Back to Journals » Cancer Management and Research » Volume 18

Inflammatory and Nutritional Biomarkers Predict Response to Neoadjuvant Dual Anti-HER2 Therapy in HER2-Positive Breast Cancer: A Retrospective Cohort Study
Authors Şahinli H ![]() , Uyar GC, Yeşilbaş E
, Uyar GC, Yeşilbaş E ![]()
Received 26 January 2026
Accepted for publication 7 April 2026
Published 16 April 2026 Volume 2026:18 598948
DOI https://doi.org/10.2147/CMAR.S598948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Hayriye Şahinli, Galip Can Uyar, Enes Yeşilbaş
Department of Medical Oncology, Ankara Etlik City Hospital, Ankara, Turkey
Correspondence: Hayriye Şahinli, Department of Medical Oncology, Ankara Etlik City Hospital, Ankara, Turkey, Email [email protected]
Purpose: Predicting response to neoadjuvant therapy (NAT) remains a clinical challenge in patients with HER2-positive breast cancer (BC). Systemic inflammatory and immune-nutritional biomarkers have emerged as potential predictors of treatment response; however, their value in patients receiving dual anti-HER2 therapy is not well defined.
Patients and Methods: This retrospective study included patients with HER2-positive BC treated with neoadjuvant dual anti-HER2 therapy between January 2023 and February 2025. A total of 136 patients were included. Pathological complete response (pCR) and radiological response assessed by positron emission tomography/computed tomography (PET/CT) were the primary outcomes. Routinely available inflammatory and immune-nutritional indices, including lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), and C-reactive protein–to–albumin ratio (CAR), were evaluated using receiver operating characteristic analysis and multivariable logistic regression. Exploratory RF models were constructed to contextualize regression-based findings, with feature importance assessed using permutation importance and the Gini index. These machine learning analyses were conducted as exploratory, hypothesis-generating tools to support and contextualize regression-based findings rather than to establish standalone predictive models.
Results: Among 136 patients, 74% had locally advanced disease; pCR was achieved in 52.9%, and radiological response in 84.6%. Higher LMR (≥ 2.98) was independently associated with increased odds of pCR, whereas elevated SII and CAR were associated with reduced response. For radiological response, LMR, CAR, baseline CA 15– 3 levels, and intermediate Ki-67 expression (20– 30%) remained independently associated with outcomes. Exploratory machine-learning analyses consistently identified inflammatory and immune-nutritional biomarkers among the most influential predictors.
Conclusion: Routinely available systemic inflammatory and immune-nutritional biomarkers, particularly LMR, SII, and CAR, are independently associated with pathological and radiological response to neoadjuvant dual anti-HER2 therapy in HER2-positive BC. These findings support the potential role of host-related biomarkers in treatment response prediction, pending prospective validation.
Plain Language Summary: In patients with HER2-positive breast cancer, predicting response to neoadjuvant therapy remains challenging. This study evaluated whether simple blood-based inflammatory and nutritional biomarkers, including lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), and C-reactive protein-to-albumin ratio (CAR), are associated with treatment response.
The results showed that these routinely available biomarkers were significantly associated with both pathological complete response and radiological response. Because these markers are inexpensive, widely accessible, and easy to calculate, they may provide a practical tool to support treatment decision-making in real-world clinical settings.
These findings suggest that incorporating host-related biomarkers alongside standard clinical factors may improve response prediction. However, further prospective and multicenter studies are needed before these biomarkers can be routinely used in clinical practice.
Keywords: breast cancer, HER2-positive, neoadjuvant therapy, pathological complete response, inflammation
Introduction
Breast cancer (BC) remains the most frequently diagnosed malignancy among women worldwide, with its incidence continuing to rise annually.1 Approximately 10–34% of invasive BCs exhibit overexpression or amplification of the human epidermal growth factor receptor 2 (HER2), a molecular subtype historically associated with aggressive tumor biology and unfavorable clinical outcomes.2 The introduction of HER2-targeted therapies has substantially improved survival in this population, particularly in the neoadjuvant setting, where dual anti-HER2 regimens have led to marked increases in pathological complete response (pCR) rates.3–5
Neoadjuvant therapy (NAT) is currently established as the standard of care for patients with early-stage and locally advanced HER2-positive BC, offering important clinical advantages such as tumor downstaging, increased breast-conserving surgery rates, and in vivo assessment of treatment efficacy.3–5 Achieving pCR after NAT has been consistently associated with improved long-term outcomes, especially in HER2-positive disease.5 However, despite the widespread use of dual anti-HER2 regimens, a substantial proportion of patients fail to achieve optimal pathological or radiological responses.6 Early identification of patients unlikely to benefit from standard NAT therefore represents a critical unmet clinical need.
Systemic inflammation and nutritional status are increasingly recognized as key modulators of tumor progression, host immune response, and sensitivity to anticancer therapy.7,8 Inflammatory and immune-nutritional biomarkers derived from routine blood tests, such as the lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), and C-reactive protein–to–albumin ratio (CAR), have been associated with prognosis and treatment outcomes across multiple malignancies, including BC.9,10 However, most previous biomarker studies in BC were conducted in heterogeneous patient populations, often before the routine use of dual anti-HER2 therapy, and primarily focused on prognosis rather than direct prediction of neoadjuvant treatment response. Nevertheless, the predictive value of these biomarkers for both pCR and radiological response in patients receiving neoadjuvant dual anti-HER2 therapy remains incompletely defined, and existing evidence in this specific clinical context is limited.
