Back to Journals » International Journal of General Medicine » Volume 16
The Occurrence and Factors Associated with Overt Urinary Retention Among Postpartum Women After Vaginal Delivery with Labor Epidural Analgesia
Authors Li S, Zhang X, Liu Y, Wang Y ![]() , Zheng X
, Zheng X
Received 18 September 2023
Accepted for publication 9 November 2023
Published 16 November 2023 Volume 2023:16 Pages 5333—5341
DOI https://doi.org/10.2147/IJGM.S440161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Sen Li,1 Xiaohong Zhang,1 Yan Liu,1 Yongli Wang,1 Xujuan Zheng2
1Department of Obstetrics and Gynecology, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China; 2Medical School, Shenzhen University, Shenzhen, 518060, People’s Republic of China
Correspondence: Xujuan Zheng, Medical School, Shenzhen University, Shenzhen, People’s Republic of China, Tel +8613392839664, Email [email protected]
Background: Early recognition and prompt intervention for overt postpartum urinary retention (PUR) takes on a critical significance when a woman chooses labor epidural analgesia for pain relief. However, there have been rare fewer reports on the incidence and factors influencing overt PUR in women after vaginal delivery with labor epidural analgesia in China. Therefore, this study aimed to investigate the incidence and factors correlated with overt urinary retention in postpartum women undergoing vaginal delivery with labor epidural analgesia.
Methods: In total, 462 Chinese postpartum women with labor epidural analgesia and vaginal delivery were recruited in one tertiary hospital in Beijing from Dec. 2020 to Nov. 2021. Factors associated with overt PUR for these women were identified through multivariate logistic regression analysis.
Results: The incidence of overt PUR was obtained as 10.2% among these women after vaginal delivery with labor epidural analgesia. As indicated by the result of univariate analysis, forceps-assisted delivery, lateral episiotomy, perineal pain, and fluid administration in the delivery room were correlated with PUR. The result of the multivariate logistic regression suggested that forceps-assisted delivery (odds ratio [OR]=2.46, 95% confidence interval [CI]: 1.14– 5.32, P=0.022), lateral episiotomy (OR=4.55, 95% CI: 1.91– 10.80, P=0.001), and perineal pain (OR=4.23, 95% CI: 2.05– 8.73, P< 0.001) were factors affecting overt PUR for these women.
Conclusion: Postpartum women undergoing vaginal delivery with labor epidural analgesia showed a high incidence of overt PUR, and health-care providers should pay more attention to their postpartum urination status in clinical practice. Effective and timely intervention is strongly recommended to reduce the occurrence of overt PUR for these kinds of postpartum women undergoing vaginal delivery with labor epidural analgesia, such as ones experienced forceps-assisted delivery, lateral episiotomy, and more severe perineal pain.
Keywords: labor epidural analgesia, vaginal delivery, postpartum urinary retention, incidence, risk factors
Introduction
As a common complication after vaginal delivery, postpartum urinary retention (PUR) refers to the presence of urine in the bladder of postpartum women for six hours after childbirth and the inability to excrete urine by themselves (overt PUR) or the inability to completely excrete it (ie, the residual urine volume in the bladder >150 mL after trying to urinate, covert PUR).1 Since there has not been any standardized definition of PUR after vaginal delivery around the world, the incidence of PUR reported in existing research has varied widely, ranging from 1.5% to 45%.2,3 PUR can result in urinary tract infections, urinary incontinence, bladder rupture, renal dysfunction, and others,4 which detrimentally affect the well-being of postpartum women.5 Previous research described that there were many risk factors for PUR (eg, epidural anesthesia, forceps-assisted delivery, lateral episiotomy or perineal laceration, primiparity, macrosomia, and prolonged second stage of labor), whereas the results vary to a certain extent from different reports.2,6–8
As labor analgesia techniques and concepts have been vigorously implemented in China over the past few years, labor epidural analgesia has been extensively performed in various midwifery institutions nationwide.9,10 It is worth noting that with the gradually increased rate of labor epidural analgesia, the incidence of PUR has become more widespread and complicated. Existing research has suggested that epidural anesthesia is a vital risk factor for overt PUR.2,6,7 Early recognition and prompt intervention for overt PUR take on a critical significance when a woman chooses labor epidural analgesia for pain relief. In contrast, there have been rare fewer reports on the incidence and factors influencing overt PUR in women after vaginal delivery with labor epidural analgesia in China. Thus, this study aimed to investigate the incidence of overt urinary retention in Chinese women who delivered vaginally with labor epidural analgesia and to analyze the factors associated with overt PUR to provide a theoretical basis for preventing the incidence of PUR for these postpartum women.
