Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Life Engagement Improvement Following Initiation of Brexpiprazole Treatment in Patients with MDD: A Naturalistic, Retrospective Real-World Study
Authors Wee SN, Liman C ![]() , Waters HC
, Waters HC ![]() , Houle CR, Renteria M
, Houle CR, Renteria M ![]() , Mukherjee SS
, Mukherjee SS ![]() , Surendran S, Marcovici J, Brubaker M, Rasmussen Meehan S, de Jong-Laird A, Rush AJ
, Surendran S, Marcovici J, Brubaker M, Rasmussen Meehan S, de Jong-Laird A, Rush AJ ![]() , Sarkar J
, Sarkar J
Received 16 November 2022
Accepted for publication 4 March 2023
Published 18 March 2023 Volume 2023:15 Pages 195—208
DOI https://doi.org/10.2147/CEOR.S395255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Soon Nan Wee,1,* Christian Liman,1,* Heidi C Waters,2 Christy R Houle,3 Miguel Renteria,1 Sankha S Mukherjee,1 Subina Surendran,1 Joshua Marcovici,1 Malaak Brubaker,2 Stine Rasmussen Meehan,4 Anne de Jong-Laird,2 A John Rush,5– 7 Joydeep Sarkar1
1Holmusk Technologies, Inc, New York, NY, USA; 2Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, NJ, USA; 3Lundbeck, Deerfield, IL, USA; 4H. Lundbeck A/S, Valby, Denmark; 5Department of Psychiatry, Duke-National University of Singapore, Singapore, Singapore; 6Department of Psychiatry, Duke University School of Medicine, Durham, NC, USA; 7Health Sciences Center, Texas Tech University, Odessa, TX, USA
*These authors contributed equally to this work
Correspondence: Heidi C Waters, Otsuka Pharmaceutical Development & Commercialization, Inc, 508 Carnegie Center Drive, Princeton, NJ, 08540, USA, Tel +1 609 535 9626, Email [email protected]
Purpose: Life engagement encompasses concepts such as life fulfillment, well-being, and participation in meaningful activities, encompassing cognitive, physical, social, and emotional dimensions. Patients with MDD experience impaired functioning across multiple domains of life engagement and have ranked concepts related to life engagement and fulfillment as important predictors of treatment success. Post-hoc analyses of three clinical trials of patients with MDD treated adjunctively with brexpiprazole have reported a significantly greater improvement in life engagement. This study investigated improvements in life engagement among patients with MDD following initiation of brexpiprazole treatment using a real-world dataset.
Patients and Methods: Information was extracted from semi-structured clinical notes of the Mental Status Examination (MSE) of patients in a real-world setting to develop an outcome measure for quantifying life engagement of psychiatric patients. Measures of life engagement and its four sub-domains (emotional, physical, social, and cognitive) were calculated at each clinical visit for 624 adult patients with MDD during the 6 months following brexpiprazole initiation. Paired t-tests assessed differences between the index event and time periods within 6 months of the index event. Kaplan–Meier survival analyses were used to quantify the improvement in life engagement scores following brexpiprazole initiation.
Results: The study identified 54 clinical features associated with life engagement. Statistically significant improvements were observed from as early as 1 month following brexpiprazole initiation, with 20.6%, 37.9%, and 53.9% of the patients demonstrating improved life engagement scores within 1, 3, and 6 months, respectively. The improvements were particularly apparent for the emotional and social sub-domains.
Conclusion: The results of this study provide evidence of improved life engagement following brexpiprazole initiation in a real-world dataset.
Keywords: brexpiprazole, major depressive disorder, real-world evidence, mental status examination, life engagement
Introduction
Major depressive disorder (MDD) is a common mental disorder that affects >6% of the adults in the United States (US).1 It is characterized by persistent sadness and loss of interest, negatively affecting how a person feels, thinks, and behaves, and leading to various emotional and physical problems.2,3 Patients with MDD typically experience impaired functioning across multiple domains, including work, social, and family functioning.4,5 Although numerous antidepressant treatments (ADTs) have established efficacy in treating MDD,6 treatment response in the real world has remained relatively modest and inadequate.7–10 With any first-line treatment, approximately 50% of the patients will respond to treatment (defined as a 50% reduction in depression symptoms), and about 20–30% of those will achieve full remission.7 Not achieving disease remission has been associated with a higher risk of relapse, impairment in social and work functioning, and a worse long-term prognosis.7 In such cases, treatment may be augmented via adjunctive therapy. Treatment augmentation with an atypical antipsychotic is a strategy that has shown considerable success in patients with inadequate response.11
Brexpiprazole is an atypical antipsychotic approved as adjunctive therapy to ADT to treat MDD in the United States and several other countries.12 Results from Phase 3 trials and open-label studies in patients with MDD have demonstrated improvements in efficacy and safety endpoints, including the Montgomery–Åsberg Depression Rating Scale (MADRS) total score and Sheehan Disability Scale (SDS), within 6–12 weeks from adjunctive brexpiprazole initiation.13–16
While many clinical trials on adjunctive antipsychotics and ADTs are evaluated using clinician-rated depressive symptom scales,6,17 there is an increasing drive towards patient-reported outcomes (PROs) in clinical research, which may capture meaningful information such as quality of life.18,19 From a patient’s perspective, treatment may help the patient regain optimism and self-confidence, return to their usual self and premorbid levels of functioning.20 The Inventory of Depressive Symptomatology Self-Report (IDS-SR) is a 30-item rating scale of depressive symptoms often used in clinical trials.21
Life engagement encompasses concepts such as life fulfillment, well-being, and participation in valued and meaningful activities.22,23 Life engagement includes cognitive, physical, social, and emotional dimensions.22 Previous research has demonstrated an association between purposeful life engagement and health benefits among older adults, such as extended longevity and reduced risk for various disease outcomes.23 In MDD, there is an unmet need for treatments that can help patients achieve their desired outcomes,24 including improved life engagement. Patients with MDD ranked concepts related to life engagement and fulfillment as some of the most important predictors of treatment success,25 and symptoms related to lack of life engagement such as loss of interest in things and lack of motivation are often the catalyst for treatment of depression.26 As such, assessing the efficacy of a treatment in improving life engagement would be valuable.