Accordingly, the present study aimed to investigate whether routinely available inflammatory and nutritional biomarkers are associated with pCR and radiological response in patients with HER2-positive BC treated with neoadjuvant dual anti-HER2 therapy. Conventional regression analyses were used to identify independent predictors of treatment response, while exploratory machine learning (ML) methods were applied to support and contextualize biomarker-based predictions and to assess the relative contribution of individual variables.
Materials and Methods
Study Design and Population
This retrospective cohort study included patients with early-stage or locally advanced HER2-positive breast cancer who were diagnosed and treated at Ankara Etlik City Hospital between January 2023 and February 2025. Clinicopathological and laboratory data were obtained from electronic medical records and institutional patient file archives. No missing data were present for variables included in the analyses; therefore, a complete-case approach was applied.
Inclusion criteria were: (i) histologically confirmed breast cancer; (ii) HER2 positivity defined as immunohistochemistry (IHC) score 3+ or IHC 2+ with HER2 gene amplification confirmed by in situ hybridization (ISH); (iii) availability of complete clinicopathological and laboratory data; and (iv) completion of neoadjuvant therapy, radiological assessment, and definitive surgery. Patients with HER2-negative disease, metastatic disease at diagnosis, primary tumor size <2 cm with negative lymph nodes, or a history of another malignancy were excluded.
Baseline clinicopathological variables included age, menopausal status, smoking history, Eastern Cooperative Oncology Group performance status (ECOG-PS), body mass index (BMI), tumor size, clinical T and N stage, histologic grade, estrogen receptor (ER) and progesterone receptor (PR) expression, HER2 expression level, Ki-67 proliferation index, comorbidity burden, baseline medication use, and pretreatment laboratory parameters.
Menopausal status was determined based on clinical records at diagnosis. ECOG-PS was recorded at treatment initiation. BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2). Weight loss during neoadjuvant therapy was calculated as the percentage change from baseline body weight, with ≥10% weight loss considered clinically significant.
Comorbidity burden was assessed using the modified Charlson Comorbidity Index (mCCI), calculated based on documented comorbid conditions at diagnosis.11 Baseline medication use, including metformin and lipid-lowering therapy, was recorded at the time of treatment initiation. Serum carcinoembryonic antigen (CEA) and cancer antigen 15–3 (CA15-3) levels were measured prior to the initiation of NAT.
Treatment Protocol
All patients received standard neoadjuvant chemotherapy consisting of doxorubicin plus cyclophosphamide followed by a taxane in combination with dual anti-HER2 therapy (trastuzumab and pertuzumab). Definitive surgery was performed after completion of NAT in accordance with institutional treatment protocols.
Assessment of Pathological and Radiological Response
Radiological response was assessed using PET/CT in accordance with the PET Response Criteria in Solid Tumors (PERCIST).12,13 Target lesions were defined based on the highest standardized uptake value normalized to lean body mass (SULpeak) of the most metabolically active lesion. Radiological complete response (CR) was defined as complete resolution of ^18F-fluorodeoxyglucose (^18F-FDG) uptake to background levels, with no residual metabolically active disease detected on PET/CT. Partial response was defined as a significant reduction in metabolic activity of target lesions according to PERCIST criteria. Patients achieving complete or partial metabolic response (CR or PR) were classified as radiological responders, whereas those with stable or progressive metabolic disease (SD or PD) were classified as non-responders. Pathological complete response (pCR) was defined as the absence of invasive tumor cells in both the surgically resected breast tissue and axillary lymph nodes at definitive surgery.
Inflammatory and Nutritional Biomarkers
Inflammatory and nutritional indices were calculated using routine pretreatment laboratory parameters. The LMR was defined as the ratio of absolute lymphocyte count to monocyte count. The SII was calculated as (platelet count × neutrophil count) / lymphocyte count.9,14 The CAR was calculated as serum C-reactive protein (CRP, mg/L) divided by serum albumin (g/L).
Biomarkers were primarily analyzed as continuous variables in regression analyses. In addition, receiver operating characteristic (ROC) curve analysis was performed to determine optimal cutoff values using the Youden index, and biomarkers were subsequently dichotomized for evaluation of diagnostic performance metrics, including sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy.
Statistical Analysis
All statistical analyses were performed using SPSS software, version 25.0 (IBM Corp., Armonk, NY, USA) and R software, version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were summarized as medians with interquartile ranges (IQR), and categorical variables as frequencies and percentages. The Shapiro–Wilk test was used to assess the normality of continuous variables. Group comparisons were performed using the Mann–Whitney U-test for non-normally distributed continuous variables and the Pearson chi-square test for categorical variables, as appropriate.
