Back to Journals » ImmunoTargets and Therapy » Volume 14
Predicting ICU Admission in Patients with Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy
Authors Su XH, Li WP, Xu XF, Su XL, Liu J, Feng SY, Liu JY, Dong RQ, Ngai IK, Yang L, Xu L, Li ZQ, Li DC, Jiang Y, Peng FH ![]()
Received 19 March 2025
Accepted for publication 29 July 2025
Published 8 August 2025 Volume 2025:14 Pages 799—814
DOI https://doi.org/10.2147/ITT.S522190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah Wheeler
Xiao-Hong Su,1,* Wei-Peng Li,2,3,* Xiao-Feng Xu,1,* Xiao-Ling Su,4 Jia Liu,1 Shi-Yuan Feng,1 Jun-Yu Liu,1 Rui-Qi Dong,1 Iok Keng Ngai,1 Lu Yang,1 Li Xu,1 Zhe-Qi Li,1 Dong-Cheng Li,1 Ying Jiang,1 Fu-Hua Peng1
1Department of Neurology, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 2School of Traditional Chinese Medicine, Southern Medical University, Guangzhou, People’s Republic of China; 3Department of Neurology, Southern Medical University Hospital of Integrated Traditional Chinese and Western Medicine, Southern Medical University, Guangzhou, People’s Republic of China; 4Department of Cardiovascular and Oncology, Zhongshan People’s Hospital of Torch Development Zone, Zhongshan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fu-Hua Peng; Ying Jiang, Department of Neurology, The Third Affiliated Hospital, Sun Yat-Sen University, 600 Tianhe Road, Guangzhou, Guangdong, 510630, People’s Republic of China, Tel +86-20-85253275, Email [email protected]; [email protected]
Introduction: Autoimmune glial fibrillary acidic protein astrocytopathy (A-GFAP-A) is an increasingly recognized neurological disorder with significant clinical management challenges, particularly in predicting the need for intensive care unit (ICU) admission. This study aimed to develop and validate predictive models to identify A-GFAP-A patients at increased risk for ICU admission.
Methods: We retrospectively analyzed 107 patients (January 2021 - August 2024), randomly assigned to training and validation cohorts (7:3). Variable selection for model development was performed using random forest, least absolute shrinkage and selection operator (LASSO), and extreme gradient boosting (XGBoost). Logistic regression was used to construct a nomogram, and a decision tree was developed to facilitate rapid clinical decision-making. Model performance was assessed by area under the curve (AUC), calibration plots, and decision curve analysis (DCA).
Results: Four key predictors of ICU admission were identified: Glasgow Coma Scale (GCS) score at admission, seizures, maximum body temperature, and C-reactive protein (CRP) levels. The nomogram demonstrated excellent predictive accuracy with AUCs of 0.923 (95% CI, 0.858– 0.987) in training cohort, 0.922 (95% CI, 0.836– 1.000) in validation cohort, and 0.93 (95% CI, 0.883– 0.972) in bootstrap validation. The model showed excellent calibration, and DCA confirmed its clinical utility. The decision tree identified GCS < 15, seizures, and temperature > 39°C as the most relevant indicators for high-risk stratification.
Discussion: This study presents the first validated nomogram and decision tree for ICU admission risk in A-GFAP-A, based on the largest reported cohort to date, providing a valuable tool for clinical decision-making and resource optimization.
Keywords: prediction model, glial fibrillary acidic protein astrocytopathy, intensive care unit
Introduction
Since its identification in 2016, autoimmune glial fibrillary acidic protein astrocytopathy (A-GFAP-A) has garnered increasing attention,1 particularly due to its association with various clinical manifestations, including encephalopathy, myelitis, and meningitis, affecting both the central and peripheral nervous systems.2–5 In severe cases, A-GFAP-A can manifest with frequent seizures, coma, and extensive spinal cord involvement leading to paraplegia.5–8 These patients often face poor prognoses, requiring prolonged rehabilitation and experiencing long-term sequelae such as limb disability and cognitive impairment.9 Clinical observations reveal that many of these severe cases necessitate admission to the intensive care unit (ICU), highlighting the complexity and severity of A-GFAP-A.10,11 It has been reported that 36% of A-GFAP-A patients had been admitted to ICU.4
ICU admission in A-GFAP-A patients often indicates disease progression and a poorer prognosis. Early identification of patients at risk for ICU admission is critical for improving prognosis and optimizing healthcare resources.12,13 However, to the best of our knowledge, no predictive models are currently available to guide ICU admission decisions for A-GFAP-A patients, limiting opportunities for timely intervention.
In this study, we aimed to identify the clinical features and risk factors linked to ICU admission in A-GFAP-A patients and to develop predictive models to help recognize those at higher risk. Based on the largest and most comprehensive retrospective cohort to date, these models are intended to support clinical decision-making, enhance patient management, and optimize healthcare resource allocation.
Materials and Methods
Study Population and Ethics
The study was conducted in accordance with the principles of the Declaration of Helsinki, and the protocol was approved by the medical ethics committee at the Third Affiliated Hospital of Sun Yat-Sen University (ethics number [2022] 02-093-01).
We retrospectively analyzed data from 107 Chinese Han A-GFAP-A patients between Jan 2021 and August 2024 at the Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China. All enrolled patients underwent antibody testing in both serum and cerebrospinal fluid (CSF) using a combination of cell-based assay (CBA) and tissue-based assay (TBA), with CBA used as the primary diagnostic tool and TBA serving as supplementary evidence. In addition, metagenomic next-generation sequencing (mNGS) was performed to exclude infectious etiologies. Inclusion criteria: (1) Positive GFAP-IgG antibodies in CSF confirmed by CBA (Rationale: CSF CBA is the most specific and reliable method for diagnosing A-GFAP-A.14 Serum-only positivity may be non-pathogenic or incidental and was therefore excluded to avoid diagnostic ambiguity); (2) Presence of one or more characteristic clinical syndromes, including meningitis, encephalitis, myelitis, or optic neuritis (Rationale: Inclusion required a clinical phenotype consistent with the disease to ensure pathophysiological relevance of antibody positivity); (3) Availability of complete clinical, laboratory, and imaging data (Rationale: Complete datasets were essential for outcome analysis, including ICU admission risk, and allowed for meaningful statistical comparisons). Exclusion criteria: (1) Positive GFAP-IgG antibodies in serum only, without CSF confirmation (Rationale: Isolated serum positivity is less specific and may represent subclinical or incidental autoimmunity; inclusion could lead to misclassification); (2) Incomplete clinical or diagnostic records (Rationale: Missing essential data precludes accurate analysis of ICU predictors and model development).
Data Collection
Clinical and laboratory data were collected and evaluated at the time of initial discharge, including demographic information, clinical symptoms (eg, fever, headache, altered consciousness, seizures), neurological assessments (eg, Glasgow Coma Scale [GCS] score, modified Rankin scales [mRS] score, Clinical Assessment Scale for Autoimmune Encephalitis [CASE] score), imaging results (eg, magnetic resonance imaging findings), laboratory results (eg, CSF analysis and blood test), treatment details and clinical outcomes, which were similar to those described in our previous work.15 The primary outcome of interest was ICU admission. The GCS scores and mRS scores were assessed by independent neurologists who did not participate in the treatment.
