Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
A Structured Classification of Pyrotinib-Containing Neoadjuvant Regimens for HER2-Positive Breast Cancer: Efficacy, Safety, and Regimen Selection
Authors Liu J ![]() , Peng X, Yang Y, Huang X, Du Y
, Peng X, Yang Y, Huang X, Du Y ![]() , Liu K
, Liu K
Received 2 February 2026
Accepted for publication 15 May 2026
Published 20 May 2026 Volume 2026:18 600575
DOI https://doi.org/10.2147/BCTT.S600575
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Jiani Liu,1,* Xinyu Peng,2,* Yang Yang,3,* Xuhui Huang,1,* Yongtao Du,1 Keming Liu1
1Department of Breast Surgery, Baoding No. 1 Central Hospital, Baoding, Hebei, 071000, People’s Republic of China; 2Department of Gastrointestinal Surgery, Affiliated Hospital of Hebei University, Baoding, Hebei, 071000, People’s Republic of China; 3Department of Medical Oncology, Affiliated Hospital of Hebei University, Baoding, Hebei, 071000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiani Liu, Department of Breast Surgery, Baoding No. 1 Central Hospital, 320 Changcheng North Street, Lianchi District, Baoding, Hebei, 071000, People’s Republic of China, Tel +86-159-3121-9836, Email [email protected]
Abstract: This structured review presents a classification framework for pyrotinib-containing neoadjuvant regimens in HER2-positive breast cancer. Studies were identified through a comprehensive literature search and categorized into four strategies: pyrotinib plus chemotherapy, pyrotinib plus trastuzumab with chemotherapy, pyrotinib combined with cell-cycle inhibitors, and pyrotinib combined with antibody-drug conjugates (ADCs). We summarized the pathological complete response(pCR) rates and adverse event profiles of these approaches for neoadjuvant treatment of HER2-positive breast cancer. The pCR rates vary substantially across categories, ranging from approximately 28% to 74%, as do the grade ≥ 3 toxicity patterns. Therefore, the key to selecting an optimal pyrotinib-based neoadjuvant regimen is to match the regimen choice with tumor characteristics such as hormone receptor status, HER2 immunohistochemical level, intrinsic molecular subtype, and early response to initial therapy, while balancing efficacy and safety and considering patient-specific factors like age and cardiac risk. Existing studies are generally limited by small sample sizes and a lack of long-term survival data, and high-level evidence directly comparing pyrotinib-based strategies with trastuzumab plus pertuzumab is scarce. Future research should prioritize biomarker-driven patient selection, response-adaptive trial designs, and standardized toxicity management to optimize clinical decision-making.
Keywords: breast cancer, pyrotinib, neoadjuvant therapy, HER2, pathological complete response
Introduction
The systemic treatment of cancer has undergone a profound evolution over the past century, progressing from non‑specific cytotoxic agents to molecularly targeted therapies and, more recently, to combination strategies that aim to overcome adaptive resistance. As outlined in the comprehensive historical review by Sonkin et al, the introduction of trastuzumab (a monoclonal antibody against HER2) in 1998 marked the beginning of the era of molecularly targeted cancer therapy Since then, targeted therapies have significantly improved outcomes for several malignancies, yet resistance—both primary and acquired—remains a major challenge.1 In the context of HER2‑positive breast cancer, the clinical trajectory has moved from single‑agent trastuzumab to dual blockade (trastuzumab plus pertuzumab) and, more recently, to tyrosine kinase inhibitors (TKIs) and antibody–drug conjugates (ADCs), reflecting a continuous effort to optimize efficacy while managing toxicity and overcoming resistance. In this broader therapeutic context, the value of comparing pyrotinib-containing regimens lies not in simply ranking pCR rates, but in understanding which patient subgroups benefit most from which incremental treatment intensification or de-escalation.
HER2-positive breast cancer accounts for approximately 15%–20% of all breast cancers globally, and a Chinese report suggested an incidence of 22.5%.2,3 Neoadjuvant therapy (NAT) has been widely implemented in the comprehensive management of HER2-positive breast cancer. Evidence indicates that achieving total pathological complete response (tpCR) after NAT in early-stage or locally advanced disease is a strong predictor of long-term survival. The NeoSphere trial4 and the PEONY trial5 established trastuzumab plus pertuzumab (HP) as the cornerstone of neoadjuvant anti-HER2 therapy. Studies including TRAIN-2 and others6–9 demonstrated that HP combined with chemotherapy can increase tpCR rates to approximately 60%. Nevertheless, about 40% of patients do not achieve tpCR after these regimens and have relatively poorer prognoses. How can the efficacy of neoadjuvant therapy for HER2-positive breast cancer be further improved?
Pyrotinib (Py) is an irreversible pan-ErbB tyrosine kinase inhibitor originally developed in China. As an alternative HER2 blockade strategy, pyrotinib offers multi-target inhibition, oral administration, and potentially lower cardiotoxicity. Pyrotinib acts intracellularly by covalently binding to the ATP‑binding pocket of HER1, HER2, and HER4, thereby blocking downstream PI3K/AKT and MAPK signaling. In contrast, trastuzumab is a monoclonal antibody that binds to the extracellular domain of HER2, inhibiting receptor dimerization and recruiting antibody‑dependent cellular cytotoxicity (ADCC). When combined, pyrotinib (intracellular) and trastuzumab (extracellular) provide dual‑compartment HER2 blockade, which can overcome adaptive resistance and enhance antitumor efficacy. Similarly, antibody–drug conjugates (ADCs) use HER2‑directed antibodies to deliver cytotoxic payloads specifically into tumor cells via receptor‑mediated internalization; the released payload induces DNA damage or mitotic arrest. Adding pyrotinib to an ADC may concurrently suppress residual HER2 signaling through intracellular TKI activity while the ADC provides targeted chemotherapy, offering a complementary mechanism. A downstream node critical for cell cycle progression is the cyclin D–CDK4/6–Rb axis; preclinical evidence shows that CDK4/6 inhibition synergizes with HER2 blockade, supporting the combination of pyrotinib with CDK4/6 inhibitors.