Univariable logistic regression analyses were conducted to identify clinicopathological and laboratory variables associated with pathological complete response and radiological response. Variables with a p-value <0.10 in univariable analyses were entered into multivariable logistic regression models. Multicollinearity was assessed using variance inflation factor (VIF) and tolerance values, with VIF ≥5 or tolerance ≤0.20 indicating collinearity. Model calibration was evaluated using the Hosmer–Lemeshow goodness-of-fit test, and model discrimination was assessed using Nagelkerke R2.
ROC curve analysis was performed to evaluate the predictive performance of inflammatory and nutritional biomarkers. Area under the curves (AUC) with 95% confidence intervals (CIs) were calculated, and optimal cutoff values were determined using the Youden index. Based on these cutoff values, biomarkers were dichotomized, and diagnostic performance metrics, including sensitivity, specificity, PPV, NPV, and overall accuracy, were calculated. A two-sided p-value <0.05 was considered statistically significant.
Exploratory Random Forest (RF) Analysis
In addition to conventional statistical analyses, exploratory RF analyses were conducted to support and contextualize biomarker-based findings. RF classifiers were implemented using the “randomForest” package in R. For each outcome (pCR and radiological response), classification models were constructed using all candidate clinicopathological and laboratory variables.
Hyperparameters were selected based on empirical optimization, with the number of trees (ntree) set to 500 to ensure model stability, and the number of variables randomly sampled at each split (mtry) determined using the square root of the number of predictors. No extensive hyperparameter tuning was performed, as analyses were predefined as exploratory.
Model performance was internally evaluated using stratified train–test splits (70% training and 30% testing). Discriminative ability was assessed using the area under the receiver operating characteristic curve (AUC), along with complementary classification metrics derived from confusion matrices, including accuracy, sensitivity, and specificity.
Feature importance was assessed using both permutation importance and mean decrease in impurity (Gini index) methods to evaluate the relative contribution of individual variables to model predictions.
Given the retrospective design and moderate sample size, RF analyses were considered exploratory and interpreted cautiously. The very high discriminative performance observed in the RF model for pCR (AUC approaching 1.0) may reflect potential overfitting, and therefore these results should be interpreted with caution. These analyses were performed to complement conventional regression-based inference rather than to establish standalone predictive models.
RF models were not used for formal variable selection but rather to complement conventional regression analyses and to provide additional insight into variable importance and potential non-linear relationships.
Ethics Approval
The study was approved by the Ethics Committee of Ankara Etlik City Hospital (Approval No: 2025–565) and conducted in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective study design. All data were anonymized prior to analysis.
Results
Patient Characteristics, Treatment Response, and Survival Outcomes
A total of 196 patients with HER2-positive BC were initially assessed for eligibility between January 2023 and February 2025. After applying the predefined inclusion and exclusion criteria, 136 patients met the eligibility criteria and were included in the final analysis (Figure 1).
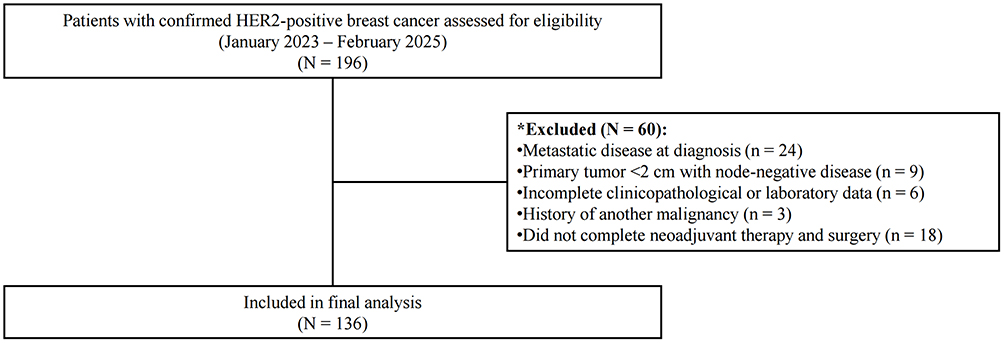 |
Figure 1 Study flow diagram. HER2 positivity was defined according to contemporary ASCO/CAP guidelines using immunohistochemistry and/or in situ hybridization. Exclusion criteria were applied sequentially; patients may have met more than one exclusion criterion. Note: * Reasons for exclusion from the study. |
The median age was 49.0 years (IQR, 42.0–62.5), and all patients were female. At diagnosis, 87 patients (64.0%) had clinically node-positive disease, and 115 patients (84.6%) had tumors larger than 2 cm. ER expression ≥10% was observed in 81 patients (59.6%), while 75 patients (55.1%) were PR–negative. A high proliferative index (Ki-67 ≥30%) was present in 90 patients (66.2%). pCR was achieved in 72 patients (52.9%). Based on PET/CT assessment, 115 patients (84.6%) were classified as radiological responders, including 74 patients (54.4%) with CR and 41 patients (30.1%) with PR. SD and PD were observed in 20 patients (14.7%) and 1 patient (0.7%), respectively. Baseline clinicopathological and laboratory characteristics stratified by pCR and radiological response are summarized in Table 1.
