Back to Journals » Advances in Medical Education and Practice » Volume 16
Knowledge, Attitudes and Practices of Clinical Laboratory Workers Towards Achieving the Sample Collection Method and Turnaround Time in Dhamar Hospitals -Yemen
Authors Amer AH ![]() , Al-Shammakh AA, Al-Kholani MA
, Al-Shammakh AA, Al-Kholani MA
Received 27 June 2025
Accepted for publication 5 November 2025
Published 11 November 2025 Volume 2025:16 Pages 2075—2086
DOI https://doi.org/10.2147/AMEP.S550037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Abdulrahman H Amer,1,2 Abdulqawi Ali Al-Shammakh,3 Mohammed A Al-Kholani4
1Department of Laboratory Medicine, Faculty of Medical Sciences, Thamar University, Dhamar, Yemen; 2Department of Medical Laboratory, Faculty of Medical Sciences, Al-Saeeda University, Dhamar, Yemen; 3Department of Biochemistry, Faculty of Medicine, Thamar University, Dhamar, Yemen; 4Department of Community Medicine, Faculty of Medicine, Thamar University, Dhamar, Yemen
Correspondence: Abdulrahman H Amer, Department of Laboratory Medicine, Faculty of Medical Sciences, Thamar University, Dhamar, Yemen, Tel +967777750189, Email [email protected]
Background: Effective management of laboratory turnaround time (TAT) and adherence to sample collection protocols are essential for clinical efficiency and patient care. While WHO recommends TAT monitoring for performance evaluation, resource-limited settings such as Yemen face systemic challenges, including inconsistent training, poor infrastructure, lack of ongoing oversight, and limited use of electronic archiving systems, which can undermine compliance.
Aim: This study assessed the Knowledge, Attitudes, and Practices (KAP) of clinical laboratory workers in Dhamar, Yemen, regarding sample collection methods and TAT to identify gaps and guide interventions.
Methods: A cross-sectional study surveyed 97 laboratory workers (technicians, supervisors) across public and private hospitals using a structured questionnaire to assess their KAP regarding TAT and sample collection. Data analysis was performed using SPSS version 26.0. The association between overall KAP levels and demographic factors was assessed using chi-square tests. A p-value < 0.05 was considered statistically significant. Ethical approval was obtained prior to data collection, and informed consent was obtained from all participants.
Results: A survey of 97 laboratory professionals revealed significant gaps in Turnaround Time (TAT) knowledge, with nearly half (50.5%) demonstrating poor understanding and only 23.7% correctly defining TAT; knowledge was significantly influenced by job role (p = 0.017) but not by education or gender. Despite 95.9% acknowledging TAT’s importance, key challenges included high workload (67%) and equipment malfunctions (45.3%).
Conclusion: Critical gaps in TAT knowledge and inconsistent practices persist, driven by inadequate training and resource limitations. Standardized protocols, infrastructure upgrades, and targeted training are urgently needed to align practices with global standards and improve healthcare outcomes in Yemen.
Keywords: turnaround time, phlebotomy, pre-analytical phase, quality control, laboratory personnel, Yemen
Introduction
Clinical laboratories are fundamental to modern healthcare, underpinning disease diagnosis, monitoring, and prognosis. Over 70% of clinical decisions rely on laboratory test results, making accurate and timely diagnostics critical for effective patient care.1 However, the precision of these diagnostics hinges significantly on two key factors: rigorous adherence to proper sample collection protocols and the achievement of established Turnaround Time (TAT) benchmarks. Deficiencies in either area contribute substantially to diagnostic errors, compromised patient outcomes, and reduced healthcare efficiency.2
The pre-analytical phase, particularly sample collection, represents a major vulnerability. Errors such as mislabeling, incorrect handling, contamination, or insufficient volume are prevalent and can drastically alter test results, leading to specimen rejection, delayed treatment, or misdiagnosis.3,4 Ensuring quality necessitates a well-trained laboratory workforce proficient in standardized collection methods.
Similarly, TAT – the interval from sample receipt to result availability – is a crucial performance indicator.5 Delays disrupt clinical workflows and impede timely decision-making, especially in critical care, adversely affecting patient satisfaction and operational efficiency.6 Despite its recognized importance, achieving optimal TAT is often hindered by resource constraints like inadequate staffing and high workload, particularly in low-resource settings such as Dhamar, Yemen.7
The total Turnaround Time (TAT) in the laboratory testing cycle is collectively determined by the analytical and post-analytical phases, in addition to the pre-analytical phase. Delays due to instrument malfunctions, repeated testing, slow verification of results, or information system failures in these later phases can significantly prolong TAT, undermining earlier efficiencies and ultimately delaying critical clinical decisions.8
The Knowledge, Attitudes, and Practices (KAP) of laboratory workers are pivotal in addressing these challenges. Knowledge encompasses understanding procedures and error implications; attitudes reflect commitment to best practices; and practices denote the actual implementation of standards.9 Assessing KAP provides vital insights into performance gaps and targets for improvement. In settings like Dhamar, compounded by socio-economic instability, limited resources, and lack of standardized training, evaluating KAP becomes urgent to identify deficiencies and guide interventions.10,11
While global and regional studies highlight the persistence of pre-analytical errors and TAT delays,3,10 research specific to Yemen’s unique challenges is scarce. This study therefore aims to evaluate the KAP of clinical laboratory workers in Dhamar hospitals regarding sample collection methods and TAT adherence. By identifying knowledge gaps, attitudinal barriers, and practical challenges, this research seeks to provide actionable insights for enhancing laboratory performance and patient care quality in this resource-constrained environment.
Materials and Methods
Study Design and Participants
A cross-sectional study was conducted among laboratory workers in Dhamar, Yemen, to identify patterns and relationships between knowledge, attitudes, and practices. The study population included all laboratory personnel such as technicians, specialists, and supervisors employed within the clinical laboratories of public and private hospitals across Dhamar Governorate.
Sample Size Determination and Sampling Technique
Due to the small size of the study population of clinical laboratory workers in Dhamar City, a purposive sampling method was used. All available laboratory workers including technicians, specialists, and supervisors working in both public and private hospitals during the study period were invited to participate.
Data were collected using a structured questionnaire distributed to 120 eligible participants. After excluding 23 individuals who either declined to participate or did not fully complete the questionnaire, the final sample size comprised 97 respondents.
Eligibility Criteria
Eligible participants were required to meet the following inclusion criteria: they must have been laboratory workers including technicians, supervisors, and medical laboratory specialists with a minimum of six months of experience, whose duties involved sample collection, analysis, or the management of laboratory workflows, and who were willing to provide informed consent. Participants were excluded from the study if they were on any form of extended leave, such as sick or sabbatical, for the entirety of the data collection period, or if they were new staff members who had not yet attained six months of experience in their role.
