Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Assessing Students’ Knowledge and Attitudes Regarding the Risks and Prevention of Consanguineous Marriage: A Cross-Sectional Online Survey
Authors Jairoun AA ![]() , Al-Hemyari SS
, Al-Hemyari SS ![]() , Shahwan M
, Shahwan M ![]() , Karuniawati H, Zyoud SH, Abu-Gharbieh E, Zyoud SH
, Karuniawati H, Zyoud SH, Abu-Gharbieh E, Zyoud SH ![]() , Al-Ani M, Habeb M, Jairoun M
, Al-Ani M, Habeb M, Jairoun M
Received 11 November 2023
Accepted for publication 5 February 2024
Published 20 March 2024 Volume 2024:17 Pages 1251—1263
DOI https://doi.org/10.2147/JMDH.S449348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ammar Abdulrahman Jairoun,1,2 Sabaa Saleh Al-Hemyari,2,3 Moyad Shahwan,4,5 Hidayah Karuniawati,6,7 Samer H Zyoud,4,8– 10 Eman Abu-Gharbieh,11 Sa’ed H Zyoud,12,13 Mena Al-Ani,14 Mustafa Habeb,15 Maimona Jairoun5
1Health and Safety Department, Dubai Municipality, Dubai, United Arab Emirates; 2Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia (USM), Pulau Pinang, 11800, Malaysia; 3Pharmacy Department, Emirates Health Services, Dubai, United Arab Emirates; 4Centre of Medical and Bio-Allied Health Sciences Research, Ajman University, Ajman, 346, United Arab Emirates; 5Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, 346, United Arab Emirates; 6Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia (USM), Pulau Pinang, 11800, Malaysia; 7Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Muhammadiyah Surakarta, Surakarta, 57102, Indonesia; 8Department of Mathematics and Sciences, Ajman University, Ajman, United Arab Emirates; 9Nonlinear Dynamics Research Center (NDRC), Ajman University, Ajman, United Arab Emirates; 10School of Physics, Universiti Sains Malaysia (USM), Penang, 11800, Malaysia; 11Department of Clinical Sciences, College of Medicine, University of Sharjah, Sharjah, 27272, United Arab Emirates; 12Department of Clinical and Community Pharmacy, College of Medicine and Health Sciences, An-Najah National University, Nablus, 44839, Palestine; 13Clinical Research Centre, An-Najah National University Hospital, Nablus, 44839, Palestine; 14Developmental Biology & Cancer Department, University College London, UCL Great Ormond Street Institute of Child Health, London, UK; 15Edgware Community Hospital Barnet, Enfield and Haringey Mental Health NHS Trust, London, UK
Correspondence: Ammar Abdulrahman Jairoun; Moyad Shahwan, Tel +971558099957; 9716 705 6249, Email [email protected]; [email protected]
Background: Several studies indicate a correlation between consanguinity and genetic disorders, congenital malformations, harm to reproductive health, and increased child mortality.
Objective: To assess students’ knowledge and attitudes about risks and prevention of consanguineous marriage.
Methods: Demographic details of the participants and data on knowledge and attitudes concerning the risks and prevention of consanguineous marriage were obtained using an online self-administered questionnaire. The factors associated with good knowledge and attitude toward consanguineous marriage were investigated by logistic regression analysis.
Results: A total of 667 participants enrolled in the study. The average knowledge score about consanguineous marriage risk and prevention was 78.6% with a 95% confidence interval (CI) [77.3, 79.8], and the average attitude was 79.7% with a 95% confidence interval (CI) [79, 80.6]. A better knowledge score was observed in older participants (OR 1.01; 95% CI 1.004– 1.024), females (OR 1.69; 95% CI 1.48– 1.94), participants with parental history of consanguinity (OR 1.33; 95% CI 1.17– 1.52), participants with family history of consanguineous marriage (OR 5.18; 95% CI 2.19– 7.10), and participants with family history of inherited disease (OR 1.52; 95% CI 1.25– 1.86).
Conclusion: In general, the overall level of knowledge and attitudes toward consanguineous marriage risk and prevention was good among university students. To efficiently control and manage the adverse health impacts associated with consanguineous marriage, there is an urgent need to develop and implement evidence-based counseling and screening programs for consanguineous marriage that would significantly reduce the number of at-risk marriages.
Keywords: consanguineous marriage, knowledge, attitude, perception, consanguineous marriage risk, prevention, university students
Introduction
Marriage, an institution, in society holds philosophical interpretations regarding its purpose, function and implications. From a perspective marriage is often seen as an agreement where individuals come together based on mutual consent and shared values. Philosophers like John Locke highlight the importance of marriage in safeguarding rights and the pursuit of happiness. Moreover, ethical theories such as virtue ethics or utilitarianism contribute to discussions about the aspects of relationships. When examining the role of marriage in society it becomes clear that it acts as a cornerstone for strengthening family bonds and alliances. The discourse surrounding marriage becomes more diverse when considering African and South Asian cultures. In societies marriage is frequently regarded as an affair that not only strengthens connections between individuals but also fosters unity within extended families and communities. Asian perspectives, influenced by diversity and religious beliefs often place significant emphasis on the sacred and spiritual dimensions of marriage, with rituals and traditions shaping marital unions.
To better understand these interpretations and cultural differences scholars, like Kwame Gyekye (1997)1 offer insights into African perspectives on philosophy while works such as Arvind Sharmas (1998)2 scholarship shed light on the South Asian philosophical and religious views, on marriage. Viewing marriage through a lens allows us to explore its societal roles, ethical implications and diverse cultural influences that shape this fundamental aspect of human life.