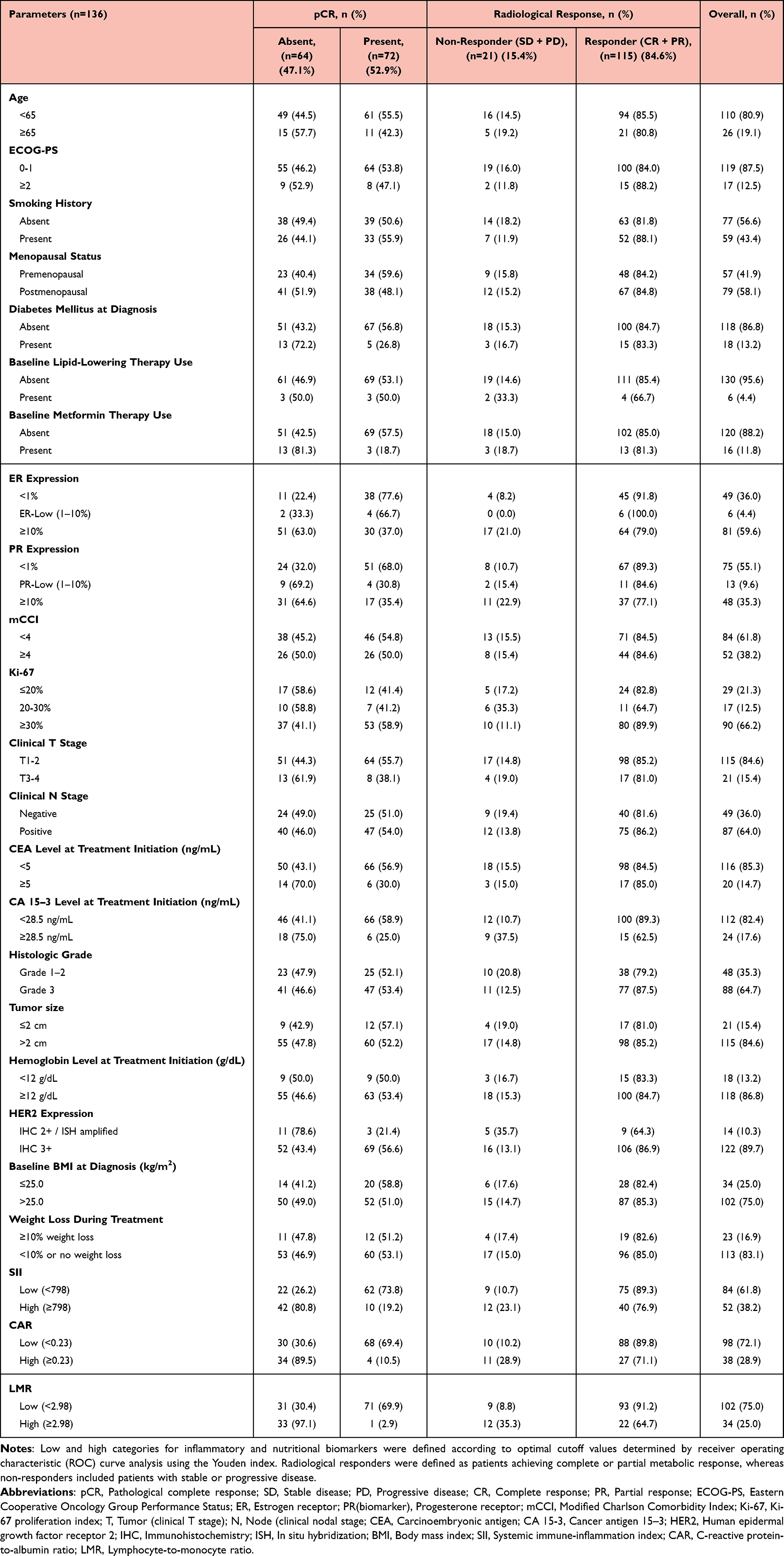 |
Table 1 Clinicopathological and Laboratory Characteristics Stratified by Pathological Complete Response (pCR) and Radiological Response in Patients with HER2-Positive Breast Cancer Treated with Neoadjuvant Dual Anti-HER2 Therapy |
With a median follow-up of 18.6 months (IQR, 12.4–26.8 months), 14 patients (10.3%) experienced an event-free survival (EFS) event and 4 patients (2.9%) died during the study period. Due to the limited number of events, the median EFS and overall survival (OS) were not reached. The estimated 12-month EFS rate was 90.4% (95% CI, 84.1–96.7), and the 24-month EFS rate was 82.1% (95% CI, 72.4–91.8). The estimated 12-month OS rate was 98.5% (95% CI, 96.0–100.0), while the 24-month OS rate was 95.8% (95% CI, 90.9–100.0). Survival analyses were considered exploratory given the relatively short follow-up duration and the low number of observed events.
Association Between Radiological Response and Pathological Complete Response
Among the 74 patients classified as having a radiological response, pCR was achieved in 72 patients (97.3%), while pCR was not achieved in 2 patients. All patients with radiological complete response (n=72) achieved pCR, whereas none of the patients with PR, SD, or PD achieved pCR. Radiological response demonstrated excellent discrimination for pCR, with an AUC of 0.986 (95% CI, 0.962–1.000; p<0.001).