Materials and Methods
Study Subjects
Upon approval by the Ethics Committee of Peking University People’s Hospital (Approval number: 2023PHB036-001), a quantitative cross-sectional study was conducted. A total of 462 cases of women undergoing vaginal delivery with labor epidural analgesia were collected from December 2020 to November 2021 in the obstetric department of a tertiary hospital in Beijing through convenience sampling. Inclusion criteria were: (1) women with epidural analgesia who delivered vaginally; (2) singleton pregnancy. Exclusion criteria were: (1) women with severe verbal communication disorder, mental disorder, or cognitive impairment; (2) women who appeared serious maternal complications or their infant with neonatal complications; (3) women with urinary tract disease or kidney disease. All study subjects understood the research content and process, and they were willing to participate in the study and signed the informed consent form before data collection. The flow chart of our study population selection is shown in Figure 1.
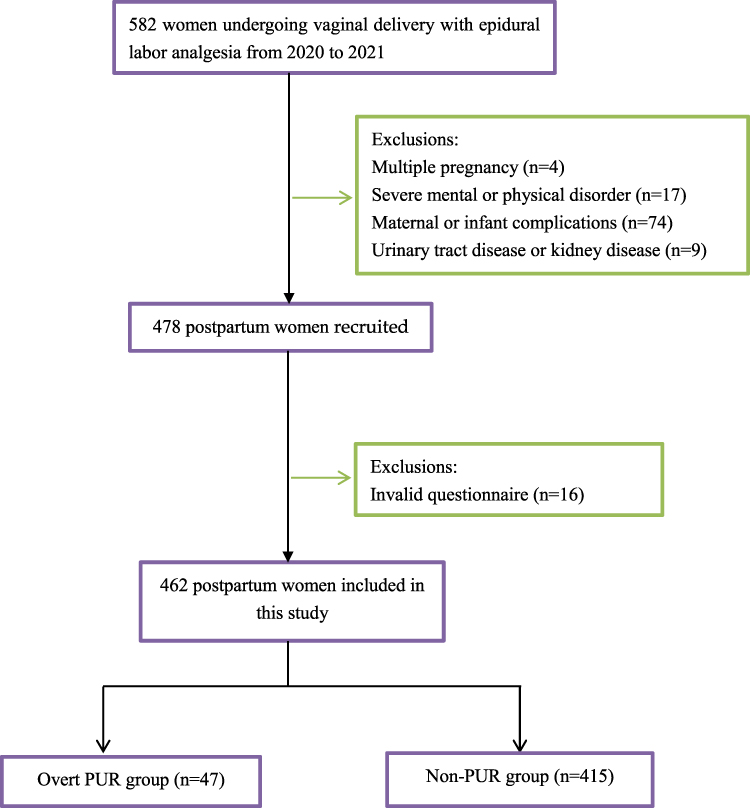 |
Figure 1 Flow chart of the study population selection. Abbreviation: PUR, postpartum urinary retention. |
In regard to the results of our retrospective data analysis, the incidence of PUR after forceps-assisted delivery in women with labor epidural analgesia was about 25%, the incidence of PUR without forceps-assisted delivery was 5%, and the rate of forceps-assisted delivery in our hospital was about 15%. After setting α=0.05 and β=0.20, a minimum of 300 women are required to see any difference in the incidence of PUR in women with or without forceps-assisted delivery by calculating with PASS (Power Analysis & Sample Size) 2019 software.
Survey Methods and Content
In the present study, all investigators attended the unified, standardized training for data collection and clarified the aim of this survey, the main content, and the corresponding confidentiality principles to the respondents, then collected data in combination with participants’ medical records. The content of data is presented as follows: (1) basic information of postpartum women (eg, age, education, height, weight, body mass index, weight gain during pregnancy, week of pregnancy, number of pregnancy, presence of pregnancy complications); (2) childbirth status (eg, the removal of analgesic pump immediately or not after delivery, mode of delivery, duration of the first and second stage of labor, whether to catheterize during labor, the manual removal of placenta or not, the amount of fluid given during labor, whether to conduct lateral episiotomy, birth weight of the newborn, whether and to what extent there was perineal edema, as well as whether and to what extent there was perineal pain); (3) observation of postpartum urination (eg, time of first voiding and amount of urine voided, amount of water consumed after delivery until first voiding, method used to promote postpartum voiding, whether to catheterize, and amount of first catheterization).