The practice consanguinity has historical roots and implications that differ across cultures and regions. Throughout history it has been particularly common, among families to consolidate power and maintain lineage. The significance of marriages varies depending on society with some viewing them to reinforce social status, caste, or ethnicity while others prioritize individual choice. Regional differences are notable with rates reported in the Middle East, North Africa, South Asia, Sub Saharan Africa, and parts of Latin America compared to other countries. Various societal factors such as considerations and cultural norms contribute to the continuation of consanguinity practices, which impact family structures and honor. Moreover, there are implications associated with unions since they carry an increased risk of inherited disorders among offspring. Therefore, comprehending the complexities surrounding this phenomenon requires an approach that considers its context along, with cultural and genetic factors.3–5
Definitions of consanguineous marriage outline it as the union of close biological relatives. The literature has classified these marriages according to the closeness of the familial relationship between the spouses: as unions of first cousins on either the paternal or maternal side or of second cousins, third cousins, uncle-niece marriages, or distant relatives.6–8 Many countries practice consanguinity, with the highest rates occurring in North and sub-Saharan Africa, the Middle East, and west, central, and south Asian countries.3 For example, a study in Turkey found a consanguineous marriage frequency of 18.5% in its sample, with 57.8% of those marriages between first cousins.9 Likewise, a study in Oman revealed that more than half of marriages are between close biological kin; unions between first cousins are the most common type, constituting 39% of all marriages and 75% of all consanguineous marriages.10
Consanguinity occurs more frequently among women with the following traits: large families, young age at the time of marriage, older marriage groups, less than a high school education, rural location, unemployed, lack of exposure to mass media, monogamously married, lower economic status, and marriage to husbands without higher education.9–11 Unions between closely related kin are generally motivated by culture, tradition, or socioeconomic and psychological benefits.3,12–15
These marriages are respected, especially among Arabs, because of the perceptions that they strengthen family ties and promote family stability, reduce dowry or bridewealth payment requirements, simplify pre-marital negotiations, ensure increased compatibility between spouses and other family members, lower the risk of hidden financial and health issues, and keep family property within parental families.3,12–15 For example, these marriages strongly correlate with marital stability and reduced divorce risk because they promote a more harmonious and loving relationship between the bride, groom, and in-laws as a family.10 Here, the significantly lower remarriage rate among women married to close biological relatives demonstrates consanguineous marriages’ stability: 29% of consanguineously married women were married more than once, compared to 71% of non-consanguineously married women.10
However, consanguineous marriages demonstrate adverse health impacts. Several studies indicate a correlation between consanguinity and genetic disorders, congenital malformations, harm to reproductive health and increased child mortality.16,17 For example, one study revealed that the rate of child mortality under the age of 5 years was remarkably higher among children of close biological kin (16.62%) as compared to non-consanguineous marriage groups (5.77%).17 As such, people—and thus, students—must be aware of consanguineous marriages’ risks and detrimental effects on their health and offspring.15 In this respect, students’ knowledge, attitudes, and perceptions about consanguinity and marriage practices are vital in preventing possible health consequences while developing a positive attitude toward prevention. Therefore, this study explores students’ knowledge and attitudes about the risks and prevention of consanguineous marriage so that it can be used as a reference in developing an information guide on consanguineous marriage related to health effects and its prevention. Our study aims to explore several hypotheses investigating the factors associated with a higher level of knowledge regarding consanguineous marriage and its health implications:
- Participants with a parental history of consanguinity are hypothesized to possess better knowledge and more positive attitudes toward consanguineous marriage and its health implications. This assumption is grounded in the belief that personal experiences within their families may contribute to an increased awareness and understanding of potential health consequences.
- Participants from the Middle East are expected to score higher in knowledge and exhibit more positive attitudes toward the health consequences of preventing risks associated with consanguineous marriage.
- It is anticipated that older participants will generally exhibit positive attitudes toward taking precautions against risks arising from consanguineous marriage. This inclination may be influenced by their age and how it shapes their perspectives on practices, ultimately impacting reproductive health.
Methods and Materials
Study Settings and Design
This study was a descriptive cross-sectional survey performed online. The target population comprised Ajman University students aiming to evaluate their knowledge and attitudes concerning the risks and prevention of consanguineous marriage. The participants each received an email with a link to the questionnaire. The survey was conducted from 12 Sept 2022 to 16 Dec 2022.
Research Instrument Development
Prior studies examining knowledge, beliefs and attitudes regarding consanguineous marriage were used as the basis for the development of the questionnaire in the present study.8,10,12,13 The main components in the pre-existing studies that were relevant to the research issue were hereby used to create an English-language questionnaire to be self-completed by the respondents; some questionnaire elements were altered to ensure that the instrument was suitable for the UAE context. The design, relevance and content of the questionnaire were examined and reviewed by experts in the field, who also offered opinions on its fluency and legibility. Four academic professionals from the field of pharmacy at Ajman University then validated the questionnaire, and their advice was used to perform further minor modifications. The resulting instrument was then tested in a pilot phase before being administered to the sample population. The pilot involved emailing a link to the questionnaire to 22 participants who were chosen via convenience sampling.
We calculated Lawshe’s content validity ratio (CVR) for each item of the questionnaire in order to assess their quantitative content validity.18 Items scoring at least 0.78 were considered acceptable, while items that scored below the 0.78 threshold were removed from the final instrument.18 The mean CVR of the items with acceptable values was used to produce the instrument’s final content-validity index (CVI), which was found to be 0.85, ie satisfactory.19
As the pilot phase revealed no major issue with the survey questionnaire, it was utilized for the main research with minor modifications. These changes were made based on the results from the pilot study to ensure that the final research instrument’s had good dependability. For instance, the scientific terminology was defined, the question and page numbering was altered, the term (Gender) was used in place of the term (Sex), some questions were linked, and the questionnaire was concluded using specific items. The final analysis did not include the pilot study findings. The reliability of the final questionnaire was assessed via Cronbach’s alpha; the alpha of 0.76 indicated satisfactory internal consistency.
Research Instrument Sections
The survey used in this study examined the knowledge, attitudes, and perceptions among the respondents concerning the risks and prevention of consanguineous marriage. To this end, the questionnaire had three sections. The first section captured the demographic details of the participants (ie, age, gender, nationality, major, study year, nationality, parental history of consanguinity, family history of consanguinity, and family history of congenital disease).
The second section focused on the participant’s knowledge of the risks and prevention of consanguineous marriage using ten questions to which respondents gave categorical responses (ie yes, no, do not know). One score was given to each correct response, while incorrect responses scored zero. The scores for this section were summed to determine the total score for each respondent concerning their knowledge of the risks and prevention of consanguineous marriage.
The third section captured the attitudes towards the risks and prevention of consanguineous marriage among the participants using 15 items rated on a 5-point Likert-type scale (1=“Strongly Disagree”, 2= “Disagree”, 3= “Neutral”, 4= “Agree”, 5= “Strongly Agree”). The ratings were then totaled for each participant to obtain raw scores on attitudes towards the risks and prevention of consanguineous marriage.
Study Population (Inclusion and Exclusion Criteria)
The target population was students in the UAE, whether national or resident, aged at least 18 and demonstrating a willingness to participate in this research. Students were excluded if they were below the age of 18 or unwilling to participate.
Sample Size and Sampling Technique
As far as we know, there is an absence of prior literature indicating to what extent students may have an awareness of the issue of consanguineous marriage. Consequently, to ensure that adequate sample size was used for the main research, we conducted a pilot study. Based on the responses to the pilot survey question, “Do you know of any relationship between consanguineous marriage and children with congenital disease?”, it was possible to estimate the optimal sample size for the main research. More than half (65%) of the participants answered “Yes” to this question. An alpha level of 5% was selected for this study, meaning a 95% confidence interval (CI). With the precision (D) of 5%, 10% was taken to be the maximum width of the 95% CI. Thus, 700 individuals were considered to be a sufficient size for the final survey, based on a non-response rate of 50%. An Excel file with the relevant details (name, study year, college, email address) of the students of Ajman University was provided by the Admissions and Registration Department of the university. The sample was chosen using basic random sampling using ID numbers stratified by department and college. Overall, 667 respondents were selected for inclusion in the main research.
