Back to Journals » Journal of Inflammation Research » Volume 18
Identifying Chemokine System-Related Phenotype to Predict Immune Feature in Pan-Cancer and Prognostic Signature for Lung Adenocarcinoma
Authors Zhao T, Wu X, Guo S, Nie J, Fang S, Wang L, Li X, Nie T, Yao K ![]() , Du X, Wang Y, Yuan Y, Ni J
, Du X, Wang Y, Yuan Y, Ni J ![]()
Received 18 May 2025
Accepted for publication 4 September 2025
Published 22 September 2025 Volume 2025:18 Pages 13213—13234
DOI https://doi.org/10.2147/JIR.S537256
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Junhao Wang
Tianming Zhao,1– 4,* Xu Wu,1,2,* Shiqi Guo,5,* Jun Nie,5 Shitao Fang,5 Liangchao Wang,6 Xiaojuan Li,1,2 Tingting Nie,1,2 Kecheng Yao,7 Xinge Du,1,2 Yingnan Wang,1,2 Yurong Yuan,8 Jixiang Ni6
1Department of Respiratory and Critical Care Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Yichang Central People’s Hospital, Yichang, Hubei, People’s Republic of China; 3Third-Grade Pharmacological Laboratory on Traditional Chinese Medicine, State Administration of Traditional Chinese Medicine, China Three Gorges University, Yichang, People’s Republic of China; 4Clinical Medical Research Center for Precision Diagnosis and Treatment of Lung Cancer and Management of Advanced Cancer Pain of Hubei Province, Yichang, Hubei, People’s Republic of China; 5Department of Cardiothoracic Surgery, The First College of Clinical Medical of Science, Yichang Central People’s Hospital, China Three Gorges University, Yichang, People’s Republic of China; 6Department of Pulmonary and Critical Care Medicine, The Central Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 7Department of Geriatrics, The First College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei, People’s Republic of China; 8Yichang Emergency Medical Center, Yichang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yurong Yuan, Email [email protected] Jixiang Ni, Email [email protected]
Background: The chemokine system modulates tumor cell characteristics and influences immune cell function. This research investigates the roles of chemokines and their receptors (CaCRs) across multiple cancers and establishes a reliable CaCRs-based prognostic model for lung adenocarcinoma (LUAD).
Methods: Gene expression data were sourced from the UCSC-Xena platform and the GEO database. The chemokine score was calculated using the ssGSEA algorithm. A CaCRs-based prognostic signature was constructed and validated for LUAD. Expression levels of signature genes in lung cancer tissues were verified.
Results: Dysregulation of CaCRs expression was observed in multiple cancers. The chemokine score has shown prognostic features in various tumors. In the LUAD cohort, a seven-gene signature of CaCRs (CCR2, CCR4, CCR6, XCR1, CCL20, CXCL17, and XCL2) was constructed as a prognostic model, identifying a poorer prognosis for high-risk groups. mRNA levels of CCR2, CCR4, CCR6, and XCR1 were significantly reduced in lung cancer tissues compared to adjacent normal tissues, while CCL20 was markedly overexpressed in tumor tissues. Furthermore, CCL20 promoted A549 cell proliferation via the MAPK pathway, with JNK inhibitors effectively blocking CCL20-induced proliferation.
Conclusion: This study highlights the substantial role of CaCRs in immunity and prognosis. The identified seven-gene signature of CaCRs provides a new prognostic tool for LUAD.
Keywords: chemokine, chemokine receptor, prognosis, pan-cancer, LUAD
Introduction
Cancer poses an increasing threat to public health. Although tremendous developments have been made in cancer treatment, the long-term survival of patients remains dismal.1 Recent breakthroughs, particularly in molecular-targeted therapies and immunotherapies like chimeric antigen receptor T-cell (CAR-T) therapy, have transformed treatment approaches, especially for hematologic cancers.2 Immune checkpoint inhibitors have also achieved notable clinical success, and certain small molecules with anti-tumor properties have shown immunostimulatory effects that enhance the efficacy of checkpoint inhibitors.3 Chemokines play a crucial role in orchestrating the immune microenvironment and modulating responses to immunotherapy. Elevated CCL3 in myeloid cells recruits CCR1+ monocytes to metastases, promoting the accumulation of myeloid cells and an immunosuppressive tumor microenvironment.4 Thus, dysregulation within chemokine systems can influence tumor progression through direct or indirect mechanisms, impacting both pro- and anti-tumorigenic activities.5
Chemokines are small (8–12 kDa) chemoattractant proteins that play essential roles in regulating cell migration, adhesion, positioning, and interaction through specific receptor binding.6 The chemokine system comprises approximately 50 chemokine ligands, 20 canonical chemokine receptors (which are transmembrane G protein-coupled receptors, GPCRs), and 4 atypical chemokine receptors (ACKRs).7 Chemokines and their receptors (CaCRs) are expressed by both tumor and non-tumor cells, including immune and stromal cells. Chemokines influence tumor cell behaviors such as proliferation, invasion, and stemness, as well as stromal cell activities including fibrosis, angiogenesis, and neurogenesis.8 For example, melanoma cells express chemokines like CCL2, CCL5, CXCL1, CXCL2, CXCL3, and CXCL8, which drive tumor growth and progression.9 Tumor-derived CCL5 facilitates the recruitment of fibroblasts, promoting angiogenesis and collagen synthesis via the CCR5-SLC25A24 pathway.9 Additionally, chemokines coordinate the chemotaxis of immune cells within the tumor microenvironment (TME), thereby affecting the tumor immune response. CXCL14 enhances the recruitment of CD8+ T cells and improves survival outcomes in patients with glioma.10 Combining pemetrexed and cisplatin (PEM/CDDP) with MEK inhibitors stimulates the secretion of CXCL10, which attracts CD8+ T cells and sensitizes lung cancer to immune checkpoint blockade.11 Conversely, tumor-associated macrophage (TAM)-derived CCL5 contributes to an immunosuppressive environment, promoting the progression of clear cell renal cell carcinoma.12 Modulating the chemokine network has shown promise in enhancing CAR-T cell targeting of tumors, addressing a major hurdle in the development of CAR-T therapies for solid tumors.13
Thus, the chemokine network within the TME represents a complex system involving diverse cell types and signaling pathways that regulate tumor growth, invasion, metastasis, and immune responses. Given the importance of CaCRs in cancer progression and immune response, we conducted a comprehensive analysis to investigate their prognostic value across multiple cancers. We also developed a chemokine score to assess its relationship with prognosis and immune cell infiltration patterns in specific tumors. Notably, in lung adenocarcinoma (LUAD), the chemokine score demonstrated strong prognostic relevance. Building on this, we identified a CaCRs-based signature to predict overall survival and immune characteristics in the LUAD cohort.
Materials and Methods
Data Source
Gene expression data for The Cancer Genome Atlas (TCGA) Pan-Cancer cohort were retrieved from the UCSC Xena platform (https://toil.xenahubs.net). Information on prognostic survival was also obtained. Immune cell infiltration estimates for TCGA pan-cancer samples were downloaded from the Timer 2.0 database using the CIBERSORT algorithm. Additionally, the LUAD cohort (GSE72094) was retrieved from the Gene Expression Omnibus (GEO) database (https://www.ncbi.nlm.nih.gov/geo/).
CaCRs Expression and Survival Analysis
CaCRs gene expression across various cancers were analyzed using the limma package in R. Differentially expressed genes (DEGs) between tumor and normal tissues were identified using linear models and empirical Bayes methods. Log2 fold change (FC) values were visualized via heat maps, while box plots illustrated gene expression differences. Only cancer types with a minimum of five para-cancerous samples were included to ensure statistical reliability. To assess the prognostic significance of CaCRs expression, samples were categorized into high- and low-expression groups. Kaplan-Meier survival analysis and Log rank tests, implemented through the survival package in R, were used to compare survival outcomes between these groups.
Identification of the Relationship of CaCRs
Chemokine receptors interact with ligands to mediate various biological processes. Correlation coefficients between ligand-receptor and corresponding significance were calculated for global pan-cancer samples. Protein-protein interactions (PPIs) were predicted via the STRING database, and Cytoscape software (v3.4.0) was used to construct interaction networks. Network connectivity was analyzed using the CytoNCA plug-in.
Survey of Drug Sensitivity
Regression models were developed to predict IC50 values of chemotherapeutic drugs based on gene expression profiles from GDSC and TCGA. Significant associations between CaCRs expression and drug IC50 values were identified using Pearson correlation coefficients (|r| > 0.3, p < 0.05).
Pathways Involved in CaCRs
Using 51 HALLMARK gene sets from the MSigDB database, pathway enrichment scores were calculated via GSVA. Spearman correlation coefficients and corresponding p-values were computed to link CaCRs expression levels with specific pathways.
Analysis of Immune-Related Functions, Immune Infiltration, and Immune Checkpoints
The ESTIMATE algorithm was employed to calculate stromal, immune, and ESTIMATE scores based on CaCRs expression. Heat maps showed Spearman correlations between CaCRs and these scores. Immune cell infiltration levels and immune checkpoint expression were also analyzed in relation to CaCRs across TCGA pan-cancer samples.
Construction of Chemokine Score
The ssGSEA algorithm was used to calculate chemokine scores for each sample. Associations between chemokine scores and prognosis were examined using univariate Cox regression and Kaplan-Meier survival analysis. Score distributions were compared between cancerous and normal tissues.
Construction and Validation of the Prognostic Gene Signature of CaCRs in LUAD
Prognosis-related CaCRs genes were identified using univariate Cox regression in the TCGA-LUAD cohort. We then applied the LASSO Cox regression model with 20-fold cross-validation to further refine the selection of prognostically relevant genes. The final prognostic model was established using the selected genes and their corresponding regression coefficients. This multi-step approach, incorporating stringent cross-validation, was designed to minimize overfitting and enhance the robustness of the model. Risk scores were calculated for each patient, and their association with survival outcomes was validated in external cohorts (GSE72094). Nomograms were developed to integrate clinicopathological factors with risk scores.
Quantitative Reverse Transcription PCR (qRT-PCR)
The present study was conducted in full compliance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval was granted by the Ethics Committee of Yichang Central People’s Hospital (Protocol No. 2023–245-01). Informed consent was obtained from all participants. Thirty-one non-small cell lung cancer (NSCLC) specimens and adjacent normal tissues were collected. RNA extraction, cDNA synthesis, and gene expression quantification were performed using standardized protocols, with expression levels calculated via the 2−ΔΔCt method. Primer sequences are listed in Supplementary Table 1.
Immunohistochemistry (IHC)
CCL20 expression in LUAD and adjacent tissues was assessed through IHC. After antigen retrieval and blocking, sections were incubated with an anti-hCCL20 antibody (dilution 1:200, Proteintech, 26527-1-AP), visualized using DAB, and counterstained with hematoxylin.
Cell Culture and Cell Viability Assays
A549 cells were cultured under standard conditions and treated with CCL20, either alone or in combination with inhibitors (SP600125, PD98095). Cell viability was assessed using the CCK-8 reagent.
Western Blot
Protein expression was analyzed using SDS-PAGE and PVDF membrane transfer. Specific antibodies targeting GAPDH (dilution 1:5000, Proteintech, 10494-1-AP), phosphorylated and total JNK (dilution 1:1000, Cell Signaling Technology, 4668, 9252), ERK (dilution 1:1000, Cell Signaling Technology, 4370, 4695), and p38 (dilution 1:1000, Cell Signaling Technology, 4511, 8690) were used. Chemiluminescence and ImageJ software were employed for visualization and densitometry.
