Back to Journals » Clinical Interventions in Aging » Volume 17
Knowledge of Nutrition and Physical Activity Guidelines is Not Associated with Physical Function in Dutch Older Adults Attending a Healthy Ageing Public Engagement Event
Authors Ramsey KA ![]() , Yeung SSY, Rojer AGM, Gensous N, Asamane EA, Aunger JA, Bondarev D, Cabbia A, Doody P, Iadarola B, Rodrigues B, Tahir MR, Kallen V, Pazienza P, Correia Santos N, Sipilä S, Thompson JL, Meskers CGM, Trappenburg MC, Whittaker AC, Maier AB
, Yeung SSY, Rojer AGM, Gensous N, Asamane EA, Aunger JA, Bondarev D, Cabbia A, Doody P, Iadarola B, Rodrigues B, Tahir MR, Kallen V, Pazienza P, Correia Santos N, Sipilä S, Thompson JL, Meskers CGM, Trappenburg MC, Whittaker AC, Maier AB ![]()
Received 19 February 2022
Accepted for publication 6 November 2022
Published 2 December 2022 Volume 2022:17 Pages 1769—1778
DOI https://doi.org/10.2147/CIA.S353573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Keenan A Ramsey,1 Suey SY Yeung,1 Anna GM Rojer,1 Noémie Gensous,2 Evans A Asamane,3 Justin Avery Aunger,3 Dmitriy Bondarev,4 Andrea Cabbia,5 Paul Doody,3 Barbara Iadarola,6,7 Belina Rodrigues,8,9 Muhammad R Tahir,10 Victor Kallen,10 Paola Pazienza,6,7 Nadine Correia Santos,8,9 Sarianna Sipilä,4 Janice L Thompson,3 Carel GM Meskers,1,11 Marijke C Trappenburg,12,13 Anna C Whittaker,15 Andrea B Maier1,14,16,17
1Department of Human Movement Sciences, @AgeAmsterdam, Amsterdam Movement Sciences, Vrije Universiteit, Faculty of Behavioural and Human Movement Sciences, Amsterdam, the Netherlands; 2Department of Experimental, Diagnostic, and Specialty Medicine (DIMES), University of Bologna, Bologna, Italy; 3School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, Birmingham, UK; 4Gerontology Research Center & Faculty of Sport and Health Sciences, University of Jyväskylä, Jyväskylä, Finland; 5Department of Biomedical Engineering, Eindhoven University of Technology, Eindhoven, the Netherlands; 6Personal Genomics s.r.l., Verona, Italy; 7Department of Biotechnology, University of Verona, Verona, Italy; 8Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal; 9ICVS/3B’s, PT Government Associate Laboratory, Guimarães, Portugal; 10Department of Microbiology and System Biology, The Netherlands Organization for Applied Scientific Research, Zeist, the Netherlands; 11Department of Rehabilitation Medicine, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands; 12Department of Internal Medicine, Section of Gerontology and Geriatrics, Amsterdam UMC, Vrije Universiteit Amsterdam, Amsterdam, the Netherlands; 13Department of Internal Medicine, Amstelland Hospital, Amstelveen, the Netherlands; 14Department of Medicine and Aged Care, @Age, The University of Melbourne, The Royal Melbourne Hospital, Parkville, Victoria, Australia; 15Faculty of Health Sciences and Sport, University of Stirling, Scotland, UK; 16Healthy Longevity Translational Research Program, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 17Centre for Healthy Longevity, @AgeSingapore, National University Health System, Singapore
Correspondence: Andrea B Maier, Department of Human Movement Sciences, @AgeAmsterdam, Amsterdam Movement Sciences, Vrije Universiteit, Faculty of Behavioural and Human Movement Sciences, Van der Boechorststraat 7, Amsterdam, 1081 BT, the Netherlands, Tel +31 20 59 82000, Email [email protected]
Purpose: Evidence-based guidelines on nutrition and physical activity are used to increase knowledge in order to promote a healthy lifestyle. However, actual knowledge of guidelines is limited and whether it is associated with health outcomes is unclear.
Participants and Methods: This inception cohort study aimed to investigate the association of knowledge of nutrition and physical activity guidelines with objective measures of physical function and physical activity in community-dwelling older adults attending a public engagement event in Amsterdam, The Netherlands. Knowledge of nutrition and physical activity according to Dutch guidelines was assessed using customized questionnaires. Gait speed and handgrip strength were proxies of physical function and the Minnesota Leisure Time Physical Activity Questionnaire was used to assess physical activity in minutes/week. Linear regression analysis, stratified by gender and adjusted for age, was used to study the association between continuous and categorical knowledge scores with outcomes.
Results: In 106 older adults (mean age=70.1 SD=6.6, years) who were highly educated, well-functioning, and generally healthy, there were distinct knowledge gaps in nutrition and physical activity which did not correlate with one another (R2=0.013, p=0.245). Knowledge of nutrition or physical activity guidelines was not associated with physical function or physical activity. However, before age-adjustment nutrition knowledge was positively associated with HGS in males (B= 0.64 (95% CI: 0.05, 1.22)) and having knowledge above the median was associated with faster gait speed in females (B=0.10 (95% CI: 0.01, 0.19)).
Conclusion: Our findings may represent a ceiling effect of the impact knowledge has on physical function and activity in the this high performing and educated population and that there may be other determinants of behavior leading to health status such as attitude and perception to consider in future studies.