Questionnaire Administration
The participants, randomly pre-selected from the spreadsheet from the university’s Admissions and Registration Department, were sent a link to the online self-administered questionnaire via email. The nature and purpose of the study were explained on the questionnaire’s cover page. If a respondent clicked through to the subsequent page, they were assumed to have given their informed consent to take part. Any participants who did not respond to the initial email were sent reminder emails twice during the first month of the survey. Respondents who completed the survey were offered a message thanking them for participating. No incentives were offered for participation.
Statistical Analysis
SPSS Version 24 (Statistical Package for the Social Sciences; IBM Corp., Armonk, NY, USA) was used for the statistical analysis. Frequencies and percentages were used to describe the categorical variables, and means and standard deviations (SD) were used for the continuous, normally distributed quantitative ones. The differences among the quantitative variables across groups were assessed using unpaired Student’s t-tests, one-way ANOVA, and non-parametric variants. The normal distribution of continuous variables was evaluated through the execution of a Shapiro–Wilk test (with a p-value greater than 0.05) or by visually inspecting a normal Q-Q plot. The factors affecting the knowledge and attitudes among the participants concerning the risks and prevention of consanguineous marriage were evaluated using multivariate logistic regression models. The threshold for statistical significance was a p-value below 0.05.
Ethical Considerations
We affirm that this study complies with the ethical principles outlined in the Declaration of Helsinki. The Institutional Ethical Review Committee of Ajman University approved this study. All participants voluntarily gave their information and responses. The study goals were presented on the first page of the questionnaire, and if the respondent clicked through to the following page, they were considered to have consented to participate. No information on the respondents that could have identified them was retained, and all participants were assured of their anonymity.
Results
Demographic Characteristics of the Study Participants
A total of six hundred sixty-seven participants enrolled in the study. Among the total, 63.1% (n=421) were male, and 36.9% (n=246) were female. Last year students constituted 42.6% of the study sample, and 57.4% were first-year students. Of the total subjects, 454 (68.1%) were from medical colleges, and 213 (31.9%) were from non-medical colleges. The nationality of the study participants was as follows: 91 (13.6%) were from the Middle East, 127 (19%) were from Asia, and 449 (67.3%) were from Africa. According to the obtained data, 50.7% of the total population studied had a parental history of consanguinity, 14.5% had a family history of consanguineous marriage, and 14.5% had a family history of inherited disease. (Table 1).
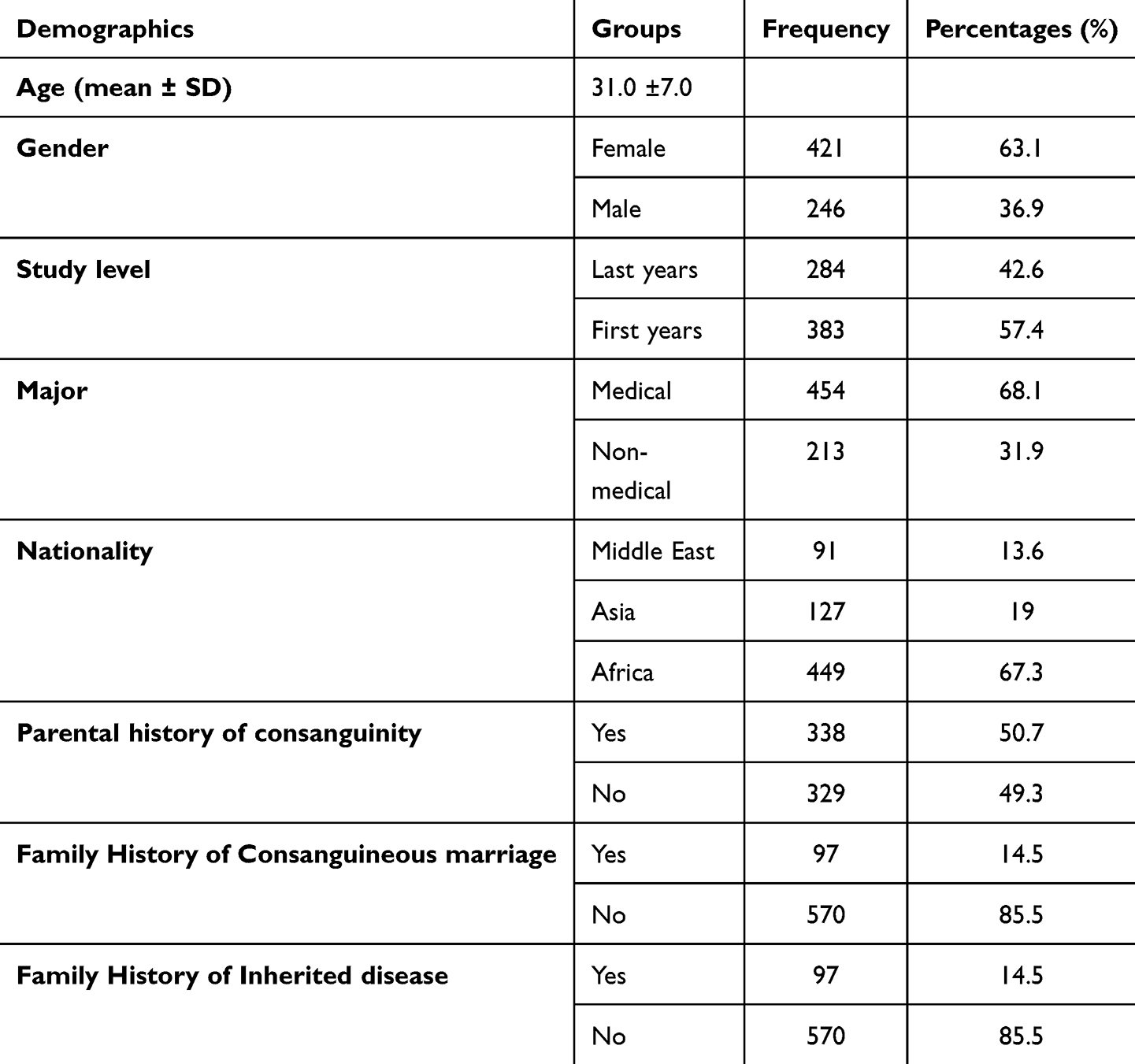 |
Table 1 Number and Percentages of the Questions on Demographics (n=667) |
Participants’ Knowledge and Attitude About Consanguineous Marriage Risk and Prevention
The average knowledge score about consanguineous marriage risk and prevention was 78.6% with a 95% confidence interval (CI) [77.3, 79.8], and the average attitude was 79.7% with a 95% confidence interval (CI) [79, 80.6]. In general, the overall level of knowledge and attitude towards consanguineous marriage risk and prevention was good among university students.
The results of each question related to knowledge and attitude about consanguineous marriage risk and prevention are shown in Tables 2 and 3.