Diagnostic Criteria for Overt PUR
In the current research, overt PUR is defined as women who cannot urinate spontaneously within 6 h after vaginal delivery and need at least one catheterization within the first 24 h postpartum.11
Statistical Methods
All data were double-checked, and data analysis was performed by the Statistical Package for Social Sciences (SPSS, 21.0). Categorical data were expressed as frequencies and percentages, and continuous data were expressed by mean and standard deviation (SD). The χ2 test for categorical variables and the independent sample t-test for continuous variables were conducted to detect any significant difference between overt PUR group and non-PUR group on the social-demographic and clinical characteristics. The factors associated with overt PUR were analyzed through the multivariate logistic regression analysis. Odds ratio (OR) and 95% confidence interval (CI) were calculated for independent risk factors and protective factors related to overt PUR. The difference was considered with statistical significance at P<0.05, with a test level of а=0.05 (two-sided).
Results
Participants’ Profile
A total of 478 questionnaires were collected, and 462 of which were valid, with an effective rate of 96.7%. Finally, 462 maternal cases were studied in, with a predominance of primiparous women, accounting for 84.8%. Their mean age was 31.26 (3.97), and about 51.9% of them had undergraduate or college degree. Approximately 56.5% of women had no comorbidities during pregnancy; 18.0% experienced the forceps-assisted delivery; and 82.3% were catheterized during labor. Almost one-fourth of women suffered from lateral episiotomy; 11.3% experienced manual placenta removal; and 40.0% had postpartum labor analgesia pump removed. Most postpartum women had mild perineal pain after delivery, accounting for nearly 82.7%; the degree of perineal edema was one degree in 48.9%. Among these women, the mean time of first stage of labor and second stage of labor was 490.43 (206.24) min and 79.12 (52.30) min, respectively; and the mean amount of fluid infused was 1308.51 (546.03) mL.
Comparison of socio-demographic and clinical characteristics of participants between overt PUR group and non-PUR group is shown in Table 1. Women with forceps-assisted delivery, with lateral episiotomy, having higher level of perineal pain, or having higher volume of fluid administration in the delivery room were more likely to suffer from overt PUR.
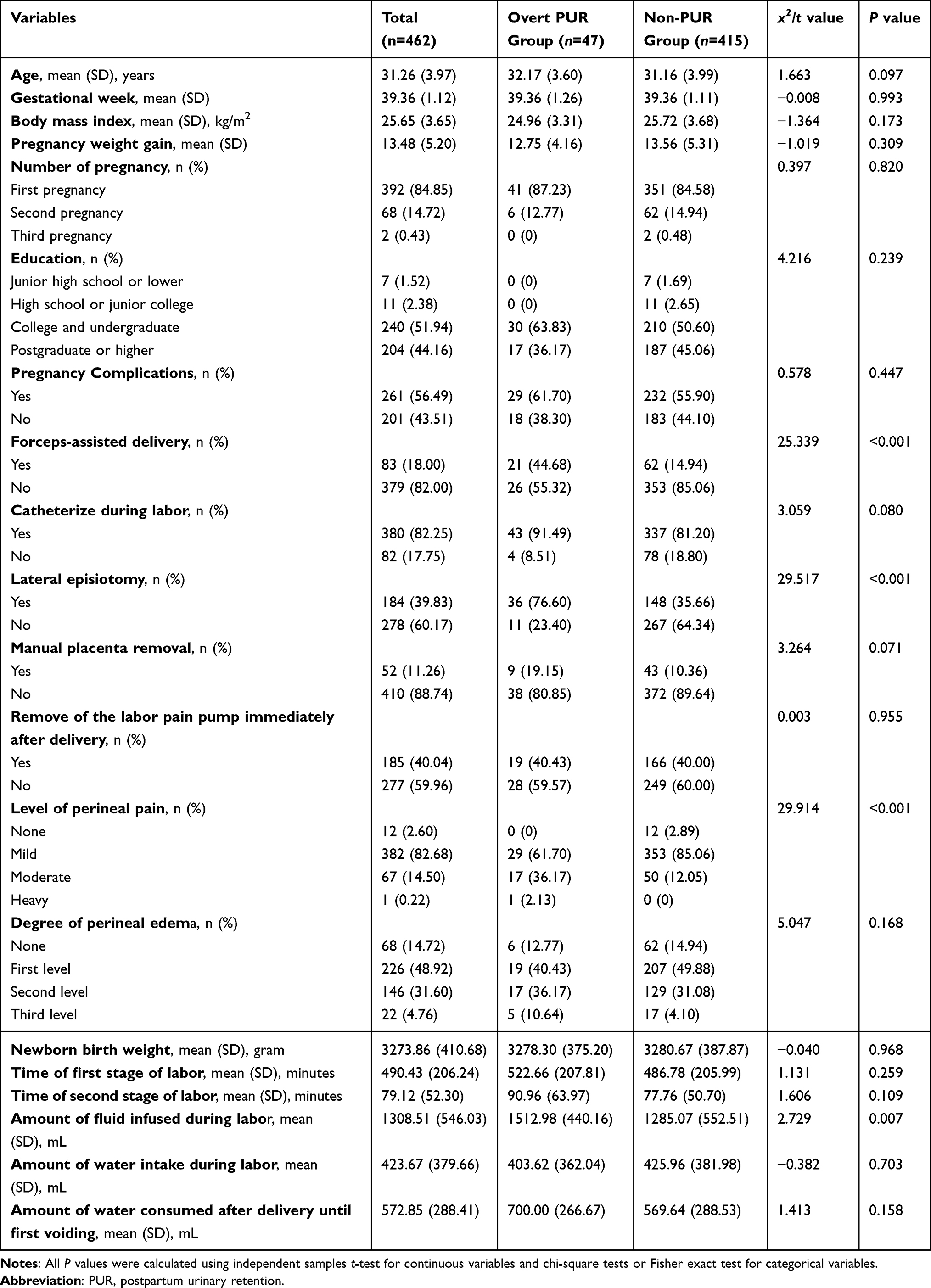 |
Table 1 Comparison of Socio-Demographic and Clinical Characteristics of Participants Between Overt PUR Group and Non-PUR Group |
Incidence of Overt PUR and Status of Initial Voiding After Labor Analgesia
In the current research, 47 cases of overt PUR were developed, and its incidence was 10.2%. Among these postpartum women in overt PUR group, the mean volume of the first catheterization was 711.96 (176.44) mL. Among women without PUR, the mean time to first postpartum voiding was 242.68 (75.43) min. In regarding to all participants, 231 (50.0%) postpartum women underwent induction therapy of voiding during urination, such as massage, hot compresses, and listening to the sound of running water. In addition, there were 22 cases of urination after application of neostigmine methosulfate intramuscular injection.
