Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Incidence and Risk Factors for Progression from Pre-COPD to COPD: A Systematic Review and Meta‑analysis
Authors Qiao L ![]() , Wu X, Chen G, Tang H, Shen H
, Wu X, Chen G, Tang H, Shen H
Received 13 September 2025
Accepted for publication 29 January 2026
Published 13 February 2026 Volume 2026:21 566518
DOI https://doi.org/10.2147/COPD.S566518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Lili Qiao,1,* Xiucen Wu,2,* Guihua Chen,3 Huan Tang,1 HuaPeng Shen1
1Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Anesthesiology, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 3Department of Nursing, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guihua Chen, Department of Nursing, The Second Affiliated Hospital of Chongqing Medical University, 288 Tianwen Avenue, Nanan District, Chongqing, 401336, People’s Republic of China, Tel +8613637889425, Email [email protected]
Objective: Pre-chronic obstructive pulmonary disease (Pre-COPD) refers to individuals who do not meet traditional diagnostic criteria for COPD but already show respiratory symptoms, abnormal lung function, or imaging changes. The purpose of this study was to complete a systematic review and meta‑analysis of the incidence and risk factors for progression from pre‑COPD to COPD.
Methods: We searched ten databases through December 31, 2024. The Newcastle–Ottawa Scale (NOS) was applied to assess the methodological quality of the eligible studies. We extracted incidence to quantify progression from pre-COPD to COPD and odds ratios (ORs) and hazard ratios (HRs) with their 95% confidence intervals (CIs) to identify associated risk factors. Effect sizes were pooled using fixed-effects and random-effects models.
Results: Among 5289 articles, 21 were eligible, and 13 reported incidence. The pooled incidence of progression from pre-COPD to COPD was 20% (n = 13, 95% CI 15– 26%). We identified five statistically significant factors linked to clinical development in pre-COPD: preserved ratio impaired spirometry (PRISm) (ORs=2.92, 95% CI 1.79– 4.74), age (ORs=1.09, 95% CI 1.03– 1.15), smoking history (ORs=4.08, 95% CI 2.14– 7.18, HRs=2.21, 95% CI 1.59– 3.07), non-obstructive chronic bronchitis (NOCB) (ORs=2.07, 95% CI 1.32– 3.24, HRs=2.46, 95% CI 1.61– 3.75), and asthma (ORs=2.50, 95% CI 1.93– 3.24).
Conclusion: This meta-analysis indicates a high incidence of progression from pre-COPD to COPD. Moreover, age, smoking history, NOCB, PRISm, and asthma were significantly associated with an increased risk of clinical progression in individuals with pre-COPD. Integrating these risk factors into clinical risk-stratification tools and follow-up strategies may help clinicians identify high-risk individuals with pre-COPD, facilitating enhanced surveillance, targeted smoking cessation interventions, optimized asthma management, and other preventive interventions to delay or prevent COPD onset.
Keywords: pre-COPD, chronic obstructive pulmonary disease, COPD, risk factors, incidence, meta--analysis
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is the third most common cause of death worldwide, and it represents a significant global health challenge, with high rates of both morbidity and mortality.1,2 As awareness of disease prevention and early intervention grows, numerous studies indicate that ultra-early intervention may enhance the long-term prognosis for COPD patients. In recent years, multiple cohort studies have demonstrated that lung function indices alone are insufficient to define COPD completely; Instead, risk factor exposure, respiratory symptoms, and structural alterations, as evidenced by imaging (CT), should also be considered essential components of its diagnostic framework.3–5 In this context, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2022 proposed the concept of pre-COPD (pre-chronic obstructive pulmonary disease) for the first time.6 It refers to individuals exhibiting respiratory symptoms, structural lung abnormalities, or physiological dysfunctions of the respiratory system, who do not satisfy the diagnostic criteria for airflow limitation.2,7
Pre-COPD includes various clinical subgroups, such as preserved ratio impaired spirometry (PRISm), non-obstructive chronic bronchitis, emphysema, diminished diffusion capacity (DLCO), and a rapidly declining forced expiratory volume in one second (FEV1).7 Epidemiologic data show that the estimated prevalence of pre-COPD in the population ranges from 7.2% to 22.3%,8,9 with regional variations in prevalence, and that a significant majority of patients are at risk of progressing to COPD over time. The large international COPDGene and SPIROMICS cohorts have demonstrated that approximately 40–50% of the pre‑COPD population exhibit symptom profiles similar to those of mild COPD, and these include emphysema, airway collapse, airway wall thickening, and elevated airway mucin levels.10,11 Moreover, over 23.5% of persons with pre-COPD demonstrate diminished quality of life and exercise capacity, and 54.1% display one or more respiratory-related functional deficits.10 An increasing volume of research indicates that pathological processes, including lung parenchymal injury, structural alterations in small airways, and mucus hypersecretion, may already manifest in the pre-COPD stage, subsequently facilitating airway remodeling and irreversible airflow limitation.12–14 Studies indicate that by the time extensive airway injury fulfills the diagnostic criteria for established COPD, up to 50% of small airways may already have been destroyed.15 The biological basis of progression from pre-COPD may involve multiple mechanisms, such as oxidative-stress-induced epithelial injury and the initiation of epithelial-mesenchymal transition (EMT), which in turn lead to airway wall thickening, scar formation, and progressive small airway narrowing or obliteration.16 Research has found that features of EMT observed in patients with established COPD are also present in smokers who are at the pre-COPD stage.17 Additionally, genetic susceptibility quantified by polygenic risk scores and early immune programming is thought to partially account for the heterogeneity in the risk of disease progression.18,19
While initial studies have elucidated the clinical characteristics and progression rate of Pre-COPD, variations in study design, duration of follow-up, and testing methodologies have led to significant heterogeneity in reported findings, precluding the formation of a unified and systematic body of evidence. Early screening and intervention for pre-COPD, a critical high-risk group for COPD development, can delay or prevent the onset of COPD. This will reduce the disease burden and optimize the allocation of healthcare resources. This work consolidates existing cohort data by systematic review and meta-analysis to estimate the incidence of pre-COPD progression to COPD and to summarize its principal risk factors, aiming to establish a scientific foundation for pre-COPD preventive and treatment strategies.
Materials and Methods
This systematic review was registered with PROSPERO (CRD42025637741). We utilized the revised criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 (PRISMA 2020) for our research.20
Data Sources and Search Strategy
We performed a comprehensive literature search throughout PubMed, Web of Science, Embase, OVID, the Cochrane Library, ProQuest, CNKI, Wan Fang Database, VIP Database, and the Chinese Biomedical Literature Database from their establishment until December 31, 2024. We first developed a search strategy for PubMed and simultaneously searched the other databases with similar terms. We used the following Medical Subject Headings terms and free words: (“Pre-COPD” OR “pre-chronic obstructive pulmonary disease” OR “early COPD” OR “early chronic obstructive pulmonary disease*” OR “early chronic pulmonary disease” OR “early chronic obstructive lung disease*”) AND (“risk*” OR “risk factor” OR “influencing factor*” OR “predictive factor*” OR “predictor*” OR “predict factor*” OR “influence factor*” OR “influential factor*” OR “affecting factors” OR “correlation factor”). Reference lists from identified studies and relevant review articles were also searched for studies eligible for inclusion.
Study Selection
The inclusion criteria were as follows; 1) were observational in design, including retrospective and prospective studies; 2) the study population comprised individuals presenting with respiratory symptoms, structural lung lesions, or abnormal pulmonary function who did not meet the diagnostic criteria for airflow obstruction;6 3) the primary outcome of interest was the development of chronic obstructive pulmonary disease (COPD) during follow-up. These outcomes should align with recognized diagnostic criteria or be diagnosed by a physician; 4) exposure factors were delineated as distinct elements or conditions recognized in the research as potential contributors to heightened progression risk.
Studies were excluded for the following reasons: 1) studies did not report risk estimates, including relative risks (RRs), hazard ratios (HRs), odds ratios (ORs), and 95% confidence intervals (CIs) or raw data in an appropriate format to calculate an effect size; 2) commentaries, conference abstracts, and reviews; 3) the language of the publication was other than English or Chinese. Two researchers (QLL and WXC) independently screened the titles and abstracts of eligible articles identified using the aforementioned search strategy. After duplicate articles were removed from the list of eligible articles, full texts of the remaining articles were reviewed to determine whether they met the predetermined inclusion criteria. Any disagreements were resolved through discussion or, if necessary, consultation with a third evaluator (TH).
