")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Investigation and Analysis of Risk Factors and Psychological Status of Chronic Obstructive Pulmonary Disease in Permanent Residents Aged 40 or Older in Hongyuan County, Aba Prefecture, Sichuan Province
Authors Xia JJ, Zou XX, Qiu Y, Li WJ, Huang L, Xie WY, Xue HH, Yang M
Received 13 December 2022
Accepted for publication 6 April 2023
Published 10 May 2023 Volume 2023:18 Pages 827—835
DOI https://doi.org/10.2147/COPD.S399279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Jun-Jie Xia,1 Xing-Xiong Zou,2 Yu Qiu,1 Wen-Jun Li,1 Ling Huang,1 Wen-Ying Xie,1 Hui-Hong Xue,1 Ming Yang1
1Department of Respiratory, The Third Hospital of Mianyang/Sichuan Mental Health Center, Mianyang, Sichuan, 621000, People’s Republic of China; 2Department of Radiology, The Third Hospital of Mianyang/Sichuan Mental Health Center, Mianyang, Sichuan, 621000, People’s Republic of China
Correspondence: Ling Huang, Email [email protected]
Background: COPD is an important public health problem worldwide, and there is a lack of epidemiological data on COPD in high-altitude areas in Sichuan province. Thus, we aimed to investigate the prevalence, risk factors and psychological status of COPD in Hongyuan County, Aba Prefecture, Sichuan Province, which is located at an average altitude of 3507 meters.
Methods: The 40 years old or greater permanent residents of Hongyuan County were selected by random sampling method, and the lung function test and questionnaires were conducted to determine the disease situation of COPD. The prevalence of COPD was compared among different factors of investigation, and multivariate logistic regression analysis was used for different factors to determine the independent influencing factors of COPD disease.
Results: A total of 456 permanent residents aged 40 years or older in Hongyuan County, 436 qualified for quality control, among which 53 cases confirmed COPD, the total prevalence was 12.16%, among which the prevalence was 14.55% for men and it was 8.07% for women. There were significant differences in different gender, ethnicity, age, smoking status, smoking years, educational level, heating style, history of tuberculosis, and prevalence of BMI (P < 0.05). Binary logistic regression analysis showed that age ≥ 60 years (OR = 2.810, 95% CI: 1.0457.557), Han Nationality (OR: 3.238, 95% CI: 1.290– 8.127), the heating method including biofuels (OR: 18.119, 95% CI: 4.140– 79.303) and coals (OR: 6.973, 95% CI: 1.856– 26.200), medical history of pulmonary tuberculosis (OR: 2.670, 95% CI: 1.278– 5.578), the education level including junior high school (OR: 3.336, 95% CI: 1.2259.075), high school and above (OR: 5.910, 95% CI: 1.796– 19.450), and smoking (OR: 10.774, 95% CI: 3.622– 32.051) were independent risk factors for COPD disease. The prevalence of anxiety was 16.98%, and the prevalence of depression was 13.2%.
Conclusion: The prevalence of COPD in Hongyuan County was higher than the national level; age, ethnic group, education, smoking, heating method, and history of tuberculosis are the independent influencing factors of COPD in Hongyuan County. The prevalence of anxiety and depression is low.
Keywords: chronic obstructive pulmonary disease, prevalence, risk factors, psychological status
Introduction
Chronic obstructive pulmonary disease (COPD) is an important public health problem worldwide. As a populous province, Sichuan province has insufficient epidemiological data on COPD, which is only reported in Chengdu community and Mianyang City. A recent epidemiological investigation study of COPD in Sichuan Province1 Aba state is also not included as a sampling survey area. Hongyuan County, Aba Prefecture, with an average altitude of 3507 meters, the highest nomadic Tibetan county in Sichuan Province, lacks relevant epidemiological survey data. Expert consensus of COPD screening in Chinese counties points out that2 county hospitals in China have insufficient knowledge of COPD, standardized management is not in place, and the public awareness rate of diseases is low. In this study, the epidemiological investigation of COPD was conducted on permanent residents aged≥40 years in Hongyuan County, Aba Prefecture, Sichuan Province, which filled the gap in the Tibetan plateau areas in Sichuan Province.
