Back to Journals » Journal of Inflammation Research » Volume 19
Intestinal Stenosis Related to Immune Checkpoint Inhibitors Caused by Sintilimab: A Case Report
Authors Li HY, Liu Y, Hu SL, Li YQ, Tang TY
Received 21 August 2025
Accepted for publication 26 December 2025
Published 10 January 2026 Volume 2026:19 556800
DOI https://doi.org/10.2147/JIR.S556800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Caminero
Hong Yan Li, Yue Liu, Si Leng Hu, Yu Qin Li, Tong Yu Tang
Gastroenterology Department, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China
Correspondence: Yu Qin Li, Gastroenterology Department, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China, Email [email protected] Tong Yu Tang, Gastroenterology Department, The First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) as an immunotherapy have significantly prolonged the overall survival (OS) and progression-free survival (PFS) of patients with various advanced cancers, and have significantly increased the objective response rate. However, excessive activation of the immune system may attack normal organs, triggering a series of immune-related adverse reactions. Among them, due to the relatively high incidence of immune-mediated colitis (IMC), it is particularly worthy of attention. Xindili Antibody is a fully human immunoglobulin G4 monoclonal antibody that targets the programmed cell death receptor 1 (PD-1) pathway. It is of great significance in cancer immunotherapy and has shown good anti-tumor effects in various malignant tumors. Here, we report a case of a 64-year-old male with colorectal cancer and lung metastasis. After using Sintilimab, the patient developed inflammatory intestinal obstruction. The colonic stenosis caused by immune checkpoint inhibitors may be the result of the combined effects of chronic immune inflammation, microbial flora imbalance, and disrupted tissue repair. This case report emphasizes the importance of early identification and appropriate intervention to prevent the permanent interruption of immune checkpoint inhibitor treatment and the prevention of colitis complications.
Keywords: immune checkpoint inhibitors, colitis, anti-PD-1, immune-mediated colitis, Sintilimab
Introduction
Immune checkpoint inhibitors are one of the most important categories in immunotherapy. They consist of monoclonal antibodies and are designed to enhance and rejuvenate the immune system by binding to these co-inhibitory receptors, thereby inducing immune-mediated tumor cell death. During this process, ICI will induce excessive activation of the immune system, thereby leading to immune-related adverse events (irAE).1–3 This inflammatory toxicity can affect any organ, most commonly the skin, gastrointestinal tract, endocrine system and respiratory system, and less frequently the nervous system, heart, and blood system.4,5 Currently, the FDA has continuously approved three different types of ICI drugs: CTLA-4 inhibitors (ipilimumab and tremelimumab), PD-1 inhibitors (nivolumab, pembrolizumab and cemiplimab), and PD-L1 inhibitors (atezolimumab, durvalumab and avelumab).6 It is reported that among the patients receiving these drug treatments, up to 0.3% to 1.3% of them experienced fatal immune-related adverse events (irAEs).7 It is known that conventional endoscopic examinations can be used for the diagnosis of colitis. Li Haiyan et al proposed a method for evaluating ulcerative colitis based on fine-grained lesion learners and noise suppression gating, called UCFN-Net. It aims to effectively extract the precise details of small lesions by leveraging local features, enhancing transmission, while reducing feature loss and suppressing noise. It is also highly likely to be applied to immune-mediated colitis in the future.8 The exact mechanism of ICI-induced colitis is not yet clear, but it may be related to autoimmune dysregulation and changes in the intestinal microbiome.9 Wang Jiang et al10 demonstrated through cell and mouse experiments the crucial role of the ubiquitination-related protein N4BP3 in colitis. N4BP3 promotes the NOD2-MAPK/NF-κB signaling pathway through RIPK2 ubiquitination, and the TLR4-NF-κB signaling pathway through IκBα ubiquitination, thereby facilitating the release of pro-inflammatory cytokines and colonic inflammation. Sintilimab by binding to PD-1, can block its interaction with PD-L1 and PD-L2, thereby inhibiting the PD-1/PD-L1 pathway that leads to tumor immune tolerance, and activating the function of T cells, enhancing the immune surveillance and killing ability of T cells against tumors, generating tumor immune responses, and thus achieving the goal of treating tumors.11 The common adverse reactions during the treatment with Sintilimab include anemia, fever, thyroid dysfunction, and more severe immune disorders.3 As far as we know, this is the first case report of intestinal stenosis caused by Sintilimab has been published.