Data Extraction
Two independent investigators (QLL and WXC) extracted data from the included studies. Disputes were settled through dialogue or by a third investigator where required. All extracted data were preserved in a uniform Microsoft Excel spreadsheet format. The recorded information includes the first author’s name, publication year, country, setting, design, age, sample size, gender, pre-COPD follow-up population, follow-up durations, COPD incidence, and clinical risk factors for pre-COPD progression.
Quality Assessment
Two researchers (QLL and WXC) independently assessed the quality of the final included literature using the Newcastle-Ottawa Scale(NOS),21 which consists of eight items. A score of ≥6 indicates moderate to high quality of the literature.22 The detailed Newcastle–Ottawa Scale quality assessment results are provided in Additional Table 1.
Statistical Analysis
All analyses were conducted utilizing the comprehensive meta-analysis program, Stata 18. A random-effects model was employed to aggregate the incidence of progression from pre-COPD to COPD, along with the associated 95% confidence interval (CI). Secondly, we employed meta-analysis to investigate the risk factors associated with pre-COPD development using adjusted effect estimates (ORs or HRs). We performed a systematic review of all individual yet relevant factors. The adjusted odds ratios (ORs), hazard ratios (HRs), and their respective 95% confidence intervals (CIs) were aggregated utilizing fixed-effects or random-effects models. A two-tailed p-value less than 0.05 was deemed significant. If relevant factors were consistently recorded, they were aggregated in a meta-analysis. The I-square test statistic (I2) was utilized to evaluate study heterogeneity. Medium or high heterogeneity was deemed present when I2 exceeded 50% or 75%, and p-values were below 0.05, respectively.23 Random models were adopted to synthesize the risk effects if heterogeneity was medium or high. Funnel plot and Egger’s test were used to evaluate the publication bias of research results.
To explore potential sources of heterogeneity in incidence, we performed subgroup and sensitivity analyses on the included studies. The incidence of progression from pre-COPD to COPD, with corresponding 95% confidence intervals, was calculated for subgroups according to country (Western vs Eastern), follow-up duration (< 5 years vs ≥ 5 years), publication year (Pre-2022 vs Post-2022), study design (prospective cohort vs retrospective cohort), and pre-COPD sample size (< 100 vs 100–500 vs ≥ 500). Meta-regression was not possible because there were fewer than 10 studies for each covariate.
Results
Search results
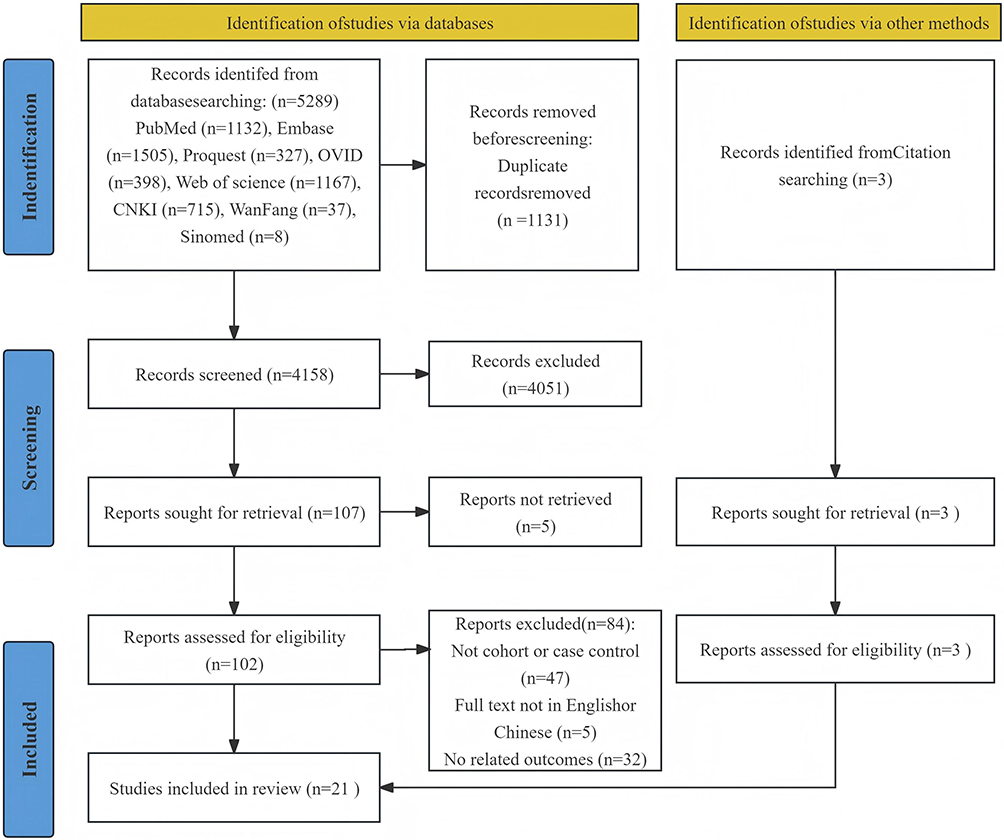
Overall, 5,289 reports were identified through PubMed, Web of Science, EMBASE, Ovid, the Cochrane Library, ProQuest, CNKI, Wanfang, VIP, and the China Biomedical Literature Database. After excluding 1,131 duplicate records, the remaining 4,158 studies were screened by title and abstract, excluding 4,051 irrelevant records. Five additional studies were excluded due to unavailable full texts, leaving 102 reports for full-text assessment. Of these reports, 84 were excluded for the following reasons: non-cohort design (n = 47), non-English/Chinese publication (n = 5), and no relevant outcome data on COPD incidence and/or risk factors (n = 32). We additionally identified three studies after searching the reference lists of the included studies, which expanded our list of eligible studies to 21 (Figure 1). Given the considerable heterogeneity in terminology and at-risk populations across studies, the operational definitions of pre-COPD-related at-risk groups in each included study are summarised in Additional Table 3.
 |
Characteristics of the Included Studies
The characteristics of the included studies are shown in Table 1. The 21 studies included 17 prospective cohort studies3,24–39 and 4 retrospective cohort studies.40–43 The studies were from eight countries (the US, the UK, Japan, the Republic of Korea, Croatia, Australia, Denmark, and China). Of them, the majority took place in the US (n = 9) and the Republic of Korea (n = 3), followed by China (n = 2), the UK (n = 2), Denmark (n = 2), Japan (n = 1), Australia (n=1), and Croatia (n = 1). The majority (71.4%) were multicenter studies. These studies involved a total of 417,066 participants. The methodological quality of the included research is assessed by the NOS. All included studies achieved Newcastle Ottawa Scale scores of 6 and above, indicating moderate-to-high quality.
