Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitude, and Practice of Chronic Prostatitis Patients Regarding Electrophysiological Therapy in a Chinese Tertiary Hospital: A Cross-Sectional SEM Study
Authors Chi Z, Wan Q, Zhang Y ![]() , Zhu T, Liu G, Lin W, Hong X, Zhang Y
, Zhu T, Liu G, Lin W, Hong X, Zhang Y
Received 18 December 2025
Accepted for publication 24 March 2026
Published 31 March 2026 Volume 2026:20 590096
DOI https://doi.org/10.2147/PPA.S590096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zepai Chi,1,2,* Qianying Wan,3,* Yuanfeng Zhang,1 Tianxiang Zhu,4 Guoyuan Liu,1 Weiqiang Lin,1 Xuwei Hong,1,2 Yonghai Zhang1
1Department of Urology, Shantou Central Hospital, Shantou, 515031, People’s Republic of China; 2Shantou Clinical Medical College of Jinan University, Shantou, 515031, People’s Republic of China; 3Depatment of Nursing Teaching, Shantou Health School, Shantou, 515073, People’s Republic of China; 4Department of Education and Research, Shantou Central Hospital, Shantou, 515031, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuwei Hong, Email [email protected] Yonghai Zhang, Email [email protected]
Purpose: This study aimed to examine the knowledge, attitudes, and practices (KAP) of patients with chronic prostatitis (CP) concerning electrophysiological therapy.
Methods: A cross-sectional survey was conducted at Shantou Central Hospital between March 2025 and June 2025. Data were collected using a structured, self-administered questionnaire specifically designed to assess the three domains of KAP. To investigate the interrelationships among knowledge, attitudes, and practices, structural equation modeling (SEM) was employed.
Results: A total of 338 valid questionnaires were collected, with a mean age of 39.11 years (standard deviation: ± 10.56). Their knowledge, attitude, and practice scores were 12.04 ± 6.40 (possible range: 0– 24), 23.87 ± 6.86 (possible range: 10– 50), and 25.41 ± 11.30 (possible range: 10– 50), respectively. SEM analysis showed the negative direct effect of knowledge on both attitude (β = − 0.344, P = 0.01), as well as the positive direct effect of attitude on practice (β = 0.494, P = 0.016); furthermore, knowledge negatively and indirectly affected practice through attitude (β = − 0.17, P = 0.019).
Conclusion: Patients diagnosed with CP demonstrated insufficient knowledge, negative attitudes, and suboptimal practices regarding electrophysiological therapy. These findings may help inform the design of patient education strategies and highlight the importance of considering behavioral and perceptual factors when promoting non-pharmacological therapies. The results should be interpreted in light of the single-center design and self-reported data.
Keywords: chronic prostatitis, electrophysiology, health knowledge, attitudes, practice, patient compliance, cross-sectional study
Background
Chronic prostatitis, particularly chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS), represents one of the most prevalent and challenging urological conditions in men.1 Epidemiological studies indicate that its global prevalence ranges between 2% and 10%, with an average around 8% among adult males, and it accounts for over 90% of all prostatitis cases.1,2 Consistent with global estimates, studies conducted in China have reported a prevalence of approximately 8.4%, with the highest burden observed among young and middle-aged men between 20 and 40 years.3 Beyond prevalence, CP/CPPS exerts a significant negative impact on quality of life, comparable to chronic diseases such as diabetes and coronary heart disease.4
Management of CP has traditionally focused on symptom relief and improving quality of life.2 Standard treatments include antibiotics, α-blockers, nonsteroidal anti-inflammatory drugs, and phytotherapeutic agents.5,6 However, pharmacological interventions are often hindered by the limited penetration of drugs into prostatic tissue and the associated adverse effects, leading to inconsistent efficacy and poor long-term adherence.7 Consequently, non-pharmacological therapies have gained increasing attention, including acupuncture, thermal therapy, extracorporeal shockwave therapy, pelvic floor rehabilitation, and biofeedback.6,8 Among these, electrophysiological therapies, such as transcutaneous electrical nerve stimulation, pelvic floor electrical stimulation, and sacral neuromodulation, have shown promise in modulating neuromuscular function, improving local circulation, and reducing pelvic pain.9,10 However, the effectiveness of such therapies is not solely determined by their physiological mechanisms; patient cognition, including their understanding and perception of treatment modalities, plays a critical role in determining treatment adherence and long-term prognosis. Behavioral models offer a practical lens for specifying these links. In the Health Belief Model, information can shape perceived benefits, perceived barriers, and self-efficacy, which in turn influence uptake of a therapy. In the Theory of Planned Behavior, beliefs inform attitudes and perceived control, which affect intention and actual behavior. Based on these ideas, we specified directional paths among knowledge, attitude, and practice for SEM. At the same time, knowledge may not always translate into acceptance if the information is fragmented, technical, or raises concerns about discomfort and risks, which could dampen attitudes and reduce follow-through.