To date, evidence for pyrotinib in the neoadjuvant setting remains limited, and combination regimens with chemotherapy or other targeted agents are heterogeneous. How to optimize regimens and balance efficacy and toxicity is a key unresolved issue. In parallel, given the notable activity of cyclin-dependent kinase inhibitors (CDKis) and ADCs in advanced breast cancer, investigators have begun exploring these agents in neoadjuvant strategies. Here, we classify and summarize pyrotinib-containing neoadjuvant regimens to provide a reference for rational clinical practice. Notably, HER2-positive breast cancer is a highly heterogeneous disease. At present, however, anti-HER2 treatment decisions in the neoadjuvant setting are not yet well guided by biomarkers; clinical stratification remains largely empirical, with limited integration of molecular features into routine practice. Looking forward, as multi-omics biomarkers, intrinsic molecular subtyping, and treatment-response dynamics become increasingly incorporated into clinical reasoning within a precision oncology framework, treatment selection may progress toward more individualized and response-adaptive strategies.
For this review, we searched PubMed, Embase, and Cochrane Library databases up to December 2025 using keywords including “pyrotinib,” “HER2-positive breast cancer,” and “neoadjuvant,” and all eligible studies were categorized into four regimen types for descriptive synthesis.
Pyrotinib as Single Anti-HER2 Targeting Combined with Chemotherapy
Small retrospective studies by Yao10 and Tian11 evaluated pyrotinib combined with TAC as neoadjuvant therapy and reported objective response rates (ORR) of 100%, with tpCR rates of 45.5% (10/22) and 37.0% (10/37), respectively. In small prospective studies, Xiang12 (ChiCTR1900028212) and Ye13 (ChiCTR2100050870) investigated pyrotinib combined with T, reporting tpCR rates of 54.5% (12/22) and 48.4% (15/31), which were higher than the tpCR rates observed with TH in NeoSphere4 (NCT00545688) and PEONY5 (NCT02586025) (29.0% and 21.8%, respectively). However, head-to-head comparisons between pyrotinib and trastuzumab in the neoadjuvant setting remain unavailable, and whether pyrotinib monotherapy-based neoadjuvant therapy is superior to trastuzumab requires further investigation.
Li14 (ChiCTR1900026061) evaluated pyrotinib plus EC, reporting an ORR of 97.3% and a tpCR rate of 28.6% (10/35). This design was partly motivated by concerns that concurrent anthracyclines and trastuzumab may increase cardiotoxicity; however, the regimen did not yield a notably higher tpCR rate. Wang15 investigated pyrotinib plus capecitabine as neoadjuvant therapy in elderly patients, reporting an ORR of 100% and a tpCR rate of 43.5% (10/23). Although an all-oral regimen may facilitate home-based treatment in frail elderly patients, the high incidence of diarrhea (82.6%) warrants careful attention.
Overall, studies of pyrotinib as single anti-HER2 targeting combined with chemotherapy are limited by small sample sizes and heterogeneity in enrolled populations. Whether these regimens outperform trastuzumab-based approaches, and whether pyrotinib offers specific advantages in subgroups such as patients with cardiac comorbidities or older adults, remains to be determined.
HPy Combined with Different Chemotherapy Regimens
TCb/P–HPy
The Panphila study (NCT03735966) was a prospective, multicenter, single-arm Phase II trial of TCbHPy as neoadjuvant therapy. Among 75 patients with stage II–III disease, 61 completed six planned 3-week cycles, achieving a tpCR rate of 57.4% (35/61).16 In another study by Liu et al (ChiCTR2100043523), 34 patients completed six planned 3-week cycles of TCbHPy, with a tpCR rate of 55.9% (19/34).17 In NeoATP study (NCT04126525), patients received pyrotinib plus trastuzumab combined with weekly paclitaxel plus cisplatin(P) for four cycles, achieving a tpCR rate of 69.81% (37/52).18 Notably, NeoATP had the shortest treatment duration and the highest proportion of stage III patients (73.58%), yet reported the highest tpCR rate, potentially reflecting the intensive paclitaxel–cisplatin schedule. However, grade ≥3 neutropenia occurred in 49%, substantially higher than in other studies.
In comparative studies, Zheng et al enrolled 32 young patients with locally advanced breast cancer and found that TCbHPy achieved a significantly higher tpCR rate than TCbH (43.8% vs 25.0%, P=0.0287).19 Ding et al (NCT03756064) conducted a multicenter, randomized, double-blind, placebo-controlled phase II trial comparing TCbHPy with TCbH in Chinese patients with early-stage or locally advanced HER2-positive breast cancer. In the intention-to-treat population, the overall pCR rate was 65.5% (19/29) in the TCbHPy group versus 33.3% (10/30) in the placebo group (p=0.013).20
The NeoPaTHer study (NCT03847818) enrolled 129 patients and used magnetic resonance imaging (MRI) after two cycles of TCbH to assess early response. Responders (group A, 62/129; 48.1%) continued therapy and achieved a tpCR rate of 30.6%. Among non-responders, 26 continued TCbH (group B; tpCR 15.4%), whereas 41 received additional pyrotinib (group C; tpCR 29.3%). Multivariable logistic regression suggested comparable odds of tpCR in groups A and C,21 implying that pyrotinib nearly doubled tpCR among non-responders. However, as this study lacked a pertuzumab-containing comparator, it cannot establish whether adding pyrotinib is superior to adding pertuzumab for TCbH non-responders.
In a retrospective analysis by Zhu et al (NCT03735966), 545 patients received TCb chemotherapy with different targeted regimens: HPy (n=63), HP (n=198), or H alone (n=284). The pCR rate was similar between TCbHPy and TCbHP (55.6% vs 56.6%, P=0.896) and higher than TCbH (55.6% vs 32.7%, P<0.001).22 These results expand neoadjuvant options for HER2-positive breast cancer.