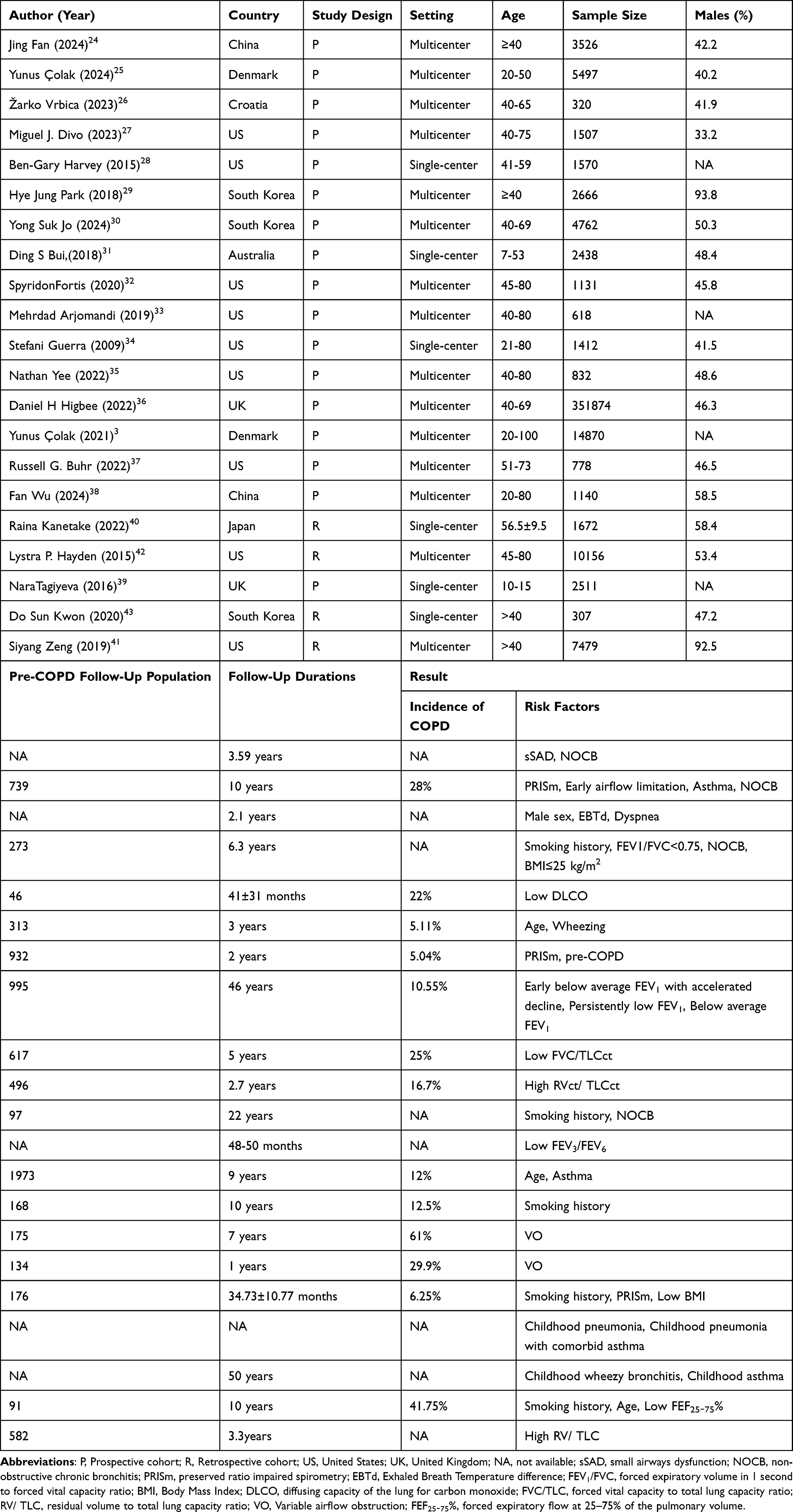 |
Table 1 Detailed Characteristics of Included Studies |
Incidence of Progression of Pre-COPD to COPD
In the 13 studies available for the meta-analysis,3,25,28–33,36–38,40,43 the incidence of progression from pre-COPD to COPD ranged from 5.0% to 61%. The included studies observed considerable heterogeneity (I2 = 97.7%, p < 0.001). Therefore, using the random effects model, the results demonstrated that the pooled incidence of progression from pre-COPD to COPD was 20% (95% CI 15–26%) (Figure 2).
 |
Figure 2 Forest plot of the incidence pre-COPD progressing to COPD3,25,28–33,36–38,40,43 (n = 13, random effect). |
Subgroup Analysis and Sensitivity Analysis
Subgroup analysis was used to investigate heterogeneity in the study. Subgroup analyses were performed according to country, follow-up duration, year of publication, study design, and sample size of pre-COPD subjects (Table 2). Subgroup analyses suggested that follow-up duration (p = 0.006), study design (p = 0.003), and sample size of the pre-COPD cohort (p = 0.004) may influence the reported estimates of progression incidence from pre-COPD to COPD across studies. The subgroup meta-analysis showed the pooled incidence proportions were 27% (95% CI 18–35%) in studies with a follow-up duration ≥5 years, and 13% (95% CI 7–18%) in those with a follow-up duration <5 years. In the study design subgroup, the pooled incidence was 20% (95% CI 14–26%) with prospective cohort studies and 10% (95% CI 7–14%) with retrospective cohort studies. The subgroup analysis of pre-COPD sample size revealed that the pooled incidence of progression to COPD was the highest in studies with ≤ 100 subjects (33%, 95% CI 26–41%), higher than that in studies with 100–500 subjects (22%, 95% CI 10–33%), and the lowest in studies with ≥ 500 subjects (16%, 95% CI 9–23%).
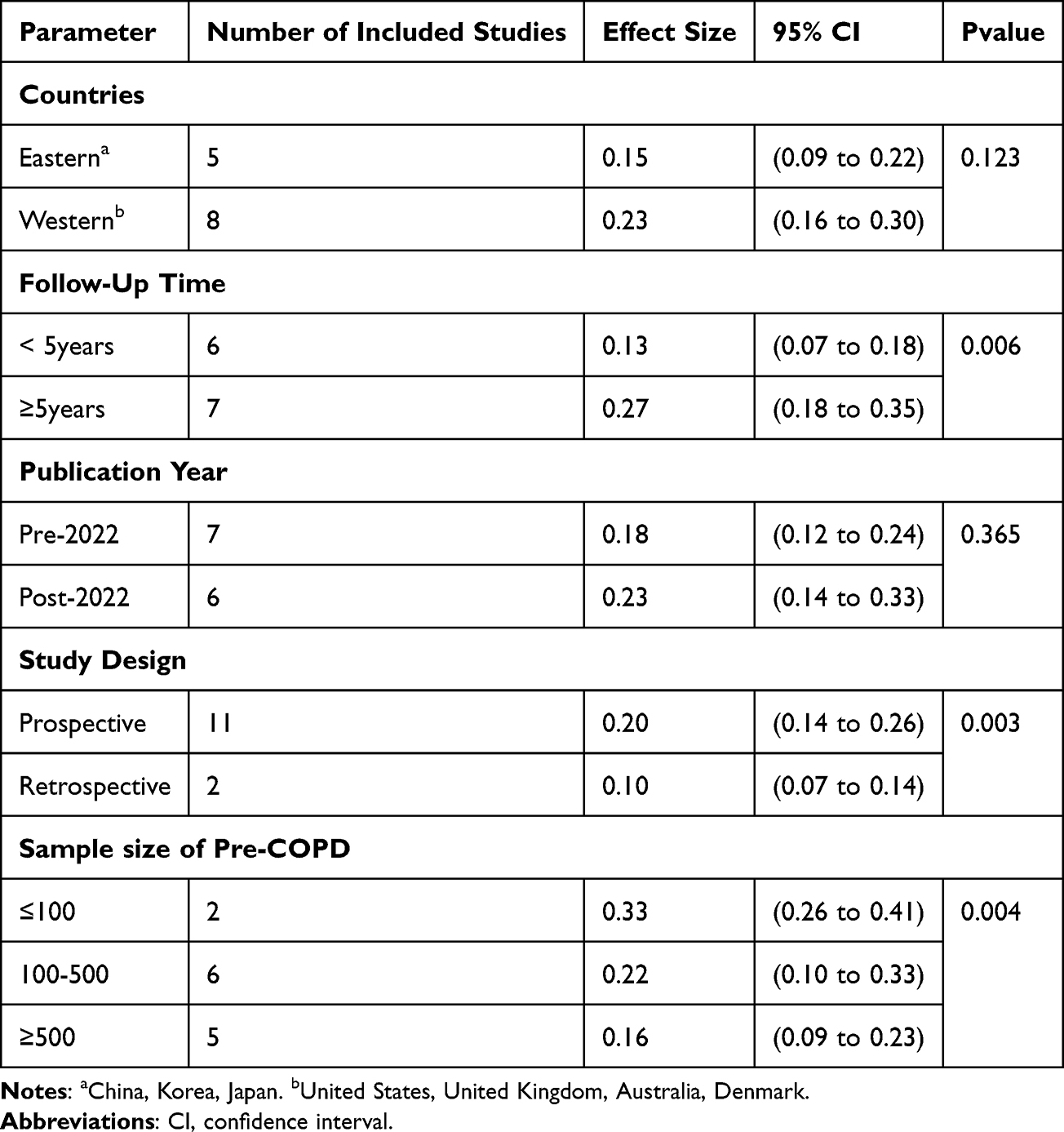 |
Table 2 Subgroup Analysis of the Incidence of Progression From Pre-COPD to COPD3,25,28–33,36–38,40,43 (n=13) |
Sensitivity analysis was performed by eliminating individual studies one at a time. The pooled incidence of progression from pre-COPD to COPD fluctuated between 17% and 22%, with little difference between the obtained results and the overall incidence, implying that our findings were stable The details of the sensitivity analysis are presented in Additional Table 2.
