Back to Journals » Journal of Inflammation Research » Volume 19
Identification of Monocyte CD11c as a Potential Biomarker for Distinguishing Sepsis From Non-Infectious Inflammation and Predicting the Outcome of Sepsis
Authors Kong L, Zhou Y, Li D, Hua N, Zhang Y, Li H, Ding P, Nan Y, Zhou H ![]() , Yang P, Shuai W, Zhang S, Ju Y, Yang X, Song J, Liu X, Yu W, Jiang S
, Yang P, Shuai W, Zhang S, Ju Y, Yang X, Song J, Liu X, Yu W, Jiang S
Received 18 August 2025
Accepted for publication 24 January 2026
Published 17 February 2026 Volume 2026:19 557223
DOI https://doi.org/10.2147/JIR.S557223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anh Ngo
Limin Kong,1,* Yujun Zhou,1,* Dawei Li,2,* Ning Hua,3 Yanfang Zhang,1 Hangyang Li,4 Peili Ding,4 Yuyu Nan,4 Hua Zhou,5 Ping Yang,1 Wuping Shuai,1 Sheng Zhang,6 Yuanzhi Ju,1 Xiaohui Yang,7 Jiasheng Song,7 Xuesong Liu,2 Wenqiao Yu,4 Saiping Jiang1
1Department of Clinical Pharmacy, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2College of Pharmaceutical Sciences, Zhejiang University, Hangzhou, People’s Republic of China; 3Department of Biophysics, and Department of Neurology of The Fourth Affiliated Hospital, Zhejiang University School of Medicine, Yiwu, People’s Republic of China; 4Department of Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 6Department of Intensive Care Unit, Taizhou Hospital of Zhejiang Province, Taizhou, People’s Republic of China; 7School of Pharmacy, Hangzhou Normal University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenqiao Yu, Department of Intensive Care Unit, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected] Saiping Jiang, Department of Clinical Pharmacy, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Objective: To investigate whether monocyte CD11c (mCD11c) can serve as a promising biomarker for the diagnosis and prognosis of sepsis, distinguishing it from non-infectious inflammatory conditions.
Methods: A prospective, observational cohort study was conducted using a discovery cohort (sepsis, mild infection, patients after cardiovascular surgery, recovered sepsis patients, and healthy controls) and a validation cohort (sepsis, mild infection, and patients after cardiovascular surgery). Peripheral blood samples were analyzed using Cytometry by Time-of-Flight (CyTOF), single-cell RNA sequencing, and flow cytometry to assess the immune cell composition and mCD11c expression. Clinical data and outcomes were collected for analysis.
Results: The discovery cohort showed a significant downregulation of mCD11c in patients with sepsis. The validation cohort confirmed a lower mCD11c% in sepsis than in the other groups. Receiver operating characteristic (ROC) curve analysis showed that mCD11c had a higher AUC (0.939, P < 0.001) than traditional markers in distinguishing sepsis from non-infectious inflammation. mCD11c% was an independent prognostic factor for 7-day mortality (P < 0.05), with significant differences in survival rates between patients with mCD11c% above and below 96.445%.
Conclusion: mCD11c is a promising biomarker for early sepsis diagnosis and short-term survival prediction, outperforming the traditional markers. Larger multicenter studies are needed to validate these findings and to explore their potential as intervention targets.
Keywords: sepsis, biomarker, monocyte CD11c, diagnostic value, survival prognosis
Sepsis is characterized by a dysregulated host response to infection leading to life-threatening organ dysfunction.1,2 Delayed treatment has been identified as a significant risk factor for mortality in patients with sepsis.3 Early identification and appropriate therapy initiation are crucial in reducing sepsis-related deaths, highlighting the importance of timely and accurate diagnosis.4
Currently, there is no gold standard for sepsis diagnosis. Traditional inflammatory indicators, such as C-reactive protein (CRP), interleukin-6 (IL-6), and white blood cell (WBC) counts, show limited diagnostic specificity for sepsis. Procalcitonin (PCT) is the only marker in clinical guidelines used for guiding antibiotic usage, but recent meta-analysis also revealed its unreliability in distinguishing infected from uninfected patients in critically ill cohorts.5 The Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sepsis-related Organ Failure Assessment (SOFA)6 scores were widely used for diagnosing sepsis and assessing its severity and outcomes, but they are limited by complex calculations and lack of speed and simplicity. Given these challenges, the search for new sepsis biomarkers is crucial for improving diagnostic accuracy, optimizing treatment, and determining the timing of antibiotic use in clinical settings. Previous studies have shown that CD11c expression on neutrophils exhibits high sensitivity and specificity for sepsis diagnosis,7 and it is involved in the recruitment of monocytes and macrophages during inflammatory responses.8 These findings suggest a potential link between CD11c expression and sepsis pathogenesis. However, the role of CD11c expressed specifically by monocytes (mCD11c) in sepsis-particularly its diagnostic and prognostic value-has not been systematically studied, representing a key knowledge gap.
With the advancements in high-dimensional immunoassay techniques, multi-omics technologies have been widely used to search for new biomarkers in sepsis.9–11 This study used mass cytometry (Cytometry by Time-of-Flight, CyTOF) combined with flow cytometry to detect the changes of immune components in peripheral blood of patients with sepsis, and aimed to solve this gap by studying whether the expression of mCD11c in patients with sepsis was significantly lower than that in patients with non-infectious inflammation and healthy controls. We hypothesized that mCD11c could be used as a potential biomarker to distinguish sepsis from noninfectious inflammatory state and predict short-term clinical outcomes.