Data Collection Tools
Data were collected via a pretested questionnaire covering demographics and a Knowledge, Attitudes, and Practices (KAP) assessment. Knowledge was evaluated using six items on TAT definitions and test-specific timeframes, with scores from 0 to 6. Attitudes were measured using 15 Likert-scale items grouped into three themes: challenges, influencing factors, and perceived importance of TAT. Practices were assessed through 15 items on specimen collection protocols. Knowledge and practices were categorized as “Good” or “Poor” using median-based cutoffs, while attitude scores were analyzed as percentages of the maximum possible, with challenge items reverse-coded.
Scoring and Cutoffs
- Knowledge/Practices:
- Knowledge: “Good” (>3/6 correct), “Poor” (≤3).
- Practices: “Good” (>10/15 correct), “Poor” (≤10), based on median cutoffs.
- Attitudes:
- Mean scores converted to percentage of maximum (5 points).
- Reverse coding for challenges (lower scores = stronger agreement).
Study Data Collection Procedure
Research team were trained on the study objectives, data collection tools, and ethical considerations. The questionnaire was distributed to laboratory workers in Dhamar hospitals. Participants were given time to complete the questionnaire, and assistance was provided if needed.
Statistical Analysis
Data were analyzed using both descriptive and inferential statistics. Descriptive statistics, including frequencies, percentages, means, standard deviations (SD), medians, and interquartile ranges (IQR), were used to summarize the data. Inferential analyses involved Chi-square tests to assess associations between knowledge, attitude, and practice levels and demographic variables (gender, education, and job role). Likert-scale responses were analyzed using mean scores and agreement percentages. All analyses were performed using SPSS version 26, with statistical significance set at p < 0.05.
Operational Definitions
Turnaround Time (TAT)
The interval between “the time of sample collection” and ‘the report dispatch to the physicians.
Laboratory Technician
A laboratory technician supports scientific investigations by performing a variety of technical tasks, including sample preparation, testing, and record-keeping. They work under the supervision of scientists in a clinical laboratory. Qualifications typically include a degree or diploma in medical laboratory.
Supervisor
A Clinical Laboratory Supervisor manages the daily operations and personnel of a clinical laboratory, ensuring accuracy, efficiency, and compliance with regulations. They are responsible for supervising testing personnel, monitoring test analyses, and reporting results, while also implementing quality control measures. Qualifications typically include a bachelor’s, master’s or PhD degree in a relevant science field, significant laboratory experience, and strong leadership and communication skills.
Other
Other positions include medical laboratory professionals holding a bachelor’s degree and extensive experience. These encompass administrative roles like Laboratory Director and Laboratory Manager, as well as roles specializing in quality control, accreditation, and information analysis.
Clinical Laboratory Worker
Personnel working in clinical laboratories of public or private hospitals in Dhamar Governorate, Yemen, including:
- Laboratory Technicians
- Laboratory Supervisors
- Medical Laboratory Specialists
- Other roles directly involved in sample handling or TAT processes.
Ethical Considerations
Ethical approval for this study was granted by the Institutional Ethical Committee of Al-Saeeda University (Ref: IEC/SRC/SU/2024/Ex.21/010/24). Official permissions were obtained from relevant public and private hospitals in Dhamar city. All participants provided written informed consent after being thoroughly informed of the study’s purpose. Voluntary participation and ethical compliance were ensured throughout the research.
Results
Demographic Characteristics of Participants
A total of 97 clinical laboratory workers participated in the study. With regard to gender, the distribution was nearly equal (48.5% male, 51.5% female). Concerning education, 48.5% held bachelor’s degrees, 47.5% held diplomas (2- or 3-year programs), and 4.1% possessed master’s degrees or higher. In terms of professional roles, technicians constituted the majority (61.9%), followed by “other” roles such as specialists or assistants (30.9%), while supervisors comprised 7.2% of participants. Based on chi-square analysis of demographic variables, the study found no significant association between gender and knowledge level. While males demonstrated a higher proportion of “Good” knowledge (55.3%) compared to females (44.0%), this difference was not statistically significant (X2 = 1.242, p = 0.312). Analysis by education level suggested a trend towards higher knowledge with higher education (eg, 75% “Good” among Master’s degree holders), but extremely small subgroup sample sizes (eg, n = 4 for Master’s) limited statistical power and resulted in a non-significant overall association (X2 = 2.632, p = 0.452). In contrast, job role showed a significant association with knowledge level in the initial three-category analysis (X2 = 8.200, p = 0.017), with “Other roles” having the highest proportion of “Good” knowledge (70%), followed by Supervisors (57.1%), and Lab Technicians (38.3%). However, caution is warranted due to the small sizes of some job role subgroups (eg, Supervisors, n = 7), which reduced statistical power. While job role appears to potentially influence knowledge levels, these findings, particularly the education trends and job role differences, require validation with larger and more balanced samples to draw firmer conclusions, Table 1.