Factors Associated with PUR in Women After Vaginal Delivery with Labor Epidural Analgesia
Factors with P values less than 0.1 for univariate analysis (Table 1), and the duration of the second stage of labor were included in the multivariate logistic regression to further analyze the main factors influencing PUR. The results suggested that lateral episiotomy (OR=4.55, 95% CI: 1.91–10.80), forceps-assisted delivery (OR=2.46, 95% CI: 1.14–5.32), and degree of perineal pain (OR=4.23, 95% CI: 2.05–8.73) were risk factors for overt PUR in women after vaginal delivery with labor epidural analgesia, as shown in Table 2.
 |
Table 2 Logistic Regression Analysis of Factors Influencing Overt PUR in Women After Vaginal Delivery with Labor Epidural Analgesia (n=462) |
Discussion
Current Incidence of Overt PUR in Women Undergoing Vaginal Delivery with Labor Epidural Analgesia
Overt PUR is symptomatic and need treatment, which would lead to persistent PRU if not treated properly; whereas, covert PUR is asymptomatic and mostly self-healing.2 Thus, the present research decided to concern postpartum women with overt PUR. On the basis of the worldwide literature, the average incidence of overt PUR was about 5.0%.2
The result of this study suggested that women undergoing vaginal delivery with labor epidural analgesia had an incidence of overt PUR of 10.2%, much higher than the incidence of 2.4% reported in the previous research on women after vaginal delivery without labor epidural analgesia.12 As revealed by a systematic review, the risk of PUR was 2.48 times higher in the group with labor epidural analgesia than in the group without labor epidural analgesia.7 Foon et al13 confirmed that the use of continuous epidural anesthesia during labor could result in the development of PUR, increasing the risk of acute PUR by three times as much as the usual rate. Existing research has noted that anesthetic drugs might interrupt the conduction signals between the spinal cord and the cerebral bridge, and the normal voiding reflex would be inhibited.14,15 As a result, the contraction and sensitivity of the internal urethral sphincter and detrusor muscle are reduced, which causes an increased risk of PUR. Labor analgesia is an independent high-risk factor for significant urinary retention, as indicated by a meta-analysis of 32,880 cases conducted by Mulder et al.14 Currently, the proportion of labor epidural analgesia has been rising year by year as pilot labor analgesia has been implemented in different hospitals across China.9,10 Since postpartum women with labor epidural analgesia belong to a high-risk group for overt PUR,2 medical and nursing staff should give more attention to the urination of these women and give timely treatment to reduce the incidence of overt PUR.
