Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Authors Chong Y ![]() , Wang C, Zhi T, Fang S
, Wang C, Zhi T, Fang S ![]() , Min H, Zhang L
, Min H, Zhang L ![]() , Wu X, Wang Y
, Wu X, Wang Y
Received 27 March 2023
Accepted for publication 19 May 2023
Published 29 May 2023 Volume 2023:16 Pages 1475—1489
DOI https://doi.org/10.2147/JMDH.S412485
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yue Chong,1,* Can Wang,1,* Tingting Zhi,2 Shihan Fang,3 Haiying Min,1 Lei Zhang,1 Xiaoning Wu,1 Yanbo Wang1
1Clinical Research Center for Mental Disorders, Shanghai Pudong New Area Mental Health Center, School of Medicine, Tongji University, Shanghai, 200124, People’s Republic of China; 2Shanghai Psychological Consultation Center, Shanghai Baoshan Mental Health Center, Shanghai, 201900, People’s Republic of China; 3Affiliated Mental Health Center, Zhejiang University School of Medicine, Hangzhou Seventh People’s Hospital, Hangzhou, 310005, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanbo Wang, Clinical Research Center for Mental Disorders, Shanghai Pudong New Area Mental Health Center, School of Medicine, Tongji University, Shanghai, 200124, People’s Republic of China, Tel +86-21-65986226, Email [email protected]
Background: Physical restraint is widely used in mental health services to address safety concerns. However, studies have shown that improper physical restraint can result in adverse effects. Nurses are the main practitioners of physical restraint and play a crucial role in physical restraint decisions and nursing. In China, there is a lack of large-scale investigations into the current status of psychiatric physical restraint use.
Aim: This study aims to explore the situation and influencing factors of the psychiatric nurses’ knowledge, attitudes and practices regarding physical restraint in China.
Methods: A cross-sectional multicenter descriptive study was conducted from December 2022 to February 2023, consecutively. A convenience sampling method was used to recruit 345 staff from three psychiatric hospitals in Shanghai. A psychiatric nurses’ physical restraint use status questionnaire was administered to examine their knowledge, attitude, and practice regarding physical restraint. The data were analyzed using the Mann–Whitney U-test and the Kruskal–Wallis test. Multivariate linear stepwise regression analysis was used for multi-factor analysis.
Results: Overall, nurses had a good level of knowledge with positive attitudes and adequate practices. However, they had some misunderstandings and undesirable practices. Multiple linear regression analysis revealed that educational background, position and training experience were the main factors influencing physical restraint knowledge, attitudes and practice among psychiatric nurses (p< 0.05).
Conclusion: This study highlights some important misconceptions and improper practices of psychiatric nurses about using physical restraint. It is necessary to strengthen education and training on physical restraint for nursing staff to reduce unnecessary physical restraint use.
Keywords: knowledge, attitudes, practice, physical restraint, psychiatric nursing
Introduction
The concept of “restraint” involves various techniques and degrees of coercion and implementation. There is no consensus on the definition of “restraint” in official organizations, laws and regulations, or scientific literature, and it is understood in two broad and narrow senses in practice. It covers both physical and chemical restraint, with physical restraint including both environmental and mechanical restraint. Although “physical restraint” is not the sole type of restraint, it represents the psychiatric restraint par excellence, and in international psychiatry, “restraint” is commonly referred to as “physical restraint (PR)”, which may be manual or mechanical.1 In China, PR refers to the use of restraint instruments to immobilize the patient so that he or she is unable to move freely in position or limb movement, and is most commonly used clinically with physical restraint belts. In contrast to restraint, the concept of seclusion seems to be clearer; seclusion refers to the solitary confinement of a patient with mental disorder in a designated enclosed environment while preventing communication with the outside world.2 If a patient with mental disease is confined in a specific enclosed place alongside others, this is not considered seclusion.
Physical restraint is widely used in healthcare settings, primarily to safeguard patients and prevent accidents. Currently, nurses lead the decision-making and implementation of physical restraint in clinical practice, and physical restraint is most commonly used for patients in emergency departments, neurosurgery, psychiatry, and ICU. In mental health settings, patients with mental disorders are prone to abnormal behaviors, such as suicide, self-injury, harming others, and uncooperative treatment In such cases, healthcare workers may need to use physical restraint when no other alternative measures In such cases, healthcare workers may need to use physical restraint when no other alternative measures are available to ensure patient safety and the smooth progress of treatment. In other medical settings, physical restraint is mainly used for patients with delirium or dementia who are receiving medical treatment to prevent unplanned extraction and other unsafe behaviors, and to prevent patients from falling out of bed, falling and other accidents.
However, physical restraint is not just a strapping technique; it also carries certain medical risks. Several studies have shown that improper use of restraint not only fails to achieve the purpose of protection but can also harm the physical and mental health of patients. Improper restraint can cause a range of physical complications, such as decreased physical function, impaired peripheral circulation, muscle atrophy, pressure ulcers, infection, constipation, and even asphyxia and death.3,4 Additionally, physical restraint can cause psychological experiences such as irritability, anxiety, depression, and feelings of humiliation in patients.5 Some mental health patients voluntarily accept physical restraint; however, the vast majority of patients are involuntary, and physical restraint conflicts with the patient’s wishes, restricts their freedom, and is inconsistent with the principles of trauma-informed, recovery-oriented care. Physical restraint has been identified to have deleterious physical and psychological effects for staff, and complex legal and ethical issues are associated with its use.6 A study exploring the experiences of psychiatric nurses who use physical restraint showed that nurses felt unpleasant, impotent, and stressed while doing restraint procedures, and they may also experience physical injuries.7 Currently, different guidelines advocate for the reduced use of restraint, stipulating that it should be a last resort.
Studies conducted in mental health settings worldwide have shown that the frequency of physical restraint use on admitted patients varies widely, ranging from 3.8% to 51.3%.8 In mainland China, the frequency of physical restraint use varies from 27.2% (371/1364) to 51.3% (86/160), as reported by different studies.9,10 In Taiwan, a study reported that the incidence of restraint events was 29.5%,11 while a study in Hong Kong found that 41.1% of patients claimed to have been placed in restraints at some point during their treatment period.12 An evidence-based review has concluded that the frequency of physical restraint use is higher in China compared to the global average.13
Nurses play a crucial role in the decision-making process and implementation of physical restraint in mental health settings. Although several factors such as patient characteristics and organizational atmosphere can influence the use of physical restraint, numerous studies have indicated that the attitudes of healthcare professionals, especially nurses, have a significant impact on its implementation.14,15 Nurses’ knowledge, attitudes, and practices regarding the use of physical restraints can influence their usage in psychiatric settings. In foreign countries, nursing managers regularly educate and train psychiatric nursing staff on physical restraint, including risk assessment, trauma-informed care, de-escalation techniques, cognitive-behavioral techniques, and so on. In China, the introductory training for mental health nurses mainly covers psychiatric ethics and laws and regulations, treatment and care of mental illness, and operation of physical restraint skills, and less about this aspect of humanistic care; and the training on physical restraint also mainly covers laws and regulations, selection of appliances, operation methods, precautions, complications and management, and very little about restraint substitution.