Diagnostic Performance of Inflammatory and Nutritional Biomarkers
ROC analyses were performed to evaluate the discriminative ability of inflammatory and nutritional biomarkers for predicting pCR and radiological response. For prediction of pCR, SII demonstrated significant discriminative performance (AUC 0.737, 95% CI 0.646–0.827; p=0.002), followed by CAR (AUC 0.722, 95% CI 0.635–0.810; p=0.001), while LMR showed the highest discriminative ability among the evaluated biomarkers (AUC 0.793, 95% CI 0.715–0.871; p=0.003) (Supplementary Figure 1A–C).
In analyses evaluating radiological response, SII (AUC 0.713, 95% CI 0.607–0.818; p=0.013), CAR (AUC 0.721, 95% CI 0.626–0.817; p<0.001), and LMR (AUC 0.785, 95% CI 0.705–0.866; p<0.001) all demonstrated significant predictive performance (Supplementary Figure 1D–F). Optimal cutoff values for each biomarker were determined using the Youden index, with detailed diagnostic performance metrics summarized in Supplementary Table 1.
Univariable and Multivariable Logistic Regression Analysis
Univariable logistic regression analyses were performed for initial variable screening, and the results are presented in Supplementary Table 2. Variables meeting the predefined criteria were subsequently included in multivariable logistic regression models.
In the multivariable analysis for pCR, LMR ≥2.98 was independently associated with higher odds of achieving pCR (OR: 6.12, 95% CI: 1.12–13.10; p =0.004). In contrast, CAR ≥0.23 (OR: 0.20, 95% CI: 0.03–0.86; p <0.001) and SII ≥798 (OR: 0.16, 95% CI: 0.04–0.67; p =0.012) were independently associated with lower odds of pCR. In addition, PR expression <1% was significantly associated with pCR (OR: 1.81, 95% CI: 1.29–2.54; p =0.001) (Figure 2A).
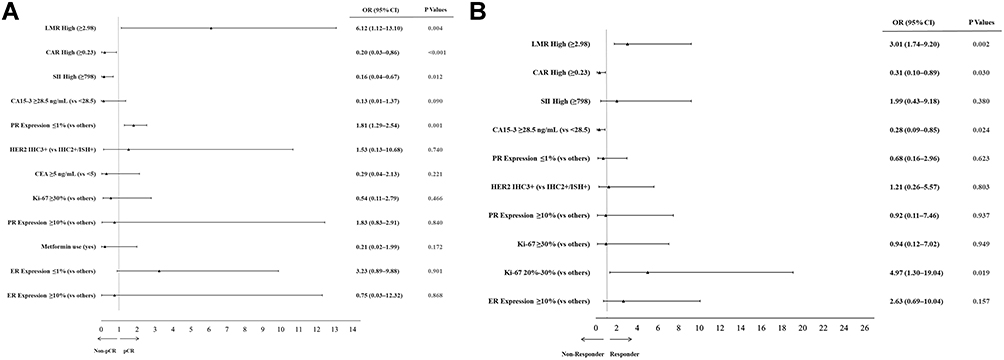 |
Figure 2 Forest plots of multivariable logistic regression analyses for treatment response. Forest plots showing independent predictors of (A) pathological complete response (pCR) and (B) radiological response in patients with HER2-positive breast cancer treated with neoadjuvant dual anti-HER2 therapy. Odds ratios (ORs) with 95% confidence intervals (CIs) are shown. Multicollinearity was assessed using variance inflation factor (VIF); diabetes mellitus was excluded from the pCR model due to collinearity with metformin use, and ER <1% was excluded from the radiological response model due to collinearity with ER ≥10%. Model calibration was evaluated using the Hosmer–Lemeshow test, and overall model significance was confirmed by the Omnibus test. Abbreviations: CAR, C-reactive protein–to–albumin ratio; CA 15–3, cancer antigen 15–3; CI, confidence interval; CEA, carcinoembryonic antigen; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; IHC, immunohistochemistry; ISH, in situ hybridization; Ki-67, Ki-67 proliferation index; LMR, lymphocyte-to-monocyte ratio; OR, odds ratio; pCR, pathological complete response; PR, progesterone receptor; SII, systemic immune-inflammation index. |
For radiological response, multivariable logistic regression analysis demonstrated that LMR ≥2.98 was independently associated with radiological response (OR: 3.01, 95% CI: 1.74–9.20; p =0.002). CAR ≥0.23 (OR: 0.31, 95% CI: 0.10–0.89; p =0.030) and baseline CA 15–3 levels ≥28.5 ng/mL (OR: 0.28, 95% CI: 0.09–0.85; p =0.024) were independently associated with reduced odds of radiological response. Furthermore, a Ki-67 proliferation index of 20–30% was independently associated with radiological response (OR: 4.97, 95% CI: 1.30–19.04; p =0.019) (Figure 2B).
Exploratory Random Forest (RF) Feature Importance (FI) Analysis
For prediction of pCR, the RF model demonstrated high discriminative performance, achieving an AUC of 0.995 (95% CI, 0.981–1.000) (Supplementary Figure 2A). For radiological response, the model demonstrated discriminative performance with an AUC of 0.791 (95% CI, 0.599–0.984) (Supplementary Figure 2B). Detailed performance metrics, including accuracy, sensitivity, specificity, predictive values, and agreement statistics, are summarized in Supplementary Table 3.