Post hoc analyses of three clinical trials of patients with MDD treated adjunctively with brexpiprazole have reported a significantly greater improvement in IDS-SR10 Life Engagement score, derived from the components of the Inventory of Depressive Symptomatology Self-Report (IDS-SR),21 in patients with adjunctive brexpiprazole within 6 weeks of treatment, compared with a placebo.27 However, there remains an evidence gap about the effect of brexpiprazole on life engagement in the real-world setting. Moreover, while clinical trials can provide insights on the efficacy of a drug from a controlled environment with low confounding effects, patients participating in clinical trials may not be representative of patients in the real world, especially in outcomes associated with daily life, such as life engagement.28
We recently developed a novel approach based on natural language processing (NLP) to extract information from patient status assessments in a semi-structured format and convert it into a structured, quantifiable format. This approach enhances the structured data stored within EHR systems.29 This methodology was applied to a set of clinical notes known as the Mental Status Examination (MSE).30,31 The MSE is a fundamental component of psychiatric assessment and is designed to evaluate a patient’s mental and emotional functioning. It involves a combination of subjective and objective evaluations, including assessments of the patient’s symptoms and behaviors, as well as evaluations of their appearance, behavior, mood, thought process, speech, memory, and cognitive abilities. The MSE serves as a tool for collecting information about a patient’s mental state, and it aids in the diagnosis of mental disorders and the development of treatment plans. In our recent publication, we demonstrate several applications of the derived clinical information contained within the MSE assessments in the EHR, including disease phenotyping, characterization of suicidality symptoms, and inference of diagnoses.29
The current study utilized real-world clinical information obtained from the MSE and processed using NLP models to obtain quantifiable psychiatry-relevant outcome measures over time. We specifically created “life engagement scores” to quantify and evaluate the life engagement outcomes of adult patients with MDD who received brexpiprazole as adjunctive therapy to ADT between 2014 and 2020. This is the first study of real-world data to assess the impact of brexpiprazole on the concept of life engagement using clinician-captured data rather than scales used in clinical trials and enhances understanding of the benefits to a patient’s quality of life beyond the standard clinical measures. It also informs the development of more personalized and targeted therapies that can positively impact individual patients in the long term.
Materials and Methods
Study Design
We conducted a retrospective study on adult patients with MDD to define and quantify a life engagement score based on clinical information collected at real-world psychiatry practices. We further leveraged these life engagement scores to assess the change within 6 months following the initiation of brexpiprazole as adjunctive therapy to ADT.
Data Source
Data were obtained from NeuroDB Version 20R1, a research-grade real-world dataset aggregated through the MindLinc EHR system and available within the NeuroBlu platform.32–34 NeuroDB is a repository of longitudinal records from patients with mental health disorders who received care at more than 25 hospitals/care systems in the United States. The database comprises over 20 years of consolidated longitudinal, real-world data for more than 560,000 patients and more than 14 million clinical visits.
Ethical Approval
NeuroDB has been de-identified and normalized into a common data model that conforms with the Observational Health Data Sciences and Informatics (OHDSI) data standards. Institutional review board approval for this study was not required because MindLinc EHR data are anonymized and thus exempt from Health Insurance Portability and Accountability Act (HIPAA) requirements.
NeuroDB contains both demographic and clinical information, including comorbid psychiatric diagnoses, prescribed medications, and outcome measures such as the CGI-S scale [27], a 7-point clinician rating of the severity of the patient’s illness at the time of assessment, and the GAF score,30 a 0–100 scale that measures day-to-day function. In addition, NeuroDB also contains clinical labels derived from the MSE, recorded initially in semi-structured clinical notes, and processed using NLP models. These NLP clinical labels represent the behavioral, mental, and cognitive state of the patient captured during a clinical visit.29
Development of a Life Engagement Score
Various types of information gathered from real-world clinical practice and captured in the electronic health records (EHRs) can be leveraged to estimate life engagement and complement the information reported by patients. In real-world clinical settings, several validated measures are recorded to capture the patients’ condition, such as the Clinical Global Impressions – Severity (CGI-S) scale35 and the Global Assessment of Functioning (GAF) score.36 However, unlike these two measures, life engagement is not routinely and systematically measured in real-world clinical practice. Recently, we introduced a new method to analyze mental health assessments using NLP models. This process converts semi-structured free-text summaries of patient status assessments into a structured and quantifiable format, allowing for effective comparisons between patients and tracking of their mental states over time. With these quantifiable representations, we can monitor the effects of medications at both the individual and population levels.29
In this study, we developed a life engagement score by evaluating the impact of each clinical label derived from the MSE on life engagement. Our findings align with prior research suggesting a connection between engaged life and better outcomes.23 To further understand this connection, we assessed the correlation between each clinical label and the GAF scores, which measure the overall functioning of a person in a real-world clinical setting.36
To maximize the generalizability of our life engagement scores across various clinical presentations, our analyses included all psychiatric patients in NeuroDB with ≥1 record of both MSE and GAF scores recorded during the same visit. From this criterion, 295,068 patients with psychiatric disorders in NeuroDB over 22 years (from January 1999 to August 2020) were selected for the life engagement score development.
Figure 1 illustrates the development process of life engagement scores in the present study. Prior research efforts resulted in the creation of a total of 241 clinical labels derived from the MSE notes using NLP models.31 These clinical labels were further mapped and simplified into 86 dichotomous labels with input from independent clinical psychiatry key opinion leaders (KOLs) (see Supplementary Section S1; Supplementary Tables 1-4).
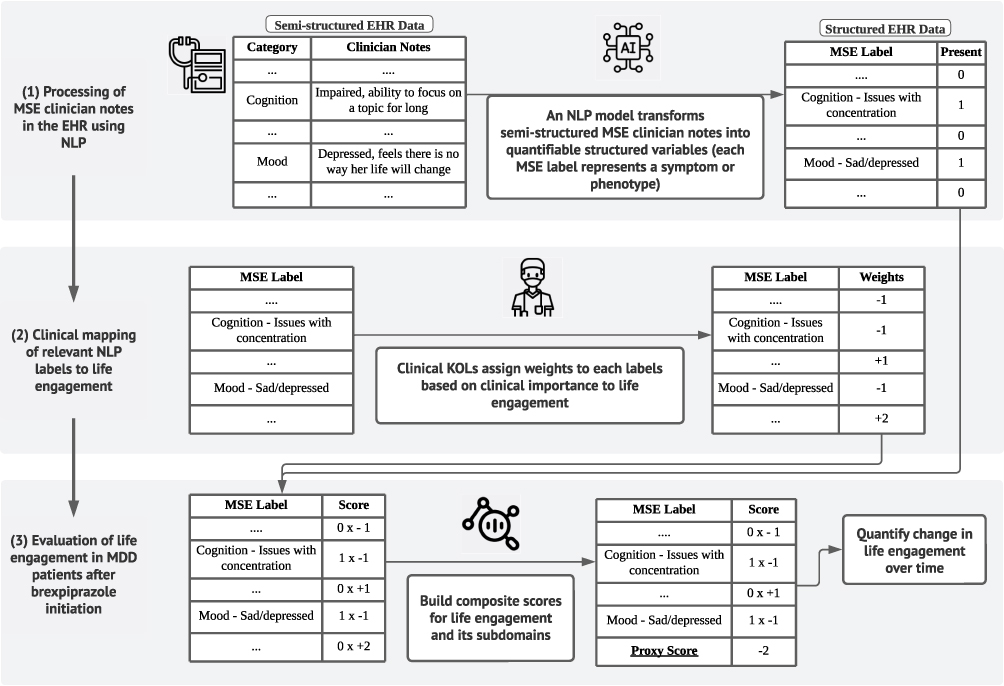 |
Figure 1 Construction of life engagement scores. Notes: The process of creating a life engagement score involved utilizing Natural Language Processing (NLP) to transform unstructured free-text data from the patient’s electronic health records (EHR) into structured variables (NLP labels) representing symptoms, behaviors, or observable phenotypes present in the patient at the time of evaluation. Clinical experts then assigned importance weights to each NLP label based on their clinical significance. The resulting life engagement scores were calculated by combining the relevant NLP labels and quantifying variations in life engagement over time, across multiple clinical visits. |
To identify clinical labels relevant to life engagement, the labels were selected and validated using a combination of clinical input and statistical modeling. First, preliminary work with input from clinical psychiatrists was conducted to identify labels deemed relevant to life engagement based on their clinical estimation. Second, data processing and a series of statistical models were used to further assess the pre-selected labels’ relevance. Bivariate analyses, variance inflation factor (VIF) analyses, and multivariable analyses were conducted to assess correlation with GAF in this real-world dataset and minimize human bias. Both the bivariate and multivariable analyses were performed using linear mixed-effects models (see Supplementary Section S2; Supplementary Figure 1; Supplementary Table 5).37 Finally, the life engagement score was developed using the clinical labels selected through both of the above steps. The score was defined as a weighted sum of the clinical labels relevant to life engagement, hereafter referred to as the life engagement factors. The weights for each life engagement factor were assigned with clinicians’ input based on their perceived positive or negative effect on life engagement.