Moreover, the present study indicated that 231 (50.0%) postpartum women were induced to urinate during voiding, and 22 cases voided after application of Neostigmine MethylsuIFAte intramuscular injection. As revealed by the result, postpartum women undergoing vaginal delivery with labor epidural analgesia should be induced by clinical care providers to urinate as early as possible, and related methods (eg, massage, acupuncture, hot compresses, and listening to the sound of running water to induce urination) have been widely conducted in clinical practice. Extensive studies have verified the effectiveness of the above induction interventions.16,17 If the induction of voiding is ineffective at 4 h after delivery and the woman cannot urinate on her own, pharmacological interventions should be given promptly in conjunction with cystometry, and urethral catheterization is recommended if she cannot urinate on her own at 6 h after delivery.18
Effect of Forceps-Assisted Delivery on Overt PUR
The results of logistic regression analysis suggested that forceps-assisted delivery was one main risk factor of overt PUR for these postpartum women, which was in line with the previous research findings.2 Gupta et al19 have noted that the incidence of overt and covert PUR in women with forceps-assisted delivery is 20.6%. Forceps-assisted delivery is capable of damaging the urethral sphincter, Santorini muscle, and pelvic floor muscle to a certain extent, thus causing urinary disturbance.20 Pifarotti et al21 studied 105 patients with overt urinary retention and 300 controls, and found that the rate of forceps-assisted delivery in the overt urinary retention group is 31.1% compared with 7.4% in the control group. In this study, 44.7% of women in the overt PUR group underwent forceps-assisted delivery, which took up a large area in the birth canal, and the traction process may injure the pelvic floor, pubic muscles and nerves, resulting in abnormal reflexes, decreased bladder sensitivity, and dysfunction of the detrusor muscle and internal bladder sphincter.11 Besides, the traction of forceps even caused organ edema or congestion and damage to the perineum nerve and pelvis nerve, leading to impaired voluntary urination.19 The result suggested that the operation of forceps should be performed by experienced and trained medical personnel in strict accordance with the indications and operating principles. Furthermore, it is imperative for the operator to clearly identify the indications for using forceps, master the corresponding operating techniques, avoid violent pulling during the operation, and move gently to avoid damage to maternal soft tissues.22
Effect of Lateral Episiotomy and Perineal Pain on Overt PUR
The research findings suggested that lateral episiotomy and perineal pain were the main factors affecting overt PUR among postpartum women after vaginal delivery with labor epidural analgesia. The other research also reported that episiotomy was identified as an independent risk factor for PUR.2,6,12 In the present study, 39.8% of women with vaginal delivery and labor epidural analgesia underwent lateral episiotomy. Some studies have indicated that perineal pain was a direct result of lateral episiotomy, with over 90% of women feeling significant pain within 24 h after delivery and 88% of women experiencing pain relief until two months later.23 The mechanism is yet to be determined, but it may be that pain caused by perineal trauma leads to changes in bladder sensation, central nervous system inhibition, and persistent urethral spasm.24 Previous research has confirmed that moderate perineal protection techniques reduced perineal incision rates and perineal lacerations.25 Accordingly, the use of noninvasive delivery assistance techniques at the second stage of labor to control the delivery speed of the elevated head can reduce overt PUR due to perineal injury to a certain extent. Furthermore, pain-relieving treatments (eg, cold compresses on the perineum, far-infrared or low-intensity laser therapy, medication or psychotherapy) are actively given to women with lateral episiotomy to decrease the degree of pain after delivery and thus reduce the incidence of complications such as overt PUR.26
Influence of the Amount of Fluids Given During Labor on Overt PUR
Some research has shown that limiting fluid intake to less than 1000 mL during operation significantly reduces the incidence of urinary retention after surgery.27 Other studies have noted that fluid intake during labor is a high-risk factor for developing persistent PUR.28 It has been reported that intravenous access is routinely opened prior to labor analgesia to replenish maternal energy and facilitate the administration of medications, whereas there is a lack of uniformity in the clinical management of inflow for labor analgesia.29,30 It should be emphasized that the amount of fluid given during labor was not identified as one risk factor for overt PUR in this study, whereas the results in the univariate analysis revealed that the amount of fluid given during labor was significantly higher in the overt PUR group than in the non-urinary retention group. Since it may be correlated with the relatively small sample size with overt PUR and the high volume of fluids infused during labor in all participants of the present study. Therefore, the sample size should be continuously expanded in future research, and more attention should be paid to the effect of the volume of fluids infused during labor on PUR in depth.