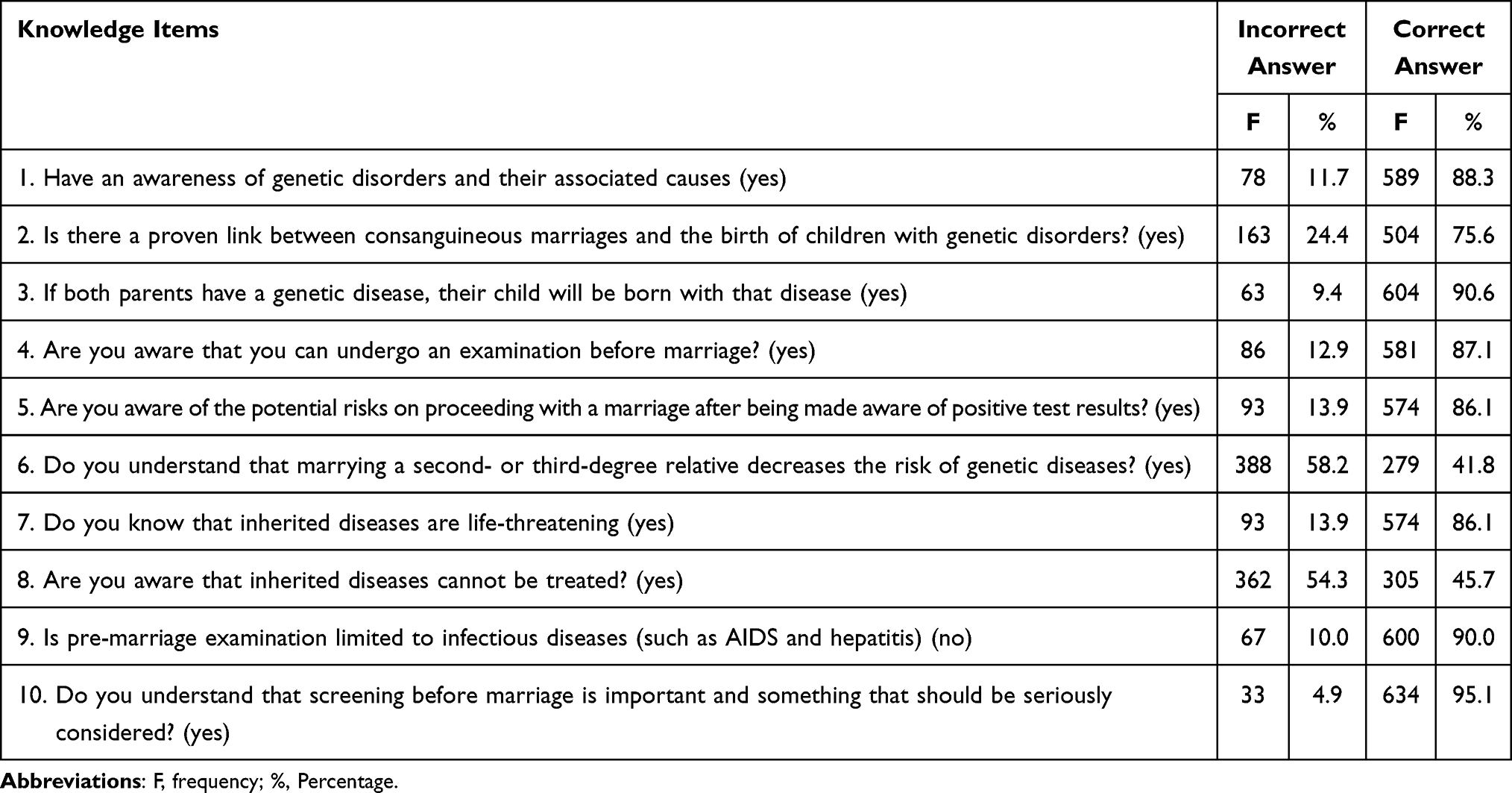 |
Table 2 Number and Percentage of the Questions on Knowledge Items (n=667) |
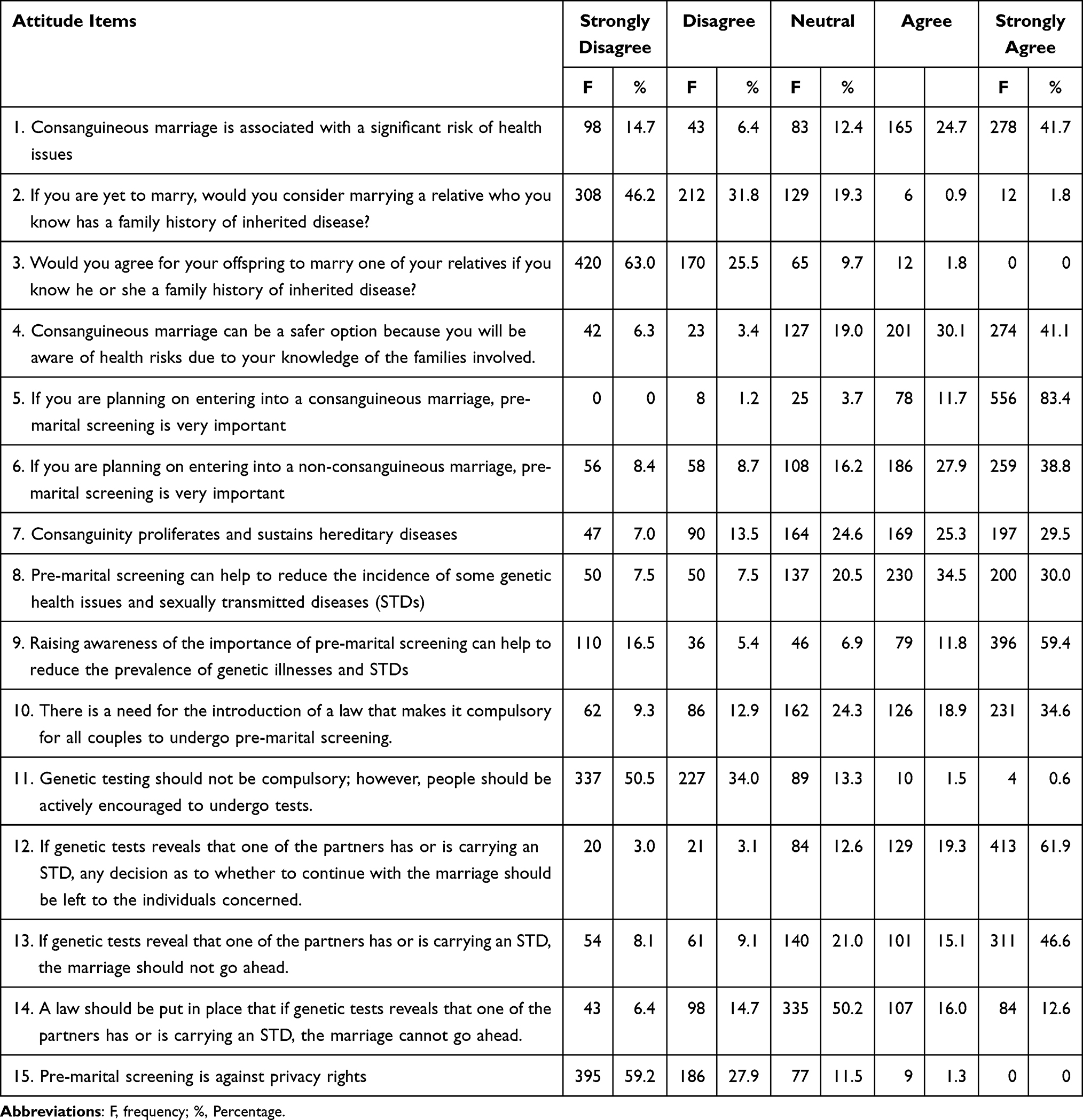 |
Table 3 Number and Percentage of the Questions on Attitude Items (n=667) |
The results of the bivariate analysis revealed that gender (P<0.001), major (P=0.016), nationality (P=0.007), Parental history of consanguinity (P=0.009), Family History of Consanguineous marriage (P<0.001) and Family History of Inherited disease (P=0.001) were more likely to score better in the knowledge about consanguineous marriage risk and prevention. The same pattern of the results was observed in attitude about consanguineous marriage risk and prevention according to demographic characteristics (Table 4).
