Back to Journals » Cancer Management and Research » Volume 18

Identifying of Ubiquitin-Fold Modifier 1 as a Potential Prognostic Biomarker for Unresectable Pancreatic Cancer by Proteomics Analysis
Authors Wang J, Xu K, Xu L, Geng J, Liu C, Gu X, Li X ![]()
Received 31 October 2025
Accepted for publication 19 February 2026
Published 24 February 2026 Volume 2026:18 573143
DOI https://doi.org/10.2147/CMAR.S573143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Juan Wang,1 Kun Xu,2 Longjin Xu,3 Jiaxiao Geng,4 Chengxin Liu,4 Xinhang Gu,4 Xiaodong Li5
1Department of Radiation Oncology, The Affiliated Hospital of Qingdao University, Qingdao, Shandong, People’s Republic of China; 2Department of Colorectal Surgery, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 3Department of Health Inspection and Testing Institute, Shandong Center for Disease Control and Prevention, Jinan, Shandong, People’s Republic of China; 4Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, People’s Republic of China; 5Department of Radiation Oncology, Gansu Provincial Maternity and Child-Care Hospital (Gansu Provincial Central Hospital), Lanzhou, Gansu, People’s Republic of China
Correspondence: Xiaodong Li, Department of Radiation Oncology, Gansu Provincial Maternity and Child-Care Hospital (Gansu Provincial Central Hospital), Lanzhou, Gansu, People’s Republic of China, Email [email protected] Xinhang Gu, Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, 250117, People’s Republic of China, Email [email protected]
Background: The prognosis for unresectable pancreatic cancer remains poor, with limited biomarkers available to predict treatment response and survival. This study aimed to identify novel protein biomarkers associated with therapeutic resistance in this disease.
Methods: We performed proteomic analysis by Data-Independent Acquisition mass spectrometry on FFPE tissues from 10 patients with unresectable pancreatic cancer, comparing treatment-sensitive and treatment-resistant groups. Differentially expressed proteins were identified, and the candidate was validated by immunohistochemistry in an independent cohort of 91 patients. Survival analysis and Cox regression were used to evaluate the prognostic significance of protein expression.
Results: In this study, proteomic analysis revealed Ubiquitin-fold modifier 1 (UFM1) as a significantly upregulated protein in treatment-resistant. High UFM1 expression was significantly associated with advanced TNM stage (P < 0.05) and poorer treatment response (P = 0.016). Patients with high UFM1 expression had significantly shorter median PFS (6.5 vs 12.0 months; HR = 0.335, 95% CI: 0.209– 0.537, P < 0.001) and OS (10.4 vs 20.5 months; HR = 0.298, 95% CI: 0.184– 0.484, P < 0.001) compared to those with low expression. Multivariate Cox regression confirmed UFM1 as an independent prognostic factor for both PFS (HR = 0.343, P < 0.001) and OS (HR = 0.304, P < 0.001).
Conclusion: UFM1 is a promising prognostic biomarker for unresectable pancreatic cancer, with high expression indicating aggressive disease and inferior outcomes. These findings support its potential utility in risk stratification and treatment personalization.
Keywords: pancreatic cancer, ubiquitin-fold modifier 1, prognosis, biomarker, proteomic
Introduction
Pancreatic cancer, a highly lethal malignancy of the digestive system, is linked to an increasing prevalence and mortality rate globally, particularly in cases of unresectable pancreatic cancer, including locally advanced and metastatic pancreatic cancer.1 With 30–35% of the cases being diagnosed as locally advanced and 50–55% as metastatic, surgical intervention is no longer an option for most patients.2,3 The prognosis for unresectable pancreatic cancer is extremely poor, with a 5-year survival rate of 5%–10%.4 This poses a significant challenge in clinical management.
The current treatments for unresectable pancreatic cancer include chemotherapy, radiotherapy, and anti-angiogenic therapy. However, despite recent advancements in research, the overall therapeutic outcomes remain unsatisfactory. For instance, a Phase II clinical study demonstrated that gemcitabine combined with albumin-paclitaxel converted unresectable disease to surgically resectable disease in only 16% (17/106) of the patients.5 The MPACT study revealed that the median OS in the nab-paclitaxel plus gemcitabine group was 8.5 months, with 20% (80/431) of patients experiencing progressive disease (PD) as the best response.6 In addition, emerging therapies, including immunotherapy and targeted therapies, have demonstrated limited promise for treating unresectable patients with pancreatic cancer. The phase II trial of sotolacib for the treatment of patients harboring the KRAS G12C mutation has shown enhanced efficacy; however, the median progression-free survival (PFS) was only 4.0 months (95% CI, 2.8–5.6), and the median overall survival (OS) was 6.9 months.7 The Check PAC study demonstrated that the combination of nivolumab and ibritumomab with radiotherapy yielded a higher clinical benefit rate (34.2% vs 17.1%) in patients with metastatic pancreatic cancer. However, the median OS of patients in both treatment arms was only 3.8 months.8 These data indicate that current treatment regimens confer limited benefits to the outcome of unresectable pancreatic cancer.
The pathogenesis of pancreatic cancer and its recalcitrance to therapy are driven by a confluence of genetic, cellular, and microenvironmental factors.9–11 Genetically, sequential alterations in drivers such as KRAS, TP53, CDKN2A, and SMAD4 orchestrate tumor initiation and progression.12–14 At the cellular level, reprogrammed metabolism and dysregulated DNA damage response (DDR) pathways further promote survival and adaptation.15 Perhaps most critically, the tumor microenvironment in pancreatic cancer is characterized by a dense fibroinflammatory stroma that fosters immunosuppression through the recruitment of regulatory T cell, myeloid-derived suppressor cell, and tumor-associated macrophages,16,17 while simultaneously creating a physical and biochemical barrier to drug delivery.18
Circulating biomarkers remain central to non-invasive monitoring. Carbohydrate antigen 19–9 (CA19-9) is the most widely utilized serum marker, holding significant value in the diagnosis, assessment of treatment response, and detection of recurrence in pancreatic ductal adenocarcinoma (PDAC). CA19-9 is the sole FDA-approved serum biomarker for the early detection, progression, and monitoring of treatment response in pancreatic cancer. Serum CA19-9 levels correlate with therapeutic response and overall survival in PDAC patients.19,20 However, the utility of CA19-9 in predicting baseline therapeutic efficacy is suboptimal due to its moderate specificity and susceptibility to false elevations in benign biliary conditions.21 Circulating tumor DNA (ctDNA), particularly profiling of KRAS mutations, is a rapidly advancing field. KRAS gene mutations are present in nearly all PDACs, making ctDNA KRAS a candidate alternative disease biomarker.22 The ultrasensitive nature of ctDNA detection highlights its potential for use in the detection, prognosis, and assessment of therapeutic response in PDAC. It shows promise for real-time monitoring of tumor dynamics, minimal residual disease, and emerging resistance mechanisms, yet its standardization for routine prognostication and its cost-effectiveness require further validation.23,24 Research efforts have identified other potential biomarkers, including human equilibrative nucleoside transporter 1 (hENT1) for gemcitabine sensitivity.25 SMAD4 loss associated with a more aggressive phenotype, and various stromal or immune signatures.26,27 However, the translation of these markers into routine clinical prognostication and decision-making has been hampered by a lack of standardization in assay methods and validated cut-off values.
Post-translational modifications, particularly those within the ubiquitin and ubiquitin-like modifier (UBL) systems, are fundamental regulators of the oncogenic processes described above. Ubiquitin-fold modifier 1 (UFM1) is a recently characterized UBL that is conjugated to target proteins via a dedicated enzymatic cascade—a process termed ufmylation.28,29 This cascade involves the E1 activating enzyme UBA5, the E2 conjugating enzyme UFC1, and the primary E3 ligase UFL1 (the “writer”).29,30 This modification can be reversed by the specific protease UFSP2 (the “eraser”). Ufmylation is essential for cellular processes relevant to cancer, including endoplasmic reticulum homeostasis, the DNA damage response, and the regulation of cell proliferation and survival.30–32 Perturbations in the UFM1 pathway have been implicated in the pathogenesis and poor prognosis of several malignancies, such as oral squamous cell carcinoma and gastric cancers.33,34 Given its central role in managing cellular stress and promoting survival, we hypothesized that the UFM1 system might be a critical, yet unexplored, contributor to therapeutic resistance in pancreatic cancer.