Knowledge, Attitude, and Practice (KAP) surveys represent a well-established framework for exploring patient perspectives in clinical care.11,12 By systematically assessing what patients know, how they feel, and how they behave toward a specific condition or therapy, KAP studies provide valuable insights into health literacy, misconceptions, and treatment adherence.13,14 In the context of CP, where disease chronicity and high recurrence rates necessitate long-term management, patient knowledge and attitudes directly influence treatment-seeking behavior and compliance. Previous research has shown that many men harbor misconceptions about the causes of prostatitis, with some incorrectly attributing it primarily to sexually transmitted infections.15 Such misunderstandings may contribute to delays in care-seeking or reliance on unproven remedies.16 Conversely, adequate knowledge is associated with more proactive health behaviors and improved adherence to prescribed treatments. Evidence from KAP work in other chronic conditions also suggests that the link between knowledge and behavior can be weak or even go in an unexpected direction. For example, in chronic respiratory disease settings, patients may report higher knowledge while still showing limited engagement with recommended rehabilitation behaviors, especially when perceived burden, worry, or low confidence remains. Similar patterns have been discussed in chronic kidney disease among people with type 2 diabetes and in hypertension management, where information alone did not reliably translate into better adherence when barriers were prominent. Despite this, few studies have comprehensively examined the KAP status of patients with CP, particularly regarding their views on novel electrophysiological interventions. To address this gap, this study aims to investigate the knowledge, attitudes, and practices of CP patients in China concerning the disease itself and the role of electrophysiological therapies in its management. Specifically, we aimed to describe the overall levels of knowledge, attitudes, and practices regarding electrophysiological therapy among CP patients, to explore demographic and clinical factors related to KAP scores, and to examine the directional associations among knowledge, attitude, and practice using SEM, including a potential indirect pathway from knowledge to practice through attitude.
Methods
Study Design and Participants
This cross-sectional study was conducted at the Urology Clinic of Shantou Central Hospital between March 2025 and June 2025, involving the recruitment of patients with CP. Eligibility for participation was determined based on the following inclusion criteria: 1) meeting the diagnostic criteria for CP as defined in the 2022 edition of the Guidelines for the Diagnosis and Treatment of Urological and Andrological Diseases in China; 2) age over 18 years and disease duration exceeding 3 months; 3) awareness of the treatment plan and ability to follow medical instructions; 4) no history of mental illness; and 5) absence of serious cardiovascular or cerebrovascular diseases. Patients were excluded if they met any of the following criteria: 1) unwillingness to participate in the study; 2) completion of the questionnaire in less than 90 seconds or more than 1800 seconds; or 3) illogical responses, abnormal BMI, or extreme anthropometric parameters (weight >125 kg or height >2.0 m), which could confound interpretation. The study protocol was reviewed and approved by the Shantou Central Hospital Ethics Committee (Ethics approval number: 2025-Scientific Research 011). Informed consent was obtained from all participants prior to data collection in accordance with ethical research standards.
Procedures
A self-developed questionnaire was employed as the primary data collection tool. Its initial design was informed by relevant clinical guidelines and existing literature and subsequently refined based on the recommendations of five senior urology experts who have long been engaged in frontline clinical practice to enhance its content validity. A pilot test involving 30 participants was conducted to assess the instrument’s reliability. Cronbach’s alpha from the pilot indicated good internal consistency (α = 0.937). For the final analysis, 338 completed questionnaires were included, with an overall Cronbach’s alpha of 0.866, demonstrating satisfactory internal reliability. As a self-developed instrument, the questionnaire has limited external validation, and further psychometric evaluation in independent samples is warranted.
The finalized questionnaire, administered in Chinese, comprised four domains with a total of 45 items: 14 items assessed basic demographic and clinical information, while the remaining 31 items were distributed across the knowledge (11 items), attitude (10 items), and practice (10 items) dimensions (Supplementary Material). The total possible score of the knowledge section ranged from 0 to 24. The attitude and practice sections adopted a five-point Likert scale, and the total score for both the attitude and practice dimensions ranged from 10 to 50.
Interpretation thresholds were predefined for each dimension: knowledge scores below 50% of the maximum (≤11) indicated insufficient knowledge, scores between 50% and 75% (11–16.5) were considered moderate, and scores exceeding 75% (≥16.5) reflected adequate knowledge. Attitude and practice scores followed a similar structure: total scores ≤25 indicated negative responses, scores between 26 and 37.5 indicated neutral positions, and scores ≥38 were categorized as positive.
A questionnaire survey was conducted on patients with CP in the urology outpatient clinic of our hospital through convenience sampling. Three nurses served as research assistants to assist in the distribution of questionnaires. These nurses were trained in advance by the project researchers to fully understand the content of the questionnaire and were explicitly instructed not to answer questions on behalf of the patients to ensure the accuracy of the responses. Participants logged in and completed the questionnaire by scanning a WeChat-distributed QR code. The nurses were responsible for patiently and thoroughly explaining the questionnaire content to patients who had difficulties understanding it, thereby helping them answer more accurately. To ensure data quality and integrity, each IP address was allowed only one submission, and all items were mandatory. The research team thoroughly checked all submitted questionnaires for completeness, internal consistency, and logical coherence. Data collection was facilitated via Wenjuanxing, a WeChat-based online survey platform. A QR code linked to the questionnaire was disseminated through WeChat, allowing participants to access and complete the survey by scanning the code. To ensure data integrity, each IP address was restricted to a single submission, and all questionnaire items were mandatory. The research team conducted a thorough quality control check on each submission, excluding responses with a completion time under 90 seconds, internally inconsistent logic, or uniform answer patterns across all items within any of the KAP dimensions.
Sample Size Calculation
The required sample size was calculated according to established guidelines for psychometric research, which recommend a minimum of 5 to 10 participants per questionnaire item when conducting structural modeling or scale validation analyses.17,18 The final version of the questionnaire included 31 scored items across three dimensions—knowledge (11 items), attitude (10 items), and practice (10 items). Based on this criterion, the minimum sample size should range between 155 and 310 participants. A total of 338 valid responses were collected, which exceeded the upper threshold and ensured adequate statistical power and reliability for subsequent analyses.
