Back to Journals » Journal of Inflammation Research » Volume 16
Prognostic Value of Body Composition and Systemic Inflammatory Markers in Patients with Locally Advanced Cervical Cancer Following Chemoradiotherapy
Authors Guo H, Feng S, Li Z, Yin Y, Lin X, Yuan L, Sheng X, Li D
Received 18 August 2023
Accepted for publication 31 October 2023
Published 10 November 2023 Volume 2023:16 Pages 5145—5156
DOI https://doi.org/10.2147/JIR.S435366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tara Strutt
Hui Guo,1 Shuai Feng,1 Zhiqiang Li,1 Yueju Yin,1 Xueying Lin,2 Lingqin Yuan,1 Xiugui Sheng,3 Dapeng Li1
1Department of Gynecologic Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 2Department of Surgery, Liaocheng Dongchangfu District Maternal and Child Health Hospital, Liaocheng, Shandong, People’s Republic of China; 3Department of Gynecologic Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Dapeng Li, Department of Gynecologic Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, No. 440, Jiyan Load, Jinan, Shandong, 250117, People’s Republic of China, Email [email protected]
Background: Abnormal changes in body composition and systemic inflammation response have been associated with poor survival of cancer patients. Our study was to explore the prognostic value of the association between body composition indicators and systemic inflammation markers among patients with locally advanced cervical cancer (LACC) who underwent concurrent chemoradiotherapy (CCRT).
Methods: We retrospectively reviewed medical records of LACC patients treated between 2016 and 2019. Subcutaneous, visceral and intra-muscular adipose index (SAI, VAI and IMAI) and skeletal muscle index (SMI) were derived from computed tomography (CT). Kaplan-Meier analysis and Univariate and multivariate Cox analyses were used to evaluate the survival. A nomogram was constructed to assess the prognostic value.
Results: The study included 196 patients treated with CCRT. According to multivariable Cox analyses, IIIC1r (P = 0.045), high systemic immune-inflammation index (SII) (P = 0.004), sarcopenia (P = 0.008), high SAI (P = 0.016) and high VAI (P = 0.001) were significantly risk factors for overall survival (OS). Kaplan-Meier analysis showed that patients with low lymphocyte-to-monocyte ratio (LMR) and sarcopenia had longer OS than those with high LMR and sarcopenia (P = 0.023). The high neutrophil-to-lymphocyte ratio (NLR) in non-sarcopenic patients showed better survival (P = 0.022). Low VAI (P = 0.019) or low IMAI (P = 0.019) combined with low SII had a favorable OS. Low LMR combined with low SAI was associated with longer OS (P = 0.022). The calibration plots of nomogram predicting the 3-year and 5-year OS rates were close to the ideal models.
Conclusion: Inflammation factors were closely associated with abnormal muscle and fat distribution. The combined prognostic value of body composition indicators and systemic inflammation markers was reliable in predicting survival for LACC patients.
Keywords: body composition, systemic inflammatory markers, cervical cancer, overall survival, nomogram
Introduction
Activation of the systemic inflammatory response is associated with tumorigenesis, progression, and metastasis.1 The systemic inflammatory state in cancer patients can be reflected by peripheral blood cells and inflammatory proteins. Increasing evidence suggested that systemic inflammatory biomarkers were valid predictors of prognosis in multiple cancers.2–5 Blood inflammation parameters such as neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR), neutrophil-to-platelet ratio (NPR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR) and index of systemic immune-inflammation (SII) have been associated with the prognosis of cervical cancer.6–8
Computed tomography (CT) - derived body composition measures have been widely studied as important prognostic markers in patients with cancer.9 Body composition metrics mainly include measurements of skeletal muscle and adipose tissue. Cancer patients routinely require CT examinations for baseline staging and assessment of treatment efficacy, which provides the convenience of obtaining body composition parameters. The cross-sectional areas of skeletal muscle and adipose tissue on a single CT slice at the third lumbar spine level have correlated with the total skeletal muscle and fat masses.10 Most previous studies on the prognosis of cervical cancer focused on tumour or treatment-related factors.11,12 However, the prognostic implications of body composition remain unclear in patients with cervical cancer.
Cervical cancer is the fourth most common cause of cancer incidence and mortality in women.13 Concurrent chemo-radiotherapy (CCRT) is the standard treatment for locally advanced cervical cancer (LACC). Although screening tests and treatment methods have advanced in recent years, cervical cancer related mortality remains high. Therefore, survival predictors must be identified to guide clinical treatment and improve prognosis. Both systemic inflammatory markers and body composition are associated with clinical outcomes in patients with cervical cancer.8,14,15 However, these indicators were analyzed separately in most studies. The association and joint prognostic predictive effect of body composition and systemic inflammation markers among LACC patients with CCRT have not been reported.
Therefore, this study intends to explore the association between body composition based on CT imaging and systemic inflammation and assess their prognostic values. Considering a nomogram model was widely used to predict cancer outcomes, we will further build a nomogram to evaluate their combined predictive effect.