Keywords: health knowledge, attitudes, practice, lifestyle, physical performance, aged
Introduction
Nutrition and physical activity are important domains for healthy ageing.1 However, in older adult populations, the risk of malnutrition is high2 and levels of physical activity are low,3 which are both associated with morbidity,4,5 mortality6,7 and poor physical function.8–11 Evidence-based guidelines are intended to provide the public with information regarding which nutrition and physical activity patterns are associated with health gains and promote a healthy lifestyle.12–14 However, despite their wide dissemination, in older adults, actual knowledge of nutrition and physical activity guidelines seems limited and their implications for health status remain unclear.15,16
Knowledge of nutrition and physical activity may be associated with health outcomes that can be modified by lifestyle such as physical function through physical activity. Previous studies have identified health literacy as a predictor for self-reported physical function.17,18 Health literacy describes one’s capacity to obtain, process, and understand basic health information needed to make appropriate health decisions. Health literacy is therefore a prerequisite for knowledge attainment (eg nutrition and physical activity knowledge), but represents a different and ideological construct (concept) than knowledge.19 Further, self-reported measures of physical function are subject to bias.21 Previous studies assessing knowledge have been inconclusive and evidence in the older adult population using objective measures of physical function is sparse. One study in community-dwelling older adults, using a brief 2-item questionnaire to assess knowledge of physical activity and one objective measure of physical function (chair stand test) reported the absence of an association.20 However, given the emphasis on guidelines as a public health tool, the relationship between knowledge of nutrition and physical activity guidelines and objective measures of physical function requires further quantification using more in depth measures of health knowledge including nutrition knowledge and objective measures of physical function representing different functional domains.
This cross-sectional study aimed to investigate the level of knowledge of nutrition and physical activity guidelines and their association with physical activity and objective measures of physical function in an inception cohort of Dutch community-dwelling older adults who attended a public engagement event on healthy ageing.
Materials and Methods
Study Design
This cross-sectional inception cohort included older adults attending a healthy ageing public engagement event, “PANINI: Recipe for becoming older”, on October 1st, 2018 in Amsterdam, The Netherlands and was hosted and delivered by the Physical Activity and Nutritional INfluences In ageing (PANINI) consortium.22 Participants were recruited through email lists from previous research, general practitioners, senior organizations, community centers, and bridge clubs. No exclusion criteria were applied. Data collection began immediately at the start of the event before any educational information regarding healthy ageing was delivered to participants. This study was reviewed and approved by the local ethical committee, The Scientific and Ethical Review Board (VCWE) of the Faculty of Behavior & Movement Sciences, VU University Amsterdam (VCWE-2018-128), and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki. All participants gave written informed consent.
Participant Characteristics
Self-administered questionnaires, developed by the PANINI consortium via the PANINI Toolkit, were used to ascertain age, gender, marital status, education, living situation, medication use, medical history, smoking status, and alcohol use (Supplementary Material). Height was measured to 0.1 centimeters and body mass (weight) was measured to the nearest 0.1 kg using a height and weight measuring system (DS-102; Dong Sahn Jenix Co., Seoul, Korea). Body mass index (BMI) was calculated by dividing the body mass (kg) by height squared (m) and expressed in kg/m2. The Physical Frailty Phenotype was used to determine frailty status and consists of five criteria: weight loss, exhaustion, weakness, slowness, and low physical activity. This tool classifies participants as robust (none of the criteria below threshold), pre-frail (1–2 criteria below threshold), or frail (≥3 criteria below threshold).23
Knowledge Assessment of Dutch Dietary and Dutch Physical Activity Guidelines
Self-administered questionnaires (Supplementary Material) developed by the PANINI consortium were used to assess knowledge and subjective fulfillment of the Dutch dietary guidelines13 and the Dutch physical activity guidelines.14 Both knowledge questionnaires in English were sent to experts in their respective fields to check for accuracy and consistency and piloted in older adults in five different countries, then refined based upon their performance and feedback, and finally translated into Dutch. The questionnaires were designed to contain questions pertaining to knowledge of guidelines, attitudes towards following these guidelines, and evaluations of the outcomes of the healthy behavior through a series of short multiple-choice questions such as: “Do you think the following food products are a good source of protein?” were asked with possible response options, “poultry”, “cheese”, “fruit”, “butter”, and/or “nuts” (multiple answers correct); “What is the recommended maximum amount of salt intake every day to pursue a healthy dietary pattern?” with possible responses “2 grams per day”, “4 grams per day”, “6 grams per day”, or “I don’t know”; “Which of the following activities constitutes moderate intensity physical activity?” with possible responses “watching TV sitting”, “walking at usual pace”, “washing the dishes”, “dancing”, “cycling at a pace that raises your heart rate”, and/or “I don’t know” (multiple answers correct); “How many minutes a week should one participate in moderate physical activity to pursue a healthy lifestyle?” with possible responses “at least 60 minutes per week”, “at least 150 minutes per week”, “at least 300 minutes per week”, and “I don’t know.” Questionnaires were scored based on difficulty by weighting each question based on the frequency of a correct answer. The PANINI nutrition knowledge questionnaire consisted of 11 questions (possible score of 0–36) (Supplementary Material, questions #20–30) and the PANINI physical activity knowledge questionnaire consisted of nine questions (possible score of 0–13) (Supplementary Material, questions #37–45) with higher scores indicating greater knowledge.