Publication Bias
We used the funnel chart and Egger’s test to test the publication bias of the pooled incidence of progression from pre-COPD to COPD. Upon visual inspection, the funnel plot revealed significant asymmetry (Additional Figure 1). Egger’s test (P = 0.013) indicated the presence of publication bias.
Risk Factors for Progression from Pre-COPD to COPD
We categorized these factors into three subcategories, namely demographic and behavioral characteristics, clinical symptoms and medical history, and physiological and imaging indicators, as per previous research (Table 3).44 We pooled ORs and HRs from multivariate analyses to assess the risk factors associated with the clinical progression of pre‑COPD. Among the investigated variables, five factors were found to be statistically significant predictors of progression: age, smoking history, NOCB, PRISm, and asthma. Based on this, we combined ORs to obtain the summary ORs and their 95% CIs for the clinical progression factors of pre-COPD (Table 4). Similarly, we did the same analysis for HRs (Table 5). Due to the limited number of studies, funnel plots could not be estimated. Furthermore, we conducted descriptive analyses for risk factors that could not be quantitatively synthesized due to substantial differences in measurement methods, effect size units, definitions, or reporting formats. The remaining risk factors are detailed in Table 3.
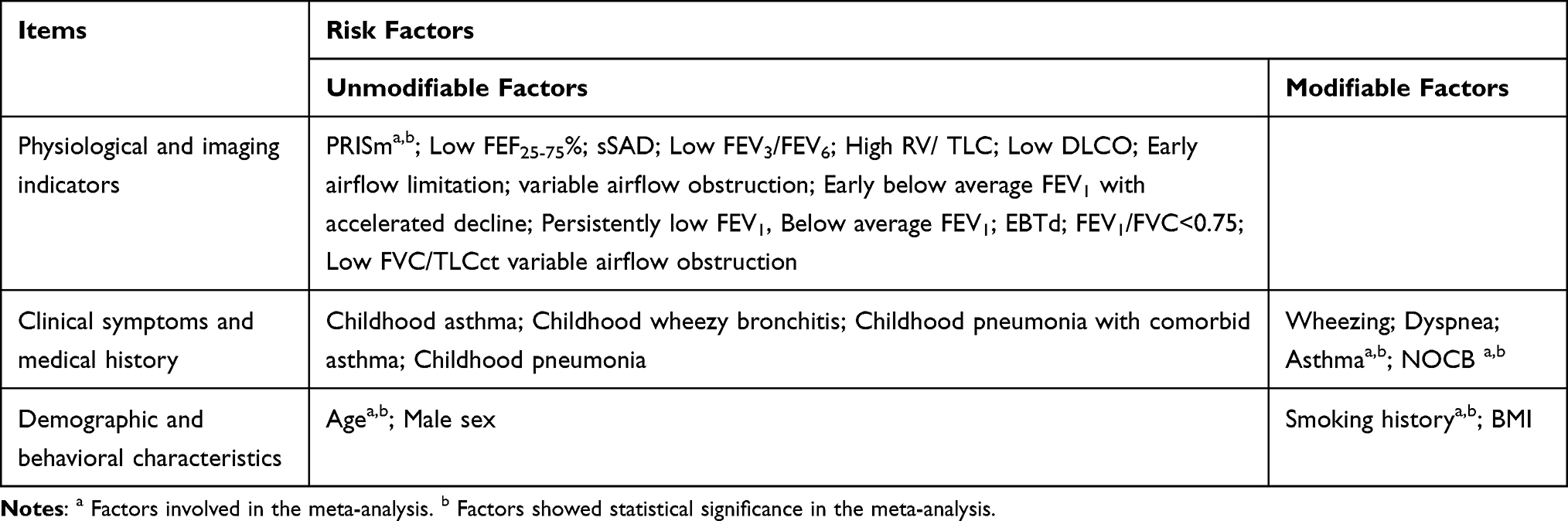 |
Table 3 Potential Risk Factors for Progression from Pre-COPD to COPD |
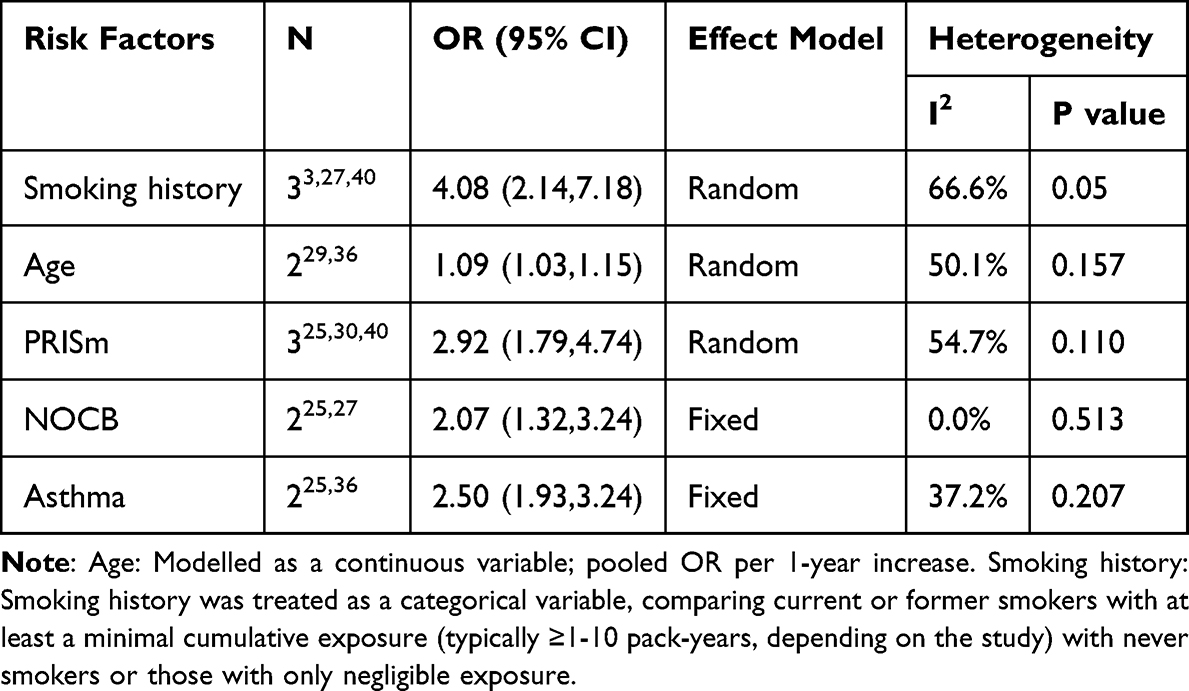 |
Table 4 Meta-Analysis Results of OR-Based Progression of Pre-COPD to Major Risk Factors for COPD |
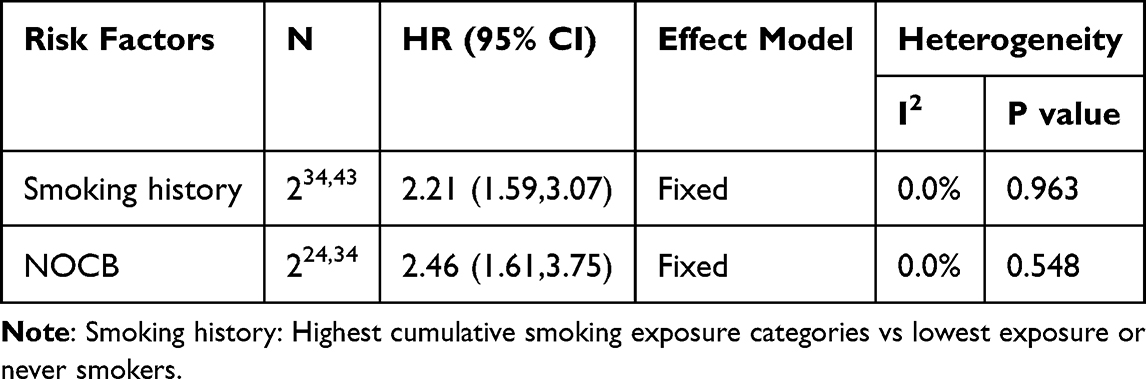 |
Table 5 Results of Meta-Analysis of HR-Based Progression of Pre-COPD to Major Risk Factors for COPD |
Demographic and Behavioral Characteristics
Demographic and behavioural attributes encompassed age, body mass index (BMI), and smoking history. Three studies assessed the correlation between age and the progression of pre-COPD to COPD. In the two studies included in the meta-analysis, age was analysed as a continuous variable. The pooled analysis showed that each 1-year increase in age was associated with a higher risk of progression from pre-COPD to COPD (ORs = 1.09, 95% CI 1.03–1.15, I2 = 50.1%, P = 0.157).29,36 Furthermore, one study modelled BMI as a continuous variable and found that lower BMI was associated with an increased risk of clinical progression from pre-COPD (per 1 kg/m2 increase: OR = 0.88, 95% CI 0.79–0.98, P = 0.015).40 In contrast, another study dichotomised BMI at 25 kg/m2 and reported that participants with BMI≤25 kg/m2 had a markedly increased progression risk (OR = 2.40, 95% CI 1.43–4.03, P = 0.0009).27 Given the different BMI definitions in the two studies, we did not calculate a pooled odds ratio. In the meta-analysis, three cohort studies reported odds ratios for different levels of smoking exposure. In these studies, smoking history was defined as current or former smoking with at least a minimal cumulative exposure in pack-years. It was compared with never smoking or only negligible exposure. The pooled analysis indicated that individuals with a smoking history had a significantly increased risk of progression from pre-COPD to COPD (ORs = 4.08, 95% CI 2.14–7.18, I2 = 66.6%, P = 0.05).3,27,40 Based on two cohort studies reporting hazard ratios, the meta-analysis further showed that, compared with never smokers or those with very low cumulative smoking exposure, long-term smokers in the highest cumulative pack-year categories had approximately a twofold higher risk of developing COPD (HRs = 2.21, 95% CI 1.59–3.07, I2 = 0%, P = 0.963).34,43 Due to the limited number of studies, funnel plots could not be constructed.