Statistical Analyses
Statistical analyses were conducted using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) and Analysis of Moment Structures (AMOS) version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were first assessed for normality. Variables following a normal distribution were expressed as means with standard deviations (SD) and compared using independent samples t-tests (for two groups) or analysis of variance (ANOVA) for comparisons across three or more groups. Non-normally distributed continuous variables were reported as medians with interquartile ranges (IQR) and compared using the Wilcoxon Mann–Whitney U-test or the Kruskal–Wallis H-test, as appropriate. For variables involving multiple pairwise subgroup comparisons, post hoc analyses were performed with Bonferroni adjustment to control for multiple testing. Categorical variables were presented as frequencies and percentages (n, %) and analyzed using the chi-square test or Fisher’s exact test where applicable. Post hoc pairwise comparisons were performed using Bonferroni adjustment for variables with significant group differences. Correlations between continuous variables were examined using Pearson’s correlation coefficient for normally distributed data and Spearman’s rank correlation coefficient for skewed data. To identify potential predictors of adequate knowledge, positive attitudes, and proactive behavioral practices, univariate and multivariate logistic regression analyses were performed, incorporating relevant sociodemographic covariates. Structural equation modeling (SEM) was conducted to investigate the hypothesized relationships among knowledge, attitude, and practice (KAP). Given the cross-sectional design, the SEM paths should be interpreted as hypothesized associations rather than causal relationships. To further evaluate the construct validity of the questionnaire, confirmatory factor analysis (CFA) was performed using AMOS. Sampling adequacy was assessed using the Kaiser–Meyer–Olkin (KMO) test. Standardized factor loadings greater than 0.40 were considered acceptable indicators of construct validity. The SEM framework posited three directional paths: (1) knowledge directly influences attitude; (2) attitude directly influences practice; and (3) knowledge exerts both direct and indirect effects on practice through attitude. Model fit was assessed using standard goodness-of-fit indices, including the root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker–Lewis index (TLI), and comparative fit index (CFI). All statistical tests were two-tailed, and a P-value of less than 0.05 was considered indicative of statistical significance. To reduce instability caused by sparse data in subgroup analyses, categories with very small cell sizes were combined where appropriate before group comparisons.
Results
Demographic Information on Participants and KAP Scores
Initially, this study collected a total of 372 questionnaires. Samples with missing data from cases 339 to 372 were excluded, resulting in a final sample of 338 valid questionnaires, with an effective rate of 91.13%.
This study included 338 male CP patients with a mean age of 39.11±10.56 years. Most had a normal BMI (58.9%) and no state health insurance (59.5%). Their knowledge, attitude, and practice scores were 12.04 ± 6.40, 23.87 ± 6.86, and 25.41 ± 11.30, respectively. Knowledge scores differed significantly by BMI (overweight/obese vs light weight, P = 0.024), medical insurance (state-insured vs uninsured, P = 0.020), COPD comorbidity (no COPD vs COPD, P = 0.040), and absence of comorbidities (none vs other conditions, P = 0.021). Attitude scores varied