Case Presentation
A 64-year-old male presented with abdominal distension and reduced bowel movements and flatulence in June 2021. The symptoms gradually worsened without any obvious trigger. The symptoms gradually worsened and he was admitted to our emergency department for CT examination, which revealed small intestinal obstruction at the terminal ileum in the right lower abdomen, with thickening of the adjacent ileocecal wall. The diagnosis was intestinal obstruction. On June 20, 2021, he underwent right hemicolectomy and ileostomy. The postoperative pathology indicated mucinous adenocarcinoma of the ileocecal region. From July 16, 2021, he started chemotherapy with the XELOX (oxaliplatin + capecitabine) regimen for 6 courses. On December 12, 2022, a re-examination of the lung CT indicated lung metastasis, suggesting disease progression. From January 19, 2023, he received treatment with FOLFIRI (irinotecan: Calcium Folinate, 5-fluorouracil (5-FU) + bevacizumab) for 8 courses. After 3 courses of chemotherapy, the efficacy evaluation was stable disease (SD). On July 26, 2023, due to the continuous increase in tumor markers, the treatment plan was changed to FOLFIRI + regorafenib. Four courses of treatment have been completed. On October 16, 2023, the re-examination indicated disease progression, and anti-tumor treatment with fuzituximab + Sintilimab was initiated. Four courses of treatment have been completed. After 3 courses of treatment, the efficacy evaluation was stable disease. On January 30, 2024, the patient was admitted to the hospital due to diarrhea. The patient reported that the diarrhea started 3 days before admission (18 days after the previous treatment course, 3 days after discontinuation of oral fuzituximab) and occurred about 10 times per day, each about 200–300 mL, with blood in the stool, covered with mucus, accompanied by nausea, abdominal distension, abdominal pain, relieved after defecation. The symptoms were relieved after symptomatic treatment with oral montmorillonite powder. However, the relief was not obvious. After admission, the fecal examination indicated negative results for stool culture and Clostridium difficile detection, as well as negative serum EB virus antibodies, nucleic acids, and IgM and IgG antibodies of cytomegalovirus, and negative nucleic acids. The statistics of relevant blood markers of the patient during this admission and before and after the onset are shown in Table 1. The tumor markers (CEA and CA199) did not show significant changes compared to the previous treatment course. At this time, the tumor was still in stable disease (SD). On February 1, 2024, a colonoscopy was performed, indicating that the colon from the anal verge to approximately 22 cm was narrowed, and the endoscopy could not pass through. The rectal and sigmoid colon mucosa showed diffuse erythema, with inflammatory exudates, multiple sizes of erosions and ulcers, disappearance of vascular texture, and increased congestion and edema of the surrounding mucosa, with increased fragility (Figure 1). The pathology indicated active chronic colitis in the ileocecal, ascending, descending, and rectosigmoid junction regions, with atrophy of some glands and cryptitis and crypt abscesses (Figure 2). The patient’s admission CRP was 48.35 (mg/L), which was more than twice higher than that of the previous hospitalization. During the hospitalization, intravenous ceftriaxone treatment was ineffective. The patient still had abdominal pain and abdominal distension symptoms, and the frequency and nature of diarrhea did not improve. Combined with the patient’s medication history, colonoscopy and pathological examination, the immune checkpoint inhibitory colitis CTCAE grade 3 was considered. In terms of treatment, methylprednisolone sodium 60mg was given intravenously, parenteral nutrition was provided, and PPI antacid, calcitriol, vitamin D, and potassium citrate were given to prevent adverse reactions to hormones. Blood pressure, blood sugar, and other adverse reactions were monitored. The abdominal pain and abdominal distension symptoms improved significantly within 3 days of treatment, the frequency of diarrhea decreased significantly, about 2–3 times per day, and the blood and mucus in the stool decreased. Oral intake began, and the hormone was changed to Methylprednisolone Tablets 48mg (12 tablets) after discharge. After 25 days (2024-02-25), the patient was re-examined in the outpatient clinic, with disappearance of abdominal pain and abdominal distension, the frequency of diarrhea returning to 1–2 times per day, and the stool nature returning to normal. The hormone dosage was reduced to 36mg per day. At this time, the serum CRP significantly decreased. A colonoscopy was re-performed, and the intestinal mucosa showed significant improvement. The intestinal stenosis and ulcers disappeared. The mucosa of the ascending colon, transverse colon, descending colon and sigmoid colon was smooth, with clear vascular networks. No ulcers or tumors were observed. The rectal mucosa about 10 cm below the anal verge was congested and edematous, and patchy erosion was visible (Figure 3). The pathology suggested: [Ascending colon] active chronic colitis, with glandular branches, and occasional cryptitis. [Transverse colon, sigmoid colon, rectum] active chronic colitis, with slightly twisted glands, and occasional cryptitis (Figure 4). At this time, the re-examination of serum tumor markers indicated that CEA was slightly elevated, and CA199 was significantly elevated. At this point, the assessment of the tumor suggested tumor progression. According to the CTCAE diagnostic grading standard, the patient’s colitis had reached grade 3 or above. Therefore, the treatment was stopped with Sintilimab, and the treatment plan was changed to Fruquintinib + Tegafur, Gimeracil and Oteracil Porassium Capsules, with the hormone dosage reduced by 4 mg every week. Unfortunately, the patient was admitted to the hospital for the last time due to severe pneumonia combined with multiple pulmonary metastases on April 6, 2024, and lost follow-up.