Recent studies have suggested that staff attitudes towards physical restraint have evolved over the last two decades, especially in countries that have made significant efforts to reduce its usage.16–18 To standardize the use of psychiatric restraints, the Mental Health Law of the People’s Republic of China has clearly stipulated that “in the absence of alternative measures, medical institutions and their medical personnel may implement protective medical measures such as restraint and isolation when incidents occur or will occur in medical institutions among patients who may harm themselves, endanger the safety of others, or disrupt the medical order”. In 2022, the Mental Health Professional Committee of the Chinese Nursing Association developed the Expert Consensus on the Implementation and Removal of Protective Restraints in Psychiatry to provide a basis for standardizing the implementation and release of physical restraints in psychiatric facilities. The utilization of physical restraint has also become an important indicator of the quality of nursing in China.19
In mainland China, hospitals are classified into three groups based on their functions, facilities, and technical expertise, with tertiary hospitals being considered the highest level group. Nurses in China are divided into five groups according to their clinical experience, research competence, English proficiency and teaching level. These groups are junior nurse, senior nurse, charge nurse, assistant chief senior nurse and chief senior nurse. Most of the time, charge nurses, assistant chief senior nurses, and chief senior nurses are often served as department managers.20 In China, “psychiatric nurses” are registered nurses who work in the field of psychiatry.
While a significant number of studies have been conducted in other countries regarding the knowledge, attitudes, and practices of psychiatric staff regarding physical restraint, there is a lack of relevant research on the use of physical restraint in mental health services in China. Specifically, there is very limited research on the knowledge, attitudes, and practices of nursing staff in psychiatric facilities regarding physical restraint.
The primary objectives of this study are twofold: (1) To examine the current level of knowledge, attitudes, and practice of physical restraint among psychiatric nurses in China, and (2) To identify the factors that influence psychiatric nurses’ knowledge, attitudes, and practices related to physical restraint. This exploratory research aims to provide initial data support for psychiatric nursing managers to develop physical restraint training and related systems, which will promote the implementation of reasonable physical restraint by nursing staff and ultimately reduce the use of restraint.
Methods
Design
This investigation was a multicentre cross-sectional study.
Participants
Participants were consecutively recruited from three Mental Health Centers in Shanghai from December 2022 to February 2023, serving as a representative sample. The inclusion criteria were: (1) Being registered medical and nursing staff; (2) Having worked in a psychiatric ward for at least one year; (3) Being willing to participate in the study. Exclusion criteria were: (1) Being temporary employees of the hospital; (2) Having been on leave for more than 6 months. A convenience sample of 345 registered nurses who agreed to participate was recruited.
Measures
Sociodemographic Characteristics
The first part of the questionnaire gathered the demographic data of respondents: age, gender, ethnicity, family, hospital level, marital status, monthly household income, education, political affiliation, title, position, management mode of the ward, years of nursing work, years of psychiatric nursing work, possession of a national psychological counselor/therapist certificate, and whether they have received training related to physical restraint.
Psychiatric Nurses′ Knowledge, Attitudes, and Practice Regarding Physical Restraint
The original questionnaire of psychiatric nurses′ knowledge, attitudes, and practice regarding physical restraint is a 30-items questionnaire, including 13 single-choice items and 17 multiple-choice items.21 The single-choice items have “yes” and “no” options, while multiple-choice questions are self-selected by the respondents. The questionnaire has a positive expert coefficient of 100.00%, an expert authority coefficient of 0.947, and an expert coordination coefficient of 0.106, indicating that it is authoritative and scientifically sound. The Cronbach’s α for this questionnaire in this study was 0.731, indicating considerable reliability. This questionnaire helps to gain insight into nurses’ intuitive thoughts about the restraint process, restraint implementation behavior, and physical and psychological feelings after restraint implementation, and can be used to investigate the current status of medical physical restraint use among psychiatric nurses.
The single-choice questions with “yes” and “no” answers have 10 items. Each item is scored as 1 or 0 according to whether the response is “yes” or “no”, respectively, and negative questions are scored in reverse. The total score ranges from 0 to 10. The higher the score is, the more positive the psychiatric nurse’s attitude toward physical restraint and the more appropriate its use.
Data Collection
The questionnaires were distributed and collected through the online form of Questionnaire Star.
Data Analysis
The data collected were entered into Excel and analyzed using SPSS 26.0 statistical software. For non-normally distributed measures, the median and quartiles [M (P25, P75)] were used, while for normally distributed measures, the mean and standard deviation ( ) were used. Qualitative data were expressed as the number and percentage (%). Independent t-tests or ANOVA were used to compare normally distributed total scores, while a Mann–Whitney U-test or Kruskal–Wallis test was used to compare scores between sub-groups (eg, males vs females) when the scales were non-normally distributed. Multivariate linear stepwise regression analysis was used for multi-factor analysis. A statistically significant difference was considered when the p-value was less than 0.05.
) were used. Qualitative data were expressed as the number and percentage (%). Independent t-tests or ANOVA were used to compare normally distributed total scores, while a Mann–Whitney U-test or Kruskal–Wallis test was used to compare scores between sub-groups (eg, males vs females) when the scales were non-normally distributed. Multivariate linear stepwise regression analysis was used for multi-factor analysis. A statistically significant difference was considered when the p-value was less than 0.05.
Ethical Approval
The study protocol received approval from the Ethics Committee of Pudong New Area Mental Health Center (PDJWLL2022006) and was conducted in accordance with ethical standards. The investigator provided a detailed explanation of the study’s purpose, procedures, and confidentiality of records to each participant. Those who agreed to participate in the study were asked to sign a consent form and complete a self-report questionnaire.
Results
Description of the Participants’ Demographic Data
A total of 345 psychiatric nurses participated in this study, comprising 317 females and 28 males. Among them, 304 worked in secondary hospitals and 34 worked in tertiary hospitals. The age range of participants was 20 to 60 years old, with an average age of 33 (28, 40). There were 107 participants aged 30 years or older, and 238 aged younger than 30. The length of psychiatric nursing experience ranged from 1 to 35 years, with an average length of 9 (3, 17) years. Of the participants, 93 had less than a bachelor’s degree, 245 had a bachelor’s degree, 6 had a master’s degree, and 1 had a doctoral degree.