ECPy–THPy
In a phase II study by Xuhong et al (ChiCTR1900022293), 20 patients were enrolled and 19 completed neoadjuvant therapy followed by surgery. The ECPy–THPy regimen achieved an ORR of 100% and a tpCR rate of 73.7%, including tpCR in both stage IIIC patients with supraclavicular lymph node metastasis.23 The investigators subsequently conducted a Phase III study enrolling 175 patients, with 156 undergoing surgery; the ORR was 89.1% and the tpCR rate was 68.6%.24 In another study by Liu et al, 138 patients were included (ECPy–THPy, n=55; EC–TH, n=83), and the pCR rate was higher in the ECPy–THPy group than in the EC–TH group (63.64% vs 39.76%, P<0.05).25
Collectively, ECPy–THPy appears to be a promising neoadjuvant regimen for stage II–III HER2-positive breast cancer. Early incorporation of pyrotinib may address a limitation of conventional EC–THP-like approaches, in which anti-HER2 therapy is absent during the initial anthracycline cycles, and may contribute to higher tpCR rates. Notably, Liu et al observed an increasing number of patients achieving clinical complete response (cCR) with additional cycles, suggesting that shortening the overall duration may risk insufficient response. However, eight cycles of preoperative treatment is a relatively long course, which may reduce patient compliance.
When compared with the TCbHPy regimen discussed above, ECPy–THPy generally yields numerically higher tpCR rates (63%–74% vs 55%–66%). However, it should be noted that the platinum-containing TCbHPy regimen is associated with substantial hematologic toxicity—particularly thrombocytopenia—which can be especially pronounced in Chinese patients. Moreover, the platinum doses used in clinical trials conducted in Chinese populations may be difficult to fully replicate in routine clinical practice due to tolerability concerns, potentially leading to a reduction in pCR rates in real-world settings. Direct head-to-head comparisons between ECPy–THPy and TCbHPy are lacking, so no definitive conclusion about superiority can be drawn. At present, the choice between these two strategies involves a clinical trade-off: ECPy–THPy offers an anthracycline-containing approach with early TKI integration that may achieve higher tpCR rates but requires a longer treatment course (eight cycles vs six cycles), whereas TCbHPy provides a shorter, platinum-based option whose real-world efficacy may be somewhat attenuated by dose modifications necessitated by hematologic toxicity.
THPy
Zhong et al (NCT04152057) conducted a single-arm phase II study enrolling 21 patients and reported an overall pCR rate of 57.1% with THPy, with an ORR of 100%.26 In a study by Wang et al (n=72; THPy, n=34; TH, n=38), the tpCR rate was higher in the TH+Py group than in the TH+placebo group (47.06% vs 23.68%, P=0.049).27 The PHEDRA trial (NCT03588091), a multicenter, double-blind, randomized phase III study enrolling 335 patients, showed a higher tpCR rate with TH+Py versus TH+placebo (41.0% vs 22.0%, P<0.0001).28 Based on these data, pyrotinib was approved in China for the neoadjuvant indication in HER2-positive breast cancer, and THPy is recommended in Chinese guidelines.29
Although THPy generally yields lower tpCR rates than TCb/P–HPy or ECPy–THPy, it is associated with fewer adverse events and may offer a favorable safety profile. Therefore, identifying patients who can achieve high tpCR rates with reduced chemotherapy intensity is of considerable clinical interest. In NJMU-BC01 (NCT05659056), patients were stratified by BluePrint and MammaPrint. After six cycles of THPy, tpCR reached 53% (23/43) in the BluePrint HER2-enriched subtype versus 30% (7/23) in non–HER2-enriched subtypes; tpCR was 61% (24/39) in the MammaPrint ultra-high-risk group versus 22% (6/27) in the high-risk group (P=0.0024).30 These findings suggest that de-escalation strategies may be particularly promising for HER2-enriched disease, emphasizing the importance of reliable predictive factors for precise patient selection.
Pyrotinib Combined With Cell Cycle Inhibitors
Multiple studies indicate that standard anti-HER2 strategies may be less effective in triple-positive breast cancer (TPBC). For example, in Panphila, tpCR was higher in HR-negative than HR-positive patients (86.4% vs 40.4%, P<0.001).16 Accordingly, chemotherapy-free oral neoadjuvant regimens combining pyrotinib and the CDK4/6 inhibitor dalpiciclib have been explored. In a multicenter, single-arm phase II study by Niu et al (NCT04486911), five cycles of oral pyrotinib, dalpiciclib, and letrozole achieved a tpCR rate of 30.4% (24/79; 95% CI, 21.3–41.3), which was suboptimal.31 Subsequently, Huo et al (NCT05228951) added trastuzumab to this backbone and reported a tpCR rate of 58% (7/12).32 Although evidence remains limited, these results suggest that chemotherapy-free combination strategies may represent an alternative neoadjuvant option in selected patients.
Preclinical evidence indicates that the cyclin D–CDK4/6 complex is a direct downstream effector of HER2 signaling, and CDK4/6 inhibition can synergize with anti-HER2 therapy to suppress proliferation and invasion of HER2-positive breast cancer cells. This rationale applies not only to HR-positive/HER2-positive models but also across HR statuses, supporting the biological plausibility of CDK4/6 inhibition in HER2-positive disease.33–36 In XYBC01 (ChiCTR2200060748), trastuzumab plus pyrotinib plus dalpiciclib plus letrozole was evaluated in HR-negative/HER2-positive patients, achieving a tpCR rate of 63.3% (19/30; 95% CI, 45.5–78.1%) with acceptable toxicity.37 NeoPICD (NCT06234137) further suggested that non-responders exhibited enrichment of genes related to cytoplasmic translation, mRNA metabolism, RNA splicing, telomerase activity, intermediate filament organization, and protein folding, indicating high cell-cycle activity after two treatment cycles and implying that CDK inhibition may reverse resistance.38 Overall, the chemotherapy-free combination of trastuzumab, pyrotinib, letrozole, and dalpiciclib may be a viable preoperative strategy for early-stage or locally advanced HER2-positive breast cancer.