The study also sought to quantify patient life engagement in four specific domains – emotional, physical, social, and cognitive.38 The four-domain framework was derived from a panel discussion with psychiatrists and a review of transcripts and field notes from exit interviews. The life engagement factors were also mapped into at least one of the four life engagement domains. The weighted sum for the presence of the factors in each domain forms the domain-specific life engagement score.
Study Cohort Selection
The present study focused on adult patients (>18 years old) with a diagnosis of MDD who were prescribed brexpiprazole as adjunctive therapy to ADT. The time of brexpiprazole initiation was defined as the index event. MDD diagnoses were identified using diagnosis codes according to the ICD-9 and ICD-10 codes (see Supplementary Section S3; Supplementary Table 6) [2]. Due to the possibility of patients dropping out of the treatment early due to side effects, which may confound the analysis, only patients who were prescribed brexpiprazole for ≥30 days were included. Due to limitations in how prescription information was recorded in NeuroDB, several approaches were introduced to handle short gaps between subsequent prescriptions. Further information on how such conditions were handled is available in Supplementary Section S4.
As the life engagement score is based on MSE records from which the scores were derived, we only included patients with available MSE records around the index event, defined as the period within 7 days before the index event, including the time of brexpiprazole initiation; and at ≥1 follow-up point(s) within 6 months from the index event. Finally, due to the variability of symptoms and prognosis across different psychiatric disorders, we excluded patients with bipolar disorder, schizophrenia, and other psychotic disorders at any point in time. From these criteria, 624 patients with MDD, hereafter referred to as the study cohort, who had received brexpiprazole as adjunctive therapy to ADT between October 2015 and August 2020 were selected for analysis of life engagement outcomes. Attrition diagrams are shown in Supplementary Section S5; Supplementary Figure 2.
The life engagement score was then constructed as follows. First, bivariate analysis was performed on all clinical labels using a linear regression model against the GAF score measured in the same visit. Clinical labels whose p-values met the significance level of 0.01 were deemed statistically significant and subsequently selected. Second, variance inflation factor (VIF) score was then calculated for each of the remaining labels to identify multicollinearity among the remaining clinical labels. Specifically, clinical labels with high VIF score were excluded. Third, the remaining labels were used as independent variables in the linear mixed-effects (LME) model, with GAF score as the dependent variable. The p-values obtained from the LME model were then identified and used to assess statistical significance after adjustment for confounding factors, for which labels with p-value less than 0.01 were deemed as relevant. These clinical labels then formed the set of clinical labels used in the life engagement score. Weights were assigned to each of these labels based on clinical judgement and interpretation of the labels, ie, whether these labels were believed to have a positive or negative relationship against life engagement.
We leveraged the derived life engagement scores and calculated the change in scores from the index event. A change in the occurrence of a clinical label would change the calculated score. Hence, a reduction in the number of clinical labels associated with worsening in life engagement corresponds to an improvement in the life engagement score. For example, a patient with clinical label of “Mood – Depressed” observed at index event would be deemed as having an improvement in the life engagement score if such label was no longer present at follow-up. Using the change in scores from the index event, we conducted two types of analyses to assess life engagement outcomes associated with brexpiprazole.
Statistical Analyses
Discrete Timepoint Analysis
Paired t-tests were conducted to assess if a statistically significant (α=0.05) change in life engagement scores was observed between the index event and different follow-up time points within 6 months from the index event. We assessed six follow-up time points independently: 1-month, 2-month, 3-month, 4-month, 5-month, and 6-month.
Survival Analysis
A binary endpoint representing an improvement in life engagement score relative to the index event was defined. Following a normalization process designed to account for variations in clinical labels captured by different care systems and clinicians, a life engagement score increase of >0.1 was defined as a significant improvement in life engagement based on data exploration and inputs from clinical psychiatry KOLs. Kaplan–Meier survival analyses were used to quantify the improvement in life engagement scores following brexpiprazole initiation. Both analyses were also performed for the domain-specific life engagement scores. All data processing and analysis were conducted using Python 3.8 (Python Foundation).
Results
Descriptive Statistics
The demographic and clinical characteristics of the 624 patients with MDD are shown in Table 1. Only 67.3% of the patients in the study cohort had ethnicity information recorded in NeuroDB, which is attributable to practice differences in the collection of patients’ sociodemographic information across clinics.