Measures of Physical Function and Physical Activity
Gait Speed
Gait speed, a measure of physical function, was assessed by a four-meter walk test where participants were asked to walk a course of five meters at their normal walking speed. Participants were instructed not to slow down before the four-meter line and their fastest time to reach the four-meter line, of two trials, was recorded, expressed in meters per second (m/s) and used for analysis.24
Hand Grip Strength (HGS)
HGS represents a participant’s ability to squeeze a handheld dynamometer (Jamar 5030J1 hand dynamometer; Sammons Preston Rolyan, Bolingbrook, IL, USA) as hard as possible with each hand three times and is a measure of physical function.25 The maximal HGS was recorded in kilograms (kg) and used for analysis.
Physical Activity
Self-reported physical activity was assessed by an adapted version of the short Minnesota Leisure Time Physical Activity Questionnaire.26 Activities were expanded from those on the original questionnaire based on the population (Supplementary Material). The total minutes of physical activity per week (minutes/week) were calculated and used for analysis.
Statistical Analysis
Descriptive statistics for continuous variables were presented as mean and standard deviation (SD) when data were distributed normally or as median interquartile range [IQR] if the data had a skewed distribution. Categorical variables were reported as the sample size/number (n) and the percentage (%) of the total study population. Knowledge scores were assessed continuously and categorized based on the median scores of the nutrition and physical activity questionnaires, respectively, into three groups: knowledge in neither, at least one, or both domain(s) above the median(s). Pearson’s correlation (R) was used to determine the association between nutrition and physical activity knowledge scores and a scatterplot was used to visualize the results. Linear regression analysis was used to study the association between continuous and categorical knowledge scores with each of the three outcomes measures of physical function and physical activity. Results are presented as unstandardized regression coefficients (B) with their 95% confidence interval (95% CI) and p-value, stratified by gender and performed unadjusted (crude model) and adjusted for age (Model 1). All analyses were conducted using SPSS (Statistical Package for the Social Sciences), version 24.0 (SPSS Inc. Chicago, IL, USA). A p-value of less than 0.05 was considered statistically significant.
Results
Participant Characteristics
This study included 106 Dutch older adults, with a mean age of 70.1 (SD 6.6) years. Participants were mostly female (69.8%), independently living (95.2%), and highly educated (83.0%). The majority of participants were classified as robust (81.2%), 18.8% were classified as pre-frail and no participant was classified as frail (Table 1).
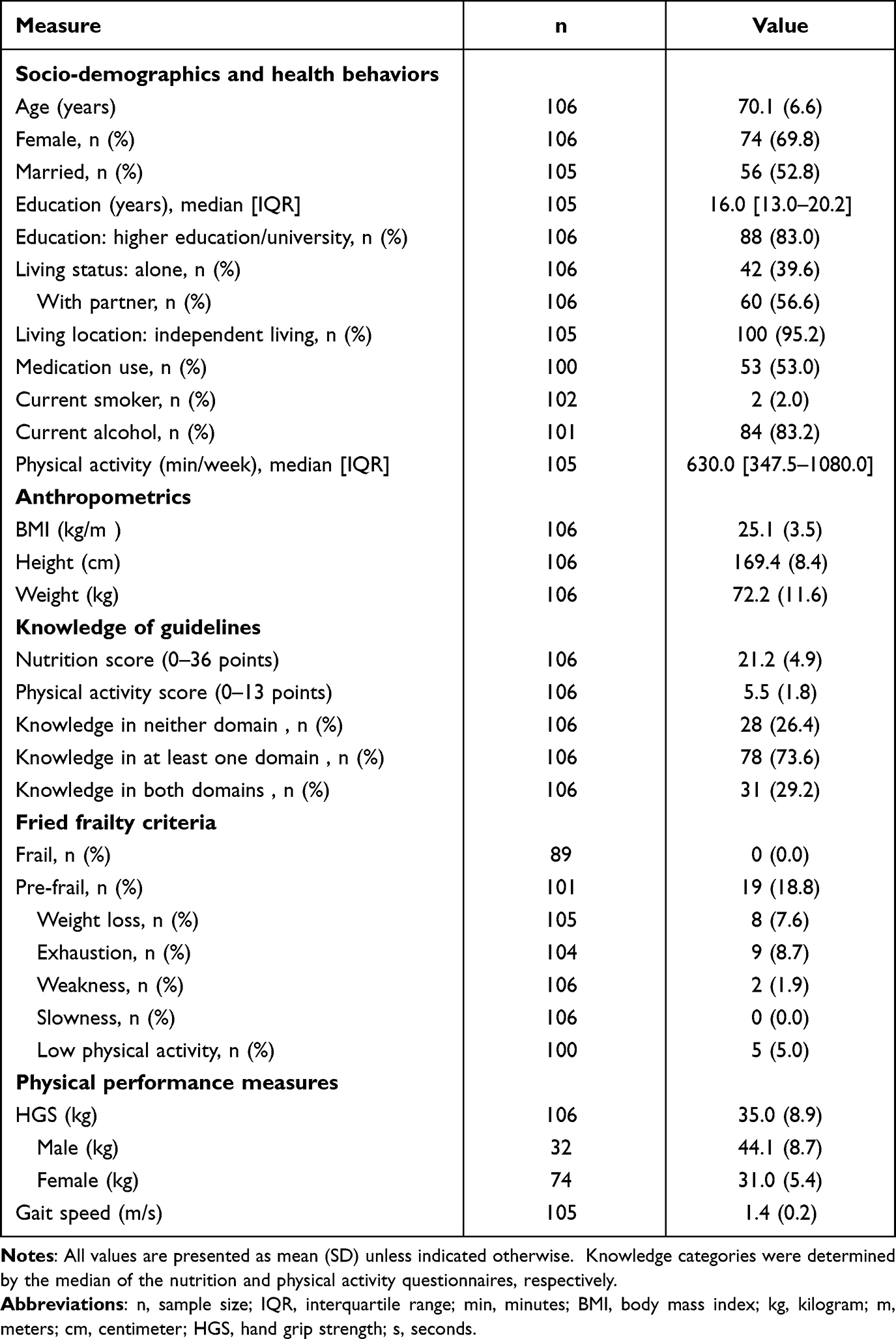 |
Table 1 Participant Characteristics |
Knowledge of Nutrition and Physical Activity Guidelines
Average knowledge scores were 21.2 (SD=4.9) out of 36 points and 5.5 (SD=1.8) out of 13 points for the nutrition and physical activity questionnaires, respectively. On average, 58.9% of nutrition questions were answered correctly, compared to, 42.3% of physical activity questions. Knowledge of nutrition scores and physical activity scores were not significantly associated with each other (R2=0.013, p=0.245) (Figure 1).