In light of the limitations of current biomarkers and the urgent need for reliable predictors of therapeutic response in unresectable pancreatic cancer, this study aimed to identify novel protein biomarkers associated with treatment resistance using a proteomics approach. Specifically, we sought to evaluate the prognostic significance of UFM1 and its potential utility in clinical risk stratification.
Materials and Methods
Patients and Sample Collection
A total of 10 formalin-fixed and paraffin-embedded (FFPE) specimens from 10 patients with pretreated, unresectable pancreatic cancer were collected for proteomic analysis. The treatment-sensitive group consisted of five patients with a survival duration exceeding 550 days; those meeting the criteria for Partial Response (PR) were included in this cohort. The treatment-resistant group consisted of five patients who experienced rapid progression after three courses of treatment. In addition, a cohort of 91 patients with unresectable pancreatic cancer was identified for immunohistochemistry (IHC) and survival analyses. All these patients were treated at Shandong Cancer Hospital between January, 2018, and January, 2021. The study follow-up period extended from the time of initial diagnosis to the last follow-up date in August 2023, with survival outcomes recorded accordingly. Clinical data, including age, sex, stage, and treatment modalities, were obtained from the patients’ medical records. The efficacy of the treatment was evaluated in accordance with the RECIST 1.1 criteria, and the survival time of the patients was also documented. All FFPE tissue samples used for immunohistochemical analysis were reviewed by an experienced pathologist to confirm the presence of representative tumor regions prior to staining.
Dewaxing Treatment and Pressure Cycling Technology-Based Protein Digestion
The staining rack with the FFPE samples was placed in the 37°C oven for 30 min. Heptane was then added to the staining jar in which the sample was submerged and the lid placed to cover the jar. After 10 min of standing at ambient temperature, the liquid was discarded; this process of addition of heptane and discarding the liquid was repeated. Next, 100% ethanol was added to the staining jar to cover the sample and the lid used to cover the jar and discard the liquid. Then, 90% ethanol and 75% ethanol were added in that order and the liquids discarded each time. Deionized water was added to the staining jar to soak the sample; the samples were then taken out individually and transferred to pressure cycling technology (PCT) tubes (Pressure BioSciences, South Easton, USA) with a blade. After adding 12.5 μL of 100 mM Tris hydrochloride (Tris-HCl, pH = 10) to the PCT tubes containing the samples, the tubes were agitated on a horizontal shaker (Thermo Fisher Scientific, Waltham, USA) at 600 rpm for 30 min at 95°C. Next, 6 M urea/2 M thiourea/100 mM triethylammonium bicarbonate (TEAB, 30 μL), 200 mM Tris (2-carboxyethyl) phosphine (TCEP, 5 μL), and 800 mM iodoacetamide (IAA, 2.5 μL) was added to conduct reduction and alkylation reactions using a PCT System (Pressure BioSciences, South Easton, USA) at 45,000 psi for a total of 90 cycles at 30°C; every cycle included 30s of high pressure and 10s of ambient pressure. TEAB (85 μL) was added to the PCT tubes to lower the urea concentration to <1.5 M. Thereafter, we added 10 μL of trypsin (0.5 μg/μL) and 5 μL of Lys-C (0.25 μg/μL) to digest the proteins at 20,000 psi for a total of 120 cycles at 30°C; every cycle included 50s of high pressure and 10s of ambient pressure. We transferred the trypsinized peptides to 1.5-mL tubes and added 10% TFA (15 μL) to terminate the reaction. The sample pH was confirmed to be 2–3. The samples were then desalted with SOLAμ (Thermo Fisher Scientific™, San Jose, USA), and the desalted peptide samples were sent for mass spectrometric (MS) analysis.
Mass Spectrometry
An ultrahigh performance liquid chromatography (UHPLC) system (Bruker Daltonics, Bremen, Germany) – nanoElute model – coupled with a timsTOF Pro mass spectrometer (Bruker Daltonics, Bremen, Germany) equipped with a CaptiveSpray ion source was used to conduct liquid chromatography–mass spectrometry for data-independent acquisition (DIA). Mobile phase A consisted of 100% water with 0.1% formic acid, and mobile phase B comprised 100% acetonitrile with 0.1% formic acid. Every reagent used was of MS grade (Thermo Fisher Scientific, Waltham, USA).
For the proteomic analysis, we employed DIA for all samples during which we initially added peptides onto a pre-column (Bruker Acclaim PepMap 100 C18, 5 mm × 300 µm internal diameter [i.d.], 5 µm particle size, 100 Å pore size) at 217.5 bar before adding them to an analytical column (Bruker Acclaim PepMap RSLC C18, 1.9 µm particle size, 120 Å pore size, 150 mm × 75 µm i.d.) maintained at 40°C. The flow rate was set to 300 nL/min and examined them with a 60-min LC gradient (0–50 min, 5–27% B; 50–60 min, 27–40% B). Mass spectrometry parameters included PASEF MS mass scanning at 100–1700 m/z, 1/k0 scanning at 0.6–1.6, and a peak detection threshold at 5000 counts; PASEF MS/MS scanning count set to 10, charge of 0–5, and peak detection threshold at 2500 counts per second (cts/s).
MS Data Processing
DIA-NN (1.8.1) and the Human protein database accessed at UniProtKB on 15 May 2023 (Fasta file including 42,431 reviewed protein sequences) were employed to analyze the MS data, with the false discovery rate being set at 0.01. The data were normalized to the total peptide level. All other parameters were at default values.
Statistical and Bioinformatics Analyses
A total of 9522 proteins were detected from 10 pancreatic cancer FFPE tissue samples, with an overall missing rate of 10.51%. We used seqKNN v1.0.1 to impute the missing values and handle outliers in the data. To compare protein levels in different groups, we computed log2 (fold change) based on average values. The group pair was examined using two-sided unpaired Welch’s t-test. Finally, B-H correction was utilized to determine adjusted P-values. We defined B-H adjusted P-values as <0.05 and |log2 (fold change) >0.585 to select differentially expressed proteins.
All the statistical and bioinformatics analyses were performed in R (v.4.0). The missing value was imputed with 0. We carried out principal component analysis for visualizing group separation using the statistics package of R. Moreover, this study utilized R package cluster Profiler for performing gene ontology and Kyoto Encyclopedia of Genes and Genomes analyses. GSEA was implemented using the R/Bioconductor package clusterProfiler. Fold changes in proteins were ranked in a descending manner for both phenotypes. Later, the whole list was used for assessing the gene set distribution for the determination of the enrichment score during GSEA.
Multiple Immunofluorescence Analysis (mIF) and Multichannel Imaging
Deparaffinization of tissue sections was done through the addition of a gradient of xylene solutions and rehydration done by the addition of a decreasing gradient of ethyl alcohol. AR6 buffer (Akoya Biosciences, Marlborough, USA) was used for antigen retrieval in a microwave oven (Panasonic, Osaka, Japan) set to 750 W for 15 min. Endogenous peroxidase was inactivated by incubation in 3% H2O2 for 10 min. Multiplex immunohistochemistry was performed by several rounds of staining, each including a protein block with 1% bovine serum albumin followed by the addition of a primary antibody and the corresponding secondary horseradish peroxidase-conjugated anti-mouse and anti-rabbit immunoglobulins (Akoya Biosciences, Marlborough, USA). The slides were then incubated in different Opal fluorophores (1:100) diluted in 1X Plus Amplification Diluent (Akoya Biosciences, Marlborough, USA). After tyramide signal amplification and covalent linkage of the individual Opal fluorophores (Akoya Biosciences, Marlborough, USA) to the relevant epitope or epitopes, the primary and secondary antibodies were removed via antigen retrieval as previously mentioned and the next cycle of immunostaining was initiated. The sequence of primary antibody and Opal fluorophore was anti-CK (ZM-0069, dilution 1:200, ZSGB-BIO, Beijing, China)/Opal 480 and anti-UFM1 (AB109305, dilution 1:200, Abcam, Cambridge, UK)/Opal 520. All slides were counterstained with spectral 4’,6-diamidino-2-phenyldindole (DAPI, Akoya Biosciences, Marlborough, USA) and mounted with Anti-fade fluorescence mounting medium (ab104135, Abcam, Cambridge, UK). Multichannel imaging was performed on a PANNORAMIC SCAN II Imaging System (3Dhistech, Budapest, Hungary) equipped with a 20× Plan-Apochromat objective (numerical aperture = 0.8). Fluorescence signals were captured using specific filter sets: Opal 480 (excitation/emission: 470/500 nm), Opal 520 (500/530 nm), and DAPI (350/470 nm), with exposure times optimized to avoid signal saturation (Opal 480: 500 ms; Opal 520: 600 ms; DAPI: 300 ms). Image analysis was conducted using CaseViewer software (v2.4, 3Dhistech, Budapest, Hungary). The slides were imaged at ×200 magnification.
