Back to Journals » International Journal of General Medicine » Volume 16
Patterns of Non-Communicable Disease, Multimorbidity, and Population Awareness in Bahir Dar, Northwest Ethiopia: A Cross-Sectional Study
Authors Alamnia TT, Sargent GM, Kelly M
Received 18 May 2023
Accepted for publication 4 July 2023
Published 13 July 2023 Volume 2023:16 Pages 3013—3031
DOI https://doi.org/10.2147/IJGM.S421749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tilahun Tewabe Alamnia,1,2 Ginny M Sargent,2 Matthew Kelly2
1College of Medical and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australian Capital Territory, Australia
Correspondence: Tilahun Tewabe Alamnia, 62 Mills Road, Acton ACT 2601, Tel +61474199180, Email [email protected]
Objective: Ethiopia, like other developing countries, is going through an epidemiological transition, and high rates of non-communicable diseases (NCDs) are having a significant impact on the health system; however, there is limited evidence about community level NCD prevalence, multimorbidity, and population awareness that could inform targeted interventions and policy responses. This study aimed to identify factors associated with NCD prevalence, multimorbidity, and population awareness of NCDs in Bahir Dar, Northwest Ethiopia.
Methods: A community-based cross-sectional survey was conducted with 417 randomly sampled adults. We performed descriptive and logistic regression analyses to evaluate associations between NCD prevalence (cardiovascular diseases, diabetes, cancer, chronic respiratory diseases, chronic kidney disease, and hypertension) multimorbidity (2 or more NCDs) and demographic, socioeconomic, individual risk factors, anthropometrics, knowledge, and attitude.
Results: This study reveals that 24% of participating adults have an NCD, and 8% have multimorbidity. One-third (34.5%) have some NCD knowledge, and 75% consider NCDs more dangerous than communicable diseases. We find low NCD prevalence in participants: younger than 40 years of age (AOR 0.17, 95% CI 0.07 to 0.39); with normal body mass index (AOR 0.27, 0.10 to 0.77) and; with a family history of NCD (AOR 7.7, 4.2 to 14.1). Multimorbidity is lower in young adults (AOR 0.08, 0.03 to 0.26). NCD knowledge is higher in men (AOR 1.76, 1.06 to 2.93) and employed adults (AOR 2.91, 1.52 to 5.57), and NCD attitude in normal-weight adults (AOR 3.23, 1.42 to 7.39).
Conclusion: This study reveals a high prevalence of NCD and overall low NCD awareness in the population. Age above 40 years, family history of NCD, and weight in the obese category are significant predictors of NCD prevalence. These findings can help health professionals, health offices, and concerned stakeholders to plan targeted health interventions to reduce NCDs in the population.
Keywords: prevalence, epidemiology, demographic, socioeconomic status, individual risk factors, knowledge, attitudes, risk behaviours, chronic disease, Ethiopia
Introduction
Prevention of non-communicable diseases (NCDs) and their consequences is a global public health priority, causing more than 70% of annual deaths worldwide.1 NCDs are increasingly burdening population health in developing countries.2 The majority (77%) of the premature mortality burden of NCDs occurs in these settings, in people between 30 and 70 years.1 This pattern is attributable to socioeconomic disparities, demographic transitions towards an ageing population, high prevalence of individual risk factors, poverty and lack of access to health care and prevention/control programs in the regions.3–7
The burden of NCDs causes severe socioeconomic impacts in developing countries.8,9 Morbidities and disabilities that come with chronic NCDs hinder economic productivity and aggravate poverty at the individual and household levels.10,11 NCDs exacerbate social inequity as NCD health care can be expensive and complex, and payments are often private and out-of-pocket. The lack of attention to NCDs and poor primary healthcare services in a population lead to poor prevention, inadequate treatment, and late hospital presentations with complications, which create a heavier economic burden on people with low socioeconomic status (SES): the poor, less educated, and remote.10,12–14
Ethiopia, located in East Africa, is a developing country experiencing demographic and epidemiological transitions.15,16 The country is currently experiencing the effects of rapid urbanization, globalization, and climate change.6,17,18 The population of Ethiopia has doubled over the past two decades, with an average fertility rate of 4.4.19,20 Government action to improve health, including the 2003 nationally launched health extension program for achieving universal coverage of primary health care in four main areas: hygiene and sanitation, disease prevention and control, family health services, and health education and communication21 and emphasis on maternal and child health programs have decreased infectious and maternal and child deaths to some extent, and there are some gains in life expectancy.16,19 However, over the last three decades, the population pyramid has shifted from the largest part of the population being children under-five to adults now constituting a significant portion of the population (demographic dividend), increasing the chronic disease burden.15 As well, the socioeconomic and lifestyle changes coupled with the current globalization, rapid urbanization, and changes in food markets have led to shifts in people’s dietary habits, a so called nutrition transition. People’s dietary patterns shift from traditional healthy diets to processed, packaged, and fast foods.22–24 Due to demographic and dietary changes, as well as lifestyle changes such as increases in sedentary behaviour, like other developing countries, Ethiopia is going through an epidemiological transition from communicable diseases to chronic diseases.
Although community-level evidence on the prevalence of NCDs is lacking in Ethiopia, estimates show that the proportion of the disease burden caused by NCDs in the country was 22% in 2000, 33% in 2010, and 43% in 2019.25 In 2018 WHO reported that 40% of the burden of diseases in the country is due to NCDs, mainly from cardiovascular diseases (CVDs) (16%), cancer (7%), chronic respiratory diseases (2%), and diabetes (2%).26 A recent study in Addis Ababa found that NCDs caused 62% of total deaths: mostly from CVDs (27%), cancer (12%), diabetes (5%), chronic respiratory diseases (2%), and other NCDs (15%).27 Moreover, a 2015 national NCD risk factor survey revealed that the majority of adults in the country are at risk for developing NCDs; the prevalence of inadequate fruit/vegetable intake was 98%, current alcohol consumption was 41%, physical inactivity was 22%, and tobacco use was 4%.28 In light of the prevalence of risk factors, NCDs can be expected to rise steeply in the coming years unless appropriate preventive measures are set in place.
In most developing countries, including Ethiopia, the emphasis is on managing symptoms and complications of NCDs. Little attention has been given to prevention, mitigating risk factors, and reducing the likelihood of developing these diseases.2 The common individual risk factors contributing to the majority of NCDs are tobacco use, alcohol consumption, insufficient physical activity, and unhealthy diets.1 Socioeconomic status disparities such as education, occupation, income, and healthcare access are drivers of the individual risk factors for NCDs.5,29 Reviews of empirical evidence show that in high-income countries, high SES, such as wealth and high educational achievement, is associated with a lower risk of NCDs.13,30 However, with the stage of the epidemiological transition and contextual health variations,31,32 higher SES individuals in LMICs may engage in unhealthy lifestyles, which increases the risk of NCDs.33,34 For example, systematic reviews conducted in such countries show that individual risk factors such as alcohol, tobacco use and inadequate fruit/vegetable intake, and cardiovascular diseases and cancer were higher in people with low SES. In contrast, consumption of fats, salts, packaged foods, and diabetes prevalence’s were higher in people with high SES.5,29 Furthermore, studies show that people’s knowledge about NCD prevention is low in developing countries, which could contribute to unhealthy behaviors and the rise of these diseases.35 Given that evidence are scant regarding NCD prevalence and population distribution, while prevention programs are complex and require a plethora of stakeholders to reduce risk behaviors,1 close gaps in SES, and raise community awareness about the diseases;36 studying the impact of SES, individual risk factors, peoples knowledge and attitude on NCDs can help policymakers, stakeholders, and health care providers to facilitate prevention programs effectively.