Effect of Intrapartum Catheterization on Overt PUR
The result of this study indicated that the presence or absence of catheterization during labor was not one factor associated with the development of overt PUR, which is inconsistent with the findings of Polat et al.24 The prior study showed that women who are not catheterized during childbirth have a 2.2 times higher risk of developing PUR than women who are catheterized.24 Rosenberg et al likewise revealed that the number of urinary catheters inserted during labor and delivery in labor analgesic women is correlated with the incidence of PUR.11 It has been shown that infrequent catheterization can cause overfilling of the bladder, thus leading to underactivity of the detrusor muscle and voiding dysfunction;31 meanwhile, overfilling of the bladder may lead to bladder nerve damage and inhibition of bladder voiding reflex function.32 There are no national or international recommendations for intrapartum bladder management in women undergoing labor epidural analgesia. As a result, obstetric protocols for intrapartum and postpartum bladder management vary widely worldwide.33,34 The correlation between catheterization during labor and PUR was not reported in this study, probably because the majority (82.3%) of these women were catheterized during labor in this study. As a result, the number of women who were not catheterized during labor was relatively small, such that statistical difference results may not be obtained. The above finding reveals that future studies can further analyze the effect of whether catheterization during labor and the number of catheterizations on overt PUR.
Several limitations need to be noted in the current research. First, all study subjects were recruited in one hospital in Beijing that could limit the generalizability of the findings. Therefore, similar studies in other cities of China are strongly recommended to verify the results. Second, owing to the strict definitions of overt PUR and selection criteria, a relatively small study size was recruited. It could cause that the effects of the amount of fluids given during labor and whether to catheterize during labor on overt PUR in women with labor epidural analgesia were not reported in the present study, which should be explored in further research. Third, this cross-sectional survey cannot capture any dynamic changes in prevalence of overt PUR over time. A longitudinal study is anticipated in the future.
Conclusion
Postpartum women undergoing vaginal delivery with labor epidural analgesia had a high incidence of overt urinary retention. Thus, health-care providers should pay more attention to their postpartum urination status in these women in the clinical setting. In addition, research findings indicate that forceps-assisted delivery, episiotomy, and perineal pain were main factors affecting overt PUR for postpartum women after vaginal delivery with labor epidural analgesia. Effective and timely intervention is strongly recommended to reduce the occurrence of overt PUR for these kinds of postpartum women undergoing labor epidural analgesia, such as ones experienced forceps-assisted delivery, lateral episiotomy, and more severe perineal pain.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Ethics Approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Peking University People’s Hospital institutional ethics committee (Ethical approval number: 2023PHB036-001).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors thank all the postpartum women with labor epidural analgesia and vaginal delivery who participated in this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ain QU, Shetty N, S K. Postpartum urinary retention and its associated obstetric risk factors among women undergoing vaginal delivery in tertiary care hospital. J Gynecol Obstet Hum Reprod. 2021;50(2):101837. doi:10.1016/j.jogoh.2020.101837
2. Cao D, Rao L, Yuan J, Zhang D, Lu B. Prevalence and risk factors of overt postpartum urinary retention among primiparous women after vaginal delivery: a case-control study. BMC Pregnancy Childbirth. 2022;22(1):26. doi:10.1186/s12884-021-04369-1
3. Mulder FE, Hakvoort RA, Schoffelmeer MA, Limpens J, Van der Post JA, Roovers JP. Postpartum urinary retention: a systematic review of adverse effects and management. Int Urogynecol J. 2014;25(12):1605–1612. doi:10.1007/s00192-014-2418-6
4. Nutaitis AC, Meckes NA, Madsen AM, et al. Postpartum urinary retention: an expert review. Am J Obstet Gynecol. 2023;228(1):14–21. doi:10.1016/j.ajog.2022.07.060