Regarding titles, 78 participants were junior nurses, 153 were senior nurses, 110 were charge nurses, 3 were assistant chief senior nurses, and 1 was a chief senior nurse. Of the total participants, 279 were clinical front-line nurses, and 45 were nursing managers. Additionally, 255 worked in closed wards, 53 in semi-open wards, and 37 in open wards. Among the participants, 25 held a national psychological counseling/therapist certificate, and 234 had received training in physical restraint knowledge (see Table 1).
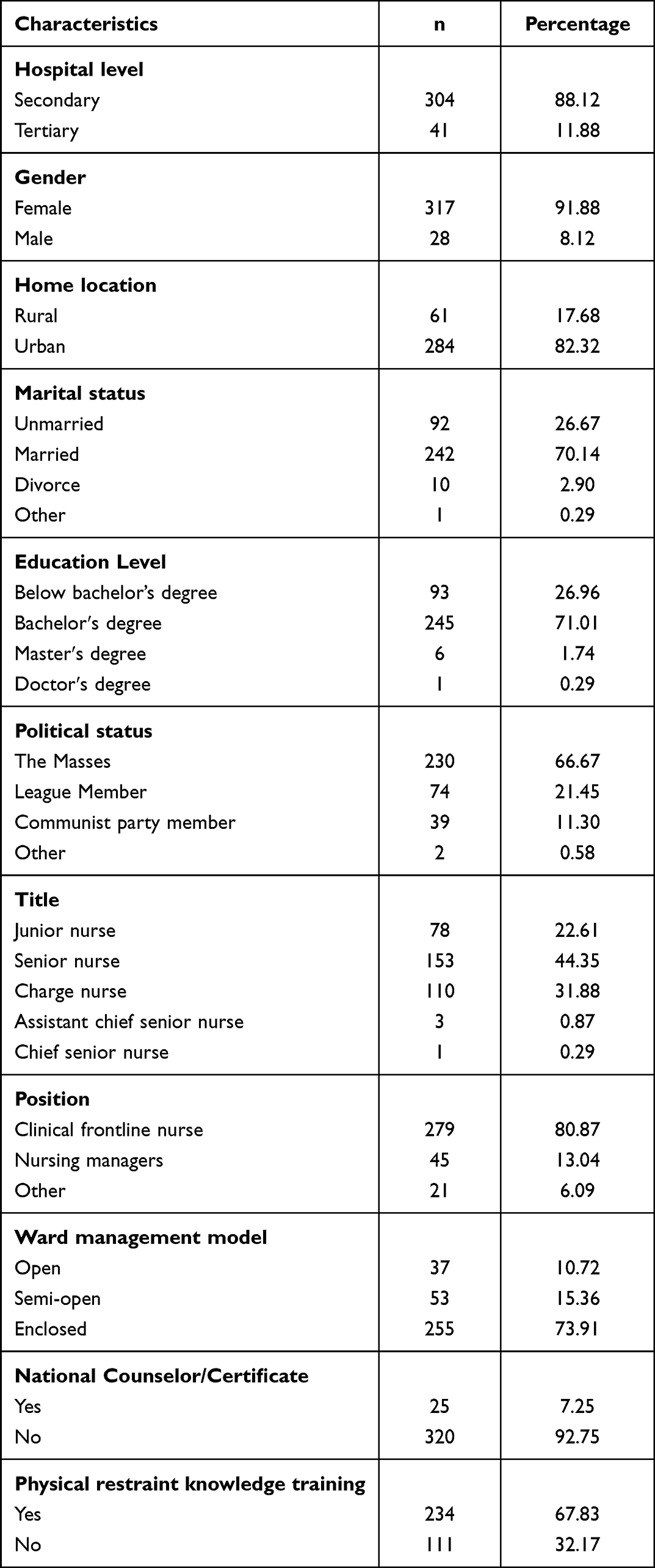 |
Table 1 Basic Information of Participants (n=345) |
Knowledge, Attitudes and Practice Regarding Physical Restraint Use
Table 2 displays the current attitudes, knowledge, and behaviors of 345 psychiatric nurses towards physical restraint. The scores of nurses, representing their knowledge, attitudes, and practices of restraint, ranged from 2 to 10, with an average score of 9 (8, 9), indicating an overall high level of understanding. Prior to restraining patients, the majority of nurses informed patients (92.46%) and family members (91.30%) in advance and obtained consent. Only a small percentage of nurses did not consider it necessary to obtain consent from patients and family members. Additionally, 96.23% of nurses introduced the purpose or function of physical restraint to patients before restraining them, and 97.10% of nurses were aware of the laws and regulations related to restraint.
 |
Table 2 Current Status of Knowledge, Attitudes and Practices of Psychiatric Nurses Toward Physical Restraint (n=345) |
The main reasons for using restraint by nurses were impulsive behavior by the patient (75.07%), suicidal tendencies (82.32%), the patient being a threat to staff safety (73.91%), and the patient posing a threat to the safety of other patients (67.54%). Over three-quarters of nurses believed that restraint was not overreached (76.23%), and the majority of nurses believed that restraint was replaceable (86.38%) and attempted to use alternative nursing measures before resorting to physical restraint. Among the alternatives to physical restraint, “psychological reassurance of the patient” (26.67%) and “drug treatment” (34.49%) were the main needs.
More than half of the nurses reported inadequate staff during restraint (73.91%), fear of injury during restraint (60.87%), and fear that physical restraint would lead to disputes or adverse events (59.13%). The majority of nurses claimed to have been injured during restraint (70.43%), experienced physical reactions such as shortness of breath (46.67%) and back discomfort (35.65%) after restraint, and had no psychological reactions (50.72%) or psychological reactions such as tension (26.38%) and anxiety (23.19%) after restraint (See Table 2).
Factors Affecting Psychiatric Nurses’ Knowledge, Attitudes and Practice Towards Use of Physical Restraint
Statistically significant differences were found in nurses′ scores towards physical restraint when comparing their demographic information, particularly their education level. Nurses with a bachelor′s degree had the highest scores (p = 0.049). Position (p<0.001) and physical restraint knowledge training (yes/no) (p<0.001) also significantly influenced the total score. Clinical frontline nurses scored higher than care managers and caregivers in other positions, and nurses who received physical restraint knowledge training performed better than those who did not receive such training (See Table 3).