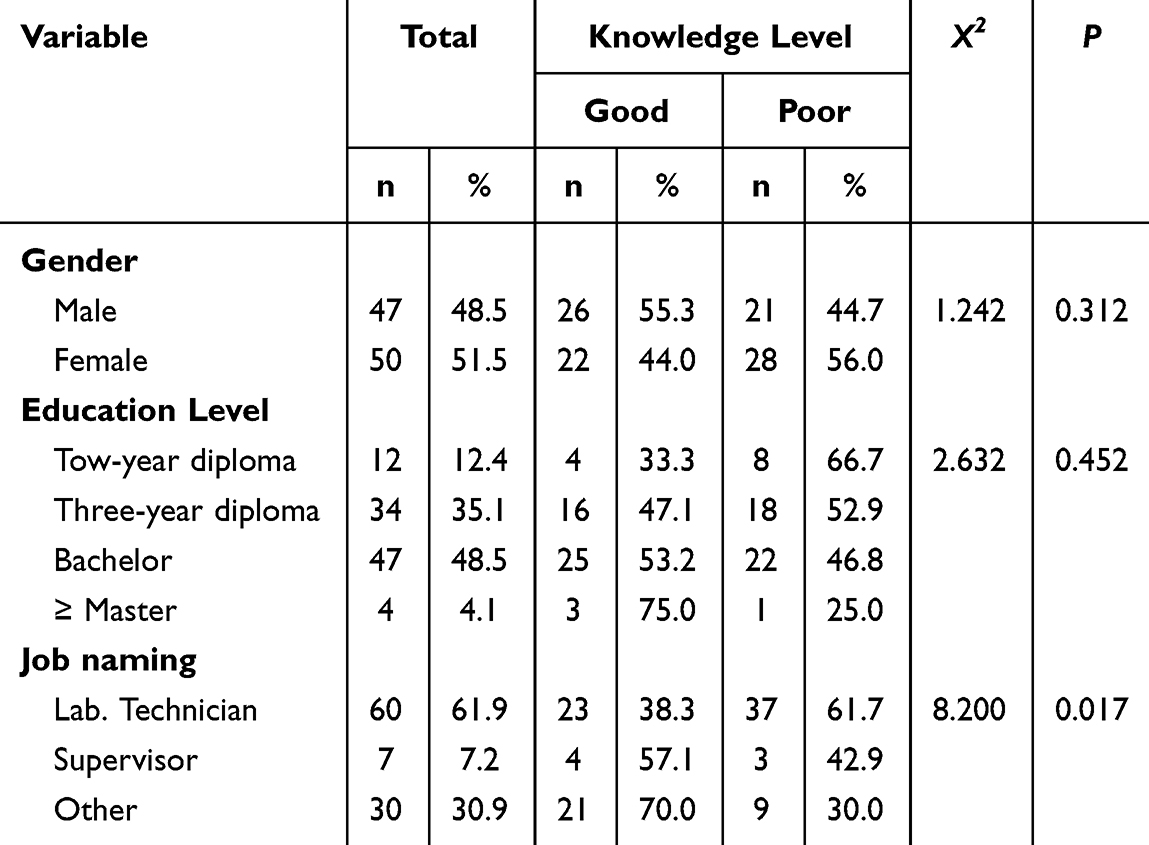 |
Table 1 Participants’ Knowledge Level According to Their General Characteristics |
Knowledge of Turnaround Time (TAT)
Only 23.7% correctly defined TAT as the interval between “the time of sample collection” and the report issuance and dispatch to the physicians.
Most participants (41.2%) incorrectly believed TAT starts at sample arrival at the lab, and 34.0% defined it as collection to result appearance. 1% expressed uncertainty.
Perceived TAT for Tests
Blood Gases: 88.7% of participants correctly identified the TAT. 19.6% of participants correctly identified the TAT for the CKMB test, and 73.2% of participants correctly identified the TAT for the troponin test, and 85.6% of participants correctly identified the TAT for the APTT test.
Total Knowledge Scores
49.5% scored above the cutoff (>3, “good” knowledge), while 50.5% had “poor” knowledge (≤3).
Mean score: 3.47/6 ± 0.98 SD (57.9% correct). 49.5% had “good” knowledge (score >3); 50.5% had “poor” knowledge (score ≤3), Table 2.
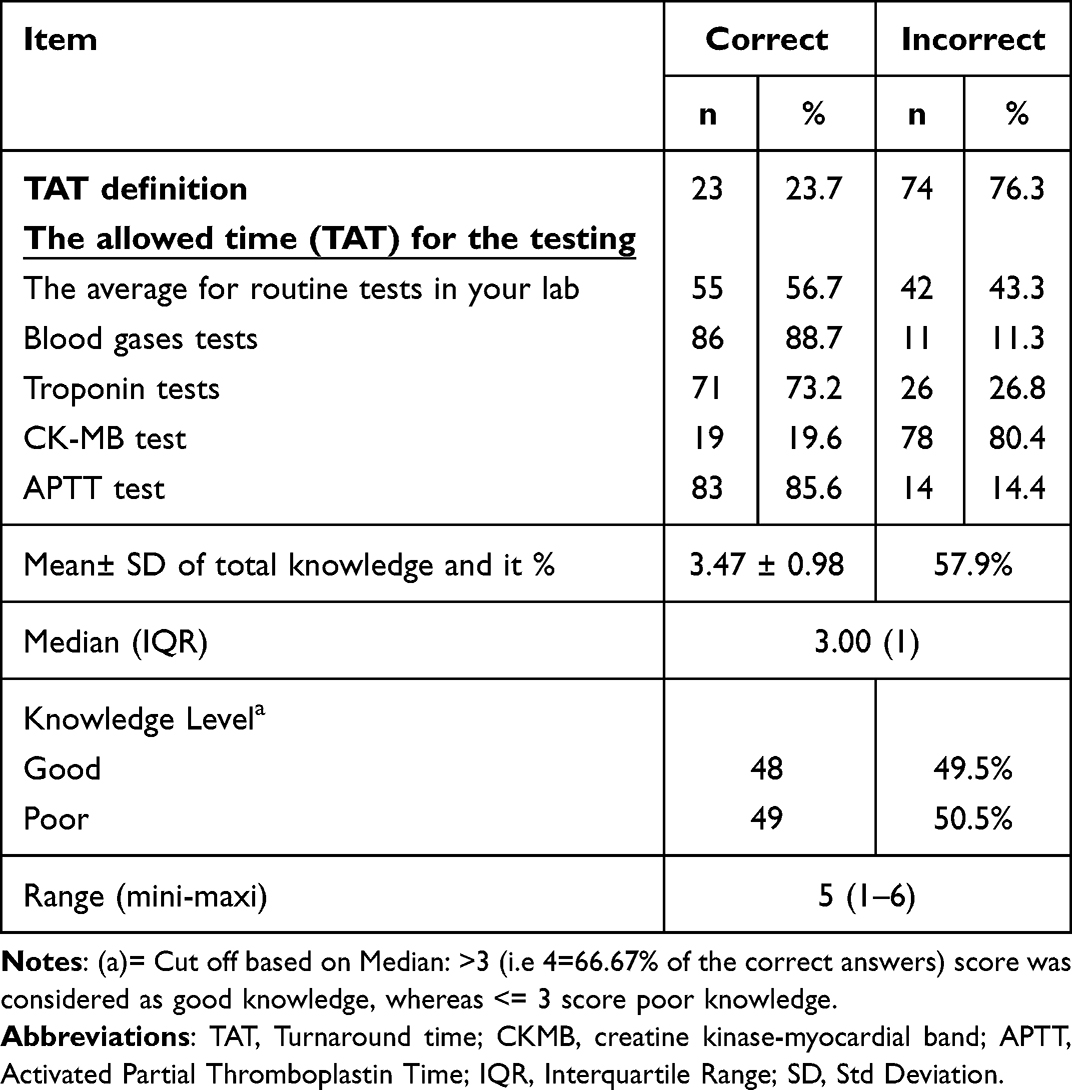 |
Table 2 Participants’ Knowledge Towards Turnaround Time (TAT) (n = 97): Correct Vs Incorrect Rates |
The highlight significant gaps in understanding. The data underscores variability in knowledge across test types, suggesting a need for targeted education on TAT protocols and underperforming test categories.
Nearly half the participants lacked adequate knowledge, emphasizing the need for targeted education to standardize TAT understanding and practices, as shown in Table 2.