Bahir Dar, a city located in Northwest Ethiopia, is one of the fast growing and most populous cities in Ethiopia. Bahir Dar has a different sociodemographic composition population than other cities in the country, such as Addis Ababa. However, there is a lack of evidence about community level prevalence of NCDs and risk factors. There is also a lack of information about the knowledge and attitudes of the population about NCDs. To fill evidence gaps and inform decision making for appropriate NCD prevention, this study investigates three research questions: (1) what are the most commonly reported NCDs among adults in Bahir Dar? (2) what is the population level of knowledge and attitudes about NCDs? (3) What are the factors associated with the prevalence of NCD, multimorbidity, knowledge and attitudes in adults? We examined the association between various explanatory variables (SES, individual risk factors, knowledge about NCDs, attitudes about NCDs, and biomedical risk factors) and the prevalence of NCDs.
Materials and Methods
Study Design, Period, Setting, and Population
This community-based quantitative cross-sectional study is reported in line with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement.37 Data were collected between May 2021 and June 2021. This study focuses on the prevalence of NCDs, multimorbidity, population awareness and variations across adults’ SES, individual risk factors, knowledge, and attitude. The study was conducted in Bahir Dar town, Northwest Ethiopia, the capital city of Amhara regional state. Based on the 2007 Central Statistical Agency report, the town’s total population is 221,991.38 The city consists of six sub-cities with 17 administrative units (kebeles). The town has three public hospitals and ten primary health care centers.
The sample size (n = 423) of this study was calculated by using single population proportion formula (Za/22p(1-p)/d2), where “p” represents the prevalence of the outcome variable, “d” margin of error, and “Z” the statistical value of the normal distribution. The following values were used to calculate the sample size: a 50% prevalence rate, a Z-value of 1.96, a margin of error of 5%, and a 10% estimated non-response rate. We considered a 50% prevalence rate due to the absence of similar studies in the study area, thus maximizing the sample size estimation.
Participants in this study were sampled from adult residents in Bahir Dar town, by household (Figure 1). Using households as a sampling unit, data collectors started with a random household in each of the six sub-cities and progressed through a fixed interval (every 28 houses) to select the next household. This interval was estimated by dividing the total number of households (N = 12,000) by the calculated sample size (n = 423). One eligible participant from each selected household was invited to join the study. The inclusion criteria to participate in this study were adults between the ages of 18 and 65, being permanent residents (having lived in the town for at least six months), and who were able to provide the necessary information. If there were more than one eligible participant in the household, one was selected by lottery. Revisits were arranged for participants who were eligible but not available at home during the first research visit. However, if they were absent on the second visit, data collection moved to the adjacent house to invite an alternative study participant.
 |
Figure 1 Study household sampling and recruitment flow chart. |
The data collection was performed by four health care providers (nurses) after two days of training on how to interview participants and perform physical measurements. Data collectors practiced the questionnaire, measurements, and participant information sheet. Appropriate feedback was provided until everyone performed the measurements consistently. A research team collected data on a wide range of demographic, SES, individual risk factors, knowledge, attitude, and physical measurements during a home visit using a structured interviewer-administered questionnaire and anthropometric measuring tools. The questionnaire was adopted from the WHO steps risk factors surveillance tool39 and other similar studies assessing knowledge and attitudes about NCDs.40,41 We translated the questionnaire into Amharic (local language). We pretested the instrument in 5% of the sample size in a similar setting to assess participants’ response rate and clarity of the questions. Close supervision and monitoring were conducted throughout data collection by the primary investigator. The completeness and consistency of collected information and measurements were checked daily, and corrections were taken if errors were found before the next day’s activity.
Reporting of the prevalence of NCDs and participants’ knowledge and attitudes about NCDs are based on the following:
NCD Prevalence
The presence of NCD was assessed by the participant’s self-report to the question, “Have you been diagnosed by a health care professional with any of the following chronic diseases?” The list of NCDs included in the questionnaire are CVDs, diabetes mellitus, cancer, chronic respiratory diseases, chronic kidney diseases, hypertension, and “others” to capture others mentioned by the participant. These six diseases were selected because they are the most common NCDs in developing regions, accounting for more than 80% of cases.
NCD Knowledge
Adults were interviewed about their level of knowledge about NCDs. We first assessed adults’ general understanding about NCDs by asking the following “yes” or “no” question: “A non-communicable disease is one that cannot be spread between people?” After that, participants’ knowledge was assessed based on the following questions, “How much do you know about the following NCDs?” It was queried separately for hypertension, cardiovascular diseases, cancer, and diabetes. The response options for these questions include nothing at all, only heard the term before, know some about the disease, and know a lot about it. We considered a participant to have some knowledge about NCDs if they reported having some knowledge regarding each of the above four mentioned chronic diseases. Diabetes knowledge was further assessed using seven validated diabetes knowledge questions having three response options: true, false, or not sure. We summarized the participant’s correct answers for each question. Adults were considered knowledgeable if they correctly answered at least four of the seven questions.
NCD Attitude
First, the general attitude of adults about NCDs was assessed using the following Likert scale statement: “chronic non-communicable diseases are more dangerous than communicable diseases” having five response options: strongly agree, agree, neutral, disagree, and strongly disagree. Adults who responded, “strongly agree” or “agree”, were categorized together to describe adults’ attitudes towards NCDs as “more dangerous” than communicable diseases. We then assessed participants’ attitudes about specific NCDs, “Have you ever been concerned about developing chronic diseases such as CVDs and cancer?” These questions have three response options: “yes, often”, “yes, sometimes”, and “not at all”. These responses were later classified into two categories: yes (“yes, often” and “yes, sometimes”) and no (not at all) to describe participants’ concerns about the diseases.