Cell- and Tissue-Based Immunofluorescence Assays
To diagnose A-GFAP-A, serum and CSF samples were tested for GFAP-IgG using a cell-based assay (CBA) employing HEK293 cells co-transfected with human GFAP and pEGFP-N1 plasmids. CBAs were also performed to screen for other autoimmune antibodies, including CNS-targeting antibodies (GFAP, MBP, AQP-4, MOG, NMDAR, AMPAR, GABAAR, GABABR, CASPR2, IgLON5, LGI1, DPPX, mGluR1, mGluR5, GlyR1, D2R, neurexin 3α) and paraneoplastic antibodies (Hu, Yo, Ri, Ma1, Ma2, CV2, SOX1, Tr/DNER, Zic4, Titin, PKC-γ, recoverin, GAD65, and amphiphysin).14,16 Tissue-based immunofluorescence assays (TBA) were performed on 4-µm cryosections of adult macaque cerebellum and hippocampus. Thresholds for positivity were defined as titers ≤1:2 in CSF. All assays were conducted in collaboration with ImmunoArt Company (Guangzhou, China) using self-developed reagents not available commercially.
mNGS Procedures
A total of 2 mL of CSF was collected from each patient, immediately frozen on dry ice, and submitted for PACEseq mNGS (Hugo biotech company, Beijing, China).17 DNA was extracted from 200 µL using the TIANamp Micro DNA Kit (Tiangen, Cat# DP316) with an internal “No Template” control. Libraries preparation was prepared using the QIAseq™ Ultralow Input Kit (Qiagen, Cat# 180495), and libraries were assessed using Qubit 4.0 Fluorometer (Thermo Fisher Scientific) and gel electrophoresis. Sequencing was carried out on the NextSeq 550 platform (Illumina) using 150-cycle paired-end reads, yielding approximately 5–10 million reads per sample. High-quality reads were filtered and aligned against a curated microbial genome database (based on NCBI RefSeq) for pathogen identification.
Treatment Strategies
The patients received first-line and maintenance immunotherapies, which included pulse-dose intravenous methylprednisolone (IVMP, 1000 mg/d for 3–5 days, followed by a gradual tapering of oral prednisolone), intravenous immunoglobulin (IVIg) (0.4 g/kg/day for 3–5 days), efgartigimod (20 mg/kg administered intravenously on the 1st and 5th day), or protein A immunoadsorption (PAIA). And maintenance immunotherapies consisted of oral corticosteroids, mycophenolate mofetil (MMF) and azathioprine, among others.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median with interquartile range (IQR) and compared using Student’s t test or the Mann–Whitney U-test, as appropriate. Categorical variables were summarized as frequencies and percentages and compared using the Chi-square test or Fisher’s exact test. Univariate analysis was initially used to identify candidate predictors of ICU admission, followed by machine learning methods,18,19 including random forest, least absolute shrinkage and selection operator (LASSO), and eXtreme Gradient Boosting (XGBoost), to refine the selection and identify the most significant predictors. A total of 107 A-GFAP-A patients were enrolled and randomly assigned to a training (n = 74) and a validation (n = 33) cohort in a 7:3 ratio. A logistic regression-based nomogram model was then developed and evaluated using the area under the receiver operating characteristic (ROC) curve (AUC). Calibration was evaluated using calibration plots and Hosmer-Lemeshow tests. Furthermore, decision curve analysis (DCA) was used to evaluate the net benefit of the model. Model robustness was confirmed via internal validation with 500 bootstrap resamples. A decision tree was fitted using all patients and the most relevant predictor variables to develop a simplified prediction model for rapid clinical use.
All analyses were performed in R (version 4.4.0). LASSO, random forest, and XGBoost were conducted using the “glmnet”, “randomForest”, and “xgboost” packages, respectively. Multivariate logistic regression, nomogram development, and calibration plots were performed using the “rms” package. DCA was conducted with the “rmda” package. The decision tree analysis was conducted using “party” package. Additional statistical visualization was performed using GraphPad Prism (version 6.0). A p-value < 0.05 was considered statistically significant.
Results
General Characteristics and Baselines
The study flowchart is presented in Figure 1. Out of 120 patients initially identified with A-GFAP-A, 7 patients were excluded due to having only serum-positive GFAP antibodies, and 6 were excluded due to incomplete records (3 lacked cerebrospinal fluid results and 3 lacked imaging information). Ultimately, 107 patients were included in the study, with 38 (35.5%) requiring ICU admission during hospitalization, whom were assessed using the GCS, mRS, CASE and APACHE II (see Table 1 and Figure S1). Compared to those not admitted to the ICU, patients in the ICU group had significantly lower GCS scores (p < 0.001) and higher mRS and CASE scores (both p < 0.001), and were also more likely to present with headache (75.4% vs 94.7%, p = 0.025), fever (73.9% vs 92.1%, p = 0.044), higher maximum temperature (median: 38.6°C vs 39.5°C, p < 0.001), impaired consciousness (30.4% vs 86.8%, p < 0.001), urinary disorders (49.3% vs 76.3%, p = 0.012), psychiatric symptoms (27.5% vs 63.2%, p = 0.012), seizures (17.4% vs 60.5%, p < 0.001), and co-infection with Epstein-Barr (EB) virus (7.2% vs 28.9%, p = 0.006) (see Table 1). Furthermore, ICU-admitted patients exhibited higher percentages of neutrophils (69% vs 79%, p<0.001) and higher levels of CRP (p = 0.034) (see Table 1 and Table 2). Notably, there were no significant differences in treatment strategies targeting A-GFAP-A between the two groups (see Table S1). However, when compared to the non-ICU group, patients in the ICU cohort exhibited poorer outcomes and a greater prevalence of residual symptoms at one month (see Table S2 and Figure S2). Therefore, predicting the risks of ICU admission are critical. To develop a predictive model, the patients were randomly assigned to the training cohort (n = 74) and validation cohort (n = 33) in a 7:3 ratio. Baseline characteristics were comparable between the two cohorts, ensuring no significant differences that could bias the predictive modeling (see Table 1 and Table 2).