Material and Methods
Study Design
This prospective, observational cohort study was conducted in the First Affiliated Hospital, Zhejiang University School of Medicine between April 2022 and May 2024. The study comprised two independent cohorts, namely the discovery and validation cohorts, and the workflow for the study is illustrated in Figure 1. The discovery cohort involved five distinct groups: 1) patients diagnosed with sepsis (Sepsis); 2) patients who had undergone cardiovascular surgery representing non-infectious inflammation (Surgery); 3) patients who recovered from sepsis (Recovery); 4) patients with mild infection (Mild); and 5) age- and sex-matched healthy donors (Healthy Controls, HC). The validation cohort consisted of three distinct groups: Sepsis, Surgery, and Mild.
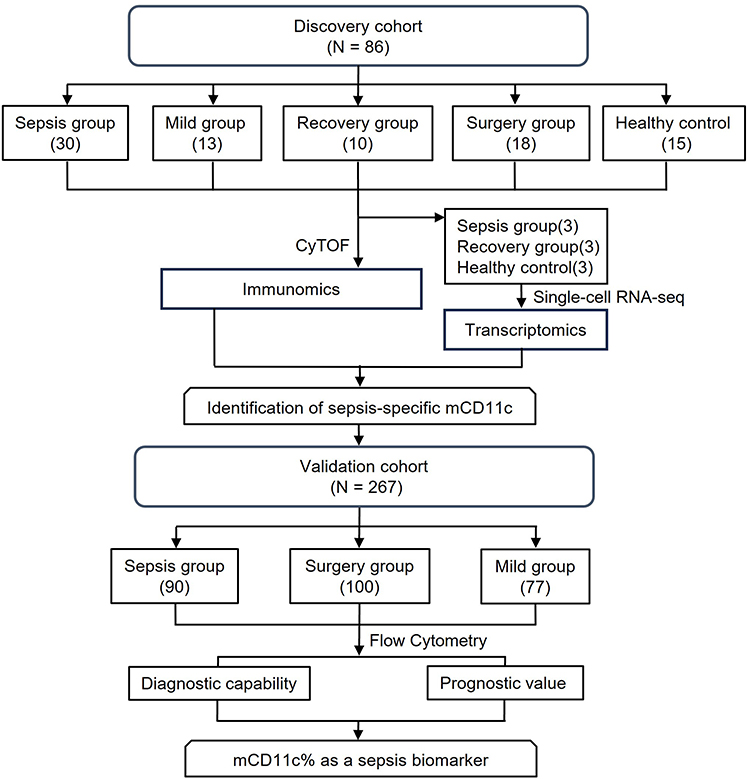 |
Figure 1 Workflow chart of the study. |
Peripheral blood samples (5 mL per person) of the Sepsis, Mild, and Surgery groups were collected within 24 hours after infection diagnosis or after surgery, while the blood samples of the Recovery group were collected again on the seventh day after the patient was diagnosed with sepsis. All the samples were transported to the laboratory for further processing within 12h at room temperature. More details on peripheral blood mononuclear cells (PBMCs) processing are provided in Supplementary Methods.
Inclusion and Exclusion Criteria
Patients in the Sepsis group should be diagnosed according to the definition of Sepsis 3.0,12,13 which requires a clear focus of infection or positive blood culture and a SOFA score of 2 or higher. Patients in the Recovery group were previously diagnosed with sepsis, but later showed improvement in clinical symptoms and laboratory tests, with SOFA scores decreasing by > 2 from baseline. After expert assessment, they were deemed to have recovered and enrolled in the study. Patients in the Mild group were diagnosed with infection; however, the SOFA score increased by less than 2. All types of cardiovascular surgery in the Surgery group were confirmed using the ICD9-CM-3 operation code.14 Individuals under the age of 18, those who were pregnant or breastfeeding, as well as patients diagnosed with malignancies, organ transplants, HIV infection, or autoimmune diseases, and those receiving immunosuppressive therapy were excluded from the cohort study. The inclusion and exclusion criteria for the patients in the discovery and validation cohorts were consistent.
Cytometry by Time-of-Flight Analysis
PBMCs were collected from 30 Sepsis patients, 13 Mild patients, 10 Recovery patients, 18 Surgery patients, and 15 HC subjects for CyTOF analysis (Figure 2A). The antibody panel comprised of 42 markers (Table S1). CyTOF experiments were conducted by PLTTECH (Hangzhou, China), and the sample processing and analysis processes are detailed in the Supplementary Methods.