5. Chen HT, Luo TZ, Jiang ZY, et al. Noninvasive external therapy of traditional Chinese medicine for preventing postpartum urinary retention in women with vaginal delivery: a network meta-analysis. Medicine. 2023;102(41):e35399. doi:10.1016/10.1097/MD.0000000000035399
6. Kawasoe I, Kataoka Y. Prevalence and risk factors for postpartum urinary retention after vaginal delivery in Japan: a case-control study. Jpn J Nurs Sci. 2020;17(2):e12293. doi:10.1111/jjns.12293
7. Li Q, Zhu S, Xiao X. The risk factors of postpartum urinary retention after vaginal delivery: a systematic review. Int J Nurs Sci. 2020;7(4):484–492. doi:10.1016/j.ijnss
8. Benítez-Andrades JA, García-Ordás MT, Álvarez-González M, Leirós-Rodríguez R, López Rodríguez AF. Detection of the most influential variables for preventing postpartum urinary incontinence using machine learning techniques. Digit Health. 2022;8:20552076221111289. doi:10.1177/20552076221111289
9. Fu CY, Wang LZ, Tang XJ, Xia F. Association of labor epidural analgesia use with exclusive breastfeeding up to six months: a online-based cross sectional survey in Jiaxing, China. BMC Pregnancy Childbirth. 2022;22(1):973. doi:10.1186/s12884-022-05332-4
10. Tong S, Rao C, Min S, et al. Obstetric anesthesia clinic childbirth course combined with labor epidural analgesia is associated with a decreased risk of postpartum depression: a prospective cohort study. BMC Anesthesiol. 2022;22(1):389. doi:10.1186/s12871-022-01931-y
11. Rosenberg M, Many A, Shinar S. Risk factors for overt postpartum urinary retention-The effect of the number of catheterizations during labor. Int Urogynecol J. 2020;31(3):529–533. doi:10.1007/s00192-019-04010-y
12. Suzuki S, Kakizaki E, Kobayashi R, Teshima S. Risk factors for postpartum urinary retention after vaginal delivery at term without epidural anesthesia. J Matern Fetal Neonatal Med. 2019;32(20):3470–3472. doi:10.1080/14767058.2018.1465559
13. Foon R, Toozs-Hobson P, Millns P, Kilby M. The impact of anesthesia and mode of delivery on the urinary bladder in the postdelivery period. Int J Gynaecol Obstet. 2010;110(2):114–117. doi:10.1016/j.ijgo.2010.03.024
14. Mulder FE, Schoffelmeer MA, Hakvoort RA, et al. Risk factors for postpartum urinary retention: a systematic review and meta-analysis. BJOG. 2012;119(12):1440–1446. doi:10.1111/j.1471-0528.2012.03459.x
15. Choe WS, Kwang NB, Atan IK, Lim PS. Acceptable postvoid residual urine volume after vaginal delivery and its association with various obstetric parameters. Obstet Gynecol Int. 2018;2018:5971795. doi:10.1155/2018/5971795
16. Zhu Y, Wang F, Zhou J, et al. Effect of acupoint hot compress on postpartum urinary retention after vaginal delivery: a randomized clinical trial. JAMA Netw Open. 2022;5(5):e2213261. doi:10.1001/jamanetworkopen
17. Chen HZ. Research progress on the causes and care of postpartum urinary retention. Chin Nurs Res. 2016;30(16):1924–1927. doi:10.3969/j.issn.1009-6493.2016.16.002 In Chinese.
18. Jiang LJ, Lin L. Research progress of postpartum urinary retention. Chin J Clin Obstet Gynecol. 2018;19(4):372–374. doi:10.13390/j.issn.1672-1861.2018.04.027 In Chinese.
19. Gupta A, Pampapati V, Khare C, Murugesan R, Nayak D, Keepanasseril A. Postpartum urinary retention in women undergoing instrumental delivery: a cross-sectional analytical study. Acta Obstet Gynecol Scand. 2021;100(1):41–47. doi:10.1111/aogs.13954
20. Kekre AN, Vijayanand S, Dasgupta R, Kekre N. Postpartum urinary retention after vaginal delivery. Int J Gynaecol Obstet. 2011;112(2):112–115. doi:10.1016/j.ijgo.2010.08.014
21. Pifarotti P, Gargasole C, Folcini C, et al. Acute post-partum urinary retention: analysis of risk factors, a case-control study. Arch Gynecol Obstet. 2014;289(6):1249–1253. doi:10.1007/s00404-014-3144-5
22. Evanson SM, Riggs J. Forceps Delivery. 2022. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
23. Shahrahmani H, Kariman N, Jannesari S, et al. The effect of green tea ointment on episiotomy pain and wound healing in primiparous women: a randomized, double-blind, placebo-controlled clinical trial. Phytother Res. 2018;32(3):522–530. doi:10.1002/ptr.5999
24. Polat M, Şentürk MB, Pulatoğlu Ç, Doğan O, Kılıççı Ç, Budak MŞ. Postpartum urinary retention: evaluation of risk factors. Turk J Obstet Gynecol. 2018;15(2):70–74. doi:10.4274/tjod.43931
25. Ma DM, Hu W, Wang YH, Luo Q. A multicentre study on the effect of moderate perineal protection technique: a new technique for perineal management in labour. J Obstet Gynaecol. 2020;40(1):25–29. doi:10.1080/01443615.2019.1587605
26. Lu YX, Liu SY, Peng W. Advances in the treatment of pain after lateral episiotomy. Perioperat Safety Qual Assur. 2021;6:455–459. In Chinese.