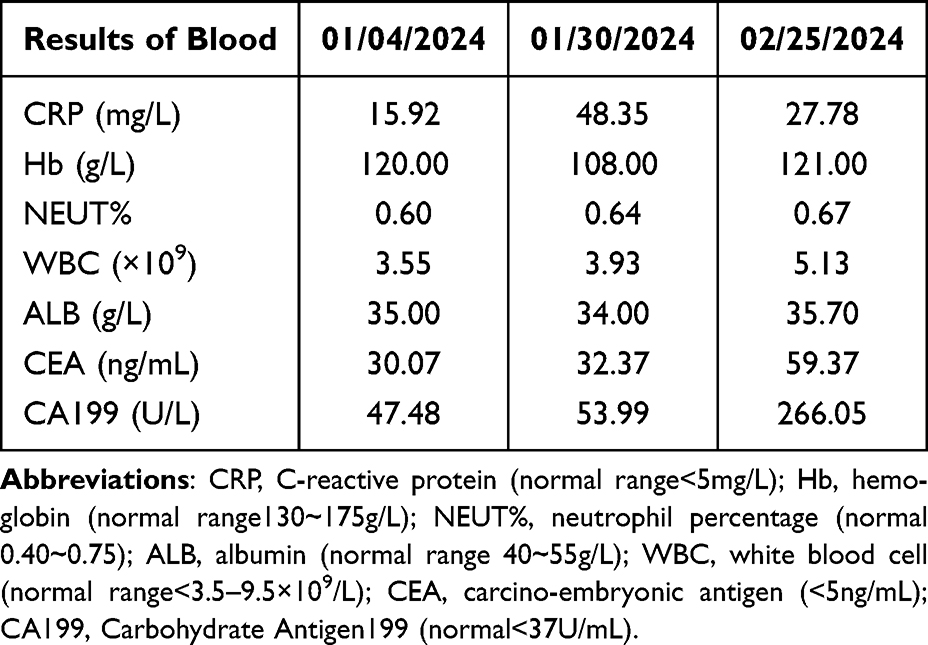 |
Table 1 The Results of Blood of the Patient |
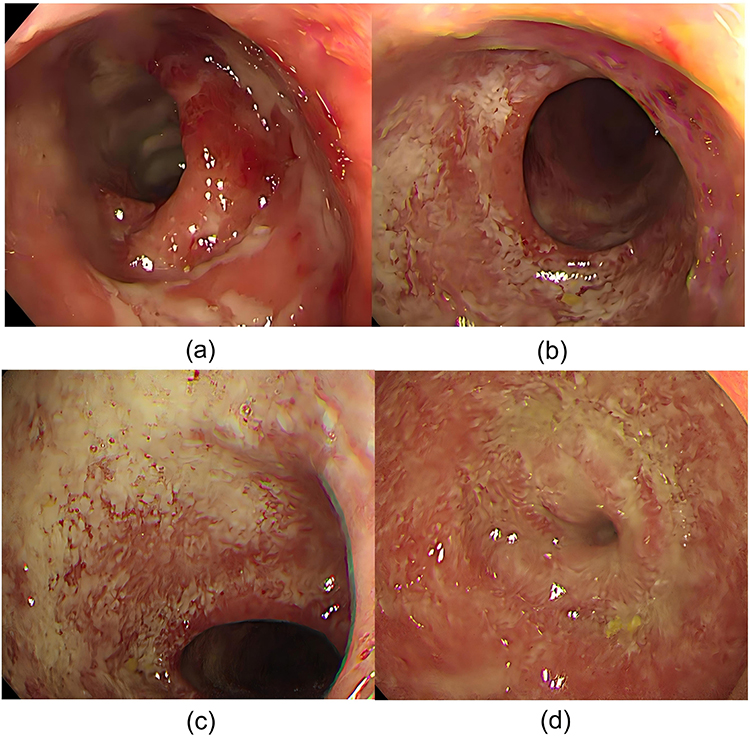 |
Figure 1 (a) The rectal mucosa shows diffuse erythema, with inflammatory exudates, multiple erosions and shallow ulcers of varying sizes, disappearance of vascular structures, hyperemia of the surrounding mucosa, and increased fragility. (b and c) The surface mucosa of the sigmoid colon is diffusely hyperemic and edematous, with erosions of varying sizes and disappearance of vascular structures. A large amount of mucus and fibrin-like attachments are visible, and fragility is increased. (d) The mucosa of the sigmoid colon is extensively hyperemic and edematous, with shallow erosions. A large amount of mucus and fibrin-like exudates are attached, and the lumen is significantly narrowed, with the endoscope unable to pass through. |
 |
Figure 2 [Rectum and Sigmoid Colon] Active chronic colitis, with partial glandular atrophy, showing cryptitis and crypt abscesses.Original magnification: (a)×40, (b) ×100, and (c) ×200. |
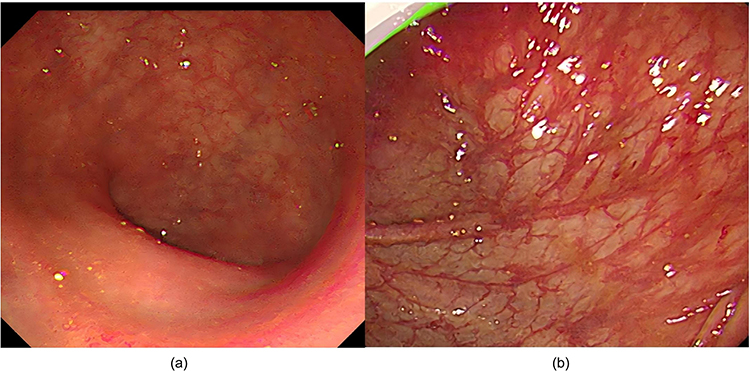 |
Figure 3 (a) The surface of the rectal mucosa is smooth, with no ulcers or erosions observed, and the vascular network is clear. (b) The surface of the sigmoid colon mucosa is smooth, and there is no congestion, edema, or erosion. |
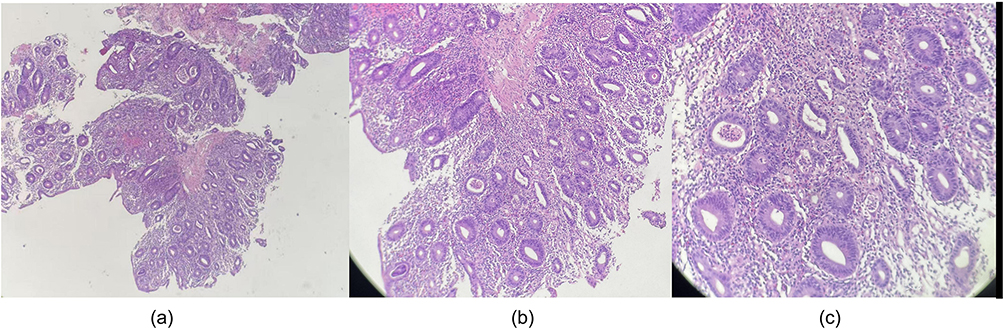 |
Figure 4 Pathological findings: [Ascending Colon] Active chronic colitis, with glandular branches, occasional cryptitis. [Transverse Colon, Sigmoid Colon, Rectum] Active chronic colitis, with slightly twisted glands, occasional cryptitis. Permeates the edematous stroma. Original magnification: Figure (a) ×40, (b) ×100, and (c) ×200. |
Discussion
Immune checkpoint inhibitors (ICI), such as programmed death 1/ligand 1 (PD-1/L1) inhibitors and cytotoxic T lymphocyte-associated protein 4 (CTLA-4) inhibitors, are promising drugs that can enhance the immune system in cancer treatment.12 Immune checkpoint molecules play a crucial role in regulating self-antigen tolerance; therefore, blocking immune checkpoint molecules such as anti-CTLA-4 or anti-PD-1 can lead to autoimmune damage, resulting in irAE.13 The mechanism of ICI-induced colitis seems to be related to autoimmune events. Although the pathogenesis is not fully understood, the key factors include excessive activation of T cells, increased memory T cells, lymphocyte infiltration, activation of cytokines, and changes in the interaction between the intestinal microbiota and the immune system.14 Research shows that there is a study indicating that CD8+ tissue-resident memory T (TRM) cells are the main activated T cell subset in ICI colitis.15,16 These cells express CD69 and CD10, and they influence mucosal immunity by recruiting CD8 and CD4 T cells from the general circulation. In ICI colitis, TRM CD8+ cells differentiate into cytotoxic T lymphocytes, which can release interferon-γ (IFNγ), thereby damaging the intestinal epithelial barrier.15 Studies have detected an increase in the content of Tregs in colonic inflammation.17,18 Under normal circumstances, Tregs can suppress intestinal inflammation, and this function is clearly impaired in IMC.19 In colon biopsies of IMC patients, ipilimumab treatment often leads to an increase in the number of Tregs, defined as FOXP3+ cells.20