5-Ethynyl-2’deoxyuridine (EdU) Proliferation Assay
Cell proliferation was evaluated using an EdU incorporation assay. Cells were fixed, permeabilized, and treated with a click reaction solution, followed by nuclear staining with Hoechst 33342. EdU-positive cells were subsequently visualized and recorded using a fluorescence microscope.
Statistical Analysis
Bioinformatics analyses were conducted using R software (R3.6.1). Experimental data are presented as the mean ± standard deviation (SD) or mean ± standard error of the mean (SEM). One-way ANOVA or t-tests were used for comparisons, with p < 0.05 considered statistically significant.
Results
CaCRs Level in Different Cancers
First, 45 chemokine genes and 24 chemokine receptor genes (Supplementary Table 2) were retrieved from the literature. We investigated the differential expression of CaCRs genes between tumor and normal tissue samples across 18 types of cancers in the TCGA database. Results showed a more pronounced difference in chemokine ligand expression compared to receptors (Figure 1). CaCRs were more frequently downregulated in cancers such as LUAD, lung squamous cell carcinoma (LUSC), kidney chromophobe (KICH), and breast invasive carcinoma (BRCA). Conversely, CaCRs were more often upregulated in glioblastoma multiforme (GBM), kidney renal clear cell carcinoma (KIRC), cholangiocarcinoma (CHOL), head and neck squamous cell carcinoma (HNSC), esophageal carcinoma (ESCA), and stomach adenocarcinoma (STAD). Specifically, CCL14 and CCL23 were downregulated in most cancers, except for GBM, while CXCL9, CXCL10, CXCL11, CCL25, and CCR8 were upregulated in the majority of cancer tissues compared to normal samples. This differential expression pattern highlights the potential roles of these chemokines and receptors in cancer-specific alterations of the immune microenvironment.
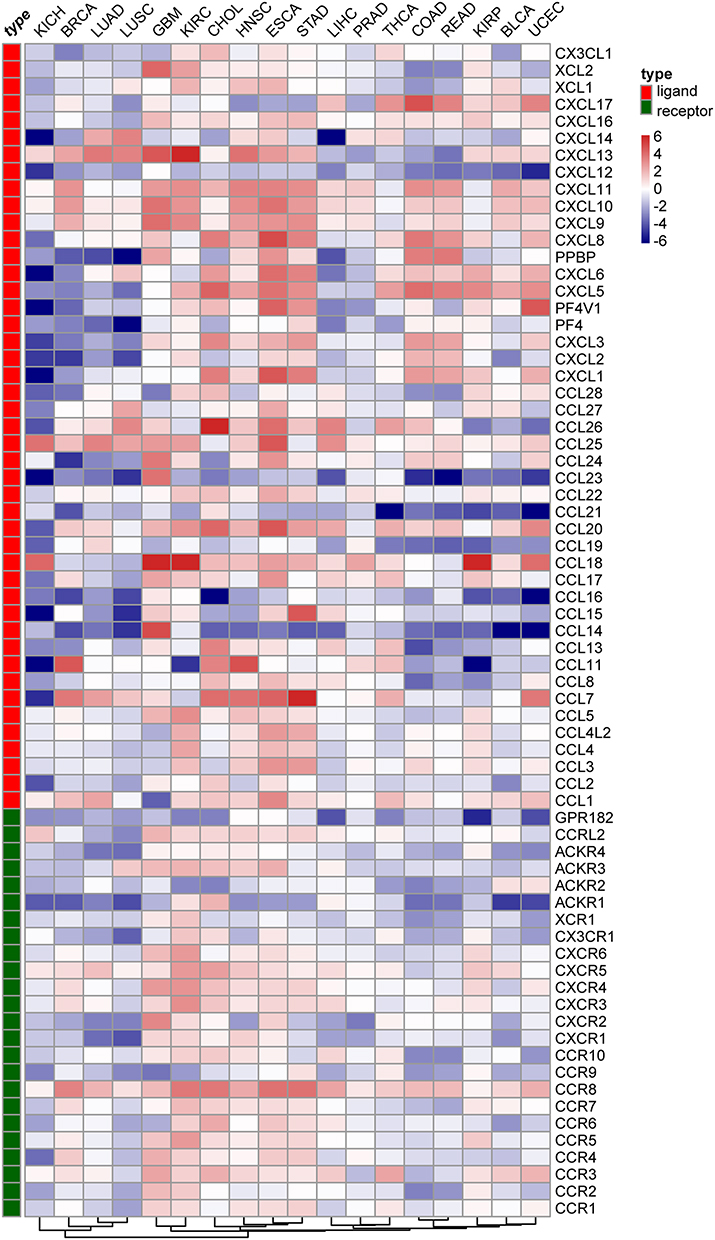 |
Figure 1 Expression features of CaCRs in multiple cancers. |
The Relationship Between CaCRs Expression and CaCRs-Related Pathways
We explored the regulation of CaCRs gene expression by transcription factors (TFs). Notably, RELA, NFKB1, SP1, STAT6, and STAT1 emerged as key regulators, each predicted to influence three or more CaCRs genes (Supplementary Figure 1). Chemokine receptors are crucial for binding specific chemokines, highlighting the correlation between CaCRs and chemokines at the tissue level of expression. To explore this relationship, we conducted a correlation analysis between chemokines and their corresponding receptor genes across pan-cancer datasets (Figure 2A). CCR5 showed significant correlations with several ligands, including CCL3, CCL4, CCL5, CCL7, CCL8, and CXCL11, with CCR5 and CCL5 exhibiting the strongest correlation (Figure 2A and B). We also constructed a protein-protein interaction (PPI) network for CaCRs using the STRING database. The analysis identified CXCL10, CCL2, CCL5, CCR3, CCR5, and CXCR4 as hub genes with the highest connectivity, indicating their central involvement in CaCRs-mediated processes (Figure 2C).
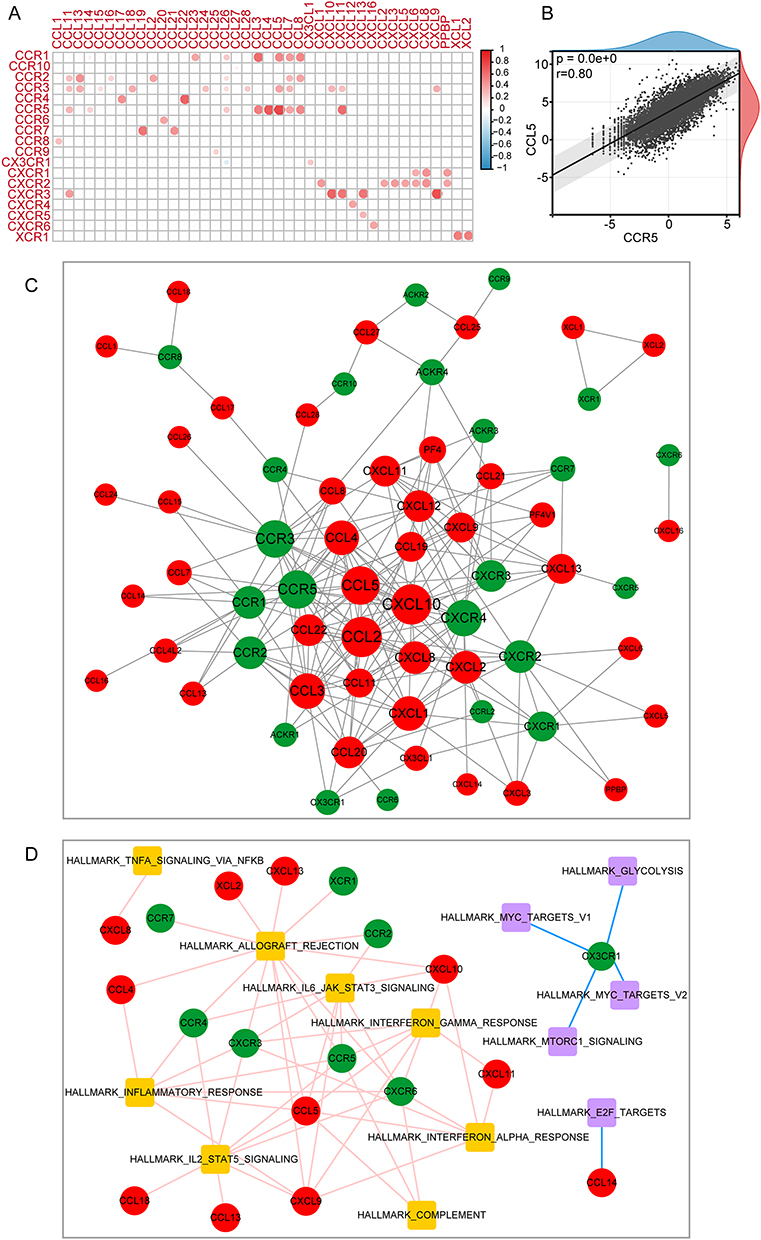 |
Figure 2 Correlation of CaCRs transcription levels and involved functional pathways. (A) Heat map of correlation between CaCRs. (B) Correlation scatter plots of CCL5 and CCR5 in pan-cancer. (C) Interaction networks between CaCRs. (D) Correlation networks between CaCRs and the HALLMARK gene sets. |
Next, we calculated the enrichment pathway scores for the HALLMARK gene sets in each sample and analyzed their correlation with the expression levels of CaCRs. Enrichment pathways positively associated with most chemokines included TNFA-signaling, allograft-rejection, IL-6-JAK-STAT3-signaling, interferon γ-response, interferon-α-response complement, IL2-STAT5-signaling, and inflammatory response, whereas MYC-targets, glycolysis, mTORC1 signaling, and E2F-targets were negatively correlated (Figure 2D). These pathway associations highlight how CaCRs may integrate inflammatory and immune responses, modulating cancer progression.
Prognostic Potential of CaCRs in Cancers
The prognostic value of most CaCRs in human cancers remains unknown. Therefore, we analyzed the prognosis of each CaCR gene in each cancer. Most CaCRs have prognostic value in SKCM (Figure 3A). In CHOL and diffuse large B-cell lymphoma (DLBCL), only CXCL17 showed prognostic significance (Figure 3A). CaCRs have different prognostic values for different tumors. For instance, CXCL9 acted as a protective factor in SKCM, ovarian cancer (OV), and BRCA, while serving as a significant risk factor in uveal melanoma (UVM), lower-grade glioma (LGG), and pancreatic adenocarcinoma (PAAD) (Figure 3B). These findings underscore the varied prognostic roles of CaCR genes across different cancers, indicating that individual CaCRs may operate uniquely within specific tumor microenvironments.