27. Petros JG, Bradley TM. Factors influencing postoperative urinary retention in patients undergoing surgery for benign anorectal disease. Am J Surg. 1990;159(4):374–376. doi:10.1016/s0002-9610(05)81274-7
28. Tiberon A, Carbonnel M, Vidart A, Ben Halima M, Deffieux X, Ayoubi JM. Risk factors and management of persistent postpartum urinary retention. J Gynecol Obstet Hum Reprod. 2018;47(9):437–441. doi:10.1016/j.jogoh.2018.08.002
29. Chen XF, Sun XQ, Chen ZF, Xin DD, Zhang WX. Comparison of varied intake management approaches during painless delivery. J Nurs Sci. 2020;35(14):25–28. doi:10.3870/j.issn.1001-4152.2020.14.025 In Chinese.
30. Sperling JD, Dahlke JD, Sibai BM. Restriction of oral intake during labor: whither are we bound? Am J Obstet Gynecol. 2016;214(5):592–596. doi:10.1016/j.ajog.2016.01.166
31. Groutz A, Levin I, Gold R, Pauzner D, Lessing JB, Gordon D. Protracted postpartum urinary retention: the importance of early diagnosis and timely intervention. Neurourol Urodyn. 2011;30(1):83–86. doi:10.1002/nau.20926
32. Madersbacher H, Cardozo L, Chapple C, et al. What are the causes and consequences of bladder overdistension? ICI-RS 2011. Neurourol Urodyn. 2012;31(3):317–321. doi:10.1002/nau.22224
33. Zaki MM, Pandit M, Jackson S. National survey for intrapartum and postpartum bladder care: assessing the need for guidelines. BJOG. 2004;111(8):874–876. doi:10.1111/j.1471-0528.2004.00200.x
34. Napoe GS, Adjei NN, Cooper AC, Raker CA, Korbly NB. Postpartum urinary retention: a survey of obstetrics and gynaecology residents in the United States. J Obstet Gynaecol. 2020;40(8):1118–1121. doi:10.1080/01443615.2019.1706159
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Scoping Review on the Status of Female Breast Cancer in Asia with a Special Focus on Nepal
Dhakal R, Noula M, Roupa Z, Yamasaki EN
Breast Cancer: Targets and Therapy 2022, 14:229-246
Published Date: 26 August 2022
Incidence and Risk Factors for Retinopathy of Prematurity in a Tertiary Hospital in China
Hu X, Zhang J, Zhang M, Chen X, Han S, Zhu J
Clinical Ophthalmology 2023, 17:3189-3194
Published Date: 25 October 2023
Risk Factors for Postpartum Hemorrhage Following Vaginal Deliveries in China: A Case-Control Study of Second Births After IUD Removal
Shen L, Xu Y, Li B, Long Y
International Journal of Women's Health 2025, 17:1203-1214
Published Date: 1 May 2025
Incidence and Risk Factors for Progression from Pre-COPD to COPD: A Systematic Review and Meta‑analysis
Qiao L, Wu X, Chen G, Tang H, Shen H
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:566518
Published Date: 13 February 2026
Incidence and Risk Factors of Chemotherapy-Induced Hepatotoxicity: A Cross-Sectional Study
Joel S, Bukke SPN, Mamilla Mugaiahgari BK, Kyomya J, Idrine KK, Godwin N, Muasya PK, Abdi AA, Makuza KR, Tumwebaza JM, Narapureddy BR, Goruntla N, Mwandah DC, Shogar AE, Abdalla SA, Isiiko J, Yadesa TM
Cancer Management and Research 2026, 18:589840
Published Date: 25 March 2026