Methods
Subjects of Investigation
A sample of 456 individuals were randomly selected from the population register of communities and villages in Hongyuan County, Aba Prefecture, Sichuan Province, using a random sampling method. Inclusion criteria: aged≥40 years, living in the current residence for more than 10 years. Except for the following conditions: residents living in functional areas, such as student dormitories, army, sheds, nursing homes, temple; mental illness and cognitive impairment (dementia, comprehension disorders, deaf, etc.); high paraplegia; pregnant or lactating women; newly detected and treated tumors. This study was conducted according to the Declaration of Helsinki and approved by the Ethics Review Committee of Mianyang Third People’s Hospital. All of the survey respondents signed the informed consent form.
Methods of Investigation
The survey used uniform methods, procedures, questionnaires and US spiro-PD portable lung function instrument. Nationwide epidemiological survey of COPD questionnaire,3 the Global COPD Prevention Initiative, the COPD Burden Research project, and the Hamilton Anxiety Scale and Hamilton Depression Rating Scale, 17 item are the reference for this study questionnaire.4 In the method of household survey, the uniformly trained respiratory physicians asked the respondents face to face and asked questions in the independent and quiet room according to the questionnaire items, and completed the scale filling and the lung function examination. Lung function test: using the American spiro-PD portable lung function instrument, height and weight were measured in the standing position and repeated 3–8 times of lung ventilation function test, with each interval> 1 min. During the measurement, the subject was required to have no cough, early or sudden discontinuation, air leakage and mouthparts obstruction, and the maximum difference between the first second forced breath volume (FEV 1) and forced lung capacity (FVC) was within 0.2 L, and the best value was taken. For those with airflow limitation, 200 ug of albuterol was measured again after 15–30 min, and the best detection value was taken. The project leader supervised and controls the whole process of the epidemiological survey.
COPD Diagnostic Criteria and Related Definitions
(1) Diagnosis criteria for COPD: 5 The ratio of FEV 1 to FVC (FEV 1 / FVC) was <70% after inhalation, and other cardiopulmonary diseases were excluded. (2) Smoking: 1 cigarette per day, continue smoking for 1 month, or total smoking 100; (3) Tuberculosis history: refers to the respondents who were diagnosed with tuberculosis in a regular medical institution and have been cured for more than 1 year or more. (4) Anxiety patients: HAMA score≥7 points; depression patients: HAMD-17 total score≥7 points.
Statistical Analysis
Statistical analysis was carried out using SPSS 17.0. Utilization rate or composition ratio represents count data, mean ± standard deviation, χ2 Tests or Fisher’s exact test were used for group comparisons, and multivariate analysis used binary Logistic regression analysis as statistically significant at P <0.05.
Results
General Situation
A total of 456 permanent residents aged 40 years old and above were surveyed, and a total of 436 people were intact and passed the quality control of lung function, with a qualified rate of 95.61%. The respondents included 275 men (63.07%) and 161 women (36.93%), aged from 40 to 93 years, with a mean age of 56.02 ± 11.52 years.28.9% of the population (Figure 1).