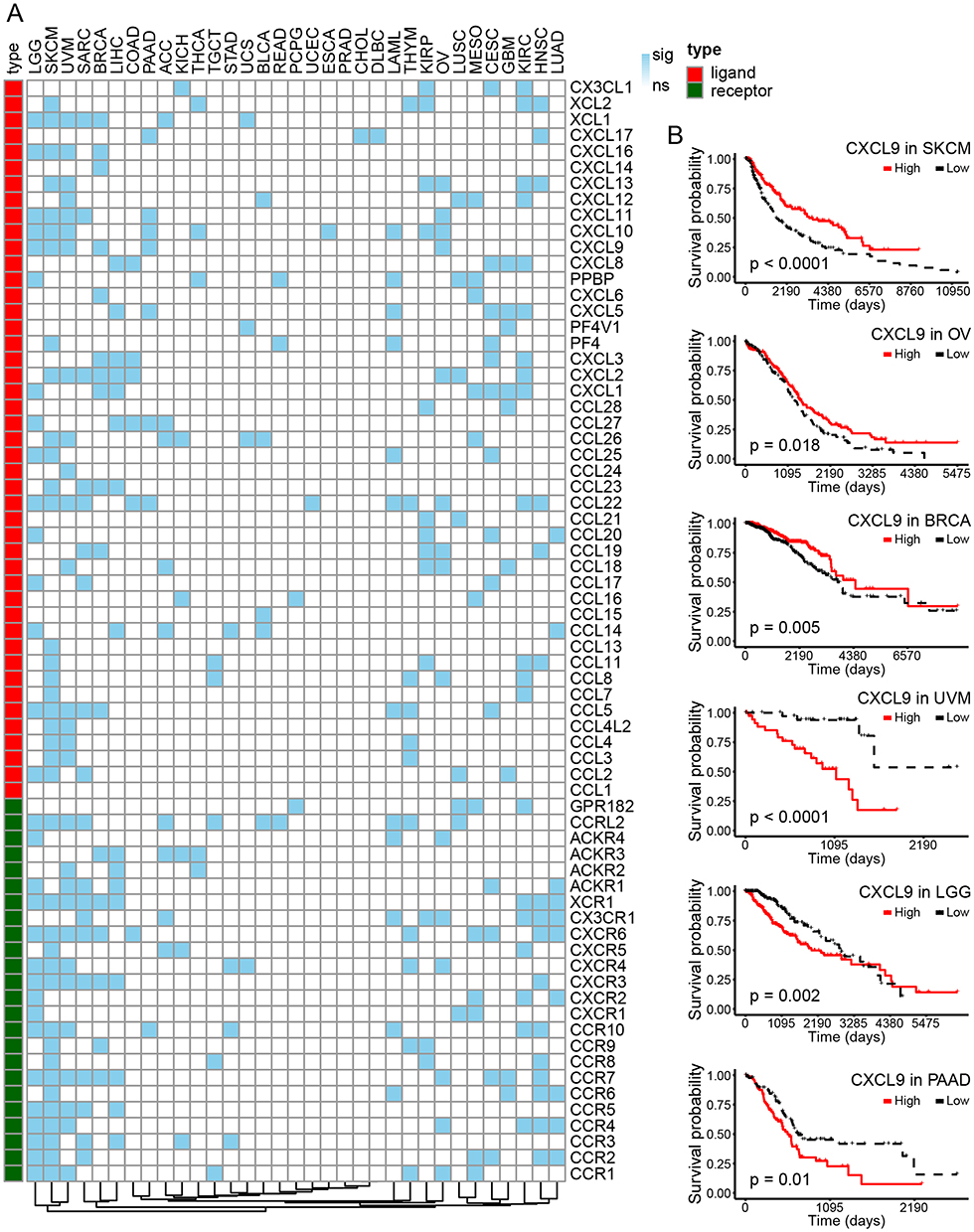 |
Figure 3 Prognostic roles of CaCRs. (A) Distribution of prognostic significance of CaCRs in individual cancers. (B) Kaplan-Meier curves of CXCL9 expression in the six tumors most significantly associated with the disease. |
CaCRs and Immune Features
Recent studies have shown that TME-associated alterations can serve as predictors of clinical outcomes. We calculated the stromal score, immune score, and ESTIMATE score across various cancer types to investigate the association between CaCRs expression and these scores. Most CaCRs exhibit positive correlations with stromal score (Supplementary Figure 2), immune score (Supplementary Figure 3), and ESTIMATE score (Supplementary Figure 4). Notably, we determined that many CaCRs showed strong positive correlations with M1 macrophages and CD8+ T cells, particularly the ligands CXCL9, CXCL10, and CXCL11 (Figure 4). Conversely, activated mast cells and monocytes were negatively correlated with several CaCRs (Figure 4). Correlations with immune checkpoint genes (Supplementary Figure 5) showed that most CaCRs, including several receptors and ligands, positively associated with checkpoints. These findings suggest that CaCRs play a pivotal role in shaping the TME by fostering immune cell infiltration and strengthening interactions with immune checkpoints.
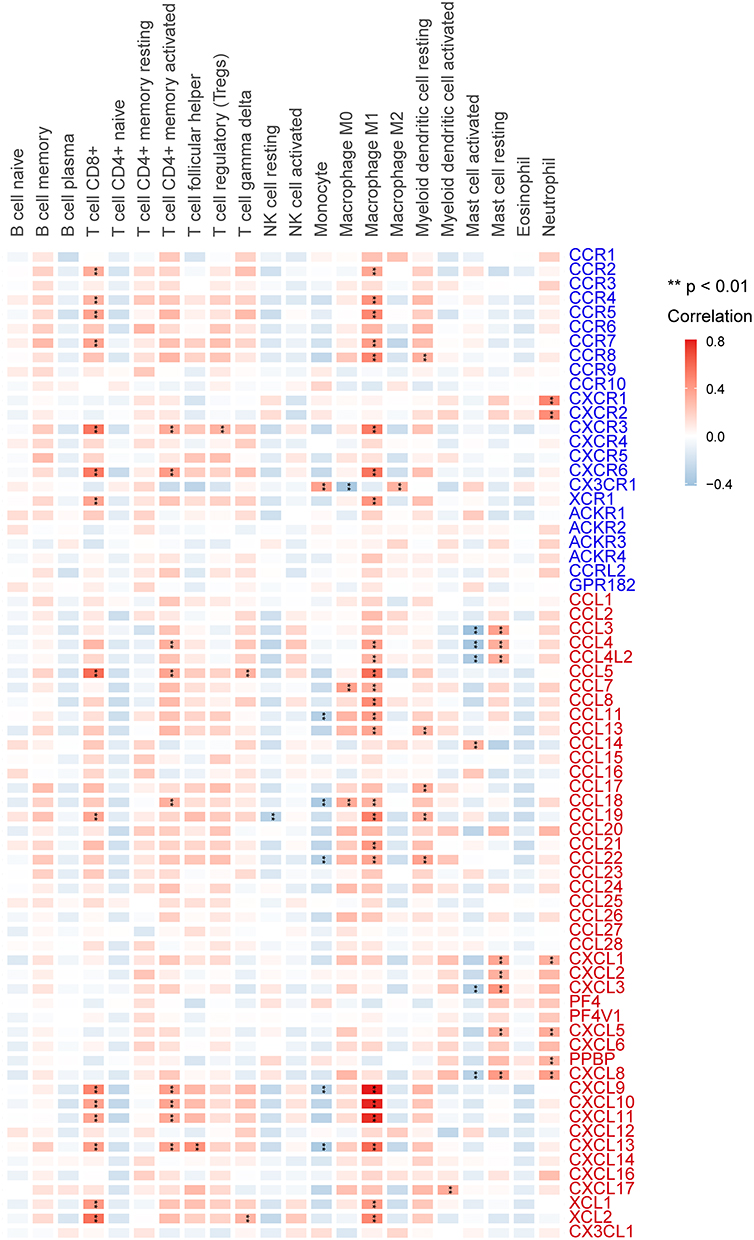 |
Figure 4 The relationship between CaCRs and the levels of infiltration of 22 immune-related cells. **p < 0.01. |
Drug Sensitivity Associated with CaCRs
The correlation between CaCRs mRNA levels and drug sensitivity was analyzed (Figure 5). Specifically, pyrimethamine, rapamycin, roscovitine, and sunitinib exhibited a negative correlation with most CaCRs, suggesting that higher CaCRs levels could be a biomarker for increased sensitivity to certain drugs, as evidenced by lower IC50 values. Conversely, elesclomol, nutlin-3a, imatinib, and axitinib displayed positive IC50 correlations, indicating that lower CaCRs levels may enhance the effectiveness of these treatments. Several CaCRs, including CCR1, CCR2, CCR3, CXCR3, CXCR6, XCR1, CCL5, CCL17, CXCL12, CXCL13, XCL1, and XCL2, demonstrated a particularly strong negative correlation with the IC50 of anticancer drugs, underscoring the potential role of these genes in modulating drug sensitivity.
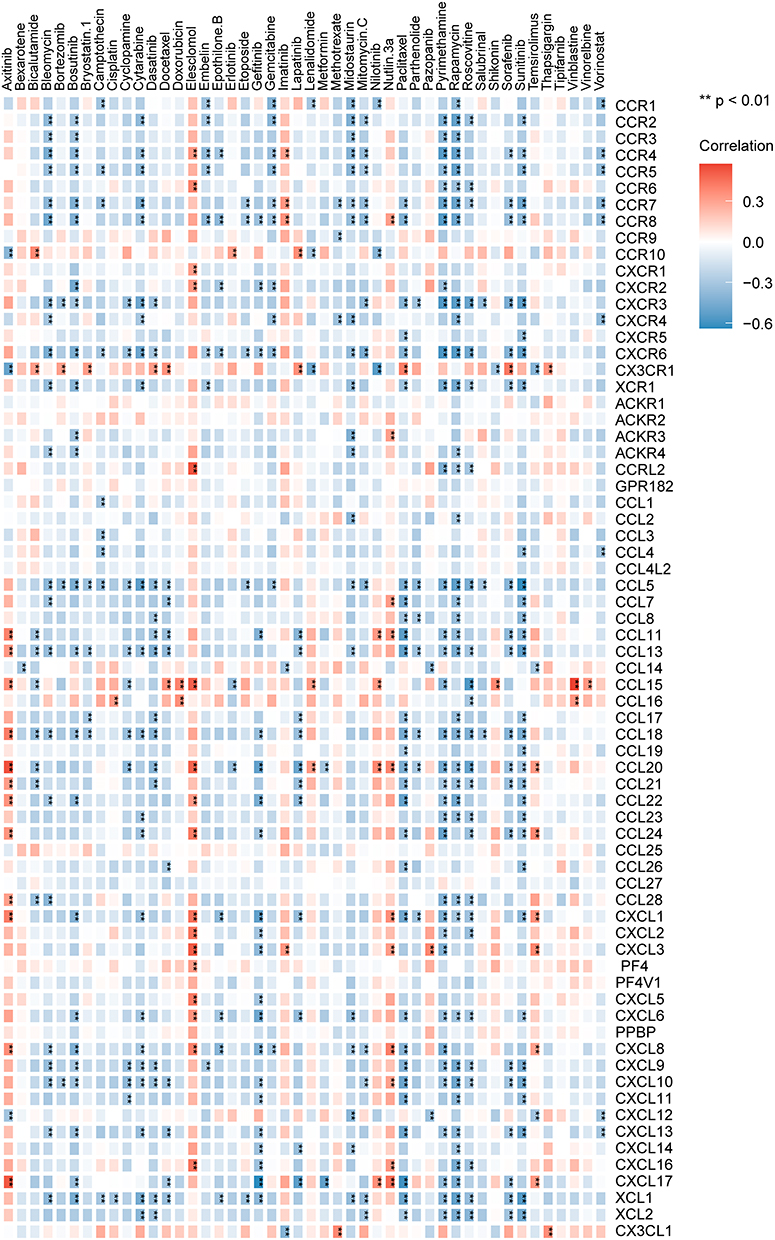 |
Figure 5 Correlations between drug IC50 values and CaCRs. **p < 0.01. |
Diagnostic and Prognostic Significance of Chemokine Score
Here, gene set variation analysis (GSVA) was conducted in the R programming environment to calculate a chemokine score for each sample. Tumor tissues generally exhibited lower chemokine scores compared to normal tissues in a pan-cancer context (Figure 6A). Interestingly, specific cancers, such as ESCA, GBM, KIRC, and kidney renal papillary cell carcinoma (KIRP), displayed higher chemokine scores in tumor tissues compared to their normal counterparts. Conversely, bladder urothelial carcinoma (BLCA), BRCA, colon adenocarcinoma (COAD), KICH, liver hepatocellular carcinoma (LIHC), LUAD, and LUSC were characterized by reduced chemokine scores in tumor samples (Figure 6B). Next, we divided the patients into two groups according to the median chemokine score to analyze the prognostic significance of the chemokine score. Univariate Cox regression analysis was performed for each cancer type. (Figure 6C). This analysis revealed that elevated chemokine scores were correlated with improved survival in cancers such as adrenocortical carcinoma (ACC), SKCM, sarcoma (SARC), and LUAD (Figure 6D). Higher scores were associated with worse prognoses in acute myeloid leukemia (LAML), KIRC, and UVM (Figure 6D). Additionally, the association between chemokine scores and tumor mutation burden (TMB) as well as microsatellite instability (MSI) was explored. A positive relationship was identified between chemokine scores and TMB in cancers, including COAD, BRCA, BLCA, uterine corpus endometrial carcinoma (UCEC), and ovarian serous cystadenocarcinoma (OV), indicating that higher chemokine activity might coincide with increased mutation frequencies. In contrast, cancers such as ACC, thyroid carcinoma (THCA), testicular germ cell tumors (TGCT), PAAD, Mesothelioma (MESO), HNSC, GBM, and DLBCL showed a negative correlation (Figure 6E). Regarding MSI, COAD was the only cancer where a significant positive correlation with the chemokine score was observed (Figure 6F).