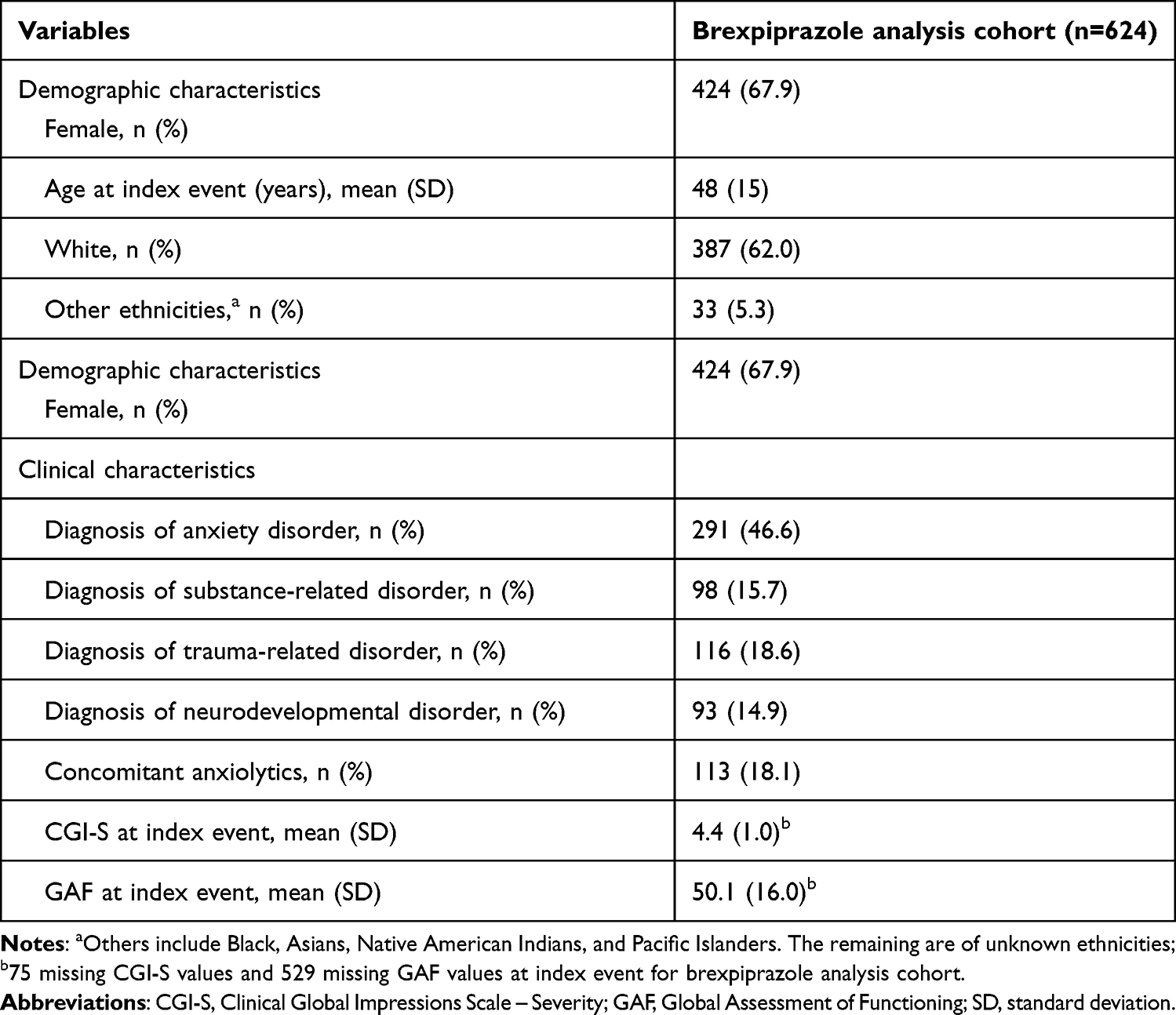 |
Table 1 Demographic and Clinical Characteristics at the Start of Treatment |
Most patients were female (67.9%), white (62.0%), middle-aged (mean age = 48 years). Most patients were diagnosed with comorbid anxiety disorder (46.6%) at the start of treatment. In addition, disease severity of most patients at treatment initiation was moderately severe (mean CGI-S = 4.4) while their quality of life was severely impaired or showed serious symptoms (mean GAF = 50.1).
Life Engagement Scores
Among the 86 clinical labels, 67 were selected by the bivariate analyses. Subsequently, 8 of them were removed due to high multicollinearity with some of the other remaining labels (VIF ≥ 5), and a further five labels were removed due to non-significant correlation with GAF following adjustment of confounding factors.
The 54 life engagement factors selected by the filtering process, with their assigned weights and domain(s) based on the four-domain framework Examples of these labels, assigned into the four domains, are shown in Table 2. A complete list of the 54 clinical labels selected as life engagement factors is given in Supplementary Section S2. Following assessment by clinicians, nine were identified as positive factors, indicating that these factors are associated with better life engagement, whereas 45 were identified as negative factors. The magnitude of the weights assigned to each life engagement factor (hereafter referred to as factors) ranges between 1 and 4, with a larger magnitude indicating a more profound impact on life engagement. Based on the four-domain framework for life engagement, 24 factors were mapped to the cognitive domain, 15 to the emotional domain, 11 to the physical domain, and 9 to the social domain. Out of the 54 life engagement factors, five are mapped to more than one domain, indicating that these factors have a multifaceted impact on life engagement. The derived life engagement score ranges from −60 to 12, with higher scores indicating better life engagement for the patient and vice versa.
 |
Table 2 Summary of Selected Clinical Labels for Life Engagement Score |
Further normalization steps were conducted to maximize generalizability depending on the type of analysis (ie, discrete timepoint analysis or survival analysis). Scores were normalized by the difference between the theoretical maximum and minimum scores prior to normalization, given by the weighted sum associated with the presence of all possible positive and negative factors, respectively. Further details are given in Supplementary Section S6.
Life Engagement Outcomes Analysis
Summary of Life Engagement Scores
At the baseline, patients had, on average, a negative life engagement score, with the cognitive domain displaying the lowest scores across the four domains. In terms of the first change in life engagement score, overall, there was a slight improvement across all domain categories, except for the cognitive domain where a slight decrease was observed. For the variable “maximum change observed across the follow-up period”, a positive change in life engagement scores was generally observed across all domain categories, even after normalization (details available in Table 3).
 |
Table 3 Descriptive Statistics for Baseline, Maximum Change, and First Change in Life Engagement Score |
Discrete Time Point Analysis
Figure 2 illustrates the change in life engagement scores at the cohort level between the index event and several follow-up times within 6 months from the index event. Statistically significant changes in life engagement scores were observed from as early as 1 month after the index event (Mean change = 0.37, SD = 1.73, one-sided p < 0.001). Overall, a general trend of improvement relative to the index event was observed within the first 6 months from the index event, with statistically significant improvements observed at all follow-up times except Month 4 (Mean change at Month 6 = 0.35, SD = 2.07, one-sided p = 0.043).
 |
Figure 2 Comparison of life engagement scores at index event and different follow-up time points. |
Results of analyses for the domain-specific life engagement scores are illustrated in Figure 3. Early improvement was also observed in the emotional (Mean change at Month 1 = 0.23, SD = 1.22, one-sided p < 0.001) and social (Mean change at Month 1 = 0.11, SD = 0.92, one-sided p = 0.012) domains. Moreover, statistically significant improvements were observed in the emotional domain for the first 4 months from the index event (Mean change at Month 4 = 0.24, SD = 1.51, one-sided p = 0.010). While a positive change in the physical domain was observed on a population level, no statistically significant change was observed at all follow-up times except Month 4 (Mean change at Month 4 = 0.11, SD = 0.79, one-sided p = 0.020). No statistically significant change in the cognitive domain was observed at the selected follow-up times.