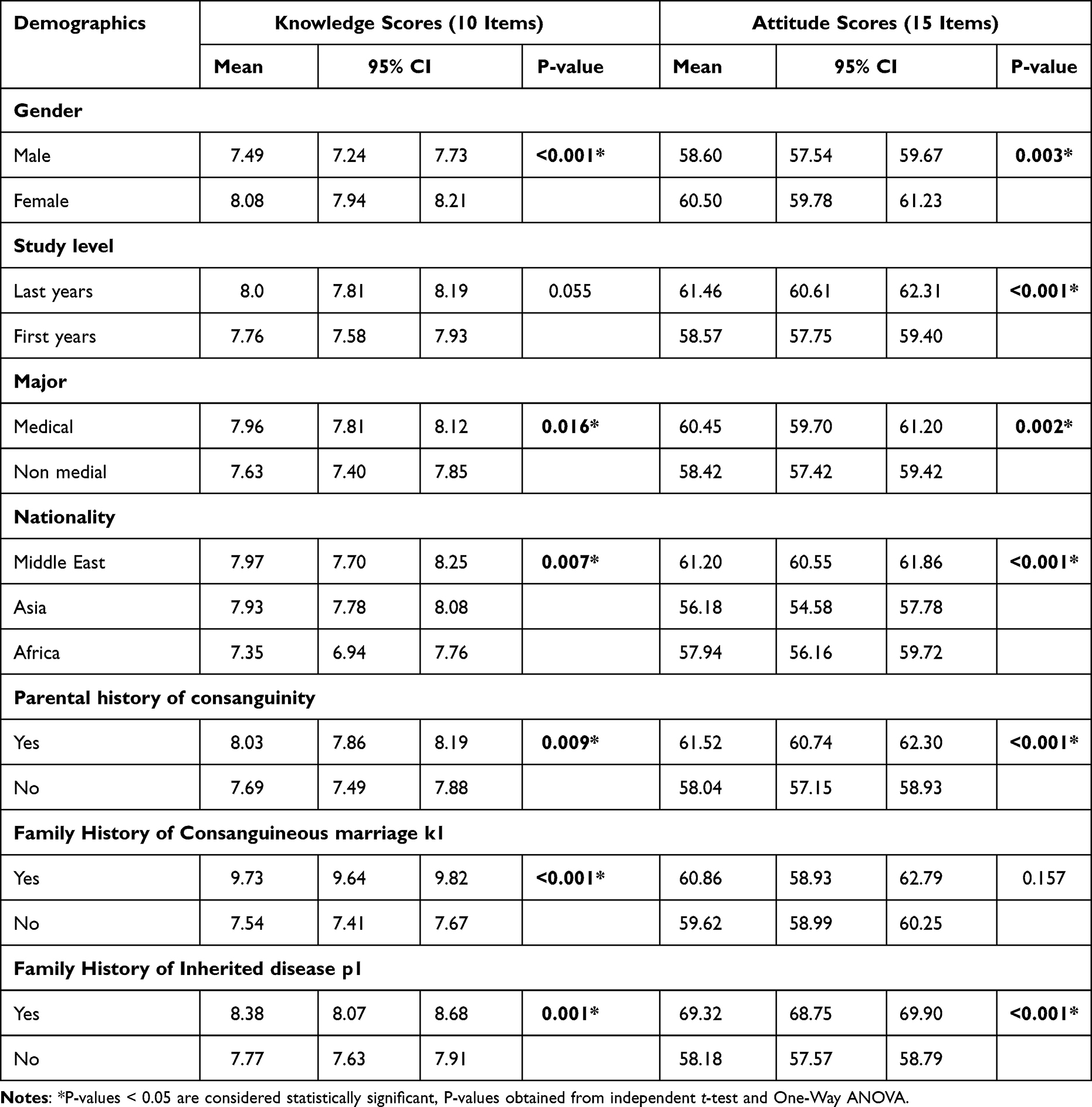 |
Table 4 Comparing Knowledge and Attitude According to Demographics |
Factors Influencing Participants’ Knowledge and Attitude About Consanguineous Marriage Risk and Prevention
Table 5 presents the results of multivariate logistic regression analysis for the factors associated with knowledge and attitude about consanguineous marriage risk and prevention.
