Back to Journals » Infection and Drug Resistance » Volume 17
SPINK1 is a Potential Diagnostic and Prognostic Biomarker for Sepsis
Authors Chen D, Shi Z, Gao X, Yang Y, Lei X ![]() , Hu Y
, Hu Y ![]()
Received 8 October 2023
Accepted for publication 19 February 2024
Published 8 March 2024 Volume 2024:17 Pages 875—884
DOI https://doi.org/10.2147/IDR.S440117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Dexiu Chen,1 Zhangjing Shi,1 Xiaolan Gao,1 Yuxiang Yang,1 Xianying Lei,1,* Yingchun Hu2,*
1Department of Critical Care Medicine, The Affiliated Hospital, Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China; 2Department of Emergency Medicine, The Affiliated Hospital, Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingchun Hu, Department of Emergency Medicine, The Affiliated Hospital, Southwest Medical University, 25 Taiping Street, Jiangyang District, Luzhou, Sichuan, 646000, People’s Republic of China, Tel +86-830-3165851, Email [email protected] Xianying Lei, Department of Critical Care Medicine, The Affiliated Hospital, Southwest Medical University, 25 Taiping Street, Jiangyang District, Luzhou, Sichuan, 646000, People’s Republic of China, Tel +86-830-3165527, Email [email protected]
Purpose: There are no satisfactory diagnostic biomarkers for sepsis. Accordingly, this study screened biomarkers valuable for sepsis diagnosis and prognosis using data-independent acquisition (DIA) combined with clinical data analysis.
Patients and Methods: Serine protease inhibitor Kazal-type 1 (SPINK1) is a differentially expressed protein that was screened using DIA and bioinformatics in sepsis patients (n = 22) and healthy controls (n = 10). The plasma SPINK1 levels were detected using an enzyme-linked immunosorbent assay (ELISA) in an expanded population (sepsis patients, n = 52; healthy controls, n = 10). The diagnostic value of SPINK1 in sepsis was evaluated using receiver operating characteristic (ROC) curve analysis based on clinical data. The prognostic value of SPINK1 for sepsis was evaluated using correlation and survival analyses.
Results: DIA quality control identified 78 differential proteins (72 upregulated and six downregulated), among which SPINK1 was highly expressed in sepsis. The ELISA results suggested that SPINK1 expression was significantly elevated in the sepsis group (P < 0.05). ROC analysis of SPINK1 yielded an area under the curve (AUC) of 0.9096. Combining SPINK1 with procalcitonin (PCT) for ROC analysis yielded an AUC of 1. SPINK1 expression was positively correlated with the Sequential Organ Failure Assessment (SOFA) score (r = 3497, P = 0.0053) and APACHE II score (r = 3223, P = 0.0106). High plasma SPINK1 protein expression was negatively correlated with the 28-day survival rate of patients with sepsis (P = 0.0149).
Conclusion: The plasma of sepsis patients contained increased SPINK1 protein expression. Combining SPINK1 with PCT might have a high diagnostic value for sepsis. SPINK1 was associated with the SOFA score, APACHE II score, and the 28-day survival rate in patients with sepsis.
Keywords: serine protease inhibitor Kazal-type 1, sepsis, DIA, PCT, biomarker
Introduction
Sepsis is a severe condition characterized by dysfunctional organ systems resulting from an imbalanced immune response to infection. Sepsis presents a significant medical and healthcare challenge globally, leading to a mortality rate of approximately one-third to one-sixth of affected individuals. Timely recognition and intervention in sepsis cases substantially decrease patient mortality.1 However, the current screening methods utilized for early detection, including the Systemic Inflammatory Response Syndrome (SIRS) criteria, quick Sequential Organ Failure Score (qSOFA), and SOFA criteria, are subject to limitations. A high-sensitivity and high-specificity screening tool is currently lacking.2–4 Pursuing effective sepsis biomarkers is necessary to determine the presence of bacterial infection and the severity of the patient’s condition. Such biomarkers would enable the prompt initiation of appropriate treatment during the early disease stages.5 Scientists are conducting extensive research on sepsis biomarkers involving a wide range of humoral innate immune responses, cytokines, and chemokines, such as C-reactive protein (CRP), serum amyloid P component (SAP), and pentraxin 3 (PTX-3).6 Additionally, many non-coding RNAs, such as microRNA (miR)-1, miR-124, and miR-34a, are useful as sepsis biomarkers.7 However, these markers need to be further confirmed by more clinical studies, and the most clinical studies are currently on procalcitonin (PCT).