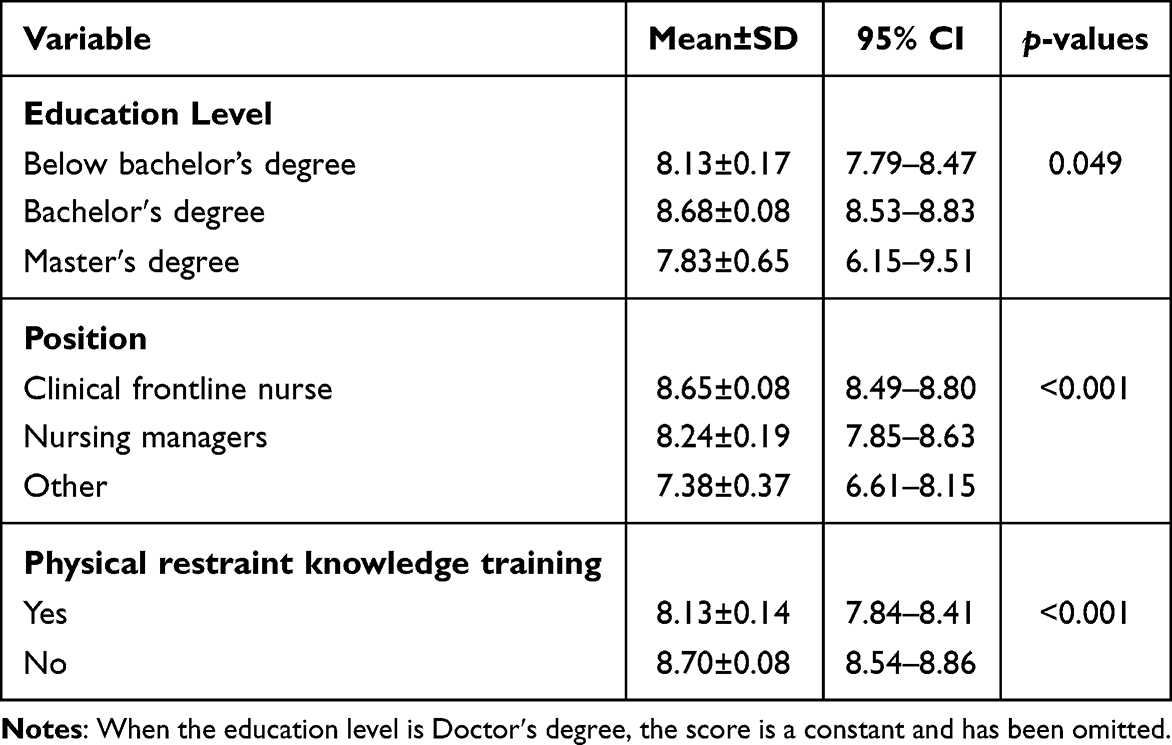 |
Table 3 Factors Affecting Psychiatric Nurses’ Knowledge, Attitudes and Practices Toward Use of Physical Restraint (n=345) |
Multiple linear stepwise regression analysis was performed with the statistically significant variables in Table 3 as independent variables and total scores of physical restraint knowledge, attitudes, and practices as dependent variables, and the results showed that education, position, and whether or not they had attended physical restraint knowledge training were the influential factors affecting the scores of psychiatric nurses’ physical restraint knowledge, attitudes, and practices. The total score regression equation had F=14.025, p<0.001. The adjusted R was 0.102, which explained 10.2% of the variance in the total physical restraint score, and the higher the education, the closer the position to first-line clinical, and the higher the total physical restraint score of psychiatric nurses who had attended physical restraint training (See Table 4).
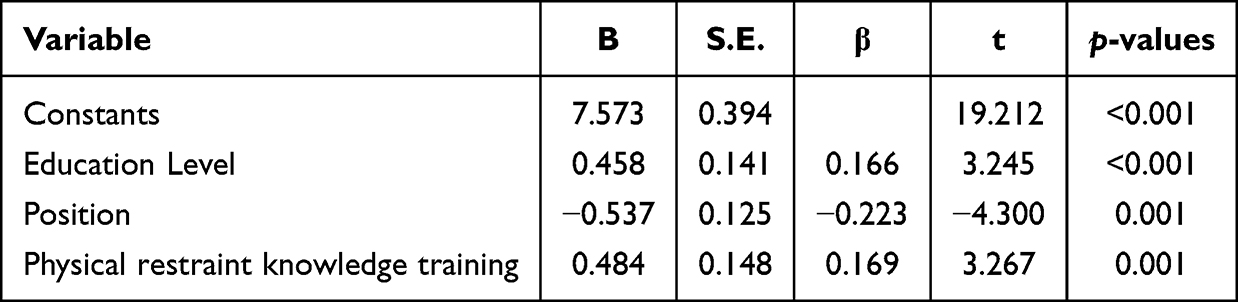 |
Table 4 Multiple Linear Stepwise Regression Analysis of Psychiatric Nurses’ Knowledge, Attitudes and Practices Toward Use of Physical Restraint (n=345) |
Discussion
The current study is the first multicenter cross-sectional survey to explore in depth psychiatric nurses′ knowledge, attitudes, and practices toward physical restraint in China. Our study provides support for improvement of the status of physical restraint.
The survey results revealed that over 50% of nurses believed that the use of physical restraint required informed consent from patients and their families, and the majority of nurses were aware of restraint-related laws and regulations, indicating that nursing staff had improved legal and ethical awareness. These findings suggest that the implementation of laws and regulations, particularly the Mental Health Law of the People’s Republic of China in 2013, has led to increased training on physical restraint knowledge and improved understanding of patients’ and families’ rights among clinical nurses. However, a small percentage of nurses still did not believe that patient consent was necessary for physical restraint use, and some nurses were not aware of physical restraint laws and regulations, indicating a need for further education on ethical issues and legal requirements related to patients’ rights and physical restraint to prevent accusations and complaints. This result is consistent with Mahmoud’s study,22 which found that a significant portion of nurses disagreed with the notion that families had the right to refuse restraint. It is important to note that physical restraint should only be used as a last resort when non-restraint alternatives have failed and when it is in the best interest of the patient to protect their basic rights.
In this study, 86.38% of nurses agreed that “physical restraint can be replaced” and expressed their willingness to try physical restraint alternatives. This marks an increase in nurses’ readiness to utilize alternative measures compared to a study conducted over a decade ago, which showed that only half of nurses would consider alternative options before resorting to physical restraint.23 We can interpret this as an increase in nurses’ willingness to use alternatives to physical restraint. However, 13.62% of nurses in the current study lacked knowledge regarding alternatives to physical restraint and were unfamiliar with the content and benefits of such measures. Therefore, the development of alternative physical restraint strategies remains a critical focus of restraint minimization programs.