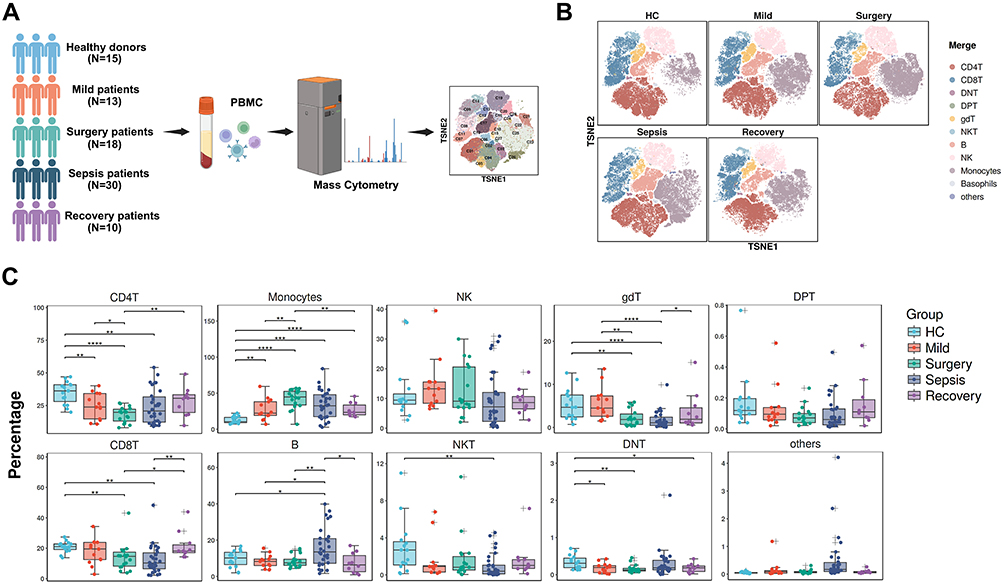 |
Figure 2 Analysis of major peripheral immune composition of sepsis patients by CyTOF. (A) The flow chart of the experimental design of the CyTOF analysis. The number of each group are shown. (B) T-SNE projection of peripheral blood cells in each group analyzed by CyTOF. (C) Box plots were employed to present the distribution of major immune cell subsets among the different groups. Statistical significance was denoted by *, P < 0.05; **, P < 0.01; ***, P < 0.001; ****, P < 0.0001. |
Single-Cell RNA-Sequencing
PBMCs from 3 Sepsis patients, 3 Recovery patients, and 3 HC subjects were collected for single-cell RNA-sequencing to verify the immune signatures that distinguished sepsis from the other groups. Detailed processes are provided in the Supplementary Methods.
Flow Cytometric Analysis
PBMCs from 90 Sepsis patients, 77 Mild patients, and 100 Surgery patients were collected, processed using the same method as for CyTOF, and analyzed using flow cytometry. The analysis process is described in detail in the Supplementary Methods.
Clinical Data Collection
Collected clinical data and demographic characteristics of the patients, including gender, age, underlying diseases, infection sites, infectious pathogens, WBC counts, percentage of neutrophils, CRP, PCT, blood creatinine, and bilirubin within 24 h of blood collection, as well as the APACHE II and SOFA scores within 24 h of admission for the Sepsis or Surgery group. During the follow-up period, mortality rates of the Sepsis group at 7-day, 14-day, and 28-day were recorded.
Statistical Analysis
Statistical software SPSS 26.0 and R v4.3.1, were used for data processing. The measurement data that conformed to the normal distribution were represented as mean ± standard deviation, and an independent sample t-test was used for inter-group comparisons. Measurement data that did not follow a normal distribution were represented as median (quartile) IM (QL, QU); intergroup comparisons were performed using the Mann–Whitney U-test. Categorical data are expressed as percentages. Receiver operating characteristic (ROC) curves were plotted to evaluate the predictive ability of CD11c for sepsis. Cox regression analysis was used to perform univariate and multivariate survival analyses for the sepsis group. Kaplan-Meier survival curves were generated to analyze the relationship between mCD11c and clinical outcome (7-day, 14-day and 28-day mortality), and between-group comparisons of Kaplan-Meier survival curves were performed using the Log rank test. P ≤ 0.05 was used to indicate statistical significance.
Results
Patient Characteristics
A total of 30 Sepsis patients, 13 Mild patients, 18 Surgery patients, 10 Recovery patients, and 15 HC subjects were enrolled in the discovery cohort. The validation cohort included 90 Sepsis patients, 77 Mild patients and 100 Surgery patients, and the Sepsis patients had significantly higher APACHE II and SOFA scores on the day of ICU admission than that of Surgery patients. The median WBC, CRP, and PCT levels of Sepsis patients in the validation cohort were also significantly higher than those in the Mild and Surgery groups. The basic demographic and clinical characteristics of the participants are summarized in Table S2.
Peripheral Immune Composition in Patients with Sepsis
We detected 42 leukocyte markers in each sample, including surface and intracellular markers, which defined 28 subpopulations (Figure S1) across ten distinct immune cell types (Figure 2B): CD4 positive T cells (CD4+ T cells), CD8 positive T cells (CD8+ T cells), double-negative T cells (DNT), double-positive T cells (DPT), γδT cells (gdT), natural killer T cells (NKT cells), B cells, natural killer cells (NK cells), monocytes, and basophils. The peripheral immune composition undergoes significant changes during the onset of sepsis. Compared to the HC group, we observed significant decreases in CD4+ T cells, CD8+ T cells, γδT cells, and NKT cells, while there was an obvious increase in B cells and monocytes (Figure 2C). No significant alterations were observed in NK or DPT cells across different groups (Figure 2C). After comparing changes in immune cell lineages, we selected monocyte clusters for further analysis. Compared to the HC group, monocyte clusters significantly increased by approximately three times in the Sepsis group and two times in the Mild group, but decreased somewhat after recovery compared to the Sepsis group, although this reduction was not statistically significant (Figure 2C). Monocytes in the Surgery group were also obviously increased compared to the HC group. However, no significant differences were observed in monocytes between the Surgery and Sepsis groups. Therefore, monocyte subpopulations must be further classified to search for more specific sepsis biomarkers.