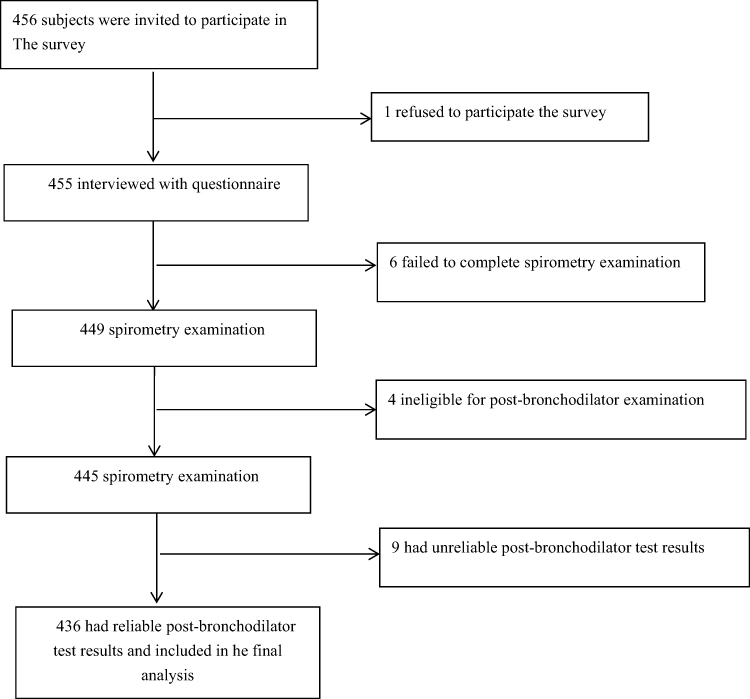 |
Figure 1 Flow chart of study. |
Major Risk Factors
(1) General situation: 87 cases of Han nationality, accounting for 19.95%, and 349 cases of Tibetan nationality, accounting for 80.05%. Among the respondents, 35.32% years old were 40–49,26. 15% were 50–59, 22.94% were 60–69, and 14.68% were older than 70. Urban residents accounted for 50.46%, and rural residents accounted for 49.54%. The educational level was generally low, with primary school education or below accounting for 62.16%. BMI between 24 and 28 was 42.2%. (2) Smoking status: the smoking rate was 28.9%, with 19 women and 107 men. 96 Tibetan and 30 Han cases. The average smoking volume was: 13.68 cigarettes per day. The age of smoking was less than or equal to 20 years accounted for 69.84%, and the age of starting smoking was between 21 and 40 years old, accounting for 62.7%. (3) Living environment: 136 (31.19%) housing buildings, 283 (64.91%), 17 (3.90%) tents. The