significantly with BMI (light weight vs overweight/obese, P = 0.003), smoking status (current smokers vs never smokers, P = 0.013), medical insurance (state-insured vs uninsured, P = 0.001), and family history of prostate conditions (no family history vs positive history, P = 0.007). Practice scores showed significant associations with BMI (light weight vs overweight/obese, P = 0.002), alcohol consumption (current drinkers vs former drinkers, P = 0.019), stroke history (no stroke vs stroke, P = 0.031), absence of comorbidities (none vs other conditions, P = 0.016), and uncertainty about comorbidities (not sure vs certain, P = 0.041) (Table 1). Detailed results of the post-hoc comparisons are provided in Table S1.
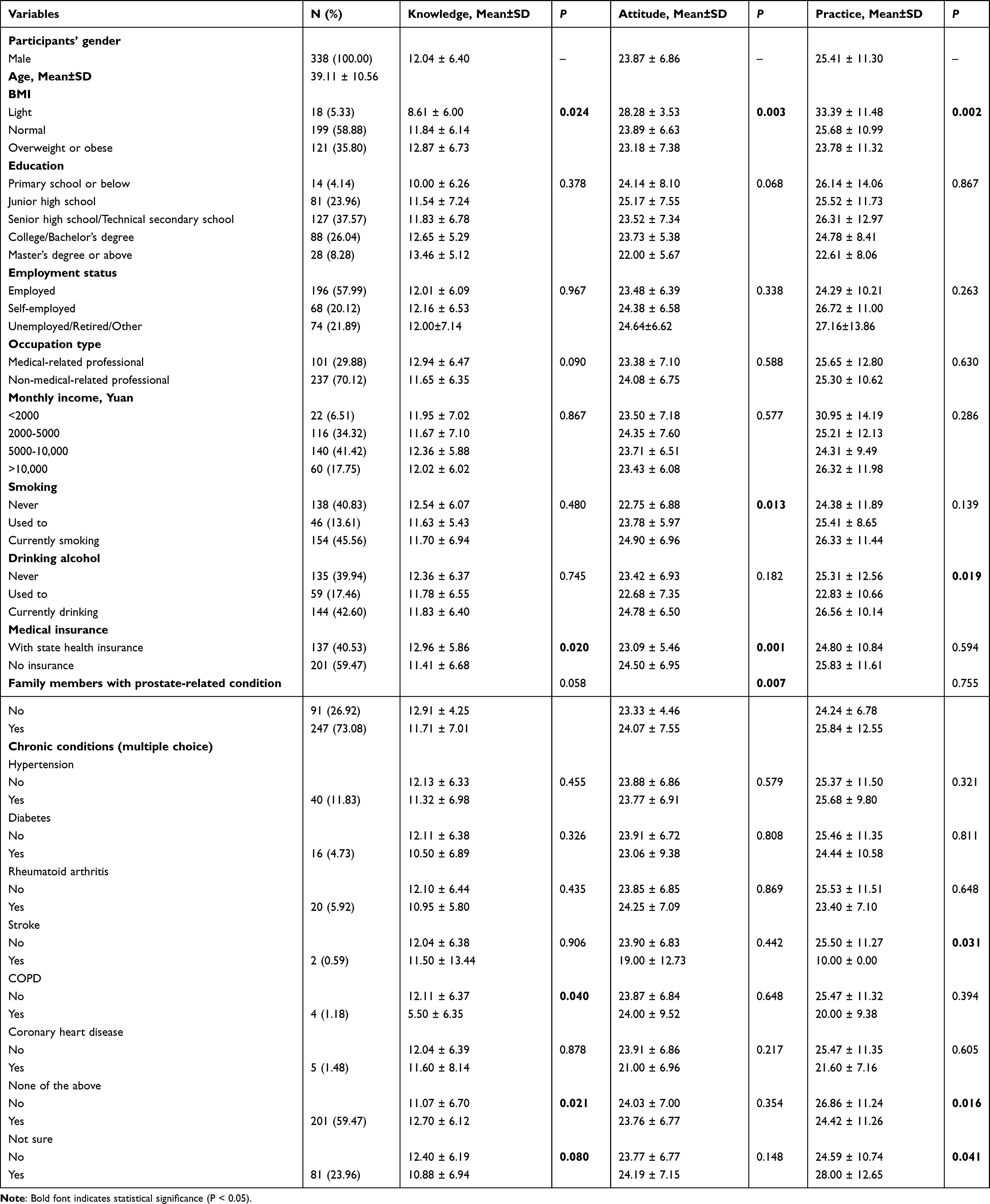 |
Table 1 Demographic Characteristics and KAP Scores |
Distribution of Responses to Knowledge, Attitude, and Practice
The knowledge assessment revealed pronounced gaps in key areas of electrophysiological therapy for CP. The items with the highest proportion of zero scores were: knowledge of electrode placement sites (K7, 85.8%), awareness of potential benefits (K5, 60.65%), and understanding of precautions during therapy (K10, 56.8%) (Table S2). The specific scoring rules and options can be found in the attached questionnaire.
Responses to the attitude dimension showed that only 14.2% strongly agreed that electrophysiological therapy is currently the best treatment option for their CP (A8), and only 15.68% strongly agreed that they are confident that electrophysiological therapy can improve their symptoms and quality of life (A5). Meanwhile, 17.16% are very concerned and 24.85% concerned about possible discomfort during electrophysiological therapy (A4) (Table S3).
Responses to the practice dimension showed that 21.6% rarely and 14.5% never keep up with the latest research findings and technological advancements in electrophysiological therapy (P10), 6.21% rarely and 15.38% never recommend electrophysiological therapy to other patients with CP (P8), and 5.33% rarely and 15.68% never follow the doctor’s instructions and undergo electrophysiological therapy on schedule (P1) (Table S4).
Correlation Analysis
In the correlation analysis, significant negative correlations were found between knowledge and attitude (r = −0.306, P < 0.01) as well as knowledge and practice (r = −0.275, P < 0.001). A positive correlation was found between attitude and practice (r = 0.469, P < 0.01), respectively (Table 2).
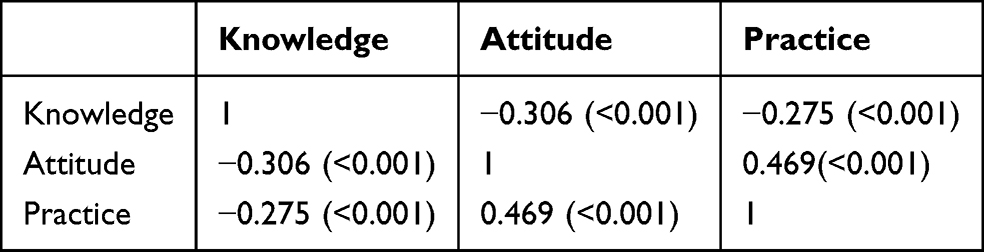 |
Table 2 Correlation Analysis |
Measurement Model Validation
The measurement model demonstrated acceptable construct validity. The KMO value was 0.940 (P < 0.001), indicating excellent sampling adequacy for factor analysis. CFA showed that most standardized factor loadings exceeded 0.50 across the three latent constructs (knowledge, attitude, and practice), suggesting adequate representation of the underlying dimensions (Table S5). Model fit indices indicated an acceptable fit (χ2/df = 3.560, RMSEA = 0.054, IFI = 0.886, TLI = 0.877, CFI = 0.886).
SEM Analysis
The SEM demonstrated highly favorable model fit indices (CMIN/DF value: 2.109, RMSEA value: 0.057, GFI value: 0.813), suggesting a well-fitting model (Table 3), and the effect estimates between the various paths have been presented (Table 4 and Figure 1). The results of SEM analysis showed that the negative direct effect of knowledge on both attitude (β = −0.344, P = 0.01) and the positive direct effect of attitude on practice (β = 0.494, P = 0.016); furthermore, knowledge negatively and indirectly affected practice through attitude (β = −0.17, P = 0.019) (Table 5).