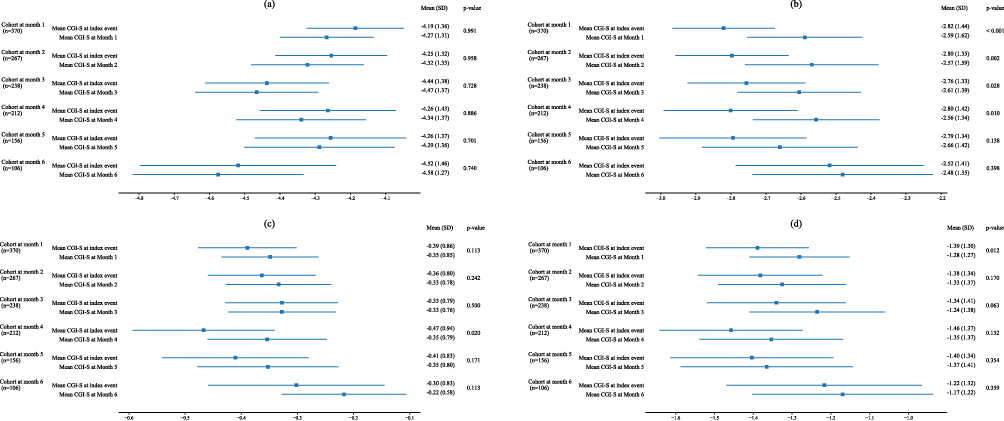 |
Figure 3 Comparison of domain-specific life engagement scores at index event and different follow-up time points: (A) cognitive domain, (B) emotional domain, (C) physical domain, (D) social domain. |
Survival Analysis
Figure 4A illustrates the proportion of patients with or without improving their life engagement scores over time. Within a month from the start of brexpiprazole treatment, 20.6% of the patients demonstrated an improvement in their standardized life engagement score by more than 0.1 (Survival prob. = 0.79; 95% CI [0.76–0.82]). Subsequently, 37.9% (Survival prob. = 0.62; 95% CI [0.58–0.66]) and 53.3% (Survival prob. = 0.47; 95% CI [0.39–0.54]) demonstrated an improvement within the first three and 6 months, respectively.
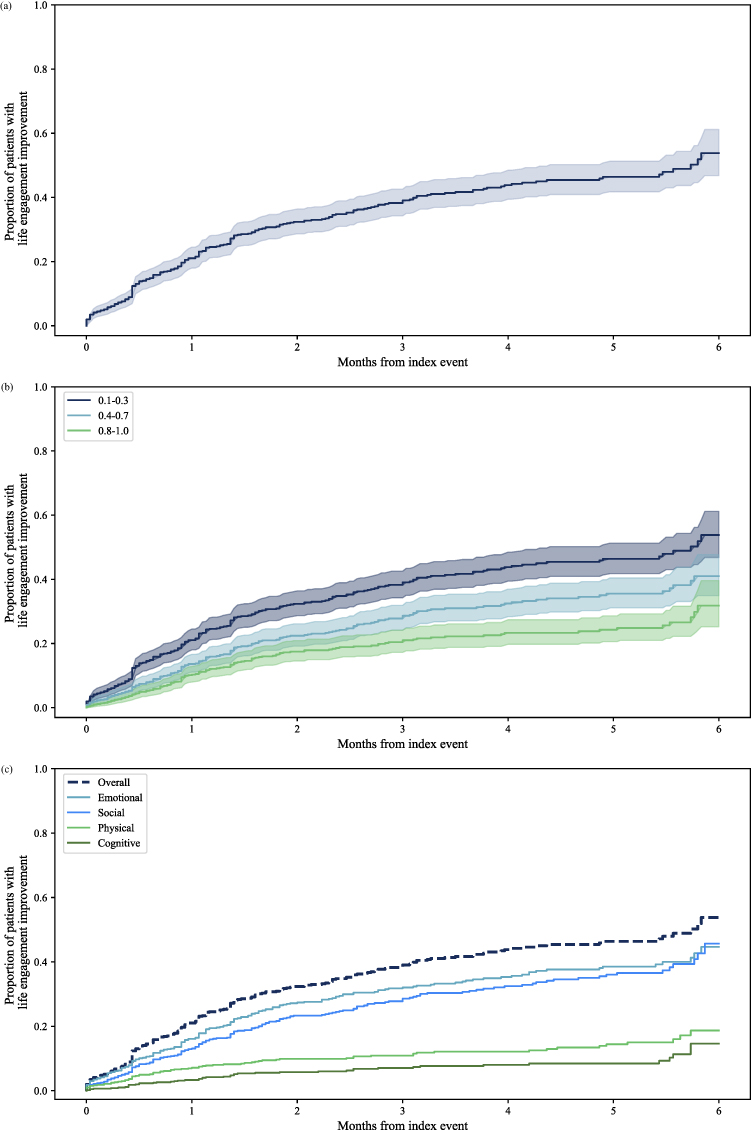 |
Figure 4 Survival analysis for time to life engagement score improvement among brexpiprazole patients (ordered from top to bottom): (A) Cumulative rates of patients with life engagement improvement over time. (B) Cumulative rates of patients with life engagement score improvement over time using different thresholds for life engagement score improvement indicators. (C) Cumulative rates of patients with domain-specific improvement over time. |
We performed an exploratory analysis with cumulative distribution functions to determine the minimum change in life engagement score that could be a significant indicator of life engagement improvement. The cumulative distribution function represents the cumulative proportion of individuals in the group experiencing improvements in life engagement scores over time. We used the same function for thresholds of 0.1 to 0.3, 0.4 to 0.7, and 0.8 to 1.0. Our results (Figure 4B) indicate that even with a much higher threshold of minimum change in life engagement (eg, from 0.8 to 1.0), 31.8% of the patients would still experience an improvement in their life engagement scores. That proportion was 53.3% when the threshold was between 0.1 and 0.3, and 40.9% when the threshold was between 0.4 and 0.7. Therefore, we defined improvement in life engagement score as a change more than 0.1 was used as a significant indicator of life engagement score improvement.
Results for the analysis of domain-specific life engagement scores are shown in Figure 4C. Significant improvements were observed in the emotional and social domains, with 44.5% (Survival prob. = 0.56; 95% CI [0.48–0.62]) and 45.6% (Survival prob. = 0.54; 95% CI [0.45–0.63]) of patients demonstrating an improvement within the first 6 months, respectively. Less profound improvements were observed in the physical (Survival prob. = 0.81; 95% CI [0.75–0.86]) and cognitive (Survival prob. = 0.86; 95% CI [0.79–0.91]) domains within the first 6 months.