Physiological and Imaging Indicators
Physiological and imaging indices included PRISm, reversible airflow obstruction (VO), RV/TLC ratio, small airway function indices (Low FEV3/FEV6, sSAD, low FEF25-75%), early airflow limitation, and FEV1/FVC < 0.75. A meta-analysis of three studies indicated that PRISm correlates with a heightened risk of COPD (HRs = 2.92, 95% CI 1.79–4.74, I2 = 54.7%, P = 0.110).25,30,40 Heterogeneity across the studies was moderate. Due to the limited number of studies, funnel plots could not be estimated. Two studies showed an association between reversible airflow obstruction and future risk of COPD (HR = 6.2, 95% CI 4.6–8.3, P < 0.001, OR = 3.87, 95% CI 2.46–6.39, P < 0.001).37,38 Due to the difference in the estimate effect unit, the pooled effect could not be evaluated. In addition, two investigations assessed the correlation between the RV/TLC ratio and COPD. The findings indicated that patients exhibiting a high RV/TLC ratio possessed a markedly elevated risk of getting COPD (OR = 5.689, 95% CI 2.446–13.228, P<0.001, OR = 1.30, 95% CI 1.03–1.65, P = 0.027).33,41 Nonetheless, data could not be pooled due to discrepancies in measurement techniques, such as computed tomography (CT) versus volumetric plethysmography. Three cohort studies reported that Low FEV3/FEV6 (HR = 2.11, 95% CI 1.48–3.03, P < 0.001),35 small‑airway dysfunction (sSAD) (HR = 2.74, 95% CI 2.07–3.61, P < 0.0001),24 and reduced FEF25–75% (HR = 3.31, 95% CI 1.65–6.63, P < 0.001) were each associated with future risk of COPD occurrence.43 Due to differences in indicator definitions and measurement methods, quantitative meta-analysis was not possible. However, all results uniformly underscore that small‑airway impairment substantially elevates the risk of COPD occurrence. Notably, a large-scale cohort study conducted in the United States identified a baseline FEV1/FVC ratio of <0.75 as the strongest predictor of future airflow limitation (OR = 15.32, 95% CI 9.14–25.69, P<0.0001).27 Similarly, a study from Denmark demonstrated a significant association between early airflow limitation and an increased risk of developing COPD (OR = 21.8, 95% CI 14.8–32.0, P < 0.0001).25 Data could not be aggregated due to substantive differences in definitional criteria, measurement methods.
Clinical Symptoms and Medical History
Clinical symptoms and past medical history include NOCB, asthma, and respiratory symptoms (wheezing, dyspnea). Among the four studies analysed, two reported odds ratios (OR),25,27 and the other two supplied risk ratios (HR) were employed to assess the association between non‑obstructive chronic bronchitis and the probability of developing COPD.24,34 The meta-analysis demonstrated that non‑obstructive chronic bronchitis significantly increases the likelihood of developing COPD (ORs = 2.07, 95% CI 1.32–3.24, I2 = 0.0%, P = 0.513, HRs = 2.46, 95% CI 1.61–3.75, I2 = 0.0%, P = 0.548). In two studies, asthma was associated with the future occurrence of COPD (ORs = 2.50, 95% CI 1.93–3.24, I2 = 37.2%, P = 0.207).25,36 Heterogeneity across the studies was low. In addition, two studies separately reported associations of wheezing29 and dyspnea26 with increased future COPD risk, yielding ORs of 4.56 (95% CI 1.08–19.35, P = 0.04) and 1.69 (95% CI 1.14–2.51), respectively. Quantitative synthesis was not performed due to heterogeneity in symptom types and assessment instruments. Nonetheless, both suggest that respiratory symptoms may be an essential clinical signal for the progression of pre-COPD. More prospective studies are still needed to verify this in the future.
Discussion
Our study presents a meta-analysis examining the incidence of progression from pre-COPD to COPD and its associated risk factors. The analysis revealed a pooled incidence of 20% for progression from pre-COPD to COPD. We discovered five statistically significant indicators linked to clinical development in pre-COPD: age, smoking history, NOCB, PRISm, and asthma. Understanding prognostic factors for pre-COPD clinical progression, including readily accessible objective indicators, is essential for formulating personalized therapeutic strategies for this chronic progressive disease. It can furnish patients and their families with critical information to facilitate informed decision-making.
This study summarizes all available data from population‑based analyses. It is worth noting that pre‑COPD, as a clinical state that still lacks a precise definition, exhibits diverse clinical phenotypes.7 Moreover, the included studies varied in design, sample origin, and geographical distribution, resulting in inevitable heterogeneity in results. The meta-analysis revealed that the aggregated incidence of progression from pre-COPD to COPD was 20%. Studies with more than five years of follow‑up reported a significantly higher incidence in the subgroup analysis by follow-up duration. This may indicate the temporal aspect of clinical progression in pre-COPD, underscoring the need for healthcare professionals to prioritize long-term surveillance of high-risk individuals. The Subgroup analysis stratified by study design demonstrated that the incidence rate was higher in prospective cohort studies (20%) than in retrospective studies (10%). This observation likely reflects standardized data‐collection methods in prospective studies, which are more effective in thoroughly documenting disease progression. The outcomes of retrospective studies were mainly derived from medical records and related databases. They were subject to the common limitations of their retrospective design, including selection bias, misclassification bias, and residual confounding.45 Subgroup analyses indicate that the incidence of progression from pre-COPD to COPD was elevated in studies with pre-COPD sample sizes of ≤ 100. This may be attributed to the propensity of small-sample studies to recruit high-risk populations or to exhibit selective bias, potentially resulting in an overestimation of incidence.
The funnel-plot asymmetry and Egger’s test indicate potential publication bias, which may arise from substantial heterogeneity in pre-COPD study criteria, hindering the publication of negative findings with low incidence rates. Additionally, there may be a preferential publication of novel data on clinical progression among individuals at high risk for COPD.