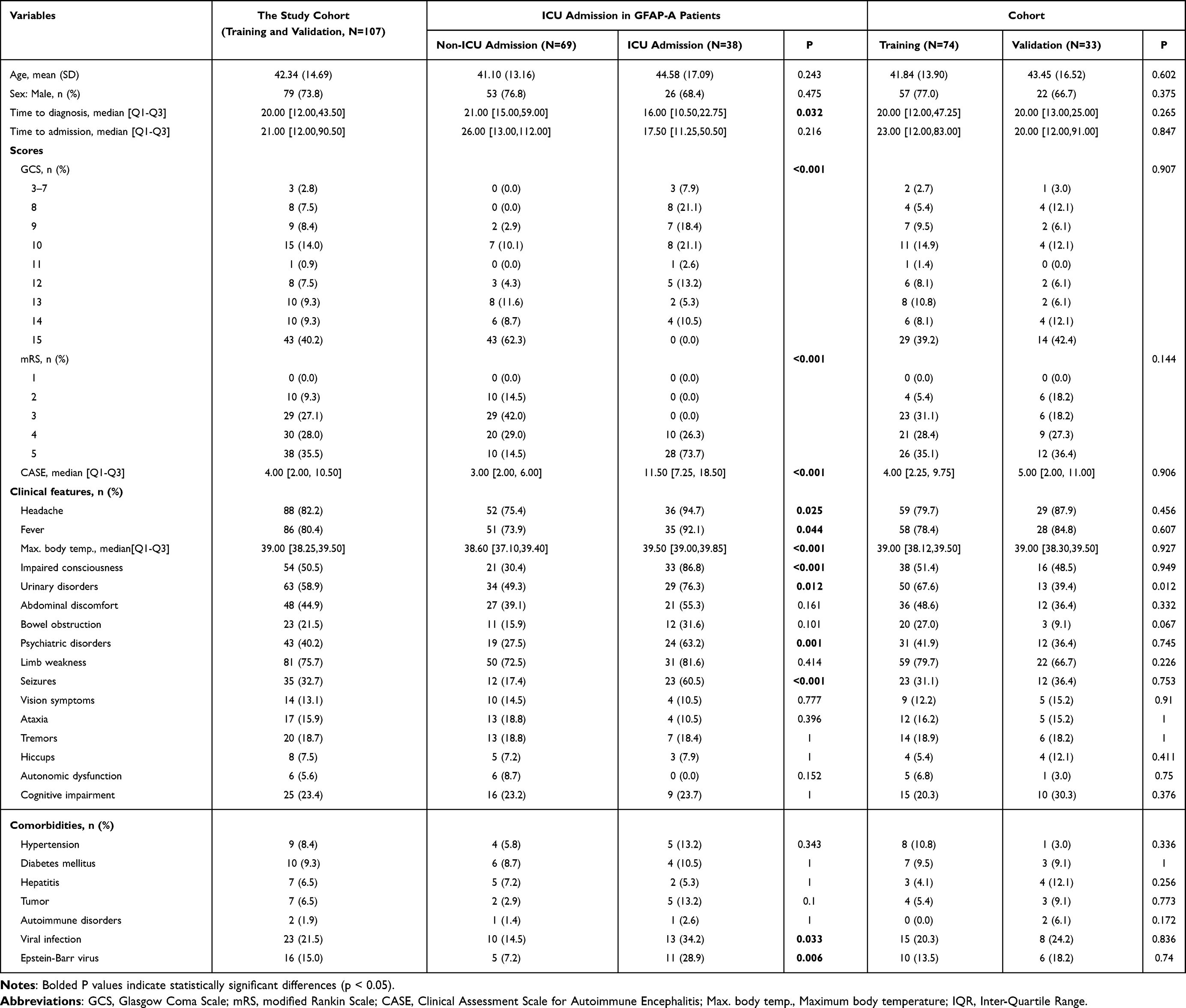 |
Table 1 Demographic and Clinical Characteristics of Patients |
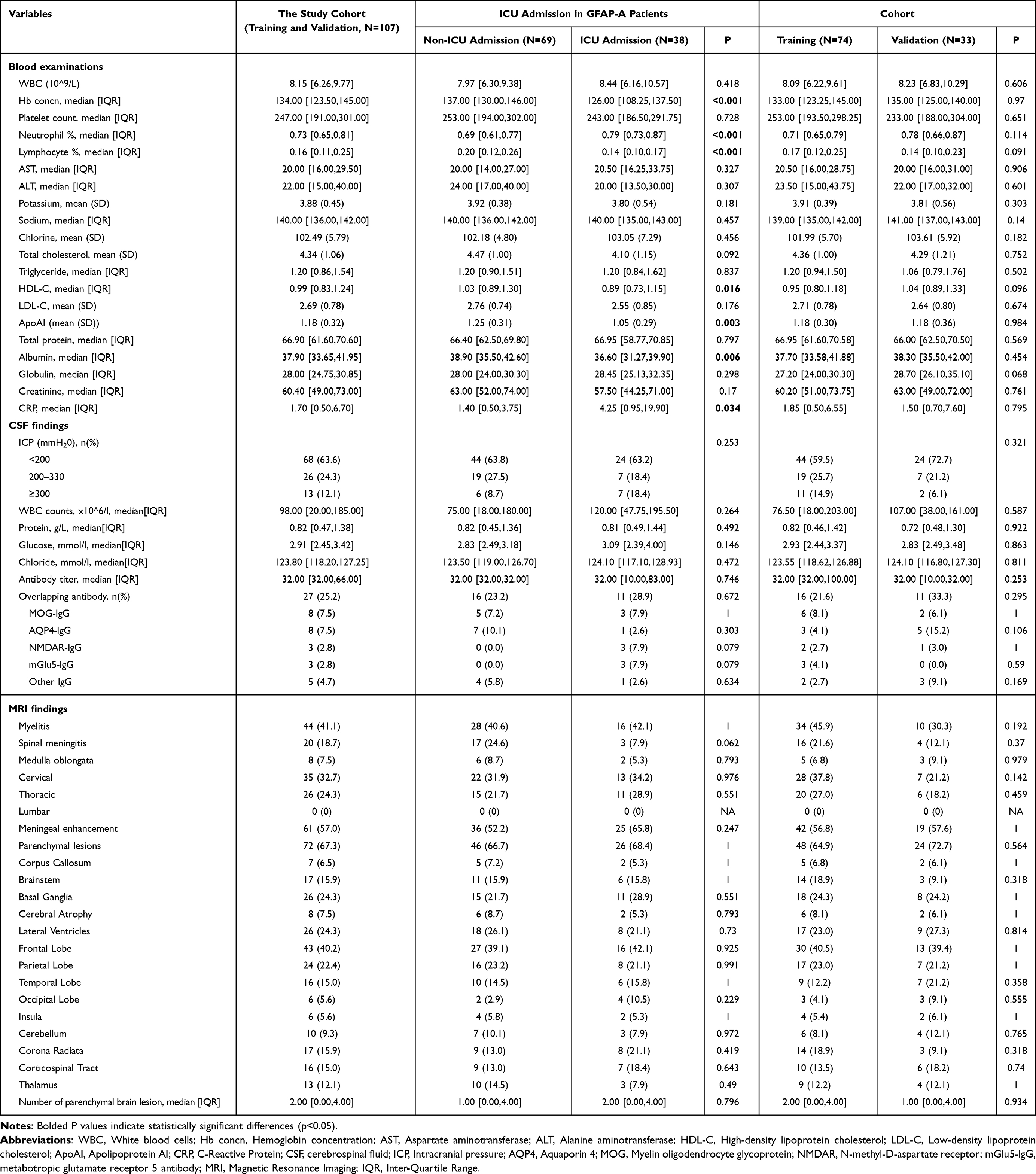 |
Table 2 Laboratory, CSF and Imaging Findings |
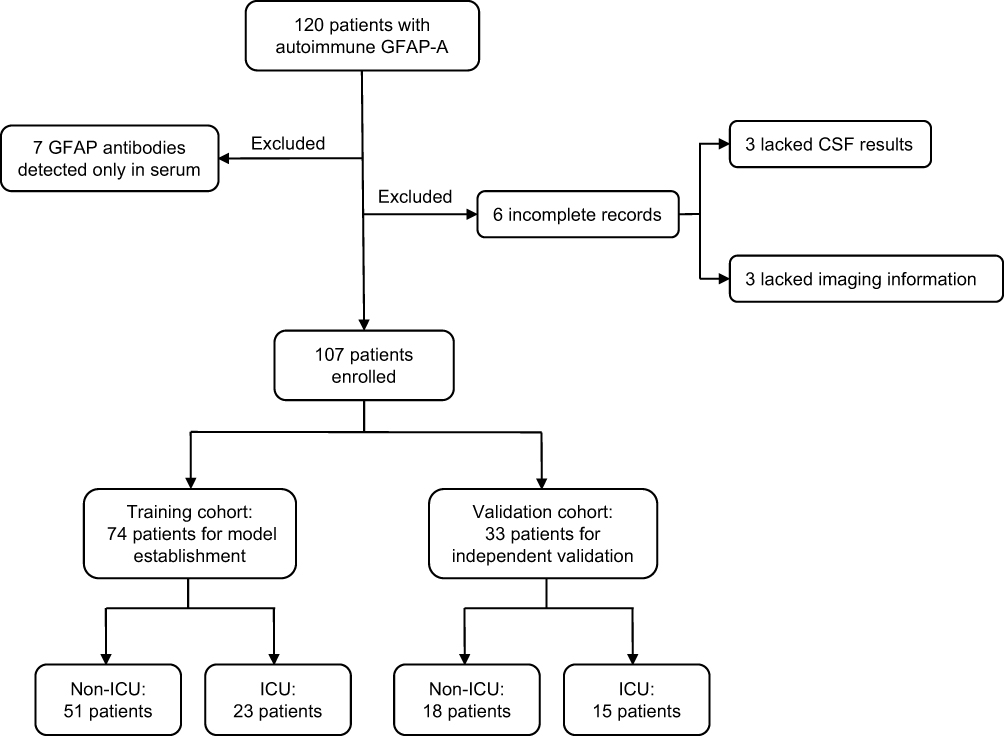 |
Figure 1 Study flowchart. |
Screening for Predictive Variables
To further identify the key predictors that significantly contribute to the risk of ICU admission in A-GFAP-A patients, we employed a combination of machine learning methods, including LASSO, random forest, and XGBoost. Variables with a p-value < 0.10 on univariate analysis were selected for further analysis. The most important variables selected through the LASSO regression (with 10-fold cross-validation) included gender, spinal meningitis, GCS at admission, C-reactive protein (CRP), CASE at admission, impaired consciousness, present of EB virus in the CSF, mRS at admission, maximum temperature, and seizures (see Figure 2A–D). Similarly, random forest analysis identified 10 key predictors (see Figure 2E and F), including GCS at admission, maximum temperature, mRS at admission, CASE at admission, impaired consciousness, seizures, neutrophil percentage, present of EB virus in the CSF, RBC, gender, and CRP. XGBoost analysis highlighted the relative importance of these variables, assigning variable importance scores to GCS at admission, maximum temperature, CASE at admission, mRS at admission, neutrophil percentage, seizures, and CRP (see Figure 2G and H).
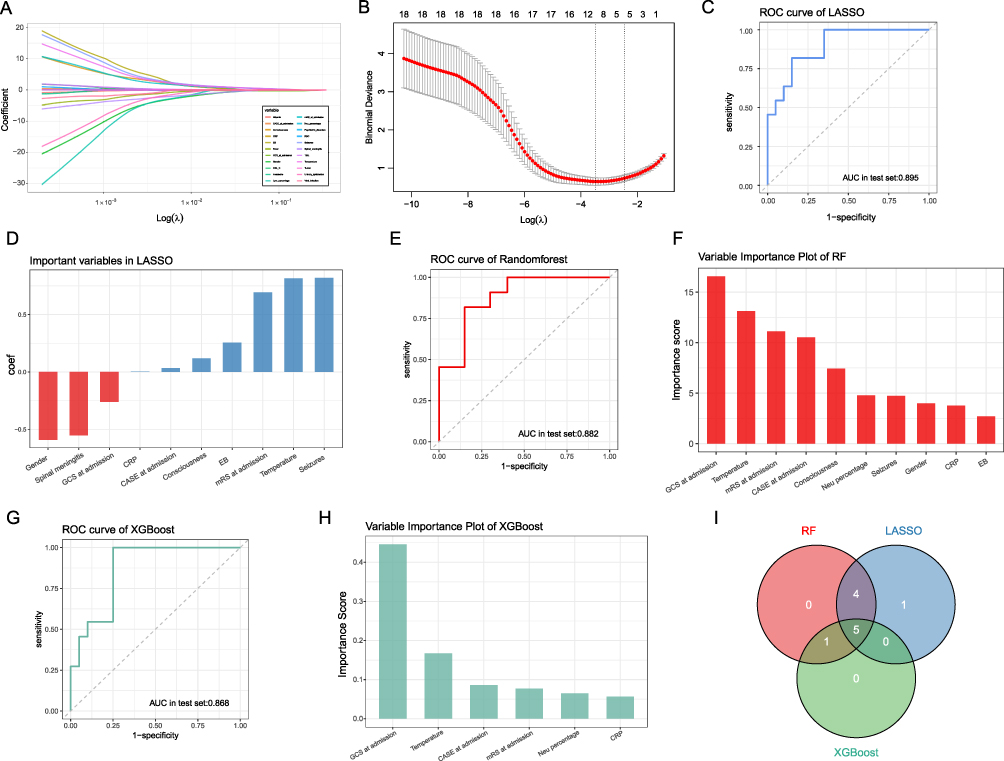 |