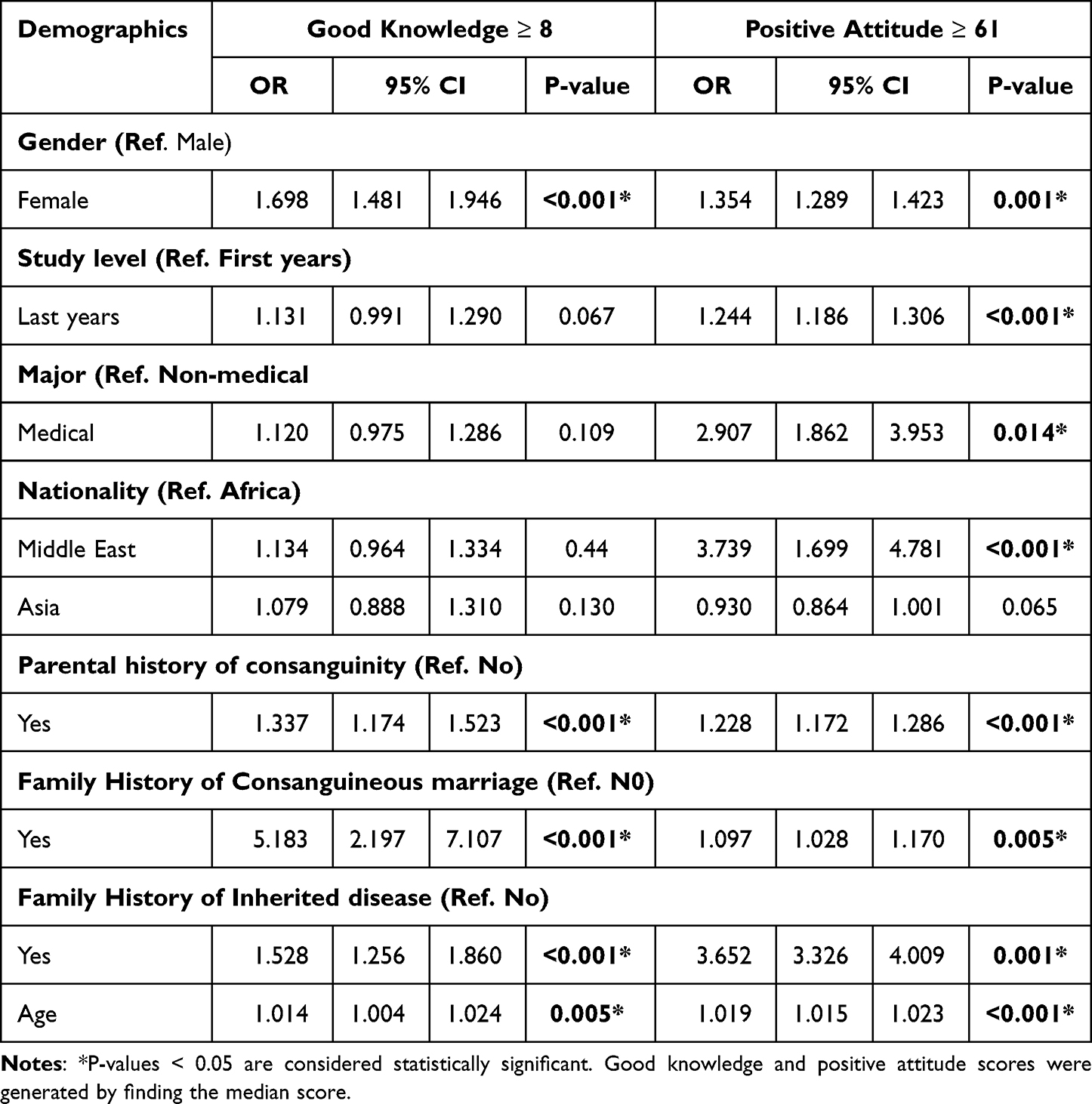 |
Table 5 Multivariate Analysis for the Factors That Associated with Knowledge and Attitude About Consanguineous Marriage Risk and Prevention |
Better knowledge score was observed in the older participant (OR 1.01; 95% CI 1.004–1.024), female (OR 1.69; 95% CI 1.48–1.94), participants with parental history of consanguinity (OR 1.33; 95% CI 1.17–1.52), participants with family History of Consanguineous marriage (OR 5.18; 95% CI 2.19–7.10) and participants with family History of Inherited disease (OR 1.52; 95% CI 1.25–1.86).
Better attitude score was observed in the older participant (OR 1.02; 95% CI 1.015–1.023), female (OR 1.35; 95% CI 1.28–1.42), last year’s students (OR 1.24; 95% CI 1.18–1.31), medical students (OR 2.90; 95% CI 1.86–3.95), participants from the Middle East (OR 3.73; 95% CI 1.69–4.78), participants who with Parental history of consanguinity (OR 1.28; 95% CI 1.17–1.82), participants with family history of consanguineous marriage (OR 1.09; 95% CI 1.28–1.17) and participants with family History of Inherited disease (OR 3.65; 95% CI 3.32–4).
Discussion
Consanguineous marriage has become a widespread concern because of the possible predictions of health-related risks. This study aims to determine the knowledge and attitudes of respondents towards inbreeding marriage related to the risks and prevention. This needs to be done to identify gaps in knowledge and attitudes towards risks and prevention of incestuous marriages so that action needs to be taken to minimize the risks of incestuous marriages. In this study, 67.3% of respondents came from Africa, 19% from Asia, and 13.6% from the Middle East, where 50.7% of respondents had a parental history of consanguinity, 14.5% had a family history of consanguineous marriage, 14.5% had a family history of inherited disease. North and Sub-Saharan Africa, the Middle East, and West, Central, and South Asia have the highest rates of consanguineous marriage.3,20
The advantages or main reasons for a preference for consanguineous marriages are sociocultural, economic, and psychological benefits, such as strengthening family ties, keeping possessions within the family, family property consolidation, improving the stability of the family, traditions, continuity of a culture and way of life, ease of marriage arrangements, enhanced female autonomy, greater compatibility with in-laws, lower domestic violence, lower divorce rates and less expensive dowries.3,12–15 Furthermore, 14.5% had a family history of inherited disease. Several studies revealed that consanguineous marriages were associated with the incidence of several single gene and multifactorial diseases and congenital malformations, including bronchial asthma, hearing defect, heart diseases, and sickle cell anemia (p < 0.05).16,17 In addition, consanguineous marriages cause higher expression of recessive alleles, leading to the clustering of mutations in a particular community.21 Another study shows that mental retardation, physical retardation, bilateral cleft lip ± cleft palate, cystic fibrosis, and congenital blindness are associated with first-cousin marriage.22
In the current study, it was found that university students demonstrated a high level of knowledge about consanguineous marriage risk and prevention, with an overall knowledge level of 78.6%. This result is consistent with the previous study in Saudi Arabia23 but higher when compared with the previous study in India, where 62% of students had moderate knowledge, and 12% had inadequate knowledge regarding the health consequences of consanguineous marriage.24 A study in Bangladesh also revealed that most participants had poor knowledge of consanguineous marriage’s possible hereditary burden. Only one in every 14 respondents previously knew the potential complications associated with consanguineous marriages.17 Another study reported that most respondents had poor knowledge and a negative attitude (53.31% and 57.21%, respectively).25 In the current study, more than 80% of respondents know about genetic disorders and the causes of genetic disorders (Q1), and inherited diseases are life-threatening (Q7). Respondents also know the possibility of health-related effects of consanguineous marriages on their children (Q2, Q3, Q5). This differs from previous research, which stated that more than 30% of respondents had no idea that consanguineous couples may have more diseased offspring than non-consanguineous couples.25 The current study shows that more than half of the respondents are incorrect in whether inherited diseases can be treated (Q8). In order to prevent possible adverse impacts, most respondents know and believe that pre-marital screening is a realistic action and can be considered in carrying out a marriage (Q4, Q10). Most of them (90%) also know that examination before marriage is not limited to infectious diseases (such as hepatitis and AIDS) (Q9). This is in line with previous research that most respondents agreed that pre-marital screening reduces the incidence of diseases.26 Women, students in health-related colleges, and a participant’s parents’ non-consanguineous marriage were all significantly associated with knowledge of pre-marital screening.27
This study demonstrated that knowledge scores on consanguineous marriage risk and prevention were influenced by age, gender, parental history of consanguinity, family history of consanguineous marriage, and family history of inherited disease. Similar study findings were noted in Ojha, 2020 that age was significantly associated with knowledge regarding consanguineous marriage.24 Female, last year student level, medical student, and students from Middle East countries, participants with parental history of consanguinity, participants with a family history of consanguineous marriage, and participants with a family history of inherited disease tend to have better knowledge. It has been found that women are more knowledgeable about consanguineous marriage risk and prevention than men, which is strengthened by the participant’s educational background (medical student and, in the last year, student level). The knowledge barrier was significantly higher among males.14 In contrast to research conducted in Bangladesh, almost half of those polled were unaware of the negative effects of consanguineous marriage. Despite the fact that 26% of the couples were aware of the impact of consanguinity, the interviews were indifferent.17
The overall attitude (average 79.7%) towards consanguineous marriage risk and prevention was good among university students, similar to the previous study in Saudi Arabia.23 More than half of the respondents (66.4%) believe that Consanguineous marriage causes health problems that may lead to hereditary diseases. However, consanguineous marriage has benefits. If there are any health risks, these health risks will be known because the families know each other. By knowing each other’s health, they can prevent health-related consanguineous marriage problems by not marrying relatives with a history of inherited disease and not marrying their children to someone from their relatives with a family history of inherited disease. Most respondents believe that pre-marital screening is important to prevent health problems in the case of consanguineous marriage (95%). The current study aligns with previous research, which found that most respondents agreed that pre-marital screening could help reduce the incidence of diseases.26 As such, it is important to consider pre-marital screening as an important measure in addition to other methods of disease prevention. This is supported by the survey results, which indicate that over 80% of respondents believe that pre-marital screening does not infringe on personal privacy. Raising awareness about pre-marital screening before marriage is important because it will reduce the prevalence of some genetic and sexually transmitted diseases (STDs). A study by Memish, 2011 performed over six years shows that pre-marital screening in Saudi Arabia markedly reduced the number of at-risk marriages, which may considerably reduce the genetic disease burden in Saudi Arabia in the next decades. The prevalence of β-thalassemia steadily decreased from 32.9 to 9.0 per 1000 examined persons (P<0.001).28 In the discovery of having or carrying STDs, more than 60% of respondents stated that marriage decisions must be left to the couple’s freedom. They believe that test results showing genetic diseases should change the marriage decision.