most common exhaust facility in the kitchen is the chimney, accounting for 87.61%), (4) cooking and heating: the most common heating fuel is biofuel, accounting for 36.24%; followed by coal, accounting for 34.86%; the most common cooking fuel is also coal and biofuel, accounting for 51.15% and 35.09% respectively. (5) Past medical history and comorbidities: the history of respiratory diseases accounted for 27.29%. (6) Aware of COPD and occupational exposure: the overall population had almost no long-term occupational exposure and dust exposure, the awareness rate was about 6.3%, the lung function examination rate was about 1.5%, and the utilization rate of inhaled drugs was about 0.3%.
Prevalence of COPD
53 (12.16%) of COPD patients diagnosed in this survey, 13 females, with a prevalence of 8.07% and 40 men, with a prevalence of 14.54%. The prevalence of the Han nationality was higher than that of the Tibetan nationality. The prevalence of COPD varies in different age groups, with it increasing with age.
Prevalence of COPD and Univariate Analysis (Table 1)
Analysis of Risk Factors of COPD, Table 2 Assigns a Value Table to the Variables
Used binary Logistic regression analysis to statistically analyze the risk factors with differences in single factor analysis, the results showed that the risk factors for COPD included ethnicity, age, smoking status, heating method, education level and history of tuberculosis (Table 3).
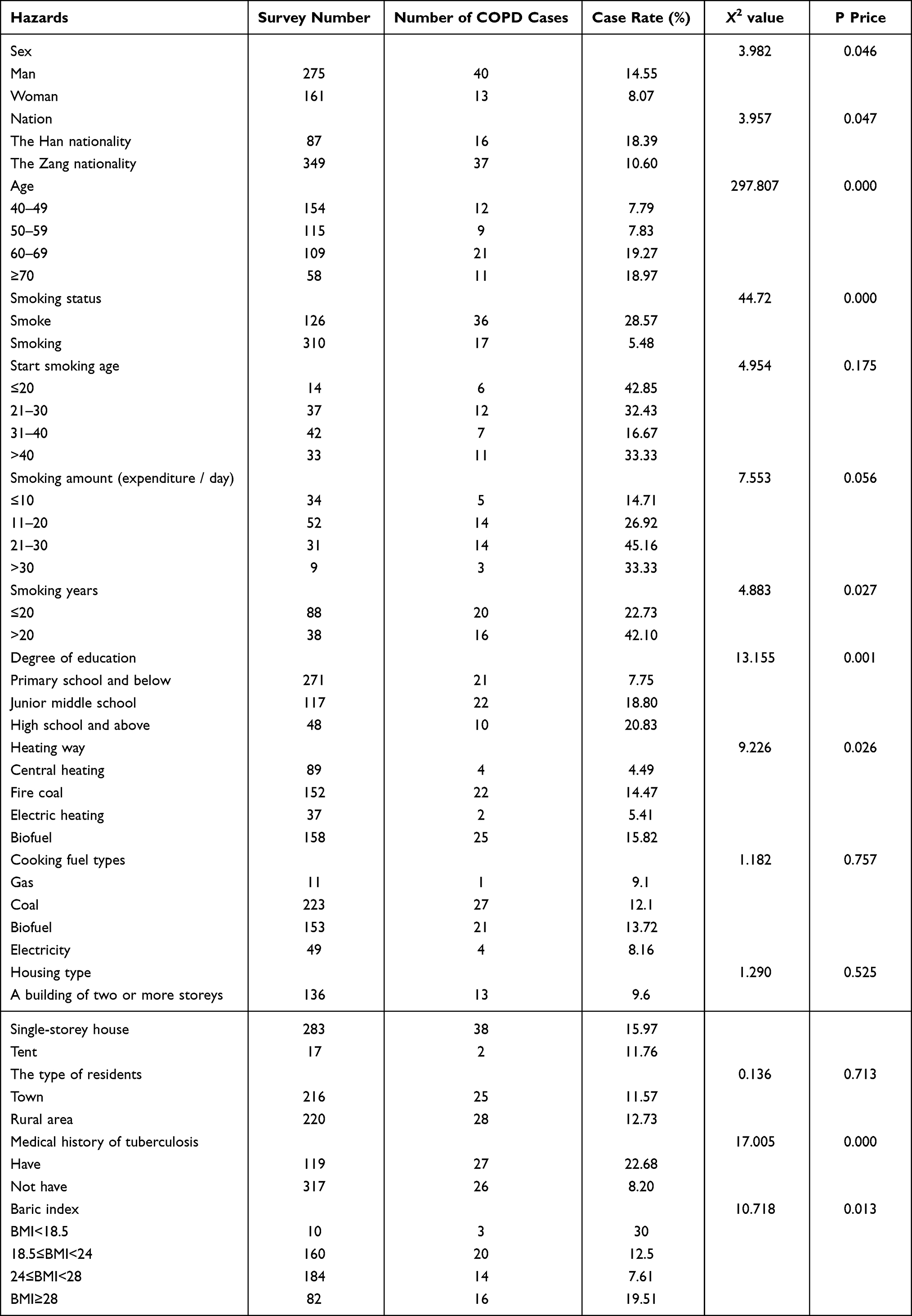 |
Table 1 Univariate Analysis of the Risk Factors for COPD |
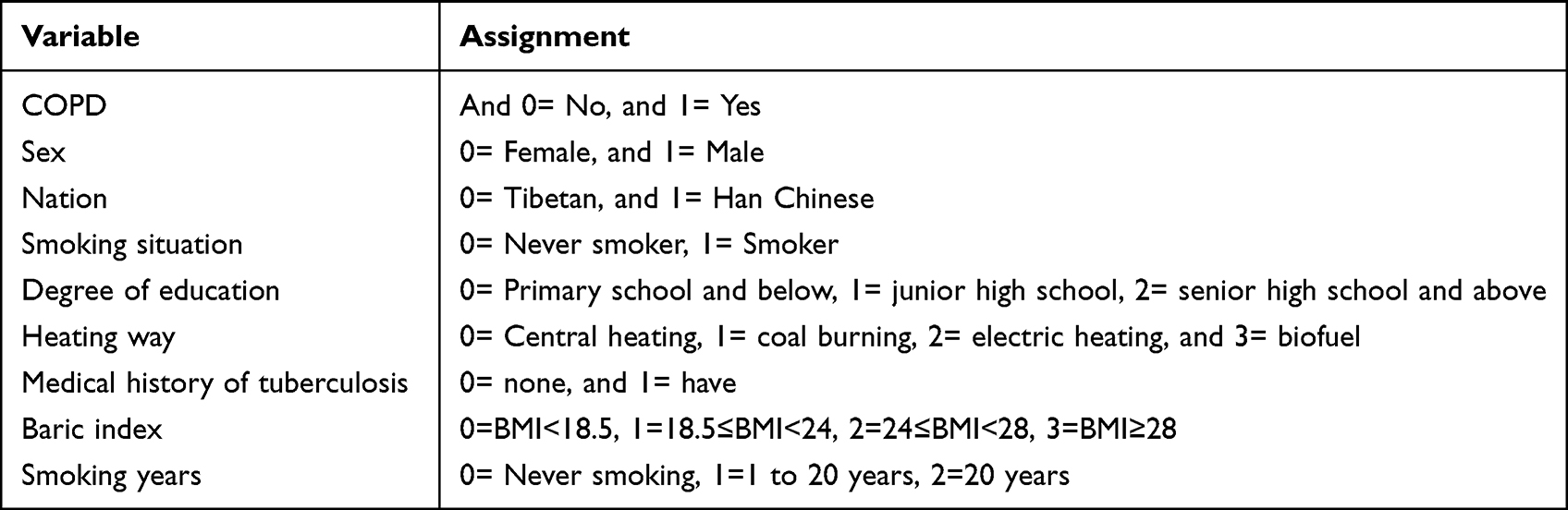 |
Table 2 Value Table for Binary Logistic Regression Analysis |
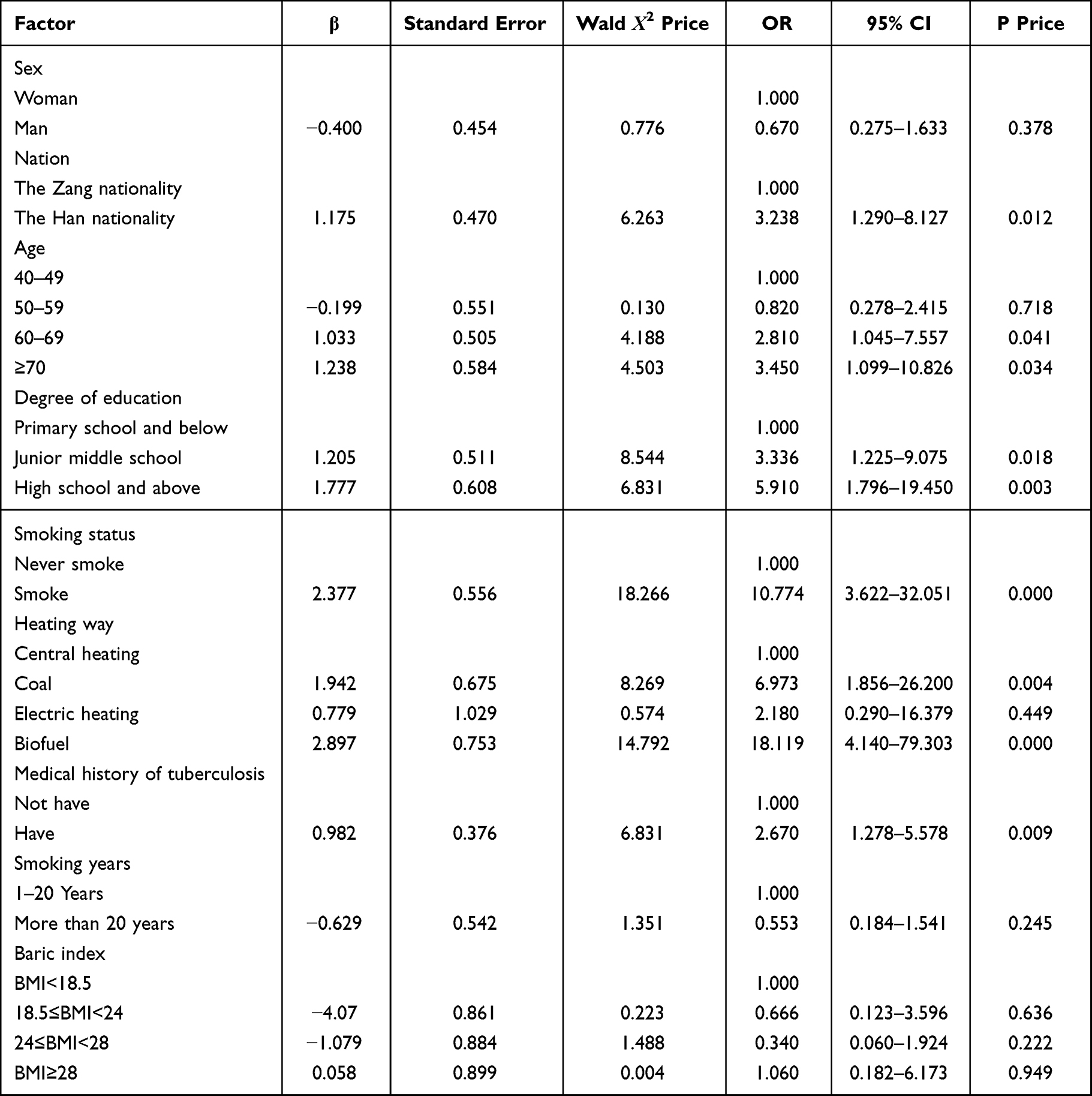 |
Table 3 Multivariate Analysis of COPD |
Among the 53 Patients Detected COPD
9 cases (16.98%) were anxious, of which 7 had symptoms of anxiety and 2 had obvious anxiety. There were 7 patients with depression (13.2%), including 6 with mild depression and 1 with moderate depression.