Methods and Materials
Patient Selection
This retrospective study included 196 patients with cervical cancer between January 2016 and June 2019 at Shandong cancer hospital and Institute. We screened 231 patients with LACC who underwent CCRT from 2016 to 2019 in the electronic medical record. In these cases, 15 were excluded for unfinished radiotherapy, 6 for incomplete chemotherapy, 9 for having chronic diseases such as hematologic illness or autoimmune disease, and 5 for combining with other malignant tumours. Thus, we finally included 196 eligible patients with LACC.
The inclusion criteria were as follows: (1) diagnosed with cervical cancer through biopsy; (2) stage IIB to IIIC disease according to the 2018 International Federation of Gynecology and Obstetrics (FIGO) staging system; (3) treated with CCRT; (4) complete medical records and follow-up records; (5) available CT scans taken before treatment; (6) include controlled comorbidities. The exclusion criteria were as follows: (1) incomplete chemotherapy or radiotherapy; (2) combined with hematologic illness, autoimmune disease, acute or chronic infection, and other diseases that may impact hematologic indexes; (3) suffered from other malignant tumours. This study was approved by the Ethics Committee of Shandong cancer hospital and Institute. All patients routinely followed treatment: every three months during the first two years, every six months during the following three years and annually after that.
Treatment of Patients
All patients were treated with external beam radiation therapy (EBRT) and brachytherapy (BT). EBRT included intensity modulated radiation therapy (IMRT) or tomotherapy (TOMO), with prescription doses ranging from 45 to 50 Gy delivered in 25 to 28 fractions (5 fractions/week). All patients completed radiotherapy within 7–8 weeks. BT was performed at 25–30 Gy doses in 4 to 5 fractions (1 fraction/week) before the EBRT course was complete or in the last week of pelvic EBRT. Positive Lymph node regions were treated to a total dose of 50 to 60 Gy. All patients were treated with four cycles of concurrent chemotherapy during the radiation therapy. The chemotherapy regimens included paclitaxel (135 mg/m2) on day one and cisplatin (75 mg/m2) on day two every four weeks.
Measurement and Classification of Skeletal Muscle and Adipose Tissue
Before initial treatment, a single-enhanced CT image at the third lumbar vertebra was used to evaluate the cross-sectional area of skeletal muscle and adipose tissue. A senior radiologist was employed to correctly identify L3 level on CT, which both transverse processes were initially fully visualized.16 Two authors used SliceOmatic (version 5.0; TomoVision, Magog, Canada) to delineate and calculate skeletal muscle and adipose tissue area based on tissue-specific ranges measured in Hounsfield units (HU).17 The skeletal muscle area includes the psoas, paraspinal, transversus abdominis, rectus abdominis, and internal and external oblique muscles. Skeletal muscle was identified with a radiation density between −29 and +150 HU. Subcutaneous and intermuscular adipose tissue was divided from extra-muscular tissue with a radiation density between −190 and −30 HU. Visceral adipose tissue was calculated with a radiation density between −150 and −50 HU. The cross-sectional areas (cm2) of skeletal muscle, subcutaneous adipose, visceral adipose, and intra-muscular adipose tissue were normalized by dividing by height (m)2 (SMI, VAI, SAI, and IMAI, respectively). Sarcopenia was defined as SMI of < 41.0 cm2 /m2 according to the definition of Martin et al.18 Because there were no widely recognized cut-off values for SAI, VAI and IMAI, we set the optimal cut-off values by using X-tile software (Yale University, New Haven, CT, USA).19
Systemic Inflammatory Biomarkers
Baseline platelets, neutrophils, monocytes, lymphocytes and red blood cell distribution width (RDW) were obtained from the complete blood count within one week before treatment. NLR, NPR, PLR and LMR were then calculated. The prognostic nutritional index (PNI) was calculated as serum albumin (g/L) + 5 × lymphocyte count (109/L). The SII was calculated as the neutrophil count × platelet count/lymphocyte count (109/L). We set optimal cut-off points for the above laboratory parameters by X-tile software, which was used to divide the patients into two subgroups for further analysis.
Statistical Analysis
Overall survival (OS) was defined as the period from the date of diagnosis to the date of death. Characteristics of baseline data were presented with mean values, standard deviation (SD), and frequencies. The association between clinical factors and body composition were analyzed by binary logistic regression. The Kaplan-Meier method was applied to estimate the survival rates. The Log rank test was used to compare the differences between groups. Univariate and multivariate analyses were performed using the Cox proportional hazards model to identify the potential risk factors. A nomogram model was constructed to evaluate the combined prognostic predictive value. A two-sided P < 0.05 was defined as statistically significant. Statistical analysis was performed using SPSS version 22 and R version 4.2.1.