FI was evaluated using permutation importance and mean decrease in impurity (Gini index) to explore the relative contribution of variables to treatment response. For prediction of pCR, inflammatory and immune-nutritional biomarkers, particularly LMR, SII, and CAR, ranked among the most influential features across both importance metrics, followed by hormone receptor status and tumor size (Supplementary Figure 3A and B). For radiological response, LMR and pretreatment hemoglobin levels ranked among the most prominent features in both permutation- and Gini-based analyses, with additional contributions from HER2 expression, CAR, and BMI depending on the importance metric applied (Supplementary Figure 4A and B).
Overall ranking patterns were concordant between permutation and Gini importance methods. All RF analyses were considered exploratory and were performed to contextualize and complement the results of conventional regression models rather than to establish standalone predictive tools.
Discussion
In this retrospective cohort of patients with HER2-positive BC treated with NAT, we found that baseline inflammatory and immune-nutritional biomarkers were significantly associated with both pCR and radiological response. Among the evaluated markers, LMR, SII, and CAR consistently emerged as the most informative predictors across complementary analytical approaches, including multivariable regression and exploratory RF analyses. These biomarkers retained independent associations with treatment response after adjustment for established clinicopathological factors, whereas several conventional parameters demonstrated limited predictive value. In addition, selected tumor- and disease-related variables, including PR status, Ki-67 proliferation index, and baseline CA15-3 levels, showed outcome-specific independent associations with pCR or radiological response, reflecting the multifactorial nature of treatment response. In parallel, radiological response showed excellent discrimination for pCR, underscoring the clinical relevance of imaging-based assessment. Collectively, these findings suggest that host-related inflammatory and immune-nutritional status may contribute meaningfully to neoadjuvant treatment response in HER2-positive BC.
The associations observed between inflammatory and immune-nutritional biomarkers and treatment response in this study are biologically plausible and align with current concepts regarding host–tumor interactions in BC.7,8,15 A higher LMR is thought to reflect a preserved antitumor immune response, whereas elevated monocyte levels are associated with immunosuppressive tumor-associated macrophage activity and tumor progression.16,17 Similarly, SII, integrating neutrophil- and platelet-driven inflammatory burden, may capture protumorigenic inflammatory signaling that adversely affects treatment efficacy, while CAR represents a composite marker of systemic inflammation and nutritional reserve.9,10,18–20 Although previous studies have reported associations between these biomarkers and prognosis or neoadjuvant treatment response in heterogeneous BC populations,9,17,21,22 our findings extend this evidence by demonstrating their independent and consistent predictive value for both pCR and radiological response in a contemporary, homogeneous cohort of patients with HER2-positive BC treated with dual anti-HER2 NAT. These results support the notion that sensitivity to neoadjuvant therapy is influenced not only by tumor-centered pathological features but also by host-related inflammatory and immune-nutritional status. Notably, the concordant ranking of LMR, SII, and CAR across both conventional regression models and exploratory RF feature importance analyses further supports the robustness of these associations, while reinforcing their role as complementary, rather than standalone, predictive markers.
Several conventional clinicopathological variables traditionally associated with NAT response, including clinical T and N stage, histologic grade, baseline BMI, comorbidity burden, and performance status, did not retain independent significance in multivariable analyses. This observation is consistent with emerging evidence suggesting that, in the era of highly effective dual anti-HER2 NAT, the predictive value of classical tumor burden–related parameters may be attenuated.3,6,23 The high rates of pathological and radiological response observed across clinical subgroups in our cohort likely reduced the discriminative capacity of these traditional factors. Similarly, while proliferation markers such as Ki-67 and tumor markers such as CA 15–3 demonstrated associations with radiological response, their predictive value for pCR was less consistent. This divergence may reflect fundamental differences between metabolic imaging–based response and histopathological tumor eradication, with radiological response being more sensitive to early changes in tumor activity rather than complete cellular clearance.12,13 In contrast, host-related inflammatory and immune-nutritional biomarkers appeared to capture systemic biological processes that influence treatment sensitivity across both response domains. Importantly, the lack of independent significance for several conventional variables should not be interpreted as evidence of their clinical irrelevance but rather as an indication that host-related systemic factors may exert a dominant influence on neoadjuvant response once potent HER2-targeted therapy is administered. This shift underscores the importance of complementing tumor-centered assessment with biologically informed host-related markers when evaluating neoadjuvant response in uniformly treated HER2-positive populations.
From a clinical and translational perspective, our findings align with a growing body of evidence emphasizing the importance of host-related factors in modulating treatment response beyond tumor-intrinsic characteristics. Previous studies have suggested that systemic inflammation, nutritional reserve, and immune competence influence sensitivity to anticancer therapies and long-term outcomes in BC and other solid tumors.7,15,16 In HER2-positive disease specifically, recent reports indicate that highly effective dual anti-HER2 regimens may diminish the relative prognostic weight of traditional tumor burden–related variables, shifting attention toward biological host–tumor interactions.3,23 Within this context, our results suggest that routinely available inflammatory and immune-nutritional biomarkers may serve as pragmatic adjuncts to standard clinicopathological assessment, particularly in homogeneous treatment settings where response rates are uniformly high. Importantly, the concordance between radiological response and pCR observed in our cohort supports prior evidence that metabolic imaging captures early treatment sensitivity,12,13,24 while systemic biomarkers may provide complementary information reflecting the host’s capacity to sustain an effective therapeutic response. Future studies should evaluate whether integrating these biomarkers with imaging-based assessment can refine risk stratification, guide treatment adaptation, or inform surveillance strategies in HER2-positive BC.