The previous study reported that in the event of positive results for either inherited or infectious diseases, about half of the respondents (50.79–56.61%) tend to proceed with marriage.26 Another study shows that about 178 (37.4%) respondents were willing to cancel their marriages if their pre-marital screening results were incompatible.27 Knowledge of pre-marital screening, enrollment in a health-related college, and the conviction that pre-marital screening does not affect one’s destiny positively correlate with attitude toward pre-marital screening.27 More than half (53.5%) of the respondents think that there is a law that obligates all future couples to do pre-marital screening is important. This is in line with previous research that 47.62% of respondents (45.71% of men and 48.74% of women) agreed that pre-marital screening should be required before engagement.26 Even so, (50%) of respondents answered “neutral” to the question, ‘it is important to apply a law that stops marriage upon discovery of the presence of a genetic disease.’ This indicates the marriage decision must be left to the couple’s freedom.
In the current study, a significant association of attitude regarding the consanguineous marriage risk and prevention with socio-demographic variables such as gender, study level, nationality, family history of consanguinity, and family history of consanguineous marriage. Female, last year student level, medical student, and students from Middle East countries, participants with parental history of consanguinity, and participants with a family history of inherited disease tend to have a better positive attitude regarding consanguineous marriage risk and prevention. These results are slightly different from the results of previous studies, where most of the people who showed a positive attitude to consanguineous marriage were from the older age group, males, those who are married to their relatives, and people who have a family history of consanguineous marriage.17 Another study reported that males, older age groups, those married to relatives, those with a high frequency of consanguineous marriages in their families, and participants with parental consanguinity all had significantly higher attitude scores toward consanguineous marriage. Age and education can predict a person’s attitude toward consanguineous marriage.25
The lack of consanguinity-related knowledge, attitude, and practice suggests that training programs at various educational levels should focus more on consanguinity counseling. Evidence-based counseling for consanguineous marriage is one of the recommendations of the Consanguinity Study Group of international experts and counselors at the Geneva International Kinship Workshop 2010.20 Carrier detection and genetic counseling programs have significantly lowered the prevalence of inherited disorders in many populations. However, these programs work best when they are sensitive to the cultural backgrounds of the populations in which they are implemented.29 For example, based on a study, six years of pre-marital screening in Saudi Arabia significantly reduced the number of at-risk marriages. This may significantly reduce Saudi Arabia’s genetic disease burden in the coming decades28
A comprehensive Social and Behavioral Change Communication (SBCC) campaign to educate and sensitize members of a different section of the community about the issues with marrying close relatives is suggested to prevent several health consequences that could result from it.24 Health education should play a significant role in preventing genetic diseases, which might be integrated into the secondary and university curriculum. Screening for hereditary disease before engagement will help significantly to avoid at-risk marriages and to reduce these diseases.30 Education could be included at the undergraduate level through a well-designed curriculum that includes genetics courses and practical applications, as well as in the health care setting through continuous education. It is suggested that health authorities incorporate consanguinity counseling into their mandatory pre-marital screening programs14,17,20
Prenatal screening can help to reduce the number of live births caused by inherited diseases.29 In addition, prenatal screening is the best approach for lowering the burden of genetic disorders and congenital disabilities that significantly impair postnatal function. For common genetic diseases and congenital anomalies like Down syndrome, beta-thalassemia, and neural tube defects, universal prenatal screening is advised.31
Conclusion
In general, the overall level of knowledge and attitudes towards consanguineous marriage risk and prevention was good among university students. To efficiently control and manage the adverse health impacts associated with consanguineous marriage, there is an urgent need to develop and implement evidence-based counseling and screening programs for consanguineous marriage that would significantly reduce the number of at-risk marriages.
Ethics Approval
The Institutional Ethical Review Committee of Ajman University approved this study. All participants voluntarily gave their information and responses.
Consent to Participate
The study goals were presented on the first page of the questionnaire, and if the respondent clicked through to the following page, they were considered to have consented to participate. No information on the respondents that could have identified them was retained, and all participants were assured of their anonymity.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gyekye K. Tradition and Modernity: Philosophical Reflections on the African Experience. Oxford University Press; 1997.
2. Sharma A. A Hindu Perspective on the Ethics of Marriage. In: McCarthy DM, Bongiovanni AE, editors. Marriage and the Family: Philosophical Perspectives. Rowman & Littlefield; 1998:183–194.
3. Bittles AH, Black ML. Consanguinity, human evolution, and complex diseases. Proc Natl Acad Sci. 2010;107(Suppl 1):1779–1786. doi:10.1073/pnas.0906079106
4. Hamamy H. Consanguineous marriages: preconception consultation in primary health care settings. J Commun Gene. 2012;3(3):185–192. doi:10.1007/s12687-011-0072-y
5. Tadmouri GO, Nair P, Obeid T, Al Ali MT, Al Khaja N, Hamamy HA. Consanguinity and reproductive health among Arabs. Reproductive Health. 2009;6(1):17. doi:10.1186/1742-4755-6-17
6. Bittles AH Consanguinity in Context. Cambridge Studies in Biological and Evolutionary Anthropology. Cambridge: Cambridge University Press; 2012. Available from: https://www.cambridge.org/core/books/consanguinity-in-context/EF569931B5FE4C33D2ADBB9FA164891D.