The explanatory variables collected to examine their association with the prevalence of NCD, multimorbidity, knowledge, and attitude (outcome variables) are described in Table 1.
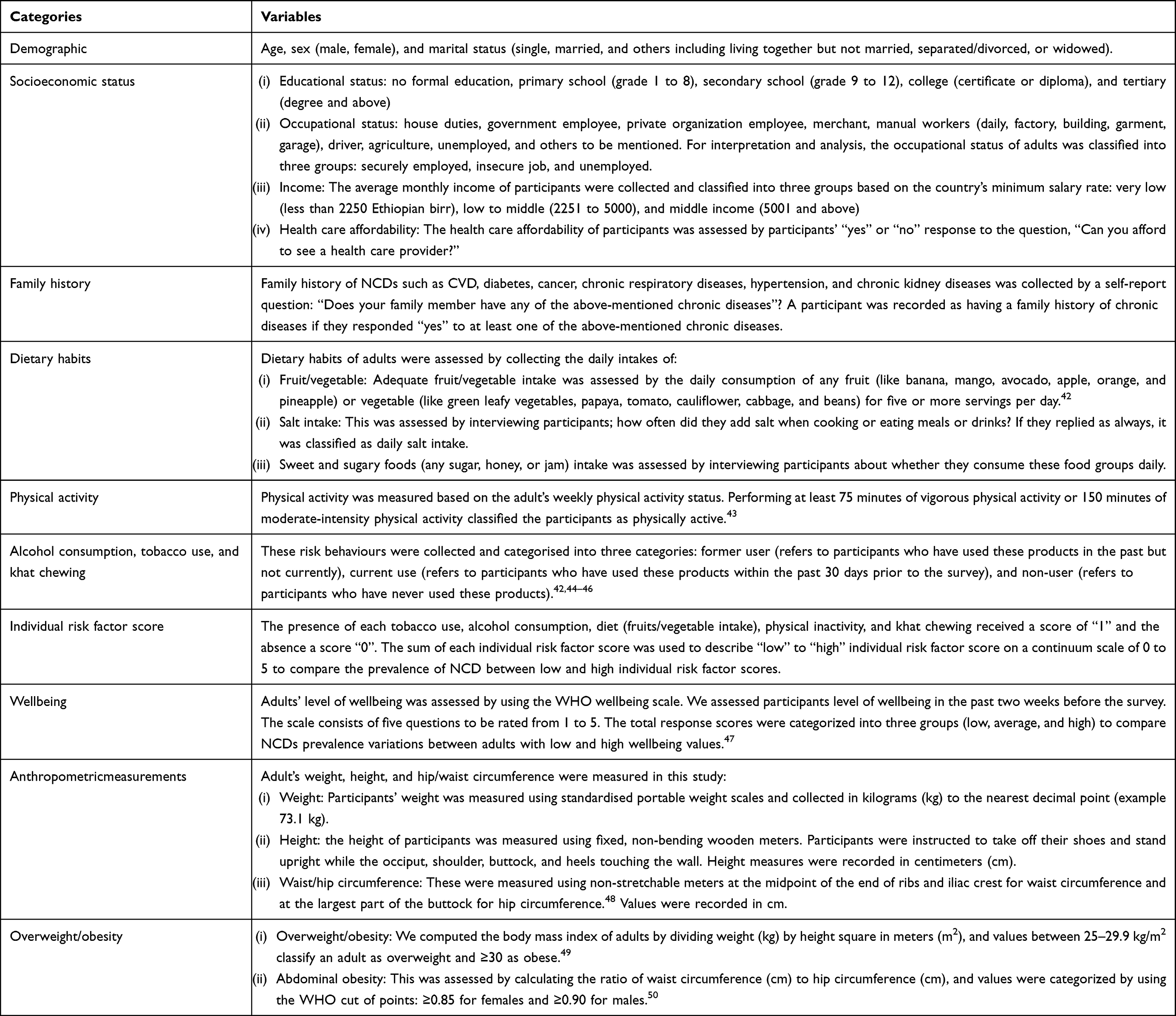 |
Table 1 Independent Variables and Measurements |
Statistical Analysis
Survey data were entered into Epi-data software version 3.1 and exported to SPSS (Statistical Package for Social Sciences) version 28 for analysis. We performed descriptive (frequencies and percentage) and inferential statistics (Chi-Square and logistic regression) to present the results of this study. The prevalence of NCDs, knowledge, and attitudes about NCDs are summarized using frequency and percentage. We categorized the number of NCDs reported by adults into three groups in line with previous studies:51–53 “0” free from NCDs, “1” have one form of NCD, and “2” have at least two types of NCDs. In order to describe the prevalence of NCDs, the reported numbers of NCDs are categorized into two groups: “yes” for adult’s having at least one form of NCD, and “no” for adults without NCD. To assess the prevalence of multimorbidity, these numbers are further categorized into two groups: “yes” for adults with two or more NCDs and “no” for adults without any NCD or those with only one type of chronic disease. The knowledge and attitudes of adults are categorized according to the criteria outlined earlier in this manuscript. We used Chi-square tests to explore NCD prevalence, multimorbidity, knowledge, and attitudes across adult’s demographic (age, sex, marital status), socioeconomic (education, occupation, income, health care affords), individual risk factors (diet, physical activity, alcohol intake, tobacco use, and khat chewing), and biomedical risk factors (overweight/obesity), and with other pertinent variables. We performed logistic regression analyses to identify significant predictors of NCD prevalence, multimorbidity, knowledge, and attitudes. We first examined associations between the explanatory variable and the outcome variables in the bivariable analysis. Variables that showed associations in the bivariable analysis were adjusted in the multivariable logistic regression to determine significant predictors of the outcome variables. For NCD prevalence and multimorbidity, demographic (age, marital status), socioeconomic (education, health care affords), individual risk factors (diet, alcohol), family history, weight status, NCD knowledge, and attitudes were adjusted in the multivariable logistic regression. To identify the significant predictors of NCD knowledge and attitudes, the final models were adjusted for demographic variables (age, sex, and marital status), socioeconomic factors (education, occupation, and income), and individual risk factors (physical inactivity, diet, salt intake, alcohol consumption, and khat use). We examined the presence of collinearity among the variables adjusted in each model, and variance inflation factors (VIF) of less than three were achieved for all variables for all models, indicating the absence of collinearity. The final models were checked for significant Omnibus tests of model coefficients (p<0.05) and non-significant Hosmer-Lemeshow goodness fit test (p>0.05). We used adjusted odds ratios with corresponding 95% confidence intervals (CI) to report the findings of the study and α significance level at a p-value of less than 0.05 as criteria to declare statistical significance.
Results
Non-Communicable Diseases by Socioeconomic and Individual Risk Factors
Out of all 423 visited houses having eligible participants, 417 adults agreed to participate in this study, making a response rate of 98.6%. Table 2 summarises participant’s sociodemographic characteristics and individual risk factors, and Figure 2 shows the prevalence of NCDs and multimorbidity.
 |
Table 2 Sociodemographic Characteristics of Participants, Individual Risk Factors, and Non-Communicable Disease |
 |
Figure 2 Prevalence of non-communicable diseases and multimorbidity. |
More than half (55%) of the participants in this study were female. The mean age of respondents was 35.6 ± 12.6 years, with 74.8% of participants aged 18 to 40. More than half of the participants were married (56.4%) and post-secondary educated (54.4%). The average monthly income of participants was 8574 ± 8776 Ethiopian birr per month, with 13.2% of adults being classified as having low income, less than 2250 birr per month. Above one-third (36.2%) of adults reported being unable to afford health care services. Forty percent of participants reported having a family history of chronic diseases: 3.4% of adults with a family history of cancer, 4.3% with CVDs, 11.3% with chronic respiratory diseases, 13.2% with diabetes, and 17.3% with hypertension.
From all participating adults in this study, 24% (n = 100) reported having one form of NCD, and 8% (n = 33) have multimorbidity. About 5.5% (n = 23) of adults reported having diabetes, 3.6% have COPD, 3.1% (n = 13) have CVD, 1.7% (n = 7) have cancer, and 16.1% (n = 67) have hypertension.
The distribution of NCDs and multimorbidity was higher in adults aged 56 years and above (p<0.01). NCDs were more commonly reported in married and uneducated adults (p<0.01). The prevalence of NCD was also higher in adults who said they could not afford health care costs (p<0.01); in adults with a family history of chronic diseases; with individual risk factors such as salt intake, sweet foods intake, and alcohol consumption; and with biomedical factors like overweight/obesity (p<0.01).
Knowledge and Attitude
Table 3 summarises the knowledge and attitudes of adults about NCDs. Most adults (87%) know that NCDs are chronic diseases that do not spread between people, and 76% of participants perceive that NCDs are more dangerous than communicable diseases. Most (70%) participants reported having some knowledge about hypertension; 94% of adults knew that hypertension could have negative health consequences, and 91% appreciated the importance of regular blood pressure checkups. About 54% of adults know something about CVDs, although 21% of participants did not know whether they are preventable, and 62% of adults have never been concerned about developing CVDs. Fifty-five percent of adults know something about cancer, and 73% of participants know something about diabetes. However, 25% of adults did not know whether diabetes could be preventable Only one-third (34.5%) of participating adults have some overall knowledge about NCDs. The prevalence of NCD was lower in adults who have some knowledge about NCDs (17%) than in adults who have not (29%) (p=0.02).