Pyrotinib Combined With ADCs
The MUKDEN 06 trial (NCT05426486) is a multicenter, randomized Phase 2b study comparing ARX788 (an anti-HER2 ADC) plus pyrotinib with a standard neoadjuvant regimen TCbHPy (docetaxel, carboplatin, trastuzumab, and pyrotinib) in HER2-positive breast cancer. The tpCR rate was 70.6% (48/68) in the ARX788-plus-pyrotinib group versus 51.5% (35/68) in the standard group, yielding an absolute difference of 19.1% (95% CI, 2.7–34.6; p=0.023). Patients with node-positive disease (77.1% vs 48.9%) and stage IIIA–IIIC disease (74.2% vs 46.7%) appeared to derive greater benefit from ARX788 plus pyrotinib.39 These findings suggest that ADC–TKI combinations may be particularly advantageous for more advanced disease, although larger studies and additional safety data are needed.
FASCINATE-N (NCT05582499) is a randomized, open-label, single-center phase II study. The pCR rate was 63.2% (55/87) with SHR-A1811 alone, 62.5% (55/88) with SHR-A1811 plus pyrotinib, and 64.4% (58/90) with TCbHP, with no significant differences among groups.40 Given that SHR-A1811 monotherapy required fewer dose modifications and discontinuations due to adverse events compared with TCbHP, SHR-A1811 may represent a feasible neoadjuvant option.
Collectively, these data support the potential of combining anti-HER2 ADCs with TKIs as neoadjuvant strategies for HER2-positive breast cancer. Distinct toxicity profiles across regimens suggest that different approaches may be better suited to different patient populations, underscoring the need for individualized treatment. Although ADC–TKI combinations show unique safety characteristics and require further optimization, they may provide new options for patients with poor response to conventional neoadjuvant therapy or more advanced-stage disease.
Safety
Diarrhea is the most common adverse event (AE) in pyrotinib-containing regimens, with an incidence of approximately 88%–98%, and is a major reason for dose reduction, treatment delay, or discontinuation. Loperamide administration for primary prevention can make this side effect controllable.In TCbHPy regimens, grade ≥3 diarrhea occurs in roughly 40%–45%. Platinum-containing regimens also increase the risk of grade ≥3 thrombocytopenia (approximately 10%), whereas non-platinum regimens report grade ≥3 thrombocytopenia rates of about 0%–1%. Across 3-week chemotherapy schedules incorporating pyrotinib, grade ≥3 neutropenia occurs in approximately 4%–20%; in NeoATP, which used weekly chemotherapy, grade ≥3 neutropenia reached 49%. Multiple studies suggest that pyrotinib itself does not increase myelosuppression. Because pyrotinib plus dalpiciclib is an oral–oral regimen and may not routinely incorporate long-acting granulocyte colony-stimulating factor, careful monitoring for grade ≥3 neutropenia is warranted. Compared with chemotherapy-based combinations, pyrotinib plus ADC regimens may reduce hematologic toxicity; however, interstitial lung disease has been reported at a rate up to 42%, including grade ≥3 events in 4%.
Toward Biomarker-Guided Treatment Selection
The marked intertumoral heterogeneity of HER2-positive breast cancer necessitates a shift from empirical regimen selection toward biomarker-informed precision strategies. Recent multi-omics profiling efforts have begun to illuminate this heterogeneity at the molecular level: transcriptomic analyses have identified four distinct subtypes of HER2-positive breast cancer—ranging from classical HER2-addicted to basal/mesenchymal-like tumors—each harboring distinct therapeutic vulnerabilities.41 Although these molecular taxonomies have not yet been translated into routine clinical practice, they provide a compelling conceptual framework for rationalizing the differential efficacy of anti-HER2 therapies and point toward a future in which treatment selection may be progressively aligned with the molecular features of individual tumors.
Intrinsic molecular subtyping represents one promising classifier. In the NJMU-BC01 trial, patients with BluePrint-defined HER2-enriched tumors achieved a tpCR rate of 53% with de-escalated THPy, compared with only 30% in non–HER2-enriched subtypes, suggesting that transcriptomic profiling may identify tumors amenable to reduced chemotherapy intensity.30
Triple-positive breast cancer—characterized by bidirectional crosstalk between HER2 and estrogen receptor signaling—often exhibits suboptimal response to standard dual blockade. In this subgroup, the cyclin D–CDK4/6 axis serves as a convergent downstream node, providing mechanistic rationale for chemotherapy-free combinations of pyrotinib with CDK4/6 inhibitors.32,39 Spatial multi-omics analysis from NeoPICD further refines this logic: non-responders after two cycles of anti-HER2 therapy showed enrichment of genes related to cytoplasmic translation, mRNA metabolism, and cell-cycle progression, indicating that persistent proliferative drive may be susceptible to CDK4/6 inhibition.38
Specific genomic alterations also act as powerful determinants of drug response. Somatic PIK3CA mutations, which constitutively activate the PI3K pathway, are a well-established resistance driver. In a phase III trial of ECPy–THPy, tpCR was starkly lower in PIK3CA-mutant tumors (26.3%) than in wild-type tumors (80.8%), suggesting that this aberration may limit the benefit of pyrotinib-based intensification.24 Similarly, HER2 protein overexpression assessed by immunohistochemistry (IHC) remains a practical and robust biomarker. In Panphila, tpCR was 60.7% in IHC 3+ tumors versus 30.8% in IHC 2+/FISH(+) tumors,16 a pattern recapitulated across other pyrotinib studies. This gradient of HER2 signaling dependency implies that IHC 2+/FISH(+) tumors—harboring lower HER2 addiction—may derive particular benefit from more potent ADC–TKI combinations, as suggested by the markedly higher tpCR observed with ARX788 plus pyrotinib in node-positive and stage III disease.39
Beyond genomic and transcriptomic features, the tumor–immune spatial architecture has emerged as a novel dimension of vulnerability. Yang et al demonstrated that favorable outcomes correlated with specific spatial interactions between epithelial cells expressing high IDO and HLA-DR and surrounding Ki67+ M1 macrophages and CD163− T cells; the absence of these immunostimulatory niches was associated with a fibroblast-induced immune barrier that could be overcome by adding pyrotinib.38 Although these spatial signatures have not yet been validated in large prospective cohorts, they illustrate the potential of integrating immune contexture into treatment algorithms. In clinical practice, response-adapted strategies—as exemplified by the NeoPaTHer trial—provide a pragmatic and independently valuable approach: among patients who failed to achieve early MRI response after two cycles of TCbH, the addition of pyrotinib nearly doubled the tpCR rate (29.3% vs 15.4%), demonstrating that early pharmacodynamic assessment can identify tumors resistant to conventional anti-HER2 therapy and that adding pyrotinib may partially reverse this resistance.21 It should be noted, however, that the TCbH backbone used in NeoPaTHer does not reflect the current standard of trastuzumab plus pertuzumab-based neoadjuvant regimens; whether pyrotinib can similarly salvage non-responders to dual HER2 blockade with trastuzumab and pertuzumab warrants dedicated clinical investigation. Looking forward, integrating upfront multi-omics classification (eg., intrinsic subtype, PIK3CA status, and HER2 IHC level) with on-treatment response dynamics could construct a more comprehensive two-dimensional stratification algorithm—directing patients toward de-escalated chemotherapy, intensified targeted combinations, or novel ADC–TKI strategies. As multi-omics technologies mature and become more accessible, such an integrated framework may transform a diverse menu of pyrotinib-containing regimens into a profile of precision-tailored therapeutic sequences.
