence interval (95% CI) were estimated to determine the best predictors for scheduled ANC attendance among the participants.
Results
Sociodemographic Characteristics of the Respondents
The sample was composed of 266 pregnant women or postpartum mothers ageing between 18 and 44 years, with a mean age of 28.01 years (SD = 6.04). One-half of the respondents aged 25–34 years. In terms of educational status, approximately 29.7% graduated with a bachelor’s degree or higher, and 28.6% completed senior high school. Most of them were married (91.4%) and had health coverage such as universal coverage, social security scheme and civil servant medical benefit scheme (90.6%). In addition, more than one-fourth of the mothers were housewives, followed by an office staff in private companies (21.1%). Additionally, approximately 52% had a family income above 15,000 baht (1 USD = 35 baht) with average income of 27,824.01 baht (SD = 34,687.18), and majority (72.6%) claimed to have adequate income (Table 1).
 |
Table 1 Sociodemographic Characteristics of Pregnant Women During Lockdown (N = 266) |
Parametric and nonparametric continuous data are presented as mean and SD. The mean age of the ANC attendance group was slightly higher than that of the non-ANC attendance group (28.2 vs 27.1 years). Two variables, namely, access to health services and social support, were likely included, and their mean scores were higher in the ANC attendance group than in the non-ANC attendance group (70.0 vs 66.3 and 133.7 vs 128.9, respectively). The ANC attendance group also had higher family income (945 vs 835 USD). Meanwhile, the mean KAP-COVID-19 scores were equal between these two groups (score = 1.2) (Table 2).
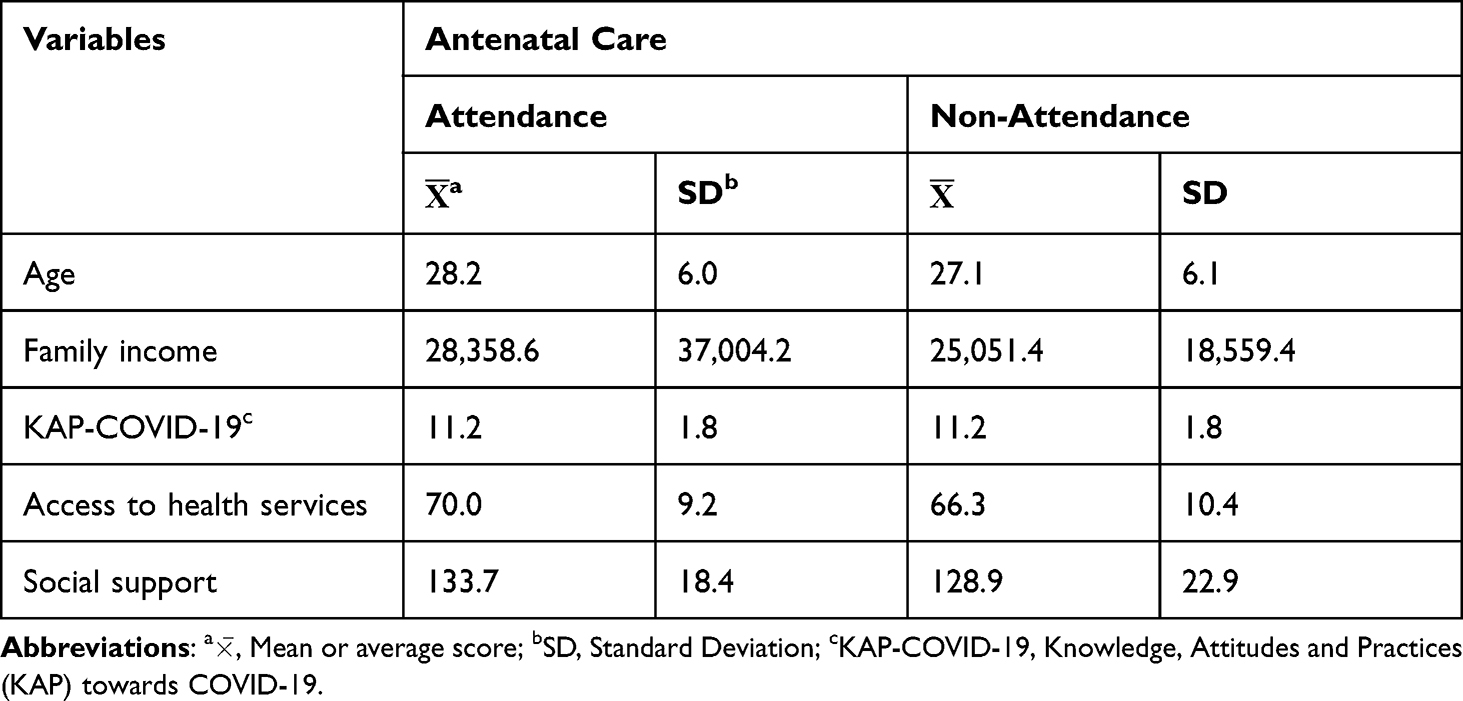 |
Table 2 Mean and Standard Deviation of the Continuous Variables (N = 266) |
ANC During Lockdown
During the COVID-19 lockdown in Thailand, most pregnant women (83.8%) attended their ANC appointment on time, whereas the remaining 16.1% had no ANC schedule or were late in their ANC appointment for more than a week.