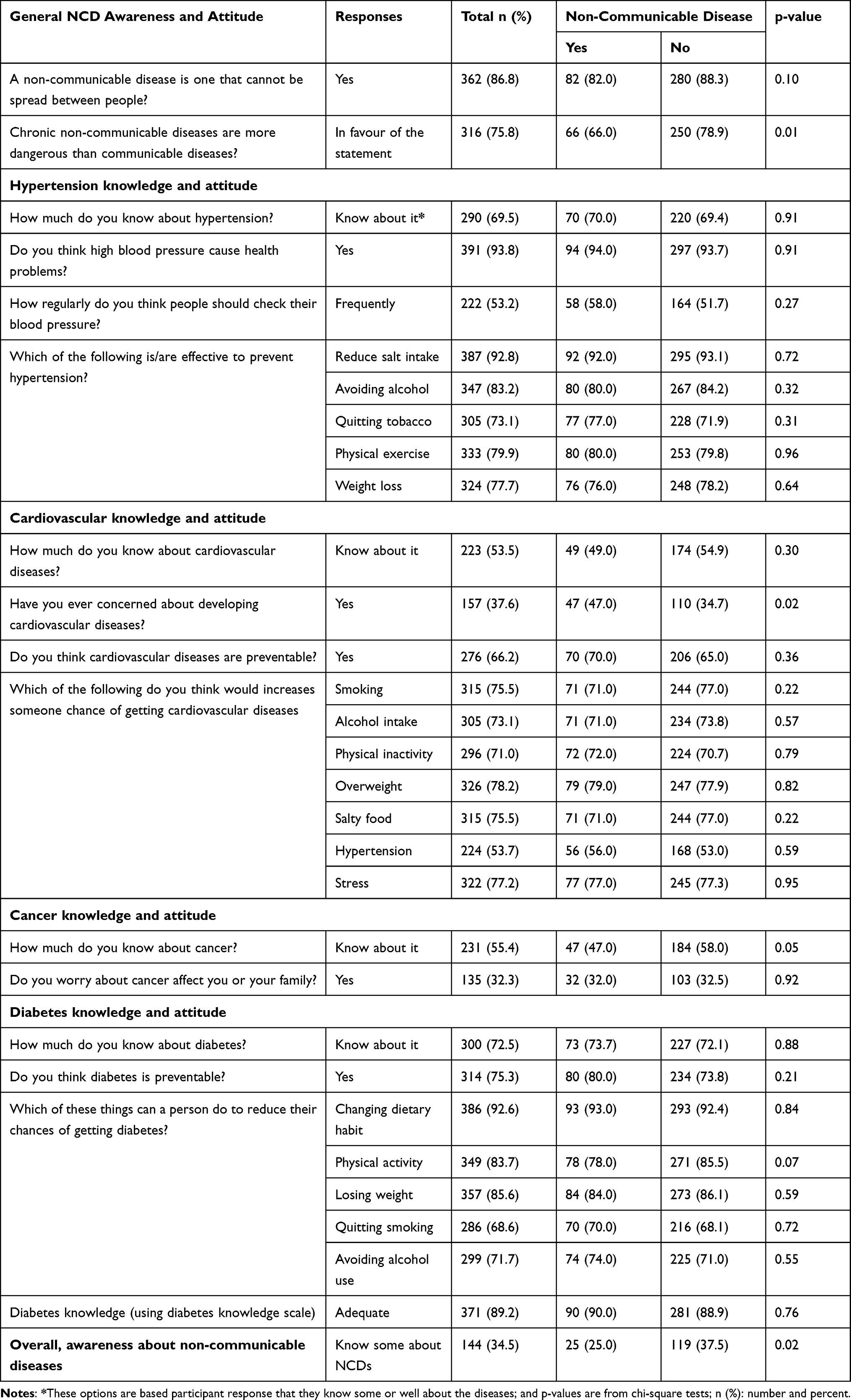 |
Table 3 Knowledge and Attitudes of Participants About Selected Non-Communicable Diseases |
Factors Associated with the Prevalence of NCD
The final predictors for the prevalence of NCD are age, family history of chronic diseases, and the weight status of adults—the results are presented in Table 4.
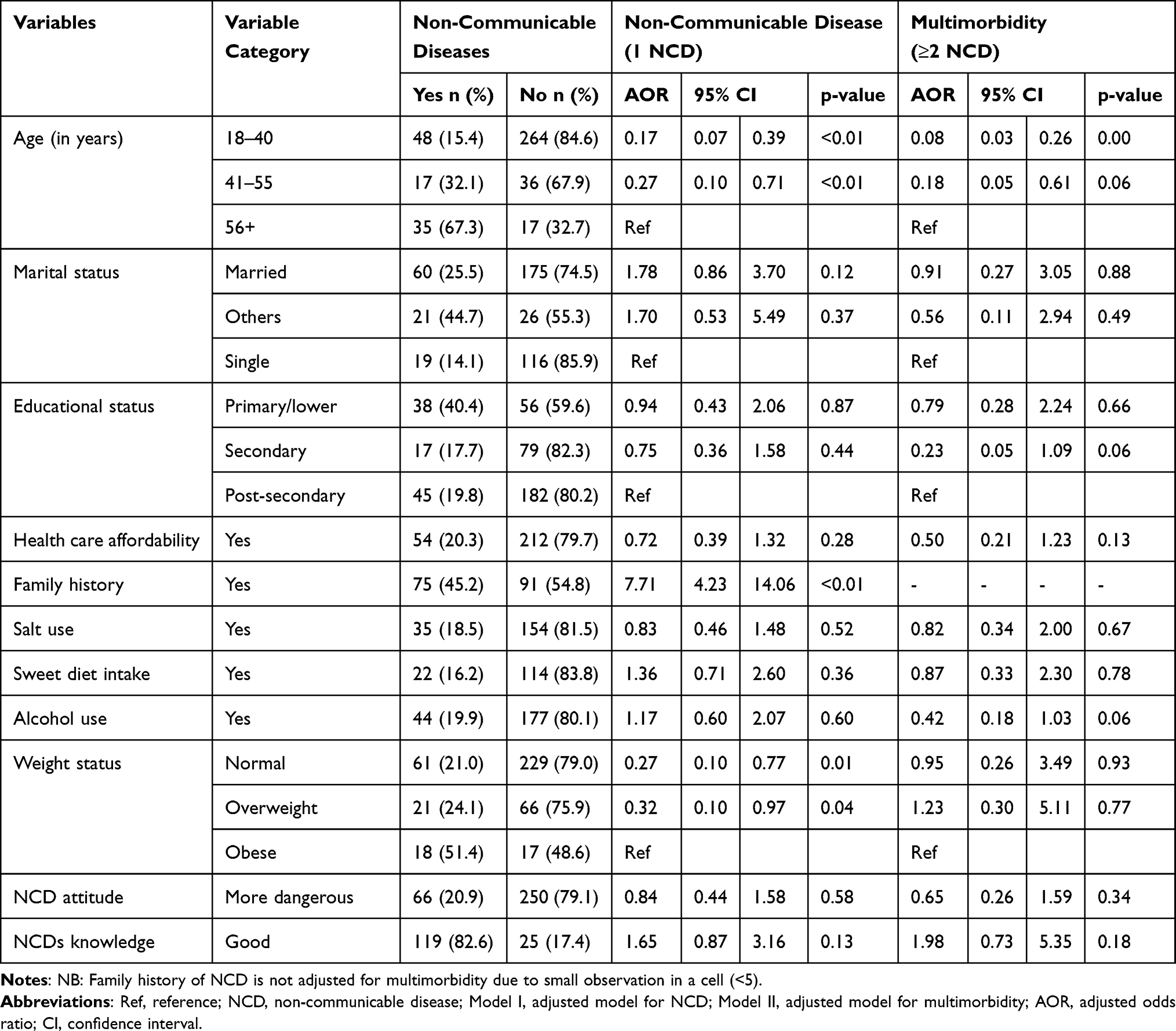 |
Table 4 Adjusted Odds Ratio (AOR) and 95% Confidence Intervals for Multivariable Logistic Regression for NCD Prevalence and Multimorbidity |
The age of participants is significantly associated with the prevalence of NCD. Adults who were between the ages of 18 and 40 years are 83% less likely to have NCD than adults aged 56 years and above (AOR 0.17, 95% CI 0.07 to 0.39), and adults between the ages of 40 and 55 are 73% less likely to have NCD than adults aged 56 and above (AOR 0.27, 95% CI 0.10 to 0.71). Multimorbidity of NCDs is less likely to be reported in adults younger than 40 than adults aged 56 years and above (AOR 0.08, 95% CI 0.03 to 0.26).
A family history of chronic diseases is significantly associated with NCD prevalence. Adults with a family history of chronic disease are almost eight times more likely to have an NCD than adults without a family history of chronic disease (AOR 7.71, 95% CI 4.23 to 14.06).
Adult weight status is significantly associated with the prevalence of NCDs. Normal-weight adults are 73% less likely to have NCD than obese adults (AOR 0.27, 95% CI 0.10 to 0.77), and overweight adults are 68% lower to have NCD than obese adults (AOR 0.32, 95% CI 0.10 to 0.97).