IHC
Pre-treatment pathological specimens were collected from a validation cohort comprising 91 patients with unresectable pancreatic cancer and subjected to immunohistochemical staining using a Leica Bond-Max automated staining system (Leica Biosystems, Wetzlar, Germany) following the manufacturer’s standard protocol to analyze protein levels. Briefly, deparaffinization and rehydration were performed automatically, followed by antigen retrieval with AR6 buffer (Akoya Biosciences, Marlborough, USA) at 95°C for 20 min. Sections were blocked with 1% bovine serum albumin for 30 min and incubated with anti-UFM1 antibody (AB109305, dilution 1:200, Abcam, Cambridge, UK) at 4°C overnight. After washing with phosphate-buffered saline (PBS), sections were incubated with a horseradish peroxidase-conjugated secondary antibody (ZSGB-BIO, Beijing, China) for 30 min at room temperature, followed by visualization with 3,3’-diaminobenzidine (DAB) substrate (ZSGB-BIO, Beijing, China) and counterstaining with hematoxylin. Stained slides were scanned using a PANNORAMIC SCAN II Imaging System (3Dhistech, Budapest, Hungary) at ×40 magnification. The percentage of protein-positive cells was quantified using QuPath software (v0.4.4, University of Edinburgh, UK) with a standardized thresholding algorithm. Using the median value (43.8%) as the cutoff, patients were classified into high- and low-expression groups.35,36
Statistical Analysis
Any discrepancy in protein intensities in both groups was determined using a two-sided Student’s t-test. Differences in baseline characteristics between both groups were assessed by Chi-square and Fisher’s exact tests; the relationship between the treatment response and clinicopathological factors was also evaluated. Univariate as well as multivariate regression was performed using Cox proportional hazard models for identifying variables independently for predicting PFS and OS. We also employed the Kaplan–Meier method for assessing the PFS and OS of the patients, followed by a log rank to compare the rates. P < 0.05 indicated significant differences, with all tests being two-tailed. Data analyses and graphing were conducted using SPSS software (v 27.0) and R software (v 4.3.2.3).
Results
UFM1 as a Differentially Expressed Protein Related to Treatment Sensitivity
To unravel the molecular mechanisms related to treatment response and survival outcomes, we conducted ad hoc proteomic profiling. A total of 9522 proteins were identified from 10 pancreatic cancer FFPE tissue sample. There were 226 differentially expressed proteins between the treatment-resistant and treatment-sensitive groups (Figure 1A). Compared to the treatment-resistant group, 122 proteins were upregulated in the treatment-sensitive group (eg PDGFA, Log2FC=+0.75; GXYLT2, Log2FC=+0.88; CCN1, Log2FC=+0.11; SRPX2, Log2FC =+1.23; and SERPINB2, Log2FC =+1.84;), while 104 proteins were downregulate (e.g, UFM1, Log2FC =−0.72; CMPK1, Log2FC=−0.79; NHERF1, Log2FC=−1.01; NIPSNAP2, Log2FC =−0.77; and AKR7A3, Log2FC =−1.66)(see Figure 1B). The proteins that were highly expressed in the treatment-resistant group are implicated in several pathways, including cellular aldehyde (metabolic), fructose 1,6−bisphosphate (metabolic), cellular amino acid (catabolic), cellular amino acid (catabolic), fibroblast activation, and alpha−amino acid (catabolic) processes (Figure 1C).
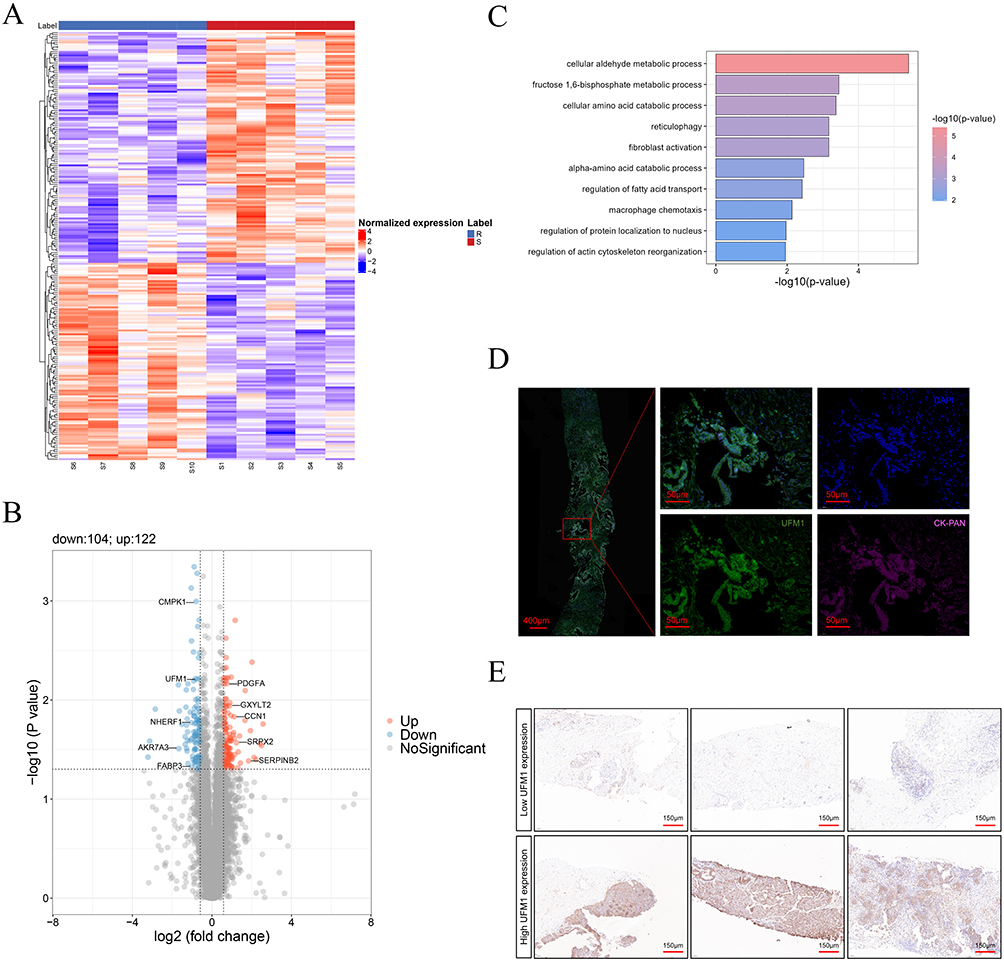 |
Figure 1 Proteomic analysis of patients with unresectable pancreatic cancer and representative immunohistochemical and multiplex immunofluorescence images of the target proteins. (A) Heatmap representation of the abundance profiles of all proteins in treatment-resistant and - sensitive groups. Colors represent normalized gene expression levels: red indicates high expression, and blue indicates low expression. (B) Volcano plot of differentially expressed proteins (red, up; blue, down; gray, nonsignificant). Key candidates, including UFM1, are labeled. (C) Bar graph illustrating enriched pathways identified based on significantly upregulated/downregulated proteins. (D) A multispectral mixed image of panel 1 from the mIF showing representative illustrations of tumor cells and UFM1. The red box demarcates a region of interest (with a magnified inset showing details of this region). The scale bar indicates the actual length in the image. (E) Representative immunohistochemical images of PDAC tissues with high and low expression of UFM1. Images show staining results for different experimental group. Brown staining indicates positive expression of the target protein. The scale bar indicates the actual length in the image. Abbreviations: mIF, multiplex immunofluorescence; PDAC, pancreatic ductal adenocarcinoma; UFM1, Ubiquitin-fold modifier 1. |
The pivotal role of UFM1 in post-translational modification pathways, including protein modification and regulation, cellular stress responses, as well as cell survival and proliferation, coupled with recent literature reports emphasizing the significance of UFM1 in the onset and prognosis of various tumors,37–39 further substantiates its high relevance to our study. Consequently, we selected UFM1 for in-depth analysis. As shown in Figure 1D, UFM1 is present in the cytoplasm of epithelial cells. Its expression within the tumor was significantly higher in the treatment-resistant group than in the treatment-sensitive group, as evidenced by IHC images from the cohort (Figure 1E). These findings indicate that UFM1 may be useful as a biomarker for predicting the treatment response in patients with unresectable pancreatic cancer.