Challenges Impacting TAT Goals: Survey participants identified key obstacles to achieving Turnaround Time (TAT) targets using a 5-point Likert scale. The most significant challenge was high workload (67% agreement), followed by equipment issues: malfunctions (45.3%) and delays/poor maintenance (47.4%). Staffing and training concerns were also noted: insufficient staff (37.1%) and lack of training (42.2%). While the overall trend was neutral, indicating mixed agreement, the data highlights workload and equipment reliability as primary areas for intervention, with staffing and training needing targeted focus.
Factors Affecting TAT Performance: The survey pinpointed several operational factors influencing TAT: specimen collection methods, laboratory equipment, staff availability, sample transportation, and inter-staff coordination. Among these, specimen collection methods garnered the highest agreement as a critical factor, while staff availability had the lowest agreement. The results suggest specimen handling and coordination between staff represent key areas for operational improvement.
Perceived Importance of TAT: Laboratory workers demonstrated strong consensus (overall mean: 4.45/5 ± 0.59) on the critical role of TAT in clinical services. Nearly all respondents (97.9%; 74.2% SA + 23.7% Agree) affirmed that “TAT is an important aspect of clinical services” (Mean 4.69). High agreement also existed on TAT’s link to better patient outcomes (72.2% SA, >80% SA/A combined), its enhancement of care quality, and its importance for team discussions. Even the statement with the lowest agreement (88.6% SA/A) – staff repeatedly considering TAT’s effect on patient outcomes (Mean 4.29) – reflected a strong perception of TAT’s impact on healthcare efficiency, as shown in Table 3.
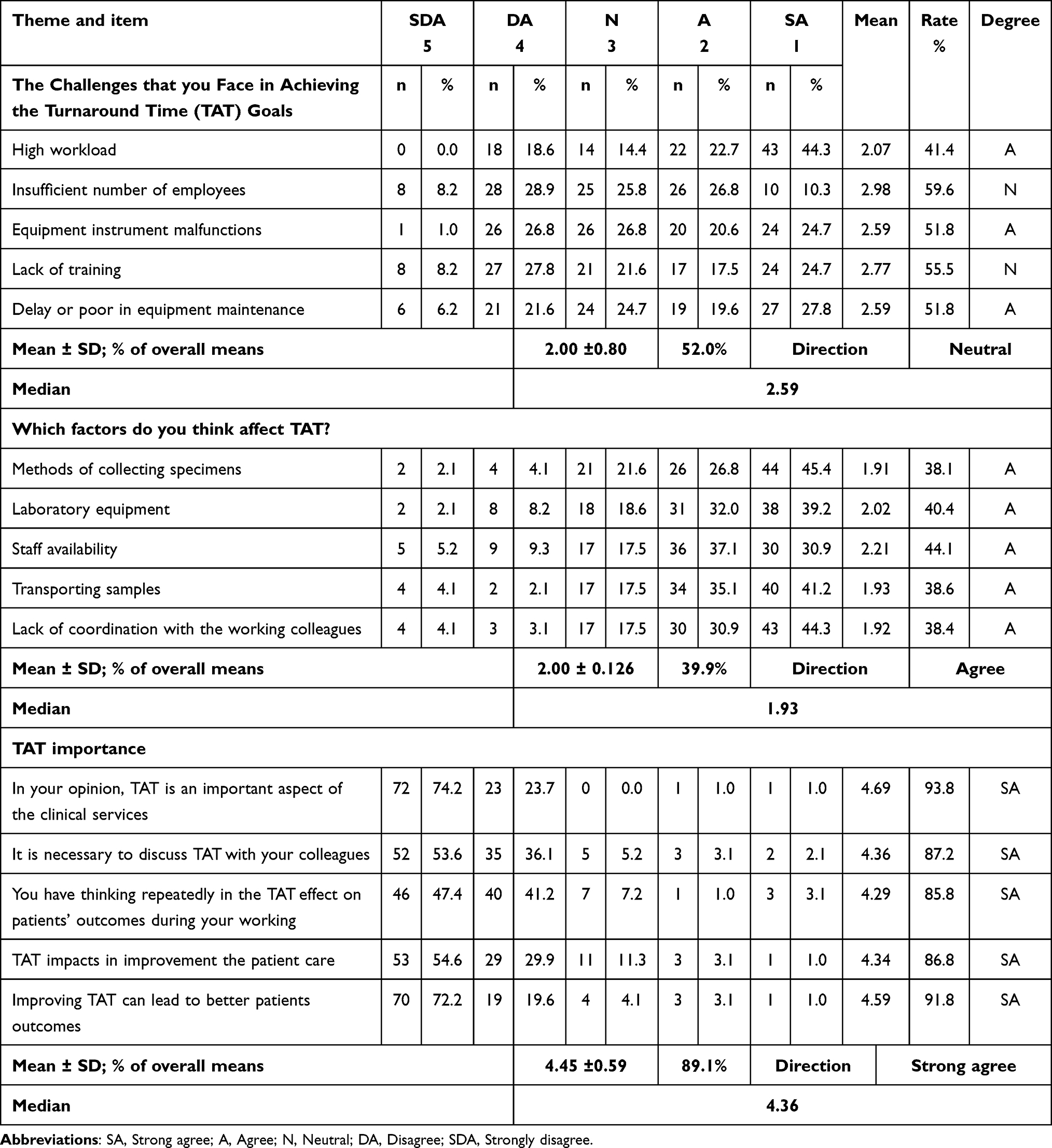 |
Table 3 Participants’ Attitudes Towards the Turnaround Time (TAT) According to Five-Points of Likert Scale |
Figure 1: The first section examines perceived challenges in achieving TAT goals, with 40.2% agreeing challenges exist, 35.1% neutral, and 24.7% disagreeing. The second section identifies factors affecting TAT, revealing a strong consensus: 71.1% agree factors significantly influence TAT, while only 4.1% disagree. Results highlight a notable contrast: challenges in meeting TAT goals elicit divided opinions, whereas external/internal factors impacting TAT are widely acknowledged.
 |
Figure 1 Perceptions of Challenges, Influencing Factors and Importance:in Achieving Turnaround Time (TAT) Goals: A Three-Point Likert Scale Survey Analysis. |
Clinical laboratory professionals’ attitudes toward the importance of turnaround time (TAT), as analyzed using a three-point Likert scale (agree, neutral, disagree) showed favorable attitudes towards importance of TAT.
Among 97 clinical laboratory professionals surveyed, an overwhelming 95.9% (93/97) agreed that turnaround time (TAT) is important, demonstrating near-universal consensus. Only 3.1% (3/97) were neutral and 1.0% (1/97) disagreed. This data strongly affirms TAT’s critical role as an organizational and operational priority, as shown in Figure 1.