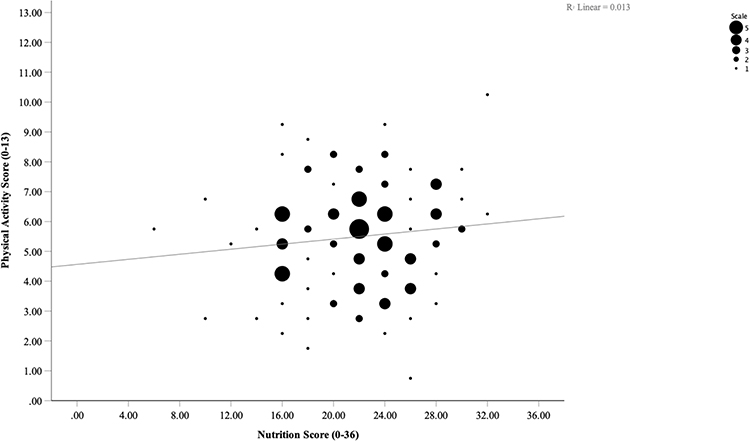 |
Figure 1 Scatterplot of weighted nutrition and physical activity scores. Marker size (scale) represents the number of participants. |
Most participants had knowledge in at least one domain (73.6%), followed by smaller portions having knowledge in both domains (29.2%), and knowledge in neither (26.4%).
Associations of Knowledge with Physical Function and Physical Activity
A significant positive association was found between nutrition knowledge and HGS strength in males before adjustment. A one-unit increase in nutrition score was associated with 0.64 kg (95% CI: 0.05, 1.22; p=0.034) better HGS in males. This association did not persist after adjustment for age and was not present in females. Effect sizes were consistently positive for associations between nutrition knowledge and outcomes gait speed and physical activity and conversely, effect sizes were consistently negative for associations between physical activity knowledge with these outcomes. (Table 2).
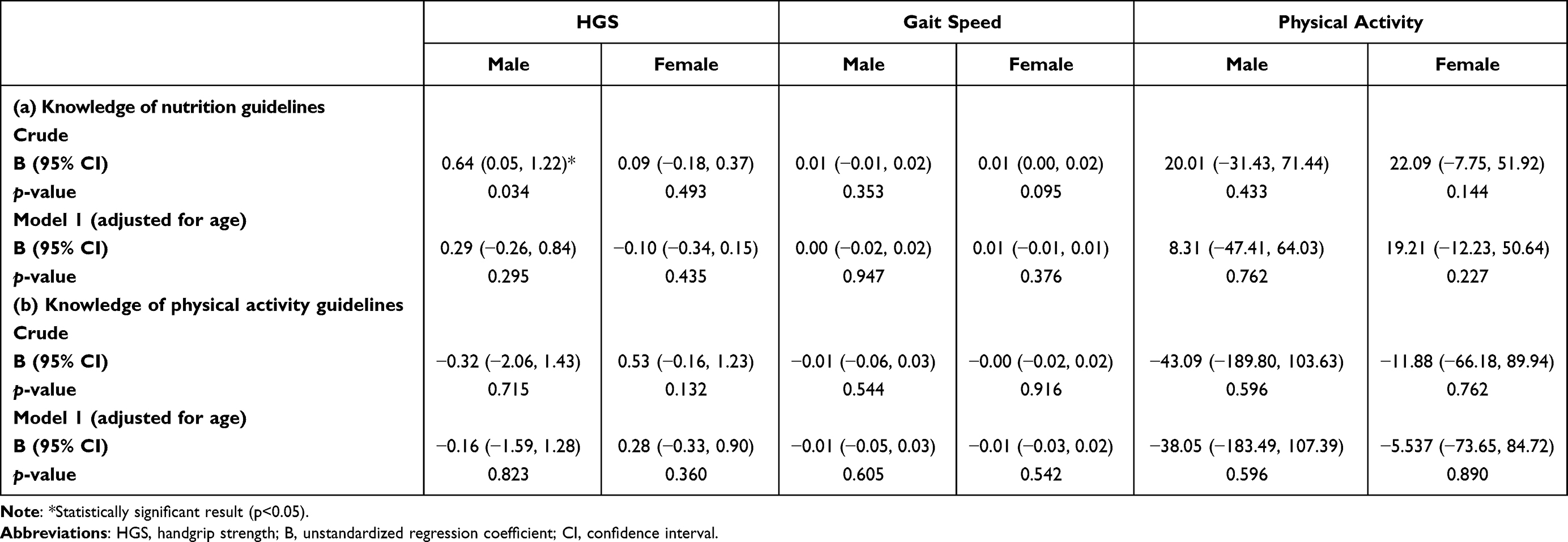 |
Table 2 The Association of Knowledge of (a) Nutrition and (b) Physical Activity Guidelines with Physical Function and Physical Activity |
Similarly, categorical measures of knowledge showed a lack of an association with outcome measures. In females, knowledge in at least one domain was associated with a 0.10 m/s (95% CI: 0.01, 0.19; p=0.044) slower gait speed compared to without knowledge in either domain. After adjustment for age, this association became non-significant. No other significant associations were found (Table 3).