Result
Patients’ Characteristics
Among these patients, the average age was 52 years. The most histological type was squamous cell carcinoma. 17.9%, 42.3% and 39.8% of patients were diagnosed with 2018 FIGO stage IIB, IIIB and IIIC1r cervical cancer, respectively. Most patients had tumour size ≥ 4cm (81.1%) and tumour grade G3 (48%). The cut-off values of different body composition and inflammatory parameters were defined as follows by the X-tile software: LMR (4.04), NLR (2.38), NPR (0.014), PLR (178.61), RDW (10.83), PNI (54.34), SII (1377.37), SMI (41), VAI (91.77), SAI (34.89), and IMAI (5.85). Other baseline characteristics are shown in Table 1.
 |
Table 1 Basic Clinicopathologic Characteristics of Cervical Cancer |
Association Between Body Composition, Systemic Inflammatory Markers and Clinicopathologic Parameters
Univariate and multivariate logistic analysis showed that body mass index (BMI) was lower in sarcopenic patients (P < 0.05) (Table 2). High BMI was significantly associated with high SAI (P < 0.05), VAI (P < 0.05) and IMAI (P < 0.05) (Tables 3–5). Multivariate analysis showed that sarcopenia was associated with older age (OR = 3.49, 95% CI = 1.63–7.8, P = 0.002), advanced tumour size (OR = 2.46, 95% CI = 1.08–5.95, P = 0.038), and increased PLR (OR = 1.97, 95% CI = 1.04–3.79, P = 0.039) (Table 2).
 |
Table 2 Univariate and Multivariate Logistic Analysis Among Clinicopathologic Parameters, Systemic Inflammatory Markers, and Sarcopenia |