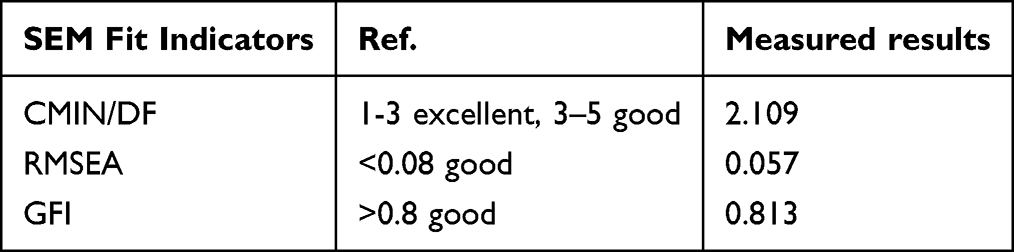 |
Table 3 SEM Fit Indicators |
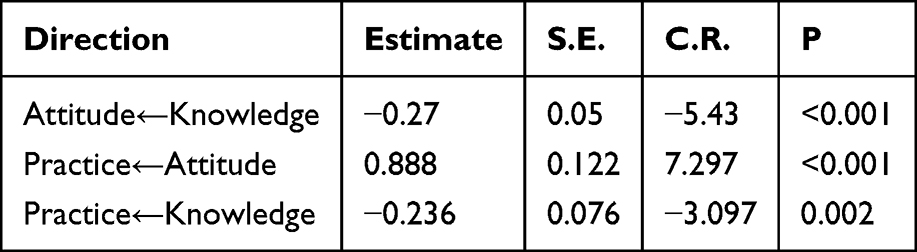 |
Table 4 Estimated Total Effect Coefficient |
 |
Table 5 SEM Direct and Indirect Effects |
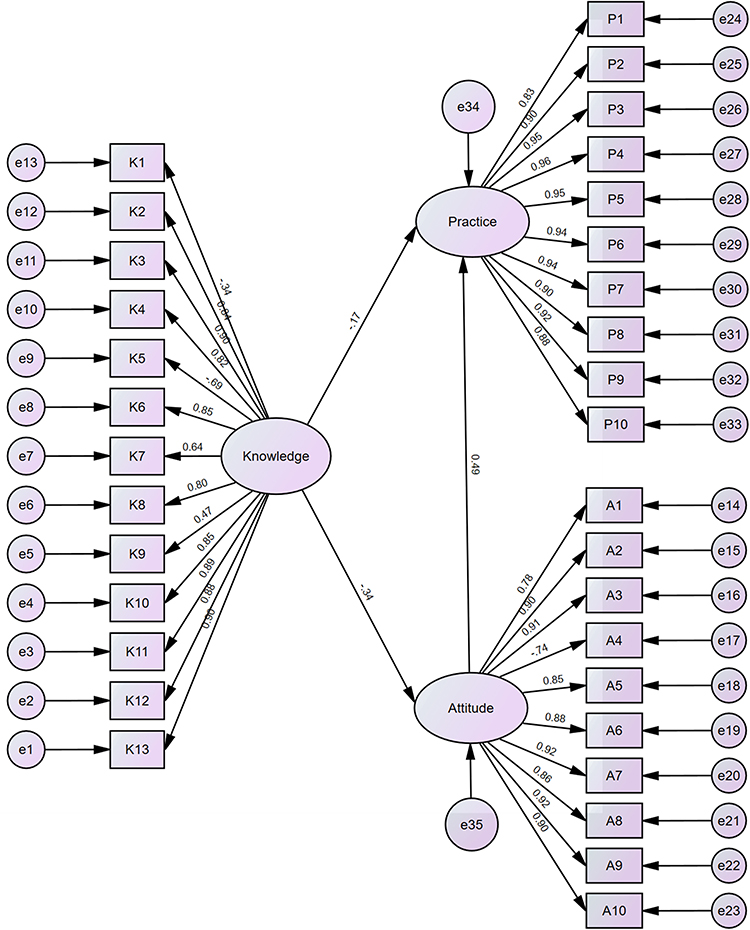 |
Figure 1 Structural equation modeling. |
Discussion
Patients diagnosed with CP demonstrated insufficient knowledge, negative attitudes, and only marginally proactive practices concerning electrophysiological therapy. To enhance treatment acceptance and optimize outcomes, it is recommended that clinicians implement structured educational interventions targeting patient misconceptions, alongside attitude-oriented counseling strategies, to facilitate informed engagement with non-pharmacological therapies in routine urological care.
Prior studies on therapeutic compliance have underscored the importance of baseline disease knowledge in fostering health-seeking behavior. Yet, among the surveyed population of CP patients, responses to knowledge items revealed widespread factual uncertainty and conceptual ambiguity. The particularly low accuracy regarding procedural aspects of electrophysiological therapy—such as electrode placement, treatment duration, and contraindications—suggests that even among those exposed to the terminology of such therapies, comprehension remains superficial.