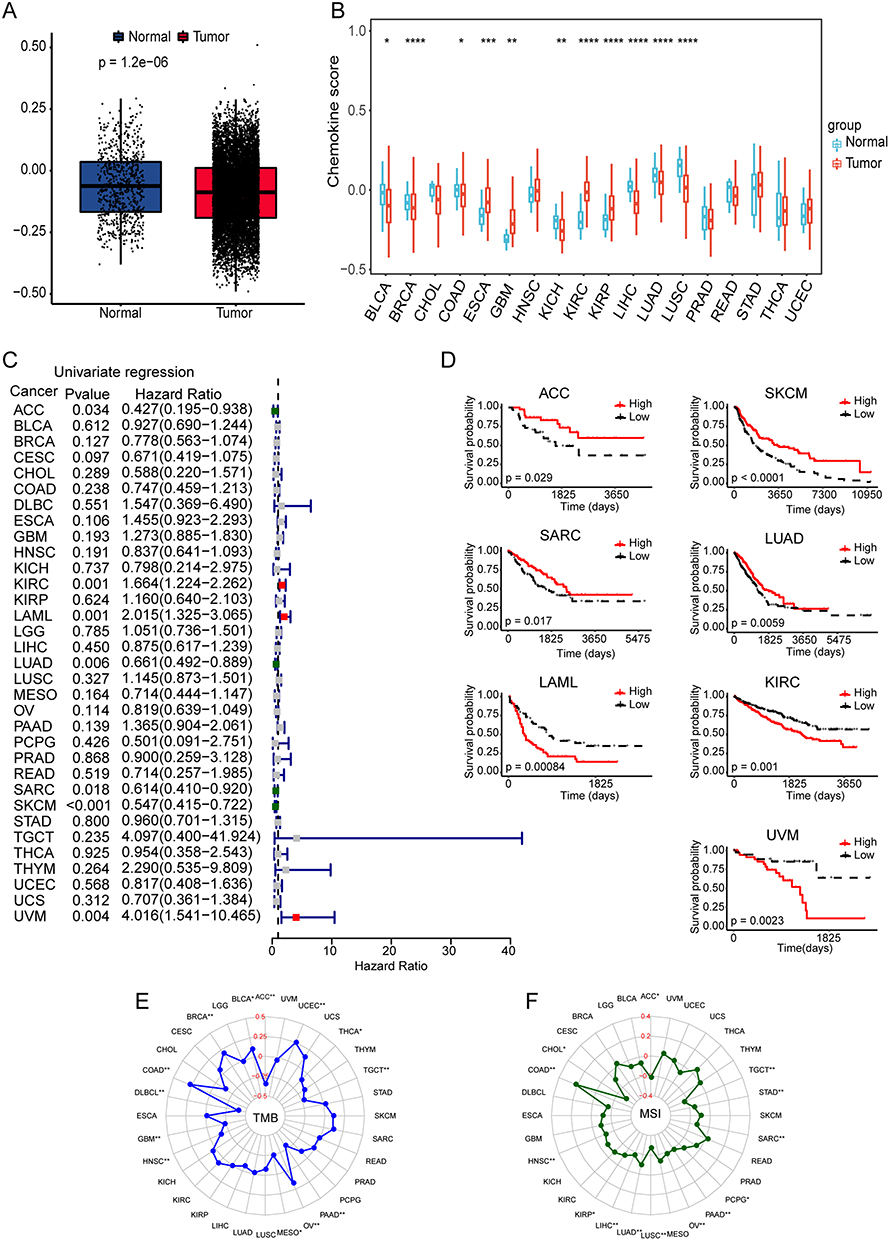 |
Figure 6 Chemokine score distribution and prognostic value. (A) Chemokine score distribution in pan-cancer samples. (B) Chemokine score of tumor and normal samples in individual cancer. (C) Univariate Cox regression of chemokine score in individual cancers. (D) Kaplan-Meier OS curves of chemokine score in the seven tumors most significantly associated with the outcome. (E) Radar map illustrating the relationship between chemokine score and TMB. (F) Radar map illustrating the relationship between chemokine score and MSI. *p < 0.05, **p < 0.01, ***p < 0.001, and ****p < 0.0001. |
Chemokine Score and Immune Checkpoint
The relationship between chemokine scores and immune checkpoint gene expression was assessed across various cancers (Figure 7). In these cancer types, chemokine scores demonstrated a strong positive correlation with the majority of immune checkpoint genes. Notably, genes such as PDCD1 (PD-1), CTLA4, TIGIT, CD48, CD70, and CD80 were positively associated with higher chemokine scores in several tumors, suggesting that elevated chemokine activity may drive the upregulation of these immune checkpoints. In contrast, VTCN1 was found to have a negative correlation with chemokine scores (Figure 7).
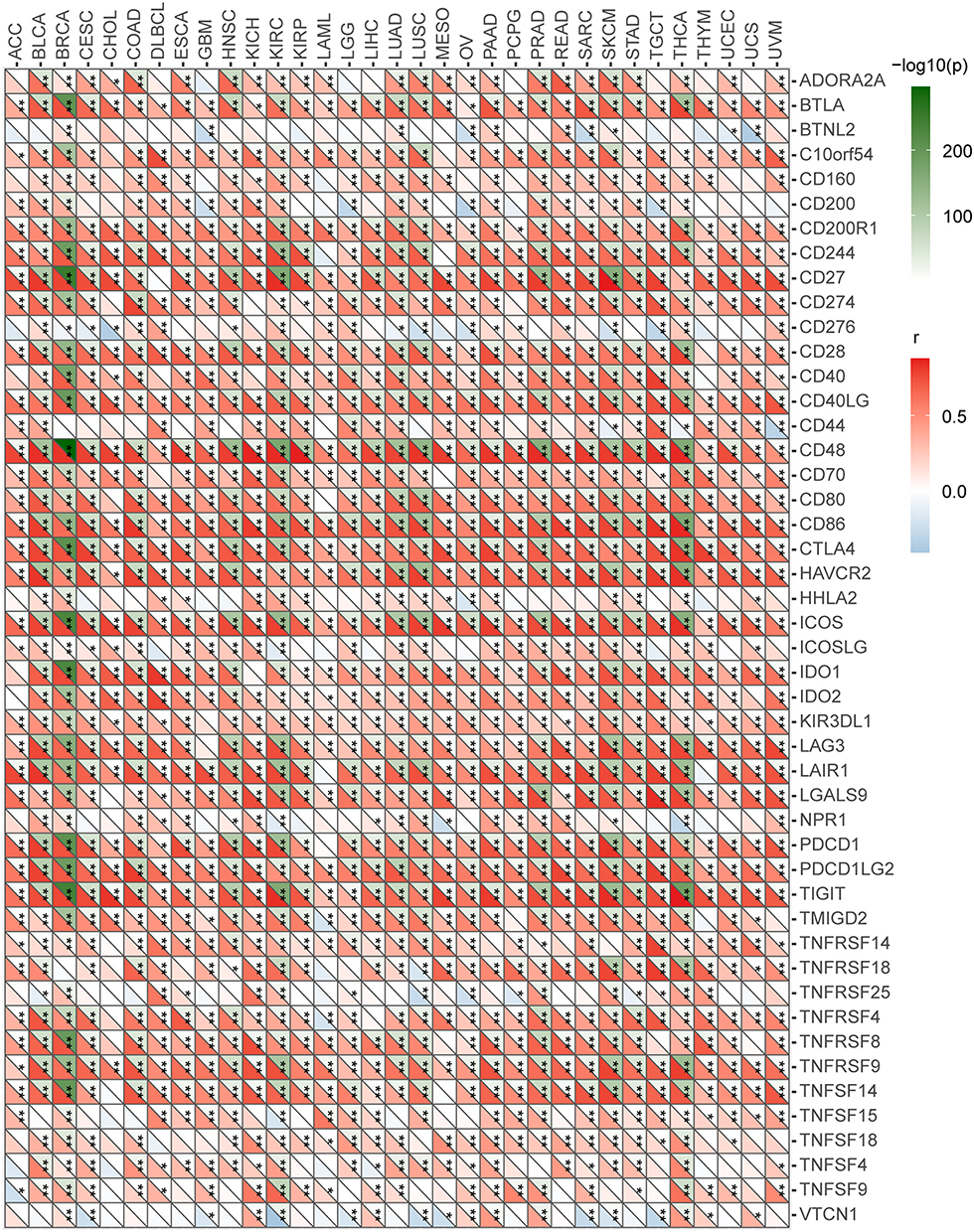 |
Figure 7 The relationship between chemokine score and immune checkpoint genes in individual cancers. *p < 0.05, **p < 0.01. |
Construction and Validation of a CaCRs-Based Signature in LUAD Cohorts
It is well known that lung cancer has a high morbidity and mortality rate.1 The screening and validation processes indicated that CaCRs possess strong prognostic significance in LUAD. Subsequently, a CaCRs-based signature was developed to predict clinical outcomes for LUAD patients in the TCGA cohort. From this analysis, sixteen prognostic CaCRs were selected and further analyzed using LASSO regression in the training cohort (Figure 8A). A risk model incorporating seven CaCRs was then established through multivariate Cox stepwise regression analysis (Figure 8B). The risk score for each LUAD patient was calculated (Table 1). A significant inverse correlation was observed between the risk score and chemokine score (Figure 8C). Based on the median risk score, patients in the training cohort (TCGA-LUAD) were stratified into high- and low-risk groups (Figure 8D). Individuals with higher risk scores exhibited shorter survival times (Figure 8E), and Kaplan–Meier survival analysis confirmed significantly reduced overall survival in the high-risk group compared to the low-risk group (Figure 8F). The AUC values for predicting 1-, 3-, and 5-year overall survival in the training cohort were 0.682, 0.676, and 0.652, respectively (Figure 8G). Additionally, gene expression profiles revealed that increasing risk scores were associated with decreased expression of CCR2, CCR4, CCR6, XCR1, CXCL17, and XCL2, and increased expression of CCL20 (Figure 8H).