 |
Table 3 Univariate and Multivariate Logistic Analysis Among Clinicopathologic Parameters, Systemic Inflammatory Markers, and SAI |
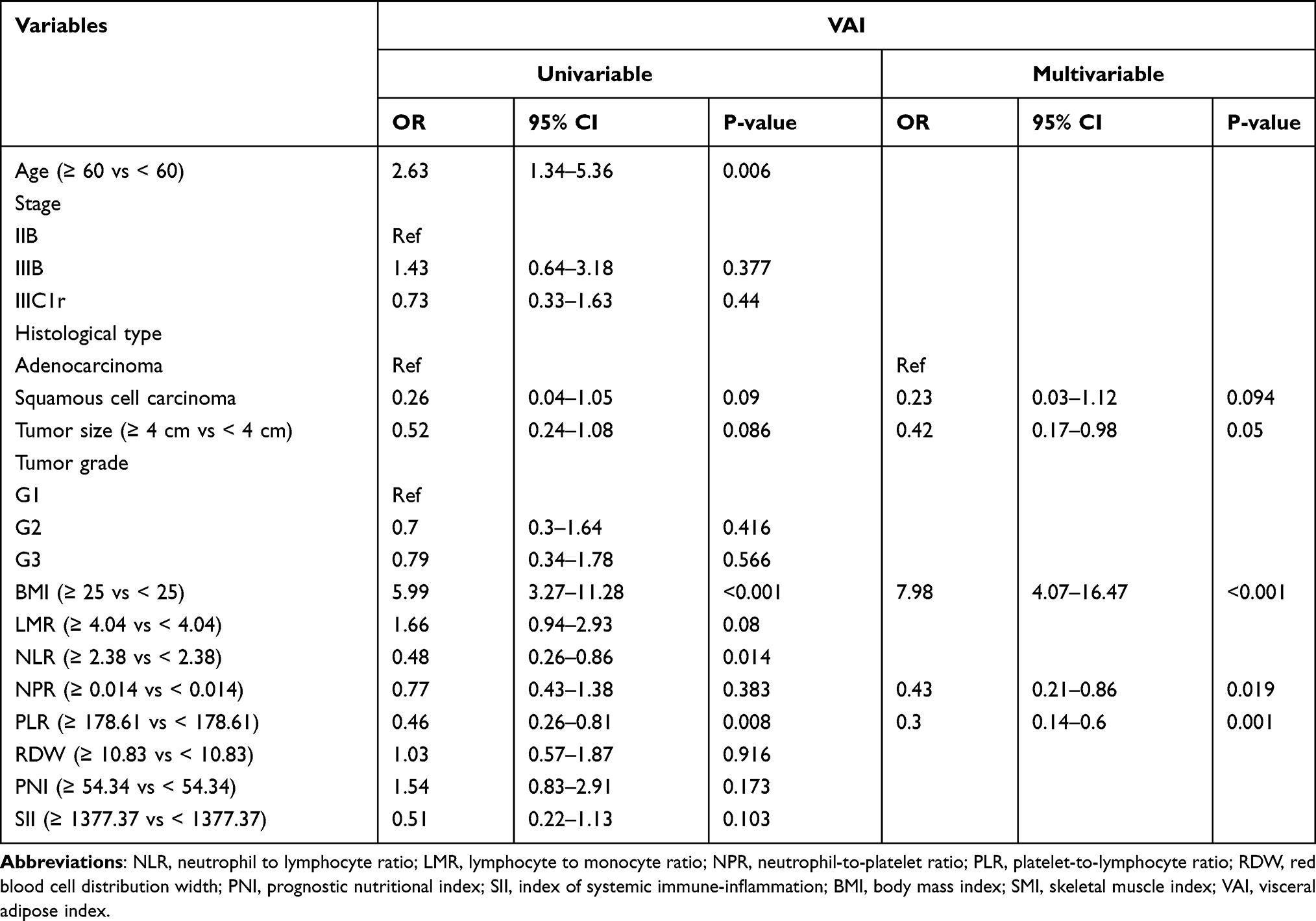 |
Table 4 Univariate and Multivariate Logistic Analysis Among Clinicopathologic Parameters, Systemic Inflammatory Markers, and VAI |
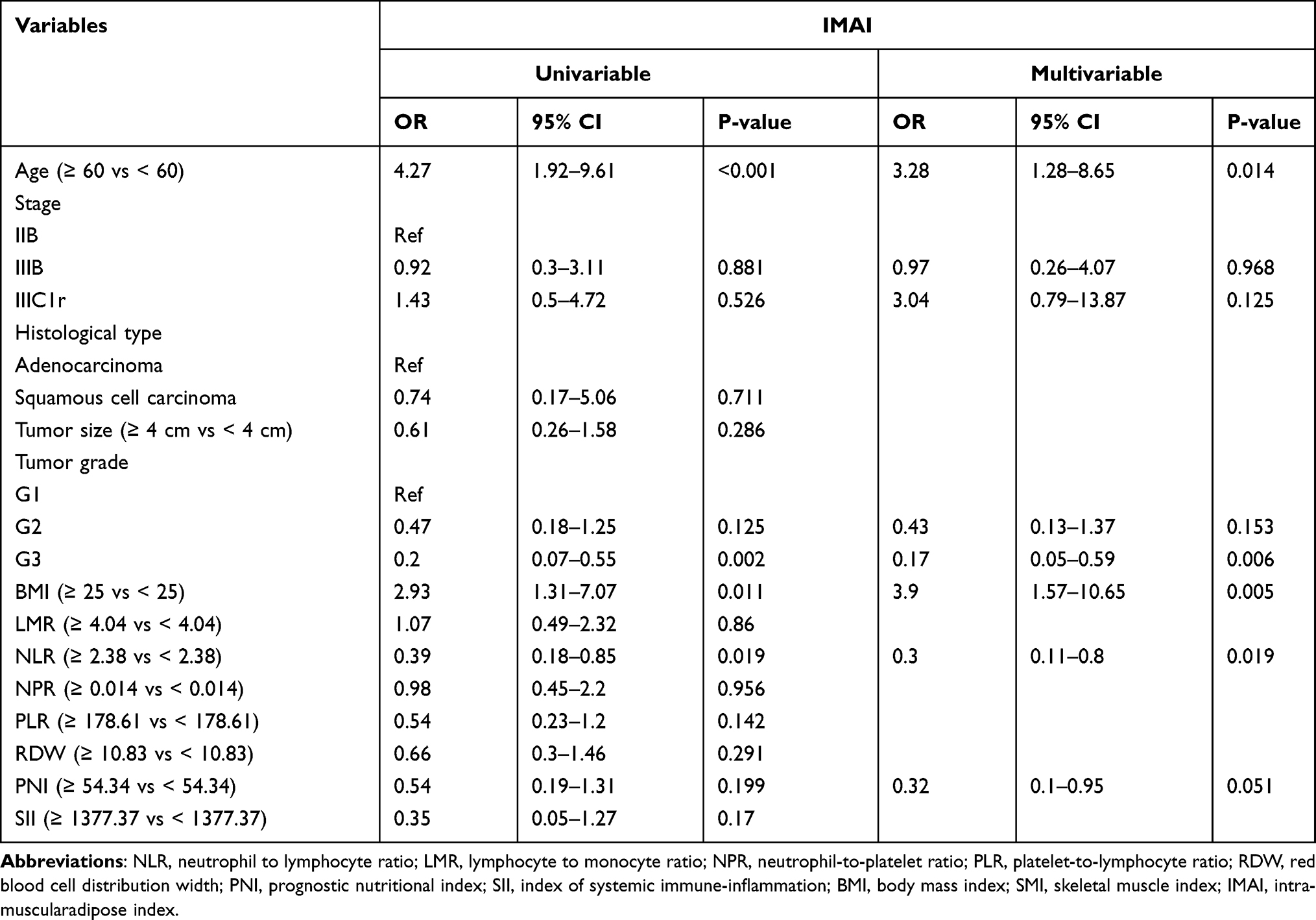 |
Table 5 Univariate and Multivariate Logistic Analysis Among Clinicopathologic Parameters, Systemic Inflammatory Markers, and IMAI |
Multivariate analysis showed that SAI was significantly lower in patients with high tumour size (OR = 0.27, 95% CI = 0.08–0.87, P = 0.028) and increased NPR (OR = 0.35, 95% CI = 0.13–0.91, P = 0.034) (Table 3). In univariate analysis, high VAI was associated with older age (OR = 2.63, 95% CI = 1.34–5.36, P = 0.006), NLR (OR = 0.48, 95% CI = 0.26–0.86, P = 0.014) and PLR (OR = 0.46, 95% CI = 0.26–0.81, P = 0.008) (Table 4). In multivariate analysis, high VAI was associated with NPR (OR = 0.43, 95% CI = 0.21–0.86, P = 0.019) and PLR (OR = 0.3, 95% CI = 0.14–0.6, P = 0.001) (Table 4). Univariate and multivariate logistic analysis showed that high IMAI was related to stage G3 (OR = 0.2, 95% CI = 0.07–0.55, P = 0.002; OR = 0.17, 95% CI=0.05–0.59, P = 0.006), age (OR = 4.27, 95% CI = 1.92–9.61, P < 0.001; OR = 3.28, 95% CI = 1.28–8.65, P = 0.014) and NLR (OR = 0.39, 95% CI = 0.18–0.85, P = 0.019; OR = 0.3, 95% CI = 0.11–0.8, P = 0.019) (Table 5).