Patients’ Baseline Characteristics in Validation Cohort
All patients enrolled in this study had a definitive pathological diagnosis of pancreatic cancer, as determined by hematoxylin and eosin and IHC staining. The validation cohort of IHC specimens ultimately comprised 91 patients, including 56 (61.5%) males and 35 (38.5%) females, with a median age of 63 years (range 35–81years). The median rate of UFM1-positive cells was 43.8%. A total of 37 (40.7%) patients were classified as stage III, while 54 (59.3%) were classified as stage IV. Of the stage IV patients, 14 (25.9%) received a combination of radiotherapy and chemotherapy, while 40 (74.1%) received chemotherapy alone. In contrast, 25 (67.5%) of the stage III patients received a combination of radiotherapy and chemotherapy, while 12 (32.5%) received chemotherapy alone. No correlation was observed between UFM1 protein levels and patient characteristics such as sex, age, Eastern Cooperative Oncology Group performance status, T stage, and N stage (P > 0.05). However, a correlation was observed with respect to the TNM stage (AJCC 8th edition), with a higher proportion of patients with stage IV in the high UFM1 expression group than in the low-UFM1-expression group (see Table 1, Figure 2A and B).
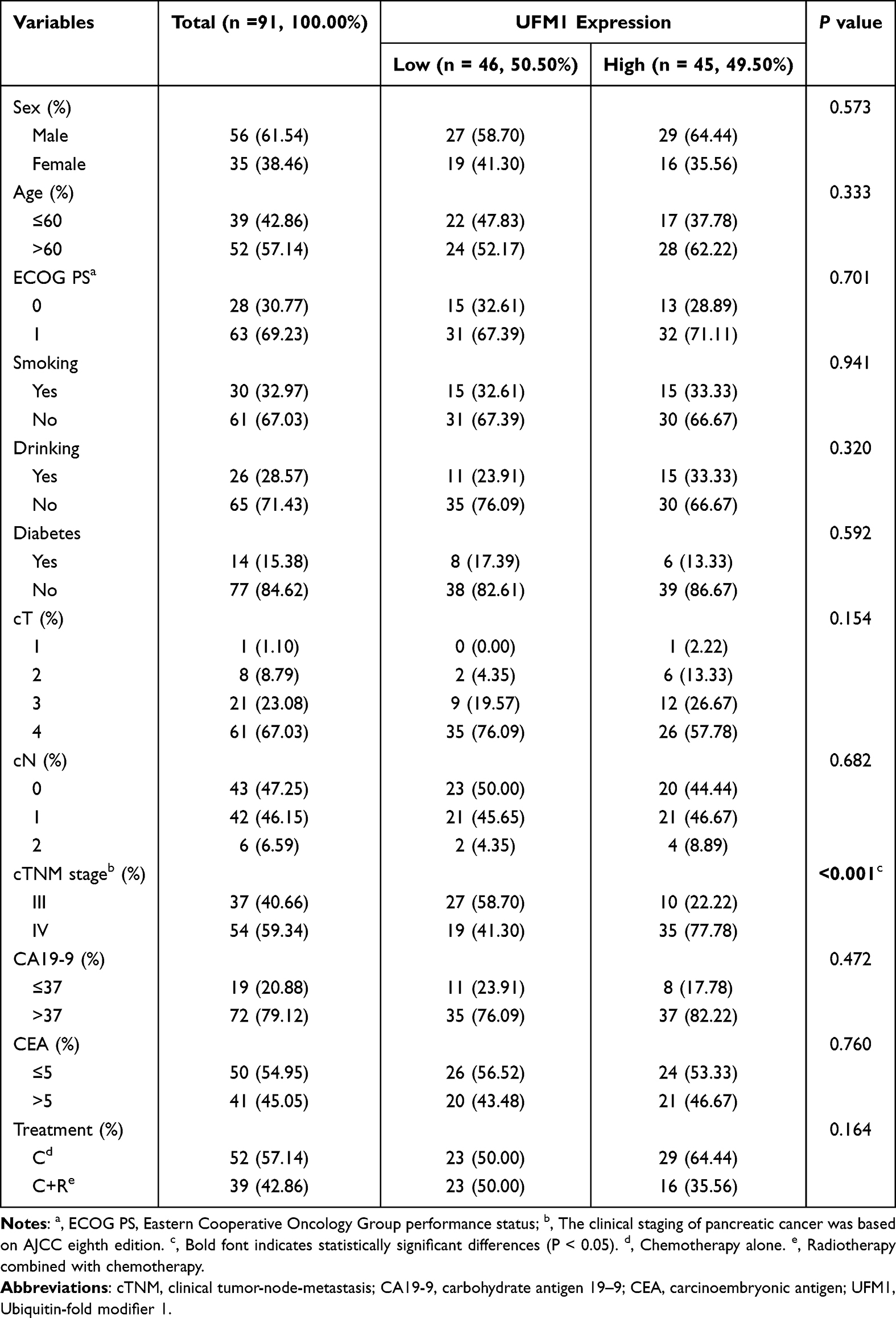 |
Table 1 Clinicopathologic Characteristics of Patients in Different UFM1 Expression Levels |
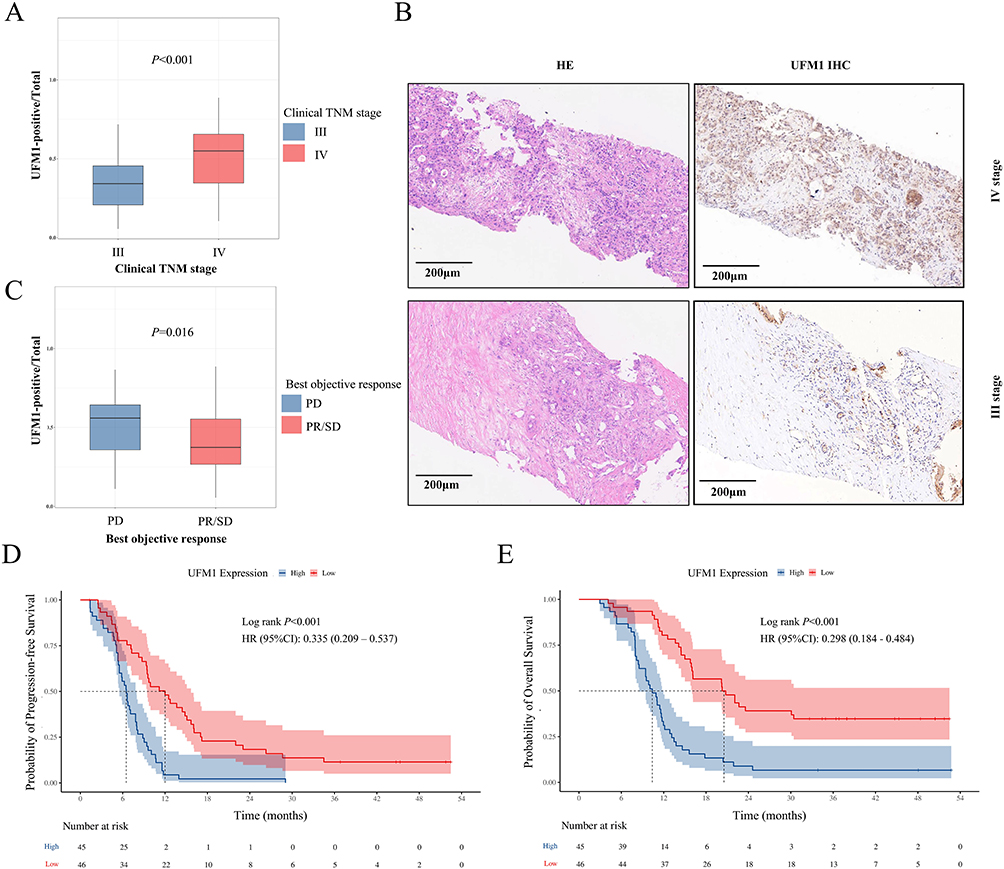 |
Figure 2 UFM1 expression is associated with advanced disease stage, poor treatment response, and unfavorable survival in unresectable pancreatic cancer. (A) UFM1 expression levels measured by IHC are significantly higher in patients with TNM stage IV disease compared to those with stage III. Data are presented as box plots. (B) Representative images of HE staining and UFM1 IHC in tumor tissues. (C) UFM1 expression levels are significantly higher in patients with PD as their best objective response compared to those with PR or SD. (D) Kaplan-Meier curves show PFS for patients stratified by UFM1 expression levels (High vs Low, using the median IHC value as the cutoff). (E) Kaplan-Meier curves show OS for patients stratified by UFM1 expression levels. Abbreviations: UFM1, Ubiquitin-fold modifier 1; HE, hematoxylin and eosin; IHC, immunohistochemistry; TNM, tumor-node-metastasis; PR, partial response; SD, stable disease; PD, progressive disease; PFS, progression-free survival; OS, overall survival. |
Outcomes Correlated with UFM1 Expression Levels
Among the 91 patients, 27 achieved a PR as their best objective response, 33 had stable disease (SD), and 31 showed PD. The proportion of UFM1-positive cells was significantly lower in the PR + SD group compared to the PD group (P= 0.016, Figure 2C).