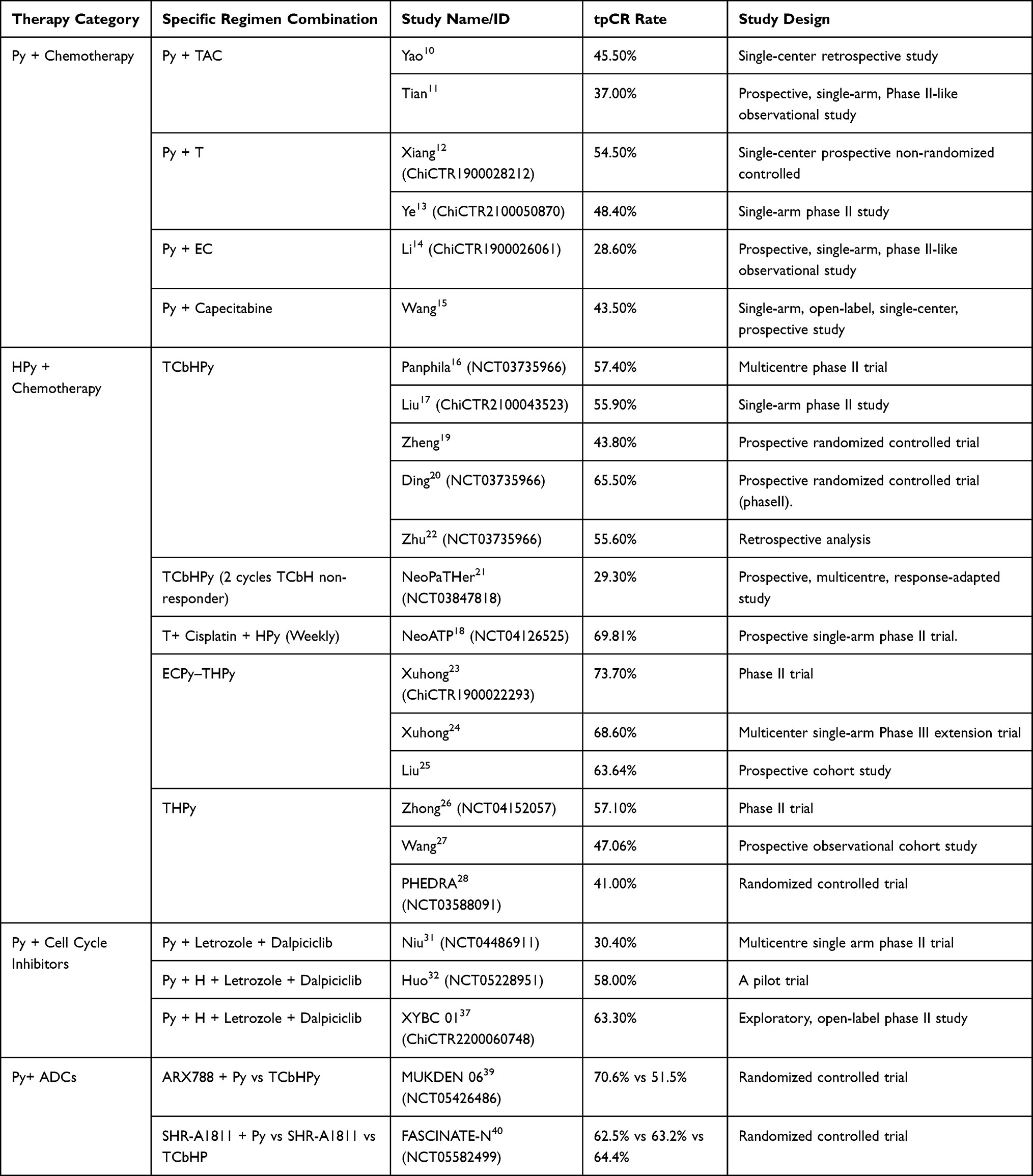 |
Table 1 Summary of tpCR Rates for Pyrotinib-Containing Neoadjuvant Therapy Regimens in HER2-Positive Breast Cancer |
Summary and Outlook
Compared with prior reviews, this article provides a more granular classification of pyrotinib-containing neoadjuvant regimens, summarizes tpCR outcomes across strategies, and discusses potentially suitable populations, thereby supporting clinical decision-making (Table 1). A central premise underscored by the evidence reviewed herein is that HER2-positive breast cancer is not a monolithic entity but a spectrum of molecularly distinct diseases with divergent therapeutic vulnerabilities. Accordingly, future progress hinges on three interdependent priorities: identifying sensitive populations, discovering robust predictive biomarkers, and balancing efficacy with safety.