Attitudes indicate that agreement regarding the presence of factors influencing TAT was consistently high across all demographic categories (gender, education level, job role), and perceptions of TAT challenges themselves showed significant variation by education level only (P = 0.022). Specifically, those with a bachelor’s degree reported the highest agreement with TAT challenges (51.1%), while those with a master’s degree or higher showed the highest disagreement (75.0%). Differences in perceptions of TAT challenges based on gender (P = 0.07, approaching significance) and job role (P = 0.301), and differences in perceptions of contributing factors across all demographic categories, were not statistically significant. Overall, the results suggest that education level is the primary demographic factor influencing whether staff perceive significant TAT challenges as shown in Table 4.
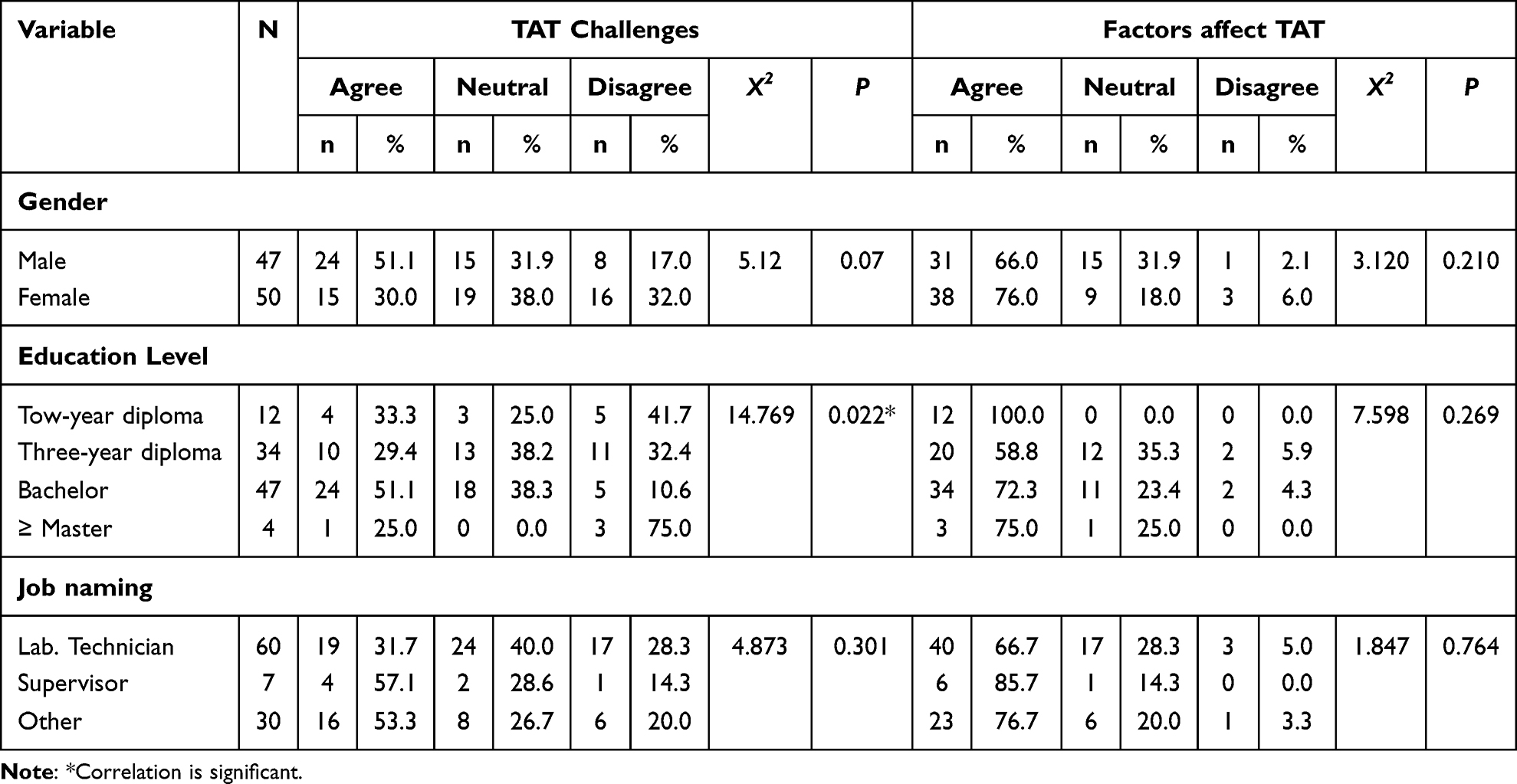 |
Table 4 Demographic Variations in Perceptions of TAT Challenges and Contributing Factors: A Cross-Tabulated Analysis with Chi-Square Statistics |
The foundational safety protocols (eg, patient identity verification at 96.9% correct, appropriate tube selection for biochemical/hormone tests at 92.8%) demonstrate near-universal adherence, significant gaps exist in operational and TAT-related workflows. Performance declines notably in anticoagulant knowledge (81.4%), documentation (66.0%), and tube-handling procedures (64.9–71.1%), with critical weaknesses emerging in TAT management: only 41.2% discuss TAT with colleagues, 36.1% apply tourniquets correctly for the recommended duration, and a mere 33.0% prioritize sample-processing tasks appropriately. This stark contrast between high-compliance safety items and low-compliance operational/TAT items explains the earlier finding of marginal overall practice quality (52.6% “poor”), highlighting an urgent need for targeted training in workflow prioritization, TAT communication, and technical procedures like tourniquet use, Table 5.