Figure 2 Selection and importance ranking of predictive variables for ICU admission in A-GFAP-A patients using machine learning methods. (A) LASSO coefficient profiles for candidate variables, showing the shrinkage of coefficients as the regularization parameter (lambda) increases. (B) Ten-fold cross-validation plot for LASSO regression, indicating the optimal lambda value corresponding to the minimum mean cross-validated error. (C) Receiver Operating Characteristic (ROC) curve for the LASSO model. (D) Bar plot of variable coefficients selected by the LASSO model. (E) Variable importance plot from the Random Forest model. (F) ROC curve for the Random Forest model. (G) Feature importance plot from the XGBoost model. (H) ROC curve for the XGBoost model. (I) Venn diagram summarizing common predictors identified across all three machine learning methods. |
In addition, the AUC (area under the ROC curve) values for these three models were 0.895, 0.882, and 0.868, respectively, indicating that each model demonstrated good performance (see Figure 2C, E and G). However, considering that some variables identified by these methods were linearly correlated, we selected the more sensitive variables as predictive factors (see Figure S3). A Venn diagram was used to extract the common important variables across LASSO, random forest, and XGBoost (see Figure 2I), with the following variables consistently emerging as key predictors: GCS at admission, seizures, maximum temperature, and CRP in CSF. These variables were subsequently used to construct the nomogram.
Establishment of the Nomogram and Validation
To predict the probability of ICU admission in A-GFAP-A patients, we developed a logistic regression-based nomogram incorporating the identified predictive variables into a single tool (see Figure 3). Each predictor was assigned a specific score, allowing the calculation of a total score that estimates the probability of ICU admission for each patient.