According to the univariate and multivariate logistic regression analyses, both relocation and access to health service were major predictors of ANC attendance during the lockdown. Univariate logistic regression analyses revealed that the factors non-relocation and access to health service were significantly associated with ANC attendance. After controlling for the effect of other variables, the multivariate analysis results also showed that pregnant women who did not relocate were 2.91 times more likely to attend ANC than those who relocated (AOR = 2.91, 95% CI: 1.01–8.38). In addition, pregnant women who had higher scores of access to health services were 2.23 times more likely to attend ANC than those with low scores (AOR = 2.23, 95% CI: 1.12–4.44) (Table 3).
 |
Table 3 Univariate and Multivariate Logistic Regression Analyses of Factors Influencing Pregnant Women’s Antenatal Care Attendance During the COVID-19 Lockdown in Thailand (N = 266) |
Discussion
During the lockdown period, the statistics of ANC attendance tended to decrease compared with that in the early COVID pandemic. In 2019, the World Bank reported that 98.6% of Thai pregnant women received ANC.4 Therefore, most mothers (83.8%) attended scheduled ANC during the first wave of the pandemic. In fact, this percentage was higher than those in Ethiopia (29.3%),9 Kenya (47%),21 Jordan (40.5%)22 and the United States.23 ANC appointments were cancelled or rescheduled for several reasons, both healthcare system and individual issues. For example, the Kenya’s health service system already did not accept patients because of being too busy or unable to afford care until being closed as a result of COVID-19.21 In India, the Indian Council for Medical Research guidelines recommend healthcare providers to minimise ANC appointments at least four times (12, 20, 28 and 36 weeks of gestation), except for complicated pregnancy, to reduce the risk of COVID-19 exposure.24 In the individual aspect, the overwhelming COVID-19 mortality rates had affected people’s attitudes towards COVID-19, which is the most formidable disease to date.25 Pregnant women were scared to contract COVID-19 when going to a hospital or health facility. In addition, the COVID-19 pandemic resulted in face mask shortage and curfew implementation, which were both barriers to ANC attendance.21,26 In the first COVID-19 wave in Thailand, the rate of COVID-19 infection was relatively low (200 COVID-19 cases per day nationwide or 3081 cumulative COVID-19 cases until 31 May 2020).27 The percentage of ANC attendance in pregnant women was rather high, although the government announced a lockdown to limit the spread of infection and to prevent health care system collapse. During this time, the demand for medical products, especially personal protective equipment (PPE), dramatically increased, while the supply chain was disrupted worldwide.28 Meanwhile, the government and the Ministry of Public Health planned to provide adequately PPE (masks, gowns and gloves), inpatient beds, drugs and working plans for a limited health workforce.29 These transitions also affected the maternal-child healthcare service system. In the health service management at the clinic or hospital level, obstetric physicians or midwives assessed each pregnant woman to tailor the appropriate schedule for low- and high-risk ANC attendance. Several health education programmes, such as those about nutrition, exercise or physical activity and breastfeeding, took place through telehealth service or an online mode during ANC attendance. Each pregnant woman accessed other video clips via the QR code to learn by themselves at home, consistent with the studies conducted in Jordan22 and the US.23 However, some new pregnant Thai women experienced difficulties in commencing the ANC system because many clinics were limiting the number of new ANC attendees each day, especially private or after-hour clinics. Similarly, pregnant women in Kenya had higher odds of delayed ANC initiation. Most of them initiated ANC already in the second trimester.21 In addition, some scheduled ANC appointments from after-hour clinics were cancelled, and pregnant women had to contact the clinic by themselves. However, they did not know “How to start”?; Consequently, they did not attend ANC until delivery. Therefore, these pregnant women did not receive the quantity and completeness of ANC services that they deserved.30 In East Africa, maternal health workers reported low numbers of women attending maternal health clinics, and more women went to the hospital late without sufficient ANC.31 The responses to the pandemic greatly varied, although all have led to a maternity service provision being adapted to the individuals’ circumstances and the country’s concern.