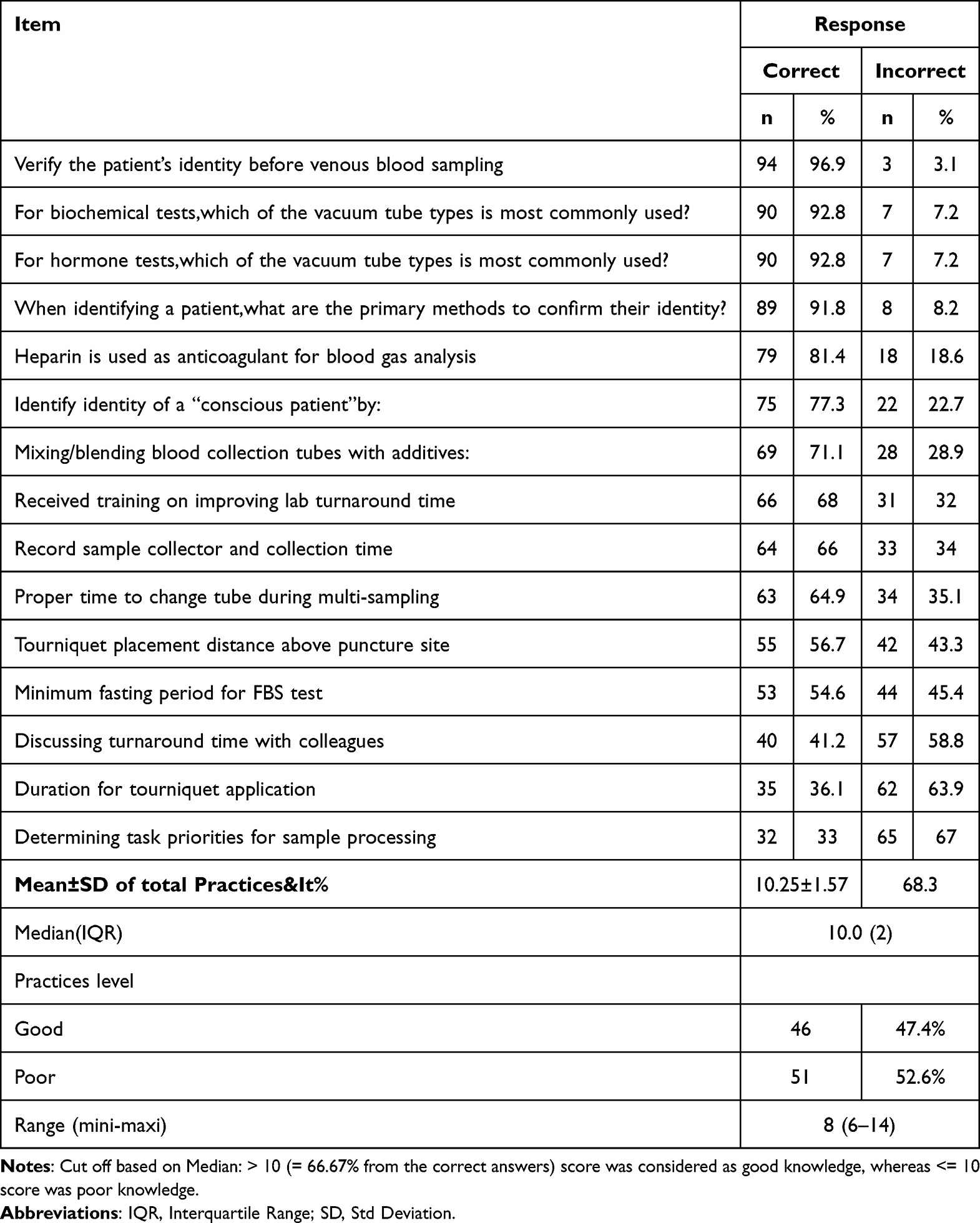 |
Table 5 Compliance Rates and Overall Scores for Specimen Collection and Turnaround Time Practices (n = 97) |
Also Table 5: showed a near-even split but slight majority of participants (52.6%, n = 51) demonstrating poor practices, while 47.4% (n = 46) exhibited good practices, based on a cutoff score of >10 (>66.7% correct answers). Despite a mean score of 10.25 ± 1.57 (68.3% of maximum) marginally exceeding the “good” threshold, the median score was exactly 10.0 (IQR = 2), indicating that half of participants scored at or below the cutoff. The narrow score range (6–14) and low variability (SD = 1.57) reveal that performance was closely clustered around the threshold, underscoring how minor improvements could shift the current slim majority in “poor” practice into the “good” category, as shown in Table 5.
Analysis of practice levels revealed no statistically significant differences based on gender or education level. While males reported a higher rate of “Good” practices (53.2%) compared to females (42.0%), this difference was not significant (χ2 = 1.217, p = 0.312). Similarly, education level showed a trend where respondents with a Bachelor’s degree or higher had the highest “Good” practice rate (54.9%), followed by those with a two-year diploma (41.7%) and a three-year diploma (38.2%), but these differences also lacked statistical significance (χ2 = 2.455, p = 0.293). In contrast, job designation showed a notable pattern approaching marginal significance (χ2 = 5.509, p = 0.064). Supervisors demonstrated the strongest performance (71.4% “Good”), followed by “Other” roles (60.0% “Good”). Lab Technicians, however, reported the lowest rate of “Good” practices (38.3%), indicating a potential area of concern, as shown in Table 6.
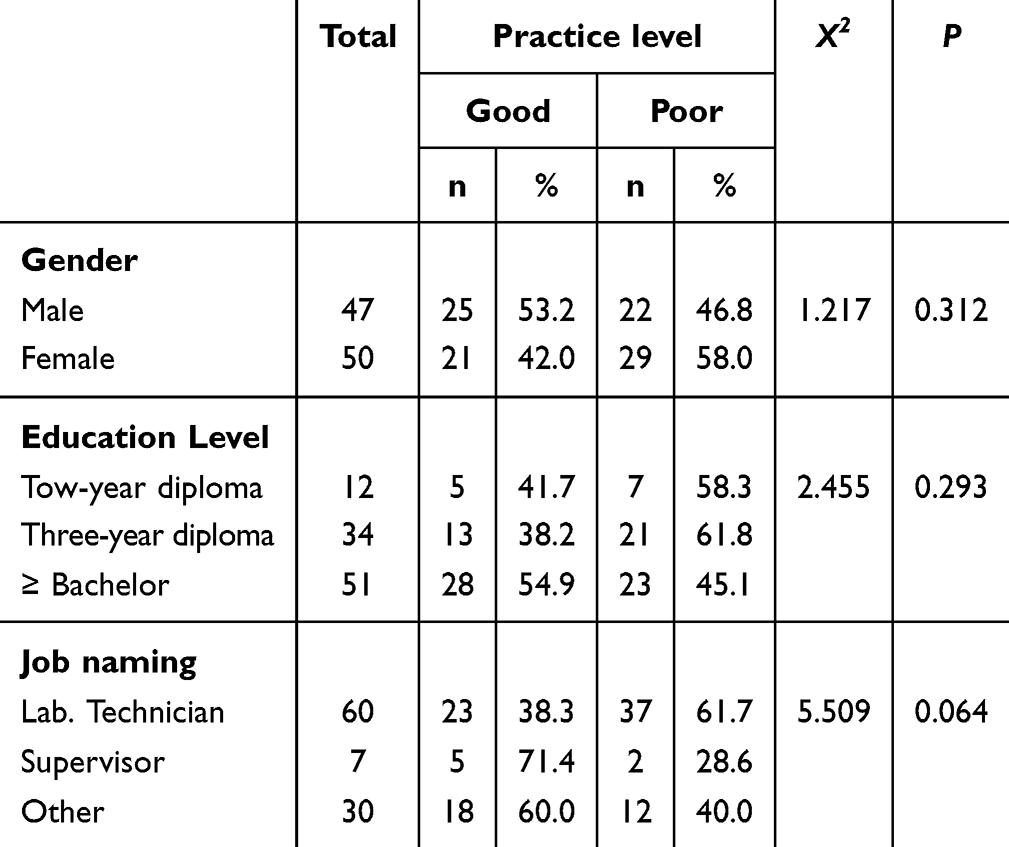 |
Table 6 Association Between Demographic Characteristics and Practice Levels in Specimen Collection and Turnaround Time |
Discussion
The findings of this study offer critical insights into laboratory professionals’ knowledge, attitudes, and practices (KAP) regarding (TAT) and sample collection, aligning with and diverging from prior research in key areas.