The results of the survival analysis indicated that the median PFS in the low UFM1 expression group was significantly longer than in the high UFM1 expression group (12.0 months vs 6.5 months, HR = 0.335, 95% CI: (0.209, 0.537), P < 0.001, Figure 2D). The median OS in the low UFM1 expression group was 20.5 months, while the median OS in the high UFM1 expression group was 10.4 months. Thus, the high expression group exhibited a significantly lower median OS than the low expression group (HR = 0.298, 95% CI: 0.184, 0.484, P < 0.001, Figure 2E).
The better survival outcomes of the low UFM1 expression group compared with the high UFM1 expression group appeared to be consistent across all patient subgroups. In patients who received chemotherapy alone, the median PFS (HR = 0.214, 95% CI: 0.102–0.451, P<0.001, Figure 3A) and OS (HR = 0.242, 95% CI: 0.126–0.465, P<0.001, Figure 3B) were longer in the low UFM1 expression group than in the high UFM1 expression group. In patients who received a combination of radiotherapy and chemotherapy, the low UFM1 expression group showed a better median PFS (HR = 0.471, 95% CI: 0.235–0.944, P = 0.030, Figure 3C) and OS (HR = 0.380, 95% CI, 0.174–0.832, P = 0.012, Figure 3D) than the high UFM1 expression group.
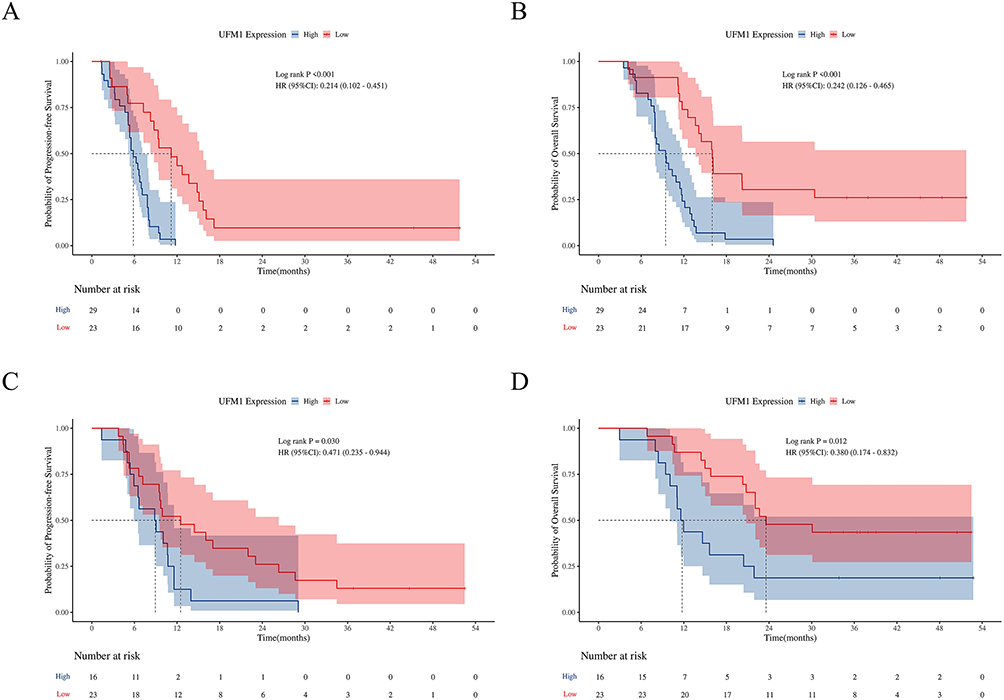 |
Figure 3 UFM1 expression is associated with survival outcomes in patients with unresectable pancreatic cancer receiving different treatment regimens. (A) Progression-free survival (PFS) and (B) overall survival (OS) in patients treated with chemotherapy alone, stratified by UFM1 expression level. (C) PFS and (D) OS in patients treated with chemoradiotherapy, stratified by UFM1 expression level. Abbreviations: UFM1, Ubiquitin-fold modifier 1; PFS, progression-free survival; OS, overall survival. |
COX Regression Analysis
A Cox regression analysis of multivariate factors demonstrated that TNM stage (HR = 0.456, 95% CI: 0.276, 0.754, P = 0.002) and UFM1 expression (HR = 0.343, 95% CI: 0.207, 0.567, P < 0.001) were independent predictors of PFS (see Table 2). Additionally, TNM stage (HR = 0.243, 95% CI: 0.127, 0.465, P < 0.001), treatment regimens (HR = 0.548, 95% CI: 0.326, 0.919, P = 0.023), and UFM1 expression (HR = 0.304, 95% CI:0.182, 0.510, P < 0.001) were also identified as independent predictors of OS. Thus, high UFM1 expression was associated with poor survival outcomes in patients with pancreatic cancer.