Subpopulation Analysis of Monocytes in Sepsis
Cluster analysis of monocytes across different groups revealed 19 subpopulations (C1-C19) based on 42 leukocyte markers (Figure 3A). The monocyte subpopulations were categorized as classical (CD14++CD16-), intermediate (CD14++CD16+), and non-classical (CD14+CD16++) based on CD14 and CD16 expression.15 Several classical monocyte subpopulations exhibited significant differences across different groups, suggesting a link between sepsis and innate immunity (Figure 3B–D). Notably, the C01, C03, C05, C09, C11, and C12 subpopulations were significantly lower in the Sepsis group than in the HC group (P < 0.01 or P < 0.0001, respectively). The significant difference in C11 expression between the HC and Sepsis groups drew our attention. The percentage of C11 decreased 2-fold in the Mild group (P < 0.01) and nearly 8-fold in the Sepsis group (P < 0.0001) compared to that in the HC group. C11 levels were significantly increased in the Recovery group compared with those in the Sepsis group, showing a correlation with disease severity and improvement. Additionally, the C11 percentage varied significantly between the Surgery and Sepsis groups, suggesting the potential to differentiate between non-infectious inflammatory conditions and sepsis.
 |
Figure 3 CyTOF analysis of monocytes. (A) The visualization of different monocyte subsets based on distinct marker expressions across various groups through the utilization of a t-SNE plot. (B) The visualization of CD14 expressions of the monocytes through the utilization of a t-SNE plot. (C) The visualization of CD16 expressions of the monocytes through the utilization of a t-SNE plot. (D) Box plots were employed to present the labeling of monocytes in different subpopulations. Statistical significance was denoted by *, P < 0.05; **, P < 0.01; ***, P < 0.001; ****, P < 0.0001. |
Specific Expression of CD11c+ Monocytes Subpopulation in Sepsis
Given the significant alterations in the monocytic C11 percentage between the Sepsis group and the other groups, we further explored the markers predominantly expressed in the C11 subpopulation. We observed that CD11c, CD11b, and CD33 were highly expressed in the C11 subpopulation (Figure 4A). The t-SNE plot revealed that mCD11c distribution coincided with that of the C11 subpopulation (Figures 3A and 4B). Analysis of mCD11c expression showed significant differences between the Sepsis group and other groups (Figure 4C). Compared to the HC group, mCD11c expression decreased markedly in the Mild group and further declined in the Sepsis group. mCD11c expression in the Surgery group was significantly higher than that in the Sepsis group, suggesting its potential to distinguish sepsis from non-infectious conditions. We also confirmed that CD11c was primarily expressed in monocytes of the Sepsis group (Figure 4D).
 |
Figure 4 Discovery of monocytic CD11c as a potential biomarker in sepsis. (A) Heatmaps were constructed to visually represent the normalized expression levels of markers present in monocyte subsets. (B) The t-SNE plots were employed to present the CD11c labeling of monocytes in different groups. (C) Boxplot was employed to present the expression of CD11c of monocytes in different groups. (D) The expression of CD11c in major immune cell subsets. (E) UMAP projection of the major peripheral immune composition of peripheral blood cells in Sepsis group analyzed from a single-cell sequencing result. UMAP, Uniform Manifold Approximation and Projection. (F) UMAP projection of CD11c expression in Sepsis group analyzed from a single-cell sequencing result. (G) CD11c expression level in major peripheral immune composition of Sepsis group showing by a Violin diagram. (H) CD11c expression features in major peripheral immune composition of Sepsis group analyzing by a Bubble chart. (I) The expression of CD11c in HC, Sepsis and Recovery group from a single-cell sequencing analysis. Statistical significance was denoted by **, P < 0.01; ****, P < 0.0001. |
Further investigation of the peripheral immune composition in patients with sepsis via single-cell sequencing (Figure 4E) confirmed that CD11c was predominantly expressed in monocytes in the Sepsis group (Figure 4F–H). The transcription level of CD11c was significantly reduced in the Sepsis group, but was elevated in the Recovery group (Figure 4I), consistent with the findings of the CyTOF analysis.
CD11c+ Monocytes as a Novel Biomarker in Distinguishing Sepsis From Non-Infectious Diseases
Flow cytometry was used to detect the difference in the percentage of CD11c-expressing monocytes (mCD11c%) across different groups in the validation study (Figure 5A). The box plot showed a significant decrease in mCD11c% in the Sepsis group compared with that in the Mild or Surgery groups (Figure 5B). Further subgroup analysis of the Sepsis group revealed that the mCD11c% was independent of age, gender, and infection site. However, a significant difference was observed based on the type of infecting bacteria; patients with gram-negative bacterial infections exhibited markedly higher mCD11c% than those with gram-positive infections (Figure 5C). Impressively, mCD11c% exhibited an AUC of 0.939 (P < 0.001) under the ROC curve between the Sepsis and Surgery groups, significantly surpassing WBC, PCT, and CRP (Figure 5D), supporting the mCD11c’s predictive value in distinguishing sepsis from noninfectious inflammation compared to other indicators. Furthermore, mCD11c displayed the highest AUC (0.774) between the Surgery and Mild groups (P < 0.001) (Figure 5E). In the comparison between the Sepsis and Mild groups, mCD11c’s AUC was 0.751 (P < 0.001), ranking second only to PCT (Figure 5F).
