Back to Journals » Cancer Management and Research » Volume 14
Optimal Choice of Neoadjuvant Chemotherapy for HER2-Negative Breast Cancer: Clinical Insights
Received 15 May 2022
Accepted for publication 5 August 2022
Published 17 August 2022 Volume 2022:14 Pages 2493—2506
DOI https://doi.org/10.2147/CMAR.S341466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Mairi W Lucas,1 Catherine M Kelly2
1Royal College of Surgeons in Ireland, St Stephen’s Green, Dublin, Ireland; 2Mater Private Hospital, Dublin, Ireland
Correspondence: Catherine M Kelly, Consultant Medical Oncologist, UCD Clinical Professor, Mater Private Hospital, Eccles Street, Dublin, Ireland, Email [email protected]
Abstract: The neoadjuvant setting provides immense opportunities for translational research and drug development. The acceptance of pathological complete response (pCR) as a surrogate endpoint for clinical benefit has led to the widespread use of neoadjuvant treatment. Optimal neoadjuvant therapies are determined based on their ability to achieve the highest rates of pCR. Predicted rates of pCR for triple negative breast cancer (TNBC) treated with sequential taxane/anthracycline regimens range from 35% to 48%. With the addition of a platinum agent pCR rates of 55% are predicted. Further increases have been observed with the addition of immune checkpoint inhibitors to this standard chemotherapy backbone. In the pivotal KEYNOTE-522 clinical trial pCR rates of 65% and 69% were reported for chemotherapy plus pembrolizumab in the overall and PD-L1-positive subgroup respectively. The role of the neoadjuvant chemotherapy is less clear in hormone receptor (HR)-positive, human epidermal growth factor receptor-2 (HER2)-negative breast cancer. In general, HR–positive cancers have the least chance of achieving a pCR after neoadjuvant chemotherapy, especially if they are low-grade. If neoadjuvant chemotherapy is given for high-risk HR-positive, HER2-negative breast cancer, standard adjuvant anthracycline/taxane regimens are appropriate. Optimum endocrine therapy is the standard-of-care in the adjuvant setting regardless of pCR. There are several genomic signatures available to guide decisions regarding adjuvant chemotherapy use however these assays are not routinely used in the neoadjuvant setting. For high-risk patients meeting the criteria for the monarchE trial adjuvant abemaciclib in addition to endocrine therapy is associated with an improvement in disease free survival (DFS) at 3 years. Based on the OlympiA trial patients with germline BRCA mutations should be considered for adjuvant olaparib therapy. In this article we review neoadjuvant clinical trials that guide optimum treatment options for TNBC and HR-positive, HER2-negative breast cancer.
Keywords: neoadjuvant, pathological complete response, platinum agents, immune checkpoint inhibitors, PARP inhibitors, endocrine therapy
Introduction: The Clinical Rationale for Using Neoadjuvant Chemotherapy
Historically, the goal of preoperative or neoadjuvant chemotherapy was to downstage inoperable cancers to allow surgery. As this setting evolved, the focus became downstaging non-conservable cancers to allow breast conservation. Over 30 years ago the pivotal NSABP B-18 trial randomized 1523 patients with operable breast cancer to preoperative versus postoperative doxorubicin and cyclophosphamide (AC) chemotherapy. The study reported more breast conserving surgeries in the preoperative group compared to the post-operative chemotherapy group. At 9-years follow up there was no disease free survival (DFS) or overall survival (OS) difference whether the same chemotherapy regimen was given pre or post operatively. This was an important milestone as it allowed the exploration of the research opportunities offered by the neoadjuvant setting.1,2 Adding weight to this evidence the NSABP B-27 trial randomized 2411 patients with operable breast cancer to receive preoperative or postoperative chemotherapy. At 6.5 years follow-up again there was no difference in DFS or OS when the same chemotherapy was given pre- or postoperatively.3
Providing evidence that there was no loss of efficacy by administering chemotherapy before surgery enabled investigators to exploit the huge translational research opportunities of the neoadjuvant setting. This in turn paved the way for the contemporary practice-changing clinical trials that are improving breast cancer outcomes for the present generation of patients with breast cancer. These studies and others provided important early insights into the long-term prognostic implications of pathological complete response (pCR) and the importance of biological subtype in predicting chemotherapy-sensitivity and likelihood of achieving a pCR.1–6
Over the last two decades clinical trials conducted in the neoadjuvant setting have provided unprecedented translational research opportunities. In 2014 the US Food and Drug Administration (FDA) accepted pCR as a surrogate endpoint for clinical benefit for neoadjuvant therapies and acceptable for accelerated drug approval.7 This has led to the widespread use of the neoadjuvant setting as a means to rapidly incorporate novel therapeutic agents into smaller often biomarker-driven studies. This approach is epitomised by the I-SPY platform of studies. The adaptive, multi-agent design of I-SPY allows for several drugs (or combinations) to be evaluated in parallel. Drugs or regimens that show a high Bayesian predictive probability of being more effective than standard therapy graduate from the trial with their corresponding biomarker signature(s). New drugs enter when those that have undergone testing complete their evaluation.8 For example, by demonstrating a doubling in the pCR rate with the addition of pembrolizumab to standard chemotherapy the ISPY-2 trial accurately predicted a high likelihood of success in Phase III trials with this agent in triple negative breast cancer (TNBC).9
As neoadjuvant therapy has become the standard-of-care approach for TNBC and the HER2-positive breast cancer subtype so has the emergence of clinical trials designed exclusively for patients with subtype-specific residual disease post neoadjuvant therapy. Adjuvant therapy informed by success or failure to achieve a pCR in patients with HER2-positive and TNBC is now the standard-of-care based on the Katherine (NCT01772472) and CREATE-X (UMIN000000843) randomized trials respectively.10,11
The Residual Cancer Burden (RCB) Score as a Standardised Measure of Response to Neoadjuvant Therapy
The burden of residual disease post neoadjuvant treatment can be further stratified to provide more information regarding prognosis. The residual cancer burden score (RCB score) is a continuous variable but can be reported as 4 discrete categories, RCB-0 indicating a pCR and then RCB-I, RCB-II, RCB-III with increasing volume of disease post neoadjuvant treatment. The score incorporates measures of tumor bed area, cancer cellularity, percentage in situ disease, the number of positive lymph-nodes and the diameter of the largest metastasis.12
Relapse-free survival (RFS) is significantly different for each group with estimated 10-year relapse-free survival rates in TNBC of 86%, 81%, 55% and 23% for RCB-0, RCB-I, RCB-II and RCB-III respectively.12 The RCB is also consistent in providing prognostic information for each breast cancer subtype. A recent meta-analysis consolidated the value of the RCB score. The study included 5161 patients who received neoadjuvant therapy between 1994 and 2019 across 12 sites.13 The overall event-free survival (EFS) estimates at 5-years were 88%, 80%, 65% and 45% for RCB-0, RCB-I, RCB-II, RCB-III, respectively. The association between RCB score and prognosis was consistent across the breast cancer subtypes. The hazard ratio for an event associated with a 1-point increase in RCB was 1.55 in ER-positive/HER2-negative breast cancer, and 2.16 in ER-negative/HER2-positive subgroup. The RCB score remained prognostic after adjustment for age, grade and tumor size and nodal status. The RCB score has become a standard for reporting response to neoadjuvant treatment in clinical trials.
What is the Optimal Neoadjuvant Regimen for TNBC?