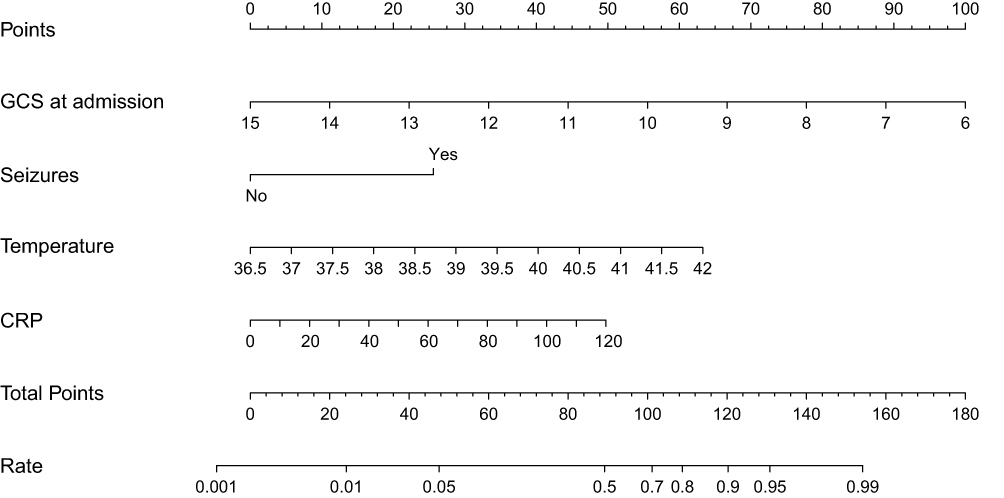 |
Figure 3 Nomogram for predicting the risk of ICU admission in patients with GFAP astrocytopathy. |
The nomogram model demonstrated excellent predictive performance, with an area under the ROC curve (AUC) of 0.953 (95% CI, 0.911–0.996) in the training cohort, and 0.929 (95% CI, 0.845–1) in the validation cohort, indicating strong discrimination ability (see Figure 4). Additionally, the robustness of the nomogram was validated using bootstrapping methods with 500 resamples, resulting in an AUC of 0.94 (95% CI, 0.893–0.976) (see Figure S4).
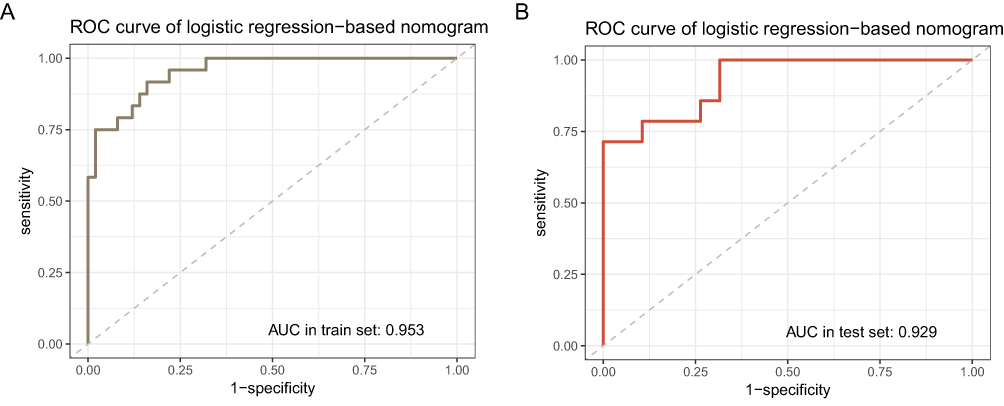 |
Figure 4 Performance evaluation of the nomogram predicting ICU admission in A-GFAP-A patients using ROC analysis. |
Calibration of the nomogram was assessed using calibration plots, which showed strong agreement between predicted and observed outcomes in both the training and validation cohorts (see Figure 5). The Hosmer-Lemeshow test p-value of the model were 0.971 and 0.995, suggesting no significant deviation from a perfect fit between predicted and observed values. The DCA curves showed significant net benefit of the predictive model in both the training and validation cohorts (see Figure 6), highlighting its valuable practical application in clinical settings.
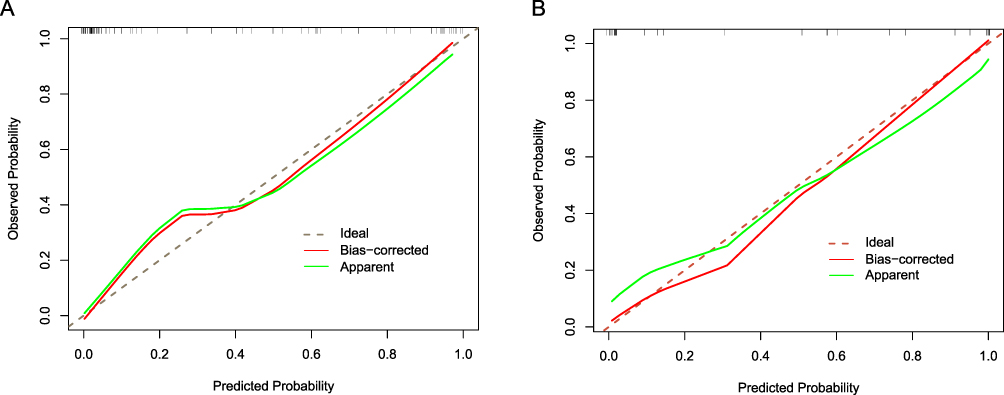 |
Figure 5 Calibration plots of the nomogram for predicting ICU admission in A-GFAP-A patients. (A) Training cohort (n = 74): Predicted probabilities closely aligned with observed outcomes along the 45° reference line, indicating excellent calibration (Hosmer-Lemeshow p = 0.971). (B) Validation cohort (n = 33): Similarly strong agreement with minimal deviation from the ideal line (Hosmer-Lemeshow p = 0.995). |
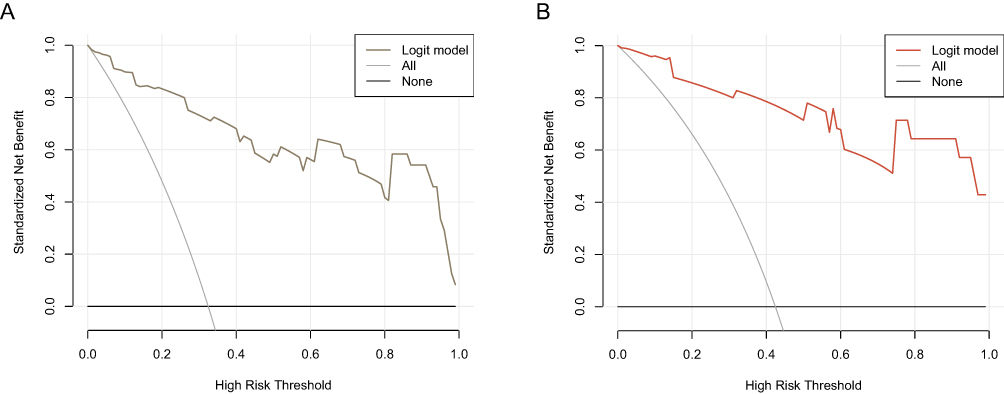 |
Figure 6 DCA of the nomogram for ICU admission prediction in A-GFAP-A patients. (A) Training cohort (n = 74): The model showed clear net clinical benefit across a range of threshold probabilities compared to “treat-all” and “treat-none” strategies. (B) Validation cohort (n = 33): Demonstrated comparable net benefit, supporting the model’s clinical applicability. |
Establishment of the Decision Tree for ICU Admission Prediction
To facilitate rapid prediction, a simplified decision tree model was developed to assist clinicians in making quicker diagnoses and informed decisions. The model indicates that patients with a GCS score below 15, seizures, and a maximum body temperature over 39°C are at higher risk of ICU admission (see Figure 7).