 |
Figure 5 Validation of monocytic CD11c as a biomarker in sepsis. (A) The flow chart of the experimental design of the flow cytometry analysis. (B) Boxplot was employed to present mCD11c% in different groups. (C) Boxplot was employed to present mCD11c% in patients with sepsis divided by age, gender, infection site and pathogenic bacteria. (D–F) ROC curves for WBC, CRP, PCT and mCD11c% were utilized to distinguish Sepsis from Surgery group, Surgery from Mild group and Sepsis from Mild group. Statistical significance was denoted by **, P < 0.01; ****, P < 0.0001. |
Association Between CD11c+ Monocytes and 7-Day Mortality in Sepsis
The all-cause mortality rates in patients with sepsis were 14.4% (13/90) on day 7, 20.0% (18/90) on day 14, and 25.6% (23/90) on day 28. Cox univariate regression analysis suggested that common baseline variables (gender, age, infection site, and pathogenic bacteria) did not significantly affect survival duration, while mCD11c% (HR = 0.817, 95% CI 0.737–0.907, P < 0.001), SOFA score (HR = 1.461, 95% CI 1.261–1.693, P < 0.001), and APACHE II score (HR = 1.190, 95% CI 1.096–1.292, P < 0.001) provided significant prognostic value for 7-day all-cause mortality. No other laboratory indicators were significantly correlated (Table 1). Cox multivariate regression analysis revealed that mCD11c% (HR = 0.879, 95% CI 0.778–0.993, P = 0.038) and SOFA score (HR = 1.327, 95% CI 1.084–1.625, P = 0.006) significantly affected 7-day mortality in sepsis (Table 2). Only the SOFA score remained significant association with survival duration at 14day (Tables S3 and S4). Kaplan-Meier analysis of 7-day survival rates in patients of Sepsis, stratified by the mCD11c% cut-off value (96.445%), demonstrated a significantly lower survival probability in the subpopulation with lower mCD11c% (Figure 6).
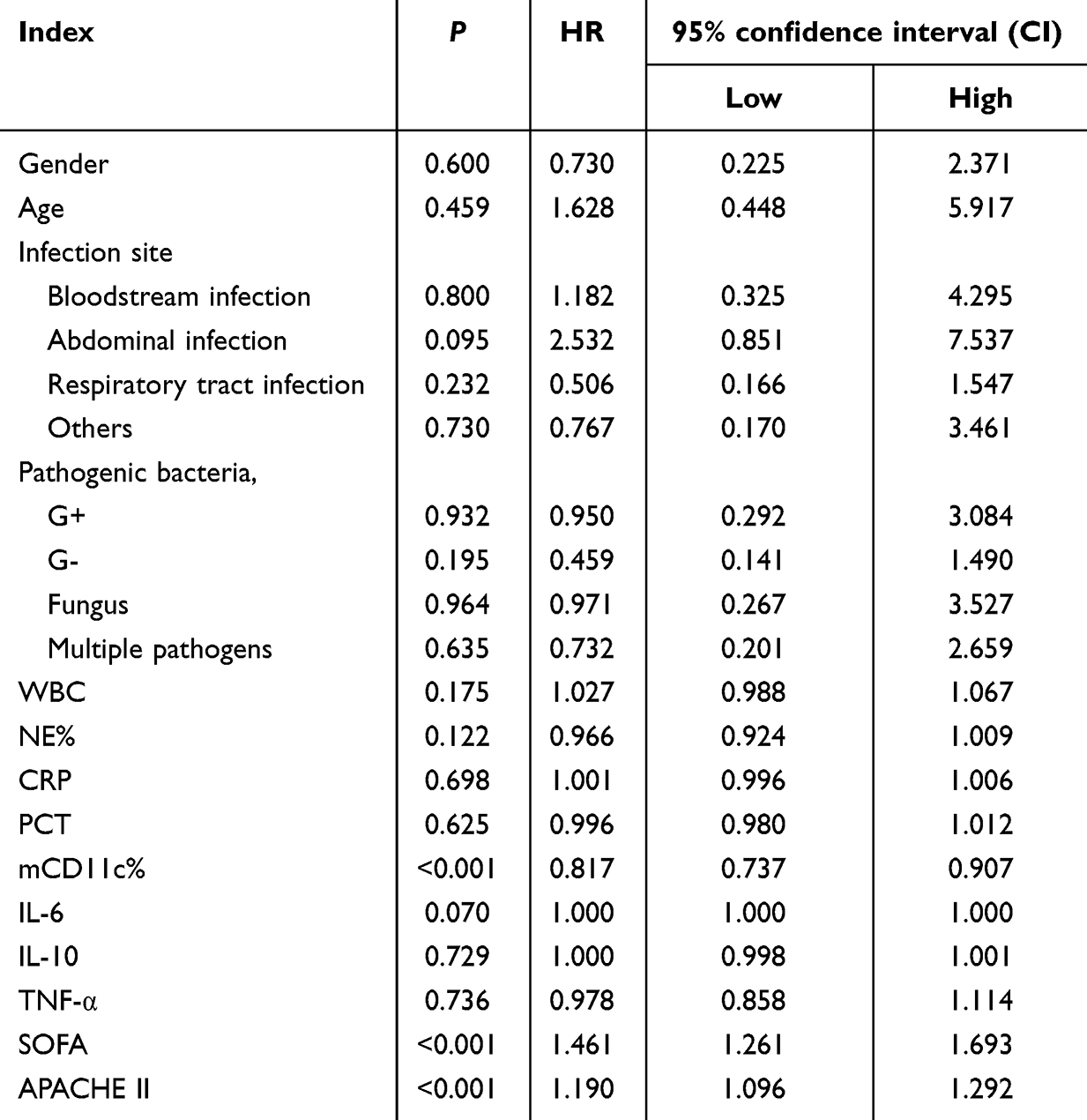 |
Table 1 Univariate Cox Regression Analysis of 7-Day Mortality Rate in Patients with Sepsis |
 |
Table 2 Multivariate Cox Regression Analysis of 7-Day Mortality Rate in Patients with Sepsis |
 |
Figure 6 The 7-day Kaplan-Meier Curve for the patients with sepsis by mCD11c%. P values were calculated using Log Rank test. P < 0.05 means statistically significant. |
Discussion
Sepsis is characterized by a multifaceted pathogenesis and rapid progression, which present considerable challenges for clinicians in making treatment decisions. Early recognition and appropriate intervention using biomarkers in the initial stages of disease onset can improve the prognosis of sepsis.16 In this study, CyTOF and flow cytometry techniques were employed to identify and validate a novel sepsis biomarker, mCD11c. Compared to conventional markers such as WBC, CRP, and PCT, mCD11c has demonstrated promise in the early diagnosis of sepsis and in predicting short-term survival outcomes in patients with sepsis.