Factors Associated with NCD Knowledge and Attitude
The final predictors for NCD knowledge are: the sex and occupational status of adults; for NCD attitude: weight status, and alcohol use; and occupational status for diabetes knowledge—the results are summarised in Table 5.
 |
Table 5 Adjusted Odds Ratio (AOR) and 95% Confidence Intervals for Multivariable Logistic Regression for NCD Knowledge, Diabetes Knowledge, and Attitude |
The sex of participants is significantly associated with the level of NCD knowledge. Male adults are almost two times more likely to have some knowledge about NCDs compared to female adults (AOR 1.76 95% CI 1.06 to 2.93). The occupational status of adults is also significantly associated with the level of NCD knowledge. Employed adults are almost three times more likely to have NCD knowledge than adults with insecure jobs (AOR 2.91, 95% CI 1.52 to 5.57); Employed adults are also three times more likely to have diabetes knowledge than their counterparts (AOR 3.41, 95% CI 1.07 to 10.82).
NCD attitude is significantly associated with the weight status and alcohol use of adults. Normal-weight adults are three times more likely to express NCDs as dangerous than obese adults (AOR 3.23, 95% CI 1.42 to 7.39), and adults who use alcohol consider NCDs more dangerous than infectious diseases compared to non-drinkers (AOR 1.85, 95% CI 1.08 to 3.14).
Discussion
This study generates new evidence on the prevalence of NCDs, multimorbidity, and population awareness among adult residents in Bahir Dar, which will have a remarkable contribution to design appropriated prevention and control programs tailored to the population. The study evaluates associations with various independent variables (demographic, socioeconomic, individual risk factors, and biomedical risk factors). Age, family history, and presence of overweight/obesity are significant predictors for the prevalence of NCD; sex and occupational status for NCD knowledge; and weight status and alcohol use for NCD attitude.
The prevalence of NCD among adults in the study population was 24%: 16.1% hypertension, 5.5% diabetes, 3.6% COPDs, 3.5% CVDs, and 1.7% cancer. In 2018 WHO reported almost similar prevalence of NCD in the country (CVDs 16%, cancer 7%, COPD 2%, and diabetes 2%),54 and the recent systematic review of NCDs in Ethiopia reported the total NCD prevalence ranges from 29 to 35%; CVD from 13 to 32%; cancer from 4 to 18%; the pooled prevalence of diabetes is 5%; and COPD ranges between 1 and 18%,55 but the current prevalence is higher than prevalence reports in Southwest Ethiopia (diabetes 0.5%, hypertension 3%, CVDs 3%, and COPDs 2%)56 and from a total NCD prevalence (2%) in Northwest Ethiopia.57 The difference might be due to variations over time and the participants’ demographic and economic characteristics.5 The previous studies were conducted with semi-urban and rural residents, while the current study involved only urban adults, which might increase risk factors like insufficient physical activity and dietary risks.58,59 The country is also undergoing demographic transitions,15 meaning that the proportion of the adult population is growing, which could increase the prevalence of some behavioral risk factors, such as alcohol consumption and tobacco use.60,61 The presence of multiple triggers in the country, such as high unemployment rates, poverty, conflicts, and instability, might also increase the prevalence of these diseases.62,63 This study also showed that the prevalence of multimorbidity of NCDs was 8% which is lower than reports in other countries, such as 16% in China53 and 30.2% in Serbia.52 This could be due to differences in population demography (age distribution), economy, health care service accessibilities, and variations in disease burden between the referenced countries and the study population.
The prevalence of NCD and multimorbidity are directly associated with the age of adults in this study. Despite differences in the method of analyses used, previous findings in Northern Ethiopia,64 studies in Brazil and Canada,65,66 and research based in low- middle- and high-income countries show that the prevalence of NCDs has a direct association with the age of participants.29,67 NCDs are developed progressively over time. They are cumulative effects of multiple exposures, such as early developmental exposure to malnutrition, environmental risk factors, infectious diseases, poverty, and individual risk factors.7,68 The chance of exposure to behavioral risk factors that are attributable to cause NCD, like alcohol consumption and physical inactivity,69 and metabolic risks such as overweight/obesity and hypertension are also directly associated with the age of participants.70 Our exploratory analysis presented in Supplementary Tables 1 and 2 shows that the age of adults is associated with employment status, family history of NCD, salt intake, alcohol consumption, khat use, and overweight and obesity; and with cardiovascular health concerns, cancer knowledge, physical activity, all which could augment the influence of age on the prevalence of NCD.
Family history of chronic diseases is a strong predictor of the prevalence of NCD among adults in the current study. Chronic diseases such as diabetes and CVD have strong genetic predispositions.71,72 The combination of genetic, physiological, environmental, and individual risk factors facilitates the development of chronic diseases.68 Risk behaviors like poor dietary habits also cluster in families;73 if a family practices unhealthy dietary habits, the offspring have a higher chance of following unhealthy dietary habits.74,75 This also applies to other risk behaviors such as alcohol consumption and tobacco use.76,77
The presence of overweight/obesity is significantly associated with the prevalence of NCD among adults. Excess weight gain alters normal body physiology in various ways by increasing the chance of insulin resistance at skeletal muscles, which leads to impaired glucose homeostasis and diabetes.78,79 When glucose metabolism is affected, excess glucose and fat metabolites are accumulated in the blood vessels. This causes the narrowing of blood vessels and atherosclerosis, which increases the risk of hypertension, CVDs, and stroke.78,79 Overweight/obesity worsens the outcome of chronic diseases, such as COPD and cancer.80–82 Risks associated with excess weight gain will continue to be a huge burden in developing countries unless appropriate attention is given.83,84 Exploration of significant variables presented in Supplementary Tables 1 and 2 shows that overweight and obesity are associated with adult health care affordability, salt intake, sweet food intake, NCD knowledge, and attitude, which may explain the effects of overweight and obesity on the prevalence of chronic diseases.
This study reveals that only one-third of adults in the study population have some knowledge about NCDs. This is lower than the 81% reported NCD knowledge in Malaysia,85 56% CVD knowledge in Nepal,86 but comparable to studies done in African countries such as <50% NCD knowledge in Cameroon,87 23% NCD knowledge in Kenya,35 and 32% CVD knowledge in university students in Ethiopia;88 and with the 27% diabetes knowledge in Kenya,89 and 56% diabetes knowledge in Southern Ethiopia.90 Overall, people in low-income countries, like in sub-Saharan African regions, have inadequate knowledge about chronic NCDs, such as cardiovascular diseases.91 The current study found that employed and male adults have better NCD knowledge than their counterparts. This might be because employed people are more educated and more likely to be exposed to health information and healthy lifestyles at work and in the media, consistent with studies that showed a strong correlation between employment status and health literacy.92,93 In Ethiopia, men are more educated and employed than women, which undeniably impacts all-rounded health knowledge.94
This study shows that three-quarters of adults consider NCDs more dangerous than communicable diseases. This finding is higher compared to the 53% NCD attitude in Malaysia,85 20% CVD attitude in Nepal,86 <50% in Cameroon,87 and 39% in Kenya.35 The multivariable logistic regression analysis reveals that overweight/obese adults have lower concerns about NCDs than normal adults. This could be due to people in low-income countries preferring to be overweight, as some associate it with beauty and wealth95,96 and are less concerned about its health effects.97
Overall, the findings of this study can help public health professionals, health offices, and concerned stakeholders to plan targeted health interventions for older adults, people with a family history of chronic diseases, and having excess weight gain to reduce NCD burden; and for women and adults with insecure jobs to raise NCD knowledge, and to obese adults to raise NCD attitude.