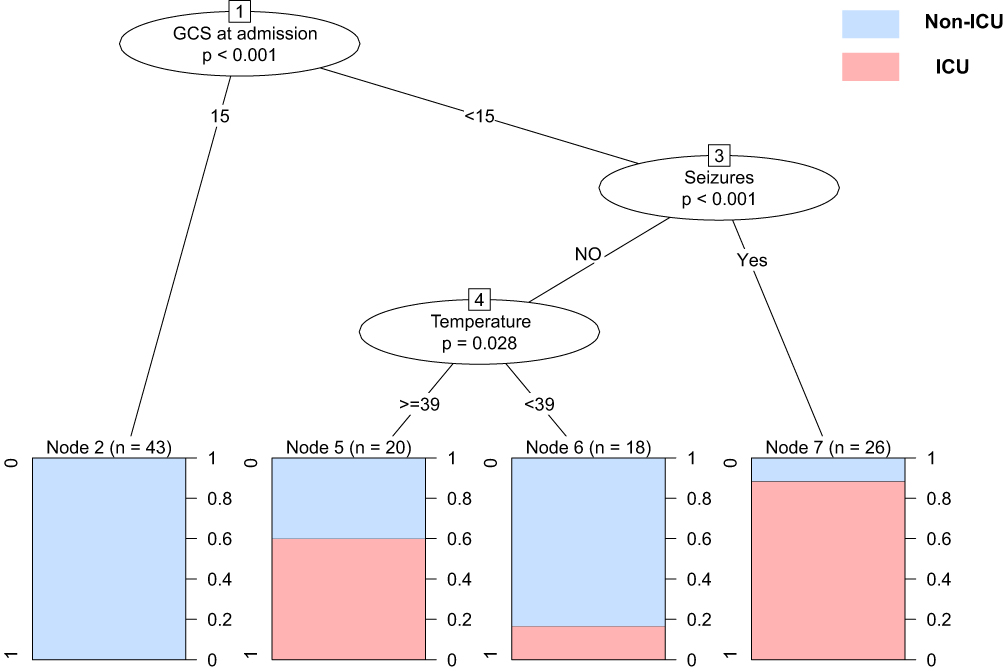 |
Figure 7 Decision tree for predicting ICU admission in A-GFAP-A patients. Key predictors include a GCS score <15 at admission, the presence of seizures, and a body temperature above 39°C. P-values at each node indicate the statistical significance of these predictors. |
Discussion
This study presents, to our knowledge, the first predictive model for ICU admission in A-GFAP-A patients, developed from the largest observational cohort reported to date. The nomogram, which incorporates four key variables, GCS at admission, seizures, maximum temperature, and CRP levels, demonstrated strong discriminatory power, calibration, and clinical utility. In addition, a decision tree model was developed to facilitate rapid clinical decision-making. Together, these models provide practical tools for guiding timely interventions and optimizing outcomes in A-GFAP-A patients.
A-GFAP-A is a rare neurological disorder characterized by acute or subacute encephalomyelitis, and with the increasing incidence, it is gradually becoming a challenge and an increasingly recognized disease worldwide.20 Many patients experience acute onset, rapid progression, and life-threatening symptoms that necessitate ICU admission.10,21–23 However, prior to this study, no models had been proposed to assess the risk of ICU admission in A-GFAP-A patients. Early identification of at-risk patients is critical for initiating appropriate treatment and improving outcomes. Our model identifies GCS at admission, seizures, maximum temperature, and CRP levels as key predictors of ICU admission. These variables are easily and quickly assessable upon admission, enabling prompt intervention and informed decision-making. Statistically, our model exhibited great discriminative ability and potential clinical benefit.
The model identified GCS at admission as one of the strongest predictors of ICU admission in A-GFAP-A patients. A low GCS score indicates reduced consciousness,24 reflecting severe neurological involvement and an increased risk of complications such as respiratory failure, or aspiration, all of which may necessitate ICU care.25 Although mRS and CASE were also initially screened as potential predictors, they exhibited a strong negative correlation with GCS. Given GCS’s superior statistical performance in predictive modeling, it was selected as the more robust and independent variable to avoid multicollinearity and redundancy. In addition, among the three scales (GCS, mRS, and CASE), GCS is the quickest to administer, making it more practical in urgent or complex clinical situations where rapid assessment is essential for ICU decision-making. As for central respiratory dysfunction, while central respiratory dysfunction may contribute independently to ICU admission,26,27 we evaluated MRI findings involving regions such as the brainstem and spinal cord but found no statistically significant differences in these imaging features between patients who required ICU care and those not admitted. These results suggest that central respiratory dysfunction related to A-GFAP-A may not be reliably diagnosed through conventional imaging, and additional clinical or physiological markers may be needed for accurate identification and differentiation.
Seizures were another important predictor of ICU admission. Particularly, status epilepticus is a medical emergency associated with high morbidity and mortality, requiring intensive monitoring and management.28,29 In our study, over 60% of patients who experienced status epilepticus required ICU care, indicating a strong association between seizure severity and the need for intensive support. Interestingly, a previous study involving 34 A-GFAP-A patients reported that 50% had hyponatremia (serum sodium <135 mmol/L), which may contribute to seizure development through the mechanisms: (1) reduced extracellular osmotic pressure causing brain cell swelling and membrane instability, and (2) impaired sodium balance disrupting GABAergic and glutamatergic signaling, increasing neuronal excitability.30,31 Additionally, 14.7% of patients in this study had coexisting neural autoantibodies (eg, NMDAR-IgG), which may interact with GFAP-IgG to worsen neuroinflammation and raise seizure risk.30 However, serum sodium levels did not differ significantly between patients with and without seizures (see Figure S5), suggesting that hyponatremia may not be the primary driver of seizure activity in our cohort. Instead, we believe seizure occurrence may be more closely related to the disease progression of A-GFAP-A itself, though the exact mechanisms remain unknown. These findings highlight the importance of careful monitoring and timely intervention in A-GFAP-A patients with seizures to prevent serious complications.
Additionally, maximum temperature was also a key predictor, reflecting the inflammatory response and potential for exacerbated central nervous system (CNS) damage in this study. Our previous research has showed that A-GFAP-A patients exhibit higher temperatures compared to those with tuberculous meningitis.32 Moreover, febrile temperatures are known to amplify pro-inflammatory Th17 cell activity,33 contributing to elevated CRP levels, which is also another critical variable in our model. Elevated CRP levels probably indicate immune activation, aligning with previous research linking CRP to severe cases of autoimmune encephalitis requiring prolonged ventilation.34,35
Interestingly, the presence of EB virus in the CSF is also associated with an increased risk of ICU admission. Although EB virus has not been extensively linked to A-GFAP-A in prior studies, it may trigger a post-infectious autoimmune response through molecular mimicry or infected B cells.27,36,37 This association suggests the need for aggressive management in such cases, given the potentially worse prognosis associated with EB virus-related complications.
The decision tree helps clinicians quickly identify high-risk patients by focusing on key parameters. In this study, we used decision trees to create a simple and practical prediction rule, building on our previous work where random forests helped identify key predictors of postinfectious inflammatory response syndrome (PIIRS) in HIV-negative immunocompetent cryptococcal meningitis patients.38 The decision tree focuses on three easily measurable parameters: a GCS score below 15, seizures, and a temperature above 39°C. By concentrating on these key factors, clinicians can rapidly assess patient risk, enabling timely decisions and more aggressive immunotherapy when necessary.