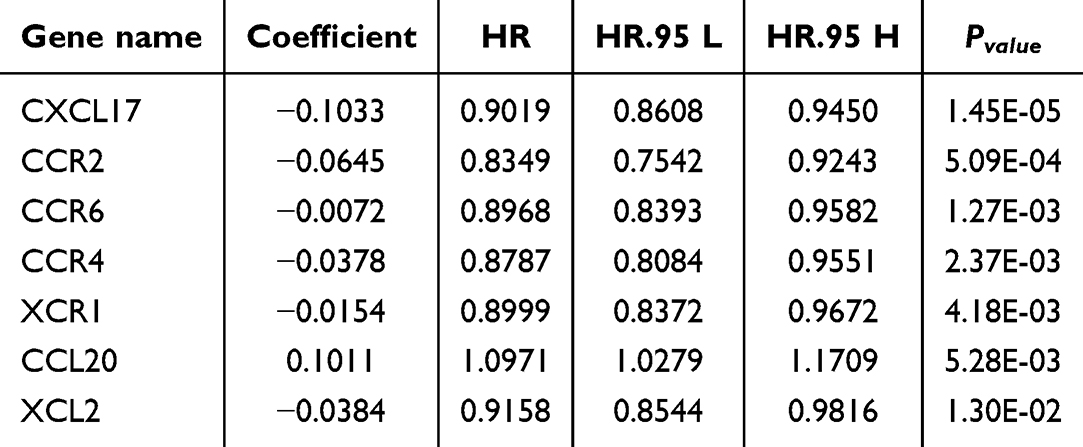 |
Table 1 Details of the Seven CaCRs in the Prognostic Mode |
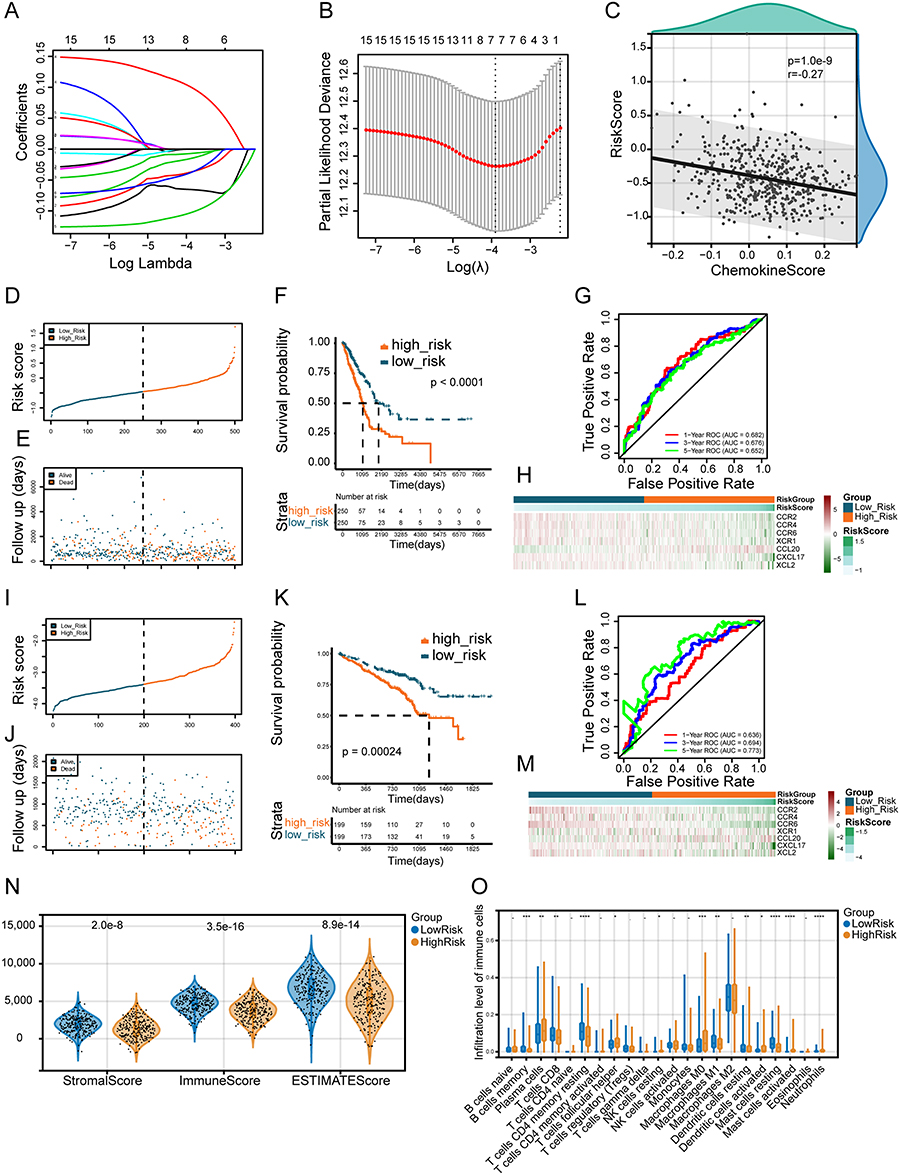 |
Figure 8 Construction and validation of a novel seven-gene signature of CaCRs in LUAD cohorts. (A) Lasso coefficients profiles of the prognosis-related CaCRs. (B) The association between deviance and log (lambda). (C) The correlation between risk score and chemokine score in the TCGA-LUAD cohort. (D) The distributions of the risk score in training cohorts. (E) Survival status of each patient in the training cohort. (F) Kaplan-Meier curves of OS-related CaCRs in training cohorts. (G) ROC curve for predicting survival by the risk score in the training cohorts. (H) Heatmap of the gene-expression profiles of model-related CaCRs in the training cohorts. (I) The distributions of the risk score in the external validation cohorts. (J) Survival status of each patient in the external validation cohorts. (K) Kaplan-Meier curves of OS-related CaCRs in the external validation cohorts. (L) ROC curve for predicting survival by the risk score in the external validation cohorts. (M) Heatmap of the gene-expression profiles of model-related CaCRs in the external validation cohorts. (N) The distribution of stromal score, immune score, and ESTIMATE score between high- and low-risk groups. (O) The distributions of immune cells between the high- and low-risk groups. *p < 0.05, **p < 0.01, ***p < 0.001, and ****p < 0.0001. |
In the validation cohort (GSE72094), similar patterns were observed. Patients were stratified into high- and low-risk groups based on the median risk score, and those in the high-risk group exhibited shorter survival durations and significantly worse overall survival (Figure 8I–K). The AUC values for predicting 1-, 3-, and 5-year overall survival in the validation cohort were 0.636, 0.694, and 0.773, respectively (Figure 8L). Gene expression trends consistent with those in the training cohort were also observed in the validation cohort (Figure 8M). These findings suggest that the CaCRs-based signature is a reliable predictor of survival outcomes in patients with LUAD.
Association of the CaCRs-Based Signature with Immune Cell Infiltration
The ESTIMATE algorithm was employed to calculate stromal, immune, and ESTIMATE scores for each TCGA-LUAD sample. Consistent with expectations, stromal, immune, and ESTIMATE scores were significantly higher in patients belonging to the low-risk group compared to those in the high-risk group (Figure 8N). Additionally, we examined the proportions of 22 infiltrating immune cell types between these groups. In the TCGA-LUAD cohort, the low-risk group exhibited significantly higher levels of infiltrating CD8+ T cells, resting memory CD4+ T cells, and M1 macrophages (Figure 8O). Conversely, the high-risk group was characterized by increased proportions of plasma cells, helper T cells, and M0 macrophages (Figure 8O).
Independent Prognostic Analysis and Construction of a Nomogram
Univariate and multivariate Cox regression analyses were conducted to assess the impact of clinicopathological characteristics (age, tumor stage, sex, T stage, N stage, and M stage) and the CaCRs-based signature risk score on the overall survival of LUAD patients in the TCGA cohort (Figure 9A and B). These analyses revealed that the CaCRs-based signature risk score, in conjunction with T stage and N stage, was an independent prognostic factor. These variables were subsequently utilized to develop a prognostic nomogram (Figure 9C). The calibration curves for 2-, 3-, and 5-year overall survival demonstrated strong alignment with the ideal model (Figure 9D). Lastly, Kaplan-Meier survival analysis showed that higher expression levels of CCL20 and lower expression levels of CCR2, CCR4, CCR6, CXCL17, XCL2, and XCR1 were significantly associated with improved survival outcomes in the TCGA-LUAD cohort (Figure 9E).
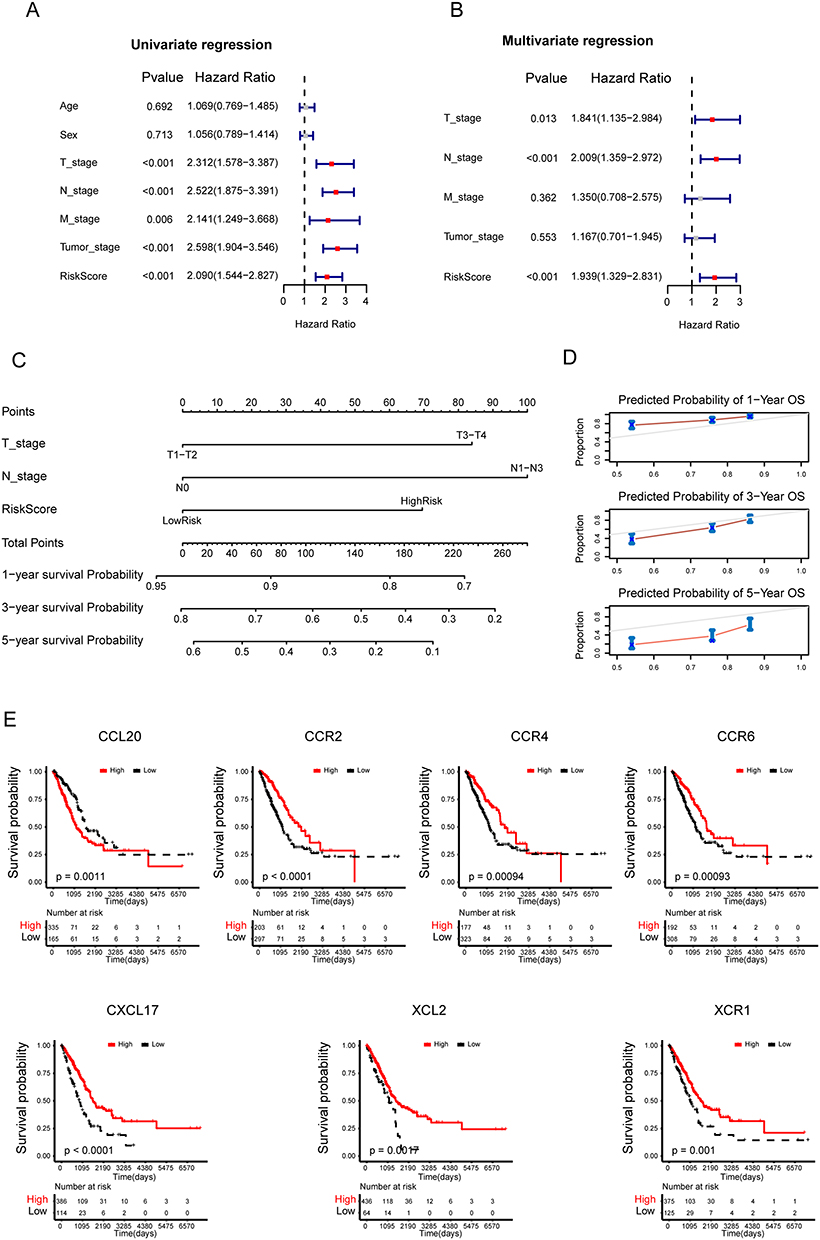 |
Figure 9 Construction of a nomogram and survival analysis of the seven-gene signature of CaCRs in LUAD cohorts. (A and B) Univariate (A) and multivariate (B) Cox regression analysis of clinicopathological variables and risk score in TCGA cohort; (C) Nomogram based on seven prognostic CaCRs predicting the overall survival probability of patients with LUAD; (D) 2-, 3- and 5-year calibration plots of the nomogram. (E) Kaplan-Meier curve analysis of the seven genes in the TCGA-LUAD cohort. |
Validation of Seven CaCRs Gene Expressions in Clinical Samples
We obtained 31 non-small cell lung cancer tissue samples and 31 adjacent normal tissues to evaluate the mRNA expression of seven core genes (Supplementary Table 3). Our findings revealed a marked increase in CCL20 expression within the tumor tissues, whereas CCR2, CCR4, CCR6, and XCR1 were significantly downregulated in these samples (Figure 10A–G). Additionally, immunohistochemical analysis was performed to assess CCL20 protein levels in four cases of lung adenocarcinoma and their corresponding adjacent normal tissues. This analysis confirmed a substantial increase in CCL20 expression within the tumor tissues (Figure 10H).