After immunotherapy, a systemic lymphocyte expansion was also observed. Compared with patients without colitis, the circulating lymphocyte levels in patients with colitis who received anti-CTLA-4 and anti-PD-1 immune checkpoint inhibitor immunotherapy showed a statistically significant increase.21 Specifically, the proliferation of Th1 CD4 cells throughout the body is obvious. During the treatment with anti-CTLA-4 immune checkpoint inhibitors, the HLA-DR/CD25/CD8 T cells and antigen-specific CD8 T cells in the peripheral blood also significantly increase and become activated.22 Furthermore, the gene expression profile of peripheral blood from patients treated with anti-CTLA-4 immune checkpoint inhibitors showed significant increases in two neutrophil activation markers: CD177 and carcinoembryonic antigen-related cell adhesion molecule (CEACAM). CD177 is a specific neutrophil surface biomarker that plays a role in activating neutrophils and recruiting inflammatory cells. CEACAM is an essential adhesion molecule for neutrophil migration. The significant increase of these markers in the peripheral blood of patients with immune checkpoint inhibitor-related colitis indicates that neutrophils may be involved in the pathogenesis of immune checkpoint inhibitor-related colitis.23 Cytokines have been proven to be important mediators of intestinal inflammation. The activation of T cells related to immune checkpoint inhibitors leads to the secretion of high levels of cytokines. These cytokines induce T cell proliferation, promote the infiltration of neutrophils and cytotoxic CD8 T cells into the tissues, impair the function of Treg cells, and increase the number of T helper 17 cells. This carefully coordinated cytokine response mediates the pathogenesis of colitis.5 The Th1 and Th17 responses are highly correlated with the pathogenesis of intestinal inflammation. Compared with healthy colons, the mRNA levels in the colons of patients with ICI colitis and IBD show upregulation of the IFNγ, IL-17 effector pathways, and TNF.20 IL-17 plays a role in the fibrosis process in many organs (including the intestine) by activating myofibroblasts and increasing collagen production.24,25 Compared with healthy controls and patients without colitis, ICI colitis is rich in mucosal Th1 effector cells, which highly express IFNγ-induced genes such as STAT1, CD74 and GBP1/5.17 Furthermore, compared to normal tissues, IL-6 is a crucial cytokine for the differentiation of naive T cells into Th17 cells. It is upregulated in the colon tissues of patients with irAE of colitis.26 In fact, it has been discovered that blocking IL-6 not only improves irAE in colitis, but also enhances the anti-tumor efficacy of the anti-CTLA-4 therapy in both mouse models and patient cohorts.26 These data collectively demonstrate the role of Th1 and Th17 effector cytokines in driving the pathogenesis of ICI colitis. A recent study using spatial transcriptomics confirmed that the production of type I and type III cytokines (including IL-17A) in inflamed colonic mucosa increased.27 The infiltrating myeloid cells of IMC patients express high levels of pro-inflammatory cytokines, such as TNF-α and IL-1β, which ultimately leads to the recruitment of immune cells from the blood and tissues to deal with the damage.17 Jonathan et al28 discovered through whole-transcriptome RNA sequencing, single-cell RNA sequencing and flow cytometry that IL-23 plays a significant role in promoting inflammation, as it can induce the production of cytotoxic lymphocytes with multifunctional IFNγ. These inflammatory factors can cause various gastrointestinal functional disorders, including movement problems, due to the excitation of the sympathetic nerve and inhibition of the parasympathetic nerve in the gut. The reduced intestinal peristalsis, combined with intestinal wall edema and fluid accumulation, and the accumulation of intestinal contents, leads to non-functional or paralytic intestinal obstruction.