Factors related to ANC attendance of pregnant women during the COVID-19 pandemic were non-relocation and access to health services. Those who did not relocate were 2.91 times more likely to have ANC attendance based on the scheduled appointment than those who relocated. In this study, pregnant women had domiciles in rural provinces, but they also had permanent residences in the area where the ANC clinic was located. Given that they did not return to their homeland during the lockdown, they could still travel back and forth for ANC attendance by means of private vehicles of husbands or relatives; travelling by public transportation was suspended during this time. These results are in line with those in Indonesia30 and Ethiopia.32 However, some women were more likely to return to their domiciles prior to the formal lockdown announcement of the government. Moreover, some pregnant women and their partners who worked as labourers in construction areas or industrial plants had experienced a change in employment status or dismissal. During the first nationwide lockdown, they needed to relocate back to their domiciles, where the cost of living is low, to reduce financial hardship.33 Nonetheless, these pregnant women still returned to the same hospital for their scheduled ANC attendance.
Regarding access to health services, pregnant women with high accessibility scores were 2.23 times more likely to attend ANC than those with low accessibility scores. During Thailand’s first COVID-19 wave, effective screening led to the spread of infection in a limited area; thus, the supply and demand of maternity care provisions, such as vitamins, supplements, medicines, essential equipment and out- and inpatient utilisation, were not affected. Most health facilities could provide maternity care similar to the pre-pandemic period. Only limited medical personnel or equipment had been allocated to prepare the healthcare system for people infected with COVID-19. In terms of the cost of care, Thai pregnant women received reimbursement from universal health coverage or social security welfare for ANC attendance. Moreover, although some pregnant women lived outside the city or country, they still had access to ANC by taking cheap suburban public train services or private transportation with relatives’ or partner’s support. Thus, they still received convenient services. Conversely, in Ireland, pregnant women were dissatisfied with maternity service modifications, which were necessary to reduce the risk of viral transmission. One of the modifications was the limited face-to-face interactions with healthcare professionals, thereby having fewer ANC appointments. In addition, pregnant women were dissatisfied with the waiting time during antenatal visits.10 In India, public transport was shut down. Hence, pregnant women had to take ambulances that were used to transport COVID-positive patients. These women were afraid of being exposed to the coronavirus when attending ANC.25 Some pregnant women could not also attend any ANC check-ups because of the lack of available physicians. Additionally, some could not access routine ANC because many health workers did not have enough time and vitamins or supplements were insufficient.25
Conclusion and Recommendation
Non-relocation and access to health services influenced ANC attendance during the first wave of COVID-19. Considering the exponential increase of COVID-19 cases and the likelihood of insufficiency in medical resources, the Thai government launched an early lockdown policy to prevent the further spread of viral transmission. Non-relocation reduced the risk of exposure to COVID-19. In addition, pregnant women were naturally afraid of travelling long distances because they were concerned that their fetuses might be affected. Hence, they often chose to live near the hospital or in areas where they could easily travel to the hospital, thereby easy to utilise ANC. Access to health services was rather flexible. Pregnant women were given priority to access health care whenever they had abnormal symptoms. Health coverage of several pregnant women was also reimbursed. In addition, digital health education was used to increase self-care, and telehealth was used to monitor their pregnancy status. However, using digital health programme limits pregnant women’s face-to-face interactions with healthcare professionals. Pregnant women’s cognition or experience of self-learning during pregnancy should also be assessed because they might not understand some contents in health education media. If they have questions, providing channels for direct contact with the healthcare professionals is essential. Moreover, data reflection of pregnant women will be useful for learning and developing practical guidelines for caring whenever a new outbreak or an emerging disease arises.