Strengths and Limitations
This study has several notable strengths. First, it focuses on a contemporary and clinically homogeneous cohort of patients with HER2-positive BC treated uniformly with dual anti-HER2 NAT, thereby minimizing treatment-related heterogeneity. Second, both pCR and radiological response were evaluated using standardized and clinically relevant criteria, allowing assessment of treatment efficacy across complementary response domains. Third, inflammatory and immune-nutritional biomarkers were derived from routine, low-cost laboratory parameters that are readily available in daily clinical practice, enhancing the translational relevance of the findings. In addition, the consistency of results across multiple analytical frameworks, including ROC analysis, multivariable logistic regression, and exploratory RF–based approaches, supports the robustness of the observed associations. Finally, the concordance observed between rCR and pCR further reinforces the internal validity of the response assessment strategy.
Several limitations should also be acknowledged. The retrospective, single-center design introduces the potential for selection bias and limits the generalizability of the findings. Although the cohort was treated with a uniform neoadjuvant regimen, the sample size was relatively modest, and the number of survival events was low, precluding definitive conclusions regarding long-term outcomes. Inflammatory and immune-nutritional biomarkers were assessed at a single pretreatment time point, and dynamic changes during therapy could not be evaluated. In addition, detailed molecular or genomic tumor characteristics beyond routine hormone receptor and HER2 status were not available and may have provided further biological insight. While exploratory RF analyses were used to contextualize and support regression-based findings, these machine learning results should be interpreted cautiously and not as standalone predictive models. Finally, external validation in independent, multicenter cohorts is required before these biomarkers can be integrated into clinical decision-making.
Conclusion
In conclusion, this study demonstrates that baseline inflammatory and immune-nutritional biomarkers, particularly LMR, SII, and CAR, are independently associated with both pCR and radiological response in patients with HER2-positive BC treated with neoadjuvant dual anti-HER2 therapy. These routinely available biomarkers appear to capture host-related biological processes that may influence treatment sensitivity beyond conventional clinicopathological parameters. The concordance observed between radiological response and pCR further supports the clinical relevance of imaging-based assessment in this setting. Although the RF analyses were exploratory, their concordance with regression-based findings reinforces the consistency of the observed associations. Future prospective, multicenter studies are warranted to validate these results and to determine whether integrating systemic inflammatory and immune-nutritional biomarkers into clinical workflows may improve risk stratification, treatment-response assessment, closer monitoring, and individualized neoadjuvant treatment planning in HER2-positive BC.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Clinical Research Ethics Committee of Ankara Etlik City Hospital (Decision No: AEŞH-BADEK-2025-565, dated November 04, 2025) and conducted in accordance with the Declaration of Helsinki.
Consent to Participate
Due to the retrospective study design, the requirement for informed consent was waived by the responsible ethics committee. All patient data were fully anonymized prior to analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was received for this work.
Disclosure
The authors declare no conflicts of interest.
References
1. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10–12. doi:10.3322/caac.21871
2. Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics. CA Cancer J Clin. 2022;72(6):524–541. doi:10.3322/caac.21754
3. Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, Phase 2 trial. Lancet Oncol. 2012;13(1):25–32. doi:10.1016/S1470-2045(11)70336-9
4. Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized Phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9):2278–2284. doi:10.1093/annonc/mdt182
5. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
6. van Ramshorst MS, van der Voort A, van Werkhoven ED, et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive breast cancer (TRAIN-2): a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2018;19(12):1630–1640. doi:10.1016/S1470-2045(18)30570-9
7. Greten FR, Grivennikov SI. Inflammation and cancer: triggers, mechanisms, and consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
8. Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. doi:10.1016/j.cell.2010.01.025