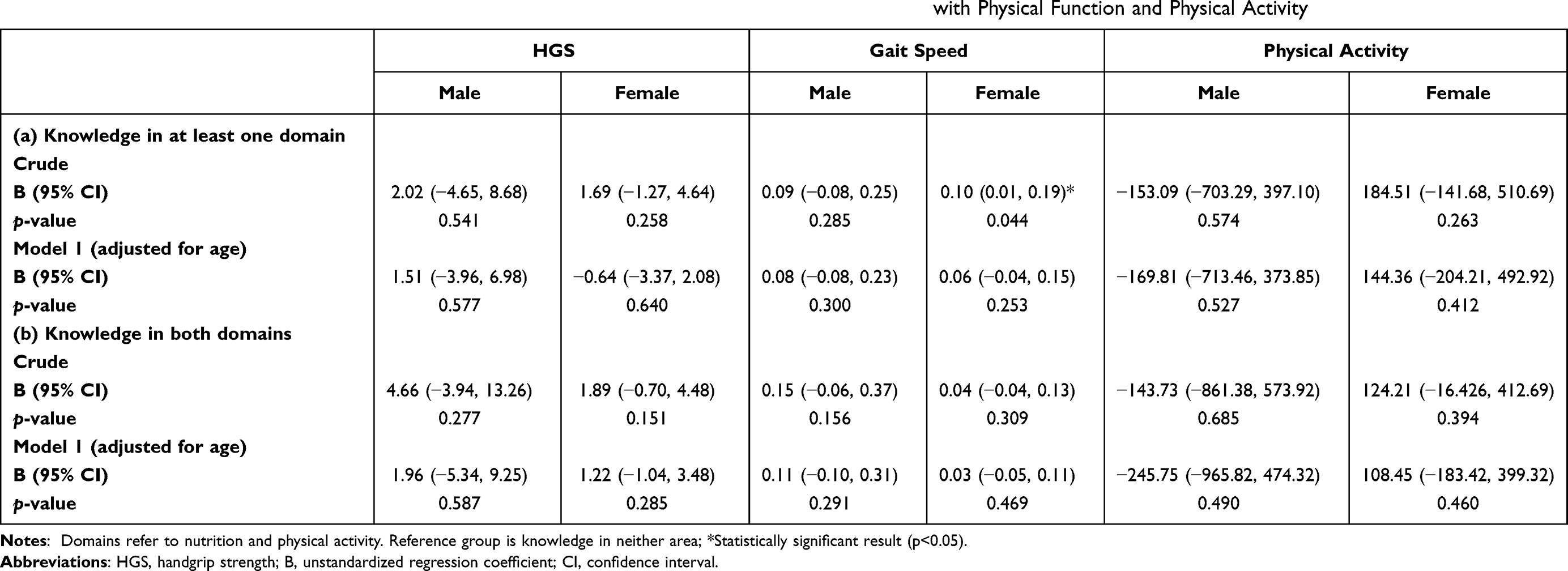 |
Table 3 The Association of Knowledge in (a) at Least One Domain and (b) Knowledge in Both Domainsa with Physical Function and Physical Activity |
Discussion
No significant associations between the knowledge of nutrition or physical activity guidelines were found with objective measures of physical function or physical activity in relatively highly educated and generally healthy Dutch older adults. Knowledge of guidelines in the domains of nutrition and physical activity was limited, indicating the presence of knowledge gaps and thus room to improve knowledge and awareness of guidelines in each domain.
Previous studies in community-dwelling older adults using specific questionnaires to capture knowledge of nutrition or physical activity guidelines, respectively, have had contrasting results compared to the current study.27–31 The discrepancies between these prior studies and the current study may be related to the high levels of physical activity reported in the current population as well as methodological limitations in previous studies including basic assessments of knowledge and issues regarding the validity of the self-reported measures to assess physical function. Although, Cheung et al 2020 used a very brief assessment of knowledge of physical activity guidelines, their study identified non-significant associations with self-reported physical activity and an objective measure of physical function (chair stand test), which is consistent with our results despite the use of different physical performance tests.20
One explanation for the non-significant findings might be that the participants in this study were recruited based on interest in attending a healthy ageing event at a university, which (as we expected) attracted a specific population of participants. There was a overrepresentation of highly educated individuals and there was an absence of frailty in this sample, compared to population estimates of prevalence between 4.0% and 17.0% in community-dwelling older adults.32 Furthermore, gait speed, HGS, and physical activity group scores were well above commonly used cut-off points to screen for poor function and low activity.33–36 Subsequently, the absence of an association found in the present study may be reflective of a ceiling effect with respect to this highly educated, generally healthy and well-performing population that has not been identified in previous studies.