Only 23.7% of participants correctly defined TAT as spanning from sample collection to report issuance, with most conflating TAT with intermediate steps (eg, sample arrival at the lab). This mirrors broader challenges identified in laboratory workflows, where inconsistent institutional protocols and ambiguous guidelines perpetuate variability in TAT interpretation.2 For instance, Morias C et al (2018),3 emphasized that pre-analytical errors such as miscommunication between departments contribute significantly to TAT delays, a finding corroborated by this study’s observation of high workload (67%) and equipment malfunctions (45.3%) as barriers. The lack of standardized definitions aligns with the International Federation of Clinical Chemistry (IFCC) Working Group’s call for harmonized protocols to reduce errors in the total testing process (TTP).4
While 68% of participants reported receiving TAT training, this did not translate to uniformly strong knowledge, suggesting a disconnect between theoretical instruction and practical application. This aligns with studies highlighting the need for competency-based education, particularly in low-resource settings where training programs often lack structured curricula.5 For example, a focus group study in Pakistan revealed that medical laboratory technologists (MLTs) face challenges due to outdated training methods and insufficient hands-on experience, which hinder their ability to troubleshoot TAT-related issues.5 Similarly, interventions like those in a previous study, which demonstrated improved KAP scores post-training, underscore the importance of integrating simulations and real-world scenarios into educational programs.
Robust practices in patient identification (96.9%) and tube selection (92.8%) reflect adherence to WHO phlebotomy guidelines, yet poor compliance with tourniquet duration (36.1%) and test prioritization (64.9%) highlights systemic inefficiencies. These findings Bhatt et al (2019), who identified pre-analytical errors as a major contributor to TAT delays, often exacerbated by staffing shortages and outdated equipment.6 The role of automation, could mitigate these issues by streamlining workflows and reducing manual errors through total laboratory automation (TLA) systems.7 However, resource constraints a barrier noted in 45.3% of responses remain a critical challenge, particularly in settings lacking infrastructure for advanced technologies.9
This study corroborates prior evidence of TAT knowledge gaps and operational challenges while highlighting the role of job-specific training. By aligning interventions with established best practices, laboratories can enhance TAT compliance and patient outcomes.
Contrary to Rajan et al (2023), higher education levels did not significantly predict better TAT knowledge in this study, possibly due to small sample sizes or variability in training quality. Instead, job roles emerged as a key factor, with administrative staff outperforming lab technicians in knowledge scores (70% vs 38.3%).10 This divergence may reflect the multifaceted responsibilities of non-technical roles, which often require cross-departmental coordination a competency highlighted discussion of interoperability in mobile laboratory deployments.11 Gender-neutral outcomes, consistent with Gupta et al (2018), suggest that TAT management challenges are systemic rather than individual.12
“Other” roles exhibited higher knowledge (70% “good”) than lab technicians (38.3%)(Table 6), diverging from Pati et al (2018), who found technicians more knowledgeable.8 This may reflect unmeasured variables, such as cross-training in multifaceted roles.
While higher education (eg, bachelor’s/master’s) trended toward better knowledge, differences were non-significant (p > 0.05) (Table 6), contrasting with Gebreyes et al (2020), who reported education as a key predictor.13 This discrepancy may stem from this study’s small master’s cohort (n = 4).
This study reveals a critical dichotomy: near-perfect compliance in patient identity verification (96.9%) and tube selection (92.8%) (Table 5) aligns with global safety standards driven by regulatory pressures (eg, Joint Commission NPSGs) and awareness of catastrophic errors like misidentification.14,15 However, operational gaps particularly in tourniquet management (36.1% correct duration), TAT communication (41.2%), and workflow prioritization (33.0%) mirror preanalytical error patterns documented in literature. Studies confirm that 61.9–68.2% of laboratory errors originate in preanalytical phases, with hemolysis (40–70% of nonconformities) and clotted specimens (32.2% of rejections) directly linking to technical lapses like prolonged tourniquet time or improper mixing.16
An assessment of laboratory staff practices related to sample collection and turnaround time (TAT) revealed a worryingly unbalanced distribution, with a small majority (52.6%, n = 51 participants) showing “poor” practices, compared to 47.4% (n = 46 participants) showing “good” practices (Table 5). This is consistent with similar findings in India (59.3%)17 and Pakistan (54.6%),18 and higher findings in Korea (98.0%)19, while results were lower in Ethiopia and lower findings in Ethiopia (16.3%) regarding the achievement of clinical chemistry tests.20 These deficiencies persist, underscoring systemic training weaknesses.
This study has several key limitations. The use of purposive sampling in a single region of Yemen may limit the generalizability of the results. Additionally, the modest sample size may have reduced statistical power for subgroup analyses.
Conclusion
The study underscores critical gaps in TAT knowledge and inconsistent practices among laboratory workers, despite strong recognition of TAT’s clinical importance. Misconceptions about TAT definitions, variability in test-specific guidelines, and operational challenges (eg, workload, equipment reliability) hinder effective TAT management. While adherence to protocols like patient identification was high, pre-analytical errors persisted, reflecting systemic inefficiencies. Demographic factors such as job roles influenced outcomes more than education or gender. These findings highlight the need for standardized training, resource allocation, and workflow optimization to align practices with global standards and improve patient care in resource-constrained settings.
To bridge the identified knowledge-practice gaps, key recommendations include introducing standardized TAT and pre-analytical training for technicians, investing in equipment and infrastructure, establishing clear institutional guidelines, and providing role-specific continuing education to improve interdisciplinary communication and quality adherence.