The American Society of Clinical Oncology (ASCO) guidelines advise that for patients diagnosed with TNBC that is clinically lymph node-positive and/or at least T1c neoadjuvant anthracycline- and taxane-containing regimens should be offered.14 The EBCTCG meta-analysis of long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer found that the one regimen that included both anthracycline and taxane had the highest frequency of complete response.15 Recent studies have examined if rates of pCR can be increased further by incorporating a platinum agent and/or an immune checkpoint inhibitor (ICI).
Platinum Agents as a Component of Neoadjuvant Chemotherapy for TNBC
The role of platinum agents in the neoadjuvant setting has been the subject of much debate. However, recent meta-analyses have provided robust data on the important role of these agents. Poggio et al conducted a meta-analysis that included 9 randomized controlled trials (RCTs) with a total of 2109 patients. The objective was to investigate platinum-based versus platinum-free neoadjuvant chemotherapy in TNBC. Platinum-based neoadjuvant chemotherapy significantly increased the pCR rate from 37.0% to 52.1% (odds ratio (OR) 1.96, 95% confidence interval (CI) 1.46–2.62, P < 0.001). Pathological complete response rates increased from 15% to 22% when the results were restricted to the three RCTs that used similar regimens. For weekly paclitaxel with or without carboplatin followed by anthracycline and cyclophosphamide chemotherapy, the pCR was 54.9% in the platinum-based chemotherapy group. It was 33.3% in the platinum-free chemotherapy group (OR 2.53, 95% CI 1.37–4.66, P = 0.003). Despite the notable increase in pCR associated with the addition of platinum agents this did not translate into an improvement in event free survival (EFS) or OS. However, survival data was only provided by two RCTs. Improvements in pCR with the addition of platinum agents came at the cost of increased haematological toxicity.
Although the numbers were relatively small (n = 98) this meta-analysis found that patients with BRCA-associated TNBC did not experience an increase in pCR with the addition of platinum agents. This might suggest that standard anthracycline-taxane chemotherapy incorporating cyclophosphamide is sufficient for patients with germline BRCA mutations.16
In a more recent meta-analysis published in 2022, Bian et al studied DFS and OS associated with the addition of a platinum to neoadjuvant chemotherapy. The meta-analysis included 7 RCTs, 4 were conducted in the neoadjuvant and 3 were adjuvant RCTs. A statistically significant improvement in DFS (hazard ratio (HR) = 0.70, 95% CI 0.58–0.84), and OS (HR = 0.78, 95% CI 0.61–1.00) was observed in favour of the addition of platinum. This meta-analysis reported that the survival benefits held whether the platinum was given in the neoadjuvant or adjuvant setting. In a supplementary analysis the investigators incorporated survival data from the BrighTNess neoadjuvant clinical trial. This recently published study reported improved EFS in favour of the addition of carboplatin to weekly paclitaxel followed by doxorubicin and cyclophosphamide (AC) in patients with stage II and III TNBC. Patients who achieved a pCR experienced the best EFS. At 4.5 years, neoadjuvant carboplatin and paclitaxel followed by AC improved EFS in stage II–III TNBC.17 When the results of the BrighTNess trial were incorporated into the meta-analysis, the pooled results were unchanged with a final HR for DFS of 0.68 (95% CI 0.57–0.81) and for OS of 0.76 (95% CI 0.60–0.0.96).18
Both meta-analyses provide robust evidence supporting the addition of platinum agents to standard neoadjuvant chemotherapy for patients with TNBC. Furthermore, ASCO and the European Society of Medical Oncology (ESMO) Guidelines recommend offering carboplatin as part of a neoadjuvant chemotherapy regimen while simultaneously weighing up the potential harms and benefits.14,19 Based on these data some of the recent neoadjuvant clinical trials studying the role of immunotherapy have included carboplatin as a core component of the chemotherapy backbone.20
The Role of Neoadjuvant Immunotherapy in Treatment of Early Stage TNBC
Programmed cell death ligand-1 (PD-L1) is expressed on the surface of tumors and infiltrating immune cells and other cell types. Programmed cell death protein-1 (PD-1) is expressed predominately on T cells. Programmed cell death protein-1 interacts with its ligands (PD-L1 and PD-L2). In doing this it directly inhibits apoptosis of tumor cells; promotes peripheral T effector cell exhaustion; and the conversion of T effector cells to immunosuppressive T regulatory cells.21
Immune checkpoint inhibitors (ICIs) are highly selective monoclonal antibodies that may be specific for PD-L1 e.g atezolizumab or for PD-1 e.g. pembrolizumab. Immune checkpoint inhibitors have revolutionized the treatment of many difficult to treat cancers such as lung and melanoma. Before the introduction of ICIs the OS for patients with metastatic melanoma or non-small cell lung cancer was approximately one year, now many patients are experiencing long-term remissions lasting years. As the most immunogenic subtype of breast cancer, the clinical benefit of ICIs has become a reality for patients with TNBC.
Immunotherapy in Metastatic TNBC
Results from Phase I and II clinical trials in metastatic TNBC found that ICIs had the highest activity when given in the first line setting. Clinical activity was increased with increasing PD-L1 expression and when ICIs were given in combination with chemotherapy.22 The Phase III IMpassion130 first line trial (NCT02425891) randomized 902 patients with metastatic TNBC to treatment with nab-paclitaxel with atezolizumab or placebo.23 The two primary end points were PFS in the intention-to-treat population (ITT) and PD-L1–positive subgroup. Overall survival was according to the study protocol to be tested in the ITT; if the finding was significant, then it would be tested in the PD-L1–positive subgroup.
The trial reported a modest improvement in PFS in the ITT population. The median PFS was 7.2 months with atezolizumab compared to 5.5 months with placebo (HR = 0.80; 95% CI 0.69 to 0.92; P = 0.002). Among patients with PD-L1–positive tumors, the median PFS was 7.5 months and 5.0 months, in favour of atezolizumab (HR = 0.62; 95% CI 0.49 to 0.78; P < 0.001). In the ITT population, the median OS was 21.3 months with atezolizumab and 17.6 months with placebo (HR for death, 0.84; 95% CI 0.69 to 1.02; P = 0.08). The improvement in OS in the ITT analysis did not reach statistical significance so as per protocol the OS analysis could not be tested in the PD-L1-positive group. However, this was presented and showed an almost 10-month improvement in median OS in favour of atezolizumab (25.0 months and 15.5 months) with a HR of 0.62; 95% CI 0.45 to 0.86. Accelerated approval was granted for atezolizumab in March 2019 based on these results. However, this approval was contingent upon results of the IMpassion131 trial (NCT03125902).24 Unfortunately, this trial failed to meet the primary end point of PFS superiority in the frontline treatment of patients with PD-L1 positivity (HR = 0.82; 95% CI 0.60–1.12; P = 0.20). There was no difference in survival advantage in the PD-L1–positive (HR 1.11, 95% CI 0.76–1.64) nor the intention to treat population. As a result, the indication for atezolizumab in combination with nab-paclitaxel for PD-L1-positive metastatic TNBC was withdrawn by Roche, the company responsible for the agent, following consultation with the FDA. This combination is still available in Europe.