Most participants in the study emphasized the importance of psychological reassurance, meeting the patient’s reasonable needs, and distracting the patient from restraint alternatives. To encourage nurses to actively seek out physical restraint alternatives and reduce the use of physical restraint, psychiatric clinical nursing staff should receive training in alternative physical restraint knowledge. This training should include de-escalation techniques, the safewards model, trauma-informed care, six core strategies, and other relevant information.24–26
Physical restraint poses a significant risk of skin injury, pressure sores, deep vein thrombosis, asphyxia, and even death.3,4 In this study, 77.68% of the nurses did not underestimate the potential somatic complications of physical restraint and would take preventive measures, such as preventing deep vein thrombosis, after the restraint. The nursing staff expressed concern about the possible risks of somatic complications, such as skin damage, venous thrombosis, and agitation leading to torso bumping during physical restraint, indicating that they were aware of the adverse physiological consequences of physical restraint on patients. However, 37.97% of nurses believed that physical restraint does not affect patients′ self-esteem or cause negative emotions. Unfortunately, nurses may not fully comprehend the emotional toll of physical restraint on patients with mental disorders and may overlook the potential psychological damage caused by its use. This negative attitude may contribute to an increase in the frequency of physical restraint. The level of empathy among caregivers is essential in reducing the use of physical restraint.27–29 Studies have shown that patients experience emotional distress such as anger, helplessness, sadness, embarrassment, and punishment as a result of physical restraint.4,5,30 Patients may also feel a loss of self-worth, degradation, and humiliation, and their autonomy and privacy may be violated when restrained.31,32 Caregivers must recognize that patients with mental disorders are particularly vulnerable and that prolonged use of physical restraint may constitute a violation of their human rights and place them at risk of significant psychological harm.33,34 Eskandari et al35 have suggested that understanding the negative consequences of physical restraint can help curtail its inappropriate or incorrect use. Therefore, mental health professionals, particularly nursing staff, should prioritize this issue, put themselves in the patients’ shoes, treat the patients as whole individuals, respect their thoughts, feelings, and needs, pay attention to physical restraint incidents in the hospital, and take effective measures to mitigate the psychological harm caused by physical restraint and enhance humanistic nursing care.
Physical restraint can also be a “challenging” process for psychiatric nurses, sometimes putting them in a dilemma. In our study, nurses pointed out the inadequate number of professionals involved in the restraint process, the unpredictability of patient aggression, and the continued high risk of exposure to adverse events related to restraint. Nursing staff believes that restraint has both the potential to prevent harm and to cause harm.36 In this study, 243 participants reported physical injuries such as scratches, bites, kicks, and punches during the restraint process. Related studies have shown that mechanical restraint triggers workplace violence among nurses, and that aggression and injuries suffered by psychiatric nurses are positively associated with the propensity to use physical restraint. After experiencing various unanticipated violent events during restraint, nursing staff fear that they will be re-injured, which can lead to an increase in physical restraint use, perpetuating a vicious cycle.37 Thus, efforts to improve the communication and de-escalation skills of mental health nurses should be emphasized to reduce the use of mechanical restraint. What’s more, from the perspective of reducing the risk of violence to nurses during physical restraint, it is recommended that future hospitals include violence management skills training in the operational training of psychiatric nurses. The content of violence management skills training should cover training on nurse quality, how to recognize impending violence, violence prevention, handling of violence and self-protection, reporting of violence, and retrospective review.38,39 Qin et al40 applied scenario simulation combined with micro-teaching in violence management operations training for junior psychiatric nurses, which improved their ability and confidence in responding to workplace violence, reduced the risk of injury, and decreased patient physical restraint use and restraint hours, making it worthy of clinical reference. In addition, this study found that the main obstacle for nurses in implementing restraint was insufficient medical and nursing staff. In addition to strengthening the team of psychiatric nurses, additional support can be made available to nurses through 24-hour monitoring, early warning systems, emergency response teams, and other technological means to respond quickly to emergencies and ensure the physical safety of patients and nurses.41 Additionally, it is suggested that doctors and nurses should jointly participate in the implementation of physical restraint, share the related responsibilities, and regulate the issuance and execution of physical restraint medical orders, which will also help to create a good hospital ethical atmosphere. Cooperation between the medical and nursing professions can eliminate unnecessary restraint, shorten the time spent in physical restraint, and clarify when physical restraint is appropriate and when it should be released.
In this study, 49.57% of the participants reported feeling anxiety and tension after a traumatic event in which the patient attacked, with 14.78% expressing fear of the patient and some developing PTSD. As a coping mechanism, 26 participants avoided going to work. Similar findings were reported by Dean et al,42 where nurses exposed to violence experienced depression, anxiety, burnout, and traumatic stress disorder, affecting their personal and professional lives. About 73.91% of nurses in this study reported wanting prompt treatment and intervention following exposure to violence, but access to psychological support is limited. To address this issue, it is recommended to assign additional psychologists dedicated to nurses in hospitals to provide immediate support and counseling to staff who have experienced violence.39 Hospitals should also actively encourage staff to report incidents of violence promptly and provide psychological comfort and material compensation to nurses who have been injured. These initiatives can reduce the adverse physical and psychological effects of violent injuries on nurses, maintain staff motivation, and ensure the orderly implementation of nursing care.
The present study revealed that the main reasons for nurses to use physical restraint were patients threatening the physical safety of staff and other patients, as well as patients displaying suicidal and impulsive tendencies. This suggests that the main principle of physical restraint use by nurses is to ensure the safety of everyone involved and avoid causing harm to patients or others. This is mainly related to the nature of psychiatric work and the violent behavior exhibited by patients with mental illness.43 Additionally, Gandhi et al44 emphasized that patients with mental disorders may be unable to control their behavior, leading to situations that may prompt the use of physical restraint.
Although the Mental Health Law of the People′s Republic of China clearly stipulates the scope of application of restraint, the indication of “disruptive medical order behavior” is vague and difficult to define, which may affect the implementation of restraint by healthcare workers. As a result, the use of physical restraint in clinical practice is still not standardized.45 It is worth noting that 23.77% of nurses in this study experienced the use of restraint beyond the scope, highlighting the urgent need to establish operational rules and standardized procedures for restraint implementation to further regulate the reasonable use of restraint.