Discussion
The present study investigated the life engagement outcomes of 624 patients with MDD who initiated treatment with adjunctive brexpiprazole by leveraging information derived from clinical notes using NLP tools. This was the first study to assess life engagement among a community-dwelling population of patients with MDD prescribed brexpiprazole. More than 50% of the patients with MDD who were prescribed adjunctive brexpiprazole demonstrated an improvement in their life engagement within 6 months, with statistically significant improvement being observed from as early as 1 month from brexpiprazole initiation. Results from sub-domains of life engagement found that emotional and social domains had greater improvements than the physical domain while cognitive domain was maintained.
These findings are consistent with those from three exploratory, short-term, open-label studies on adjunctive brexpiprazole, where 77.1% of the patients described emotional-related improvements,38 and a previous open-label study involving adjunctive brexpiprazole also demonstrated improvements in social functioning, measured by the Social Adaptation Self-Evaluation Scale (SASS), and emotional state, measured by improvement in MADRS.39 In the present study, smaller but significant improvements were observed in the emotional (44.5%) and social (45.6%) domains. Prior research on life engagement has associated the concept with improvements of anhedonia, including both the consummatory and motivational aspects,40 and apathy, which comprises the dimensions of behavior/cognition emotion, and social interaction.41 These aspects have been identified as important treatment targets in depression.42,43
The prior exploratory open-label studies of brexpiprazole also noted a smaller (36.2%) improvement in cognitive-related life functioning.38 Cognitive dysfunction in depression commonly refers to deficits in attention, executive functioning, memory, and processing speed. It has been reported in upwards of 85% of the people with depression, and up to 45% of those who have achieved disease remission.44 Cognitive function has also been shown to improve less with treatment than depressive symptoms; therefore, some cognitive decline may not be reversible despite treatment,44 which would explain the finding of this and prior studies that brexpiprazole does not improve cognitive functioning as much as social or emotional functioning. At baseline in this study, there was very little decrement in physical functioning, so there was not much room for improvement.
Concepts related to life engagement and its subdomains are important to overall functioning in patients with MDD, who have ranked concepts related to life engagement and fulfillment as some of the most important to address through treatment.25 Symptoms related to lack of life engagement such as loss of interest in things and lack of motivation often serve as the impetus for treating depression.26 Treatment response and remission are suboptimal with antidepressants, and not achieving disease remission has been associated with a higher risk of relapse, impairment in social and work functioning, and a worse long-term prognosis.7 It is therefore important for clinicians to monitor treatment success, including the presence of residual symptoms related to life engagement, and change or augment treatment when necessary.
Much of the essential information in real-world psychiatric practice is qualitative and recorded as unstructured free-text clinical notes, which can be challenging to interpret objectively. As a result, many real-world clinical studies have mainly been limited to structured data.45,46 With the MSE being reported in more than three-quarters of patients in NeuroDB, recent advances in artificial intelligence, especially in NLP, provided an opportunity to utilize this information in generating clinical insights. For example, some components of anhedonia and apathy are captured in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for MDD, specifically the markedly diminished interest or pleasure.2 However, some components of apathy, particularly the emotional and behavioral components, are not represented by the DSM-5 criterion. These may be captured by some of the life engagement factors identified in the present study, such as blunted affect, agitation or restlessness, and poor eye contact. A change from presence to absence of these factors may indicate an improvement of apathy, and ultimately, life engagement. The present study demonstrated a framework for leveraging information derived from clinical notes using NLP tools for patient phenotyping, particularly in assessing outcomes like life engagement that lack objective and standardized measures.
Despite the novelty of the approach, this study had several limitations. First, given that the development of the life engagement score required both the MSE record and concomitant GAF score, the identification of life engagement factors was based on a subset (56%) of patients in NeuroDB with recorded GAF scores; therefore, inherent selection bias may have been introduced towards patients with functional impairment. Importantly, there is also a possibility that a proportion of the observed improvement following brexpiprazole initiation is related to regression to the mean phenomenon. Future prospective studies may include a control group to enable a more accurate estimation of the effect size attributable to brexpiprazole treatment. Second, the majority (>83%) of life engagement factors identified were negative factors, for which their presence is associated with worsening in life engagement. As such, the analysis may have been biased towards negative outcomes. However, as scores were graded based on perceived severity, a person’s score could still improve from more to less negative, indicating improvement. Clinical notes rarely contained information about how the severity of the recorded signs or symptoms affected life engagement, so assumptions about severity of the clinical labels were made to develop the grading of severity. Third, information captured by NeuroDB is limited to those recorded by psychiatric-specific hospitals or care systems, which may not necessarily be the complete representation of a patient’s clinical journey, including medications prescribed by primary care providers and number of lifetime MDD episodes. Fourth, unlike most randomized controlled trials where the follow-up visits were fixed and predetermined, follow-up visits in the real world have a high degree of variability, both in terms of the timing and the frequency of the visits, depending on the patient’s condition and response to treatment. Hence, future research needs to also account for the data limitations in real-world clinical practice. Fifth, to account for real-world data variability in obtaining follow-up MSE records, a window of ±7 days was introduced, which was similarly adopted by major studies involving psychiatric patients, including the STAR*D study.46,47 MSE records outside the ±7-day window were excluded from the analysis. As diseases like MDD are episodic in nature, discrete timepoint analysis may create artifacts due to its sensitivity to time-based variations. Moreover, while the scores at different follow-up times were analyzed independently, not all patients in the study cohort were considered at each time point. Lastly, the assessment of life engagement using the four-domain framework was devised based on exit interview transcripts and discussions with psychiatrists. This approach is in line with recent efforts aimed at conceptualizing psychiatric disorders based on dimensions of observable behavior and neurobiological measures, such as those of the National Institute of Mental Health (NIMH) Research Domain Criteria (RDoC) project.48 However, as the four-domain framework has been defined based on an expert panel discussion, further validation of the framework, such as using prospective data collection of validated clinical measures associated with the four domains and gathering feedback from patient perspectives is needed.
Despite these limitations, findings from this study indicate that life engagement improved or maintained following initiation of brexpiprazole as adjunctive treatment for MDD, both in aggregate and across four separate sub-domains. Our findings also suggest that early improvement in life engagement is typically more profound before tapering off over a more extended period. The early improvements observed are consistent with the post-hoc findings from clinical trials involving adjunctive brexpiprazole, which also demonstrated that patients who described improvements in life engagement through their exit interview had a greater improvement in depressive symptoms, global severity, reduced anxiety and irritability, and improved functioning compared to those who did not describe experiencing life engagement improvements.13 Compared to prior research, the present study assessed life engagement improvements associated with brexpiprazole within a more extended follow-up period, which provided insights on the long-term benefit of adjunctive brexpiprazole beyond symptom control. Moreover, life engagement improvements assessed in the present study were observed in patients in real-world settings and observed by clinicians, which may enhance their accuracy by augmenting patients’ observation with clinical observation and judgment. Further research involving brexpiprazole, including characterization of patients who demonstrated improvements in life engagement, could also enhance our understanding of the benefits of brexpiprazole in improving life engagement.