Beyond the biological heterogeneity of the disease itself, diagnostic heterogeneity introduced by HER2 testing methods adds another layer of complexity. The consistent tpCR gradient stratified by HER2 IHC intensity—IHC 3+ tumors consistently outperforming IHC 2+/FISH(+) tumors across multiple pyrotinib studies—suggests that HER2 protein expression level, rather than gene amplification status alone, may better reflect the degree of HER2 signaling addiction. However, discordant or borderline IHC/FISH results are not uncommon in clinical practice. For instance, complete deletion of CEP17 can produce falsely elevated HER2/CEP17 ratios, potentially leading to erroneous HER2 classification and inappropriate treatment assignment.42 Such diagnostic uncertainty may dilute treatment effects in clinical trials and confound cross-study comparisons, underscoring the need for rigorous, standardized HER2 testing protocols and transparent reporting of testing methodologies in future prospective studies.
The residual disease observed in 30%–60% of patients also reflects the interplay of primary and acquired resistance mechanisms. Primary resistance may stem from incomplete oncogene addiction—as seen in tumors with low HER2 expression or PIK3CA mutations that activate downstream signaling bypass.24 Acquired resistance, by contrast, often involves adaptive cell-cycle reactivation under sustained HER2 blockade, a mechanism directly supported by the NeoPICD trial and providing rationale for the addition of CDK4/6 inhibitors.38 More broadly, functional genomics approaches such as genome-wide CRISPR screening have proven powerful in systematically identifying novel resistance drivers and corresponding therapeutic vulnerabilities;43 applied to HER2-positive breast cancer, such methodologies could inform the rational design of next-generation pyrotinib-containing combinations. Understanding whether residual disease reflects target persistence, pathway reactivation, or microenvironment-mediated protection will be critical for moving beyond empirical regimen selection toward mechanistically grounded treatment strategies.
Current studies remain predominantly limited by small sample sizes, single-arm designs, and the absence of long-term survival endpoints. Whether pyrotinib-containing neoadjuvant regimens improve invasive disease-free survival (iDFS) and overall survival (OS) beyond pCR remains unknown and represents the most critical evidence gap. The high incidence of diarrhea—affecting 88%–98% of patients—necessitates standardized prophylactic and management protocols to preserve dose intensity and quality of life. Given that pyrotinib can penetrate the blood–brain barrier, its potential to reduce the long-term risk of brain metastasis merits dedicated investigation. Encouragingly, preliminary signals from PILHLE-001 suggest antitumor activity of pyrotinib plus chemotherapy in HER2-low disease (IHC 2+/FISH−),44 hinting at a possible expansion of pyrotinib’s neoadjuvant role beyond classical HER2-positive tumors.
Given that current evidence for neoadjuvant pyrotinib is derived predominantly from Chinese populations and single-country trials, international multicenter studies, particularly those directly comparing pyrotinib-based regimens with trastuzumab–pertuzumab, are urgently needed to validate these findings in broader populations and health systems.
Looking forward, the field must move toward biomarker-driven clinical trials with response-adaptive designs, coupled with multi-omics correlative analyses and rigorous HER2 testing standardization, to translate the emerging molecular taxonomy of HER2-positive breast cancer into individualized neoadjuvant strategies that maximize efficacy while minimizing unnecessary toxicity. Only through such precision oncology reasoning can the full therapeutic potential of pyrotinib-containing regimens be realized.
Abbreviations
T, taxane (nab-paclitaxel, paclitaxel, or docetaxel); A, liposomal doxorubicin; E, epirubicin; C, cyclophosphamide; P, cisplatin (note: P is also used for pertuzumab in some contexts; here, cisplatin is denoted as P in platinum-containing regimens as in the original schema); Cb, carboplatin; Py, pyrotinib; H, trastuzumab; P, pertuzumab.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This paper is dedicated to the memory of Professor Chongzhu Hu. We sincerely thank him for inspiring the conceptual framework of this work.
Author Contributions
JL: Conceptualization, formal analysis, funding acquisition, project administration, validation, writing—review & editing. XP: Formal analysis, investigation, methodology, validation, writing—original draft. YY: Supervision, validation, writing—original draft. XH: Formal analysis, table preparation, writing—review & editing. YD: Validation, writing—review & editing. KL: Formal analysis, software, validation, writing—review & editing. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that financial support was received for the research and/or publication of this article. This work was supported by the Medical Science Research Project of Hebei (Project No. 20251432). The funding bodies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no competing interests relevant to the content of this article.
References
1. Sonkin D, Thomas A, Teicher BA. Cancer treatments: past, present, and future. Cancer Genet. 2024;286–287:18–10. doi:10.1016/j.cancergen.2024.06.002
2. Loibl S, Gianni L. HER2-positive breast cancer. Lancet. 2017;389(10087):2415–2429. doi:10.1016/S0140-6736(16)32417-5
3. Xin L, Zhou S, Jiang Z, Liu M, Breast cancer Professional Committee of Chinese Society of Clinical Oncology, Breast Surgery Group of the Chinese Medical Association Surgery Branch. Current status of neoadjuvant therapy for early HER2-positive breast cancer in 118 tertiary hospitals in China. Chin J Pract Surg. 2024;44(1):98–102.
4. Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13(1):25–32. doi:10.1016/S1470-2045(11)70336-9
5. Shao Z, Pang D, Yang H, et al. Efficacy, Safety, and Tolerability of Pertuzumab, Trastuzumab, and Docetaxel for Patients With Early or Locally Advanced ERBB2-Positive Breast Cancer in Asia: the PEONY Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020;6(3):e193692. doi:10.1001/jamaoncol.2019.3692
6. van Ramshorst MS, van der Voort A, van Werkhoven ED, et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive breast cancer (TRAIN-2): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018;19(12):1630–1640. doi:10.1016/S1470-2045(18)30570-9
7. Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9):2278–2284. doi:10.1093/annonc/mdt182
8. Hurvitz SA, Martin M, Symmans WF, et al. Neoadjuvant trastuzumab, pertuzumab, and chemotherapy versus trastuzumab emtansine plus pertuzumab in patients with HER2-positive breast cancer (KRISTINE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2018;19(1):115–126. doi:10.1016/S1470-2045(17)30716-7
9. Swain SM, Ewer MS, Viale G, et al. Pertuzumab, trastuzumab, and standard anthracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive localized breast cancer (BERENICE): a Phase II, open-label, multicenter, multinational cardiac safety study. Ann Oncol. 2018;29(3):646–653. doi:10.1093/annonc/mdx773
10. Yao DS, Wang W, Chang JY, et al. Neoadjuvant pyrotinib plus nab-paclitaxel, doxorubicin, and cyclophosphamide for HER2-positive locally advanced breast cancer: a retrospective case-series study. Gland Surg. 2021;10(12):3362–3368. doi:10.21037/gs-21-770
11. Tian C, Wang M, Liu H, Liu J, Xu M, Ma L. Efficacy and safety of neoadjuvant pyrotinib plus docetaxel/liposomal doxorubicin/cyclophosphamide for HER2-positive breast cancer. Ir J Med Sci. 2023;192(3):1041–1049. doi:10.1007/s11845-022-03093-9
12. Xiang YF, Su F, Yang JR, et al. Clinical study of Pyrotinib combined with chemotherapy in neoadjuvant treatment in HER2 positive early or locally advanced breast cancer. J Lanzhou Univ Med Sci. 2022;48(7):77–81.