Currently, the precise pathological mechanisms underlying the progression from pre-COPD to COPD remain unclear. However, certain factors, such as advanced age and smoking, have been reported to be involved in the pathogenesis of COPD. Research has demonstrated that FEV1 and FVC decrease with age in healthy adults; however, the decrease in FEV1 is more significant.46 This may be attributed to the fact that lung function diminishes as we age, which results from changes in the shape of the thorax, decreased strength of the respiratory muscles and diaphragm, and reduced lung elasticity and retraction.47 The COPDGene study demonstrated that current smokers experienced a markedly worse decrease in lung function over a 10-year follow-up compared to persons who had previously smoked but had ceased.48 The biological effect of cigarette smoking on the development of COPD remains unclear. However, cigarette smoke components, such as nicotine, hydrocarbons, and carbon monoxide, are known to trigger chronic airway inflammation, oxidative stress, and a protease-antiprotease imbalance via multiple pathways, leading to alveolar destruction, airway remodeling, and a progressive decline in lung function.49,50
In this systematic review and meta-analysis, we evaluated PRISm, high RV/TLC ratio, reversible airflow obstruction (VO), indicators of small airway function (low FEV3/FEV6, sSAD, low FEF25-75%), early airflow limitation, FEV1/FVC < 0.75. Our meta-analysis revealed that PRISm is a significant risk factor for the progression to COPD. PRISm is a spirometric phenotype characterized by abnormal non-obstructive pulmonary function, exhibiting a normal forced expiratory volume in one second to forced vital capacity ratio (FEV1/FVC ≥0.7) but presenting a reduced forced expiratory volume in one second (FEV1%pred) or forced vital capacity (FVC%pred) of less than 80%.51 Despite not fulfilling the diagnostic criteria for COPD, prior research indicates that 22.2% of patients with PRISm progressed to GOLD grade 0 and 25% to GOLD grades 1 to 4 at a 5-year follow-up,52 exhibiting an elevated risk of all-cause mortality and respiratory diseases compared to individuals with normal lung function.52–57 Furthermore, Helena Backman et al58 discovered that PRISm patients who had never smoked had a comparable 10-year risk of progression to COPD (OR=3.66) to that of current smokers (OR=4.07) and former smokers (OR=1.52). Therefore, PRISm should be emphasized as an early screening indicator to actively monitor disease progression. Recent research indicates that the advancement of PRISm to COPD can be mitigated and mortality can be diminished by enhancing cardiovascular health indicators (eg, Life’s Essential Eight score) and managing smoking and obesity.59 The RV/TLC ratio can be measured using various methods, as is widely recognised. However, the absence of a uniform measurement method renders it impossible to derive quantitative summary results for RV/TLC. In our study, quantitative synthesis was precluded by heterogeneous effect-size metrics employed to assess reversible airflow obstruction (VO) across the included investigations. However, two high-quality cohort studies confirmed that VO was significantly associated with an increased risk of incident COPD (HR = 6.20, 95% CI 4.60–8.30, P < 0.001; OR = 3.87, 95% CI 2.46–6.39).37,38 Small airway dysfunction may be present in the pre-COPD stage. Due to the absence of overt symptoms initially, this illness is frequently neglected. Extensive cohort studies, including COPDGene and SPIROMICS, have demonstrated that small airway dysfunction, exemplified by diminished FEF25%–75% projected values, is significantly correlated with the severity of COPD and the deterioration of lung function.60,61 In this meta-analysis, quantitative summary results could not be obtained due to the different small airway function assessment metrics used in the included studies. The current GOLD recommendations define airflow obstruction in COPD using a fixed FEV1/FVC ratio of <0.7. However, this threshold may inaccurately assess the risk of early or moderate obstruction in both younger and older demographics.62,63 The differing FEV1/FVC criteria utilized in the two studies included in the meta-analysis (eg, early airflow limitation versus FEV1/FVC < 0.75) precluded the quantitative aggregation of their risk estimations.
Prior meta-analyses indicate that individuals with non-obstructive chronic bronchitis exhibit an elevated risk of progressing to chronic obstructive pulmonary disease (COPD), all-cause mortality, and respiratory illnesses.64 In agreement with previously published studies, the meta-analysis in the present study further confirmed that the disease was significantly associated with the risk of developing COPD in the future. Furthermore, there is a correlation between asthma and COPD.65,66 Our findings confirm that asthma is associated with the risk of developing COPD in the future. Enhancing management for this high-risk cohort may diminish the likelihood of future COPD and elevate quality of life. Nevertheless, additional studies are necessary to validate the efficacy of this COPD prevention strategy. For instance, the prevention of asthma should commence in childhood or even earlier,67 and proactive intervention strategies, such as the promotion of immunisation, maternal smoking cessation, and adolescent smoking prevention, can effectively reduce the risk of COPD in the future. Chronic cough and sputum symptoms are alleviated by treatments that target mucus hypersecretion in chronic bronchitis, such as expectorants and mucolytics. A previous meta-analysis demonstrated that patients in the chronic bronchitis (CB)/pre-COPD group treated with N-acetylcysteine (NAC) experienced a reduction in symptom burden and improved quality of life during the study period.68 Studies on whether respiratory symptoms directly increase the risk of developing COPD are still limited, and there is inconsistency in the findings.69–72 In this meta-analysis, quantitative synthesis was not feasible due to substantial heterogeneity in the nature, pathological basis, and clinical implications of the respiratory symptoms evaluated across the included studies.
Limitations
This systematic review and meta-analysis had several limitations. First, there is significant heterogeneity in the incidence of pre-COPD progression to COPD. We performed subgroup analyses to explore potential explanations; however, other unidentified factors may have also contributed to the results. Second, there is yet no unequivocal definition of pre-COPD. Our research utilised the 2022 Global Initiative for Chronic Obstructive Lung Disease (GOLD) diagnostic standards. Third, most studies were designed as cohort studies, which may lead to bias. Furthermore, most of the included studies were from Western countries, which may restrict the generalizability of the study conclusions to Eastern countries or other locations. The search criteria might have potentially excluded eligible studies not in English due to the search being limited to the English language. Ultimately, sensitivity analysis was limited due to the small number of studies in this meta-analysis. Therefore, a prospective cohort study with high quality involving multiple institutions in different countries is imperative to draw a definitive conclusion.
Conclusions
In summary, this meta-analysis indicates an estimated 20% progression rate from pre-COPD to COPD. Key factors associated with increased risk include older age, smoking history, non-obstructive chronic bronchitis, PRISm, and co-existing asthma. These findings highlight identifiable risk profiles that could aid in stratifying patients within the pre-COPD population. Clinically, this supports enhanced monitoring and targeted early intervention in high-risk subgroups, such as optimising smoking cessation, managing chronic respiratory symptoms, and treating concurrent asthma. From a public health perspective, the results reinforce the value of early detection and multidimensional prevention strategies in at-risk populations. While the conclusions are tempered by the limited number of high-quality studies, significant heterogeneity, and the observational nature of included data, this synthesis provides a preliminary evidence base to guide clinical vigilance and future research. Prospective studies are needed to validate these risk factors and to assess whether early intervention can attenuate progression to established COPD.
Data Sharing Statement
The datasets used and/or analyzed in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The current meta-analysis is based entirely on previously published studies and does not require approval from an ethics committee.
Acknowledgments
We really appreciate the efforts of all the researchers whose articles were included in this study.
Author Contributions
Lili Qiao and Xiucen Wu are co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Chongqing Keweijianlian Medical Research Project, China [2025ZDXM010].
Disclosure
The authors declare that they have no competing interests.
References
1. Halpin DMG, Celli BR, Criner GJ, et al. The GOLD Summit on chronic obstructive pulmonary disease in low- and middle-income countries. Int J Tuberc Lung Dis. 2019;23(11):1131–15. doi:10.5588/ijtld.19.0397
2. Agusti A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Eur Respir J. 2023;61(4). doi:10.1183/13993003.00239-2023
3. Colak Y, Afzal S, Nordestgaard BG, Lange P, Vestbo J. Importance of early COPD in young adults for development of clinical COPD: findings from the Copenhagen General Population Study. Am J Respir Crit Care Med. 2021;203(10):1245–1256. doi:10.1164/rccm.202003-0532OC
4. Fazleen A, Wilkinson T. Early COPD: current evidence for diagnosis and management. Ther Adv Respir Dis. 2020;14:1753466620942128. doi:10.1177/1753466620942128
5. Lowe KE, Regan EA, Anzueto A, et al. COPDGene((R)) 2019: redefining the diagnosis of chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis. 2019;6(5):384–399. doi:10.15326/jcopdf.6.5.2019.0149
6. GIfCOL D. Global strategy for prevention, diagnosis and management of COPD. Global Initiative for Chronic Obstructive Lung Disease, Fontana, WI, USA; 2022.