Prognostic Impact of Body Composition and Inflammation Markers
Multivariable Cox analyses showed that IIIC1r (HR = 9.69; 95% CI = 1.05–89.22; P = 0.045), high SII (HR = 7.35; 95% CI = 1.88–28.66; P = 0.004), sarcopenia (HR = 3.6; 95% CI = 1.4–9.23; P = 0.008), high SAI (HR = 4.7; 95% CI = 1.33–16.66; P = 0.016) and high VAI (HR = 7.53; 95% CI = 2.27–25.01; P = 0.001) were significantly risk factors for OS (Table 6). However, the OS of patients with a high PNI (HR=0.24; 95% CI= 0.07–0.8; P = 0.02) and of those with a high BMI (HR = 0.23; 95% CI = 0.07–0.77; P = 0.017) were better than those of patients with a low PNI and those with a low BMI.
 |
Table 6 Univariable and Multivariable Cox Analyses Associated with Overall Survival |
To explore the prognostic impact of body composition combined with inflammation markers, we used Kaplan-Meier curves to display the differences between each group. The median follow-up duration was 5.4 years. Patients with low LMR and sarcopenia had longer OS than those with high LMR and sarcopenia (p = 0.023) (Figure 1A). High NLR in non-sarcopenic patients showed better survival (p = 0.022) (Figure 1B). Regarding fat indicators, low VAI (p = 0.019) (Figure 1C) or low IMAI (p = 0.019) (Figure 1D) combined with low SII had a favourable OS. Patients with low LMR and SAI were associated with longer OS (p = 0.022) (Figure 1E).
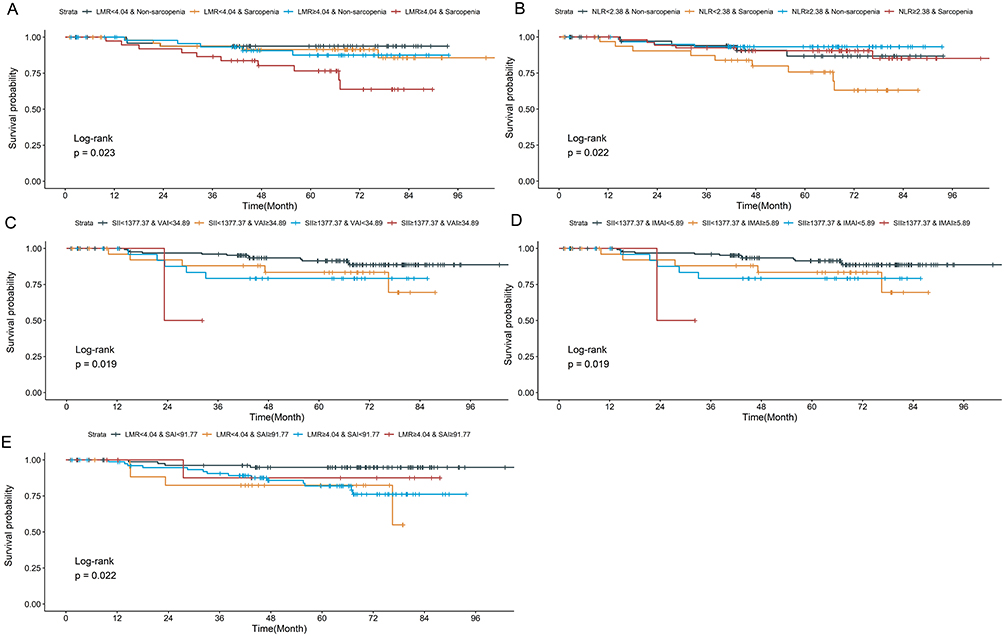 |
Figure 1 Kaplan-Meier plot of association between body composition combined with inflammation markers and OS. (A) LMR + Sarcopenia. (B) NLR + Sarcopenia. (C) SII + VAI. (D) SII + IMAI. (E) LMR + SAI. Abbreviations: OS, overall survive; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; SAI, skeletal muscle index; VAI, visceral adipose index; SII, systemic immune-inflammation index; IMAI, intra-muscular adipose index. |
Nomogram for Predicting Survival
The multivariable Cox analysis was utilized to define the significant prognostic markers. The nomogram was then constructed for OS prediction using these selected markers, including stage, BMI, NPR, PNI, SII, sarcopenia, SAI and VAI (Figure 2A). From the nomogram, a larger total point score indicated a shorter OS. The calibration plots predicting the 3-year and 5-year OS rates showed well with the ideal model (Figure 2B and C).
 |
Figure 2 Nomogram for predicting survival. (A) Nomogram to predict the 3-year and 5-year overall survival rates of LACC patients. Calibration plot of the nomogram for the (B) 3-year and (C) 5-year survival rates. |
Discussion
This study was the first to demonstrate that body composition indexes and inflammation markers had a combined effect on prognostic in LACC patients who underwent CCRT. Sarcopenia and body fat indicators (SAI, VAI and IMAI) presented an apparent association with various inflammation markers. Survival analysis demonstrated that high SII, sarcopenia, high SAI and high VAI were significant risk factors for OS. Furthermore, we developed a prognostic nomogram to predict survival including body composition and inflammation markers with favourable identification.