Monocytes are a specialized subset of leukocytes that are vital for the regulation of immune defense reactions and tissue homeostasis. The increase of monocytes in patients with sepsis indicates their activation and role in early malignant inflammatory responses.17 A recent study indicated that patients with sepsis exhibited an increased presence of monocytes, B cells, and dendritic cells, along with a reduction in NK cells and CD4/CD8 T cells.18 Another research reported a unique CD14+ monocyte subpopulation that was expanded in patients with sepsis.19 Some monocyte surface proteins, such as CD40 and HLA-DR, have been shown to be associated with the occurrence and development of sepsis.20,21 Consistent with previous reports, our research showed a significant increase in monocytes of patients with sepsis, suggesting their significant role in the pathophysiology of sepsis and highlighting the need for further investigation.
CD11c is widely acknowledged as a definitive marker for dendritic cells (DCs) and responsible for recruiting monocytes, macrophages, and DCs in numerous physiological and pathological processes.8 However, there is a lack of conclusive evidence characterizing the differential expression and diagnostic implication of mCD11c in sepsis. Studies have shown that neutrophils expressing CD11c exhibit high sensitivity and specificity in detecting sepsis, indicating a potential association between CD11c expression and sepsis progression.7 Another study found no significant differences in CD11c expression levels on monocyte surfaces, as measured by ELISA, between patients with sepsis and healthy controls. However, this study was constrained by the small sample size and the employment of a single detection methodology.22 In our study, we set up a discovery cohort and a validation cohort with a larger sample size, combined with CyTOF, single-cell sequencing, and flow cytometry, and confirmed that the Sepsis group had a significant reduction in mCD11c% compared with both the Mild and Surgery groups. The mCD11c% was not affected by age, gender or infection site, whereas it was elevated in cases of sepsis caused by gram-negative bacterial infections, which deserves further exploration. The results of the validation study were consistent with those of the discovery study. Our study demonstrated that the mCD11c subpopulation in the Sepsis group differed from that in the control group, and exhibited potential as a novel sepsis biomarker. Regarding the biological mechanism of mCD11c downregulation in sepsis, we speculate that it may be related to the dysregulation of immune cell signaling pathways. Studies have shown that sepsis-induced excessive inflammatory responses can activate the NF-κB and HIF-1α signaling pathways,17,23 which may inhibit the transcription of the CD11c gene. However, the specific mechanism still needs to be verified by further in vitro cell experiments and in vivo animal models.
To evaluate the diagnostic and prognostic value of mCD11c in sepsis, we used ROC curves and regression analysis to assess its sensitivity and specificity compared with the classic indicators including WBC, CRP, PCT, IL-6 and TNF-α.24 Research indicated that cytokines stimulate the production and release of WBC in sepsis.25–27 CRP responded to inflammation stimuli and showed better diagnostic accuracy in neonatal sepsis.27 PCT is the most extensively studied biomarker for sepsis, facilitating the effective management of antibiotic therapy in patients with sepsis.28,29 It was reported IL-6 possessed highly accurate diagnostic modality for the identification of sepsis.30 TNF-α upregulated in sepsis and showed correlation with SOFA, APACHE II and organ toxicity in sepsis.31 However, these existing markers alone are not sufficiently characteristic to identify sepsis biomarkers because of the heterogeneity and complexity of sepsis pathology. In the present study, mCD11c was identified and validated as a novel sepsis biomarker. In a previous study conducted by our group, low CD39 expression on monocytes was identified as a candidate diagnostic marker for sepsis.32 Extending this work, the present investigation employed single-cell RNA sequencing within the discovery cohort and enrolled a larger validation population. The AUC of mCD11c% under the ROC curve was significantly higher than those of CRP and PCT in distinguishing the Sepsis and Surgery groups. This indicates that mCD11c% has comparable or even better discriminatory ability between sepsis and noninfectious inflammation, which helps to detect sepsis early and quickly initiate antibiotic treatment, significantly improving the survival chances and clinical outcomes of sepsis patients.
Sepsis exhibits intrinsic heterogeneity; therefore, utilizing appropriate biomarkers to stratify the risk of patients with sepsis can be highly valuable for clinical treatment.33 Low-risk patients may be allowed to use antibiotics more wisely and can be assigned to the standard care group, whereas patients with poor prognosis not only require early and aggressive antibiotic treatment, but also require faster action from multidisciplinary medical teams.34 Our study found that mCD11c% was an independent influencing factor for 7-day mortality in patients with sepsis and has good predictive value for 7-day mortality. This helps achieve precision medicine for patients with sepsis. However, mCD11c exhibited limited performance in predicting mortality at 14- and 28-day (Figure S2), which may be attributed to the combined effects of dynamic changes in biological indicators, disease complexity and progression, and treatment interventions.