Modified ANC services offered by clinics or hospitals as a response to the COVID-19 pandemic might be a small component of the healthcare system, but it helped Thailand occupy the fifth position of the Global Health Security index ranking. Thailand is the only non–high-income country that was able to keep such a position among the top 10 countries.34
Limitations
This study conducted an online survey; therefore, some women might have limited access to the survey questionnaires.
Ethical Approval
This research received Exemption from Faculty of Nursing Mahidol University Institutional Review Board project no. IRB-NS2020/37.0610.
Acknowledgments
The authors would like to thank all research coordinators as QR code leaflet distribution Ms. Kanchana Jampathip, Ms. Uraiwan Limbutr, Mr. Weerapong Kumnimit, Ms. Kanittha Pattharasethaseranee, Ms. Nongluck Worarakthananun, Ms. Ratree Ritthirat, Ms. Saowaros Pangzup, and Ms. Hathaitip Kwanreong. The authors acknowledge the institutional support and facilities provided by the Faculty of Nursing, Mahidol University for conducting and editing this paper.
Funding
The study was funded by the China Medical Board of New York, Inc., Faculty of Nursing, Mahidol University. The funders were not involved in the study design, data collection, analysis or manuscript writing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Issac A, Radhakrishnan RV, Vijay VR, et al. An examination of Thailand’s health care system and strategies during the management of the COVID-19 pandemic. J Glob Health. 2021;11:03002. doi:10.7189/jogh.11.03002
2. Department of Disease Control. Covid-19 dashboard; 2022. Available from: https://ddc.moph.go.th/covid19-dashboard/.
3. National Statistical Office. Demography population and housing statistics; 2023. Available from: http://statbbi.nso.go.th/staticreport/page/sector/en/01.aspx.
4. The World Bank. Pregnant women receiving prenatal care - Thailand. World Bank Group. Available from: https://data.worldbank.org/indicator/SH.STA.ANVC.ZS?locations=TH.
5. Tangwiwat P. Antenatal care services in each trimester of gestation. In: Khemthong J, Limjamroon W, Thonglor T, Rhukauy P, editors. Antenatal Care Guidelines for Health Workers. Bureau of Health Promotion, Department of Health, Ministry of Health; 2022.
6. Biroli P, Bosworth S, Della Giusta M, Di Girolamo A, Jaworska S, Vollen J. Family life in lockdown. Front Psychol. 2021;12:687570. doi:10.3389/fpsyg.2021.687570
7. Thongwon T, Lumpo W, Saenthaweesuk A, et al. Challenging role of nurse-midwives during the pandemic of the Coronavirus 2019. Nurs J CMU. 2022;49(4):383–402.
8. Kansukcharearn A, Charornsuk W. Providing antenatal services under the circumstances of the epidemic of Covid-19, Hua Hin Hospital. Hua Hin Sook Jai Klai Kangwon J. 2020;5(1):1–11.
9. Esegbona-Adeigbe S. Impact of COVID-19 on antenatal care provision. Eur J Midwifery. 2020;4. doi:10.18332/ejm/121096
10. Meaney S, Leitao S, Olander EK, Pope J, Matvienko-Sikar K. The impact of COVID-19 on pregnant womens’ experiences and perceptions of antenatal maternity care, social support, and stress-reduction strategies. Women Birth. 2022;35(3):307–316. doi:10.1016/j.wombi.2021.04.013
11. Dynes MM, Miller L, Sam T, Vandi MA, Tomczyk B. Perceptions of the risk for Ebola and health facility use among health workers and pregnant and lactating women — Kenema district, Sierra Leone, September 2014. MMWR. 2015;63(51):1226–1227.
12. Luginaah IN, Kangmennaang J, Fallah M, Dahn B, Kateh F, Nyenswah T. Timing and utilization of antenatal care services in Liberia: understanding the pre-Ebola epidemic context. Soc Sci Med. 2016;160:75–86. doi:10.1016/j.socscimed.2016.05.019
13. Mugo NS, Dibley MJ, Agho KE. Prevalence and risk factors for non-use of antenatal care visits: analysis of the 2010 South Sudan household survey. BMC Pregnancy Childbirth. 2015;15:1–13. doi:10.1186/s12884-015-0491-6
14. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
15. Rios-González CM. Knowledge, attitudes and practices towards COVID-19 in Paraguayans during outbreaks: a quick online survey; 2020. Available from: https://preprints.scielo.org/index.php/scielo/preprint/view/149/179.
16. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
17. Manowwhan B-N, Yusamran C, Thananowan N. Age, education, social support, migration, and access to health services predicting antenatal visits in postpartum mothers: retrospective study. J Phrapokklao Nurs Coll. 2016;27(2):1–15.
18. Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127–140. doi:10.1097/00005650-198102000-00001
19. Brandt PA, Weinert C. The PRQ-A social support measure. Nurs Res. 1981;30(5):277–280. doi:10.1097/00006199-198109000-00007
20. Choowattanapakorn T. The relationship between hope and adaptation in malignant of lymphohemopoietic patients. 1988.
21. Landrian A, Mboya J, Golub G, Moucheraud C, Kepha S, May S. Effects of the COVID-19 pandemic on antenatal care utilisation in Kenya: a cross-sectional study. BMJ Open. 2022;12(4):e060185. doi:10.1136/bmjopen-2021-060185
22. Muhaidat N, Fram K, Thekrallah F, Qatawneh A, Al-Btoush A. Pregnancy during COVID-19 outbreak: the impact of lockdown in a middle-income country on antenatal healthcare and wellbeing. Int J Women's Health. 2020;12:1065–1073. doi:10.2147/IJWH.S280342
23. Preis H, Mahaffey B, Heiselman C, Lobel M. Vulnerability and resilience to pandemic-related stress among U.S. women pregnant at the start of the COVID-19 pandemic. Soc Sci Med. 2020;266:113348. doi:10.1016/j.socscimed.2020.113348
24. National Institute for Research in Reproductive Health. Guidance for management of pregnant women in COVID-19 pandemic ICMR. Available from: https://www.icmr.gov.in/pdf/covid/techdoc/Guidance_for_Management_of_Pregnant_Women_in_COVID19_Pandemic_12042020.pdf.
25. Bankar S, Ghosh D. Accessing Antenatal Care (ANC) services during the COVID-19 first wave: insights into decision-making in rural India. Reprod Health. 2022;19(1):158. doi:10.1186/s12978-022-01446-2
26. Goyal M, Singh P, Singh K, Shekhar S, Agrawal N, Misra S. The effect of the COVID-19 pandemic on maternal health due to delay in seeking health care: experience from a tertiary center. Int J Gynecol Obstetr. 2021;152(2):231–235. doi:10.1002/ijgo.13457
27. Department of Health. Surveillance. Ministry of Public Health; 2021. Available from: http://dashboard.anamai.moph.go.th/surveillance/default/index?year=2020.
28. Morales-Contreras MF, Leporati M, Fratocchi L. The impact of COVID-19 on supply decision-makers: the case of personal protective equipment in Spanish hospitals. BMC Health Serv Res. 2021;21(1):1170. doi:10.1186/s12913-021-07202-9
29. Malathum K, Malathum P. The COVID-19 pandemic: what we have learned from Thai experiences. Pacific Rim Int J Nurs Res. 2020;24(4):431–435.
30. Ariani N. Antenatal care services utilization during COVID-19 second wave attack in Pasuruan, Indonesia. J Med Life. 2022;15(1):7–14. doi:10.25122/jml-2021-0238
31. Pallangyo E, Nakate MG, Maina R, Fleming V. The impact of covid-19 on midwives’ practice in Kenya, Uganda and Tanzania: a reflective account. Midwifery. 2020;89:102775. doi:10.1016/j.midw.2020.102775
32. Tadesse E. Antenatal care service utilization of pregnant women attending antenatal care in public hospitals during the COVID-19 pandemic period. Int J Women's Health. 2020;12:1181–1188. doi:10.2147/IJWH.S287534
33. Johnson L. Exploring factors associated with pregnant women’s experiences of material hardship during COVID-19: a cross-sectional Qualtrics survey in the United States. BMC Pregnancy Childbirth. 2021;21(1):755. doi:10.1186/s12884-021-04234-1
34. Global Health Security Index. Country ranking view of index results; 2022. Available from: https://www.ghsindex.org/#l-section--countryranksect.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.