7. Sharma G. Pros and cons of different sampling techniques. Int J Appl Res. 2017;3(7):749.
8. Islam MM. The changing pattern and determinants of declining consanguinity in Jordan during 1990–2012. Ann Hum Biol. 2018;45(2):140–147. doi:10.1080/03014460.2018.1429655
9. Kaplan S, Pinar G, Kaplan B, et al. The prevalence of consanguineous marriages and affecting factors in Turkey: a national survey. J Biosoc Sci. 2016;48(5):616–630. doi:10.1017/S0021932016000055
10. Islam MM. The practice of consanguineous marriage in Oman: prevalence, trends and determinants. J Biosoc Sci. 2012;44(5):571–594. doi:10.1017/S0021932012000016
11. El Goundali K, Chebabe M, Zahra Laamiri F, Hilali A. The determinants of consanguineous marriages among the Arab population: a systematic review. Iran J Public Health. 2022;51(2):253–265. doi:10.18502/ijph.v51i2.8679
12. Hussain R. Community perceptions of reasons for preference for consanguineous marriages in Pakistan. J Biosoc Sci. 1999;31(4):449–461. doi:10.1017/S0021932099004496
13. Sandridge AL, Takeddin J, Al-Kaabi E, Frances Y. Consanguinity in Qatar: knowledge, attitude and practice in a population born between 1946 and 1991. J Biosoc Sci. 2010;42(1):59–82. doi:10.1017/S002193200999023X
14. Alnaqeb D, Hamamy H, Youssef AM, Al-Rubeaan K. Assessment of knowledge, attitude and practice towards consanguineous marriages among a cohort of multiethnic health care providers in Saudi Arabia. J Biosoc Sci. 2018;50(1):1–18. doi:10.1017/S0021932016000675
15. Sultana M, Perveen K, Afzal M, Gillani SA, Naseer A. Knowledge attitude and practice of rural community residents towards consanguineous marriages. IJARBSS. 2018;8(6):155–167. doi:10.6007/IJARBSS/v8-i6/4194
16. Zaini RG. Sickle-cell anemia and consanguinity among the Saudi Arabian Population. Arch Med. 20162:2.
17. Anwar S, Mourosi JT, Arafat Y, Hosen MJ, Cubellis MV. Genetic and reproductive consequences of consanguineous marriage in Bangladesh. PLoS One. 2020;15(11):e0241610. doi:10.1371/journal.pone.0241610
18. Lawshe C. A quantitative approach to content validity 1. Pers Psychol. 1975;28(4):563–575. doi:10.1111/j.1744-6570.1975.tb01393.x
19. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459–467. doi:10.1002/nur.20199
20. Hamamy H, Antonarakis SE, Cavalli-Sforza LL, et al. Consanguineous marriages, pearls and perils: Geneva international consanguinity workshop report. Genet Med. 2011;13(9):841–847. doi:10.1097/GIM.0b013e318217477f
21. Wahidiyat PA, Yo EC, Wildani MM, Triatmono VR, Yosia M. Cross-sectional study on knowledge, attitude and practice towards thalassaemia among Indonesian youth. BMJ Open. 2021;11(12):e054736. doi:10.1136/bmjopen-2021-054736
22. Kanaan ZM, Mahfouz R, Tamim H. The prevalence of consanguineous marriages in an underserved area in Lebanon and its association with congenital anomalies. Genet Test. 2008;12(3):367–372. doi:10.1089/gte.2007.0093
23. Al-Qattan HM, Amlih DF, Sirajuddin FS, et al. Quantifying the levels of knowledge, attitude, and practice associated with sickle cell disease and pre-marital genetic counseling in 350 Saudi Adults. Adv Hematol. 2019;2019:e3961201. doi:10.1155/2019/3961201
24. Ojha JK, Tutor M, Anusandhan O, Patra S. A study to assess the knowledge and attitude regarding health consequences of consanguineous marriage among students of a selected college of berhampur, Odisha to develop an information guide sheet on consanguineous marriage. Clin Med. 2020;7:11.
25. Mahboub SM, Alsaqabi AA, Allwimi NA, Aleissa DN, Al-Mubarak BA. Knowledge and attitude towards consanguineous marriage among educated adults in Riyadh. Int J Community Med Public Health. 2018;6(1):30. doi:10.18203/2394-6040.ijcmph20185223
26. Almoliky M, Abdulrhman H, Safe SH, et al. Knowledge and attitude of engaged and recently married couples toward pre-marital screening: a cross-sectional study. Inquiry. 2022;59:00469580221097424. doi:10.1177/00469580221097424
27. Al-Shafai M, Al-Romaihi A, Al-Hajri N, Islam N, Adawi K. Knowledge and perception of and attitude toward a pre-marital screening program in Qatar: a cross-sectional study. Int J Environ Res Public Health. 2022;19(7):4418. doi:10.3390/ijerph19074418
28. Memish ZA, Saeedi MY. Six-year outcome of the national pre-marital screening and genetic counseling program for sickle cell disease and β-thalassemia in Saudi Arabia. Ann Saudi Med. 2011;31(3):229–235. doi:10.4103/0256-4947.81527
29. Meyer BF. Strategies for the prevention of hereditary diseases in a highly consanguineous population. Ann Hum Biol. 2005;32(2):174–179. doi:10.1080/03014460500075217
30. Kotb MM, Hassan YA, Al-Khirat M, Hakami A. Knowledge, attitude and practices related to pre-marital screening for sickle cell Anemia in Jazan Region, Saudi Arabia. Egypt J Commun Med. 2018;36(3):103–113.
31. Phadke SR, Puri RD, Ranganath P. Prenatal screening for genetic disorders: suggested guidelines for the Indian Scenario. Indian J Med Res. 2017;146(6):689–699. doi:10.4103/ijmr.IJMR_1788_15
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitudes, and Perceptions of Tuberculosis in Indonesia: A Multi-Center Cross-Sectional Study

Kaaffah S, Kusuma IY, Renaldi FS, Lestari YE, Pratiwi ADE, Bahar MA
Infection and Drug Resistance 2023, 16:1787-1800
Published Date: 28 March 2023
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Gebremichael MA, Lema TB
International Journal of Women's Health 2023, 15:1383-1395
Published Date: 4 September 2023
University Students’ Knowledge, Attitudes, and Practices Regarding Cervical Spine Health
Liu Y, Wang H, Liu H, Li L
Journal of Multidisciplinary Healthcare 2025, 18:2375-2386
Published Date: 29 April 2025
Intensive Care Nurses’ Perceptions, Knowledge, and Attitudes Toward Pressure Injury Prevention in Prone Position Patients: A Multicenter Cross-Sectional Study in Shanghai, China
Fang W, Pan W, Liu X, Li J, Zhang Q, Qin W
Risk Management and Healthcare Policy 2025, 18:2935-2950
Published Date: 9 September 2025