The aim of this study was not to predict physical function from behavior, as it was opportunistic and implemented a cross-sectional design. However, the lack of an association found is supported by health psychology prediction models and theories of health behavior suggesting that beliefs, specifically, attitudes, perceived norms, and perceived control are more important than knowledge alone.20,37 In line with this, the NU-AGE study identified that self-reported physical function was associated with nutrition-related attitudes, but not nutrition-related knowledge.27 Behavioral interventions to improve health status should appropriately address the attitude and perception components that drive health behavior. Further, while physical activity was very high in the current population, it is important to acknowledge that a lack of opportunities and resources for older adults to engage in physical activity represents a barrier, which is important to consider in the context of health behavior and should be a focal point for health promotion efforts.38
This study identified knowledge gaps within a group of highly educated, motivated, and generally healthy individuals, which indicates that knowledge of guidelines should not be assumed to be sufficient and provides direction for public health education. Poor knowledge of guidelines in this population may reflect limited laymen translation and highlight issues regarding accessibility. Despite the lack of an association identified in the current study, older adults should have the knowledge to be able to make healthy decisions. A strength of this study is that no inclusion or exclusion criteria were applied and the use of objective measures of physical function. The small sample represents a limitation to this study and it may also be limited by the use of a customized questionnaire that was not extensively validated.
Conclusion
Despite gaps in knowledge, in an inception cohort of well-functioning and generally healthy Dutch older adults, knowledge of nutrition and physical activity guidelines are not associated with measures of physical activity or objective measures of physical function. These findings strengthen the evidence that limited knowledge of guidelines, as a barrier to healthy lifestyle and outcomes, is not straightforward and may be highly dependent on other factors, such as attitudes, perceptions, resources, and opportunities. Future studies should prioritize these factors and aim to establish the role and capacity for increases in knowledge to synergistically affect lifestyle and health status, while targeting interventions to those who need it most.
Acknowledgments
We would like to thank Stéphanie M.L.M. Looijaard for her contribution to this project. We would like also like to thank all members of the PANINI consortium: Anna C. Whittaker, School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, UK; Evans A. Asamane, School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, UK; Justin Aunger, School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, UK; Kally Bhartti, School of Sport, Exercise & Rehabilitation Science, University of Birmingham, UK; Maria Giulia Bacalini, Institute of Neurological Sciences (IRCCS), Bologna, Italy; Dmitriy Bondarev, Gerontology Research Center & Faculty of Sport and Health Sciences, University of Jyväskylä, Finland; Bart Bongers, Department of Epidemiology, Faculty of Health, Medicine and Life Sciences, Maastricht University, The Netherlands; Andrea Cabbia, Department of Biomedical Engineering, Eindhoven University of Technology, Netherlands; Massimo Delledonne, Personal Genomics, University of Verona, Italy; Paul Doody, School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, UK; Taija Finni, Neuromuscular Research Center, Faculty of Sport and Health Sciences, University of Jyväskylä, Finland; Claudio Franceschi, Department of Experimental, Diagnostic, and Specialty Medicine (DIMES), University of Bologna, Bologna, Italy; Paolo Garagnani, Department of Experimental, Diagnostic, and Specialty Medicine (DIMES), University of Bologna, Bologna, Italy; Noémie Gensous, Department of Experimental, Diagnostic, and Specialty Medicine (DIMES), University of Bologna, Bologna, Italy; Carolyn Greig, School of Sport, Exercise & Rehabilitation Sciences & MRC--Versus Arthritis Centre for Musculoskeletal Ageing Research, University of Birmingham, UK; Peter Hilbers, Department of Biomedical Engineering, Eindhoven University of Technology, The Netherlands; Barbara Iadarola, Personal Genomics, University of Verona, Italy; Victor Kallen, The Netherlands Organisation for Applied Scientific Research, The Netherlands; Katja Kokko, Gerontology Research Center & Faculty of Sport and Health Sciences, University of Jyväskylä, Finland; Anna Elisa Laria, Personal Genomics, University of Verona, Italy; Janet Lord, Institute of Inflammation and Ageing, Medical School & MRC-Arthritis Research UK Centre for Musculoskeletal Ageing Research, University of Birmingham, UK; Andrea B. Maier, Department of Human Movement Sciences, Amsterdam Movement Sciences, VU University Amsterdam, The Netherlands & Department of Medicine and Aged Care, Royal Melbourne Hospital, University of Melbourne, Melbourne, Australia; Carel G.M. Meskers, Department of Rehabilitation Medicine, VU University Medical Center & Amsterdam Movement Sciences, Amsterdam, The Netherlands; Paola Pazienza, Personal Genomics, University of Verona, Italy; Esmee M. Reijnierse, Department of Medicine and Aged Care, Royal Melbourne Hospital, University of Melbourne, Melbourne, Australia; Belina Rodrigues, School of Medicine, University of Minho, Portugal; Nadine Correia Santos, Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, and ICVS/3B’s - PT Government Associate Laboratory, Braga/Guimarães, Portugal; Nuno Sousa, Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, and ICVS/3B’s - PT Government Associate Laboratory, Braga/Guimarães, Portugal; Sarianna Sipila, Gerontology Research Center & Faculty of Sport and Health Sciences, University of Jyväskylä, Finland; Keenan A. Ramsey, Department of Human Movement Sciences, Amsterdam Movement Sciences, VU University Amsterdam, Muhammad Rizwan Tahir; The Netherlands Organisation for Applied Scientific Research, The Netherlands; Marijke C Trappenburg, Department of Internal Medicine, VU University Medical Center & Amstelland Hospital, The Netherlands; Janice L. Thompson, School of Sport, Exercise & Rehabilitation Sciences, University of Birmingham, UK; Nico van Meeteren, Health~Holland, The Hague, & Faculty of Health, Medicine and Life Sciences, Maastricht University, The Netherlands; Natal van Riel, Department of Biomedical Engineering, Eindhoven University of Technology, The Netherlands; Suey Yeung, Department of Human Movement Sciences, Amsterdam Movement Sciences, VU University Amsterdam, The Netherlands.