Acknowledgments
The authors would like to thank the study participants and health workers in governmental and private hospitals in Dhamar, Yemen, and the Faculty of Medical Sciences, Al-Saeeda University, for their cooperation during the study. We also wish to acknowledge the crucial efforts of our co-investigators (Ezzaldeen AL. Hajji, Aqeel Abo Atef, Bashar Alhajjaj, Magahid Alwasab, Mohammed Abdalfatah, Mohammed Sam & Rashad Alshamri).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit section.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Goswami B, Singh B, Chawla R, Gupta V, Mallika V. Turn around time (TAT) as a benchmark of laboratory performance. Indian J Clin Biochem. 2010;25(4):376–379. doi:10.1007/s12291-010-0056-4
2. Lubin IM, Astles JR, Bunn JD, et al. The clinical laboratory is an integral component to health care delivery: an expanded representation of the total testing process. Am J Clin Pathol. 2023;160(2):124–129. [PMID: 37105541. PMCID: PMC11195669]. doi:10.1093/ajcp/aqad038
3. Sciacovelli L, Aita A, Padoan A, et al. Performance criteria and quality indicators for the post-analytical phase. Clin Chem Laborat Med. 2016;54(7):1169–1176. doi:10.1515/cclm-2015-0897
4. Flatman R. Terminology, units and reporting–how harmonized do we need to be? Clin Chem Laborat Med. 2018;57(1):1–11. doi:10.1515/cclm-2017-1083
5. Khan FMA, Moiz B, Rehman J, et al. Advancing medical laboratory practice in Pakistan: insights from a focus group study on technologists’ training needs. BMC Med Educat. 2024;24(1):938. doi:10.1186/s12909-024-05836-x
6. Bhatt RD, Shrestha C, Risal P. Factors affecting turnaround time in the clinical laboratory of the Kathmandu university hospital, Nepal. EJIFCC. 2019;30(1):14–24. PMID: 30881271. PMCID: PMC6416806.
7. Lippi G, Da Rin G. Advantages and limitations of total laboratory automation: a personal overview. Clin Chem Laborat Med. 2019;57(6):802–811. doi:10.1515/cclm-2018-1323
8. Pati HP, Singh G. Turnaround time (TAT): difference in concept for laboratory and clinician. Indian J Hematol Blood Transfusion. 2014;30(2):81–84. doi:10.1007/s12288-012-0214-3
9. Kiwanuka SN, Namuhani N, Akulume M, Kalyesubula S, Bazeyo W, Kisakye AN. Uganda’s laboratory human resource in the era of global health initiatives: experiences, constraints and opportunities—an assessment of 100 facilities. Human Resourc Health. 2020;18(1):1–10. doi:10.1186/s12960-020-0454-5
10. Rajan D. Shift work, workload, and professionalism related motivators affecting job satisfaction: an empirical study among medical laboratory technicians. Health Economic Manage Rev. 2023;4(3):1–21. doi:10.61093/hem.2023.3-01
11. Mushasha R, Paez Jimenez A, Dolmazon V, et al. Existing operational standards for field deployments of rapid response mobile laboratories: a scoping review. Front Public Health. 2024;12:1455738. doi:10.3389/fpubh.2024.1455738
12. Al‐Mugheed K, Bayraktar N. Knowledge, risk assessment, practices, self‐efficacy, attitudes, and behaviour’s towards venous thromboembolism among nurses: a systematic review. Nursing Open. 2023;10(9):6033–6044. doi:10.1002/nop2.1914
13. Ashour A, Hassan Z. The role of the work environment on the safety performance and safety management practices: its influence on the attitudes of nurses in the Jordanian hospitals. Am J Appl Sci. 2019;16(11):314–326. doi:10.3844/ajassp.2019.314.326
14. Mrazek C, Lippi G, Keppel MH, et al. Errors within the total laboratory testing process, from test selection to medical decision-making - A review of causes, consequences, surveillance and solutions. Biochemia Medica. 2020;30(2):020502. [PMID: 32550813. PMCID: PMC7271754]. doi:10.11613/BM.2020.020502
15. Scott K. Advancing Standards for Specimen Labeling and Tracking.
16. Getawa S, Aynalem M, Melku M, Adane T. Blood specimen rejection rate in clinical laboratory: a systematic review and meta-analysis. Pract Laboratory Med. 2023;33(e00303):e00303. [PMID: 36582816. PMCID: PMC9792348]. doi:10.1016/j.plabm.2022.e00303
17. Wankar AD. Study of determination of laboratory turnaround time in tertiary care hospital in India. Int J Res Med Sci. 2014;2(4):1396. doi:10.5455/2320-6012.ijrms20141129
18. Bilwani F, Siddiqui I, Vaqar S. Determination of delay in burn around time (TAT) of stat tests and its causes: an AKUH experience. J Pak Med Assoc. 2003;53(2):65.
19. Chung H-J, Lee W, Chun S, Park H-I, Min W-K. Analysis of turnaround time by subdividing three phases for outpatient chemistry specimens. Ann Clin Lab Sci. 2009;39(2):144–149.
20. Gebreyes M, Sisay A, Tegen D, Asnake A, Wolde M. Evaluation of laboratory performance, associated factors and staff awareness towards achieving turnaround time in tertiary hospitals, Ethiopia. Ethiopian J Health Sci. 2020;30(5):767–776. doi:10.4314/ejhs.v30i5.17
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Psychiatric Nurses’ Knowledge, Attitudes, and Practice Regarding Physical Restraint in China: A Multicentre Cross-Sectional Study
Chong Y, Wang C, Zhi T, Fang S, Min H, Zhang L, Wu X, Wang Y
Journal of Multidisciplinary Healthcare 2023, 16:1475-1489
Published Date: 29 May 2023
Patterns of Non-Communicable Disease, Multimorbidity, and Population Awareness in Bahir Dar, Northwest Ethiopia: A Cross-Sectional Study
Alamnia TT, Sargent GM, Kelly M
International Journal of General Medicine 2023, 16:3013-3031
Published Date: 13 July 2023
Assessing the Knowledge, Attitudes, and Vaccination Practices Towards COVID-19 Vaccination Among Mainland Chinese Nursing Students and Interns: A Multicenter Cross-Sectional Study

Qin Z, Ye X, Liu H, Tao Y, Zheng X, Zhong Y, Chen D, Ye W, Zhan C
Infection and Drug Resistance 2023, 16:4717-4728
Published Date: 20 July 2023
Public Knowledge, Attitudes, and Practices Regarding the Use of Over-The-Counter (OTC) Analgesics in Indonesia: A Cross-Sectional Study
Sinuraya RK, Wulandari C, Amalia R, Puspitasari IM
Patient Preference and Adherence 2023, 17:2569-2578
Published Date: 17 October 2023
Oral Health Knowledge, Attitude, and Behavior Among Health Professions’ Students at Kabul University of Medical Sciences
Ehsan H, Ahmadzai N, Orfani Z, Rezayee BM, Wally M, Daftani S
Clinical, Cosmetic and Investigational Dentistry 2023, 15:349-358
Published Date: 13 December 2023