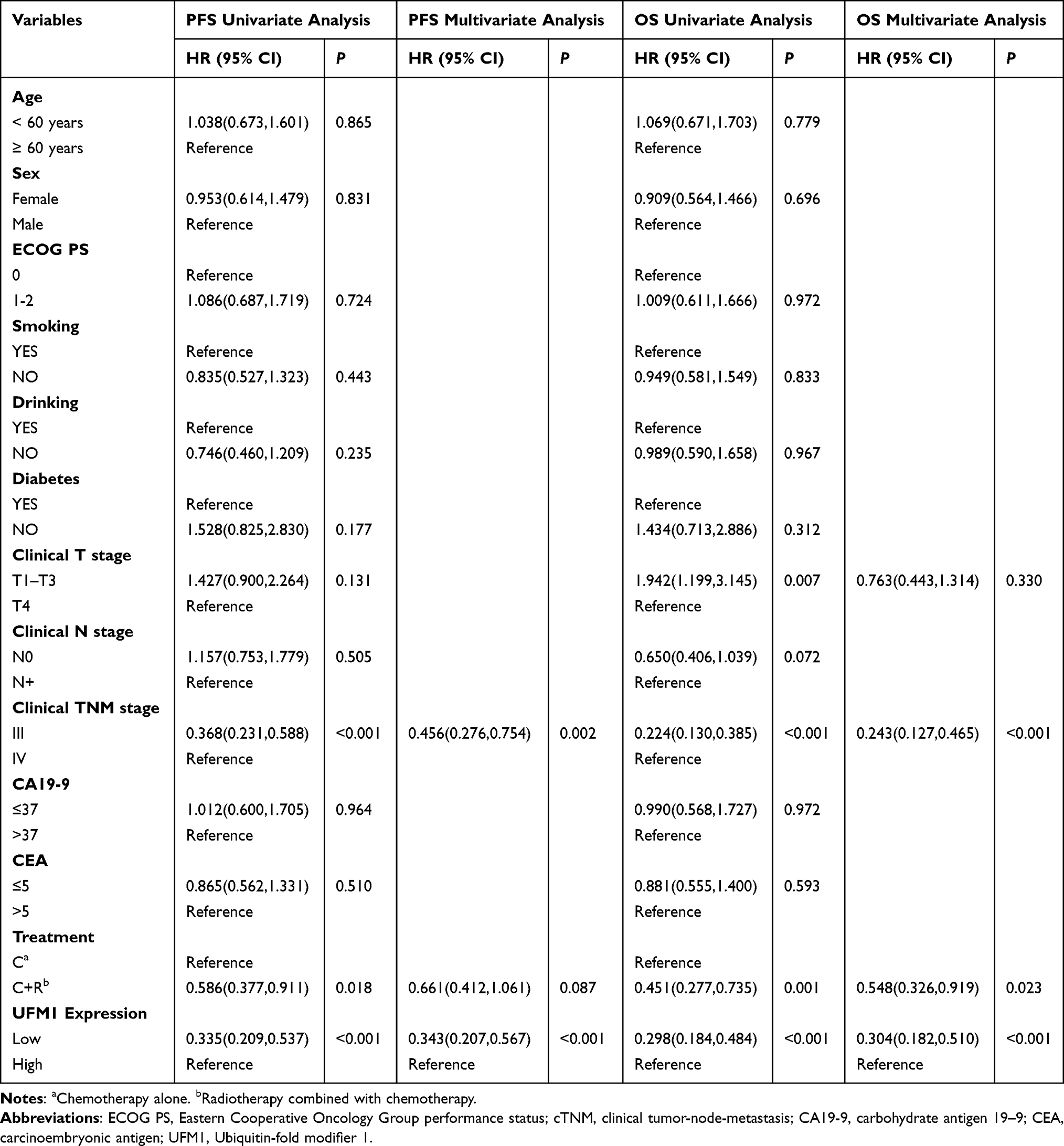 |
Table 2 Univariate and Multivariate Analysis of Clinicopathologic Characteristics for PFS and OS |
Discussion
Despite chemo and/or radiotherapy offering survival benefits, many patients with unresectable pancreatic cancer still experience rapid progression, highlighting the need for a biomarker to predict treatment efficacy and survival in these patients.6,40,41 In the present study, we identified UFM1 as a predictive biomarker for the clinical outcome of these patients. UFM1 is a ubiquitin-like protein that modifies protein substrates via the process of UFMylation.30 The ubiquitin and ubiquitin-like protein systems regulate a wide range of cellular functions, and their dysregulation is linked not only to protein synthesis and homeostasis within the endoplasmic reticulum but also to the progression of cancer.42
Tissue-based biomarkers offer insights into the tumor’s intrinsic biology and potential drug vulnerabilities. As the primary transporter of gemcitabine, hENT1 has consequently been investigated as a predictive biomarker for response to gemcitabine-based therapies.25,43 While high hENT1 expression correlates with benefit from gemcitabine, its predictive value is regimen-specific and not applicable to modern first-line regimens like FOLFIRINOX. SMAD4 is a critical tumor suppressor gene that mediates the transforming growth factor-beta signaling pathway. Inactivation of SMAD4 occurs in approximately 50–55% of PDAC cases.44 Although SMAD4 loss is a well-established marker of disease aggressiveness, correlating with a more invasive phenotype, higher metastatic rates, and poorer prognosis, its value as a predictor of specific treatment response remains unclear.45 With the advent of targeted therapies, biomarkers like mismatch repair deficiency (dMMR)/microsatellite instability-high (MSI-H) and KRAS G12C mutations have defined small but actionable subsets of patients eligible for immunotherapy or targeted agents, respectively. However, their prevalence in pancreatic cancer is low.46 In this context, UFM1 presents distinct advantages: First, it is a functional protein directly implicated in core resistance pathways like DNA damage response and immune modulation, providing a biological rationale for its association with poor outcomes. Second, it retained independent prognostic value for both PFS and OS in multivariate analysis, surpassing the prognostic power of TNM stage alone in our cohort. Third, its assessment via IHC on FFPE tissue is highly feasible and integrable into standard pathological workflows. The primary challenges for its clinical translation will be the prospective validation in larger, multi-center cohorts and the establishment of a robust, quantitative scoring system to define “high” expression. Nevertheless, its strong association with treatment resistance positions UFM1 as a promising candidate for risk stratification and a potential companion diagnostic for therapy selection.
The mechanistic link between high UFM1 expression and treatment resistance likely involves the ufmylation of specific downstream targets that promote cell survival under therapeutic stress. As a core subunit of the MRE11-RAD50-NBS1 complex, MRE11 plays a crucial role in the detection and repair of DNA double-strand breaks.47 Studies indicate that MRE11 ufmylation promotes the activation of ATM kinase, a key regulator of DDR.48 Furthermore, UFL1, the UFM1 E3 ligase, triggers replication fork degradation by MRE11 in BRCA1/2-deficient cells under replication stress.49 UFM1-mediated ufmylation regulates the stability of Programmed Death-Ligand 1 (PD-L1) by inhibiting its ubiquitin-proteasome degradation.50 PD-L1 is a critical immune checkpoint molecule expressed on tumor cells that suppresses anti-tumor immune responses by binding to PD-1 on T cells.51 This regulation plays a crucial role in tumor immune evasion. For instance, research suggests that dysregulation of ufmylation can contribute to tumor immune evasion and is considered a potential therapeutic target.50 While the specific role of the ufmylation system in tumor development and progression is still being explored, its abnormal expression and dysfunction have been observed in various cancers, including pancreatic cancer.52 Given its critical roles in multiple cellular processes, targeting the ufmylation system holds promise for enhancing the sensitivity of pancreatic cancer to chemotherapy, radiotherapy, or immunotherapy.53 Future research needs to validate this strategy through preclinical studies to identify specific ufmylation substrates and to determine the efficacy and safety of targeted interventions.
Intriguingly, analysis of public transcriptomic data (TCGA-PAAD) did not show a significant upregulation of UFM1 mRNA in pancreatic tumors compared to normal tissue. This discrepancy suggests that the elevated UFM1 protein levels we observed are likely regulated at a post-transcriptional level. Potential mechanisms include enhanced translation of UFM1 mRNA or increased stability of the UFM1 protein, both of which could lead to protein accumulation without a corresponding increase in mRNA.31 This highlights the importance of direct protein measurement in biomarker discovery and presents a compelling avenue for future research. In future studies, we will further validate the functional role of UFM1 in chemoresistance by knocking out or overexpressing UFM1 in established PDAC models (PANC-1, MIA PaCa-2) and evaluating gemcitabine sensitivity through CCK-8 and apoptosis assays.
The survival benefit of adding radiotherapy for the treatment of unresectable patients with pancreatic cancer is controversial. The Phase III randomized clinical trial LAP07 demonstrated that the addition of radiotherapy (54 Gy) to chemotherapy compared to chemotherapy alone did not significantly improve OS in patients with locally advanced pancreatic cancer (median OS: 15.2 months vs 16.5 months; HR: 1.03; 95% CI: 0.79–1.34).54 Nevertheless, the COX regression analysis of our present study indicated that combined radiotherapy is an independent protective factor affecting patient survival. Indeed, the efficacy of combined radiotherapy may be affected by the chemotherapeutic agents, radiation dose fractionation, and the side effects of combination therapy. Notably, UFM1 expression was significantly associated with TNM stage, with higher levels in stage IV patients, suggesting its role in disease progression and potential as a severity marker.
It should be noted that our study has some limitations. First, this study was retrospective in nature, which introduced the potential for selection bias and confounding variables. Despite the multifactorial regression analysis attempting to control for some of the confounding factors, there is still a possibility that unrecognized confounding variables may have affected the interpretation of the results. Second, the sample size included in this study was relatively small. Although we validated our lead candidate, UFM1, in a larger independent clinical cohort (n=91) using IHC, further prospective validation in multi-center studies with larger sample sizes is essential to confirm its robust prognostic value and establish clinically applicable cut-off values In future studies, we will increase the sample size for proteomic analyses to provide datasets with greater statistical significance. Finally, it should be noted that this study relied heavily on IHC and proteomics techniques, which are inherently subject to a certain amount of technical variability and batch effects that may have impacted the accuracy of the results. Despite the rigorous quality control measures implemented, it was not possible to completely eliminate the potential for bias due to these technical limitations.
