Back to Journals » Journal of Inflammation Research » Volume 16
Immune-Related Colitis Induced by Camrelizumab: A Case Report
Authors Cheng S, Yang Y, Yu J, Chen W, Li X ![]()
Received 3 February 2023
Accepted for publication 11 April 2023
Published 18 April 2023 Volume 2023:16 Pages 1727—1731
DOI https://doi.org/10.2147/JIR.S405023
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Sheng Cheng,1 Yun Yang,2 Junxian Yu,1 Wei Chen,1 Xingang Li1
1Department of Pharmacy, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of General Surgery, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Xingang Li, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China, Email [email protected]
Abstract: In recent years, immunotherapy has become a major research focus in the field of cancer treatment. Because of its good efficacy and lasting immune response, immune checkpoint inhibitors have benefited the long-term survival of many types of cancer patients. However, overactivation of the immune system may attack normal organs and cause a series of immune related adverse reactions. Among them, due to the high incidence of immune-related colitis, it deserves special attention. Camrelizumab is a programmed cell death 1 (PD-1) inhibitor that was developed by Jiangsu Hengrui Medicine Company. We reported the clinical data of a case of hepatocellular carcinoma with immune-related colitis after treatment with camrelizumab. A 63-year-old man with hepatocellular carcinoma developed diarrhea and hematochezia after receiving 4 cycles of camrelizumab. Endoscopy showed multiple flake congestion and edema in the terminal ileum and total colon mucosa with bright red surface. Pathological evaluation showed chronic inflammation of colonic mucosa. After giving 0.25g bid of enteric-coated sulfasalazine tablets orally for 6 weeks, his colitis improved. Camrelizumab can induce immune-related colitis. Sulfasalazine could be used to reduce adverse reactions of glucocorticoids.
Keywords: immune checkpoint inhibitor, colitis, anti-programmed cell death blockade, immune-related colitis, camrelizumab
Introduction
In recent years, immunotherapy has become a major research focus in the field of cancer treatment. Because of its good efficacy and lasting immune response, immune checkpoint inhibitors (ICI) have benefited the long-term survival of many types of cancer patients. Programmed death protein ligand (PD-1) inhibitor is one of ICIs. It mainly acts on PD-1 receptor, blocks the negative regulation mechanism of tumor cells, and restores the killing effect of immune system on tumor cells.1 PD-L1 is a ligand of PD-1, which is highly expressed on the surface of tumor cells. The binding of PD-1 and PD-L1 has negative regulation effect that inhibits the proliferation and differentiation of T cells and secretion of cytokines, and enables tumor cell to escape immune surveillance.2 However, ICIs usage is associated with multiple immune‐related adverse events (irAEs) in some patients. The most two common gastrointestinal disorders reported in clinical practice are diarrhea and colitis, which generally occur 6 to 8 weeks after treatment initiation.3,4 The incidence was during PD-1/PD-L1 inhibitor monotherapy with 1.3% for all-grade colitis, 0.9% for severe colitis.5 The risks and predictive biomarkers for colitis are still unclear.6 Hepatocellular carcinoma is the most common primary liver cancer. Camrelizumab is one of PD-1 inhibitor, and it was approved for the treatment of patients with relapsed or refractory classical Hodgkin lymphoma, hepatocellular carcinoma, non-small cell lung cancer, esophageal squamous carcinoma and nasopharyngeal carcinoma. The most common adverse reactions of camrelizumab include cutaneous capillary endothelial hyperplasia, anemia, leukopenia, aspartate aminotransferase and alanine aminotransferase elevation.7 Colitis caused by camrelizumab was rarely reported. Here, we report a case of a patient with hepatocellular carcinoma who developed colitis 21 days after treatment of camrelizumab.
Case Presentation
The patient was a 63-year-old male with chronic hepatitis B for 40 years, cirrhosis for 10 years, duodenal varicose vein sclerosis, type 2 diabetes for 5 years, and thrombocytopenia for 5 years.