The gut microbiota is increasingly being regarded as one of the potential mechanisms involved in the development of colitis caused by immune checkpoint inhibitors.29 The gut microbiome regulates both innate and adaptive immunity, exerting a significant influence on the human immune system. The pattern recognition receptors (PRR) of intestinal epithelial cells are activated by the gut microbiome, and the downstream signal transduction regulates the antibacterial response through the expression of pro-inflammatory cytokines such as tumor necrosis factor, IL-1, and IL-6.30,31 When immune checkpoint inhibitor-related colitis occurs, the diversity of the microbiota decreases and the composition of the microbiota changes. More specifically, the abundance of the Firmicutes phylum in patients with immune checkpoint inhibitor-related colitis is significantly reduced, while the abundance of the Bacteroidetes phylum is higher in patients without colitis.32 Based on the known interactions between the gut microbiota and IMC, the main mechanisms include direct action, metabolites, cytokines and immune cells. For protective bacteria, pro-inflammatory pathways such as IL-1b and TNF-a, as well as the promoted anti-inflammatory pathways (including IL-10, Th17 cells and Treg cells), are inhibited. They also regulate the differentiation of T cells through vitamins B and the tricarboxylic acid cycle. The butyrate produced by bacteria plays an anti-inflammatory role by strengthening tight junctions, inducing IL-10 and inhibiting NF-κB, among other aspects. As for harmful bacteria, they secrete some enzymes to destroy mucins and enhance pro-inflammatory pathways, such as IL-6, TNF-a, CRP and antigen production.33 The pathogenic effect of the microbiota may be caused by multiple mechanisms. Microorganisms can activate myofibroblasts through their pathogen-associated molecular patterns (PAMPs), which are sensed by similar receptors (TLRs) present in mesenchymal cells. Subsequently, this triggers the MyD88-nuclear factor (NF)-κB signaling pathway. This activation leads to the production of TGF-β1 and the initiation of fibrosis.34,35 Meanwhile, microorganisms can induce inflammation and fibrosis by interacting with TLRs expressed by intestinal epithelial cells and immune cells. They stimulate the production of chemical factors, cytokines or reactive oxygen species, and activate intestinal fibroblasts. During this process, macrophages may play a central role, as they can polarize towards the M2 phenotype in response to PAMPs (such as flagellin, microbial lipopolysaccharides and microbial metabolites), ultimately promoting fibrosis.36
According to the current research, the colonic stenosis caused by immune checkpoint inhibitors may be the result of the combined effects of chronic immune inflammation, dysbiosis of the microbiota, and imbalance in tissue repair. The underlying mechanisms may include: excessive activation and infiltration of effector T cells (especially CD8⁺ T cells), disruption of the intestinal microbiota weakening the barrier function, and continuous activation of the TGF-β-driven fibrotic pathway. At present, there are relatively few clinical reports on IMC combined with colonic stenosis or obstruction. Shunde Tan et al37 reported a 40-year-old adult patient with primary liver cancer who received ICI (Sintilimab) combined with vascular endothelial growth factor (VEGF) inhibitor (Bevacizumab). About 5 days after immunotherapy, severe diarrhea occurred, and finally diagnosed as IMC and inflammatory intestinal obstruction. After receiving combined treatment with glucocorticoids and somatostatin, the condition improved. In the cases reported here, we present a patient with advanced colorectal