In the KEYNOTE-355 trial patients were randomized to pembrolizumab or placebo and could receive any one of a number of chemotherapy options. These options were nab-paclitaxel, paclitaxel, gemcitabine, and carboplatin. The final OS results were presented at ESMO in 2021. In the subset of patients who were PD-L1-positive with a combined positive score (CPS) of at least 10 (38% of the trial population), the median overall survival was 23.0 months in the pembrolizumab arm compared to 16.1 months in the control arm (HR = 0.73; 95% CI 0.55–0.95; P = 0.0093). Median progression-free survival was 9.7 months vs 5.6 months, respectively (HR = 0.66; 95% CI = 0.50–0.88).25
Neoadjuvant Trials of Immune Checkpoint Inhibitors in Early Stage TNBC
Data from early phase trials in the metastatic setting provided strong rationale to study ICIs in early-stage breast cancers treated with curative intent. A recent comprehensive review provides an in-depth analysis into why the neoadjuvant rather than the adjuvant setting might be the most effective time to administer these agents.22 Treating upfront with chemotherapy and ICIs provides an opportunity for enhanced immune priming through the generation and release of neoantigens. Furthermore, due to lack of prior exposure of the tumor and microenvironment to chemotherapy there may exist a more immune-permissive tumor microenvironment that enhances adaptive immune engagement.22
Two early-phase studies reported pCR rates in the order of 60% when pembrolizumab was added to chemotherapy (Table 1).9,26 In the Phase II ISPY-2 trial pCR more than doubled from 22% to 60% in patients with TNBC.9 The Phase II GeparNUEVO study showed a more modest increase in pCR in overall study cohort however the rate of pCR approached 60% in the PD-L1-positive subgroup with the addition of neoadjuvant durvalumab to chemotherapy. However despite the overall modest increase in pCR there was an improvement in invasive-DFS, distant-DFS and OS in favour of durvalumab.27
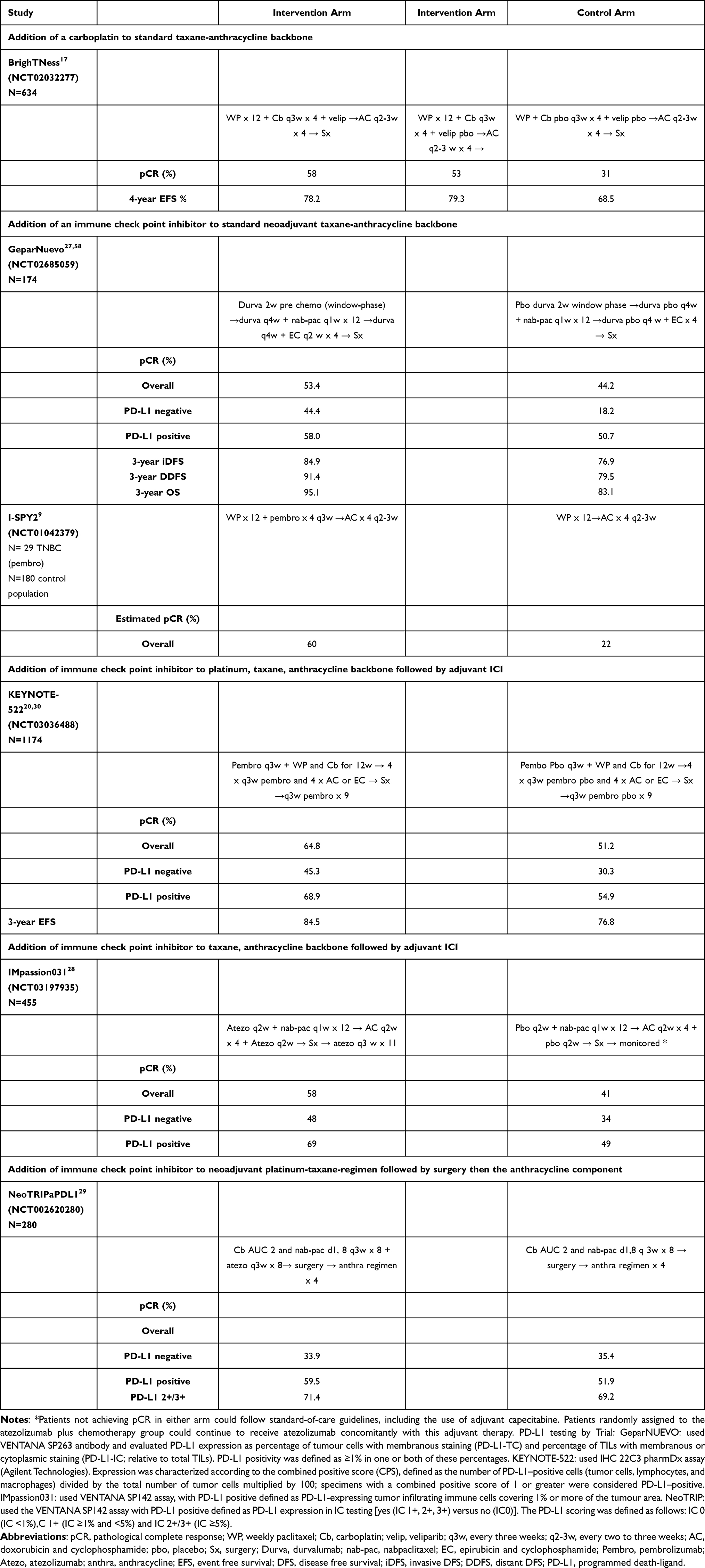 |
Table 1 Improvements in pCR with the Addition of Platinum and Immunotherapeutic Agents |
Three Phase III trials evaluating the role of ICIs in combination with neoadjuvant chemotherapy in early stage TNBC have reported (Table 1).20,28,29 The largest of these studies is the KEYNOTE-522 trial which accrued 1174 patients with stage II–III TNBC. Patients were randomized in a 2:1 fashion to four cycles of pembrolizumab at 200mg every three weeks in combination with carboplatin (AUC 5 mg/mL per minute) every three weeks or AUC 1.5 mg/mL per minute every week) and weekly paclitaxel followed by doxorubicin and cyclophosphamide or epirubicin and cyclophosphamide for 4 cycles or all of the above with placebo. Post-surgery patients received adjuvant pembrolizumab or placebo every 3 weeks for up to nine cycles.20 Primary endpoints were pCR at time of surgery and EFS in the ITT population. The first results showed an improvement in pCR of 13.6% in favour of pembrolizumab (pCR 64.8% versus 51.2%). Rates of pCR were higher again in the PD-L1-positive population 68.9% versus 54.9%. Patients with PD-L1-negative breast cancers also benefitted from pembrolizumab 45.3% versus 30.3%. This is in contrast to the metastatic setting were benefit from immunotherapy was associated with PD-L1-positivity only.23,30
The second primary endpoint of EFS was reported earlier this year and observed an EFS of 84.5% (95% CI 81.7 to 86.9) in the pembrolizumab arm compared to 76.8% (95% CI 72.2 to 80.7) in the placebo arm. The final hazard ratio for an event or death was 0.63 (95% CI 0.48 to 0.82) P < 0.001. The most frequent event was a distant recurrence. Median OS has not been reached in either arm at this time. Immune-mediated adverse events of grade 3 or higher occurred in 12.9% and 1% of the intervention and placebo arms respectively. There were two immune-mediated deaths in the pembrolizumab arm (0.3%) and none in the placebo arm. Based on these results there was an ASCO Guideline Rapid Recommendation Update endorsing the use of pembrolizumab as per KEYNOTE-522 for patients with T1cN1-2 or T2-4N0 (stage II or III), early-stage TNBC.31
In KEYNOTE-522 the EFS was higher than expected for the improvement in pCR observed. In KEYNOTE-522 this improvement has carried through to those who received pembrolizumab but did not achieve a pCR in comparison to those who also did not achieve a pCR and received placebo. This is similar to the finding from the GeparNUEVO trial were an improvement in DFS and OS was also observed despite a relatively small improvement in the rate of pCR with the addition of pembrolizumab.27 These observations suggest that pCR as a surrogate for EFS in trials that include immunotherapy may not be as robust as previously considered and that even if a pCR is not achieved a benefit may still be observed.