Strengths and Limitations of the Study
This study provides relevant information about the community-level prevalence of NCD in a developing country and explores the prevalence using various population characteristics: demographic, SES, individual risk factors, knowledge, and attitudes. Nevertheless, the study has the following limitations: 1) prevalence estimates are based on self-report of adults, not laboratory tests, and might have underestimated the actual prevalence;98 2) some of the explanatory variables, like health care affordability, were self-rated by adults and might be subject to social desirability bias; 3) although data collectors received rigorous training and close supervision during the conduct of the study for collecting anthropometric measurements (such as height, weight, and hip/waist circumference), a risk of some measurement bias remains; 4) although our sample size was met, the strength of our estimates might be limited and apparent in variables with wider confidence intervals;99,100 5) this study might have involved prevalence-incidence (Neyman) bias;101,102 6) causal inference is limited due to the cross-sectional nature of the study;103 7) the study only involved urban residents in Bahir Dar in Northwest Ethiopia, although the age and sex structure of the population is similar to the general population of the country, prevalence estimates might be influenced by the effects of urbanization and cannot reflect the reality of rural areas; and 8) the study was conducted in Bahir Dar town Northwest Ethiopia thus generalizing the findings to the whole Ethiopian adults and beyond needs cautious interpretation.
Conclusion
This study reveals a high prevalence of NCDs and overall low NCD awareness amongst participating adults in Bahir Dar, Ethiopia; one in four have an NCD, and one in ten have multimorbidity. One-third of adults have some NCD knowledge and 75% consider NCDs to be more dangerous than communicable diseases. Amongst those aged over 55, this increases to more than 32% for NCD prevalence and multimorbidity. Age above 55 years, family history of NCD, and overweight or obese weight categories are significant predictors for the prevalence of NCD. Male and employed adults have better NCD knowledge, while normal weight status and alcohol use of adults for NCD attitude.
Data Sharing Statement
All data relevant to this study are included in the manuscript.
Ethics Approval and Informed Consent
This study methods and procedures were performed in accordance with the Helsinki Declaration for biomedical research. This study received ethics approval from the Australian National University Human Research Ethics Committee (protocol number 2020/558) and local approval from the Amhara Public Health Institute Research Ethics Committee (protocol number 1/10523), Bahir Dar, Ethiopia. Informed written consent was obtained from participants prior to starting data collection. For participants who could not read and write, informed oral consent was obtained. The data collectors read the information sheet to these types of participants and for those who agreed to participate, their response was recorded in the oral consent form prepared for this purpose. The oral consent form included information such as the title of the project, information that the participant is provided with clear information about the aims of the research, confidentiality of the collected information, and the data collection date. All these procedures were approved by the above-mentioned ethics committees.
Acknowledgments
We thank the Bahir Dar city administration and health offices, data collectors, and Bahir Dar city residents for their cooperation and support during the conduct of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization. Noncommunicable Diseases. Geneva: WHO; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
2. Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Global Health. 2019;7(10):e1295–e6.
3. Tesema AG, Ajisegiri WS, Abimbola S, et al. How well are non-communicable disease services being integrated into primary health care in Africa: a review of progress against World Health Organization’s African regional targets. PLoS One. 2020;15(10):e0240984.
4. Beran D, Pedersen HB, Robertson J. Noncommunicable diseases, access to essential medicines and universal health coverage. Glob Health Action. 2019;12(1):1670014.
5. Allen L, Williams J, Townsend N, et al. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: a systematic review. Lancet Global Health. 2017;5(3):e277–e89.
6. Frumkin H, Haines A. Global environmental change and noncommunicable disease risks. Annu Rev Public Health. 2019;40:261–282.
7. Allen L, Williams J, Townsend N, et al. Poverty and risk factors for non-communicable diseases in developing countries: a systematic review. Lancet. 2016;388:S17.
8. Murphy A, Palafox B, Walli-Attaei M, et al. The household economic burden of non-communicable diseases in 18 countries. BMJ Global Health. 2020;5(2):e002040.
9. Jan S, Laba T-L, Essue BM, et al. Action to address the household economic burden of non-communicable diseases. Lancet. 2018;391(10134):2047–2058.
10. Kundu MK, Hazra S, Pal D, Bhattacharya M. A review on Noncommunicable Diseases (NCDs) burden, its socio-economic impact and the strategies for prevention and control of NCDs in India. Indian J Public Health. 2018;62(4):302. doi:10.4103/ijph.IJPH_324_16
11. Kazibwe J, Tran PB, Annerstedt KS. The household financial burden of non-communicable diseases in low- and middle-income countries: a systematic review. Health Res Policy Systems. 2021;19(1):96. doi:10.1186/s12961-021-00732-y
12. Price AJ, Crampin AC, Amberbir A, et al. Prevalence of obesity, hypertension, and diabetes, and cascade of care in sub-Saharan Africa: a cross-sectional, population-based study in rural and urban Malawi. Lancet Diabetes Endocrinol. 2018;6(3):208–222. doi:10.1016/S2213-8587(17)30432-1
13. Niessen LW, Mohan D, Akuoku JK, et al. Tackling socioeconomic inequalities and non-communicable diseases in low-income and middle-income countries under the Sustainable Development agenda. Lancet. 2018;391(10134):2036–2046. doi:10.1016/S0140-6736(18)30482-3
14. Kien VD, Van Minh H, Giang KB, Dao A, Ng N. Socioeconomic inequalities in catastrophic health expenditure and impoverishment associated with non-communicable diseases in urban Hanoi. Vietnam Int J Equity Health. 2016;15(1):1–11.
15. Admassie A, Nuru Ali S, May JF, Megquier S, Moreland S. The Demographic Dividend: An Opportunity for Ethiopia’s Transformation. Avaialble at. Washington, DC: Population Reference Bureau and Ethiopian Economics Association; 2015. Available from: https://www.prb.org/wp-content/uploads/2015/11/demographic-dividend-ethiopia.pdf.
16. Misganaw A, Haregu TN, Deribe K, et al. National mortality burden due to communicable, non-communicable, and other diseases in Ethiopia, 1990–2015: findings from the Global Burden of Disease Study 2015. Population Health Metrics. 2017;15(1):1–17
17. Zimmet PZ, Alberti KGMM. Introduction: globalization and the non-communicable disease epidemic. Obesity. 2006;14(1):1. doi:10.1038/oby.2006.1
18. Juma K, Juma PA, Shumba C, Otieno P, Asiki G. Non-communicable diseases and urbanization in African cities: a narrative review. Public Health Dev Countries Challenges Opportunities. 2019;2:31–50.
19. Misganaw A, Naghavi M, Walker A, et al. Progress in health among regions of Ethiopia, 1990–2019: a subnational country analysis for the Global Burden of Disease Study 2019. Lancet. 2022;399(10332):1322–1335.
20. The World Bank. Population, total, Ethiopia. Avaialble from: https://data.worldbank.org/indicator/SP.POP.TOTL?locations=ET.
21. Workie NW, Ramana GN. The health extension program in Ethiopia. 2013.
22. Bosu WK. An overview of the nutrition transition in West Africa: implications for non-communicable diseases. Proce Nutrition Soc. 2015;74(4):466–477.
23. Popkin BM. The nutrition transition in the developing world. Dev Policy Rev. 2003;21(5‐6):581–597.
24. Mbogori T, Mucherah W. Nutrition transition in Africa: consequences and opportunities. Global J Transformative Educ. 2019;1(1):5–10.
25. The World Bank. Cause of death by non-communicable diseases (% of total)- Ethiopia. Available from: https://data.worldbank.org/indicator/SH.DTH.NCOM.ZS?locations=ET.
26. Organization WH. Noncommunicable Diseases Country Profiles 2018; 2018.
27. Fenta EH, Sisay BG, Gebreyesus SH, Endris BS. Trends and causes of adult mortality from 2007 to 2017 using verbal autopsy method, Addis Ababa, Ethiopia. BMJ open. 2021;11(11):e047095.
28. Ethiopian Public Health Institute. Ethiopia STEPS report on risk factors for non-communicable diseases and prevalence of selected NCDs. Ethiopian Public Health Institute; 2016.