cancer with lung metastasis who received treatment with Sintilimab combined with Fruquintinib. The patient developed symptoms of inflammatory intestinal obstruction. Eventually, the patient’s symptoms were significantly relieved with glucocorticoids, and the frequency of diarrhea decreased significantly. After 25 days of re-examination, the intestinal stenosis and mucosal ulcers in the colon had disappeared. Unfortunately, this patient lost follow-up due to lung metastasis. Some studies have shown that exposure to high-dose steroids may be associated with a reduced overall survival in cancer patients receiving IPI (immune checkpoint inhibitors) treatment.38–40 It is impossible to determine whether the tumor progression of this patient is related to the high-dose glucocorticoid. It is also possible that the disease progression was caused by the patient’s own disease progression or treatment resistance. Although immune checkpoint inhibitors (ICI) significantly improve the prognosis of patients with different tumor entities, they also cause considerable toxicity. During the use of (ICIs) immunotherapy, we need to closely monitor and be vigilant for the occurrence of immune-related side effects. According to our case, the early use of glucocorticoids may be effective and can minimize the risk of intestinal toxicity. However, it should be noted that the application of high-dose corticosteroids may have an adverse effect on the treatment of tumors.
Ethical Approval
As the patient has passed away, the patient’s daughter has signed a written informed consent form, agreeing to use all the images and data contained in this article for publication. This study adheres to the provisions of the Helsinki Declaration (revised in 2013). According to institutional requirements, there is no need for ethical review and approval before publishing the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–8. doi:10.1056/NEJMoa1712126
2. Raskov H, Orhan A, Christensen JP, Gögenur I. Cytotoxic CD8(+) T cells in cancer and cancer immunotherapy. Br J Cancer. 2021;124(2):359–367. doi:10.1038/s41416-020-01048-4
3. Zhang H, Dai Z, Wu W, et al. Regulatory mechanisms of immune checkpoints PD-L1 and CTLA-4 in cancer. J Exp Clin Cancer Res. 2021;40(1):184. doi:10.1186/s13046-021-01987-7
4. Peng L, Wu Z, Sun W, Wang C. Clinical characteristics, treatment, and outcomes of nivolumab induced immune thrombocytopenia. Invest New Drugs. 2024;42(5):575–580. doi:10.1007/s10637-024-01472-w
5. Ramos-Casals M, Brahmer JR, Callahan MK, et al. Immune-related adverse events of checkpoint inhibitors. Nat Rev Dis Primers. 2020;6(1):38. doi:10.1038/s41572-020-0160-6
6. Shiravand Y, Khodadadi F, Kashani SMA, et al. Immune checkpoint inhibitors in cancer therapy. Curr Oncol. 2022;29(5):3044–3060. doi:10.3390/curroncol29050247
7. Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4(12):1721–1728. doi:10.1001/jamaoncol.2018.3923
8. Li H, Wang Z, Guan Z, et al. UCFNNet: ulcerative colitis evaluation based on fine-grained lesion learner and noise suppression gating. Comput Methods Programs Biomed. 2024;247:108080. doi:10.1016/j.cmpb.2024.108080
9. Sun BL, Elliott AS, Nolte D, Sun X. Immune checkpoint inhibitor-related colitis in patients on immunotherapy for cancer. Am J Clin Pathol. 2024;162(1):17–27. doi:10.1093/ajcp/aqae002
10. Jiang W, Yin J, Han M, et al. N4BP3 activates TLR4-NF-κB pathway in inflammatory bowel disease by promoting K48-linked IκBα Ubiquitination. J Inflamm Res. 2025;18:7167–7181. doi:10.2147/jir.S518155
11. Liu X, Yi Y. Recent updates on Sintilimab in solid tumor immunotherapy. Biomark Res. 2020;8(1):69. doi:10.1186/s40364-020-00250-z