In June 2018, the patient was diagnosed with hepatocellular carcinoma and undergone right lobe hepatectomy. Sorafenib 400mg bid was taken orally for 6 months after operation. On November 1, 2018, the electronic colonoscope showed multiple telangiectasia of the colon. In June 2019, percutaneous transhepatic portal vein and duodenal vein embolization was performed once. In August 2020, pulmonary metastasis and mediastinal lymph node metastasis were observed. Bronchial artery infusion (BAI) and splenic artery infusion chemotherapy were performed three times on September 29 and November 13, 2020, with regimen consisted of pirarubicin 60mg, fluorouracil 750mg, oxaliplatin 50mg and interleukin 2 million IU, and on December 18, 2020, with regimen consisted of gemcitabine 1g and cisplatin 40mg. The patient was also treated with 200mg of camrelizumab for four courses from September 14, 2020, to March 29, 2021. After 21 days of the last dose of camrelizumab, diarrhea appeared and gradually worsened with 5 to 6 episodes of thin mucus and bloody stools from April 19, 2021, but without abdominal pain. The blood cell analysis showed: white blood cell count (WBC) 2.93×109/L, platelet count (PLT) was 72×109/L, hemoglobin (HB) was 138g/L and C-reactive protein was 4.42 mg/L.
Afterwards, patient was admitted to hospital. His lab profile revealed alanine aminotransferase (ALT): 28U/L, serum total bilirubin (Tbil): 32.43 umol/L, serum creatinine (Cr): 45.8 umol/L, hepatitis B surface antigen (HBsAg): 0.6IU/mL. Hepatitis C antibody was negative indicated that Hepatitis C infection was excluded. Routine stool on April 21 showed brown loose stool with OB+ and red blood cell (RBC) 2/HP. No pathogenic bacterium grew in a stool culture, so we excluded infection. Abdominal CT showed there were no morphologic abnormalities of colon and rectum. Immunotherapy was interrupted. On April 23, 2021, colonoscopy showed multiple flake congestion and edema in the terminal ileum and colon mucosa. Histopathological evaluation showed chronic inflammation of colonic mucosa (Figure 1). On April 24, loperamide 5mg bid as a symptomatic treatment was given. The patient has shown improvement, with a decrease in mucus and non-bloody diarrhea to once a day. After oral administration of enteric-coated sulfasalazine capsule, 0.25g bid was given for 6 weeks, diarrhea and bloody stool disappeared. On June 8, 2021, colonoscopy showed congestion and edema of colonic mucosa, and scattered patchy erythema mainly in descending colon and sigmoid colon. The biopsy specimens were taken from the erythematous mucosa of transverse colon (Figure 1). Pathological evaluation showed chronic inflammation of colonic mucosa and hyperplastic polyp. BAI chemotherapy consisting of gemcitabine 1g, cisplatin 40mg, and interleukin-2200 IU was administered on September 7, 2021. On September 30, immune therapy was resumed. Two hundred milligrams of camrelizumab was given. No obvious discomfort occurred during follow-up. Colonoscopy was performed again in January 2022, and no colonic disease was found.