Leading on from this another important clinical question that has arisen from KEYNOTE-522 is, how much the adjuvant pembrolizumab portion adds to the overall benefit gained after neoadjuvant pembrolizumab? Unfortunately, KEYNOTE-522 was not designed to answer this question. The GeparNUEVO study reported an increase in pCR rates and improved long-term outcomes even though durvalumab was given only in the neoadjuvant setting. Long term outcomes from the IMpassion031 and NeoTRIP studies will provide further insights into this question.28,29
At this time if following the KEYNOTE-522 protocol adjuvant pembrolizumab should be continued independent of pCR results. The optimal treatment for patients with residual disease after neoadjuvant chemotherapy and ICI is an area of uncertainty. Adjuvant capecitabine has been shown to improve OS in patients with residual disease after neoadjuvant chemotherapy and recent data would also support the use of a PARP inhibitor for patients with germline BRCA1 or 2 (gBRCA1/2) mutations in this setting.
The IMpassion031 trial randomized patients with stage II–III TNBC to receive atezolizumab versus placebo in combination with nab-paclitaxel followed by doxorubicin and cyclophosphamide for 4 cycles (Table 1). After surgery and completion of pathological evaluation, unblinding occurred. Patients in the atezolizumab plus chemotherapy group continued to receive intravenous atezolizumab at 1200 mg every 3 weeks for 11 cycles for approximately 12 months. Management of patients for whom a pCR was not found followed standard-of-care guidelines, including the use of adjuvant capecitabine. Patients randomly assigned to the atezolizumab plus chemotherapy group could continue to receive atezolizumab concomitantly with this adjuvant therapy. In the placebo plus chemotherapy group, post-surgery patients who did not achieve a pCR were treated as per standard-of-care. Co-primary endpoints were pCR in all-randomized and PD-L1-positive (ie, patients with PD-L1-expressing tumor infiltrating immune cells covering ≥1% of tumor area) populations.
There were 455 patients enrolled of whom 333 were eligible and randomized. The pCR rate was 58% versus 41% representing a 17% increase in pCR (P = 0.0044) in favour of atezolizumab. For PD-L1-positive cancers the pCR was 69% versus 49% in favour of atezolizumab. No results relating to EFS have been presented to date.
The NeoTRIP neoadjuvant open label trial randomized 280 patients with high-risk early stage or locally advanced TNBC (Table 1). Patients were randomized to neoadjuvant carboplatin and nab-paclitaxel on days 1 and 8, with or without atezolizumab. Cycles were every 21 days eight were given in total, pre-surgery. Post-operatively patients received 4 cycles of an anthracycline regimen per investigator choice. The primary aim of the study was to compare EFS 5 years after randomization of the last patient and this has not been reported. A secondary endpoint of pCR has been reported and shows a numerical but statistically non-significant difference in between the two arms. Specifically 48.6% in the atezolizumab arm compared to 44.4% in the standard-of-care arm (p = 0.48). Multivariate analysis of pCR identified that tumors positive for PD-L1 expression were twice as likely to achieve a pCR compared to PD-L1-negative cancers (OR 2.08;95% CI 1.64–2.65 P < 0.0001). For PD-L1-positive cancers the addition of atezolizumab increased the pCR rate by 7.6%. There were equal numbers of patients discontinuing treatment in each treatment arm.
Understanding the reason behind reported differences in the rates of pCR between atezolizumab containing arms in NeoTRIP and IMpassion031 is complex. In IMpassion031 the rate of pCR increased by 17% compared to just 4.2% in NeoTRIP. These trials however are very different. The IMpassion031 trial included an anthracycline component in both neoadjuvant treatment arms whereas NeoTRIP reserved the anthracycline component for the adjuvant setting. It may be that by omitting anthracyclines their potent immunogenic effects were lost. The investigators also observed an imbalance for tumor infiltrating lymphocytes (TILs) with higher TILs in the chemotherapy-only arm. The implication from this observation is that as TILs are associated with increased likelihood of pCR then the fact TILs were higher in the control arm may have resulted in a higher-than-expected pCR in this arm. Event-free-survival results are greatly anticipated. If there is an improvement in EFS despite a non-significant increase in pCR then it points to a weakness in pCR being used as a surrogate for long term outcome in neoadjuvant immunotherapy studies. The NeoTRIP results were also presented with pCR given by level of PD-L1 expression and for those patients who received atezolizumab and were PD-L1 +2/+3 the rate of pCR achieved was 70%.
Neoadjuvant PARP-Inhibition for Germline BRCA-Mutation-Positive Breast Cancer
Litton et al from MD Anderson Cancer Center recently presented the results of a Phase II non-randomized open-label neoadjuvant trial. The trial examined the efficacy of the poly(ADP-ribose) polymerase (PARP)-inhibitor talazoparib in patients with gBRCA1/2 mutation-positive, early HER2-negative breast cancer. Patients were given talazoparib monotherapy for 24 weeks followed by surgery. Of the 48 evaluable patients all had TNBC. The primary endpoint of pCR was 45.8% and in the ITT population it was 49.2%. This early phase trial could represent an exciting non-chemotherapy option given the similarity of the rate of pCR to standard chemotherapy but larger confirmatory studies with long-term outcomes will be needed to bring this approach forward.32
Adjuvant Treatment Guided by Response to Neoadjuvant Therapy in TNBC
The CREATE-X trial was an open label, Phase III trial that examined the role of capecitabine for patients with residual disease post neoadjuvant chemotherapy.10 The trial involved 910 patients with HER2-negative breast cancer who had received neoadjuvant anthracycline/taxane or anthracycline/taxane-based chemotherapy and had residual disease at the time of surgery.
The final analysis showed that DFS was longer in the capecitabine group than in the control group (74.1% vs 67.6% of the patients were alive and free from recurrence or second cancer at 5 years; HR for recurrence, second cancer, or death, 0.70; 95% CI 0.53 to 0.92; P = 0.01). Overall survival was longer in the capecitabine group compared to the control group (89.2% vs 83.6% of the patients were alive at 5 years; HR for death, 0.59; 95% CI 0.39 to 0.90; P = 0.01). Among patients with TNBC, DFS was 69.8% in the capecitabine group compared to 56.1% in the control group (HR for recurrence, second cancer, or death, 0.58; 95% CI 0.39 to 0.87), and OS was 78.8% versus 70.3% (HR for death 0.52; 95% CI 0.30 to 0.90).
A recent meta-analysis of randomized studies on the basis of individual patient data found that the addition of capecitabine to standard adjuvant chemotherapy regimens prolongs DFS, whereas replacing a standard agent with capecitabine did not improve it.33
Adjuvant PARP-Inhibition for Germline BRCA-Mutation-Positive Breast Cancer with Residual Disease After Neoadjuvant Chemotherapy
The OlympiA study was a multicentre, randomized, double-blind-placebo controlled Phase III trial.34 The trial enrolled patients with gBRCA1/2 mutations with HER2-negative, high-risk disease post local treatment and chemotherapy either in the adjuvant or neoadjuvant setting. Patients who received neoadjuvant chemotherapy were eligible if they had TNBC and had residual disease or if they had HR-positive disease they had to have residual disease in addition to other high-risk features.