13. Ye G, Chen P, Liu X, et al. Short-term efficacy and safety of neoadjuvant pyrotinib plus taxanes for early HER2-positive breast cancer: a single-arm exploratory phase II trial. Gland Surg. 2024;13(3):374–382. doi:10.21037/gs-24-38
14. Li F, Liang Y, Luo M, et al. The efficacy and safety of epirubicin and cyclophosphamide combined with pyrotinib in neoadjuvant treatment for HER2-positive breast cancer: a real-world study. Front Oncol. 2023;13:1041111. doi:10.3389/fonc.2023.1041111
15. Wang W, Zhang J, Chang JY, et al. The efficacy and safety of using pyrotinib combined with capecitabine as neoadjuvant therapy in elderly patients with HER2-positive breast cancer: a single-arm prospective clinical trial. Gland Surg. 2023;12(2):208–214. doi:10.21037/gs-23-11
16. Liu Z, Wang C, Chen X, et al. Pathological response and predictive role of tumour-infiltrating lymphocytes in HER2-positive early breast cancer treated with neoadjuvant pyrotinib plus trastuzumab and chemotherapy (Panphila): a multicentre phase 2 trial. Eur J Cancer. 2022;165:157–168. doi:10.1016/j.ejca.2022.01.022
17. Liu M, Zou L, Zhang N, et al. Pathological response and metabolites’ prognostic role in HER2-positive breast cancer treated with neoadjuvant pyrotinib, trastuzumab, nab-paclitaxel, and carboplatin: a single-arm phase II trial. Breast Cancer Res. 2025;27(1):190. doi:10.1186/s13058-025-02137-z
18. Yin W, Wang Y, Wu Z, et al. Neoadjuvant Trastuzumab and Pyrotinib for Locally Advanced HER2-Positive Breast Cancer (NeoATP): primary Analysis of a Phase II Study. Clin Cancer Res. 2022;28(17):3677–3685. doi:10.1158/1078-0432.CCR-22-0446
19. Zheng XX, Zhang X, Wu J, et al. Efficacy and safety of neoadjuvant TCbH plus pyrotinib in young patients with locally advanced HER2-positive breast cancer. Chin J Gen Surg. 2021;30(11):1304–1310.
20. Ding Y, Mo W, Xie X, et al. Neoadjuvant Pyrotinib plus Trastuzumab, Docetaxel, and Carboplatin in Early or Locally Advanced Human Epidermal Receptor 2-Positive Breast Cancer in China: a Multicenter, Randomized, Double-Blind, Placebo-Controlled Phase 2 Trial. Oncol Res Treatment. 2023;46(7–8):303–311. doi:10.1159/000531492
21. Wang F, Wang Y, Xiong B, et al. Neoadjuvant pyrotinib and trastuzumab in HER2-positive breast cancer with no early response (NeoPaTHer): efficacy, safety and biomarker analysis of a prospective, multicentre, response-adapted study. Signal transduction and targeted therapy. Signal Transduction and Targeted Therapy. 2025;10(1):45. doi:10.1038/s41392-025-02138-6
22. Zhu J, Jiao D, Wang C, et al. Neoadjuvant Efficacy of Three Targeted Therapy Strategies for HER2-Positive Breast Cancer Based on the Same Chemotherapy Regimen. Cancers. 2022;14(18):4508. doi:10.3390/cancers14184508
23. Xuhong J, Qi X, Tang P, et al. Neoadjuvant Pyrotinib plus Trastuzumab and Chemotherapy for Stage I-III HER2-Positive Breast Cancer: a Phase II Clinical Trial. Oncologist. 2020;25(12):e1909–e1920. doi:10.1002/onco.13546
24. Shi Q, Qi X, Tang P, et al. A multicenter single-arm trial of neoadjuvant pyrotinib and trastuzumab plus chemotherapy for HER2-positive breast cancer. MedComm. 2023;4(6):e435. doi:10.1002/mco2.435
25. Liu L, Zhu M, Wang Y, Li M, Gu Y. Neoadjuvant pyrotinib plus trastuzumab and chemotherapy for HER2-positive breast cancer: a prospective cohort study. World J Surg Oncol. 2023;21(1):389. doi:10.1186/s12957-023-03266-5
26. Zhong X, He P, Chen J, et al. Neoadjuvant pyrotinib plus trastuzumab and nab-paclitaxel for HER2-positive early or locally advanced breast cancer: an exploratory phase II trial. Gland Surg. 2022;11(1):216–225. doi:10.21037/gs-21-911
27. Wang Y, Xu Y, Liu X, et al. The efficacy and safety of trastuzumab and albumin-bound paclitaxel with or without pyrotinib as neoadjuvant therapy for HER2-positive breast cancer: a prospective observational cohort study. Gland Surg. 2024;13(5):654–662. doi:10.21037/gs-24-81
28. Wu J, Jiang Z, Liu Z, et al. Neoadjuvant pyrotinib, trastuzumab, and docetaxel for HER2-positive breast cancer (PHEDRA): a double-blind, randomized phase 3 trial. BMC Med. 2022;20(1):498. doi:10.1186/s12916-022-02708-3
29. CSCO Breast Cancer Guidelines Working Committee. Chinese Society of Clinical Oncology (CSCO) Breast Cancer Guidelines. Beijing: People’s Medical Publishing House; 2023.