A core question in the management of A-GFAP-A is whether ICU admission reflects the intrinsic severity of the disease, its complications, or patients’ underlying conditions. Currently, no standardized criteria exist to assess disease severity in A-GFAP-A, and in our cohort, conventional diagnostic indicators such as MRI and CSF analyses did not significantly differ between ICU and non-ICU patients. In contrast, we observed substantial differences in clinical manifestations, including impaired consciousness, seizures, psychiatric symptoms, limb weakness, and urinary dysfunction, which likely represent CNS involvement and disease progression. These symptoms, particularly seizures and altered mental status, are consistent with known indications for ICU admission across neurological disorders.39–41 Fever and elevated inflammatory markers (eg, CRP) also correlated with ICU admission, suggesting that systemic inflammatory responses may exacerbate disease severity or reflect underlying disease activity.42,43 Although complications may arise from A-GFAP-A pathophysiology, current evidence does not support a definitive causal link. Our analysis also found no significant association between ICU admission and comorbid autoimmune or chronic diseases, potentially attributable to the younger demographic profile of the cohort (mean age ~42). Taken together, our findings suggest that ICU admission in A-GFAP-A is primarily driven by acute neurological and systemic manifestations rather than underlying conditions. We propose that incorporating key clinical features, such as seizures, fever, and level of consciousness, into a structured assessment may improve ICU decision-making and patient outcomes, forming the basis for future severity scoring systems tailored to A-GFAP-A.
This predictive model has several limitations. Firstly, the retrospective design and relatively small sample size restrict the generalizability of the findings. Secondly, the model was developed from a single-center cohort, which may not reflect variations across regions or healthcare systems, limiting its applicability in broader or resource-constrained settings. Third, although the model demonstrated strong internal validity, prospective multicenter studies in more diverse populations are needed for external validation and refinement. However, the high cost and limited availability of diagnostic methods such as CBA and mNGS may present practical barriers to conducting such multicenter follow-up studies and hinder broader clinical adoption. Despite these limitations, this study represents the first effort to create a reliable prediction tool for ICU admission risk in A-GFAP-A patients.
In conclusion, clinical factors included GCS at admission, seizures, maximum temperature, and CRP are crucial for predicting ICU admission risk in A-GFAP-A patients. The nomogram and decision tree models presented here are practical tools that enhance prediction accuracy and are easy to apply in clinical settings. These models offer significant benefits for improving patient outcomes by enabling earlier and more targeted interventions.
Data Sharing Statement
The data used during the study are available on reasonable request. Further inquiries can be directed to the corresponding authors.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant no. 82405071, 82071265) and Guangdong Basic and Applied Basic Research Foundation (grant no. 2021A1515110231, 2023A1515110505).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fang B, McKeon A, Hinson SR. et al. Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: a Novel Meningoencephalomyelitis. JAMA Neurol. 2016;73(11):1297–1307. doi:10.1001/jamaneurol.2016.2549
2. Flanagan EP, Hinson SR, Lennon VA, et al. Glial fibrillary acidic protein immunoglobulin G as biomarker of autoimmune astrocytopathy: analysis of 102 patients. Ann Neurol. 2017;81(2):298–309. doi:10.1002/ana.24881
3. Shan F, Long Y, Qiu W. Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: a Review of the Literature. Front Immunol. 2018;9:2802. doi:10.3389/fimmu.2018.02802
4. Theuriet J, Cluse F, Gravier-Dumonceau A, et al. Peripheral nervous system involvement accompanies central nervous system involvement in anti-glial fibrillary acidic protein (GFAP) antibody-related disease. J Neurol. 2023;270(11):5545–5560. doi:10.1007/s00415-023-11908-7
5. Allen A, Gulhar S, Haidari R, et al. Autoimmune glial fibrillary acidic protein astrocytopathy resulting in treatment-refractory flaccid paralysis. Mult Scler Relat Disord. 2020;39:101924. doi:10.1016/j.msard.2019.101924
6. Savaş M, Tzartos J, Küçükali C, et al. Glial fibrillary acidic protein (GFAP)-antibody in children with focal seizures of undetermined cause. Acta Neurol Belg. 2021;121(5):1275–1280. doi:10.1007/s13760-020-01361-y
7. Tsikopoulos I, Antoniadis G, Sakalis V, et al. Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: the Role of a Neurourogist From the Intensive Care Unit to Improving the Patient’s Quality of Life. Cureus. 2024;16(8):e67903. doi:10.7759/cureus.67903
8. Ip B, Lam C, Ip V, et al. Autoimmune glial fibillary acidic protein astrocytopathy associated meningoencephalomyelitis and bilateral sensorineuronal deafness. Mult Scler Relat Disord. 2020;40:101922. doi:10.1016/j.msard.2019.101922
9. Yang X, Liang J, Huang Q, et al. Treatment of Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy: follow-Up in 7 Cases. Neuroimmunomodulation. 2017;24(2):113–119. doi:10.1159/000479948
10. Li J, Wang C, Cao Y, et al. Autoimmune glial fibrillary acidic protein astrocytopathy mimicking acute disseminated encephalomyelitis: a case report. Medicine. 2021;100(25):e26448. doi:10.1097/MD.0000000000026448
11. Héraud C, Capet N, Levraut M, et al. Glial Fibrillary Acidic Protein (GFAP) Astrocytopathy Presenting as Mild Encephalopathy with Reversible Splenium Lesion. Neurol Ther. 2022;11(1):499–505. doi:10.1007/s40120-021-00302-y
12. Wu C, Fang Y, Zhou Y, et al. Risk Prediction Models for Early ICU Admission in Patients With Autoimmune Encephalitis: integrating Scale-Based Assessments of the Disease Severity. Front Immunol. 2022;13:916111. doi:10.3389/fimmu.2022.916111
13. Waqar U, Arshad A, Ayaz A, et al. Risk factors for intensive care unit admission and mortality among adult meningitis patients. J Pak Med Assoc. 2022;72(7):1460–1466. doi:10.47391/JPMA.4482
14. Huang J, Huang W, Zhou R, et al. Detection and significance of glial fibrillary acidic protein antibody in autoimmune astocytopathy and related diseases. Ann Transl Med. 2023;11(7):288. doi:10.21037/atm-19-330
15. Xu X, Su X, Xu L, et al. Impaired glymphatic function in autoimmune glial fibrillary acidic protein astrocytopathy: a prospective analysis. Mult Scler Relat Disord. 2025;99:106447. doi:10.1016/j.msard.2025.106447
16. Long Y, Liang J, Xu H, et al. Autoimmune glial fibrillary acidic protein astrocytopathy in Chinese patients: a retrospective study. Eur J Neurol. 2018;25(3):477–483. doi:10.1111/ene.13531