12. Marin-Acevedo JA, Kimbrough EO, Lou Y. Next generation of immune checkpoint inhibitors and beyond. J Hematol Oncol. 2021;14(1):45. doi:10.1186/s13045-021-01056-8
13. Khan S, Gerber DE. Autoimmunity, checkpoint inhibitor therapy and immune-related adverse events: a review. Semin Cancer Biol. 2020;64:93–101. doi:10.1016/j.semcancer.2019.06.012
14. Zoghbi M, Burk KJ, Haroun E, Saade M, Carreras MTC. Immune checkpoint inhibitor-induced diarrhea and colitis: an overview. Support Care Cancer. 2024;32(10):680. doi:10.1007/s00520-024-08889-2
15. Sasson SC, Slevin SM, Cheung VTF, et al. Interferon-gamma-producing CD8(+) tissue resident memory T cells are a targetable hallmark of immune checkpoint inhibitor-colitis. Gastroenterology. 2021;161(4):1229–1244.e1229. doi:10.1053/j.gastro.2021.06.025
16. Gupta T, Antanaviciute A, Hyun-Jung Lee C, et al. Tracking in situ checkpoint inhibitor-bound target T cells in patients with checkpoint-induced colitis. Cancer Cell. 2024;42(5):797–814.e715. doi:10.1016/j.ccell.2024.04.010
17. Luoma AM, Suo S, Williams HL, et al. Molecular pathways of colon inflammation induced by cancer immunotherapy. Cell. 2020;182(3):655–671.e622. doi:10.1016/j.cell.2020.06.001
18. Thomas MF, Slowikowski K, Manakongtreecheep K, et al. Single-cell transcriptomic analyses reveal distinct immune cell contributions to epithelial barrier dysfunction in checkpoint inhibitor colitis. Nat Med. 2024;30(5):1349–1362. doi:10.1038/s41591-024-02895-x
19. Izcue A, Coombes JL, Powrie F. Regulatory T cells suppress systemic and mucosal immune activation to control intestinal inflammation. Immunol Rev. 2006;212:256–271. doi:10.1111/j.0105-2896.2006.00423.x
20. Bamias G, Delladetsima I, Perdiki M, et al. Immunological Characteristics of Colitis Associated with Anti-CTLA-4 Antibody Therapy. Cancer Invest. 2017;35(7):443–455. doi:10.1080/07357907.2017.1324032
21. Nahar KJ, Marsh-Wakefield F, Rawson RV, et al. Distinct pretreatment innate immune landscape and posttreatment T cell responses underlie immunotherapy-induced colitis. JCI Insight. 2022;7(21):e157839. doi:10.1172/jci.insight.157839
22. Tietze JK, Angelova D, Heppt MV, et al. The proportion of circulating CD45RO(+)CD8(+) memory T cells is correlated with clinical response in melanoma patients treated with ipilimumab. Eur J Cancer. 2017;75:268–279. doi:10.1016/j.ejca.2016.12.031
23. Shahabi V, Berman D, Chasalow SD, et al. Gene expression profiling of whole blood in ipilimumab-treated patients for identification of potential biomarkers of immune-related gastrointestinal adverse events. J Transl Med. 2013;11:75. doi:10.1186/1479-5876-11-75
24. Ruiz de Morales JMG, Puig L, Daudén E, et al. Critical role of interleukin (IL)-17 in inflammatory and immune disorders: an updated review of the evidence focusing in controversies. Autoimmun Rev. 2020;19(1):102429. doi:10.1016/j.autrev.2019.102429
25. Speca S, Giusti I, Rieder F, Latella G. Cellular and molecular mechanisms of intestinal fibrosis. World J Gastroenterol. 2012;18(28):3635–3661. doi:10.3748/wjg.v18.i28.3635
26. Hailemichael Y, Johnson DH, Abdel-Wahab N, et al. Interleukin-6 blockade abrogates immunotherapy toxicity and promotes tumor immunity. Cancer Cell. 2022;40(5):509–523.e506. doi:10.1016/j.ccell.2022.04.004
27. Dimitriou F, Cheng PF, Saltari A, et al. A targetable type III immune response with increase of IL-17A expressing CD4(+) T cells is associated with immunotherapy-induced toxicity in melanoma. Nat Cancer. 2024;5(9):1390–1408. doi:10.1038/s43018-024-00810-4
28. Lo JW, Cozzetto D, Alexander JL, et al. Immune checkpoint inhibitor-induced colitis is mediated by polyfunctional lymphocytes and is dependent on an IL23/IFNγ axis. Nat Commun. 2023;14(1):6719. doi:10.1038/s41467-023-41798-2