Patients were randomized to receive olaparib 300 mg twice daily versus placebo for 12 months. In the cohort that received neoadjuvant therapy the 3-year DFS in the olaparib arm was 82.5% compared with 68.0% in the placebo arm (HR 0.56 95% CI 0.41–0.75). These results are considered practice-changing and the US FDA approved the use of olaparib for the adjuvant treatment of patients with gBRCA1/2-mutated, HER2-negative high-risk early-stage breast cancer who have been treated in the (neo)adjuvant setting in March 2022.
Other Agents Being Studied as Adjuvant Treatment Post NAC
Antibody drug conjugates (ADCs) are comprised of an antibody with a chemotherapeutic agent linked to it. Once the antibody binds to its cell surface target the ADC is internalised, the linker cleaved and the chemotherapeutic agent released to kill the cell with often some associated “bystander” kill. These agents made their initial impact predominantly in HER2-positive breast cancer. The ADC, trastuzumab emtansine (T-DM1) is now the standard-of-care in patients with residual disease post-neoadjuvant trastuzumab, pertuzumab-based regimens.11 Recent ADCs such as trastuzumab deruxtecan (T-DXd) have greater potency and are more efficacious than T-DM1 in the metastatic setting.35 This agent is now being studied head-to-head with T-DM1 in the residual disease setting (DESTINY- Breast05, NCT04622319) and T-DXd is also showing promise in HER2-low cancers ie breast cancers with immunohistochemical expression of 1+ and 2+.36
Sacituzumab govitecan is an ADC. It is composed of an anti-trophoblast cell-surface antigen 2 (Trop-2) IgG1 kappa antibody linked to the active metabolite of irinotecan. Trop-2 is a transmembrane calcium signal transducer that is highly expressed in multiple tumor types, including breast cancer (>90%).37,38 This ADC was shown to improve the median PFS (5.6 versus 1.7 months with a HR for disease progression or death, 0.41; 95% CI 0.32 to 0.52; P < 0.001) compared to standard chemotherapy in relapsed or refractory metastatic TNBC. The median OS was 12.1 months (95% CI, 10.7 to 14.0) with sacituzumab govitecan and 6.7 months (95% CI 5.8 to 7.7) with chemotherapy (HR for death, 0.48; 95% CI 0.38 to 0.59; P < 0.001). This ADC is now being studied in patients with HER2-negative residual disease post neoadjuvant chemotherapy in the SASCIA trial (NCT04595565) Phase III trial.
Optimal Neoadjuvant Treatment for Hormone Receptor-Positive Breast Cancer
In general, HR-positive cancers (luminal A and B) have the least chance of a pCR after neoadjuvant chemotherapy, especially if they are low-grade. A meta-analysis of almost 12,000 patients in a dozen neoadjuvant studies reported the pCR rate for low-grade tumors was only 7%, and it was 16% for grade 3 tumors.39 Most importantly however is the finding that the prognostic implications of a pCR differs depending on the breast cancer subtype. The German Breast Group studied pCR and DFS by intrinsic subgroup and showed no impact of pCR in the luminal A group or among luminal B cancers that are HER2-positive. The achievement of pCR was predictive in the three other subsets: luminal B, HER2-negative, HER2-positive/HR-negative, and TNBC.40
As a result some guidelines recommend proceeding directly to surgery for stage I disease. Neoadjuvant therapy may be considered in stage II and III disease if the chemotherapy decisions can be made without surgical pathological data.14
The pivotal NSABP B-18 and NSABP B-27 RCTs provide the evidence that there is no loss of efficacy administering chemotherapy in the neoadjuvant versus adjuvant setting.1,3 It is the extrapolation of evidence from studies such as these which allows us to consider neoadjuvant chemotherapy as a non-inferior alternative to adjuvant therapy in HR-positive HER2-negative early-stage breast cancer for those patients with clinical indications for adjuvant therapy.14
Typically the type of chemotherapy regimen used in HR-positive HER2-negative breast cancer in the neoadjuvant setting is the same as regimens used in the adjuvant setting.14 The large Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) meta-analysis compared long-term outcomes associated with different polychemotherapy regimens for early-stage breast cancer.41 The EBCTCG meta-analysis compared over 100,000 patients from over 123 trials that compared different chemotherapy regimens (ie anthracycline vs CMF, anthracycline + taxane vs anthracycline) or compared polychemotherapy to no chemotherapy. The overall outcome showed that on average the taxane-plus-anthracycline-based regimens had a small but significantly improved outcome in comparison with an anthracycline-based control regimen, RR 0.86 (P = 0.0005).41 Unlike in TNBC, further studies have shown the addition of carboplatin results in more toxicities without significant impact in the rate of pCR or EFS for HR-positive HER2-negative breast cancer.16 Therefore the chemotherapy regimen of choice in high risk HR-positive, HER2-negative breast cancer remains anthracycline/taxane-based. Non-anthracycline-based regimens may also have a role in (neo)adjuvant therapy. Based on the joint analysis from the ABC trials, although TC had an inferior four-year invasive DFS (88.2 versus 90.7%; HR 1.23, 95% CI 1.01–1.50) compared to the anthracycline and taxane-based regimen however the anthracycline-based therapy did not meaningfully improve outcomes in lower-risk, HR-positive breast cancers.42 Similarly, the West German Study Group PlanB trial reported that six cycles of TC were non-inferior to four cycles of epirubicin and cyclophosphamide, followed by four cycles of docetaxel (EC-T).43 Treatment-related deaths were however higher in the TC arm (5 versus 1) compared to the EC-T arm.