7. Han MK, Agusti A, Celli BR, et al. From GOLD 0 to pre-COPD. Am J Respir Crit Care Med. 2021;203(4):414–423. doi:10.1164/rccm.202008-3328PP
8. Lei J, Huang K, Wu S, et al. Heterogeneities and impact profiles of early chronic obstructive pulmonary disease status: findings from the China Pulmonary Health Study. Lancet Reg Health West Pac. 2024;45:101021. doi:10.1016/j.lanwpc.2024.101021
9. Cosio BG, Casanova C, Soler-Cataluna JJ, et al. Unravelling young COPD and pre-COPD in the general population. ERJ Open Res. 2023;9(1):00334–2022. doi:10.1183/23120541.00334-2022
10. Regan EA, Lynch DA, Curran-Everett D, et al. Clinical and radiologic disease in smokers with normal spirometry. JAMA Intern Med. 2015;175(9):1539–1549. doi:10.1001/jamainternmed.2015.2735
11. Woodruff PG, Barr RG, Bleecker E, et al. Clinical significance of symptoms in smokers with preserved pulmonary function. N Engl J Med. 2016;374(19):1811–1821. doi:10.1056/NEJMoa1505971
12. Xu J, Zeng Q, Li S, Su Q, Fan H. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
13. Brightling C, Greening N. Airway inflammation in COPD: progress to precision medicine. Eur Respir J. 2019;54(2):1900651. doi:10.1183/13993003.00651-2019
14. Allinson JP, Hardy R, Donaldson GC, Shaheen SO, Kuh D, Wedzicha JA. The presence of chronic mucus hypersecretion across adult life in relation to chronic obstructive pulmonary disease development. Am J Respir Crit Care Med. 2016;193(6):662–672. doi:10.1164/rccm.201511-2210OC
15. Koo H-K, Vasilescu DM, Booth S, et al. Small airways disease in mild and moderate chronic obstructive pulmonary disease: a cross-sectional study. Lancet Respir Med. 2018;6(8):591–602. doi:10.1016/S2213-2600(18)30196-6
16. Walters EH, Shukla SD, Mahmood MQ, Ward C. Fully integrating pathophysiological insights in COPD: an updated working disease model to broaden therapeutic vision. Eur Respir Rev. 2021;30(160):200364. doi:10.1183/16000617.0364-2020
17. Eapen MS, Lu W, Hackett TL, et al. Increased myofibroblasts in the small airways, and relationship to remodelling and functional changes in smokers and COPD patients: potential role of epithelial–mesenchymal transition. ERJ Open Res. 2021;7(2):00876–2020. doi:10.1183/23120541.00876-2020
18. Bui DS, Faner R, Washko G, Jenkins C, Walters EH, Dharmage SC. Pre-COPD: an evolving concept with practice potential. Lancet Respir Med. 2025;13(9):778–781. doi:10.1016/S2213-2600(25)00236-X
19. Moll M, Sakornsakolpat P, Shrine N, et al. Chronic obstructive pulmonary disease and related phenotypes: polygenic risk scores in population-based and case-control cohorts. Lancet Respir Med. 2020;8(7):696–708. doi:10.1016/S2213-2600(20)30101-6
20. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:
21. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
22. Lo CK, Mertz D, Loeb M. Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. 2014;14:45. doi:10.1186/1471-2288-14-45
23. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
24. Fan J, Fang L, Cong S, et al. Potential pre-COPD indicators in association with COPD development and COPD prediction models in Chinese: a prospective cohort study. Lancet Reg Health West Pac. 2024;44:100984. doi:10.1016/j.lanwpc.2023.100984
25. Colak Y, Lange P, Vestbo J, Nordestgaard BG, Afzal S. Susceptible young adults and development of chronic obstructive pulmonary disease later in life. Am J Respir Crit Care Med. 2024;210(5):607–617. doi:10.1164/rccm.202308-1452OC
26. Vrbica Ž, Steiner J, Labor M, Gudelj I, Plavec D. Breathlessness and “exacerbation” questions predictive for incident COPD (MARKO study): data after two years of follow-up. PeerJ. 2023;
27. Divo MJ, Liu C, Polverino F, Castaldi PJ, Celli BR, Tesfaigzi Y. From pre-COPD to COPD: a simple, low cost and easy to IMplement (SLIM) risk calculator. Eur Respir J. 2023;62(3):2300806. doi:10.1183/13993003.00806-2023
28. Harvey BG, Strulovici-Barel Y, Kaner RJ, et al. Risk of COPD with obstruction in active smokers with normal spirometry and reduced diffusion capacity. Eur Respir J. 2015;46(6):1589–1597. doi:10.1183/13993003.02377-2014
29. Park HJ, Byun MK, Rhee CK, Kim K, Kim HJ, Yoo KH. Significant predictors of medically diagnosed chronic obstructive pulmonary disease in patients with preserved ratio impaired spirometry: a 3-year cohort study. Respir Res. 2018;19(1):185. doi:10.1186/s12931-018-0896-7
30. Jo YS, Rhee CK, Kim SH, Lee H, Choi JY. Spirometric transition of at risk individuals and risks for progression to chronic obstructive pulmonary disease in general population. Arch Bronconeumol. 2024;60(10):634–642. doi:10.1016/j.arbres.2024.05.033
31. Bui DS, Lodge CJ, Burgess JA, et al. Childhood predictors of lung function trajectories and future COPD risk: a prospective cohort study from the first to the sixth decade of life. Lancet Respir Med. 2018;6(7):535–544. doi:10.1016/S2213-2600(18)30100-0
32. Fortis S, Comellas A, Kim V, et al. Low FVC/TLC in Preserved Ratio Impaired Spirometry (PRISm) is associated with features of and progression to obstructive lung disease. Sci Rep. 2020;10(1):5169. doi:10.1038/s41598-020-61932-0
33. Arjomandi M, Zeng S, Barjaktarevic I, et al. Radiographic lung volumes predict progression to COPD in smokers with preserved spirometry in SPIROMICS. Eur Respir J. 2019;54(4):1802214. doi:10.1183/13993003.02214-2018
34. Guerra S, Sherrill DL, Venker C, Ceccato CM, Halonen M, Martinez FD. Chronic bronchitis before age 50 years predicts incident airflow limitation and mortality risk. Thorax. 2009;64(10):894–900. doi:10.1136/thx.2008.110619
35. Yee N, Markovic D, Buhr RG, et al. Significance of FEV3/FEV6 in recognition of early airway disease in smokers at risk of development of COPD: analysis of the SPIROMICS cohort. Chest. 2022;161(4):949–959. doi:10.1016/j.chest.2021.10.046
36. Higbee DH, Granell R, Davey Smith G, Dodd JW. Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10(2):149–157. doi:10.1016/S2213-2600(21)00369-6
37. Buhr RG, Barjaktarevic IZ, Quibrera PM, et al. Reversible airflow obstruction predicts future chronic obstructive pulmonary disease development in the SPIROMICS cohort: an observational cohort study. Am J Respir Crit Care Med. 2022;206(5):554–562. doi:10.1164/rccm.202201-0094OC
38. Wu F, Li H, Deng Z, et al. Clinical features and 1-year outcomes of variable obstruction in participants with preserved spirometry: results from the ECOPD study in China. BMJ Open Respir Res. 2024;11(1):e002210. doi:10.1136/bmjresp-2023-002210
39. Tagiyeva N, Devereux G, Fielding S, Turner S, Douglas G. Outcomes of childhood asthma and wheezy bronchitis. A 50-year cohort study. Am J Respir Crit Care Med. 2016;193(1):23–30. doi:10.1164/rccm.201505-0870OC
40. Kanetake R, Takamatsu K, Park K, Yokoyama A. Prevalence and risk factors for COPD in subjects with preserved ratio impaired spirometry. BMJ Open Respir Res. 2022;9(1):e001298. doi:10.1136/bmjresp-2022-001298
41. Zeng S, Tham A, Bos B, Jin J, Giang B, Arjomandi M. Lung volume indices predict morbidity in smokers with preserved spirometry. Thorax. 2019;74(2):114–124. doi:10.1136/thoraxjnl-2018-211881
42. Hayden LP, Hobbs BD, Cohen RT, et al. Childhood pneumonia increases risk for chronic obstructive pulmonary disease: the COPDGene study. Respir Res. 2015;16(1):115. doi:10.1186/s12931-015-0273-8