29. Zhou CB, Zhou YL, Fang JY. Gut microbiota in cancer immune response and immunotherapy. Trends Cancer. 2021;7(7):647–660. doi:10.1016/j.trecan.2021.01.010
30. Thaiss CA, Zmora N, Levy M, Elinav E. The microbiome and innate immunity. Nature. 2016;535(7610):65–74. doi:10.1038/nature18847
31. Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell. 2010;140(6):805–820. doi:10.1016/j.cell.2010.01.022
32. Gopalakrishnan V, Spencer CN, Nezi L, et al. Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients. Science. 2018;359(6371):97–103. doi:10.1126/science.aan4236
33. Zhou G, Zhang N, Meng K, Pan F. Interaction between gut microbiota and immune checkpoint inhibitor-related colitis. Front Immunol. 2022;13:1001623. doi:10.3389/fimmu.2022.1001623
34. Zhao S, Dejanovic D, Yao P, et al. Selective deletion of MyD88 signaling in α-SMA positive cells ameliorates experimental intestinal fibrosis via post-transcriptional regulation. Mucosal Immunol. 2020;13(4):665–678. doi:10.1038/s41385-020-0259-9
35. Zhao Z, Cheng W, Qu W, Shao G, Liu S. Antibiotic alleviates radiation-induced intestinal injury by remodeling microbiota, reducing inflammation, and inhibiting fibrosis. ACS Omega. 2020;5(6):2967–2977. doi:10.1021/acsomega.9b03906
36. Amamou A, O’Mahony C, Leboutte M, Savoye G, Ghosh S, Marion-Letellier R. Gut microbiota, macrophages and diet: an intriguing new triangle in intestinal fibrosis. Microorganisms. 2022;10(3):490. doi:10.3390/microorganisms10030490
37. Tan S, Zhu G, Fan J, et al. Immune checkpoint inhibitor-induced colitis complicated with inflammatory intestinal obstruction: a case report and literature review. Transl Cancer Res. 2022;11(7):2443–2448. doi:10.21037/tcr-21-2501
38. Arbour KC, Mezquita L, Long N, et al. Impact of baseline steroids on efficacy of programmed cell death-1 and programmed death-ligand 1 blockade in patients with non-small-cell lung cancer. J Clin Oncol. 2018;36(28):2872–2878. doi:10.1200/jco.2018.79.0006
39. Faje AT, Lawrence D, Flaherty K, et al. High-dose glucocorticoids for the treatment of ipilimumab-induced hypophysitis is associated with reduced survival in patients with melanoma. Cancer. 2018;124(18):3706–3714. doi:10.1002/cncr.31629
40. Verheijden RJ, de Groot JS, Fabriek BO, Hew MN, May AM, Suijkerbuijk KPM. Corticosteroids for immune-related adverse events and checkpoint inhibitor efficacy: analysis of six clinical trials. J Clin Oncol. 2024;42(31):3713–3724. doi:10.1200/jco.24.00191
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Biologic Therapy for Refractory Immune Checkpoint Inhibitor Colitis
Alorfi NM, Alourfi MM
Biologics: Targets and Therapy 2022, 16:119-127
Published Date: 5 August 2022
Immune-Related Colitis Induced by Camrelizumab: A Case Report
Cheng S, Yang Y, Yu J, Chen W, Li X
Journal of Inflammation Research 2023, 16:1727-1731
Published Date: 18 April 2023
Risk Factors and Prognostic Analysis of Immune Checkpoint Inhibitor-Related Colitis in Lung Cancer
Wang S, Tian B, Wang H
Journal of Inflammation Research 2024, 17:7535-7542
Published Date: 21 October 2024
Case Report and Literature Review on Skin Toxicity Induced by PD-1 Inhibitor in a Penile Cancer with Massive Ulceration of Chemoradiotherapy-Resistant and Successful Treatment by Immunotherapy
Zhu Y, Cai D, Jiang J, Tu J, Tian Z, Zhang X, Luo S, Wang Y
Clinical, Cosmetic and Investigational Dermatology 2025, 18:699-707
Published Date: 22 March 2025
C-Reactive Protein in Immune Checkpoint Inhibitor-Associated Colitis: A Scoping Review of Evidence and Knowledge Gaps
Ohta R, Ryu Y, Tanaka K, Sano C, Hayashi H
Cancer Management and Research 2025, 17:2631-2641
Published Date: 7 November 2025