9. Chen L, Kong X, Wang Z, Wang X, Fang Y, Wang J. Pre-treatment systemic immune-inflammation index is a useful prognostic indicator in patients with breast cancer undergoing neoadjuvant chemotherapy. J Cell Mol Med. 2020;24(5):2993–3021. doi:10.1111/jcmm.14934
10. Zhou L, Ma S, Balde AI, Han S, Cai Z, Li Z. A retrospective propensity score matched study of the preoperative C-reactive protein to albumin ratio and prognosis in patients with resectable non-metastatic breast cancer. Med Sci Monit. 2019;25:4342–4352. doi:10.12659/MSM.913684
11. Uyar GC, Kılıç MK. Evaluation of the effects of thyroid functions on frailty in geriatric patients using the Edmonton, SOF and FRAIL scales. BMC Geriatr. 2024;24(1):1051. doi:10.1186/s12877-024-05643-5
12. Wahl RL, Jacene H, Kasamon Y, Lodge MA. From RECIST to PERCIST: evolving Considerations for PET response criteria in solid tumors. J Nucl Med. 2009;50(Suppl 1):122s–50s. doi:10.2967/jnumed.108.057307
13. Min SJ, Jang HJ, Kim JH. Comparison of the RECIST and PERCIST criteria in solid tumors: a pooled analysis and review. Oncotarget. 2016;7(19):27848–27854. doi:10.18632/oncotarget.8425
14. Uyar GC, Başaran BN, Başkurt K, et al. Predicting pathologic response in locally advanced rectal cancer using inflammatory, nutritional, and sarcopenia-based markers: a regression and AI-based analysis (CINR-AI study). Clin Colorectal Cancer. 2025;25:51–67.e7. doi:10.1016/j.clcc.2025.10.002
15. Ruggieri L, Moretti A, Berardi R, et al. Host-related factors in the interplay among inflammation, immunity and dormancy in breast cancer recurrence and prognosis: an overview for clinicians. Int J Mol Sci. 2023;24(5). doi:10.3390/ijms24054974
16. Balkwill FR, Capasso M, Hagemann T. The tumor microenvironment at a glance. J Cell Sci. 2012;125(Pt 23):5591–5596. doi:10.1242/jcs.116392
17. Ma Y, Zhang J, Chen X. Lymphocyte-to-monocyte ratio is associated with the poor prognosis of breast cancer patients receiving neoadjuvant chemotherapy. Cancer Manag Res. 2021;13:1571–1580. doi:10.2147/CMAR.S292048
18. Wei XL, Wang FH, Zhang DS, et al. A novel inflammation-based prognostic score in esophageal squamous cell carcinoma: the C-reactive protein/albumin ratio. BMC Cancer. 2015;15:350. doi:10.1186/s12885-015-1379-6
19. Hutajulu SH, Astari YK, Ucche M, et al. Prognostic significance of C-reactive protein (CRP) and albumin-based biomarker in patients with breast cancer receiving chemotherapy. PeerJ. 2025;13:e19319. doi:10.7717/peerj.19319
20. Asegaonkar SB, Asegaonkar BN, Takalkar UV, Advani S, Thorat AP. C-reactive protein and breast cancer: new insights from old molecule. Int J Breast Cancer. 2015;2015:145647. doi:10.1155/2015/145647
21. Sun Y, Guan Y, Yu H, et al. Predictive model using systemic inflammation markers to assess neoadjuvant chemotherapy efficacy in breast cancer. Front Oncol. 2025;15:1552802. doi:10.3389/fonc.2025.1552802
22. Sun Y, Li W, Li AJ, Su H, Yue J, Yu J. Increased systemic immune-inflammation index independently predicts poor survival for hormone receptor-negative, HER2-positive breast cancer patients. Cancer Manag Res. 2019;11:3153–3162. doi:10.2147/CMAR.S190335
23. Fanizzi A, Latorre A, Bavaro DA, et al. Prognostic power assessment of clinical parameters to predict neoadjuvant response therapy in HER2-positive breast cancer patients: a machine learning approach. Cancer Med. 2023;12(22):20663–20669. doi:10.1002/cam4.6512
24. Kim HD, Kim BJ, Kim HS, Kim JH. Comparison of the morphologic criteria (RECIST) and metabolic criteria (EORTC and PERCIST) in tumor response assessments: a pooled analysis. Korean J Intern Med. 2019;34(3):608–617. doi:10.3904/kjim.2017.063
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Choice of Neoadjuvant Chemotherapy for HER2-Negative Breast Cancer: Clinical Insights
Lucas MW, Kelly CM
Cancer Management and Research 2022, 14:2493-2506
Published Date: 17 August 2022
Advances in Antibody-Drug Conjugates in the Treatment of HER2-Positive Breast Cancer
Yu Y, Wang J, Liao D, Zhang D, Li X, Jia Y, Kong F
Breast Cancer: Targets and Therapy 2022, 14:417-432
Published Date: 9 December 2022
Predictive Value of Pretreatment Neutrophil to Albumin Ratio in Response to Neoadjuvant Chemotherapy of Breast Cancer
Deng YX, Zhao YJ, Nong QH, Qiu HM, Guo QL, Hu H
Breast Cancer: Targets and Therapy 2024, 16:393-402
Published Date: 23 July 2024
Efficacy and Safety of Neoadjuvant Stereotactic Body Radiotherapy (SBRT) Combined with Chemoimmunotherapy in Locally Advanced Breast Cancer: A Single-Center, Retrospective Pilot Study
Zhai M, Bi J, Ke Z, Hu M, Pi G, Li Y, He H, Li Y, Zheng H, Wu X, Verma V, Shao J, Han G
Breast Cancer: Targets and Therapy 2026, 18:577469
Published Date: 7 March 2026
A Structured Classification of Pyrotinib-Containing Neoadjuvant Regimens for HER2-Positive Breast Cancer: Efficacy, Safety, and Regimen Selection
Liu J, Peng X, Yang Y, Huang X, Du Y, Liu K
Breast Cancer: Targets and Therapy 2026, 18:600575
Published Date: 20 May 2026