The current study demonstrated that 96.81% of the nurses surveyed were able to use restraint techniques correctly, indicating that they possessed sufficient knowledge of physical restraint skills. However, a small proportion of nurses lacked proficiency in using restraint techniques, and 24.64% of nurses had used improper restraint techniques. The reasons for this were analyzed in two main ways: the shortage of restraint staff and the nature of psychiatric work. Shortage of staff can lead to unexpected situations in psychiatric settings, and nurses may resort to using restraint in a panicked state when faced with aggressive or irritable patients, resulting in irregularities in operating practices.41,46 Inappropriate restraint care techniques can lead to various nursing adverse events such as fractures, brachial plexus injury, and limb ischemic necrosis, highlighting the need for appropriate restraint skills to ensure patient safety.41 The rate of physical restraint use and the safety of physical restraint are also important nursing sensitive quality evaluation indicators.41 Furthermore, 32.17% of nurses had not received training in knowledge related to physical restraint, indicating a need for nursing managers and institutional leaders to strengthen training on restraint skills for psychiatric nurses, consolidate their specialist knowledge, and correct any deficiencies in their previous physical restraint operations.
The current study found significant differences in the attitudes, knowledge, and practices of nurses based on their education level, position, and physical restraint knowledge training, which is consistent with the results of Lee et al’s study.47 The study showed that frontline clinical nurses with higher education levels and who received physical restraint knowledge training had better knowledge and more positive attitudes towards the use of physical restraint.
The analysis of this study’s data revealed that educational level had an impact on the knowledge, attitudes, and practices of psychiatric nurses regarding the use of physical restraint; nursing staff with lower educational levels exhibited worse perceptions and behaviors as well as more unfavorable attitudes toward the use of restraints. The reason for this result may be due to the fact that nursing staff with higher levels of education have a greater ability to accept new knowledge and learn to understand. However, the educational background of psychiatric nursing staff in China is generally low, with very few educational backgrounds at the master’s level and above, as was the educational background of the nurses in this study. The findings imply that it is necessary to improve the academic qualifications of nursing staff members and to provide specialized training for nursing workers in the area of mental health.
The knowledge, attitudes and practices of psychiatric nursing staff are also affected by the lack of training related to physical restraint in mental health centers and the culture of nursing safety. Even though some training on physical restraint has been carried out in China in recent years, its training mechanism is not yet perfect, and the training content is superficial, focusing on the training of operational skills and involving less on restraint substitution and humanistic care, which shows that it is necessary to conduct thematic training for physical restraint knowledge and to continuously improve the training content and mechanism.
This study also discovered that position was an influencing factor, with low scores for managers and other positions and high scores for clinical frontline nurses. The reason for this may be that clinical frontline nurses have more experience in restraint practice.
However, factors such as hospital grade and years of experience did not significantly affect nurses’ attitudes and practices towards physical restraint, which is in line with Mahmoud’s findings.22 Since the mastery of theoretical knowledge also requires going through multiple rounds of systematic training, even though the longer and richer the working experience, the amount of experience does not yet determine the level of knowledge.
Limitations
This study has several limitations. Firstly, the sample was drawn from only one city in China, and a non-random sampling method was used, which may limit the generalizability of our findings. Therefore, future research should involve a multicenter study across several provinces in the country. Secondly, this study was self-reported by nurses, whose data may be biased, physical restraint is a relatively sensitive topic, and some nurses may not have completed the questionnaire objectively and may have deliberately obscured the true situation, which may have led to biased information in the results. Thirdly, this study did not delve into the reasons for the status of knowledge, attitudes, and practices of psychiatric nurses in depth. Hence, a qualitative method should be employed in future studies. Finally, the results may not be transferable to other countries. Differences in national circumstances, cultures of care and treatment, ethnic preferences, and legislation can lead to variations in the use of physical restraint in different countries.48–50 Therefore, our study’s findings based on Chinese culture may not be applicable to other cultures.
Conclusions
This study found that nurses in psychiatric units have good knowledge, positive attitudes, and adequate practices towards the use of physical restraint. However, the study also identified some misconceptions and undesirable practices related to physical restraint. The findings highlighted the challenges, risks, and ethical dilemmas associated with physical restraint in mental health services. It was observed that frontline clinical nurses with higher education levels and physical restraint knowledge training had better practices related to physical restraint use. However, it is crucial for nurses to understand that physical restraint should only be used as a last resort. Future education and training should focus on enhancing nurses’ ethical and sensitive considerations. In conclusion, the results of this study suggest the need for targeted intervention strategies to reduce unnecessary physical restraint use.
Implications for Practice
Physical restraint is often seen as the only option for dealing with specific circumstances of a patient’s mental disorder, but it is commonly associated with negative, harmful, and traumatic experiences. The use of physical restraint can also pose physical and emotional risks for healthcare workers and place them in an ethical dilemma.51 Therefore, it is crucial to reduce the use of physical restraint in psychiatric units. Nursing managers should develop appropriate standards for physical restraint practices, enhance education and training for nurses on physical restraint, and introduce relevant alternatives to physical restraint, ethical issues, and violence prevention to promote a change in nurses’ attitudes. Additionally, nurses should actively seek alternatives to physical restraint to reduce its use.
Data Sharing Statement
The data are not available due to privacy or ethical restrictions.
Ethical Approval
The study protocol was approved by the Ethics Committee of Pudong New Area Mental Health Center (PDJWLL2022006). After listening to the research team’s understanding of the purpose and procedures of this study, all subjects signed an informed consent form to participate in this study.