SEM indicated a negative directional relationship between knowledge and both attitudes and practices. Because our data are cross-sectional, these findings indicate associations and do not support causal inference. While this contradicts the directional assumptions embedded in many KAP-based interventions, it is not without precedent. For instance, a recent study in patients with COPD found that higher levels of disease knowledge do not necessarily translate into more positive attitudes or stronger self-efficacy, suggesting a disconnect between cognitive acquisition and emotional engagement.19 One possible explanation is that fragmented or technical information, when not well integrated into patient-centered communication, may be accompanied by greater confusion or skepticism and coincide with less favorable attitudes and lower uptake. The current findings seem to reflect such a dynamic. Where knowledge acquisition is decoupled from interpretive frameworks or patient-centered dialogue, the result may be cognitive dissonance rather than behavioral readiness. These SEM results underscore the importance of designing educational interventions that go beyond the mere transmission of factual knowledge. Given the negative direct effect of knowledge on attitude and its indirect effect on practice, interventions should incorporate affective and motivational components such as counseling, peer support, and narrative-based education to foster trust and emotional receptivity. Educational strategies must therefore be tailored to bridge the gap between cognition and action by embedding knowledge within emotionally meaningful and contextually relevant frameworks, a principle supported by behavioral health models such as the Health Belief Model and Theory of Planned Behavior.20,21 Previous studies have demonstrated that multi-dimensional interventions that include emotional engagement and behavior modeling are more effective in changing patient behavior than knowledge delivery alone.22
In the context of CP, patients often harbor misconceptions about etiology and treatment, particularly regarding non-pharmacological modalities such as electrophysiological therapy, which may further explain the observed disconnect between knowledge and positive attitudes. Differences by health insurance status and comorbidities such as COPD were particularly marked. These findings are consistent with broader patterns linking chronic disease burden and socioeconomic disadvantage to reduced access to comprehensible health education. However, the issue may not be simply one of access but also of the epistemic form in which information is delivered. The distribution of responses points not only to gaps in factual knowledge but also to the absence of clinical reasoning scaffolds that allow patients to judge relevance, weigh risks, and project therapeutic implications.
Although explicit rejection of electrophysiological therapy was rare, attitudinal responses clustered around neutral or weakly positive positions. Items tapping into affective trust—confidence in outcomes, optimism about therapeutic value—consistently drew equivocal replies. This neutralization of affective response has been observed in contexts where interventions are perceived as externally imposed but not internally assimilated, especially among patients navigating complex or poorly understood treatments.23 In this dataset, attitudes showed the strongest association with behavioral engagement, as demonstrated by both bivariate correlation and SEM pathway modeling. Yet the pathway from knowledge to attitude was again inverse. This aligns with observations from KAP literature where increases in disease-related knowledge do not uniformly translate to improved attitudes or behaviors, particularly when the information is fragmented or perceived as irrelevant.24,25
Subgroup analyses revealed that patients without state-supported insurance and those with lower BMI scores exhibited more favorable attitudes, while those with higher educational attainment did not report correspondingly positive affect. This suggests that exposure to formal knowledge systems does not necessarily increase therapeutic receptivity. In fact, studies in CKD and IBD populations have noted that higher knowledge without supportive emotional or structural framing may heighten skepticism rather than reassurance.23,26 In such cases, efforts to shift patient attitudes must engage not only with beliefs but also with the broader interpersonal and institutional settings in which those beliefs are formed. Narrative strategies—such as case-based vignettes from comparable patients—may provide a more acceptable entry point into therapeutic discourse. Attitudinal alignment is less likely to follow didactic explanation than to emerge from the situated negotiation of shared experience and embodied credibility.
Among reported practices, those aligned with passive compliance—such as cleaning treatment areas or avoiding prohibited foods—were more commonly followed than those requiring initiative, such as adhering to scheduled sessions, seeking information, or participating in follow-up. The behavioral profile that emerges is one of externally prompted rather than internally generated adherence. This distinction matters, particularly in chronic care contexts where long-term outcomes depend on continuity and self-regulation. While attitudes exerted a direct effect on practice behaviors, the influence of knowledge was mediated, indirect, and negative in total effect. This suggests that in the absence of supportive attitudinal framing, knowledge alone does not produce behavioral commitment—and may even erode it. Similar results were seen in hypertension and T2DM studies, where increased knowledge did not guarantee better behavioral outcomes without concurrent shifts in perceived benefit and reduced barriers.23,25 Stroke survivors and individuals reporting multiple comorbidities reported the lowest practice scores. In such groups, the procedural demands of therapy may exceed available cognitive and logistical bandwidth. Conversely, slightly higher adherence among current or former alcohol users raises the possibility that prior exposure to structured therapeutic environments may increase behavioral plasticity or treatment-seeking disposition, albeit in a limited and situationally contingent way.
Interventions in this domain may benefit from reducing procedural friction, in addition to addressing motivation. Johnson et al24 conducted a meta-analysis of 153 compliance interventions and found that purely educational approaches yielded only an 8% improvement, while those incorporating behavioral reinforcement saw gains of up to 24%. For instance, integrating feedback loops, simplified messaging, and low-burden follow-ups (eg., phone-based prompts or app-based check-ins) may substantially enhance adherence.22,27 In one study, a chronic care model incorporating home visits and family involvement increased medication compliance among hypertensive patients by 28%.28 Similarly, remote self-monitoring tools such as electronic diaries and SMS alerts were associated with 81.8% adherence rates in arthritis management,26 indicating high translational value for eHealth tools in managing complex regimens.