43. Kwon DS, Choi YJ, Kim TH, et al. FEF25-75% values in patients with normal lung function can predict the development of chronic obstructive pulmonary disease. Int J Chronic Obstr. 2020;Volume 15:2913–2921. doi:10.2147/COPD.S261732
44. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
45. Grimes DA, Schulz KF. Bias and causal associations in observational research. Lancet. 2002;359(9302):248–252. doi:10.1016/S0140-6736(02)07451-2
46. Kim SJ, Lee J, Park YS, et al. Age-related annual decline of lung function in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:51–60. doi:10.2147/COPD.S95028
47. Cho SJ, Stout-Delgado HW. Aging and Lung Disease. Annu Rev Physiol. 2020;10(82):433–459. doi:10.1146/annurev-physiol-021119-034610
48. Ragland MF, Strand M, Baraghoshi D, et al. 10-year follow-up of lung function, respiratory symptoms, and functional capacity in the COPDGene study. Ann Am Thorac Soc. 2022;19(3):381–388. doi:10.1513/AnnalsATS.202007-873OC
49. Yoshida T, Tuder RM. Pathobiology of cigarette smoke-induced chronic obstructive pulmonary disease. Physiol Rev. 2007;87(3):1047–1082. doi:10.1152/physrev.00048.2006
50. Kirkham PA, Barnes PJ. Oxidative stress in COPD. Chest. 2013;144(1):266–273. doi:10.1378/chest.12-2664
51. Wan ES. The clinical spectrum of PRISm. Am J Respir Crit Care Med. 2022;206(5):524–525. doi:10.1164/rccm.202205-0965ED
52. Wan ES, Fortis S, Regan EA, et al. Longitudinal phenotypes and mortality in preserved ratio impaired spirometry in the COPDGene Study. Am J Respir Crit Care Med. 2018;198(11):1397–1405. doi:10.1164/rccm.201804-0663OC
53. He D, Sun Y, Gao M, et al. Different risks of mortality and longitudinal transition trajectories in new potential subtypes of the preserved ratio impaired spirometry: evidence from the English Longitudinal Study of Aging. Front Med Lausanne. 2021;8:755855. doi:10.3389/fmed.2021.755855
54. Wan ES, Balte P, Schwartz JE, et al. Association between preserved ratio impaired spirometry and clinical outcomes in US adults. JAMA. 2021;326(22):2287–2298. doi:10.1001/jama.2021.20939
55. Washio Y, Sakata S, Fukuyama S, et al. Risks of mortality and airflow limitation in Japanese individuals with preserved ratio impaired spirometry. Am J Respir Crit Care Med. 2022;206(5):563–572. doi:10.1164/rccm.202110-2302OC
56. Wijnant SRA, De Roos E, Kavousi M, et al. Trajectory and mortality of preserved ratio impaired spirometry: the Rotterdam Study. Eur Respir J. 2020;55(1):1901217. doi:10.1183/13993003.01217-2019
57. Robertson NM, Centner CS, Tejwani V, et al. Preserved ratio impaired spirometry prevalence, risk factors, and outcomes: a systematic review and meta-analysis. Chest. 2025;167(6):1591–1614. doi:10.1016/j.chest.2024.12.025
58. Backman H, Myrberg T, Hedman L, Stridsman C, Rönmark E, Lindberg A. PRISm is an important risk factor for development of COPD, also in non-smokers. CHEST. 2025;168:83–94. doi:10.1016/j.chest.2025.02.025
59. Brusselle GG, Riemann SG. Preserved ratio impaired spirometry (PRISm): prognostic, preventable and treatable? Thorax. 2025;80(4):195–196. doi:10.1136/thorax-2024-222923
60. Young AL, Bragman FJS, Rangelov B, et al. Disease progression modeling in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(3):294–302. doi:10.1164/rccm.201908-1600OC
61. Ronish BE, Couper DJ, Barjaktarevic IZ, et al. Forced expiratory flow at 25%-75% links COPD physiology to emphysema and disease severity in the SPIROMICS Cohort. Chronic Obstr Pulm Dis. 2022;9(2):111–121. doi:10.15326/jcopdf.2021.0241
62. van Dijk W, Tan W, Li P, et al. Clinical relevance of fixed ratio vs lower limit of normal of FEV1/FVC in COPD: patient-reported outcomes from the CanCOLD cohort. Ann Fam Med. 2015;13(1):41–48. doi:10.1370/afm.1714
63. Guder G, Brenner S, Angermann CE, et al. “GOLD or lower limit of normal definition? A comparison with expert-based diagnosis of chronic obstructive pulmonary disease in a prospective cohort-study”. Respir Res. 2012;13(1):13. doi:10.1186/1465-9921-13-13
64. Wu F, Fan H, Liu J, et al. Association between non-obstructive chronic bronchitis and incident chronic obstructive pulmonary disease and all-cause mortality: a systematic review and meta-analysis. Front Med Lausanne. 2021;8:805192. doi:10.3389/fmed.2021.805192
65. Thomson NC. Asthma and smoking-induced airway disease without spirometric COPD. Eur Respir J. 2017;49(5):1602061. doi:10.1183/13993003.02061-2016
66. Lange P, Parner J, Vestbo J, Schnohr P, Jensen G. A 15-year follow-up study of ventilatory function in adults with asthma. N Engl J Med. 1998;339(17):1194–1200. doi:10.1056/NEJM199810223391703
67. Accordini S, Calciano L, Johannessen A, et al. A three-generation study on the association of tobacco smoking with asthma. Int J Epidemiol. 2018;47(4):1106–1117. doi:10.1093/ije/dyy031
68. Papi A, Alfano F, Bigoni T, et al. N-acetylcysteine Treatment in Chronic Obstructive Pulmonary Disease (COPD) and Chronic Bronchitis/Pre-COPD: distinct Meta-analyses. Arch Bronconeumol. 2024;60(5):269–278. doi:10.1016/j.arbres.2024.03.010
69. Engel RM, de Luca K, Graham PL, Kaboli Farshchi M, Vemulpad S, Byles J. Predictors of chronic obstructive pulmonary disease in women who have never smoked: a cohort study. ERJ Open Res. 2022;8(2):00532–2021. doi:10.1183/23120541.00532-2021
70. Kalhan R, Dransfield MT, Colangelo LA, et al. Respiratory symptoms in young adults and future lung disease. The CARDIA Lung Study. Am J Respir Crit Care Med. 2018;197(12):1616–1624. doi:10.1164/rccm.201710-2108OC
71. Lindberg A, Jonsson AC, Ronmark E, Lundgren R, Larsson LG, Lundback B. Ten-year cumulative incidence of COPD and risk factors for incident disease in a symptomatic cohort. Chest. 2005;127(5):1544–1552. doi:10.1378/chest.127.5.1544
72. De Marco R, Accordini S, Cerveri I, et al. Incidence of chronic obstructive pulmonary disease in a cohort of young adults according to the presence of chronic cough and phlegm. Am J Respir Crit Care Med. 2007;175(1):32–39. doi:10.1164/rccm.200603-381OC
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review on the Status of Female Breast Cancer in Asia with a Special Focus on Nepal
Dhakal R, Noula M, Roupa Z, Yamasaki EN
Breast Cancer: Targets and Therapy 2022, 14:229-246
Published Date: 26 August 2022
Investigation and Analysis of Risk Factors and Psychological Status of Chronic Obstructive Pulmonary Disease in Permanent Residents Aged 40 or Older in Hongyuan County, Aba Prefecture, Sichuan Province
Xia JJ, Zou XX, Qiu Y, Li WJ, Huang L, Xie WY, Xue HH, Yang M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:827-835
Published Date: 10 May 2023
Incidence and Risk Factors for Retinopathy of Prematurity in a Tertiary Hospital in China
Hu X, Zhang J, Zhang M, Chen X, Han S, Zhu J
Clinical Ophthalmology 2023, 17:3189-3194
Published Date: 25 October 2023
The Occurrence and Factors Associated with Overt Urinary Retention Among Postpartum Women After Vaginal Delivery with Labor Epidural Analgesia
Li S, Zhang X, Liu Y, Wang Y, Zheng X
International Journal of General Medicine 2023, 16:5333-5341
Published Date: 16 November 2023
Incidence and Risk Factors of Chemotherapy-Induced Hepatotoxicity: A Cross-Sectional Study
Joel S, Bukke SPN, Mamilla Mugaiahgari BK, Kyomya J, Idrine KK, Godwin N, Muasya PK, Abdi AA, Makuza KR, Tumwebaza JM, Narapureddy BR, Goruntla N, Mwandah DC, Shogar AE, Abdalla SA, Isiiko J, Yadesa TM
Cancer Management and Research 2026, 18:589840
Published Date: 25 March 2026