Considerations for Neoadjuvant Chemotherapy Based on 21-Gene Assay Results
There are several breast cancer biomarker assays endorsed by ASCO to guide decisions around adjuvant chemotherapy and endocrine therapy in HR-positive, HER2-negative breast cancer.44 Two large randomized controlled trials have established the role of Oncotype DX for predicting benefit from adjuvant chemotherapy in women with HR-positive, HER2-negative, lymph node-negative and -positive breast cancer.45,46 Specifically recent results from the RxPONDER trial show that postmenopausal women with a recurrence score (RS) of ≤25 do not benefit from adjuvant chemotherapy.45 This is important as, unlike TNBC and HER2-positive breast cancer where neoadjuvant chemotherapy is indicated for palpable lesions >2 cm with or without positive lymph nodes, based on the results of RxPONDER, postmenopausal women with up to 3 positive lymph nodes do not derive benefit from adjuvant chemotherapy. Therefore, upfront surgery may be appropriate for most postmenopausal women with up to 3 positive lymph nodes as if the RS in ≤25 then adjuvant chemotherapy will not be required. The role of prognostic signatures in guiding neoadjuvant therapy remains uncertain and has not yet been adopted in clinical practice. Retrospective studies have reported an association between higher Oncotype DX RS and improved pCR rate compared to having a lower RS.47 A lower RS may indicate that if a neoadjuvant approach is required endocrine therapy may be a better approach.48
Most of the currently established prognostic signature scores have shown a similar ability to predict response to chemotherapy in the neoadjuvant setting with high scores, likely reflective of more proliferative tumors.49 Further studies are underway to determine the clinical utility of multi-gene prognostic signature scores in the neoadjuvant setting however currently they are not used to guide neoadjuvant therapy.14,50
Estrogen receptor (ER)-positive breast cancers are defined as having >1% staining for ER by IHC, however a small subgroup of patients have 1–9% ER-staining and are considered “ER low positive” and have a clinical phenotype similar to TNBC.51,52
Role of Immune Checkpoint Inhibitors in the Neoadjuvant Treatment of HR-Positive, HER2-Negative Breast Cancer
Compared to TNBC, HR-positive, HER2-negative breast cancer is less immunogenic, has fewer TILs and a lower tumor mutational burden.22 However there are some promising data indicating there may be a role for ICIs in this breast cancer subtype also. The I-SPY2 study examined the addition of pembrolizumab to neoadjuvant chemotherapy.9 In HR-positive, HER2-negative patients, the addition of pembrolizumab increased the pCR rate from 13% to 34%.9 The currently accruing Phase III clinical trial, CheckMate 7FL (NCT04109066) aims to explore the benefit of neoadjuvant nivolumab added to chemotherapy in HR-positive, HER2-negative breast cancer.53
Adjuvant Therapy Guided by Response to Neoadjuvant Therapy in HR-Positive, HER2-Negative Breast Cancer Using the CPS-EG Score
Determining prognosis after neoadjuvant treatment is complex. Achieving a pCR is associated with a better prognosis particularly in TNBC and HER2-positive breast cancer but less informative in HR-positive, HER2-negative breast cancer. The RCB score is generated by pathological information only obtained post neoadjuvant therapy and can be used to calculate long-term outcome. An additional prognostic scoring system is the Clinical-Pathologic Scoring System incorporating estrogen receptor–negative disease and nuclear grade 3 tumor pathology; ER, estrogen receptor (CPS-EG). This scoring system awards points based on the clinical stage at presentation, pathologic staging parameters post neoadjuvant chemotherapy, ER-negative disease and having a tumor that is high grade to generate a score that predicts prognosis.54
In order to try and improve outcome for patients with HR-positive, HER2-negative and residual disease post neoadjuvant chemotherapy the German Breast Group led the PENELOPE-B trial (NCT01864746). The trial identified patients who were at a high risk of relapse based on their CPS-EG score and sought to determine if adding the CDK 4/6-inhibitor, palbociclib for one year to standard endocrine therapy would improve DFS.55 Unfortunately, there was no improvement to DFS with the addition of palbociclib to standard endocrine therapy.
However, the monarchE Phase III RCT randomized high risk (≥4 positive lymph nodes, or 1–3 positive nodes and either tumor size ≥5 cm, histologic grade 3, or central Ki-67 ≥ 20%) HR-positive, HER2-negative patients to standard-of-care adjuvant endocrine therapy with or without abemaciclib (150 mg twice daily for 2 years). Almost 40% of each treatment arm had received neoadjuvant treatment. At 3-year follow-up invasive disease–free survival rates were 88.8% and 83.4% for abemaciclib plus endocrine therapy compared to endocrine therapy alone respectively (hazard ratio [HR] = 0.696; P < 0.0001). The distant recurrence–free survival rate was 90.3% vs 86.1%, respectively HR = 0.687; P < 0.0001).56
The OlympiA trial also used the CPS-EG score to identify a high-risk group of patients with gBRCA mutations with HR-positive, HER2-negative breast cancer.34 Patients with a CPS-EG score of 3 were eligible for the trial. As previously discussed, the OlympiA trial showed a benefit in 3-year DFS in the favour of olaparib compared to placebo (82.5% vs 68.0%) and while the majority of the patients had TNBC, this benefit was still seen in the HR-positive, HER2-negative subgroup who were able to continue their endocrine therapy concurrently.
Discussion
Response to neoadjuvant treatment provides important prognostic information. It also guides adjuvant treatment options shown to improve breast cancer survival.10,11 Pathological complete response is an accepted surrogate endpoint for clinical benefit to neoadjuvant therapies. Achieving a pCR is associated with significantly better EFS and OS, particularly for triple-negative and HER2-positive breast cancer.57
When considering optimal neoadjuvant regimens for TNBC with the goal of achieving the highest rate of pCR the addition of platinum drugs to standard anthracycline-taxane regimens have increased pCR from 33% to 55%.16,17 Building upon this the addition of ICIs represent another very significant advance. In the PD-L1-positive, ICI-treated patients from the KEYNOTE-522, IMpassion031, and NeoTRIP (PD-L1 2+/3+) trials pCR rates of 68.9%, 69% and 71.4% were observed respectively.28–30 Statistically significant improvements in EFS associated with the addition of ICIs to neoadjuvant chemotherapy have been reported so far in the KEYNOTE-522, and the Phase II GeparNUEVO. The long-term outcome results are greatly anticipated for IMpassion031 and NeoTRIP.27–30 Interestingly, KEYNOTE 522 observed an improvement in EFS even in patients who received pembrolizumab but did not achieve a pCR compared to those who did not receive pembrolizumab and also did not achieve a pCR.30 This could Indicate that while pCR remains an important prognostic biomarker others may be needed in the setting of neoadjuvant ICI treatment.
There is uncertainty about the optimum approach for patients who do not achieve a pCR after receiving an ICI as a component of neoadjuvant therapy. In IMpassion031 patients not achieving pCR in either arm of the trial could go on to receive adjuvant capecitabine or other treatment considered standard-of-care in this setting.28 Patients randomly assigned to the atezolizumab plus chemotherapy group could continue atezolizumab concomitantly with this adjuvant therapy. However, this remains an area of controversy as both adjuvant capecitabine and for gBRCA-associated breast cancer, olaparib have been approved for patients with residual disease post-neoadjuvant therapy.10,34
The role of the neoadjuvant chemotherapy is less clear in HR-positive HER2-negative breast cancer. In general, HR-positive cancers (luminal A and B) have the least chance of a pCR after neoadjuvant chemotherapy, especially if they are low-grade. If neoadjuvant chemotherapy is given for high-risk, HR-positive, HER2-negative breast cancer, standard adjuvant anthracycline-taxane regimens are appropriate. Optimum endocrine therapy is standard-of-care in the adjuvant setting regardless of whether a pCR is achieved or not. There are several genomic signatures available to guide decisions regarding adjuvant chemotherapy use however these assays are not routinely used in the neoadjuvant setting.44
Conclusion
A neoadjuvant regimen containing an anthracycline, taxane, platinum and an ICI provides the highest likelihood of achieving a pCR for patients with TNBC. Programmed cell death ligand-1 has been measured using different assays, platforms and scoring systems across studies. However, the data are consistent in showing the highest rates of pCR in patients who are PD-L1 positive. In KEYNOTE 522 patients with early-stage disease who were PD-L1-negative also benefitted from the addition of an ICI. For high-risk, HR-positive, HER2-negative disease who require neoadjuvant chemotherapy, standard anthracycline-taxane regimens are appropriate. For patients with TNBC with residual disease post-neoadjuvant chemotherapy and being treated as per the KEYNOTE-522 trial then pembrolizumab should be continued. Other options include adjuvant capecitabine, or if gBRCA1/2 adjuvant olaparib or a clinical trial. Endocrine therapy is standard-of-care for patients with HR-positive, HER2-negative breast cancer with or without a pCR. For high risk premenopausal patients receiving ovarian suppression or postmenopausal patients the optimal endocrine therapy may include an AI with the CDK4/6 inhibitor abemaciclib, as per the monarchE trial or if gBRCA mutated then olaparib as per the OlympiA trial.34,56
Disclosure
Dr Mairi W Lucas reports personal fees from STADA, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Fisher B, Brown A, Mamounas E, et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: findings from national surgical adjuvant breast and bowel project B-18. J Clin Oncol. 1997;15(7):2483–2493. doi:10.1200/JCO.1997.15.7.2483
2. Wolmark N, Wang J, Mamounas E, Bryant J, Fisher B. Preoperative chemotherapy in patients with operable breast cancer: nine-year results from national surgical adjuvant breast and bowel project B-18. JNCI Monographs. 2001;2001(30):96–102. doi:10.1093/oxfordjournals.jncimonographs.a003469
3. Bear HD, Anderson S, Smith RE, et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: national surgical adjuvant breast and bowel project protocol B-27. J Clin Oncol. 2006;24(13):2019–2027. doi:10.1200/JCO.2005.04.1665
4. von Minckwitz G, Blohmer JU, Raab G, et al. In vivo chemosensitivity-adapted preoperative chemotherapy in patients with early-stage breast cancer: the GEPARTRIO pilot study. Ann Oncol. 2005;16(1):56–63. doi:10.1093/annonc/mdi001
5. Smith IC, Heys SD, Hutcheon AW, et al. Neoadjuvant chemotherapy in breast cancer: significantly enhanced response with docetaxel. J Clin Oncol. 2002;20(6):1456–1466. doi:10.1200/JCO.2002.20.6.1456
6. Bonadonna G, Valagussa P, Brambilla C, et al. Primary chemotherapy in operable breast cancer: eight-year experience at the Milan cancer institute. J Clin Oncol. 1998;16(1):93–100. doi:10.1200/JCO.1998.16.1.93
7. Administration FaD. Guidance for industry: pathological complete response in neoadjuvant treatment of high- risk early-stage breast cancer: use as an endpoint to support accelerated approval. Silver Spring, MD: Food and Drug Administration; 2014. Available from: https://www.federalregister.gov/d/2014-23845.