Reconsidering the Canonical KAP Model
In the canonical KAP framework, greater knowledge is generally expected to support more positive attitudes and, in turn, better health-related practices. In our sample, however, the observed pattern did not follow this commonly assumed sequence. Rather than supporting a simple linear progression from knowledge to attitude to practice, our findings suggest a more complex and potentially inverted pattern, in which greater knowledge was associated with less favorable attitudes and, indirectly, with poorer practices through attitude. Similar departures from the conventional KAP sequence have been discussed in chronic respiratory disease, hypertension, and chronic kidney disease, where information alone did not reliably translate into behavioral engagement when perceived burden, uncertainty, or low confidence remained prominent.19,23,25 Therefore, the present findings should be interpreted as hypothesis-generating rather than confirmatory, and they suggest that the canonical KAP model may require contextual adaptation when applied to patients considering electrophysiological therapy for CP.
This study has several limitations that warrant consideration. First, the cross-sectional design restricts the ability to establish causal inferences between knowledge, attitude, and practice, as it captures data at a single time point without accounting for temporal changes or the potential impact of ongoing interventions. Second, although the sample size was adequate for statistical analysis, participants were recruited from a single tertiary hospital using convenience sampling, which limits the representativeness of the cohort and restricts the extrapolation of the findings to broader populations, particularly those from rural or less medically resourced settings. Third, the use of self-reported questionnaires may introduce response bias, as participants might have over- or under-reported their knowledge or behaviors due to social desirability or misunderstanding of items. In addition, self-administered questionnaires may be influenced by cultural factors and varying levels of health literacy, which could further affect the accuracy and consistency of responses.
Conclusions
In conclusion, patients diagnosed with CP demonstrated insufficient knowledge, predominantly negative attitudes, and only marginally proactive practices regarding electrophysiological therapy. In SEM, attitude was associated with practice and accounted for part of the association between knowledge and practice, which suggests a potential indirect pathway; therefore, patient-centered education and counseling may help address misconceptions and concerns and support engagement with electrophysiological therapy. Importantly, these findings highlight the need for integrating structured health education and counseling into urological and rehabilitation practice, enabling clinicians to design targeted interventions that improve patient adherence, optimize therapeutic outcomes, and support the broader application of electrophysiological therapy in the long-term management of CP. Larger multicenter studies, preferably with longitudinal or interventional designs, are needed to confirm these pathways and to test tailored educational strategies.
Abbreviations
KAP, Knowledge, Attitude, and Practice; CP, Chronic Prostatitis; SEM, Structural Equation Modeling; BMI, Body Mass Index; COPD, Chronic Obstructive Pulmonary Disease; SD, Standard Deviation; CKD, Chronic Kidney Disease; IBD, Inflammatory Bowel Disease; T2DM, Type 2 Diabetes Mellitus.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Shantou Central Hospital Ethics Committee (Ethics approval number: 2025-Scientific Research 011). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Guangdong Province Science and Technology Special Fund Project (Grant No. STKJ202209068), Guangdong Foundation for Rural Development (Real-World Research and Promotion Application Project for Appropriate Electrophysiological Technology), the Public Welfare Project Fund for the High-quality Development of Scientific Research in Public Hospital, China Health Promotion Foundation (Grant No.GL-A003) and Shantou Medical Health Science and Technology Project (Grant No. 250721226494744).
Disclosure
The authors declare that they have no competing interests.
References
1. Song WJ, Liu XY, He LY. Research progress on the relationship between chronic prostatitis/chronic pelvic pain syndrome and the microbiota of the reproductive system. Front Cell Infect Microbiol. 2024;14:1417276. doi:10.3389/fcimb.2024.1417276
2. Qin P, Cao X, Ni H, et al. Efficacy of different acupuncture therapies for chronic prostatitis/chronic pelvic pain syndrome: a network meta-analysis. J Pain Res. 2025;18:3653–12. doi:10.2147/JPR.S530646
3. Jin C, Chen Z, Zhang J. Meta-analysis of the efficacy of Ningmitai capsule on the treatment of chronic prostatitis in China. Medicine. 2018;97(33):e11840. doi:10.1097/MD.0000000000011840
4. Khan FU, Ihsan AU, Khan HU, et al. Comprehensive overview of prostatitis. Biomed Pharmacother. 2017;94:1064–1076. doi:10.1016/j.biopha.2017.08.016
5. Appiya Santharam M, Khan FU, Naveed M, et al. Interventions to chronic prostatitis/chronic pelvic pain syndrome treatment. Where are we standing and what’s next? Eur J Pharmacol. 2019;857:172429. doi:10.1016/j.ejphar.2019.172429
6. Mondaini N, Gacci M, Cai T, et al. Efficacy of top flat magnetic stimulation for chronic pelvic pain in men: preliminary results. Int J Impot Res. 2024;36(6):665–667. doi:10.1038/s41443-023-00822-1
7. Magistro G, Wagenlehner FM, Grabe M, Weidner W, Stief CG, Nickel JC. Contemporary management of chronic prostatitis/chronic pelvic pain syndrome. Eur Urol. 2016;69(2):286–297. doi:10.1016/j.eururo.2015.08.061
8. Franco JV, Turk T, Jung JH, et al. Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome. Cochrane Database Syst Rev. 2018;5(5):Cd012551. doi:10.1002/14651858.CD012551.pub3
9. Xiang H, Zhang T, Al-Danakh A, Yang D, Wang L. Neuromodulation in chronic pelvic pain: a narrative review. Pain Ther. 2022;11(3):789–816. doi:10.1007/s40122-022-00405-w
10. Xiao G, Weng M, Wang P. Transcutaneous electrical nerve stimulation combined with levofloxacin and tamsulosin for patients with chronic prostatitis: clinical efficacy and changes in serum factors. Am J Transl Res. 2023;15(8):5267–5275.