Disclosure
Professor Janice Thompson reports grants from European Commission, during the conduct of the study. The authors report no conflicts of interest in this work.
References
1. Whittaker AC, Asamane EA, Aunger JA, et al. Physical activity and nutrition influences in ageing: current findings from the PANINI project. Adv Geriatr Med Res. 2019;1:e190005.
2. Rojer AGM, Kruizenga HM, Trappenburg MC, et al. The prevalence of malnutrition according to the new ESPEN definition in four diverse populations. Clin Nutr. 2016;35:758–762. doi:10.1016/j.clnu.2015.06.005
3. Arnardottir NY, Koster A, Van Domelen DR, et al. Objective measurements of daily physical activity patterns and sedentary behaviour in older adults: age, gene/environment susceptibility-Reykjavik study. Age Ageing. 2013;42:222–229. doi:10.1093/ageing/afs160
4. Chan YY, Sooryanarayana R, Mohamad Kasim N, et al. Prevalence and correlates of physical inactivity among older adults in Malaysia: findings from the National Health and Morbidity Survey (NHMS) 2015. Arch Gerontol Geriatr. 2019;81:74–83.
5. Cannella C, Savina C, Donini LM. Nutrition, longevity and behavior. Arch Gerontol Geriatr. 2009;49:19–27.
6. Rojer AGM, Ramsey KA, Trappenburg MC, et al. Instrumented measures of sedentary behaviour and physical activity are associated with mortality in community-dwelling older adults: a systematic review, meta-analysis and meta-regression analysis. Ageing Res Rev. 2020;61:101061.
7. Wang Y-C, Liang C-K, Hsu Y-H, et al. Synergistic effect of low handgrip strength and malnutrition on 4-year all-cause mortality in older males: a prospective longitudinal cohort study. Arch Gerontol Geriatr. 2019;83:217–222.
8. Ramsey KA, Meskers CGM, Trappenburg MC, et al. Malnutrition is associated with dynamic physical performance. Aging Clin Exp Res. 2020;32:1085–1092.
9. Reijnierse EM, Trappenburg MC, Leter MJ, et al. The association between parameters of malnutrition and diagnostic measures of sarcopenia in geriatric outpatients. PLoS One. 2015;10:e0135933.
10. van Rijssen NM, Rojer AGM, Trappenburg MC, et al. Is being malnourished according to the ESPEN definition for malnutrition associated with clinically relevant outcome measures in geriatric outpatients? Eur Geriatr Med. 2018;9:389–394. doi:10.1007/s41999-018-0057-z
11. Ramsey KA, Rojer AGM, D’Andrea L, et al. The association of objectively measured physical activity and sedentary behavior with skeletal muscle strength and muscle power in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2021;67:101266. doi:10.1016/j.arr.2021.101266
12. LeBlanc AG, Berry T, Deshpande S, et al. Knowledge and awareness of Canadian Physical Activity and Sedentary Behaviour Guidelines: a synthesis of existing evidence. Appl Physiol Nutr Metab. 2015;40:716–724. doi:10.1139/apnm-2014-0464
13. Kromhout D, Spaaij CJK, de Goede J, et al. The 2015 Dutch food-based dietary guidelines. Eur J Clin Nutr. 2016;70:869–878. doi:10.1038/ejcn.2016.52
14. Weggemans RM, Backx FJG, Borghouts L, et al. The 2017 Dutch physical activity guidelines. Int J Behav Nutr Phys Act. 2018;15:58. doi:10.1186/s12966-018-0661-9
15. Dickson-Spillmann M, Siegrist M. Consumers’ knowledge of healthy diets and its correlation with dietary behaviour. J Hum Nutr Diet. 2011;24:54–60. doi:10.1111/j.1365-277X.2010.01124.x
16. Cameron C, Craig C, Bull FC, Bauman A. Physical activity guidelines in Canada: has publication had an effect? Appl Physiol Nutr Metab. 2007;32:S179–88. doi:10.1139/H07-160
17. Chesser AK, Keene Woods N, Smothers K, et al. Health literacy and older adults. Gerontol Geriatr Med. 2016;2:233372141663049. doi:10.1177/2333721416630492
18. Berkman ND, Sheridan SL, Donahue KE, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155:97. doi:10.7326/0003-4819-155-2-201107190-00005
19. Gellert P, Tille F. What do we know so far? The role of health knowledge within theories of health literacy. Eur Heal Psychol. 2015;17:266–274.