Acknowledgments
We thank all of the persons who participated in this study and the three Mental Health Center in Shanghai that provided support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the General Project of Shanghai Teaching and Scientific Research (C2021333) and the Outstanding Clinical Discipline Project of Shanghai Pudong (Grant No. PWYgy2021-02).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Negroni AA. On the concept of restraint in psychiatry. Eur J Psychiatry. 2017;31(3):99–104. doi:10.1016/j.ejpsy.2017.05.001
2. Paradis-Gagne E, Pariseau-Legault P, Goulet MH, Jacob JD, Lessard-Deschenes C. Coercion in psychiatric and mental health nursing: a conceptual analysis. Int J Ment Health Nurs. 2021;30(3):589–603. doi:10.1111/inm.12855
3. Bellenger EN, Ibrahim JE, Lovell JJ, Bugeja L. The nature and extent of physical restraint-related deaths in nursing homes: a systematic review. J Aging Health. 2018;30(7):1042–1061. doi:10.1177/0898264317704541
4. Chieze M, Hurst S, Kaiser S, Sentissi O. Effects of seclusion and restraint in adult psychiatry: a systematic review. Front Psychiatry. 2019;10:491. doi:10.3389/fpsyt.2019.00491
5. Tingleff EB, Bradley SK, Gildberg FA, Munksgaard G, Hounsgaard L. ”Treat me with respect”. A systematic review and thematic analysis of psychiatric patients’ reported perceptions of the situations associated with the process of coercion. J Psychiatr Ment Health Nurs. 2017;24(9–10):681–698. doi:10.1111/jpm.12410
6. Gerace A, Muir-Cochrane E. Perceptions of nurses working with psychiatric consumers regarding the elimination of seclusion and restraint in psychiatric inpatient settings and emergency departments: an Australian survey. Int J Ment Health Nurs. 2019;28(1):209–225. doi:10.1111/inm.12522
7. Perez-Toribio A, Moreno-Poyato AR, Roldan-Merino JF, Nash M. Spanish mental health nurses’ experiences of mechanical restraint: a qualitative descriptive study. J Psychiatr Ment Health Nurs. 2022;29(5):688–697. doi:10.1111/jpm.12860
8. Ye JR, Wang C, Xiao AX, et al. Physical restraint in mental health nursing: a concept analysis. Int J Nurs Sci. 2019;6(3):343–348. doi:10.1016/j.ijnss.2019.04.002
9. An FR, Sha S, Zhang QE, et al. Physical restraint for psychiatric patients and its associations with clinical characteristics and the national mental health law in China. Psychiatry Res. 2016;241:154–158. doi:10.1016/j.psychres.2016.04.101
10. Zhu XM, Xiang YT, Zhou JS, et al. Frequency of physical restraint and its associations with demographic and clinical characteristics in a Chinese psychiatric institution. Perspect Psychiatr Care. 2014;50(4):251–256. doi:10.1111/ppc.12049
11. Hsu CC, Chan H-Y, Guloksuz S. Factors associated with prolonged length of stay in the psychiatric emergency service. PLoS One. 2018;13(8):e0202569. doi:10.1371/journal.pone.0202569
12. Wu KK, Cheng JP, Leung J, Chow LP, Lee CC. Patients’ reports of traumatic experience and posttraumatic stress in psychiatric settings. East Asian Arch Psychiatry. 2020;30(1):3–11. doi:10.12809/eaap1880
13. Ye JR, Xiao AX, Yu L, et al. Staff training reduces the use of physical restraint in mental health service, evidence-based reflection for China. Arch Psychiatr Nurs. 2018;32(3):488–494. doi:10.1016/j.apnu.2017.11.028
14. McKenna B, McEvedy S, Maguire T, Ryan J, Furness T. Prolonged use of seclusion and mechanical restraint in mental health services: a statewide retrospective cohort study. Int J Ment Health Nurs. 2017;26(5):491–499. doi:10.1111/inm.12383
15. Suen LKP, Lai CKY, Wong TKS, et al. Use of physical restraints in rehabilitation settings: staff knowledge, attitudes and predictors. J Adv Nurs. 2006;55(1):20–28. doi:10.1111/j.1365-2648.2006.03883.x
16. Doedens P, Vermeulen J, Boyette LL, Latour C, de Haan L. Influence of nursing staff attitudes and characteristics on the use of coercive measures in acute mental health services-a systematic review. J Psychiatr Ment Health Nurs. 2020;27(4):446–459. doi:10.1111/jpm.12586
17. Duxbury J, Baker J, Downe S, et al. Minimising the use of physical restraint in acute mental health services: the outcome of a restraint reduction programme (‘REsTRAIN YOURSELF’). Int J Nurs Stud. 2019;95:40–48. doi:10.1016/j.ijnurstu.2019.03.016
18. Lebel JL, Duxbury JA, Putkonen A, Sprague T, Rae C, Sharpe J. Multinational experiences in reducing and preventing the use of restraint and seclusion. J Psychosoc Nurs Ment Health Serv. 2014;52(11):22–29. doi:10.3928/02793695-20140915-01
19. Mental Health Professional Committee of Chinese Nursing A. Expert consensus on the implementation and removal of protective restraints in psychiatry. Chin J Nurs. 2022;57(2):146–151.
20. Wang L, Zhu XP, Zeng XT, Xiong P. Nurses’ knowledge, attitudes and practices related to physical restraint: a cross-sectional study. Int Nurs Rev. 2019;66(1):122–129. doi:10.1111/inr.12470
21. Luo W, Gao J, Xu DM, et al. Development of the application status of medical protective restraint questionnaire in psychiatric nurses based on delphi method. Chin Nurs Res. 2021;35:22–27.