8. Quantum Leap Healthcare Collaborative. The I-SPY Trials 2022. Available from: https://www.ispytrials.org/i-spy-platform/i-spy2.
9. Nanda R, Liu MC, Yau C, et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing phase 2 adaptively randomized I-SPY2 Trial. JAMA Oncology. 2020;6(5):676–684. doi:10.1001/jamaoncol.2019.6650
10. Masuda N, Lee S-J, Ohtani S, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. 2017;376(22):2147–2159. doi:10.1056/NEJMoa1612645
11. von Minckwitz G, Huang C-S, Mano MS, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. N Engl J Med. 2018;380(7):617–628. doi:10.1056/NEJMoa1814017
12. Symmans WF, Wei C, Gould R, et al. Long-Term prognostic risk after neoadjuvant chemotherapy associated with residual cancer burden and breast cancer subtype. J Clin Oncol. 2017;35(10):1049–1060. doi:10.1200/JCO.2015.63.1010
13. Yau C, Osdoit M, van der Noordaa M, et al. Residual cancer burden after neoadjuvant chemotherapy and long-term survival outcomes in breast cancer: a multicentre pooled analysis of 5161 patients. Lancet Oncol. 2022;23(1):149–160. doi:10.1016/S1470-2045(21)00589-1
14. Korde LA, Somerfield MR, Carey LA, et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline. J Clin Oncol. 2021;39(13):1485–1505. doi:10.1200/JCO.20.03399
15. Asselain B, Barlow W, Bartlett J, et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018;19(1):27–39. doi:10.1016/S1470-2045(17)30777-5
16. Poggio F, Bruzzone M, Ceppi M, et al. Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: a systematic review and meta-analysis. Ann Oncol. 2018;29(7):1497–1508. doi:10.1093/annonc/mdy127
17. Geyer CE, Sikov WM, Huober J, et al. Long-term efficacy and safety of addition of carboplatin with or without veliparib to standard neoadjuvant chemotherapy in triple-negative breast cancer: 4-year follow-up data from BrighTNess, a randomized phase III trial. Ann Oncol. 2022;33(4):384–394. doi:10.1016/j.annonc.2022.01.009
18. Bian L, Yu P, Wen J, et al. Survival benefit of platinum-based regimen in early stage triple negative breast cancer: a meta-analysis of randomized controlled trials. Npj Breast Cancer. 2021;7(1):157. doi:10.1038/s41523-021-00367-w
19. Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(10):1674. doi:10.1093/annonc/mdz189
20. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
21. Kwok G, Yau TC, Chiu JW, Tse E, Kwong YL. Pembrolizumab (Keytruda). Hum Vaccin Immunother. 2016;12(11):2777–2789. doi:10.1080/21645515.2016.1199310
22. Bianchini G, De Angelis C, Licata L, Gianni L. Treatment landscape of triple-negative breast cancer - expanded options, evolving needs. Nat Rev Clin Oncol. 2022;19(2):91–113. doi:10.1038/s41571-021-00565-2
23. Schmid P, Adams S, Rugo HS, et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379(22):2108–2121. doi:10.1056/NEJMoa1809615
24. Miles D, Gligorov J, André F, et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32(8):994–1004. doi:10.1016/j.annonc.2021.05.801
25. Rugo HSC, Cescon DW, Rugo HS, et al. KEYNOTE-355: final results from a randomized, double-blind phase III study of first-line pembrolizumab + chemotherapy vs placebo + chemotherapy for metastatic triple-negative breast cancer.
26. Schmid P, Salgado R, Park YH, et al. Pembrolizumab plus chemotherapy as neoadjuvant treatment of high-risk, early-stage triple-negative breast cancer: results from the phase 1b open-label, multicohort KEYNOTE-173 study. Ann Oncol. 2020;31(5):569–581. doi:10.1016/j.annonc.2020.01.072
27. Loibl S, Schneeweiss A, Huober JB, et al. Durvalumab improves long-term outcome in TNBC: results from the phase II randomized GeparNUEVO study investigating neodjuvant durvalumab in addition to an anthracycline/taxane based neoadjuvant chemotherapy in early triple-negative breast cancer (TNBC). J Clin Oncol. 2021;39(15_suppl):506. doi:10.1200/JCO.2021.39.15_suppl.506
28. Mittendorf EA, Zhang H, Barrios CH, et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): a randomised, double-blind, Phase 3 trial. Lancet. 2020;396(10257):1090–1100. doi:10.1016/S0140-6736(20)31953-X
29. Gianni L, Huang CS, Egle D, et al. Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple-negative, early high-risk and locally advanced breast cancer: neoTRIP Michelangelo randomized study☆. Ann Oncol. 2022;33(5):534–543. doi:10.1016/j.annonc.2022.02.004
30. Schmid P, Cortes J, Dent R, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386(6):556–567. doi:10.1056/NEJMoa2112651
31. Korde LA, Somerfield MR, Hershman DL; for the Neoadjuvant Chemotherapy ET, Panel TTfBCGE. Use of immune checkpoint inhibitor pembrolizumab in the treatment of high-risk, early-stage triple-negative breast cancer: ASCO guideline rapid recommendation update. J Clin Oncol. 2022;40:1696–1698.