30. Pan H, Ren Y, Zha M, et al. De-escalated neoadjuvant nab-paclitaxel combined with pyrotinib and trastuzumab in intrinsic HER2-enriched breast cancer (NJMU-BC01): a multicenter, single-arm, phase 2 trial. EClinicalMedicine. 2025;86:103376. doi:10.1016/j.eclinm.2025.103376
31. Niu N, Qiu F, Xu Q, et al. A multicentre single arm phase 2 trial of neoadjuvant pyrotinib and letrozole plus dalpiciclib for triple-positive breast cancer. Nat Commun. 2022;13(1):7043. doi:10.1038/s41467-022-34838-w
32. Huo S, Xue J, Wang S, et al. A pilot trial of neoadjuvant pyrotinib plus trastuzumab, dalpiciclib, and letrozole for triple-positive breast cancer. MedComm. 2024;5(3):e505. doi:10.1002/mco2.505
33. Goel S, Wang Q, watt AC, et al. Overcoming Therapeutic Resistance in HER2-Positive Breast Cancers with CDK4/6 Inhibitors. Cancer Cell. 2016;29(3):255–269. doi:10.1016/j.ccell.2016.02.006
34. Sinclair WD, Cui X. The Effects of HER2 on CDK4/6 Activity in Breast Cancer. Clin Breast Cancer. 2022;22(3):e278–e285. doi:10.1016/j.clbc.2021.08.007
35. Lee RJ, Albanese C, Fu M, et al. Cyclin D1 is required for transformation by activated Neu and is induced through an E2F-dependent signaling pathway. Mol Cell Biol. 2000;20(2):672–683. doi:10.1128/MCB.20.2.672-683.2000
36. O’Sullivan CC, Suman VJ, Goetz MP. The emerging role of CDK4/6i in HER2-positive breast cancer. Ther Adv Med Oncol. 2019;11:1758835919887665. doi:10.1177/1758835919887665
37. Xiao Z, Chen F, Liao L, et al. Efficacy and safety of neoadjuvant treatment of trastuzumab and pyrotinib plus dalpiciclib in HR-negative/HER2-positive breast cancer: an exploratory, open-label phase II study. Int J Surg. 2025;2025:1.
38. Yang C, Xu Y, Lin Z, et al. Spatial discovery of pyrotinib overcoming HER2-positive breast cancer resistance by breaking fibroblast-induced immune barriers. Drug Resistance Update. 2025;82:101261. doi:10.1016/j.drup.2025.101261
39. Niu N, Xue J, Chen G, et al. Neoadjuvant ARX788 plus pyrotinib versus trastuzumab, pertuzumab, docetaxel and carboplatin for HER2-positive breast cancer: a randomised phase 2b trial. Nat Commun. 2025;16(1):6036. doi:10.1038/s41467-025-61213-2
40. Li JJ, Wang ZH, Chen L, et al. Efficacy and safety of neoadjuvant SHR-A1811 with or without pyrotinib in women with locally advanced or early HER2-positive breast cancer: a randomized, open-label, phase II trial. Ann Oncol. 2025;36(6):651–659. doi:10.1016/j.annonc.2025.02.011
41. Li YW, Dai LJ, Wu XR, et al. Molecular Characterization and Classification of HER2-Positive Breast Cancer Inform Tailored Therapeutic Strategies. Cancer Res. 2024;84(21):3669–3683. doi:10.1158/0008-5472.CAN-23-4066
42. Wilcock DM, Zhao J, Gulbahce HE. Resolving HER2 status in breast carcinoma patients with complete deletion of CEP17 in fluorescence in-situ hybridization assays. Cancer Genet. 2025;296–297:196–199. doi:10.1016/j.cancergen.2025.07.015
43. Liu H, Wang P. CRISPR screening and cell line IC50 data reveal novel key genes for trametinib resistance. Clin Exp Med. 2024;25(1):21. doi:10.1007/s10238-024-01538-2
44. Gong C, Xia Y, Zhu Y, et al. Preclinical study and phase 2 trial of neoadjuvant pyrotinib combined with chemotherapy in luminal/HER2-low breast cancer: PILHLE-001 study. Cell Rep Med. 2024;5(11):101807. doi:10.1016/j.xcrm.2024.101807
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Choice of Neoadjuvant Chemotherapy for HER2-Negative Breast Cancer: Clinical Insights
Lucas MW, Kelly CM
Cancer Management and Research 2022, 14:2493-2506
Published Date: 17 August 2022
Pyrotinib for Elderly Patients with Advanced HER2-Positive Breast Cancer
Li Y, Ma X, Zhao Z, Li L, Gao C, Liu D, Li B, Zhao B
Breast Cancer: Targets and Therapy 2022, 14:405-415
Published Date: 6 December 2022
Real-World Outcome and Prognostic Factors Among HER2-Positive Metastatic Breast Cancer Patients Receiving Pyrotinib-Based Therapy: A Multicenter Retrospective Analysis
Liu J, Sun X, Du Q, Yao J, Dai M, Cheng Q, Xu H, Li Y, Liu X, Zhang M, Zhou Y, Yang Y
Breast Cancer: Targets and Therapy 2022, 14:491-504
Published Date: 21 December 2022
Efficacy and Safety of Neoadjuvant Stereotactic Body Radiotherapy (SBRT) Combined with Chemoimmunotherapy in Locally Advanced Breast Cancer: A Single-Center, Retrospective Pilot Study
Zhai M, Bi J, Ke Z, Hu M, Pi G, Li Y, He H, Li Y, Zheng H, Wu X, Verma V, Shao J, Han G
Breast Cancer: Targets and Therapy 2026, 18:577469
Published Date: 7 March 2026
Inflammatory and Nutritional Biomarkers Predict Response to Neoadjuvant Dual Anti-HER2 Therapy in HER2-Positive Breast Cancer: A Retrospective Cohort Study
Şahinli H, Uyar GC, Yeşilbaş E
Cancer Management and Research 2026, 18:598948
Published Date: 16 April 2026