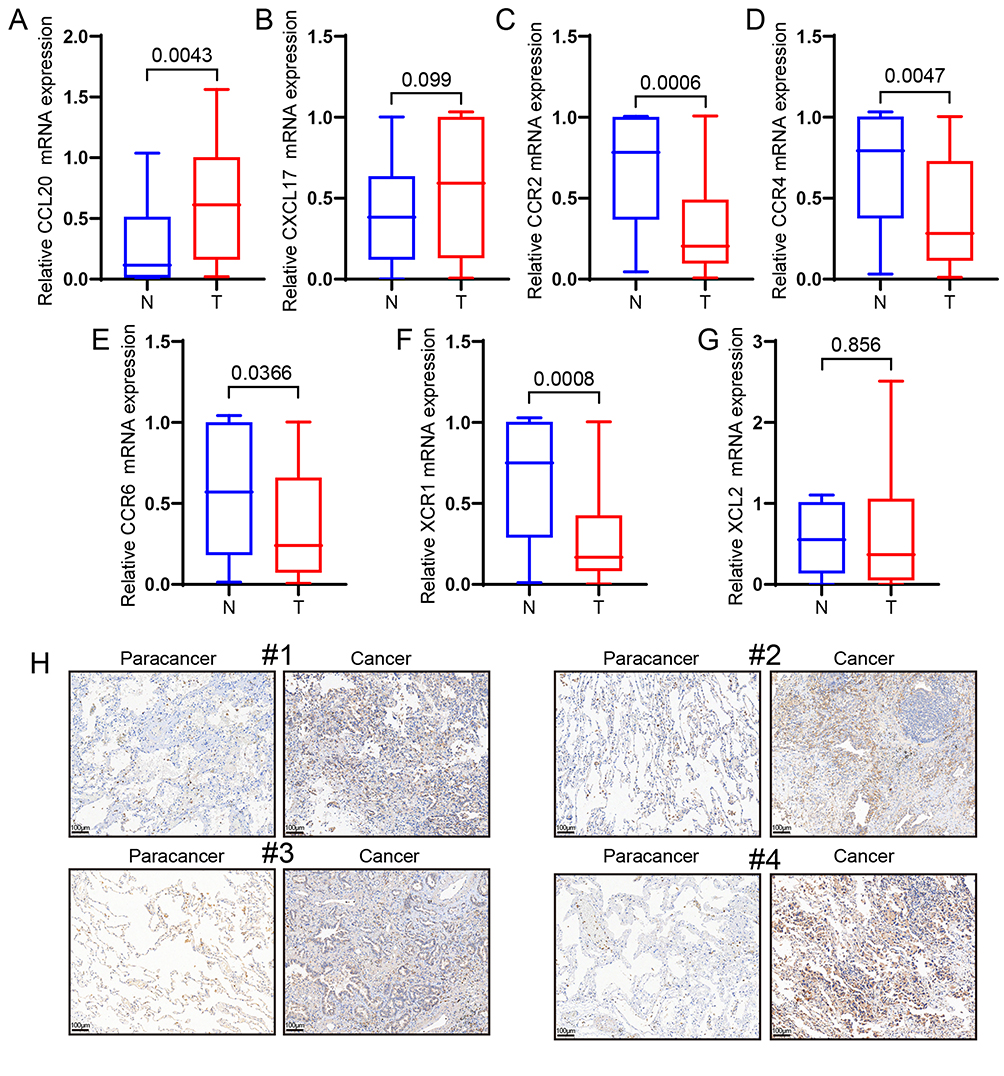 |
Figure 10 Validation of seven prognostic genes in clinical samples. (A–G) Relative expression of seven prognostic genes in non-small cell lung cancer and normal tissues. (H) The protein expression level of CCL20 in four pairs of lung adenocarcinoma and adjacent tissues (“#1”, “#2”, “#3”, and “#4” are used to indicate four individual patient samples). Data are shown as mean ± SEM. Statistical analysis was performed using two-tailed Student’s t-test. |
CCL20 Promotes A549 Cells Proliferation by Activating the MAPK Signaling Pathway
The CCL20 gene is one of the seven identified prognostic markers, demonstrating significant overexpression in NSCLC tissues compared to normal tissues. Experimental evidence indicates that silencing CCL20 suppresses the epithelial-mesenchymal transition (EMT) and reduces cell proliferation in lung adenocarcinoma cells.14 Additionally, CCL20 is a chemokine produced by macrophages.15 To explore the paracrine role of CCL20 in tumor cells, A549 cells were treated with CCL20. The findings revealed that low doses of CCL20 notably enhanced the proliferation of A549 cells (Figure 11A). Further analysis revealed that CCL20 activates the MAPK signaling pathway, as evidenced by the phosphorylation of JNK, ERK, and p38 (Figure 11B–E). Subsequently, A549 cells treated with CCL20 were exposed to JNK and ERK inhibitors. The findings demonstrated that inhibition of JNK or ERK effectively reduced CCL20-induced cell proliferation (Figure 11F and G). EdU analysis was used to further validate the suppressive impact of the JNK inhibitor SP600125 on the proliferation of A549 cells (Figure 11H and I). Collectively, these findings suggest that CCL20 induces A549 cell proliferation via activation of the MAPK signaling pathway.
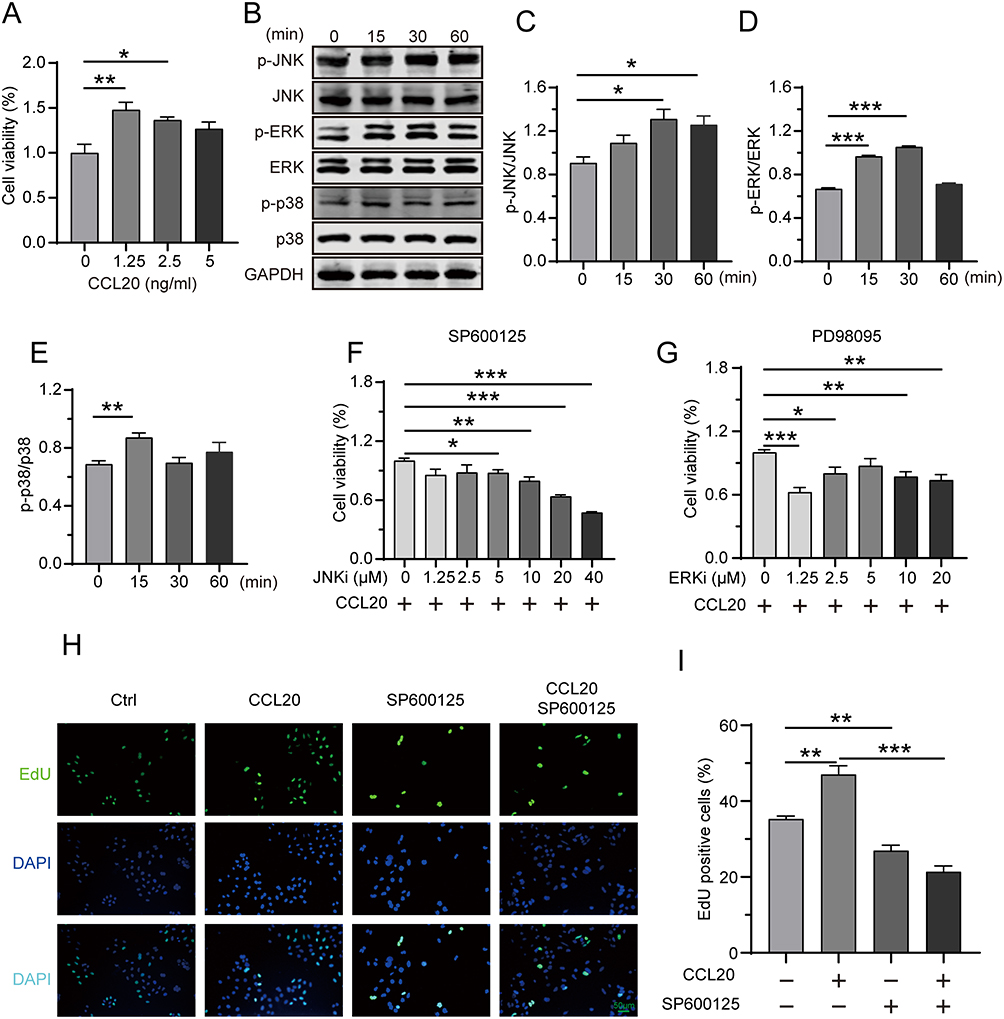 |
Figure 11 CCL20 promotes A549 cells proliferation by activating the MAPK signaling pathway. (A) Cell viability was measured in A549 cells treated with different concentrations of CCL20 using the CCK8. (B–E) The MAPK pathway was analyzed in CCL20-treated A549 cells by Western blot. (F and G) The viability of CCL20-treated A549 cells was examined in the presence of increasing concentrations of a JNK inhibitor (SP600125) or an ERK inhibitor (PD98095). (H and I) Cell proliferation was measured in CCL20-treated A549 cells with or without JNK inhibitor (SP600125) by EdU assay. Data are represented as mean ± SEM, *P < 0.05, **P < 0.01, ***P < 0.001 by one-way ANOVA. |
Discussion
The TME, composed of cancer, stromal, and immune cells, exhibits a diverse profile of CaCRs.6 CaCRs levels are often shaped by oncogenic drivers and sustained immune stress, both of which play a role in the dynamic modulation of the TME.7 The same chemokine axis contributes to both anti- and pro-tumorigenic responses, owing to heterogeneity in different tumor types.8,16 For instance, CCR2 promotes pancreatic cancer via monocyte recruitment,17 whereas mast cell–derived CCL2 recruits CCR2+ cytotoxic T cells, which possess a tissue-resident memory phenotype and enhanced cytotoxicity.17 XCR118 and CXCR319 are primarily linked to anti-tumor immunity, whereas others, such as CCR620 and CCR4,21 often support tumorigenesis. In pancreatic ductal adenocarcinoma (PDAC), a chemokine signature composed of CCL4, CCL5, CXCL9, and CXCL10 is associated with T cell–inflamed phenotypes and immunogenomic features.22
Chemokines remodel the TME by recruiting immune and stromal cells, thereby influencing responses to therapies.23 For instance, CCL2 can drive chemoresistance in ovarian cancer24 and EGFR-TKI resistance in NSCLC via EMT.25 IGFBP2 has been shown to upregulate CXCL1 expression via STAT3 signaling, enhancing the survival of lung cancer cells under gefitinib treatment,26 which is consistent with our finding that CXCL1 expression is negatively associated with gefitinib sensitivity. Recent studies have demonstrated that the CXCL12-CXCR4 signaling axis facilitates malignant progression and contributes to chemotherapy resistance in lung cancer by inducing EMT.27 CCL5 directly stimulates the proliferation of lung cancer cells.28 Multiple chemokine receptors, including CCR1, CCR3, and CCR5, enhance tumor cell migration and invasion through ligand–receptor interactions, highlighting their potential as novel therapeutic targets for suppressing tumor dissemination.28
Our analysis provides further evidence that the chemokine score is significantly associated with clinical outcomes in LUAD. Based on these insights, we propose the construction of a chemokine-related risk score model to comprehensively evaluate its prognostic value and potential utility in characterizing the immune landscape of LUAD. We developed a seven CaCRs-based (CCL20, CCR6, CXCL17, CCR2, CCR4, XCR1 and XCL2) signature that stratified LUAD into low- and high-risk groups. Across both internal and external cohorts, patients in the low-risk group showed significantly better overall survival compared to those in the high-risk group. Additionally, the low-risk group exhibited increased infiltration of immune cell subsets, particularly CD8+ T cells, which are closely associated with stronger anti-tumor activity and improved responses to immunotherapy.29 Furthermore, a model integrating T stage, N stage, and the seven-gene CaCRs risk score proved valuable in predicting the prognosis of LUAD patients, offering a potential tool for more personalized prognosis assessment and treatment planning.