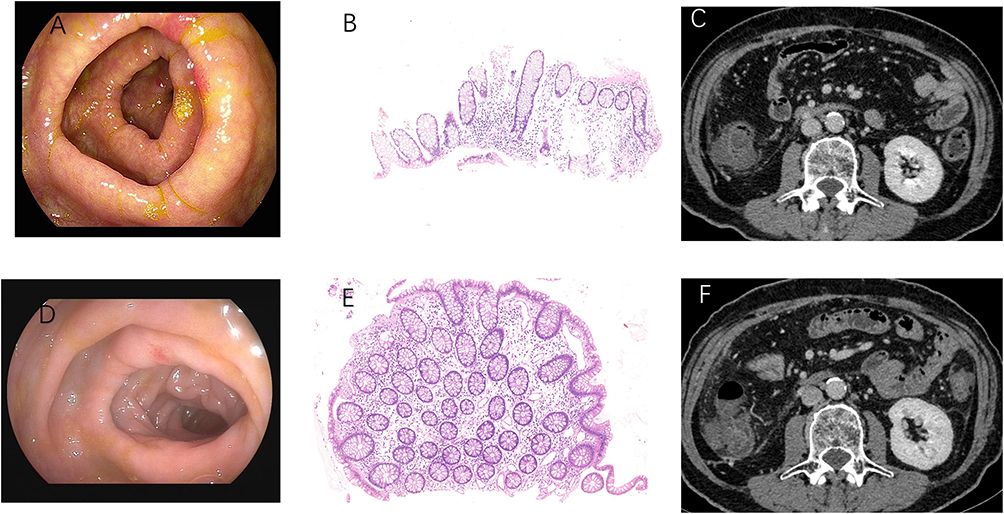 |
Figure 1 Colonoscopy revealed multiple hyperemia and edema of the transverse colon (A). Hematoxylin and eosin stained revealed chronic inflammation of colonic mucosa (B). No obvious abnormality was found on abdominal CT (C). The colonoscopy (D), hematoxylin and eosin stained (E) and abdominal CT (F) after sulfasalazine treatment. |
Discussion
In this case, the patient obtained different treatments. When the patient developed colitis, both infectious diseases and immune-related colitis could not be ruled out. So, we performed blood, stool, CT imaging and endoscopic evaluation to identify the causes of colitis. Then, we tended to think that the colitis might be caused by the administration of camrelizumab. But based on a Phase II clinical study of camrelizumab for the treatment of advanced hepatocellular carcinoma, immune-related adverse events were reported in 181 (83%) of 217 patients.8 The most common irAE was reactive cutaneous capillary endothelial proliferation (67%). There was no immune-related colitis reported in this study. So, immune-related colitis is not a common adverse event of camrelizumab. But the onset of diarrhea in patients did not consistently coincide with the timing of administration of other medications. Also, when the patient withhold camrelizumab, his pathological finding was improved quickly. We were almost certain that the colitis was caused by the camrelizumab.
The typical symptom of immune-related colitis is diarrhea. Most patients may have abdominal pain, nausea and vomiting. The occurrence time of immune-related colitis is generally 0~6.3 months after beginning of treatment, and the median occurrence time of immune-related colitis caused by PD-1 inhibitor is 25 weeks after treatment.9 As Immune-related colitis can be life-threatening, early diagnosis and management based on grading are important. In patients with grade 2 colitis, symptoms, blood, stool, and CT imaging are recommended for investigation. For patients with severe grade 3/4 colitis, digestive consultation should be considered and endoscopic evaluation is recommended. Endoscopy has the advantages of distinguishing immune-related colitis from other causes of colitis and of providing information on disease severity, which can be used to decide whether to continue immune therapy. If the patients develop immune-related colitis of G2 or above, immunotherapy should be interrupted. After the recovery of colitis, some patients may continue to be treated with ICIs. A retrospective study showed that among 93 patients with immune-related adverse events, 40 patients resumed PD-1 inhibitor treatment, and 17 patients relapsed with the same type of immune-related adverse events.10
Early treatment with corticosteroids can reduce potentially life-threatening factors caused by colitis. Depending on the severity of diarrhea/colitis, the management methods are different (Table 1).11–13 Although the guidelines do not recommend sulfasalazine for immune-related colitis treatment, some studies have found that sulfasalazine can significantly reduce the symptoms of immune-related colitis.14,15 Considering the mild symptoms of the patient, sulfasalazine is appropriate for treatment or maintenance treatment.