Conclusion
In summary, the present study has demonstrated how real-world data enriched with information derived from NLP models can be leveraged to quantify outcomes that are not systematically measured in clinical practice, such as life engagement, allowing for a more thorough understanding of treatment effectiveness. Analysis showed that more than 50% of the patients prescribed with adjunctive brexpiprazole demonstrated an improvement in their life engagement within 6 months, with statistically significant improvement being observed from as early as 1 month from brexpiprazole initiation. Furthermore, across the four domains of life engagement, emotional- and social-related improvements were the most prominent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Otsuka Pharmaceutical Development & Commercialization, Inc., and H. Lundbeck A/S.
Disclosure
SNW, CL, SSM, SS, JM, MR and JS are employees of Holmusk. AJR is a senior advisor at Holmusk. AJR also reports personal fees from Compass, Inc., Curbstone Consultant LLC, Emmes Corp., Evecxia Therapeutics, Inc., Holmusk Technologies, Inc., ICON, PLC, Johnson and Johnson (Janssen), Liva-Nova, MindStreet, Inc., Neurocrine Biosciences Inc., Otsuka-US, Liva-Nova, and Johnson and Johnson (Janssen); royalties from Wolters Kluwer Health, Guilford Press, and University of Texas Southwestern Medical Center, Dallas, TX, outside the submitted work; In addition, AJR has a patent US 7906283: Methods to Identify Patients at Risk of Developing Adverse Events During Treatment with Antidepressant Medication licensed to The United States of America as represented by the Department of Health and Human Services, Washington, DC (US); Board of Regents, The University of Texas System, Austin, TX (US); a patent US 7795033: Methods to Predict the Outcome of Treatment with Antidepressant Medication licensed to The United States of America as represented by the Department of Health and Human Services, Washington, DC (US); Board of Regents, The University of Texas System, Austin, TX (US). HCW, MB, and ADJL are or were employees of Otsuka Pharmaceutical Development & Commercialization, Inc. at the time of the study. CRH, and SRM are employees of Lundbeck. The authors report no other conflicts of interest in this work.
References
1. National Institute of Mental Health. Major Depression [WWW Document]; 2021. Available from: https://www.nimh.nih.gov/health/statistics/major-depression.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM5®). American Psychiatric Pub; 2013.
3. Otte C, Gold SM, Penninx BW, et al. Major depressive disorder. Nat Rev Dis Primers. 2016;2(1). doi:10.1038/nrdp.2016.65
4. Druss BG, Hwang I, Petukhova M, et al. Impairment in role functioning in mental and chronic medical disorders in the United States: results from the National Comorbidity Survey Replication. Mol Psychiatry. 2009;14:728–737. doi:10.1038/mp.2008.13
5. Kessler RC. The costs of depression. Psyc Clin North Am. 2012;35(1):1–14. doi:10.1016/j.psc.2011.11.005
6. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Focus. 2018;16:420–429. doi:10.1176/appi.focus.16407
7. Olchanski N, Myers MM, Halseth M, et al. The economic burden of treatment-resistant depression. Clin Ther. 2013;35(4):512–522. doi:10.1016/j.clinthera.2012.09.001
8. Papakostas GI, Jackson WC, Rafeyan R, Trivedi MH. Overcoming challenges to treat inadequate response in major depressive disorder. J Clin Psychiatry. 2020;81(3):OT19037BR4. doi:10.4088/JCP.OT19037BR4
9. Papakostas GI, Fava M. Does the probability of receiving placebo influence clinical trial outcome? A meta-regression of double-blind, randomized clinical trials in MDD. Eu Neuropsychopharmacol. 2009;19:34–40. doi:10.1016/j.euroneuro.2008.08.009
10. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163:1905–1917. doi:10.1176/ajp.2006.163.11.1905
11. Connolly KR, Thase ME. If at first you don’t succeed: a review of the evidence for antidepressant augmentation, combination and switching strategies. Drugs. 2011;71:43–64. doi:10.2165/11587620-000000000-00000
12. Eaves S, Rey JA. Brexpiprazole (Rexulti): a new monotherapy for schizophrenia and adjunctive therapy for major depressive disorder. Pharm Therapeutic. 2016;41:418–422. doi:10.1016/j.schres.2015.01.038
13. Thase ME, Zhang P, Weiss C, et al. Efficacy and safety of brexpiprazole as adjunctive treatment in major depressive disorder: overview of four short-term studies. Expert Opin Pharmacother. 2019;20(15):1907–1916. doi:10.1080/14656566.2019.1638913
14. Davis LL, Ota A, Perry P, et al. Adjunctive brexpiprazole in patients with major depressive disorder and anxiety symptoms: an exploratory study. Brain Behav. 2016;6(10):e00520. doi:10.1002/brb3.520
15. Fava M, Okame T, Matsushima Y, et al. Switching from inadequate adjunctive or combination treatment options to brexpiprazole adjunctive to antidepressant: an open-label study on the effects on depressive symptoms and cognitive and physical functioning. Int J Neuropsychopharmacol. 2017;20:22–30. doi:10.1093/ijnp/pyw087
16. Weisler RH, Ota A, Tsuneyoshi K, et al. Brexpiprazole as an adjunctive treatment in young adults with major depressive disorder who are in a school or work environment. J Affective Disorders. 2016;204(1):40–47. doi:10.1016/j.jad.2016.06.001
17. Spielmans GI, Berman MI, Linardatos E, et al. Adjunctive atypical antipsychotic treatment for major depressive disorder: a meta-analysis of depression, quality of life, and safety outcomes. Focus. 2016;2016(14):244–265. doi:10.1176/appi.focus.140202
18. Mercieca-Bebber R, King MT, Calvert MJ, et al. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–367. doi:10.2147/PROM.S156279
19. Weldring T, Smith SMS. Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs). Health Serv Insights. 2013;6:61–68. doi:10.4137/HSI.S11093
20. Zimmerman M, McGlinchey JB, Posternak MA, et al. How should remission from depression be defined? The depressed patient’s perspective. Am J Psychiatry. 2006;163(1):148–150. doi:10.1176/appi.ajp.163.1.148
21. Rush AJ, Giles DE, Schlesser MA, et al. The Inventory for Depressive Symptomatology (IDS): preliminary findings. Psychiatry Res. 1986;18(1):65–87. doi:10.1016/0165-1781(86)90060-0
22. Bartrés-Faz D, Cattaneo G, Solana J, et al. Meaning in life: resilience beyond reserve. Alzheimers Res Ther. 2018;10:1–10.