In conclusion, this study identified UFM1 as a marker linked to the treatment efficacy of unresectable pancreatic cancer, with its expression correlating to poorer clinical outcomes and shorter survival. Our findings provide a strong rationale for its further investigation and support its potential utility in risk stratification and treatment personalization, pending validation in larger, prospective cohorts.
Abbreviations
PFS, Progression-Free Survival; OS, Overall Survival; PR, Partial Response; PD, Progressive Disease; SD, Stable Disease; UFM1, Ubiquitin-Fold Modifier 1; IHC, Immunohistochemistry; HR, Hazard Ratio; FFPE, Formalin-Fixed and Paraffin-Embedded; PCT, Pressure Cycling Technology; DIA, Data-Independent Acquisition; mIF, Multiplex Immunofluorescence; DDR, DNA Damage Response; CA19-9, Carbohydrate Antigen 19-9; PDAC, Pancreatic Ductal Adenocarcinoma; FDA, Food and Drug Administration; ctDNA, Circulating Tumor DNA; hENT1, Human Equilibrative Nucleoside Transporter 1; UBL, Ubiquitin-Like Modifier; Tris-HCl, Tris Hydrochloride; TEAB, Triethylammonium Bicarbonate; TCEP, Tris(2-carboxyethyl)phosphine; IAA, Iodoacetamide; MS, Mass Spectrometry; GSEA, Gene Set Enrichment Analysis; CK, Cytokeratin; TNM, Tumor-Node-Metastasis; ECOG, Eastern Cooperative Oncology Group; dMMR, Mismatch Repair Deficiency; MSI-H, Microsatellite Instability-High; PD-L1, Programmed Death-Ligand 1; TCGA, The Cancer Genome Atlas; PAAD, Pancreatic Adenocarcinoma.
Data Sharing Statement
The datasets used and analyzed in this study are available from the corresponding author Xiaodong Li upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Cancer Hospital Affiliated with Shandong First Medical University (No.SDTHEC202510028), which waived the need for informed consent because of the study’s retrospective nature. We declare that patients’ information will be kept confidential and that we adhere to the principles of the Declaration of Helsinki.
Acknowledgments
We thank each patient for allowing us to use their clinicopathological data in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82102845), National Natural Science Foundation of China (No. 82573451), Shandong Provincial Natural Science Foundation Joint Fund (No. ZR2025LMB023), Lanzhou City Science and Technology Development Guidance Plan (2025-5-093) and Major Project of Scientific and Technological Innovation in the Health Industry of Gansu Province (No. GSWSZD2025-10).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahib L, Wehner MR, Matrisian LM, et al. Estimated projection of US cancer incidence and death to 2040. JAMA Network Open. 2021;4(4):e214708. doi:10.1001/jamanetworkopen.2021.4708
2. Park W, Chawla A, O’Reilly EM. Pancreatic cancer: a review. JAMA. 2021;326(9):851–15. doi:10.1001/jama.2021.13027
3. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33. doi:10.3322/caac.21654
4. The Lancet Gastroenterology, H. Pancreatic cancer: a state of emergency? Lancet Gastroenterol Hepatol. 2021;6(2):81. doi:10.1016/S2468-1253(20)30397-6
5. Philip PA, Lacy J, Portales F, et al. Nab-paclitaxel plus gemcitabine in patients with locally advanced pancreatic cancer (LAPACT): a multicentre, open-label Phase 2 study. Lancet Gastroenterol Hepatol. 2020;5(3):285–294. doi:10.1016/S2468-1253(19)30327-9
6. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
7. Strickler JH, Satake H, George TJ, et al. Sotorasib in KRAS p.G12C–Mutated advanced pancreatic cancer. N Engl J Med. 2023;388(1):33–43. doi:10.1056/NEJMoa2208470
8. Chen IM, Johansen JS, Theile S, et al. Randomized Phase II study of nivolumab with or without ipilimumab combined with stereotactic body radiotherapy for refractory metastatic pancreatic cancer (CheckPAC). J Clin Oncol. 2022;40(27):3180–3189. doi:10.1200/JCO.21.02511
9. Espona-Fiedler M, Patthey C, Lindblad S, et al. Overcoming therapy resistance in pancreatic cancer: new insights and future directions. Biochem Pharmacol. 2024;229:116492. doi:10.1016/j.bcp.2024.116492
10. Ischenko I, D’Amico S, Rao M, et al. KRAS drives immune evasion in a genetic model of pancreatic cancer. Nat Commun. 2021;12(1):1482. doi:10.1038/s41467-021-21736-w
11. Barrett RL, Puré E. Cancer-associated fibroblasts and their influence on tumor immunity and immunotherapy. Elife. 2020;9:e57243.
12. Bailey P, Chang DK, Nones K, et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature. 2016;531(7592):47–52. doi:10.1038/nature16965
13. Ren J, Ren B, Liu X, et al. Crosstalk between metabolic remodeling and epigenetic reprogramming: a new perspective on pancreatic cancer. Cancer Lett. 2024;587:216649. doi:10.1016/j.canlet.2024.216649
14. Stefanoudakis D, Frountzas M, Schizas D, et al. Significance of TP53, CDKN2A, SMAD4 and KRAS in pancreatic cancer. Curr Issues Mol Biol. 2024;46(4):2827–2844. doi:10.3390/cimb46040177
15. Ying H, Kimmelman A, Lyssiotis C, et al. Oncogenic Kras maintains pancreatic tumors through regulation of anabolic glucose metabolism. Cell. 2012;149(3):656–670. doi:10.1016/j.cell.2012.01.058
16. Feig C, Gopinathan A, Neesse A, et al. The pancreas cancer microenvironment. Clin Cancer Res. 2012;18(16):4266–4276. doi:10.1158/1078-0432.CCR-11-3114
17. Clark CE, Hingorani SR, Mick R, et al. Dynamics of the immune reaction to pancreatic cancer from inception to invasion. Cancer Res. 2007;67(19):9518–9527. doi:10.1158/0008-5472.CAN-07-0175
18. Olive KP, Jacobetz MA, Davidson CJ, et al. Inhibition of Hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science. 2009;324(5933):1457–1461. doi:10.1126/science.1171362
19. Duffy MJ, Sturgeon C, Lamerz R, et al. Tumor markers in pancreatic cancer: a European group on tumor markers (EGTM) status report. Ann Oncol. 2010;21(3):441–447. doi:10.1093/annonc/mdp332
20. Xing H, Wang J, Wang Y, et al. Diagnostic value of CA 19-9 and carcinoembryonic antigen for pancreatic cancer: a meta-analysis. Gastroenterol Res Pract. 2018;2018:8704751. doi:10.1155/2018/8704751
21. Azizian A, Rühlmann F, Krause T, et al. CA19-9 for detecting recurrence of pancreatic cancer. Sci Rep. 2020;10(1):1332. doi:10.1038/s41598-020-57930-x
22. Alqahtani A, Alloghbi A, Coffin P, et al. Prognostic utility of preoperative and postoperative KRAS-mutated circulating tumor DNA (ctDNA) in resected pancreatic ductal adenocarcinoma: a systematic review and meta-analysis. Surg Oncol. 2023;51:102007. doi:10.1016/j.suronc.2023.102007
23. Leiting JL, Alva-Ruiz R, Yonkus JA, et al. Molecular KRAS ctDNA predicts metastases and survival in pancreatic cancer: a prospective cohort study. Ann Surg Oncol. 2025;32(6):4453–4463. doi:10.1245/s10434-025-17036-y
24. Huerta M, Martín-Arana J, Gimeno-Valiente F, et al. ctDNA whole exome sequencing in pancreatic ductal adenocarcinoma unveils organ-dependent metastatic mechanisms and identifies actionable alterations in fast progressing patients. Transl Res. 2024;271:105–115. doi:10.1016/j.trsl.2024.05.003
25. Perera S, Jang GH, Wang Y, et al. hENT1 expression predicts response to gemcitabine and nab-paclitaxel in advanced pancreatic ductal adenocarcinoma. Clin Cancer Res. 2022;28(23):5115–5120. doi:10.1158/1078-0432.CCR-22-2576