Excessive or persistent systemic inflammatory response, which was accurately reflected by ratios of blood parameters, played an important role in cancer progression.20 SII based on peripheral lymphocyte, neutrophil and platelet counts has been considered a better prognostic value in various cancers.4,21 Previous meta-analysis indicated that SII was not associated with statistically improved OS in cervical cancer.8 However, Huang et al confirmed that SII was effective in predicting the postoperative survival of patients with cervical cancer.6,22 Our results concluded that a high pre-treatment SII was significantly associated with increased OS for LACC. The PNI was applied to assess the nutritional status and immune balance, which obviously predicted the survival of LACC patients treated with CCRT.23,24 Our study demonstrated that high PNI was a positive prognostic factor for survival in patients with LACC. These results provided a significant association between SII, PNI and survival after chemo-radiation. In addition, it also implied that oncologists should carefully evaluate the nutritional status of LACC patients and provide high-quality care.
The complex body composition was not well distinguished by BMI alone. Accumulating studies have used other measures of body composition beyond BMI, such as bio-electrical impedance analysis (BIA), CT, and dual-energy X-ray absorptiometry (DXA) imaging. Our study used a single-enhanced CT image at the third lumbar vertebra to evaluate the cross-sectional area of skeletal muscle and adipose tissue. Multivariable Cox analyses presented that sarcopenia, high SAI and high VAI were significant risk factors for OS in LACC patients. These results are consistent with previous research findings in breast and colorectal Cancer.25,26 However, most studies chose different indicators and methods to assess the association between body composition and cancer. Thus, body composition may exhibit different outcomes in the same cancer. For example, when the cut-off value of SAI and VAI was 67.3 cm2 /m2 and 41.6 cm2 /m2, respectively, Lee et al found that the pre-treatment SAI and VAI of LACC patients were not associated with outcomes.14 Our study determined the cut-off points for body parameters by X-tile software, which presented effective cut-points for the assessment between markers and outcomes.19 Although there are many different outcomes, the importance of muscle and adiposity on cancer survival was not ignored.
Most studies have shown that body composition and systemic inflammatory response parameters were predictive factors for multiple cancers individually. However, the combined prognostic value was not common. A study of 223 patients with gastric cancer who underwent adjuvant chemo-radiotherapy after radical gastrectomy observed that sarcopenic obesity combined with systemic inflammation (PLR, PNR) had a more accurate prognosis than the model without systemic inflammation.27 The survival of sarcopenic patients with head and neck cancer was enhanced when PLR was high.28 In small-cell lung cancer treated with chemotherapy or chemo-radiotherapy, they showed that sarcopenia and high NLR were independently associated with shorter OS and progression free survival (PFS).29 Our study found that sarcopenia with low LMR in LACC was an available factor for longer OS. These clinical findings may be explained by the interaction between skeletal muscle and immune cells. The immune system plays an important role in the development of skeletal muscle. Lymphocytes, monocytes and other immune cells secrete cytokines and signalling factors such as IL-6 and TNF-α, which regulate skeletal muscle metabolism.30 A previous study indicated that skeletal muscle loss during CCRT was an independent poor prognostic factor for reduced OS.14 Thus, the decreased muscle mass may be connected with immune cells and poorer outcomes in cancer patients.
Excess adipose tissue was associated with low-grade chronic inflammation characterized by elevated levels of circulating inflammatory mediators known to promote tumour progression.31 Inflammatory markers, such as C-reactive protein (CRP), tumor necrosis factor-α (TNF-α) and IL-6, have been associated with the development and progression of tumours.32,33 However, the relationship between systemic hemato-immunological indices and body fat parameters in cancer patients has not been elucidated. For the first time, our study found that low LMR was associated with better survival in LACC patients with low SAI. In addition, low SII combined with low VAI was positive prognostic indicator for LACC patients. Currently, few researchers have examined the relationship between IMAI and survival. In our study, IMAI alone was not associated with OS, but low SII patients with low IMAI owned higher OS than those with high IMAI. Thus, the combination of inflammatory factors and adipose-related indicators can improve the efficacy of prognostic prediction for cancer patients.
Based on the above findings, we further investigated the predictive value of body composition combined systemic inflammation factors in evaluating the prognosis of LACC patients who underwent CCRT. We constructed a reliable nomogram model for predicting survival that combines body composition (sarcopenia, SAI and VAI) and systemic inflammation factors (NPR, PNI, SII). This model showed excellent accuracy in predicting the survival probability of LACC patients. Clinically, body composition and systemic inflammation factors were convenient and inexpensive to assess. CT-based body composition analyses and pretreatment blood inflammation factors would be beneficial to the improvement of individualized treatment strategies.