Consistent with earlier research, elevated CCL20 levels in NSCLC are associated with a poorer prognosis.30,31 Silencing CCL20 expression has been shown to suppress EMT and reduce LUAD cell proliferation in both in vitro and in vivo studies.14 IL-1β has been reported to stimulate CCL20 production in lung cancer cells through activation of the MAPK and PI3K signaling pathways,32 suggesting a potential autocrine or paracrine role for CCL20 in tumor progression. We further demonstrate that exogenous CCL20 significantly promotes A549 cell proliferation through MAPK pathway activation. Similarly, recent evidence has revealed that PLIN3 is upregulated in LUAD and is associated with a poor prognosis, in part due to its capacity to enhance LUAD cell proliferation and migration, as well as mediate M2 macrophage infiltration.33 Although the interaction between CCL20 and its receptor, CCR6, promotes the recruitment of regulatory T cells (Tregs),16,34 we observed that CCR6 is typically expressed at lower levels in lung cancer, with lower CCR6 expression associated with poorer outcomes. CCR6-expressing CAR-T cells infiltrated solid tumors more efficiently, eradicated cancer cells, and significantly extended survival in tumor-bearing mice.35 This highlights the potential of CCL20-CCR6 as a target for enhancing the efficacy of CAR-T cells in solid tumors.
For CXCL17, lower expression in LUAD associates with poorer clinical outcomes, whereas CXCL17 overexpression in A549 enhances invasion and migration.36 These findings underscore the need for further in vivo studies to elucidate the molecular functions of CXCL17, particularly its impact on immune cell dynamics, given its ability to recruit myeloid-derived suppressor cells (MDSCs) and Tregs.37
CCR2 and CCR4 have been identified as potential prognostic markers for LUAD.38,39 Our analysis showed significant downregulation of CCR2 mRNA in lung cancer tissues. TREM2+ macrophages are recruited to intratumoral regions via the CCL2-CCR2 chemotactic axis.40 EGFR-mutated tumors appear to recruit Tregs predominantly through the CCL17/CCL22/CCR4 axis, creating a Treg-enriched TME.41 CCR4-positive Tregs are also drawn to the TME through the CCL2/CCR4 axis, where their interaction with tumor-associated macrophages enhances the metastatic potential of irradiated tumors to the lungs.42
XCR1 (also known as GPR5) is a G protein-coupled receptor (GPCR) that specifically binds the chemokine XCL1 and is predominantly highly expressed on conventional dendritic cell type 1 (cDC1).43 TIM-3 blockade enhances the spatial colocalization of CD8+ T cells with XCR1+ cDC1s and IL-12-dependent immunity.18 In NSCLC, neoadjuvant pembrolizumab plus chemotherapy expands XCR1+STING+CXCL9+ cDC1 within tumor tissues, indicating this cell subset may serve as a crucial biomarker for predicting immunotherapy response.44 High XCR1 predicts improved survival in HCC and restrains proliferation via MAPK and PI3K/AKT inhibition in vitro.45,46 Consistently, we have found XCR1 to be downregulated in NSCLC and associated with a poor prognosis, although the mechanisms remain to be defined.
XCL2 has progressively revealed its pivotal functions in tumorigenesis and progression. Existing studies have identified upregulated XCL2 expression in multiple malignancies, including angioimmunoblastic T-cell lymphoma47 and laryngeal squamous cell carcinoma.48 In this study, we observed that low XCL2 expression is correlated with a poor prognosis in LUAD. XCL1 and XCL2, primarily secreted by natural killer cells (NK cells), serve as key chemokines recruiting conventional type 1 dendritic cells (cDC1) into tumor sites,49 and also serve as single immune cell markers for predicting durable responses to immunotherapy in NSCLC.50
Despite its contributions, this study has some limitations. First, the analysis relied solely on data from public databases, which may have limited the specificity of the results. Second, some tumor types, such as GBM, have fewer corresponding adjacent tissue samples, which may lead to insufficient statistical power. Third, clinical tissue specimens are still limited, and larger-scale validation in well-characterized patient populations is still needed to further confirm the prognostic value of the identified chemokine markers. Fourth, this prognostic model demonstrated moderate predictive accuracy in LUAD cohort, which may be due to dataset heterogeneity, limited sample size, and technical variability. Future studies should validate this model in larger, multicenter cohorts and integrate more omics data to improve its performance. Lastly, the chemokine network exhibits diverse roles across various tumor types, highlighting the need for further validation in specific tumor settings.
Conclusion
In summary, we developed a chemokine score for pan-cancer analysis, which demonstrated strong prognostic value for patients with ACC, KIRC, LAML, LUAD, SARC, SKCM, and UVM. We identified a seven-gene signature derived from CaCRs that demonstrated robust accuracy and applicability in predicting clinical survival outcomes for patients with LUAD. Additionally, we found that exogenous CCL20 promotes the proliferation of A549 cells by activating the MAPK signaling pathway.
Data Sharing Statement
The datasets presented in this study are available in online repositories. https://toil.xenahubs.net, http://www.cbioportal.org, and http://www.ncbi.nlm.nih.gov/geo.
Acknowledgments
We sincerely thank the researchers who created and maintained TCGA, GEO data, and cBioPortal database.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Hubei Province (2024AFB296), Yichang Medical and Health Research Project (A23-1-025), and Open Fund Project of the Third-grade Pharmacological Laboratory on Traditional Chinese Medicine, State Administration of Traditional Chinese Medicine, China Three Gorges University (2023PTCM11).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA. 2024;74(1):12–49. doi:10.3322/caac.21820
2. Amini L, Silbert SK, Maude SL, et al. Preparing for CAR T cell therapy: patient selection, bridging therapies and lymphodepletion. Nat Rev Clin Oncol. 2022;19(5):342–355. doi:10.1038/s41571-022-00607-3
3. Offringa R, Kötzner L, Huck B, Urbahns K. The expanding role for small molecules in immuno-oncology. Nat Rev Drug Discov. 2022;21(11):821–840. doi:10.1038/s41573-022-00538-9
4. Peng H, Pan Y, Sun Y, et al. Hyperglycemia induces an immunosuppressive microenvironment in colorectal cancer liver metastases by recruiting peripheral blood monocytes through the CCL3-CCR1 axis. J ImmunoTher Cancer. 2025;13(6):e011310. doi:10.1136/jitc-2024-011310
5. Mantovani A, Savino B, Locati M, Zammataro L, Allavena P, Bonecchi R. The chemokine system in cancer biology and therapy. Cytokine Growth Factor Rev. 2010;21(1):27–39. doi:10.1016/j.cytogfr.2009.11.007
6. Griffith JW, Sokol CL, Luster AD. Chemokines and chemokine receptors: positioning cells for host defense and immunity. Ann Rev Immunol. 2014;32:659–702. doi:10.1146/annurev-immunol-032713-120145
7. Ozga AJ, Chow MT, Luster AD. Chemokines and the immune response to cancer. Immunity. 2021;54(5):859–874. doi:10.1016/j.immuni.2021.01.012
8. Yi M, Li T, Niu M, et al. Targeting cytokine and chemokine signaling pathways for cancer therapy. Sig Transduct and Targeted Ther. 2024;9(1):176. doi:10.1038/s41392-024-01868-3
9. Chow MT, Luster AD. Chemokines in cancer. Cancer Immunol Res. 2014;2(12):1125–1131. doi:10.1158/2326-6066.Cir-14-0160
10. Kumar A, Mohamed E, Tong S, et al. CXCL14 promotes a robust brain tumor-associated immune response in glioma. Clin Cancer Res. 2022;28(13):2898–2910. doi:10.1158/1078-0432.Ccr-21-2830
11. Limagne E, Nuttin L, Thibaudin M, et al. MEK inhibition overcomes chemoimmunotherapy resistance by inducing CXCL10 in cancer cells. Cancer Cell. 2022;40(2):136–152.e12. doi:10.1016/j.ccell.2021.12.009
12. Xu W, Wu Y, Liu W, et al. Tumor-associated macrophage-derived chemokine CCL5 facilitates the progression and immunosuppressive tumor microenvironment of clear cell renal cell carcinoma. Int J Bio Sci. 2022;18(13):4884–4900. doi:10.7150/ijbs.74647
13. Foeng J, Comerford I, McColl SR. Harnessing the chemokine system to home CAR-T cells into solid tumors. Cell Rep Med. 2022;3(3):100543. doi:10.1016/j.xcrm.2022.100543
14. Fan T, Li S, Xiao C, et al. CCL20 promotes lung adenocarcinoma progression by driving epithelial-mesenchymal transition. Int J Bio Sci. 2022;18(11):4275–4288. doi:10.7150/ijbs.73275
15. Lin W, Luo Y, Wu J, et al. Loss of ADAR1 in macrophages in combination with interferon gamma suppresses tumor growth by remodeling the tumor microenvironment. J ImmunoTher Cancer. 2023;11(11):e007402. doi:10.1136/jitc-2023-007402
16. Wang Y, Chen W, Qiao S, et al. Lipid droplet accumulation mediates macrophage survival and Treg recruitment via the CCL20/CCR6 axis in human hepatocellular carcinoma. Cell Mol Immunol. 2024;21(10):1120–1130. doi:10.1038/s41423-024-01199-x