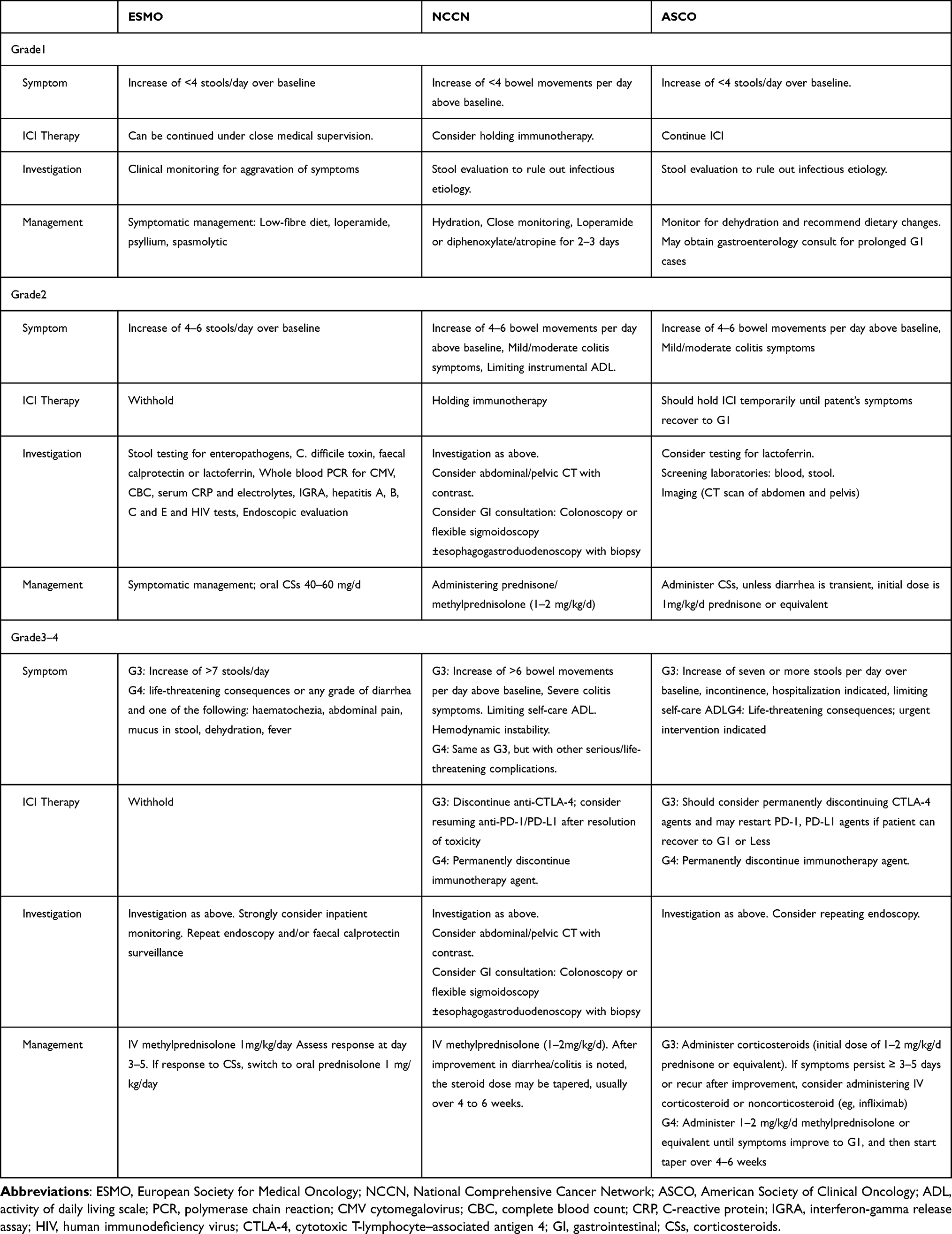 |
Table 1 Management of Immune-Related Colitis |
Conclusions
We report a case of colitis induced by PD-1 inhibitor, camrelizumab. Diarrhea and hematochezia after camrelizumab treatment may be considered of immune-related colitis. Colonoscopy, mucosal biopsies, abdominal CT scan are necessary for the diagnosis of colitis. Interruption of the immunotherapy is recommended for immune-related colitis with G2 and above. Sulfasalazine could be one of the treatment options for immune-related colitis.
Ethics Approval
This article was performed in accordance with the principles of Declaration of Helsinki. Ethical review and approval was not required to publish the case details in accordance with the local legislation and institutional requirements. The authors confirm that written consent for submission and publication of this case report including data and images has been obtained from the patient.