Overall, we managed to discover and verify a new sepsis biomarker, mCD11c, using a combination of CyTOF and flow cytometry. To our knowledge, this is the first report on the role of mCD11c in distinguishing sepsis from non-infectious inflammation. In addition, compared to patients with a lower percentage of mCD11c, patients with a higher proportion of mCD11c exhibited a higher probability of short-term survival. However, this study has several limitations. First, the study was conducted at a single center, and the small sample size may have limited the generalizability of the results and affected their statistical accuracy. Second, we did not detect the expression levels of CD11c at different stages of sepsis, and it is unclear whether CD11c can be used as an intervention target for sepsis. Therefore, larger sample sizes and further in vivo and in vitro studies are needed to explore the changes in mCD11c during the development of sepsis as well as its biological functions and mechanisms of action in sepsis.
Conclusion
In summary, we identified and validated a novel sepsis biomarker, mCD11c, using a combination of CyTOF and flow cytometry. Our research found that mCD11c was significantly higher in the Surgery and Mild groups than in the Sepsis group. This confirms the ability of mCD11c to distinguish sepsis from other inflammatory states and predict short-term mortality. This finding provides a new direction for the early diagnosis and treatment of sepsis.
Abbreviations
APACHE II, Acute Physiology and Chronic Health Evaluation II; AUC, area under the curve; CI, confidence interval; CRP, C-reactive protein; CyTOF, Cytometry by Time-of-Flight; HR, hazard ratio; IL-6, interleukin-6; IL-10, interleukin-10; mCD11c, monocyte-expressed CD11c; mCD11c%, percentage of CD11c-expressing monocytes; NE%, Neutrophil Percentage; PBMCs, peripheral blood mononuclear cells; PCT, procalcitonin; ROC, receiver operating characteristic; SOFA, sepsis-related organ failure assessment; TNF-α, tumor necrosis factor α; WBC, white blood cell.
Ethics Approval and Informed Consent
This study was approved by the Research Ethics Committee of the First Affiliated Hospital Zhejiang University School of Medicine (IIT20220071B, IIT 20220076b). Informed consent was obtained from all participating patients or, in cases of impaired decision-making capacity (eg, due to sedation, critical illness, or cognitive impairment), from their legal representatives, in accordance with the principles outlined in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science and Foundation of China (grant numbers 82241037, 82170725 and 82272338), Natural Science Foundation of Jiangxi Province (grant number 20242BAB26114), “Pioneer” and “Leading Goose” R&D Program of Zhejiang Province (grant number 2023C03096), Project of Zhejiang Pharmaceutical Association (grant number 2023ZYY01) and Clinical Scientific Project of Zhejiang Medical Association (grant number 2020ZYC-A109).
Disclosure
The authors declare no personal, financial, commercial, or academic conflicts of interest in this work.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–13. doi:10.1016/S0140-6736(19)32989-7
2. van der Poll T, Shankar-Hari M, Wiersinga WJ. The immunology of sepsis. Immunity. 2021;54(11):2450–2464. doi:10.1016/j.immuni.2021.10.012
3. Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi:10.1097/CCM.0000000000000330
4. Lane DJ, Wunsch H, Saskin R, et al. Association between early intravenous fluids provided by paramedics and subsequent in-hospital mortality among patients with sepsis. JAMA Network Open. 2018;1(8):e185845. doi:10.1001/jamanetworkopen.2018.5845
5. Arora S, Singh P, Singh PM, Trikha A. Procalcitonin levels in survivors and nonsurvivors of sepsis: systematic review and meta-analysis. Shock. 2015;43(3):212–221. doi:10.1097/SHK.0000000000000305
6. Karakike E, Kyriazopoulou E, Tsangaris I, Routsi C, Vincent JL, Giamarellos-Bourboulis EJ. The early change of SOFA score as a prognostic marker of 28-day sepsis mortality: analysis through a derivation and a validation cohort. Critical Care. 2019;23(1):387. doi:10.1186/s13054-019-2665-5
7. Lewis SM, Treacher DF, Edgeworth J, et al. Expression of CD11c and EMR2 on neutrophils: potential diagnostic biomarkers for sepsis and systemic inflammation. Clin Exp Immunol. 2015;182(2):184–194. doi:10.1111/cei.12679
8. Wang Q, Su X, He Y, et al. CD11c participates in triggering acute graft-versus-host disease during bone marrow transplantation. Immunology. 2021;164(1):148–160. doi:10.1111/imm.13350
9. van der Poll T, van de Veerdonk FL, Scicluna BP, Netea MG, van de Veerdonk FL. The immunopathology of sepsis and potential therapeutic targets. Nat Rev Immunol. 2017;17(7):407–420. doi:10.1038/nri.2017.36
10. Rahim MK, Okholm TLH, Jones KB, et al. Dynamic CD8(+) T cell responses to cancer immunotherapy in human regional lymph nodes are disrupted in metastatic lymph nodes. Cell. 2023;186(6):1127–1143.e1118. doi:10.1016/j.cell.2023.02.021
11. Lozano AX, Chaudhuri AA, Nene A, et al. T cell characteristics associated with toxicity to immune checkpoint blockade in patients with melanoma. Nature Med. 2022;28(2):353–362. doi:10.1038/s41591-021-01623-z
12. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
13. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
14. National medical insurance information business coding standard database. Available from: https://code.nhsa.gov.cn/search.html?sysflag=80.
15. Williams H, Mack C, Baraz R, et al. Monocyte differentiation and heterogeneity: inter-subset and interindividual differences. Int J Mol Sci. 2023;24(10):8757. doi:10.3390/ijms24108757
16. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–e1143.
17. Shalova IN, Lim JY, Chittezhath M, et al. Human monocytes undergo functional re-programming during sepsis mediated by hypoxia-inducible factor-1α. Immunity. 2015;42(3):484–498.