Discussion
COPD is a common disease that seriously affects the lung function and quality of life of patients. The survey showed that the prevalence of COPD in Hongyuan County, Aba Prefecture was 12.16%, higher than the national level (9.9%).6 The female prevalence rate is 8.07%, significantly higher than the national level (5.1%), and the male prevalence rate is 14.54%, which is also higher than the national level (12.4%). Studies have shown that the prevalence of COPD is higher at high altitudes.7 A meta-analysis also found that the prevalence of COPD was higher in high -altitude areas, especially in Asia, but the study concluded that altitude was not an independent risk factor,8 which indicated that there were other risks factors involved in the occurrence of disease in high altitude areas. Some studies believe that high altitude hypoxic environment leads to more population having pulmonary hypertension,9 which is related to the increase in the prevalence of COPD. There are also studies suggest that the prevalence of COPD is related to high PM2.5 exposure in high -altitude areas.10 The possible reasons analyzed in this study are that Hong yuan County, located in a plateau alpine region, undergoes long winters, which lead to the residents used biofuels for heating and cooking for a long time ten years ago, and in the past decade, they used both biof- uels and coal for heating and cooking. Furthermore, the plateau hypoxic environment leads to more pulmonary hypertension in the population, and so does a higher preval- ence of COPD.
The occurrence of COPD is related to age.11 Studies by Rafael Laniado-Laborin et al have shown that the prevalence of COPD at high altitudes is positively correlated with age.10,12 This study shows that increasing age is an important risk factor for COPD in Hongyuan area. This may be related to the decline in lung function with age and longer exposure to risk factors. Smoking is one of the main risk factors for COPD. The prevalence of smoking in high altitude areas is significantly higher than that of non-smokers.10 Harmful substances in tobacco scale the airway epithelium and cause damage to the bronchial epithelium, damage the lung immune system, making the lungs prone to infection, and finally cause lung function impaired. The results of this study also show that smoking is one of the risk factors for the prevalence of COPD in Hongyuan County. Univariate analysis showed that heating methods were associated with COPD, and further Logistic regression analysis suggested that coal and biofuels as heating fuels were important factors that increased the risk of developing COPD. The main harmful components of smoke from biofuels and coal include carbon oxides, nitrogen oxides, sulfur oxides, and unburned hydrocarbon particles, resulting in reduced lung function. Moreover, the area is located in an alpine and high-altitude area, and the heating time is so long, about 8–9 months a year, that the closed doors and windows and poor ventilation equipment lead to serious indoor pollution and thus accelerate the occurrence of COPD.
Both univariate and multivariate analyses of this study suggest that the history of tuberculosis will increase the incidence of COPD. The incidence of tuberculosis in this area is high, medical resources are scarce, people’s awareness of the disease is low, they know less about modern medical technology, and they are not willing to accept treatment. Most patients have severe lung damage when tuberculosis is discovered and treated. Guo13 also reached similar conclusions in the COPD epidemiological survey in Xinjiang and Tibet, China, in high-altitude areas.