17. Sanford DE, Belt BA, Panni RZ, et al. Inflammatory monocyte mobilization decreases patient survival in pancreatic cancer: a role for targeting the CCL2/CCR2 axis. Clin Cancer Res. 2013;19(13):3404–3415. doi:10.1158/1078-0432.Ccr-13-0525
18. Gardner A, de Mingo Pulido Á, Hänggi K, et al. TIM-3 blockade enhances IL-12-dependent antitumor immunity by promoting CD8 + T cell and XCR1 + dendritic cell spatial co-localization. J ImmunoTher Cancer. 2022;10(1):e003571. doi:10.1136/jitc-2021-003571
19. Russo E, D’Aquino C, Di Censo C, et al. Cxcr3 promotes protection from colorectal cancer liver metastasis by driving NK cell infiltration and plasticity. J Clin Invest. 2025;135(11). doi:10.1172/jci184036
20. Hanna DN, Smith PM, Novitskiy SV, et al. SMAD4 suppresses colitis-associated carcinoma through inhibition of CCL20/CCR6-mediated inflammation. Gastroenterology. 2022;163(5):1334–1350.e14. doi:10.1053/j.gastro.2022.07.016
21. Marshall LA, Marubayashi S, Jorapur A, et al. Tumors establish resistance to immunotherapy by regulating T reg recruitment via CCR4. J ImmunoTher Cancer. 2020;8(2):e000764. doi:10.1136/jitc-2020-000764
22. Romero JM, Grünwald B, Jang GH, et al. A four-chemokine signature is associated with a T-cell-inflamed phenotype in primary and metastatic pancreatic cancer. Clin Cancer Res. 2020;26(8):1997–2010. doi:10.1158/1078-0432.Ccr-19-2803
23. Nagarsheth N, Wicha MS, Zou W. Chemokines in the cancer microenvironment and their relevance in cancer immunotherapy. Nat Rev Immunol. 2017;17(9):559–572. doi:10.1038/nri.2017.49
24. Yang YI, Wang YY, Ahn JH, Kim BH, Choi JH. CCL2 overexpression is associated with paclitaxel resistance in ovarian cancer cells via autocrine signaling and macrophage recruitment. Biomed Pharmacother. 2022;153:113474. doi:10.1016/j.biopha.2022.113474
25. Diao Y, Huang S, Liu F, et al. CCL2 promotes EGFR-TKIs resistance in non-small cell lung cancer via the AKT-EMT pathway. Acta Biochim Biophys Sin. 2024;56(10):1549–1560. doi:10.3724/abbs.2024106
26. Lu H, Ai J, Zheng Y, et al. IGFBP2/ITGA5 promotes gefitinib resistance via activating STAT3/CXCL1 axis in non-small cell lung cancer. Cell Death Dis. 2024;15(6):447. doi:10.1038/s41419-024-06843-y
27. Yang Y, Li J, Lei W, et al. CXCL12-CXCR4/CXCR7 axis in cancer: from mechanisms to clinical applications. Int J Bio Sci. 2023;19(11):3341–3359. doi:10.7150/ijbs.82317
28. Dong Z, Wu J, He L, et al. EGCG inhibits tobacco smoke-promoted proliferation of lung cancer cells through targeting CCL5. Phytomedicine. 2025;139:156512. doi:10.1016/j.phymed.2025.156512
29. Yenyuwadee S, Aliazis K, Wang Q, et al. Immune cellular components and signaling pathways in the tumor microenvironment. Semi Cancer Biol. 2022;86(Pt 2):187–201. doi:10.1016/j.semcancer.2022.08.004
30. Wang GZ, Cheng X, Li XC, et al. Tobacco smoke induces production of chemokine CCL20 to promote lung cancer. Cancer Lett. 2015;363(1):60–70. doi:10.1016/j.canlet.2015.04.005
31. Zhang CY, Qi Y, Li XN, et al. The role of CCL20/CCR6 axis in recruiting Treg cells to tumor sites of NSCLC patients. Biomed Pharmacother. 2015;69:242–248. doi:10.1016/j.biopha.2014.12.008
32. Wang B, Shi L, Sun X, Wang L, Wang X, Chen C. Production of CCL20 from lung cancer cells induces the cell migration and proliferation through PI3K pathway. J Cell Mol Med. 2016;20(5):920–929. doi:10.1111/jcmm.12781
33. Yang S, Liu H, Zheng Y, et al. The role of PLIN3 in prognosis and tumor-associated macrophage infiltration: a pan-cancer analysis. J Inflamm Res. 2025;18:3757–3777. doi:10.2147/jir.S509245
34. Pant A, Jain A, Chen Y, et al. The CCR6–CCL20 axis promotes regulatory t-cell glycolysis and immunosuppression in tumors. Cancer Immunol Res. 2024;12(11):1542–1558. doi:10.1158/2326-6066.Cir-24-0230
35. Jin L, Cao L, Zhu Y, et al. Enhance anti-lung tumor efficacy of chimeric antigen receptor-T cells by ectopic expression of C-C motif chemokine receptor 6. Sci Bull. 2021;66(8):803–812. doi:10.1016/j.scib.2020.12.027
36. Koni E, Congur I, Tokcaer Keskin Z. Overexpression of CXCL17 increases migration and invasion of A549 lung adenocarcinoma cells. Front Pharmacol. 2024;15:1306273. doi:10.3389/fphar.2024.1306273
37. Oka T, Sugaya M, Takahashi N, et al. CXCL17 attenuates imiquimod-induced psoriasis-like skin inflammation by recruiting myeloid-derived suppressor cells and regulatory T cells. J Immunol. 2017;198(10):3897–3908. doi:10.4049/jimmunol.1601607
38. Zhang MY, Huo C, Liu JY, et al. Identification of a five autophagy subtype-related gene expression pattern for improving the prognosis of lung adenocarcinoma. Front Cell Develop Biol. 2021;9:756911. doi:10.3389/fcell.2021.756911
39. Karasaki T, Qiang G, Anraku M, et al. High CCR4 expression in the tumor microenvironment is a poor prognostic indicator in lung adenocarcinoma. J Thoracic Dis. 2018;10(8):4741–4750. doi:10.21037/jtd.2018.07.45
40. Wang Q, Wu Y, Jiang G, Huang X. Galectin-3 induces pathogenic immunosuppressive macrophages through interaction with TREM2 in lung cancer. J Exp Clin Cancer Res. 2024;43(1):224. doi:10.1186/s13046-024-03124-6
41. Zhao Y, Tang G, Li J, Bian X, Zhou X, Feng J. Integrative transcriptome analysis reveals the molecular events underlying impaired T-cell responses in EGFR-mutant lung cancer. Sci Rep. 2024;14(1):18366. doi:10.1038/s41598-024-69020-3
42. Chiang Y, Lu LF, Tsai CL, et al. C-C chemokine receptor 4 (CCR4)-positive regulatory T cells interact with tumor-associated macrophages to facilitate metastatic potential after radiation. Eur J Cancer. 2024;198:113521. doi:10.1016/j.ejca.2023.113521
43. Zhang X, Schlimgen RR, Singh S, Tomani MP, Volkman BF, Zhang C. Molecular basis for chemokine recognition and activation of XCR1. Proc Natl Acad Sci USA. 2024;121(48):e2405732121. doi:10.1073/pnas.2405732121
44. Wang J, Li S, Wang M, et al. STING licensing of type I dendritic cells potentiates antitumor immunity. Sci immunol. 2024;9(92):eadj3945. doi:10.1126/sciimmunol.adj3945
45. Wu W, Bao Z, Zhu K, et al. XCR1: a promising prognostic marker that pinpoints targeted and immune-based therapy in hepatocellular carcinoma. Heliyon. 2024;10(11):e31968. doi:10.1016/j.heliyon.2024.e31968
46. Yanru W, Zhenyu B, Zhengchuan N, Qi Q, Chunmin L, Weiqiang Y. Transcriptomic analyses of chemokines reveal that down-regulation of XCR1 is associated with advanced hepatocellular carcinoma. Biochem Biophys Res Commun. 2018;496(4):1314–1321. doi:10.1016/j.bbrc.2018.02.008
47. Pritchett JC, Yang ZZ, Kim HJ, et al. High-dimensional and single-cell transcriptome analysis of the tumor microenvironment in angioimmunoblastic T cell lymphoma (AITL). Leukemia. 2022;36(1):165–176. doi:10.1038/s41375-021-01321-2
48. Liu W, Zhang C, Gong X, Liao W, Xu J, Zhang X. Prognostic value of immune-related genes in laryngeal squamous cell carcinoma. Transl Cancer Res. 2020;9(10):6287–6302. doi:10.21037/tcr-20-2173
49. Böttcher JP, Bonavita E, Chakravarty P, et al. NK cells stimulate recruitment of cDC1 into the tumor microenvironment promoting cancer immune control. Cell. 2018;172(5):1022–1037.e14. doi:10.1016/j.cell.2018.01.004
50. Poma AM, Bruno R, Pietrini I, et al. Biomarkers and gene signatures to predict durable response to pembrolizumab in non-small cell lung cancer. Cancers. 2021;13(15):3828. doi:10.3390/cancers13153828
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic and Immunological Roles of Cell Cycle Regulator CDCA5 in Human Solid Tumors
He J, Zhou X, Wang X, Zhang Q, Zhang L, Wang T, Zhu W, Liu P, Zhu M
International Journal of General Medicine 2022, 15:8257-8274
Published Date: 21 November 2022
Comprehensive Analysis Reveals Distinct Immunological and Prognostic Characteristics of CD276/B7-H3 in Pan-Cancer
Ding J, Sun Y, Sulaiman Z, Li C, Cheng Z, Liu S
International Journal of General Medicine 2023, 16:367-391
Published Date: 2 February 2023
Pan-Cancer Profiling and Digital Pathology Analysis Reveal Negative Prognostic Biomarker ZPR1 Associated with Immune Infiltration and Treatment Response in Hepatocellular Carcinoma
He L, Xie Y, Qiu Y, Zhang Y
Journal of Hepatocellular Carcinoma 2023, 10:1309-1325
Published Date: 9 August 2023
Role of Kinetochore Scaffold 1 (KNL1) in Tumorigenesis and Tumor Immune Microenvironment in Pan-Cancer: Bioinformatics Analyses and Validation of Expression
Ding Y, Wang K, Zhao S, Li Y, Qiu W, Zhu C, Wang Y, Dong C, Liu J, Lu Y, Qi W
International Journal of General Medicine 2023, 16:4883-4906
Published Date: 31 October 2023
IER5L is a Prognostic Biomarker in Pan-Cancer Analysis and Correlates with Immune Infiltration and Immune Molecules in Non-Small Cell Lung Cancer
Chen X, He YQ, Miao TW, Yin J, Liu J, Zeng HP, Zhu Q
International Journal of General Medicine 2023, 16:5889-5908
Published Date: 13 December 2023