26. Murimwa GZ, Williams NE, Alzhanova D, et al. SMAD4 deficiency promotes pancreatic cancer progression and confers susceptibility to TGFβ inhibition. Cancer Res. 2025;85(16):2987–2996. doi:10.1158/0008-5472.CAN-24-1970
27. Lloyd EG, Jihad M, Manansala JS, et al. SMAD4 and KRAS status shapes cancer cell-stromal cross-talk and therapeutic response in pancreatic cancer. Cancer Res. 2025;85(8):1368–1389. doi:10.1158/0008-5472.CAN-24-2330
28. Zhou X, Mahdizadeh SJ, Le Gallo M, et al. UFMylation: a ubiquitin-like modification. Trends Biochem Sci. 2024;49(1):52–67. doi:10.1016/j.tibs.2023.10.004
29. Jing Y, Mao Z, Chen F. UFMylation system: an emerging player in tumorigenesis. Cancers. 2022;14(14):3501. doi:10.3390/cancers14143501
30. Wang X, Lv X, Ma J, et al. UFMylation: an integral post-translational modification for the regulation of proteostasis and cellular functions. Pharmacol Ther. 2024;260:108680. doi:10.1016/j.pharmthera.2024.108680
31. Chung CH, Yoo HM. Emerging role of protein modification by UFM1 in cancer. Biochem Biophys Res Commun. 2022;633:61–63. doi:10.1016/j.bbrc.2022.08.093
32. Li G, Huang Y, Han W, et al. Eg5 UFMylation promotes spindle organization during mitosis. Cell Death Dis. 2024;15(7):544. doi:10.1038/s41419-024-06934-w
33. Ke D, Guo -H-H, Jiang N, et al. Inhibition of UFM1 expression suppresses cancer progression and is linked to the dismal prognosis and immune infiltration in oral squamous cell carcinoma. Aging. 2023;15(22):13059–13076. doi:10.18632/aging.205219
34. Fang Y, Wu A, Cong Y-S, et al. The role of UFMylation in the development and progression of gastric cancer. Oncol Res. 2025;33(11):3231–3245. doi:10.32604/or.2025.066402
35. Arai H, Yang Y, Baca Y, et al. Predictive value of CDC37 gene expression for targeted therapy in metastatic colorectal cancer. Eur J Cancer. 2024;201:113914. doi:10.1016/j.ejca.2024.113914
36. Yang G, Cai S, Hu M, et al. Spatial features of specific CD103(+)CD8(+) tissue-resident memory T cell subsets define the prognosis in patients with non-small cell lung cancer. J Transl Med. 2024;22(1):27. doi:10.1186/s12967-023-04839-4
37. Mao M, Chen Y, Yang J, et al. Modification of PLAC8 by UFM1 affects tumorous proliferation and immune response by impacting PD-L1 levels in triple-negative breast cancer. J Immunother Cancer. 2022;10(12):e005668. doi:10.1136/jitc-2022-005668
38. Lin M, Lian N-Z, Cao -L-L, et al. Down-regulated expression of CDK5RAP3 and UFM1 suggests a poor prognosis in gastric cancer patients. Front Oncol. 2022;12:927751. doi:10.3389/fonc.2022.927751
39. Lin JX, Xie X-S, Weng X-F, et al. UFM1 suppresses invasive activities of gastric cancer cells by attenuating the expres7sion of PDK1 through PI3K/AKT signaling. J Exp Clin Cancer Res. 2019;38(1):410. doi:10.1186/s13046-019-1416-4
40. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. doi:10.1056/NEJMoa1011923
41. Wainberg ZA, Melisi D, Macarulla T, et al. NALIRIFOX versus nab-paclitaxel and gemcitabine in treatment-naive patients with metastatic pancreatic ductal adenocarcinoma (NAPOLI 3): a randomised, open-label, Phase 3 trial. Lancet. 2023;402(10409):1272–1281. doi:10.1016/S0140-6736(23)01366-1
42. Hoeller D, Hecker CM, Dikic I. Ubiquitin and ubiquitin-like proteins in cancer pathogenesis. Nat Rev Cancer. 2006;6(10):776–788. doi:10.1038/nrc1994
43. Bird NT, Elmasry M, Jones R, et al. Immunohistochemical hENT1 expression as a prognostic biomarker in patients with resected pancreatic ductal adenocarcinoma undergoing adjuvant gemcitabine-based chemotherapy. Br J Surg. 2017;104(4):328–336. doi:10.1002/bjs.10482
44. Principe DR, Underwood PW, Kumar S, et al. Loss of SMAD4 is associated with poor tumor immunogenicity and reduced PD-L1 expression in pancreatic cancer. Front Oncol. 2022;12:806963. doi:10.3389/fonc.2022.806963
45. Racu ML, Lebrun L, Schiavo AA, et al. The role of SMAD4 inactivation in epithelial-mesenchymal plasticity of pancreatic ductal adenocarcinoma: the missing link? Cancers. 2022;14(4):973. doi:10.3390/cancers14040973
46. Giannis D, Moris D, Barbas AS. Diagnostic, predictive and prognostic molecular biomarkers in pancreatic cancer: an overview for clinicians. Cancers. 2021;13(5):1071. doi:10.3390/cancers13051071
47. Lu R, Zhang H, Jiang Y-N, et al. Post-translational modification of MRE11: its implication in DDR and diseases. Genes. 2021;12(8):1158. doi:10.3390/genes12081158
48. Wang Z, Gong Y, Peng B, et al. Correction to ‘MRE11 UFMylation promotes ATM activation’. Nucleic Acids Res. 2024;52(18):11412. doi:10.1093/nar/gkae802
49. Tian T, Chen J, Zhao H, et al. UFL1 triggers replication fork degradation by MRE11 in BRCA1/2-deficient cells. Nat Chem Biol. 2024;20(12):1650–1661. doi:10.1038/s41589-024-01611-7
50. Zhou J, Ma X, He X, et al. Dysregulation of PD-L1 by UFMylation imparts tumor immune evasion and identified as a potential therapeutic target. Proc Natl Acad Sci U S A. 2023;120(11):e2215732120. doi:10.1073/pnas.2215732120
51. Wang R, He S, Long J, et al. Emerging therapeutic frontiers in cancer: insights into posttranslational modifications of PD-1/PD-L1 and regulatory pathways. Exp Hematol Oncol. 2024;13(1):46. doi:10.1186/s40164-024-00515-5
52. Wang K, Chen S, Wu Y, et al. The ufmylation modification of ribosomal protein L10 in the development of pancreatic adenocarcinoma. Cell Death Dis. 2023;14(6):350. doi:10.1038/s41419-023-05877-y
53. Li H, Meng F, Liang J, et al. UFMylation system: biological functions, molecular mechanisms, diseases, and drug discovery. MedComm. 2025;6(10):e70424. doi:10.1002/mco2.70424
54. Hammel P, Huguet F, van Laethem J-L, et al. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: the LAP07 randomized clinical trial. JAMA. 2016;315(17):1844–1853. doi:10.1001/jama.2016.4324
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Risk Score (P-score) Based on a Three-Gene Signature, for Estimating the Risk of Prostate Cancer-Specific Mortality
Söderdahl F, Xu LD, Bring J, Häggman M
Research and Reports in Urology 2022, 14:203-217
Published Date: 11 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Construction of a Pyroptosis-Related Genes Signature to Improve the Prognostic Prediction and Therapeutic Drugs Selection in Patients with Pancreatic Cancer
Li C, Wang M, Wei J, Zhang W, Liu H, Zhao D
International Journal of General Medicine 2022, 15:6387-6403
Published Date: 2 August 2022
NUP62CL as an Immunological and Prognostic Biomarker of Oral Squamous Cell Carcinoma
Yu X, Xu L, Zhou Y, Zhou X, Yang L, Zhou Y
Journal of Inflammation Research 2023, 16:3799-3809
Published Date: 29 August 2023
Comprehensive Bioinformatics Analyses and Experimental Validation of the Cell Cycle Related Protein SAPCD2 as a New Biomarker and Potential Therapeutic Target in Pancreatic Cancer
Liu Y, Li B, Ke L, Luo T, Wu H, Lin J, Deng Y, Huang X, Xu L, Liu Y, Qi J
Journal of Inflammation Research 2025, 18:2855-2877
Published Date: 26 February 2025