There were several limitations to our study. First, it was a single-centre retrospective observational study with a relatively small sample size. Therefore, it is necessary to further confirm in a prospective study with a larger sample size. Second, the present study failed to study the prognostic factors for PFS because data regarding PFS were not sufficient. However, this study was the first time to explore the associations among body composition conditions, systemic inflammatory markers, and OS in patients with cervical cancer who underwent CCRT.
Conclusion
In conclusion, we have demonstrated that poor body composition (sarcopenia, high SAI and VAI) measured by CT scans was associated with the survival of LACC patients who underwent CCRT. Inflammation factors were closely associated with abnormal muscle and fat distribution. The prognostic nomogram model developed from the combination of body composition and systemic inflammatory markers provided a reliable prediction method. The results presented in this study were helpful to risk stratification for patients who are beginning treatment and guide clinical treatment strategy. Future studies are needed to further elucidate the biological relationship between body composition and inflammation in patients with cancer.
Ethics Approval and Informed Consent
This study was approved by the Medical Ethics Committee Shandong Cancer Hospital and Institute (SDTHEC2023007018). It complied with the Declaration of Helsinki. This study was a retrospective study, which there is no any danger to patients and informed consent cannot be obtained from patients. With the approval of the ethics committee, it is agreed to exempt patients from informed consent forms.
Funding
This work was supported by the National Natural Science Foundation of China (No.81672591).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elinav E, Nowarski R, Thaiss CA, et al. Inflammation-induced cancer: crosstalk between tumours, immune cells and microorganisms. Nat Rev Cancer. 2013;13(11):759–771. doi:10.1038/nrc3611
2. Xie H, Ruan G, Ge Y, et al. Inflammatory burden as a prognostic biomarker for cancer. Clin Nutr. 2022;41(6):1236–1243. doi:10.1016/j.clnu.2022.04.019
3. Yamamoto T, Kawada K, Obama K. Inflammation-related biomarkers for the prediction of prognosis in colorectal cancer patients. Int J Mol Sci. 2021;22(15):8002. doi:10.3390/ijms22158002
4. Meng L, Yang Y, Hu X, et al. Prognostic value of the pretreatment systemic immune-inflammation index in patients with prostate cancer: a systematic review and meta-analysis. J Transl Med. 2023;21(1):79. doi:10.1186/s12967-023-03924-y
5. Dinca A-L, Diaconu A, Birla RD, et al. Systemic inflammation factors as survival prognosis markers in ovarian neoplasm and the relationship with cancer-associated inflammatory mediators—a review. Int J Immunopathol Pharmacol. 2023;37:3946320231178769. doi:10.1177/03946320231178769
6. Huang H, Liu Q, Zhu L, et al. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci Rep. 2019;9(1):3284. doi:10.1038/s41598-019-39150-0
7. Holub K, Biete A. Impact of systemic inflammation biomarkers on the survival outcomes of cervical cancer patients. Clin Transl Oncol. 2018;21(7):836–844. doi:10.1007/s12094-018-1991-4
8. Han X, Liu S, Yang G, et al. Prognostic value of systemic hemato-immunological indices in uterine cervical cancer: a systemic review, meta-analysis, and meta-regression of observational studies. Gynecol Oncol. 2021;160(1):351–360. doi:10.1016/j.ygyno.2020.10.011
9. Bates DDB, Pickhardt PJ. CT-derived body composition assessment as a prognostic tool in oncologic patients: from opportunistic research to artificial intelligence–based clinical implementation. Am J Roentgenol. 2022;219(4):671–680. doi:10.2214/ajr.22.27749
10. Mourtzakis M, Prado CMM, Lieffers JR, et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metabol. 2008;33(5):997–1006. doi:10.1139/h08-075
11. Nagao Y, Yokoi A, Yoshida K, et al. Clinical effects of cervical conization with positive margins in cervical cancer. Sci Rep. 2021;11(1):23288. doi:10.1038/s41598-021-02635-y
12. Singh NAS. Histopathologic parameters of prognosis in cervical cancer--a review. Int J Gynecol Cancer. 2004;14(5):741–750. doi:10.1111/j.1048-891X.2004.014504.x
13. Cibula D, Raspollini MR, Planchamp F, et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer – update 2023*. Int J Gynecol Cancer. 2023;33(5):649–666. doi:10.1136/ijgc-2023-004429
14. Lee J, Chang C-L, Lin J-B, et al. Skeletal muscle loss is an imaging biomarker of outcome after definitive chemoradiotherapy for locally advanced cervical cancer. Clin Cancer Res. 2018;24(20):5028–5036. doi:10.1158/1078-0432.Ccr-18-0788
15. Yun P, Xia B, Tian X, et al. Body composition and risk of major gynecologic malignancies: results from the UK Biobank prospective cohort. Cancer Med. 2021;10(13):4522–4531. doi:10.1002/cam4.3925