29. Williams J, Allen L, Wickramasinghe K, Mikkelsen B, Roberts N, Townsend N. A systematic review of associations between non-communicable diseases and socioeconomic status within low-and lower-middle-income countries. J Glob Health. 2018;8(2):e4.
30. Lago-Peñas S, Rivera B, Cantarero D, et al. The impact of socioeconomic position on non-communicable diseases: what do we know about it? Perspect Public Health. 2021;141(3):158–176.
31. Omran A-R. The epidemiologic transition: a theory of the epidemiology of population change/Abdel R. Omran. 2001.
32. Caldwell JC. Health transition: the cultural, social and behavioural determinants of health in the Third World. Soc Sci Med. 1993;36(2):125–135.
33. Hosseinpoor AR, Bergen N, Mendis S, et al. Socioeconomic inequality in the prevalence of noncommunicable diseases in low-and middle-income countries: results from the World Health Survey. BMC Public Health. 2012;12(1):1–13.
34. Boakye J, Mensah D, Sakhuja S, Jolly PE, Akinyemiju T. Socioeconomic disparities in the prevalence of cardiometabolic risk factors in Ghanaian women. Ann Global Health. 2017;83(3–4):423–431.
35. Temu TM, Kirui N, Wanjalla C, et al. Cardiovascular health knowledge and preventive practices in people living with HIV in Kenya. BMC Infect Dis. 2015;15(1):421.
36. Ikeda N, Saito E, Kondo N, et al. What has made the population of Japan healthy? Lancet. 2011;378(9796):1094–1105.
37. STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies. Availabe from: https://www.equator-network.org/wpcontent/uploads/2015/10/STROBE_checklist_v4_cross-sectional.pdf.
38. Central Statistical Authority. Population and Housing Census of Ethiopia. Addis Ababa: Central Statistics Authority; 2007.
39. Organization WH WHO STEPS instrument (core and expanded). Geneva, Switzerland: WHO: Available from: http://www.whoint/chp/steps/STEPS_Instrument_v2.2015;1.
40. Demaio AR, Dugee O, Amgalan G, et al. Protocol for a national, mixed-methods knowledge, attitudes and practices survey on non-communicable diseases. BMC Public Health. 2011;11(1):961.
41. Salwa M, Haque MA, Khalequzzaman M, Al Mamun MA, Bhuiyan MR, Choudhury SR. Towards reducing behavioral risk factors of non-communicable diseases among adolescents: protocol for a school-based health education program in Bangladesh. BMC Public Health. 2019;19(1):1002.
42. WHO STEPS Surveillance Manual. The WHO STEPwise Approach to Noncommunicable Disease Risk Factor Surveillance. Geneva: World Health Organization; 2020. Available from: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps/manuals.
43. World Health organization. Global Recommendations on Physical Activity for Health. Geneva: WHO; 2011.
44. Reda AA, Kotz D, Biadgilign S. Adult tobacco use practice and its correlates in eastern Ethiopia: a cross-sectional study. Harm Reduct J. 2013;10(1):1–6.
45. Gizaw AT, Amdisa D, Lemu YK. Predictors of substance use among Jimma University instructors, Southwest Ethiopia. Subst Abuse Treat Prev Policy. 2020;15(1):1–10.
46. Alebachew W, Semahegn A, Ali T, Mekonnen H. Prevalence, associated factors and consequences of substance use among health and medical science students of Haramaya University, eastern Ethiopia, 2018: a cross-sectional study. BMC Psychiatry. 2019;19(1):1–9.
47. Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychother Psychosom. 2015;84(3):167–176. doi:10.1159/000376585
48. WHO. Noncommunicable Disease Surveillance, Monitoring and Reporting; STEPS Manual. Avialable at https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps/manuals.
49. World Health Organisation. Obesity and Overweight. Geneva: WHO; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
50. OMS. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications. Report of a WHO Consultation 1999. Geneve: OMS; 1999.
51. Camacho PA, Gomez-Arbelaez D, Otero J, et al. Self-reported prevalence of chronic non-communicable diseases in relation to socioeconomic and educational factors in Colombia: a community-based study in 11 departments. Glob Heart. 2020;15(1):546.
52. Jankovic J, Mirkovic M, Jovic-Vranes A, Santric-Milicevic M, Terzic-Supic Z. Association between non-communicable disease multimorbidity and health care utilization in a middle-income country: population-based study. Public Health. 2018;155:35–42.
53. Li X, Cai L, W-l C, et al. Association of socioeconomic and lifestyle factors with chronic non-communicable diseases and multimorbidity among the elderly in rural southwest China. J Public Health (Bangkok). 2020;42(2):239–246.
54. World Health Organization. Noncommunicable Diseases Country Profiles 2018; 2018.
55. Tesfay FH, Zorbas C, Alston L, Backholer K, Bowe SJ, Bennett CM. Prevalence of chronic non-communicable diseases in Ethiopia: a systematic review and meta-analysis of evidence. Front Public Health. 2022;10.
56. Muluneh AT, Haileamlak A, Tessema F, et al. Population based survey of chronic non-communicable diseases at gilgel gibe field research center, southwest Ethiopia. Ethiop J Health Sci. 2012;22(4):7–18.
57. Abebe SM, Andargie G, Shimeka A, et al. The prevalence of non-communicable diseases in northwest Ethiopia: survey of Dabat Health and Demographic Surveillance System. BMJ open. 2017;7(10):e015496.
58. Allender S, Lacey B, Webster P, et al. Level of urbanization and noncommunicable disease risk factors in Tamil Nadu, India. Bull World Health Organ. 2010;88:297–304.
59. Goryakin Y, Rocco L, Suhrcke M. The contribution of urbanization to non-communicable diseases: evidence from 173 countries from 1980 to 2008. Econ Hum Biol. 2017;26:151–163.
60. Khademi N, Babanejad M, Asadmobini A, Karim H. The association of age and gender with risk factors of noncommunicable diseases among employees in West of Iran. Int J Prev Med. 2017;8:46.
61. Motuma A, Demissie Regassa L, Gobena T, Teji Roba K, Berhane Y, Worku A. Almost all working adults have at least one risk factor for non-communicable diseases: survey of working adults in Eastern Ethiopia. PLoS One. 2022;17(2):e0264698.
62. Shimeles A. Growth, poverty, and distribution in Ethiopia. Oxford Handbook Ethiopian Economy. 2019;3:653.
63. World Report 2021: Ethiopia Human Watch. Available from: https://www.hrw.org/world-report/2021/country-chapters/ethiopia.
64. Abera SF, Gebru AA, Biesalski HK, et al. Social determinants of adult mortality from non-communicable diseases in northern Ethiopia, 2009-2015: evidence from health and demographic surveillance site. PLoS One. 2017;12(12):e0188968.
65. Roberts K, Rao D, Bennett T, Loukine L, Jayaraman G. Prevalence and patterns of chronic disease multimorbidity and associated determinants in Canada. Health Promotion Chronic Dis Prevent Canada. 2015;35(6):87.
66. Malta DC, Bernal RTI, de Souza M, Szwarcwald CL, Lima MG, de Azevedo Barros MB. Social inequalities in the prevalence of self-reported chronic non-communicable diseases in Brazil: national health survey 2013. Int J Equity Health. 2016;15(1):153.
67. Dagenais GR, Gerstein HC, Zhang X, et al. Variations in diabetes prevalence in low-, middle-, and high-income countries: results from the prospective urban and rural epidemiological study. Diabetes Care. 2016;39(5):780–787.
68. Barouki R, Gluckman PD, Grandjean P, Hanson M, Heindel JJ. Developmental origins of non-communicable disease: implications for research and public health. Environ Health. 2012;11(1):1–9.
69. Gaskin CJ, Orellana L. Factors associated with physical activity and sedentary behavior in older adults from six low-and middle-income countries. Int J Environ Res Public Health. 2018;15(5):908.
70. Alamnia TT, Tesfaye W, Abrha S, Kelly M. Metabolic risk factors for non-communicable diseases in Ethiopia: a systematic review and meta-analysis. BMJ open. 2021;11(11):e049565.