11. Cheng C, Zhang W, Jin B, Yang S, Lu H, Ren Y. Knowledge, attitude, and practice (KAP) towards pulmonary nodules among Chinese adults: a mediation analysis. Sci Rep. 2024;14(1):28950. doi:10.1038/s41598-024-79657-9
12. Prakash S, Singh D, Rana K, Rathore C. Knowledge, attitude and practice (KAP) study on serotonin syndrome among psychiatrists. Gen Hosp Psychiatry. 2020;67:156–157. doi:10.1016/j.genhosppsych.2020.05.005
13. Li W, Deng J, Xiong W, Zhong Y, Cao H, Jiang G. Knowledge, attitude, and practice towards thyroid nodules and cancer among patients: a cross-sectional study. Front Public Health. 2023;11:1263758. doi:10.3389/fpubh.2023.1263758
14. Peng Y, Huang Q, Yu Y, Zhu L, Yuan H. Knowledge, attitude, and practice toward nutrition support and management among hemodialysis patients. Sci Rep. 2024;14(1):21825. doi:10.1038/s41598-024-72366-3
15. Ojewola RW, Oridota ES, Balogun OS, et al. Knowledge, attitudes and screening practices regarding prostatic diseases among men older than 40 years: a population-based study in Southwest Nigeria. Pan Afr Med J. 2017;27:151. doi:10.11604/pamj.2017.27.151.10605
16. Graziani A, Grande G, Martin M, et al. Chronic prostatitis/chronic pain pelvic syndrome and male infertility. Life. 2023;13(8).
17. Chen C, Lai X, Xu A, Yang S, Jin J, Yang H. The decision for hospice care in patients with terminal illness in Shanghai: a mixed-method study. Int J Nurs Sci. 2022;9(1):71–78. doi:10.1016/j.ijnss.2021.12.002
18. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Counsel Psychol. 2006;34(6):806–838. doi:10.1177/0011000006288127
19. Su L, Wang L, Ding J, et al. Knowledge, attitudes and practices regarding pulmonary rehabilitation among patients with chronic respiratory diseases: a cross-sectional questionnaire-based study in a tertiary hospital in China. BMJ open. 2025;15(1):e085944. doi:10.1136/bmjopen-2024-085944
20. Ajzen I. The theory of planned behavior. Organ Behav Human Decis Processes. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
21. Glanz KE, Rimer BK, Viswanath K. Theory, research, and practice in health behavior; 2015.
22. Bourbeau J. Defining patient engagement, health behavior change, and disease self-management. In: Enhancing Patient Engagement in Pulmonary Healthcare: The Art and Science. Springer; 2020:1–14.
23. Page R. Knowledge, attitude and practice of type 2 diabetic patients with chronic kidney disease: a literature review; 2018.
24. Johnson AP. Disease-Related Knowledge, MHLC, and Compliance with Treatment of the Patient with COPD. The University of Tennessee; 1989.
25. Lee SW, Kam S, Chun BY, et al. Therapeutic compliance and its related factors of patients with hypertension in rural area. Korean J Prev Med. 2000;33(2):215–225.
26. Hajlaoui A, Sabbah M, Bibani N, et al. Therapeutic compliance in patients with chronic inflammatory bowel disease. J Crohns Colitis. 2023;17:i533–i533. doi:10.1093/ecco-jcc/jjac190.0533
27. Schneiderman N, Antoni MH, Penedo FJ, Ironson GH. Psychosocial–Behavioral interventions and chronic disease. In: Handbook of Behavioral medicine: Methods and Applications. Springer; 2010:989–1007.
28. Doumen M, De Cock D, Van Lierde C, et al. Engagement and attrition with eHealth tools for remote monitoring in chronic arthritis: a systematic review and meta-analysis. RMD Open. 2022;8(2):e002625. doi:10.1136/rmdopen-2022-002625
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dynamics of Patient-Based Benefit-Risk Assessment of Medicines in Chronic Diseases: A Systematic Review
EL Masri H, McGuire TM, van Driel ML, Benham H, Hollingworth SA
Patient Preference and Adherence 2022, 16:2609-2637
Published Date: 20 September 2022
Family Members’ Perspectives on Integrative Chinese-Western Medicine in Cancer Care
Sun T, Wang T, Xia F, Xia L, Sun X, Jiang H, Xu P, Li P
Journal of Multidisciplinary Healthcare 2025, 18:2361-2373
Published Date: 28 April 2025
Knowledge, Attitudes, and Practices Towards Hormone Replacement Therapy Among Women with Perimenopausal Syndrome: A Cross-Sectional Analysis in Quzhou, Zhejiang Province, China
Wang J, Xia X, Lin X, Xu X
International Journal of Women's Health 2025, 17:2265-2276
Published Date: 22 July 2025
Parental Knowledge, Attitudes, and Practices Regarding Low-Temperature Plasma Adenotonsillectomy for Pediatric Obstructive Sleep Apnea Syndrome: A Structural Equation Modeling Analysis
Shi B, Mao R, Fang J, Wu Y, Liu F, Xiang S, Xia S
Journal of Multidisciplinary Healthcare 2026, 19:576607
Published Date: 28 March 2026
Educational Gaps in Epigenetics: A Cross-Sectional Study of Health Sciences Students’ Knowledge and Perceptions in Saudi Arabia
Mawlawi AH, Alzahrani BM, Alharthi RS, Khan MA, Minhas M, Kumar RS
Advances in Medical Education and Practice 2026, 17:549928
Published Date: 30 June 2026