20. Cheung C, Talley KM, McMahon S, et al. Knowledge of physical activity guidelines and its association with physical activity and physical function in older adults. Act Adapt Aging. 2020;44:106–118.
21. Ryan DJ, Wullems JA, Stebbings GK, et al. Reliability and validity of the international physical activity questionnaire compared to calibrated accelerometer cut-off points in the quantification of sedentary behaviour and physical activity in older adults. PLoS One. 2018;13:1–17. doi:10.1371/journal.pone.0195712
22. Whittaker AC, Delledonne M, Finni T, et al. Physical activity and nutrition influences in ageing (PANINI): consortium mission statement. Aging Clin Exp Res. 2018;30:685–692. doi:10.1007/s40520-017-0823-7
23. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. Journals Gerontol Ser a Biol Sci Med Sci. 2001;56:M146–M57. doi:10.1093/gerona/56.3.M146
24. Pasma JH, Stijntjes M, Ou SS, Blauw GJ, Meskers CGM, Maier AB. Walking speed in elderly outpatients depends on the assessment method. Age. 2014;36:9736. doi:10.1007/s11357-014-9736-y
25. Reijnierse EM, de Jong N, Trappenburg MC, et al. Assessment of maximal handgrip strength: how many attempts are needed? J Cachexia Sarcopenia Muscle. 2017;8:466–474. doi:10.1002/jcsm.12181
26. Richardson MT, Leon AS, Jacobs DR, et al. Comprehensive evaluation of the Minnesota leisure time physical activity questionnaire. J Clin Epidemiol. 1994;47:271–281. doi:10.1016/0895-4356(94)90008-6
27. Jeruszka-Bielak M, Kollajtis-Dolowy A, Santoro A, et al. Are nutrition-related knowledge and attitudes reflected in lifestyle and health among elderly people? A study across five European countries. Front Physiol. 2018;9:994. doi:10.3389/fphys.2018.00994
28. Clark DO. Physical activity and its correlates among urban primary care patients aged 55 years or older. Journals Gerontol. 1999;54:S41–S48.
29. Lian WM, Gan GL, Pin CH, et al. Correlates of leisure-time physical activity in an elderly population in Singapore. Am J Public Health. 1999;89:1578–1580. doi:10.2105/AJPH.89.10.1578
30. Shimada H, Lord SR, Yoshida H, et al. Predictors of cessation of regular leisure-time physical activity in community-dwelling elderly people. Gerontology. 2007;53:293–297. doi:10.1159/000103214
31. Hui SSC, Morrow JR. Level of participation and knowledge of physical activity in Hong Kong Chinese adults and their association with age. J Aging Phys Act. 2001;9:372–385. doi:10.1123/japa.9.4.372
32. Collard RM, Boter H, Schoevers RA, et al. Prevalence of frailty in community-dwelling older persons: a systematic review. J Am Geriatr Soc. 2012;60:1487–1492. doi:10.1111/j.1532-5415.2012.04054.x
33. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing. 2010;39:412–423. doi:10.1093/ageing/afq034
34. McPhee JS, Hogrel JY, Maier AB, et al. Physiological and functional evaluation of healthy young and older men and women: design of the European MyoAge study. Biogerontology. 2013;14:325–337. doi:10.1007/s10522-013-9434-7
35. Beenakker KGM, Ling CH, Meskers CGM, et al. Patterns of muscle strength loss with age in the general population and patients with a chronic inflammatory state. Ageing Res Rev. 2010;9:431–436. doi:10.1016/j.arr.2010.05.005
36. Sun F, Norman IJ, While AE. Physical activity in older people: a systematic review. BMC Public Health. 2013;13. doi:10.1186/1471-2458-13-449
37. Montaño DE, Kasprzyk D. Theory of reasoned action, theory of planned behavior, and the integrated behavioral model. In: Health Behavior: Theory, Research and Practice.
38. Milton K, Bauman AE, Faulkner G, et al. Maximising the impact of global and national physical activity guidelines: the critical role of communication strategies. Br J Sports Med. 2020;54(24):1463–1467. doi:10.1136/bjsports-2020-102324
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dynamics of Patient-Based Benefit-Risk Assessment of Medicines in Chronic Diseases: A Systematic Review
EL Masri H, McGuire TM, van Driel ML, Benham H, Hollingworth SA
Patient Preference and Adherence 2022, 16:2609-2637
Published Date: 20 September 2022
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Knowledge, Attitudes, and Practices Towards Hormone Replacement Therapy Among Women with Perimenopausal Syndrome: A Cross-Sectional Analysis in Quzhou, Zhejiang Province, China
Wang J, Xia X, Lin X, Xu X
International Journal of Women's Health 2025, 17:2265-2276
Published Date: 22 July 2025
Knowledge, Attitude, and Practice of Chronic Prostatitis Patients Regarding Electrophysiological Therapy in a Chinese Tertiary Hospital: A Cross-Sectional SEM Study
Chi Z, Wan Q, Zhang Y, Zhu T, Liu G, Lin W, Hong X, Zhang Y
Patient Preference and Adherence 2026, 20:590096
Published Date: 31 March 2026
Educational Gaps in Epigenetics: A Cross-Sectional Study of Health Sciences Students’ Knowledge and Perceptions in Saudi Arabia
Mawlawi AH, Alzahrani BM, Alharthi RS, Khan MA, Minhas M, Kumar RS
Advances in Medical Education and Practice 2026, 17:549928
Published Date: 30 June 2026