71. Iloh GUP, Chuku A, Obiegbu NP, Ofoedu JN, Ikwudinma AO. Frequency of cardiovascular risk factors in adult Nigerians with family history of non-communicable cardiovascular disease in a primary care clinic of a tertiary hospital in a resource-constrained environment of Eastern Nigeria. Am J Health Res. 2013;1(1):17–25.
72. Ranasinghe P, Cooray DN, Jayawardena R, Katulanda P. The influence of family history of hypertension on disease prevalence and associated metabolic risk factors among Sri Lankan adults. BMC Public Health. 2015;15(1):1–9.
73. Yang W, Burrows T, MacDonald‐Wicks L, Williams L, Collins C, Chee W. The Family Diet Study: a cross‐sectional study into the associations between diet, food habits and body weight status in M alay families. J Human Nutrition Dietetics. 2016;29(4):441–448.
74. Tol A, Mohebbi B, Sadeghi R. Evaluation of dietary habits and related factors among type 2 diabetic patients: an innovative study in Iran. J Educ Health Promot. 2014;3.
75. Mahmood L, Flores-Barrantes P, Moreno LA, Manios Y, Gonzalez-Gil EM. The influence of parental dietary behaviors and practices on children’s eating habits. Nutrients. 2021;13(4):1138.
76. Tully LK, Correa JB, Doran N. The relationship between family history of tobacco use and progression to tobacco use among young adult e-cigarette users. Prevent Medi Rep. 2019;15:100914.
77. Warner LA, White HR, Johnson V. Alcohol initiation experiences and family history of alcoholism as predictors of problem-drinking trajectories. J Stud Alcohol Drugs. 2007;68(1):56–65.
78. Pradhan A. Obesity, metabolic syndrome, and type 2 diabetes: inflammatory basis of glucose metabolic disorders. Nutr Rev. 2007;65(suppl_3):S152–S6.
79. Jallut D, Golay A, Munger R, et al. Impaired glucose tolerance and diabetes in obesity: a 6-year follow-up study of glucose metabolism. Metabolism. 1990;39(10):1068–1075.
80. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–591.
81. Arnold M, Leitzmann M, Freisling H, et al. Obesity and cancer: an update of the global impact. Cancer Epidemiol. 2016;41:8–15.
82. Poulain M, Doucet M, Major GC, et al. The effect of obesity on chronic respiratory diseases: pathophysiology and therapeutic strategies. Cmaj. 2006;174(9):1293–1299.
83. Kilpi F, Webber L, Musaigner A, et al. Alarming predictions for obesity and non-communicable diseases in the Middle East. Public Health Nutr. 2014;17(5):1078–1086.
84. Agyemang C, Boatemaa S, Frempong GA, Aikins A. Obesity in Sub-Saharan Africa. Metabolic Syndrome. Switzerland: Springer International Publishing; 2016:1–13.
85. Ithnin M, Nor NAUM, Nordin NJ, et al. Knowledge, attitude, and practice on Non-Communicable Diseases (NCDs) among the adult population in the urban area of Negeri Sembilan, Malaysia. Int J Res Pharm Sci. 2018;9(SPL 2):88–94.
86. Vaidya A, Aryal UR, Krettek A. Cardiovascular health knowledge, attitude and practice/behaviour in an urbanising community of Nepal: a population-based cross-sectional study from Jhaukhel-Duwakot Health Demographic Surveillance Site. BMJ open. 2013;3(10):e002976.
87. Aminde LN, Takah N, Ngwasiri C, et al. Population awareness of cardiovascular disease and its risk factors in Buea, Cameroon. BMC Public Health. 2017;17(1):545.
88. Abdela OA, Ayalew MB, Yesuf JS, et al. Ethiopian university students’ knowledge and perception towards cardiovascular disease risk factors: a cross sectional study. Am J Cardiovasc Dis. 2019;9(1):1.
89. Maina WK, Ndegwa ZM, Njenga EW, Muchemi EW. Knowledge, attitude and practices related to diabetes among community members in four provinces in Kenya: a cross-sectional study. Pan Af Med J. 2010;7(1):e0170040.
90. Kassahun CW, Mekonen AG. Knowledge, attitude, practices and their associated factors towards diabetes mellitus among non diabetes community members of Bale Zone administrative towns, South East Ethiopia. A cross-sectional study. PLoS One. 2017;12(2):76.
91. Boateng D, Wekesah F, Browne JL, et al. Knowledge and awareness of and perception towards cardiovascular disease risk in sub-Saharan Africa: a systematic review. PLoS One. 2017;12(12):e0189264.
92. Svendsen IW, Damgaard MB, Bak CK, et al. Employment status and health literacy in Denmark: a population-based study. Int J Public Health. 2021;66:598083.
93. Furuya Y, Kondo N, Yamagata Z, Hashimoto H. Health literacy, socioeconomic status and self-rated health in Japan. Health Promot Int. 2015;30(3):505–513.
94. Denu B, Tekeste A, Van Der Deijl H. Characteristics and determinants of youth unemployment, underemployment and inadequate employment in Ethiopia. Employment Strategy Papers. 2005.
95. Manafe M, Chelule PK, Madiba S. The Perception of Overweight and Obesity among South African Adults: implications for Intervention Strategies. Int J Environ Res Public Health. 2022;19(19):12335.
96. Agyapong NAF, Annan RA, Apprey C, Aduku LNE. Body weight, obesity perception, and actions to achieve desired weight among rural and urban Ghanaian Adults. J Obes. 2020;2020:46.
97. Faber M, Kruger HS. Dietary intake, perceptions regarding body weight, and attitudes toward weight control of normal weight, overweight, and obese black females in a rural village in South Africa. Ethn Dis. 2005;15(2):238–245.
98. Kämpfen F, Wijemunige N, Evangelista B. Aging, Non-Communicable Diseases, and Old-Age Disability in Low-and Middle-Income Countries: A Challenge for Global Health. Springer; 2018:1011–1012.
99. Tzeng IS. To handle the inflation of odds ratios in a retrospective study with a profile penalized log‐likelihood approach. J Clin Lab Anal. 2021;35(7).
100. Tzeng I-S. Impact of Blood Type O on Mortality of Sepsis Patients: a Multicenter Retrospective Observational Study. Diagnostics. 2020;10:826.
101. Delgado-Rodriguez M, Llorca J. Bias. J Epidemiol Community Health. 2004;58(8):635–641.
102. Hill G, Connelly J, Hébert R, Lindsay J, Millar W. Neyman’s bias re-visited. J Clin Epidemiol. 2003;56(4):293–296.
103. Levin KA. Study design III: cross-sectional studies. Evid Based Dent. 2006;7(1):24–25.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Assessment of Students’ Attitudes Towards the Nursing Profession at Wolkite University, Ethiopia, 2021
Emire MS, Haile TG, Tesu M
Nursing: Research and Reviews 2022, 12:159-168
Published Date: 25 August 2022
Epidemiology of Gastrointestinal Parasites of Cattle in and Around Hosanna Town, Southern Ethiopia
Tiele D, Sebro E, H/Meskel D, Mathewos M
Veterinary Medicine: Research and Reports 2023, 14:1-9
Published Date: 17 January 2023
Global Burden of Asthma, and Its Impact on Specific Subgroups: Nasal Polyps, Allergic Rhinitis, Severe Asthma, Eosinophilic Asthma
Rabe APJ, Loke WJ, Gurjar K, Brackley A, Lucero-Prisno III DE
Journal of Asthma and Allergy 2023, 16:1097-1113
Published Date: 6 October 2023
The Knowledge-Attitude-Behavior Paradox in E-Cigarette Adoption Among University Students at Northern Border University, Saudi Arabia
Alenezi IN, Mersal FA, Osman Mohamed HA, El Said FG, Alanazi FJ, Abu-Negm LM, Aboelola TH, Alrwili AG
Journal of Multidisciplinary Healthcare 2026, 19:578360
Published Date: 18 February 2026