17. Su X, Li W, Liu J, et al. Comparison of features and outcomes between HIV-negative patients with Cryptococcus gattii meningitis and Cryptococcus neoformans meningitis in South China. Mycoses. 2022;65(9):887–896. doi:10.1111/myc.13491
18. Chen X, Zhang H, Guo D, et al. Risk of intraoperative hemorrhage during cesarean scar ectopic pregnancy surgery: development and validation of an interpretable machine learning prediction model. EClinMed. 2024;78:102969. doi:10.1016/j.eclinm.2024.102969
19. Huang J, Tsai Y, Wu P, et al. Predictive modeling of blood pressure during hemodialysis: a comparison of linear model, random forest, support vector regression, XGBoost, LASSO regression and ensemble method. Comput Methods Programs Biomed. 2020;195:105536. doi:10.1016/j.cmpb.2020.105536
20. Hagbohm C, Ouellette R, Flanagan EP, et al. Clinical and neuroimaging phenotypes of autoimmune glial fibrillary acidic protein astrocytopathy: a systematic review and meta-analysis. Eur J Neurol. 2024;31(7):e16284. doi:10.1111/ene.16284
21. Lan W, Li J, Ai P, et al. Autoimmune glial fibrillary acidic protein astrocytopathy: clinical analysis and review of 15 cases. Acta Neurol Belg. 2023;123(4):1465–1479. doi:10.1007/s13760-023-02268-0
22. Li T, Li X, Hong S, et al. Clinical characteristics of autoimmune glial fibrillary acidic protein (GFAP) astrocytopathy in children: a case series of 16 patients. J Neuroimmunol. 2023;382:578176. doi:10.1016/j.jneuroim.2023.578176
23. Wang J, Tang C, Luo S. Letter to the Editor: a case of autoimmune glial fibrillary acidic protein astrocytopathy with acute paralytic ileus as initial symptom. Neurol Sci. 2024;45(3):1291–1293. doi:10.1007/s10072-023-07136-6
24. Reith FC, Van den Brande R, Synnot A, et al. The reliability of the Glasgow Coma Scale: a systematic review. Intensive Care Med. 2016;42(1):3–15. doi:10.1007/s00134-015-4124-3
25. Lang L, Wang T, Xie L, et al. An independently validated nomogram for individualised estimation of short-term mortality risk among patients with severe traumatic brain injury: a modelling analysis of the CENTER-TBI China Registry Study. EClinMed. 2023;59:101975. doi:10.1016/j.eclinm.2023.101975
26. Kimura A, Takekoshi A, Yoshikura N, et al. Clinical characteristics of autoimmune GFAP astrocytopathy. J Neuroimmunol. 2019;332:91–98. doi:10.1016/j.jneuroim.2019.04.004
27. Wang C, Zhang H, Lu W, et al. The EBV connection: a severe case of GFAP-A with central hypoventilation unresponsive to IVIG and literature review. Eur J Med Res. 2024;29(1):415. doi:10.1186/s40001-024-01926-0
28. Crawshaw AA, Cock HR. Medical management of status epilepticus: emergency room to intensive care unit. Seizure. 2020;75:145–152. doi:10.1016/j.seizure.2019.10.006
29. Yuan F, Damien C, Gaspard N. Severity scores for status epilepticus in the ICU: systemic illness also matters. Crit Care. 2023;27(1):19. doi:10.1186/s13054-022-04276-7
30. Ke G, Jian S, Yang T, et al. Clinical characteristics and MRI features of autoimmune glial fibrillary acidic protein astrocytopathy: a case series of 34 patients. Front Neurol. 2024;15:1375971. doi:10.3389/fneur.2024.1375971
31. Adrogué HJ, Tucker BM, Madias NE. Diagnosis and Management of Hyponatremia: a Review. JAMA. 2022;328(3):280–291. doi:10.1001/jama.2022.11176
32. Chen Y, Luo C, Zhou G, et al. The discrimination between autoimmune glial fibrillary acidic protein astrocytopathy and tuberculous meningitis. Mult Scler Relat Disord. 2024;85:105527. doi:10.1016/j.msard.2024.105527
33. Wang X, Ni L, Wan S, et al. Febrile Temperature Critically Controls the Differentiation and Pathogenicity of T Helper 17 Cells. Immunity. 2020;52(2):328–341. doi:10.1016/j.immuni.2020.01.006
34. Liu Y, Ma L, Ma X, et al. Simple and effective serum biomarkers potential for predicting status epilepticus in anti-N-methyl-D-aspartate receptor encephalitis. BMC Neurol. 2022;22(1):27. doi:10.1186/s12883-021-02545-6
35. Lin J, Xiang Q, Liu X, et al. Risk Factors and Prognosis in Patients With Anti-N-Methyl-D-Aspartate Receptor Encephalitis Requiring Prolonged Mechanical Ventilation. Front Neurol. 2022;13:814673.
36. Li XL, Wang JY, Li LK, et al. Epstein-Barr virus: to be a trigger of autoimmune glial fibrillary acidic protein astrocytopathy? CNS Neurosci Ther. 2023;29(12):4139–4146. doi:10.1111/cns.14336
37. Zhang JR, Zhuang S, Xu XD, et al. Overlapping Epstein-Barr virus encephalitis and autoimmune glial fibrillary acidic protein astrocytopathy. J Neuroimmunol. 2023;382:578174. doi:10.1016/j.jneuroim.2023.578174
38. Liu J, Luo C, Li M, et al. Predictors of postinfectious inflammatory response syndrome in HIV-negative immunocompetent cryptococcal meningitis. J Neurol Neurosurg Psychiatry. 2020;2020:1.
39. Brummel NE, Hughes CG, McNeil JB, et al. Systemic inflammation and delirium during critical illness. Intensive Care Med. 2024;50(5):687–696. doi:10.1007/s00134-024-07388-6
40. Bitar R, Khan UM, Rosenthal ES. Utility and rationale for continuous EEG monitoring: a primer for the general intensivist. Crit Care. 2024;28(1):244. doi:10.1186/s13054-024-04986-0
41. Wagner AS, Baumann SM, Semmlack S, et al. Comparing Patients With Isolated Seizures and Status Epilepticus in Intensive Care Units: an Observational Cohort Study. Neurology. 2023;100(17):e1763–e1775. doi:10.1212/WNL.0000000000206838
42. Di Rosa M, Sabbatinelli J, Giuliani A, et al. Inflammation scores based on C-reactive protein and albumin predict mortality in hospitalized older patients independent of the admission diagnosis. Immun Ageing. 2024;21(1):67. doi:10.1186/s12979-024-00471-y
43. Baran JM, Porębska A, Lesisz M, et al. Investigating Blood Biomarkers That Can Facilitate the Diagnosis of Meningitis-A Systematic Literature Review. Int J Mol Sci. 2025;26(4):1427. doi:10.3390/ijms26041427.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation Nomogram for Predicting the Survival of Patients with Thrombocytopenia in Intensive Care Units
Jiang ZH, Zhang GH, Xia JM, Lv SJ
Risk Management and Healthcare Policy 2023, 16:1287-1295
Published Date: 17 July 2023
A Retrospective Cohort Study: Predicting 90-Day Mortality for ICU Trauma Patients with a Machine Learning Algorithm Using XGBoost Using MIMIC-III Database
Yang S, Cao L, Zhou Y, Hu C
Journal of Multidisciplinary Healthcare 2023, 16:2625-2640
Published Date: 6 September 2023
Dynamic Nomogram for Subsyndromal Delirium in Adult Intensive Care Unit: A Prospective Cohort Study
Cheng J, Lao Y, Chen X, Qiao X, Sui W, Gong X, Zhuang Y
Neuropsychiatric Disease and Treatment 2023, 19:2535-2548
Published Date: 22 November 2023
Development and Validation of an ICU-Venous Thromboembolism Prediction Model Using Machine Learning Approaches: A Multicenter Study
Jin J, Lu J, Su X, Xiong Y, Ma S, Kong Y, Xu H
International Journal of General Medicine 2024, 17:3279-3292
Published Date: 24 July 2024
Analysis of Risk Factors and Development of a Predictive Model for Delirium in ICU Patients: Construction, Validation, and Clinical Implications
Li X, Zhang W, Wang T, Qiu Z, Sun X, Qu W, Zhang G
International Journal of General Medicine 2025, 18:3727-3737
Published Date: 5 July 2025