22. Mahmoud AS. Psychiatric nurses’ attitude and practice toward physical restraint. Arch Psychiatr Nurs. 2017;31(1):2–7. doi:10.1016/j.apnu.2016.07.013
23. Chien W-T, Lee IY. Psychiatric nurses’ knowledge and attitudes toward the use of physical restraint on older patients in psychiatric wards. Int J Mult Res Approaches. 2007;1(1):52–71. doi:10.5172/mra.455.1.1.52
24. Spencer S, Johnson P, Smith IC. De-escalation techniques for managing non-psychosis induced aggression in adults. Cochrane Database Syst Rev. 2018;7:Cd012034. doi:10.1002/14651858.CD012034.pub2
25. Riahi S, Dawe IC, Stuckey MI, Klassen PE. Implementation of the six core strategies for restraint minimization in a specialized mental health organization. J Psychosoc Nurs Ment Health Serv. 2016;54(10):32–39. doi:10.3928/02793695-20760920-06
26. Bowers L. Safewards: a new model of conflict and containment on psychiatric wards. J Psychiatr Ment Health Nurs. 2014;21(6):499–508. doi:10.1111/jpm.12129
27. Usenmez TY, Gumus F. The effect of empathy skills of psychiatric nurses on their attitudes and practices towards the use of physical restraint. Perspect Psychiatr Care. 2021;57(4):1595–1603. doi:10.1111/ppc.12723
28. He S, Meng Y, Liu F, Wang X, Qiu H, Zuo Z. Nurses’ knowledge, attitude, and practice regarding the use of physical restraints in children in the intensive care setting in China: a cross-sectional multicentre study. Aust Crit Care. 2022;2022. doi:10.1016/j.aucc.2022.04.007
29. Yang CPP, Hargreaves WA, Bostrom A. Association of empathy of nursing staff with reduction of seclusion and restraint in psychiatric inpatient care. Psychiatr Serv. 2014;65(2):251–254. doi:10.1176/appi.ps.201200531
30. Scholes A, Price O, Berry K. Women’s experiences of restrictive interventions within inpatient mental health services: a qualitative investigation. Int J Ment Health Nurs. 2022;31(2):379–389. doi:10.1111/inm.12966
31. Hogarth KM, Beattie J, Morphet J. Nurses’ attitudes towards the reporting of violence in the emergency department. Aust Emerg Nurs J. 2016;19(2):75–81. doi:10.1016/j.aenj.2015.03.006
32. Riahi S, Thomson G, Duxbury J. An integrative review exploring decision-making factors influencing mental health nurses in the use of restraint. J Psychiatr Ment Health Nurs. 2016;23(2):116–128. doi:10.1111/jpm.12285
33. Whitfield RW. WHO resource book on mental health, human rights and legislation. J R Soc Promot Health. 2005;125(6):288. doi:10.1177/146642400512500613
34. Knutzen M, Bjorkly S, Eidhammer G, et al. Characteristics of patients frequently subjected to pharmacological and mechanical restraint—a register study in three Norwegian acute psychiatric wards. Psychiatry Res. 2014;215(1):127–133. doi:10.1016/j.psychres.2013.10.024
35. Eskandari F, Abdullah KL, Zainal NZ, Wong LP. Use of physical restraint: nurses’ knowledge, attitude, intention and practice and influencing factors. J Clin Nurs. 2017;26(23–24):4479–4488. doi:10.1111/jocn.13778
36. Vedana KGG, da Silva DM, Ventura CAA, et al. Physical and mechanical restraint in psychiatric units: perceptions and experiences of nursing staff. Arch Psychiatr Nurs. 2018;32(3):367–372. doi:10.1016/j.apnu.2017.11.027
37. Yang BX, Stone TE, Petrini MA, Morris DL. Incidence, type, related factors, and effect of workplace violence on mental health nurses: a cross-sectional survey. Arch Psychiatr Nurs. 2018;32(1):31–38. doi:10.1016/j.apnu.2017.09.013
38. Goulet MH, Larue C, Lemieux AJ. A pilot study of “post-seclusion and/or restraint review” intervention with patients and staff in a mental health setting. Perspect Psychiatr Care. 2018;54(2):212–220. doi:10.1111/ppc.12225
39. Bekelepi N, Martin P. Experience of violence, coping and support for nurses working in acute psychiatric wards. S Afr J Psychiatr. 2022;28:1700. doi:10.4102/sajpsychiatry.v28i0.1700
40. Qin FQ, Luo WJ, Wei Q, et al. Application of scenario simulation combined with micro-teaching in training of violent processing operation among low-experience nurses in psychology department. Chin Nurs Res. 2019;33:921–924.
41. Zhang WD, Xu DM, Shao J, et al. Investigation and analysis of the implementation of protective restraint in Beiing psychiatric hospitals. Chin Evid Based Med. 2021;7:1812–1815.
42. Dean L, Butler A, Cuddigan J. The impact of workplace violence toward psychiatric mental health nurses: identifying the facilitators and barriers to supportive resources. J Am Psychiatr Nurses Assoc. 2021;27(3):189–202. doi:10.1177/10783903211010945
43. Wong WK, Bressington DT. Nurses’ attitudes towards the use of physical restraint in psychiatric care: a systematic review of qualitative and quantitative studies. J Psychiatr Ment Health Nurs. 2022;29(5):659–675. doi:10.1111/jpm.12838
44. Gandhi S, Poreddi V, Palaniappan M, et al. Indian nurses’ knowledge, attitude and practice towards use of physical restraints in psychiatric patients. Invest Educ Enferm. 2018;36(1):e10. doi:10.17533/udea.iee.v36n1e10
45. Li DJ, Ma HJ, Xie B, Shao Y. Research on psychiatrists’ perspectives to legal standards of restraints application in psychiatric hospitals. J Neurosci Ment Health. 2017;17:469–473.
46. Fereidooni Moghadam M, Fallahi Khoshknab M, Pazargadi M. Psychiatric nurses’ perceptions about physical restraint; A qualitative study. Int J Community Based Nurs Midwifery. 2014;2(1):20–30.
47. Lee TK, Valimaki M, Lantta T. The knowledge, practice and attitudes of nurses regarding physical restraint: survey results from psychiatric inpatient settings. Int J Environ Res Public Health. 2021;18(13):6747. doi:10.3390/ijerph18136747
48. Bak J, Aggernaes H. Coercion within Danish psychiatry compared with 10 other European countries. Nord J Psychiatry. 2012;66(5):297–302. doi:10.3109/08039488.2011.632645
49. Georgieva I, Mulder CL, Wierdsma A. Patients’ preference and experiences of forced medication and seclusion. Psychiatr Q. 2012;83(1):1–13. doi:10.1007/s11126-011-9178-y
50. McLaughlin P, Giacco D, Priebe S, McKenna PJ. Use of coercive measures during involuntary psychiatric admission and treatment outcomes: data from a prospective study across 10 European countries. PLoS One. 2016;11(12):e0168720. doi:10.1371/journal.pone.0168720
51. Ye JR, Xiao AX, Yu L, Wei HM, Wang C, Luo TY. Physical restraints: an ethical dilemma in mental health services in China. Int J Nurs Sci. 2018;5(1):68–71. doi:10.1016/j.ijnss.2017.12.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Knowledge, Attitudes, and Practices Among Middle-Aged and Elderly Population Towards Ultrasound Screening for Strokes
Wang W, Peng Y, Tang K, Zheng Z, He L, Yang S
Journal of Multidisciplinary Healthcare 2024, 17:147-157
Published Date: 9 January 2024
Knowledge, Attitude, and Practice of Anesthetists in Managing Severe Craniocerebral Trauma in China: A Cross-Sectional Study
Zha C, Che X, Xiong L, Ji Y, Zhang G
International Journal of General Medicine 2025, 18:1035-1046
Published Date: 25 February 2025
Family Members’ Perspectives on Integrative Chinese-Western Medicine in Cancer Care
Sun T, Wang T, Xia F, Xia L, Sun X, Jiang H, Xu P, Li P
Journal of Multidisciplinary Healthcare 2025, 18:2361-2373
Published Date: 28 April 2025
The Knowledge-Attitude-Behavior Paradox in E-Cigarette Adoption Among University Students at Northern Border University, Saudi Arabia
Alenezi IN, Mersal FA, Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM, Aboelola TH, Alrwili AG
Journal of Multidisciplinary Healthcare 2026, 19:578360
Published Date: 18 February 2026