32. Litton JK, Beck JT, Jones JM, et al. Neoadjuvant talazoparib in patients with germline BRCA1/2 (gBRCA1/2) mutation-positive, early HER2-negative breast cancer (BC): results of a phase 2 study. J Clin Oncol. 2021;39(15_suppl):505. doi:10.1200/JCO.2021.39.15_suppl.505
33. Huo X, Li J, Zhao F, et al. The role of capecitabine-based neoadjuvant and adjuvant chemotherapy in early-stage triple-negative breast cancer: a systematic review and meta-analysis. BMC Cancer. 2021;21(1):78. doi:10.1186/s12885-021-07791-y
34. Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med. 2021;384(25):2394–2405. doi:10.1056/NEJMoa2105215
35. Cortés J, Kim S-B, Chung W-P, et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. N Engl J Med. 2022;386(12):1143–1154. doi:10.1056/NEJMoa2115022
36. Dieras V, Lusque A, Deluche E, et al. Trastuzumab deruxtecan for advanced breast cancer patients, regardless of HER2 status: a phase II study with biomarkers analysis (DAISY).
37. Moon SJ, Govindan SV, Cardillo TM, D’Souza CA, Hansen HJ, Goldenberg DM. Antibody conjugates of 7-ethyl-10-hydroxycamptothecin (SN-38) for targeted cancer chemotherapy. J Med Chem. 2008;51(21):6916–6926. doi:10.1021/jm800719t
38. Goldenberg DM, Cardillo TM, Govindan SV, Rossi EA, Sharkey RM. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget. 2015;6(26):22496–22512. doi:10.18632/oncotarget.4318
39. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
40. von Minckwitz G, Untch M, Blohmer JU, et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J Clin Oncol. 2012;30(15):1796–1804. doi:10.1200/JCO.2011.38.8595
41. Peto R, Davies C, Godwin J, et al. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet. 2012;379(9814):432–444.
42. Blum JL, Flynn PJ, Yothers G, et al. Anthracyclines in early breast cancer: the ABC trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG Oncology). J Clin Oncol. 2017;35(23):2647–2655. doi:10.1200/JCO.2016.71.4147
43. Nitz U, Gluz O, Clemens M, et al. West German study PlanB trial: adjuvant four cycles of epirubicin and cyclophosphamide plus docetaxel versus six cycles of docetaxel and cyclophosphamide in HER2-negative early breast cancer. J Clin Oncol. 2019;37(10):799–808. doi:10.1200/JCO.18.00028
44. Andre F, Ismaila N, Allison KH, et al. Biomarkers for adjuvant endocrine and chemotherapy in early-stage breast cancer: ASCO guideline update. J Clin Oncol. 2022;40:1816–1837.
45. Kalinsky K, Barlow WE, Gralow JR, et al. 21-gene assay to inform chemotherapy benefit in node-positive breast cancer. N Engl J Med. 2021;385(25):2336–2347. doi:10.1056/NEJMoa2108873
46. Sparano JA, Gray RJ, Makower DF, et al. Adjuvant chemotherapy guided by a 21-gene expression assay in breast cancer. N Engl J Med. 2018;379(2):111–121. doi:10.1056/NEJMoa1804710
47. Gianni L, Zambetti M, Clark K, et al. Gene expression profiles in paraffin-embedded core biopsy tissue predict response to chemotherapy in women with locally advanced breast cancer. J Clin Oncol. 2005;23(29):7265–7277. doi:10.1200/JCO.2005.02.0818
48. Bear HD, Wan W, Robidoux A, et al. Using the 21-gene assay from core needle biopsies to choose neoadjuvant therapy for breast cancer: a multicenter trial. J Surg Oncol. 2017;115(8):917–923. doi:10.1002/jso.24610
49. Varnier R, Sajous C, de Talhouet S, et al. Using breast cancer gene expression signatures in clinical practice: unsolved issues, ongoing trials and future perspectives. Cancers. 2021;13(19):4840. doi:10.3390/cancers13194840
50. Jung JG, Kim HK, Kim Y, et al. Personalized neoadjuvant strategy in luminal A breast cancer to increase breast conserving surgery (BCS) rate [PLATO study]. J Clin Oncol. 2020;38(15_suppl):TPS603–TPS603. doi:10.1200/JCO.2020.38.15_suppl.TPS603
51. Allison KH, Hammond MEH, Dowsett M, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol. 2020;38(12):1346–1366. doi:10.1200/JCO.19.02309
52. Dieci MV, Griguolo G, Bottosso M, et al. Impact of estrogen receptor levels on outcome in non-metastatic triple negative breast cancer patients treated with neoadjuvant/adjuvant chemotherapy. Npj Breast Cancer. 2021;7(1):101. doi:10.1038/s41523-021-00308-7
53. Loi S, McArthur HL, Harbeck N, et al. A phase III trial of nivolumab with neoadjuvant chemotherapy and adjuvant endocrine therapy in ER+/HER2- primary breast cancer: checkMate 7FL. J Clin Oncol. 2020;38(15_suppl):TPS604–TPS604. doi:10.1200/JCO.2020.38.15_suppl.TPS604
54. Jeruss JS, Mittendorf EA, Tucker SL, et al. Combined use of clinical and pathologic staging variables to define outcomes for breast cancer patients treated with neoadjuvant therapy. J Clin Oncol. 2008;26(2):246–252. doi:10.1200/JCO.2007.11.5352
55. Loibl S, Marmé F, Martin M, et al. Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer—the penelope-B trial. J Clin Oncol. 2021;39(14):1518–1530. doi:10.1200/JCO.20.03639
56. Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32(12):1571–1581. doi:10.1016/j.annonc.2021.09.015
57. Spring LM, Fell G, Arfe A, et al. Pathologic complete response after neoadjuvant chemotherapy and impact on breast cancer recurrence and survival: a comprehensive meta-analysis. Clin Cancer Res. 2020;26(12):2838–2848. doi:10.1158/1078-0432.CCR-19-3492
58. Loibl S, Untch M, Burchardi N, et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol. 2019;30(8):1279–1288. doi:10.1093/annonc/mdz158
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Differences in Treatment Outcomes Between Patients with HER2-Low versus HER2-Zero, Hormone Receptor-Positive Advanced-Stage Breast Cancer Treated with Ribociclib
Sharaf B, Abu-Fares H, Tamimi F, Al-Sawajneh S, Salama O, Daoud R, Alhajahjeh A, Al-Lababidi S, Abdel-Razeq H
Breast Cancer: Targets and Therapy 2023, 15:541-548
Published Date: 28 July 2023
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
The Potent Novel CDK4/6 Inhibitor TQB3616 in Hormone Receptor Positive Breast Cancer: Preclinical Characterization with in vitro and Human Tumor Xenograft Models
Hu W, Wang L, Luo J, Zhang J, Li N
Breast Cancer: Targets and Therapy 2023, 15:899-912
Published Date: 8 December 2023
Innovative Surgical Approaches That Improve Individual Outcomes in Advanced Breast Cancer
Luțenco V, Rebegea L, Beznea A, Tocu G, Moraru M, Mihailov OM, Ciuntu BM, Luțenco V, Stanculea FC, Mihailov R
International Journal of Women's Health 2024, 16:555-560
Published Date: 30 March 2024
Recent Advances in Immunotherapy for Breast Cancer: A Review
Wen QE, Li L, Feng RQ, Li DH, Qiao C, Xu XS, Zhang YJ
Breast Cancer: Targets and Therapy 2024, 16:497-516
Published Date: 27 August 2024