23. Ryff CD, Heller AS, Schaefer SM, et al. Purposeful engagement, healthy aging, and the brain. Curr Behav Neurosci Rep. 2016;3(4):318–327. doi:10.1007/s40473-016-0096-z
24. McIntyre R, Gill H. The Unmet Needs for Major Depressive Disorder. In: Pompili M, McIntyre R, Fiorillo A, Sartoriu N editors. New Directions in Psychiatry. Springer, Cham;2020. doi:10.1007/978-3-030-42637-8_3
25. Demyttenaere K, Donneau AF, Albert A, Ansseau M, Constant E, Van Heeringen K. What is important in being cured from depression? Discordance between physicians and patients. J Affective Disorders. 2015;174:390–396. doi:10.1016/j.jad.2014.12.004
26. McIntyre RS, Weller E. Real-world determinants of adjunctive antipsychotic prescribing for patients with major depressive disorder and inadequate response to antidepressants: a case review study. Adv Ther. 2015;10(1):47.
27. Thase ME, Pedersen AM, Ismail Z, et al. Efficacy of adjunctive brexpiprazole in adults with MDD: improvement of patient engagement based on selected items from the Inventory of Depressive Symptomatology Self-Report (IDS-SR) scale.
28. Monti S, Grosso V, Todoerti M, et al. Randomized controlled trials and real-world data: differences and similarities to untangle literature data. Rheumatology. 2018;57:vii54–vii58. doi:10.1093/rheumatology/key109
29. Mukherjee SS, Yu J, Won Y, et al. Natural language processing-based quantification of the Mental State of Psychiatric patients. Computational Psychiatry. 2020;2020(4):76–106. doi:10.1162/cpsy_a_00030
30. Koita J, Riggio S, Jagoda A. The Mental Status Examination in emergency practice. Emerg Med Clin North Am. 2010;28(3):439–451. doi:10.1016/j.emc.2010.03.008
31. Walker HK, Hall WD, Hurst JW. Clinical Methods: The History, Physical, and Laboratory Examinations. Butterworth-Heinemann; 1990.
32. Gersing K, Krishnan R. Clinical computing: clinical Management Research Information System (CRIS). Psychiatric Services. 2003;54(9):1199–1200. doi:10.1176/appi.ps.54.9.1199
33. Gersing KR, Krishnan KRR. Practical evidence-based medicine. Psychopharmacol Bull. 2002;36:20–26.
34. Holmusk. NeuroBlu [WWW Document]. NeuroBlu | by Holmusk; 2020. Available from: https://www.neuroblu.ai/.
35. Guy W ECDEU assessment manual for psychopharmacology.
36. Aas IHM. Global Assessment of Functioning (GAF): properties and frontier of current knowledge. Ann Gen Psychiatry. 2010;9(1):1–10. doi:10.1186/1744-859X-9-20
37. Lindstrom MJ, Bates DM. Newton—Raphson and EM algorithms for linear mixed-effects models for repeated-measures data. J Am Statistical Assoc. 1988;83(404):1014–1022.
38. Weiss CA, Meehan SR, Michelle Brown T, et al. Exploring Patient Experiences Taking Adjunctive Brexpiprazole for Major Depressive Disorder (MDD): analysis of Exit Interviews.
39. Lepola U, Hefting N, Zhang D, et al. Adjunctive brexpiprazole for elderly patients with major depressive disorder: an open-label, long-term safety and tolerability study. Int J Geriatr Psychiatry. 2018;33(10):1403–1410. doi:10.1002/gps.4952
40. Treadway MT, Zald DH. Reconsidering anhedonia in depression: lessons from translational neuroscience. Neurosci Biobehav Rev. 2011;35:537–555. doi:10.1016/j.neubiorev.2010.06.006
41. Robert P, Lanctôt KL, Agüera-Ortiz L, et al. Is it time to revise the diagnostic criteria for apathy in brain disorders? The 2018 international consensus group. European Psychiatry. 2018;54:71–76. doi:10.1016/j.eurpsy.2018.07.008
42. Chase TN. Apathy in neuropsychiatric disease: diagnosis, pathophysiology, and treatment. Neurotoxicity Res. 2011;19(2):266–278. doi:10.1007/s12640-010-9196-9
43. Lambert C, Da Silva S, Ceniti AK, et al. Anhedonia in depression and schizophrenia: a transdiagnostic challenge. CNS Neurosci Ther. 2018;24:615–623. doi:10.1111/cns.12854
44. Tayefi M, Ngo P, Chomutare T, et al. Challenges and opportunities beyond structured data in analysis of electronic health records. WIREs Computational Statistics. 2021;13(6):e1549. doi:10.1002/wics.1549
45. Perini G, Ramusino MC, Sinforiani E, Bernini S, Petrachi R, Costa A. Cognitive impairment in depression: recent advances and novel treatments. Neuropsychiatr Dis Treat. 2019;15:1249–1258. doi:10.2147/NDT.S199746
46. Fava M, Rush AJ, Wisniewski SR, et al. A comparison of mirtazapine and nortriptyline following two consecutive failed medication treatments for depressed outpatients: a STAR*D report. Am J Psychiatry. 2006;163:1161–1172. doi:10.1176/ajp.2006.163.7.1161
47. Nierenberg AA, Fava M, Trivedi MH, et al. A comparison of lithium and T3 augmentation following two failed medication treatments for depression: a STAR*D Report. Am J Psychiatry. 2006;163(9):1519–1530. doi:10.1176/ajp.2006.163.9.1519
48. Cuthbert BN, Insel TR. Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med. 2013;11:126. doi:10.1186/1741-7015-11-126
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice in Italy: Results from the RELIEVE Study
De Filippis S, Pugliese A, Christensen MC, Rosso G, Di Nicola M, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1665-1677
Published Date: 9 August 2022
Effectiveness and Safety of Vortioxetine for Major Depressive Disorder in Real-World Clinical Practice: Results from the Single-Arm RELIEVE China Study
Wang G, Xiao L, Ren H, Simonsen K, Ma J, Xu X, Guo P, Wang Z, Bai L, Heldbo Reines E, Hammer-Helmich L
Neuropsychiatric Disease and Treatment 2022, 18:1939-1950
Published Date: 30 August 2022
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice: French Cohort Results from the Global RELIEVE Study
Polosan M, Rabbani M, Christensen MC, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1963-1974
Published Date: 31 August 2022
Long-Term Treatment with Trazodone Once-A-Day (TzOAD) in Patients with MDD: An Observational, Prospective Study
Shrashimirova M, Tyanev I, Cubała WJ, Wichniak A, Vodickova-Borzova C, Ruggieri A, Bonelli A, Lipone P, Comandini A, Cattaneo A
Neuropsychiatric Disease and Treatment 2023, 19:1181-1193
Published Date: 12 May 2023
Real-World Disability Outcomes Among Patients Treated with Cariprazine vs Other Atypical Antipsychotics as Adjunctive Treatment for Major Depressive Disorder
Masand PS, Parikh M, Ta JT, Wade SW, Haile F, Ripley S, Zanardo E, Spencer CS, Laliberté F, Nabulsi N
ClinicoEconomics and Outcomes Research 2025, 17:585-600
Published Date: 28 August 2025