18. Park S, Perumalsamy H, Gerelkhuu Z, Sunderraj S, Lee Y, Yoon TH. Phenotypic landscape of immune cells in sepsis: insights from high-dimensional mass cytometry. ACS Infect Dis. 2024;10(7):2390–2402.
19. Reyes M, Filbin MR, Bhattacharyya RP, et al. An immune-cell signature of bacterial sepsis. Nature Med. 2020;26(3):333–340. doi:10.1038/s41591-020-0752-4
20. Jämsä J, Syrjälä H, Huotari V, Savolainen ER, Ala-Kokko T. Monocyte and lymphocyte surface molecules in severe sepsis and non-septic critically ill Patients. APMIS: acta pathologica, microbiologica, et immunologica Scandinavica. APMIS. 2017;125(6):536–543. doi:10.1111/apm.12670
21. Yao RQ, Zhao PY, Li ZX, et al. Single-cell transcriptome profiling of sepsis identifies HLA-DR(low)S100A(high) monocytes with immunosuppressive function. Military Med Res. 2023;10(1):27. doi:10.1186/s40779-023-00462-y
22. Brunialti MK, Martins PS, Barbosa de Carvalho H, Machado FR, Barbosa LM, Salomao R. TLR2, TLR4, CD14, CD11B, and CD11C expressions on monocytes surface and cytokine production in patients with sepsis, severe sepsis, and septic shock. Shock. 2006;25(4):351–357. doi:10.1097/01.shk.0000217815.57727.29
23. Tang L, Zhang W, Liao Y, et al. Decoding sepsis: unraveling key signaling pathways for targeted therapies. Research. 2025;8:0811. doi:10.34133/research.0811
24. Saxena J, Das S, Kumar A, et al. Biomarkers in sepsis. Int J Clin Chem. 2024;562:119891. doi:10.1016/j.cca.2024.119891
25. Ayazi P, Mahyar A, Daneshi MM, Jahani Hashemi H, Pirouzi M, Esmailzadehha N. Diagnostic accuracy of the quantitative C-reactive protein, erythrocyte sedimentation rate and white blood cell count in urinary tract infections among infants and children. Malaysian J Med Sci. 2013;20(5):40–46.
26. Farkas JD. The complete blood count to diagnose septic shock. J Thoracic Dis. 2020;12(Suppl 1):S16–s21. doi:10.21037/jtd.2019.12.63
27. Sorsa A. Diagnostic significance of white blood cell count and c-reactive protein in neonatal sepsis; asella referral hospital, south east ethiopia. Open Microbiol J. 2018;12:209–217. doi:10.2174/1874285801812010209
28. Prkno A, Wacker C, Brunkhorst FM, Schlattmann P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock--a systematic review and meta-analysis. Critical Care. 2013;17(6):R291. doi:10.1186/cc13157
29. Hung SK, Lan HM, Han ST, Wu CC, Chen KF. Current evidence and limitation of biomarkers for detecting sepsis and systemic infection. Biomedicines. 2020;8(11):494. doi:10.3390/biomedicines8110494
30. Hou T, Huang D, Zeng R, Ye Z, Zhang Y. Accuracy of serum interleukin (IL)-6 in sepsis diagnosis: a systematic review and meta-analysis. Int J Clin Exp Med. 2015;8(9):15238–15245.
31. Kumar S, Gupta E, Kaushik S, Kumar Srivastava V, Mehta SK, Jyoti A. Evaluation of oxidative stress and antioxidant status: correlation with the severity of sepsis. Scand J Immunol. 2018;87(4):e12653. doi:10.1111/sji.12653
32. Li H, Ding P, Nan Y, et al. Low expression of CD39 on monocytes predicts poor survival in sepsis patients. Journal of Intensive Care. 2025;13(1):12. doi:10.1186/s40560-025-00784-0
33. Stanski NL, Wong HR. Prognostic and predictive enrichment in sepsis. Nat Rev Nephrol. 2020;16(1):20–31. doi:10.1038/s41581-019-0199-3
34. Taneja I, Damhorst GL, Lopez-Espina C, et al. Diagnostic and prognostic capabilities of a biomarker and EMR-based machine learning algorithm for sepsis. Clin Transl Sci. 2021;14(4):1578–1589. doi:10.1111/cts.13030
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identifying Potential Effective Diagnostic and Prognostic Biomarkers in Sepsis by Bioinformatics Analysis and Validation
Huang X, Tan J, Chen X, Zhao L
International Journal of General Medicine 2022, 15:6055-6071
Published Date: 6 July 2022
Impaired Circulating Antibody-Secreting Cells Generation Predicts the Dismal Outcome in the Elderly Septic Shock Patients
Xu H, Li T, Zhang X, Li H, Lv D, Wang Y, Huo F, Bai J, Wang C
Journal of Inflammation Research 2022, 15:5293-5308
Published Date: 13 September 2022
SPINK1 is a Potential Diagnostic and Prognostic Biomarker for Sepsis
Chen D, Shi Z, Gao X, Yang Y, Lei X, Hu Y
Infection and Drug Resistance 2024, 17:875-884
Published Date: 8 March 2024
Integrated Analysis Identified TGFBI as a Biomarker of Disease Severity and Prognosis Correlated with Immune Infiltrates in Patients with Sepsis
Shi M, Wei Y, Guo R, Luo F
Journal of Inflammation Research 2024, 17:2285-2298
Published Date: 15 April 2024
Apolipoprotein E: A Potential Prognostic and Diagnostic Biomarker for Hepatocellular Carcinoma
Li Y, Lu R, Abuduhailili X, Feng Y
Journal of Hepatocellular Carcinoma 2025, 12:301-324
Published Date: 17 February 2025