Funding
This study was funded by 2022 Bethune Quest Pharmaceutical Research Capacity Building Project of Bethune Charitable Foudation (No. 23).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sharpe AH, Pauken KE. The diverse functions of the PD1 inhibitory pathway. Nat Rev Immunol. 2018;18(3):153–167. doi:10.1038/nri.2017.108
2. Thallinger C, Füreder T, Preusser M, et al. Review of cancer treatment with immune checkpoint inhibitors: current concepts, expectations, limitations and pitfalls. Wien Klin Wochenschr. 2018;130(3–4):85–91. doi:10.1007/s00508-017-1285-9
3. Weber JS, Dummer R, de Pril V, Lebbé C, Hodi FS. Patterns of onset and resolution of immune-related adverse events of special interest with ipilimumab: detailed safety analysis from a Phase 3 trial in patients with advanced melanoma. Cancer. 2013;119(9):1675–1682. doi:10.1002/cncr.27969
4. Wang Y, Abu-Sbeih H, Mao E, et al. Endoscopic and histologic features of immune checkpoint inhibitor-related colitis. Inflamm Bowel Dis. 2018;24(8):1695–1705. doi:10.1093/ibd/izy104
5. Wang DY, Ye F, Zhao S, Johnson DB. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology. 2017;6(10):e1344805. doi:10.1080/2162402X.2017.1344805
6. Tandon P, Bourassa-Blanchette S, Bishay K, Parlow S, Laurie SA, McCurdy JD. The risk of diarrhea and colitis in patients with advanced melanoma undergoing immune checkpoint inhibitor therapy: a systematic review and meta-analysis. J Immunother. 2018;41(3):101–108. doi:10.1097/CJI.0000000000000213
7. Fang W, Yang Y, Ma Y, et al. Camrelizumab (SHR-1210) alone or in combination with gemcitabine plus cisplatin for nasopharyngeal carcinoma: results from two single-arm, Phase 1 trials. Lancet Oncol. 2018;19(10):1338–1350. doi:10.1016/S1470-2045(18)30495-9
8. Qin S, Ren Z, Meng Z, et al. Camrelizumab in patients with previously treated advanced hepatocellular carcinoma: a multicentre, open-label, parallel-group, randomised, Phase 2 trial. Lancet Oncol. 2020;21(4):571–580. doi:10.1016/S1470-2045(20)30011-5
9. Tang L, Wang J, Lin N, et al. Immune checkpoint inhibitor-associated colitis: from mechanism to management. Front Immunol. 2021;12:800879. doi:10.3389/fimmu.2021.800879
10. Simonaggio A, Michot JM, Voisin AL, et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer. JAMA Oncol. 2019;5(9):1310–1317. doi:10.1001/jamaoncol.2019.1022
11. Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33(12):1217–1238. doi:10.1016/j.annonc.2022.10.001
12. Thompson JA, Schneider BJ, Brahmer J, et al. NCCN guidelines insights: management of immunotherapy-related toxicities, version 1.2020. J Natl Compr Canc Netw. 2020;18(3):230–241. doi:10.6004/jnccn.2020.0012
13. Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J Clin Oncol. 2018;36(17):1714–1768. doi:10.1200/JCO.2017.77.6385
14. Abu-Sbeih H, Wang Y. Management considerations for immune checkpoint inhibitor-induced enterocolitis based on management of inflammatory bowel disease. Inflamm Bowel Dis. 2020;26(5):662–668. doi:10.1093/ibd/izz212
15. Yamauchi R, Araki T, Mitsuyama K, et al. The characteristics of nivolumab-induced colitis: an evaluation of three cases and a literature review. BMC Gastroenterol. 2018;18(1):135. doi:10.1186/s12876-018-0864-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intestinal Stenosis Related to Immune Checkpoint Inhibitors Caused by Sintilimab: A Case Report
Li HY, Liu Y, Hu SL, Li YQ, Tang TY
Journal of Inflammation Research 2026, 19:556800
Published Date: 10 January 2026