This study shows that the prevalence rate of Han population is higher than that of Tibetan population, suggesting that the prevalence of COPD may be related to ethnic and racial differences. Havryk14 et al studied Sherpas living at an average altitude of 4000 meters, showing that their lung capacity increased by about 12% compared to Caucasians. Wood15 conducted lung function studies on Ladakh and Tibetans living between 3300 and 4500 meters above sea level. Spirometry results in both groups showed high values of maximal mid-expiratory flow are between 130% and 150% of predicted, and a FEV1/FVC ratio of 115%. These studies suggest that, over time and over multiple generations, high-altitude populations have undergone physiological and genetic adaptations to extreme altitudes in response to chronic hypoxia and generally high-intensity exercise. Living at high altitudes is associated with accelerated lung function decline in populations with low daily smoking rates.16 However, the lung function of the Han population is lower than that of the Tibetan population, and is more susceptible to decline due to environmental factors. Moreover, the smoking rate of the Han population (34.4%) was higher than that of the Tibetan population (27.5%) in this study, which is also one of the reasons for the high prevalence.
Household Air Pollution (HAP) is known to increase the prevalence of COPD. A systematic review showed that,17 HAP resulted in a significantly increased risk of COPD in women, and the use of solid fuels for cooking and heating for more than 6 months resulted in severe lung damage. Lung pathology in individuals exposed to HAP showed small airway fibrosis and emphysema. Lung damage occurs mostly in women, who often prepare meals near a fire for hours a day in poorly ventilated homes. A study from China13 showed that the proportion of subjects exposed to HAP at high altitudes was significantly higher than that reported in the previous Chinese COPD national survey. In plateau Tibetan areas, due to differences in living habits, women are more likely to be affected by household air pollution than men, which may be the reason why there is no gender difference in the prevalence of COPD in this population, and this study is consistent with its results.
This study showed that a high level of education was positively correlated with the prevalence of COPD, contrary to previous studies.13 The reason may be that Hongyuan County is a high-altitude grassland area, and Tibetans are mainly nomadic. Due to limited living habits and economic conditions, there is less exposure to cigarette smoke and less exposure. However, with the policy of poverty alleviation in recent years, more Han people entering Tibetan areas, while bringing in knowledge and wealth, some educated and qualified Tibetans have the opportunity to be exposed to risk factors such as smoking. In this study, the smoking rate of those with primary school education and below was 14.76%, that of those with junior high school education was 52.99%, and that of those with high school education was 50%. And it may be one of the reasons that the proportion of Han people with junior high school education or above (48.27%) is higher than that of Tibetans (35.24%).
The results of the epidemiological survey in Hongyuan County, Aba Prefecture revealed that age, ethnicity, smoking, use of coal and biofuels for heating, history of tuberculosis, and high education level are independent risk factors for COPD in residents over 40 years old. To prevent and treat COPD, the primary task is still to strengthen tobacco control, reduce indoor exposure to harmful gases, and strengthen the prevention and treatment of tuberculosis. At the same time, increasing the publicity of COPD prevention and treatment, improving the medical system for chronic disease management, reducing the incidence of COPD, and reducing the burden of disease are conducive to the early prevention and treatment of COPD.
Studies have shown that anxiety and depression are common comorbidities of COPD and will increase the number of acute exacerbations and hospitalizations of patients, and reduce the quality of life of patients.18 Some data show that the incidence of depression in stable COPD patients ranges from 10% to 42%. The acute exacerbation period is 10% to 86%. The prevalence of anxiety ranges from 13–46% among ambulatory patients to 10–55% among hospitalized patients.19 In this study, the incidence rate of anxiety in COPD patients was 16.98%, and the incidence rate of anxiety was 13.2%. The incidence rate is low. The reason might be that the patients detected in this study were all in a stable period and their condition was relatively mild, and even most patients had no obvious respiratory symptoms before this investigation. Furthermore, it is also related to the lack of understanding of diseases and the special living habits in plateau Tibetan areas.
This study has certain limitations. First, the geographical scope of the study is small and the sample size is small. Second, the region is relatively cold and so this study failed to collect data on temperature changes in this region, and failed to understand the relationship between cold climate and disease in this region. Third, due to climatic reasons, some people aged 70 and above left their permanent residences, so the actual survey sampled less of this group, which may lead to an underestimation of the prevalence of COPD. Fourth, this cross-sectional survey cannot remove recall bias, such as history of tuberculosis or previous COPD diagnosis. Fifth, patients with asthma and other diseases may be misclassified, possibly leading to an overestimation of COPD prevalence. Sixth, exclusion of subjects with severe disease due to strict spirometry rules may have influenced the results. Seventh, there is a lack of further analysis of risk factors for psychological conditions.