16. Shen W, Punyanitya M, Wang Z, et al. Total body skeletal muscle and adipose tissue volumes: estimation from a single abdominal cross-sectional image. J Appl Physiol. 2004;97(6):2333–2338. doi:10.1152/japplphysiol.00744.2004
17. Mitsiopoulos NBR, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J Appl Physiol. 1998;85(1):115–122. doi:10.1152/jappl.1998.85.1.115
18. Martin L, Birdsell L, MacDonald N, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol. 2013;31(12):1539–1547. doi:10.1200/jco.2012.45.2722
19. Camp RLD, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res. 2004;10(21):7252–7259. doi:10.1158/1078-0432.CCR-04-0713
20. Ayhan S, Akar S, Kar İ, et al. Prognostic value of systemic inflammatory response markers in cervical cancer. J Obstet Gynaecol. 2022;42(6):2411–2419. doi:10.1080/01443615.2022.2069482
21. Tian BW, Yang CC, Yan LJ, et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: systemic review and meta-analysis. Immunotherapy. 2022;14(18):1481–1496. doi:10.2217/imt-2022-0133
22. Liu P, Jiang Y, Zheng X, et al. Pretreatment systemic immune-inflammation index can predict response to neoadjuvant chemotherapy in cervical cancer at stages IB2-IIB. Pathol Oncol Res. 2022;28:1610294. doi:10.3389/pore.2022.1610294
23. Haraga J, Nakamura K, Omichi C, et al. Pretreatment prognostic nutritional index is a significant predictor of prognosis in patients with cervical cancer treated with concurrent chemoradiotherapy. Mol Clin Oncol. 2016;5(5):567–574. doi:10.3892/mco.2016.1028
24. Gangopadhyay A. Prognostic nutritional index and clinical response in locally advanced cervical cancer. Nutr Cancer. 2020;72(8):1438–1442. doi:10.1080/01635581.2020.1729820
25. Caan BJ, Cespedes Feliciano EM, Prado CM, et al. Association of muscle and adiposity measured by computed tomography with survival in patients with nonmetastatic breast cancer. JAMA Oncol. 2018;4(6):798–804. doi:10.1001/jamaoncol.2018.0137
26. Caan BJ, Meyerhardt JA, Kroenke CH, et al. Explaining the obesity paradox: the association between Body Composition and Colorectal Cancer Survival (C-SCANS Study). Cancer Epidemiol Biomarkers Prevent. 2017;26(7):1008–1015. doi:10.1158/1055-9965.Epi-17-0200
27. Li Y, Wang W-B, Yang L, et al. The combination of body composition conditions and systemic inflammatory markers has prognostic value for patients with gastric cancer treated with adjuvant chemoradiotherapy. Nutrition. 2022;93:111464. doi:10.1016/j.nut.2021.111464
28. Yamahara K, Mizukoshi A, Lee K, et al. Sarcopenia with inflammation as a predictor of survival in patients with head and neck cancer. Auris Nasus Larynx. 2021;48(5):1013–1022. doi:10.1016/j.anl.2021.03.021
29. Go S-I, Park MJ, Song H-N, et al. Sarcopenia and inflammation are independent predictors of survival in male patients newly diagnosed with small cell lung cancer. Support Care Cancer. 2015;24(5):2075–2084. doi:10.1007/s00520-015-2997-x
30. Zhang X, Li H, He M, et al. Immune system and sarcopenia: presented relationship and future perspective. Exp Gerontol. 2022;164:111823. doi:10.1016/j.exger.2022.111823
31. Iyengar NM, Hudis CA, Dannenberg AJ. Obesity and cancer: local and systemic mechanisms. Annu Rev Med. 2015;66(1):297–309. doi:10.1146/annurev-med-050913-022228
32. Iyengar NM, Gucalp A, Dannenberg AJ, et al. Obesity and cancer mechanisms: tumor microenvironment and inflammation. J Clin Oncol. 2016;34(35):4270–4276. doi:10.1200/jco.2016.67.4283
33. Liu C, Zhang M, Yan X, et al. Single-cell dissection of cellular and molecular features underlying human cervical squamous cell carcinoma initiation and progression. Sci Adv. 2023;9(4):eadd8977. doi:10.1126/sciadv.add8977
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nomogram to Predict Radiation Enteritis in Cervical Squamous Cell Carcinoma
Wang J, Hu G
Cancer Management and Research 2022, 14:3303-3311
Published Date: 25 November 2022
Evaluation of Lactate Dehydrogenase and Alkaline Phosphatase as Predictive Biomarkers in the Prognosis of Hepatocellular Carcinoma and Development of a New Nomogram
Su K, Huang W, Li X, Xu K, Gu T, Liu Y, Song J, Qian K, Xu Y, Zeng H, Yang Y, Guo L, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:69-79
Published Date: 14 January 2023
Preoperative Systemic Inflammatory Markers as a Significant Prognostic Factor After TURBT in Patients with Non-Muscle-Invasive Bladder Cancer
Ding L, Deng X, Wang K, Xia W, Zhang Y, Zhang Y, Shao X, Wang J
Journal of Inflammation Research 2023, 16:283-296
Published Date: 21 January 2023
An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction
Chen Y, Xie K, Han Y, Xu Q, Zhao X
Journal of Inflammation Research 2023, 16:4061-4071
Published Date: 13 September 2023
Development and Internal-External Validation Models for Cervical Cancer Overall Survival Prognosis: A SEER-Based Study and Chinese Data
Shi Y, Xu JN, Wang QQ, Wang SY, Wang LY
International Journal of Women's Health 2025, 17:2051-2062
Published Date: 12 July 2025