Funding
This work was supported by Health Commission of Sichuan Province Scientific Research Project [NO.20PJ267].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dong T, Xinyin X, Deng Y, et al. Analysis of chronic obstructive pulmonary disease disease and its influencing factors of 40-year-old permanent residents in Sichuan Province. Public Health in China. 2021;37(12):1762–1765. Chinese.
2. Expert consensus compilation of COPD screening in China, grassroots working Committee of Respiratory Physician Branch of Chinese Medical Doctor Association. Chinese county chronic obstru ctive pulmonary disease screening expert consensus (2020). Chin Med J. 2021;101(14):989–994. Chinese.
3. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Res Pir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
4. Regional COPD working group. COPD prevalence in 12 Asia-Pacific countries and region: projections based on the COPD prevalence estimation model. Respirology. 2003;8(2):192–198. doi:10.1046/j.1440-1843.2003.00460.x
5. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Report. 2019;53:5.
6. Bao H, Fang L, Wang L, A meta-analysis of the prevalence of COPD in people aged 40 years and older in China from 1990 to 2014. Chin J Epidemiol. 2016;37(1):119–124. Chinese. doi:10.3760/cma.j.issn.0254-6450.2016.01.026
7. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133:343–349. doi:10.1378/chest.07-1361
8. Xion g H, Huang Q, He C, et al. Prevalence of chronic obstructive pulmonary disease at high altitude: a systematic review and meta analy- sis. Peer J. 2020;8:e8586. doi:10.7717/peerj.8586
9. Aguirre-Franco C, Torres-Duque CA, Salazar G, et al. Prevalence of pulmonary hypertension in COPD patients living at high altitude. Pulmonology. 2022;2(22):4–6.
10. Brakema EA, Tabyshova A, Kasteleyn MJ. High COPD prevalence at high altitude: does household air pollution play a role? Eur Respir J. 2019;53(2):1801193. doi:10.1183/13993003.01193-2018
11. Qiu J, Zhang Y, Chen J, et al. Epidemiological invest- igation and analysis of chronic obstructive pulmonary disease in Ningxia Hui Autonomous Region. Chin J Tubercul Breath. 2013;4:265–268. Chinese.
12. Laniado-Laborin R, Rendónb A, Batiz F, et al. High altitude and chronic obstructive pulmonary disease prevalence: a casual or causal correlation? Arch Bronconeu Mol. 2012;48(5):156–160.
13. Guo Y, Xing Z, Shan G. Prevalence and risk factors for COPD at high altitude: a large cross-sectional survey of subjects living between 2100–4700 m Above Sea Level. Front Med. 2020;7:581763. doi:10.3389/fmed.2020.581763
14. Havryk AP, Gilbert M, Burgess KR. Spirometry values in Himalayan high altitude residents (Sherpas). Respir Physiol Neurobiol. 2002;132(2):223–232. doi:10.1016/S1569-9048(02)00072-1
15. Wood S, Norboo T, Lilly M, et al. Cardio pulmonary function in high altitude residents of Ladakh. High Alt Med Bio. 2003;4(4):445–454. doi:10.1089/152702903322616191
16. Miele CH, Grigsby MR, Siddharthan T, et al. Environmental exposures and systemic hypertension are risk factors for decline in lung function. Thora. 2018;73(12):1120–1127. doi:10.1136/thoraxjnl-2017-210477
17. Sana A, Somda SMA, Meda N, Bouland C. Chronic obstruc- tive pulmonary disease associated with biomass fuel use in women: a systematic review and meta-analysis. BMJ Open Respir Res. 2018;5:e000246. doi:10.1136/bmjresp-2017-000246
18. Ye ZP, Chen L. Research progress of chronic obstructive pulmonary disease with anxiety and depression. Chin J Respir Crit Care. 2019;18:491–494.
19. Yohannes AM, Kaplan A, Hanania NA. Anxiety and depression in chronic obstructive pulmonary disease: recognition and management. Clev Clin J Med. 2018;85:11–18. doi:10.3949/ccjm.85.s1.03
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.