PCT is a precursor to the hormone calcitonin, which is not detectable in healthy conditions. It begins to rise within 3–4 hours after infection, peaking around 24 hours, and has a half-life of 22–35 hours. Consequently, PCT is widely regarded as a reliable indicator of the body’s response to infection. However, clinical studies have demonstrated limited PCT sensitivity and specificity in sepsis, and PCT levels may rise in non-sepsis-related conditions, such as methamphetamine poisoning, kidney failure, liver failure, severe trauma, burns, surgery, and pancreatitis. Therefore, sepsis guidelines do not recommend PCT to guide antibiotic initiation1,8,9 or its use alone in diagnosing sepsis. Thus, there is an urgent need to identify other biomarkers to improve the disease diagnosis.10
Biomedicine widely uses data-independent acquisition (DIA) technology as a large-scale proteome identification and quantitative strategy.11 In the previous stage, our research group screened the core genes LGALS3BP,12 GSTO1, C1QA, RETN, GRN13 in sepsis patients using DIA. In the present study, we identified a potential biomarker of sepsis, Serine protease inhibitor Kazal-type 1 (SPINK1), using DIA technology. SPINK1 is a secreted protein in the pancreas that inhibits trypsin. SPINK1 is also known as PCTT, PSTI, Spink3, TATI, and TCP. SPINK1 is released into the pancreatic duct by acinar cells in the exocrine pancreas and interacts with trypsin, inhibiting its intracellular and extracellular activity.14 Research on SPINK1 focuses on tumors as SPINK1 is abnormally expressed in various tumors with direct and indirect biological roles in regulating tumor proliferation, metastasis, drug resistance, transdifferentiation, and tumor stemness,15 However, SPINK1 expression in sepsis and its mechanism of action have not been studied. SPINK1 protein might be highly expressed in sepsis plasma. Thus, we validated this result by performing an enzyme-linked immunosorbent assay (ELISA) on plasma from more sepsis patients. We also evaluated SPINK1 sensitivity, specificity, and prognostic predictive value in anticipation of finding potential biomarkers for sepsis diagnosis and prognosis.
Materials and Methods
Sample Collection
In this study, peripheral blood samples were collected from sepsis patients (n = 52) and healthy volunteers (n = 10) who were hospitalized in the EICU of the Department of Emergency Medicine of the Affiliated Hospital of Southwest Medical University from January 2019 to December 2022. The inclusion criteria were as follows: 1) all patients with sepsis admitted to the emergency department EICU, 2) diagnostic criteria were based on Sepsis 3.0 guidelines (infection + SOFA score ≥ 2), 3) patient age ≥ 14 and ≤70 years, and 4) patient or their legal representative was willing to participate in the study and sign an informed consent for the study. The exclusion criteria included the following: 1) prior organ failure, 2) prior immune system disease, 3) prior hematologic disorders, and 4) unwillingness to be enrolled. We also obtained the patients’ demographic characteristics, inflammatory indicators, comorbidities, etiological data, SOFA score, APACHE II score, and 28-day outcome (Table 1). The Ethics Committee of the Affiliated Hospital of Southwest Medical University Ethics Committee approved this study (Ethics Nos. ky2018029 and ky2022094). The patient or family members signed each specimen to indicate consent. The clinical trial registration numbers were ChiCTR1900021261 and ChiCTR2200057401. This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.
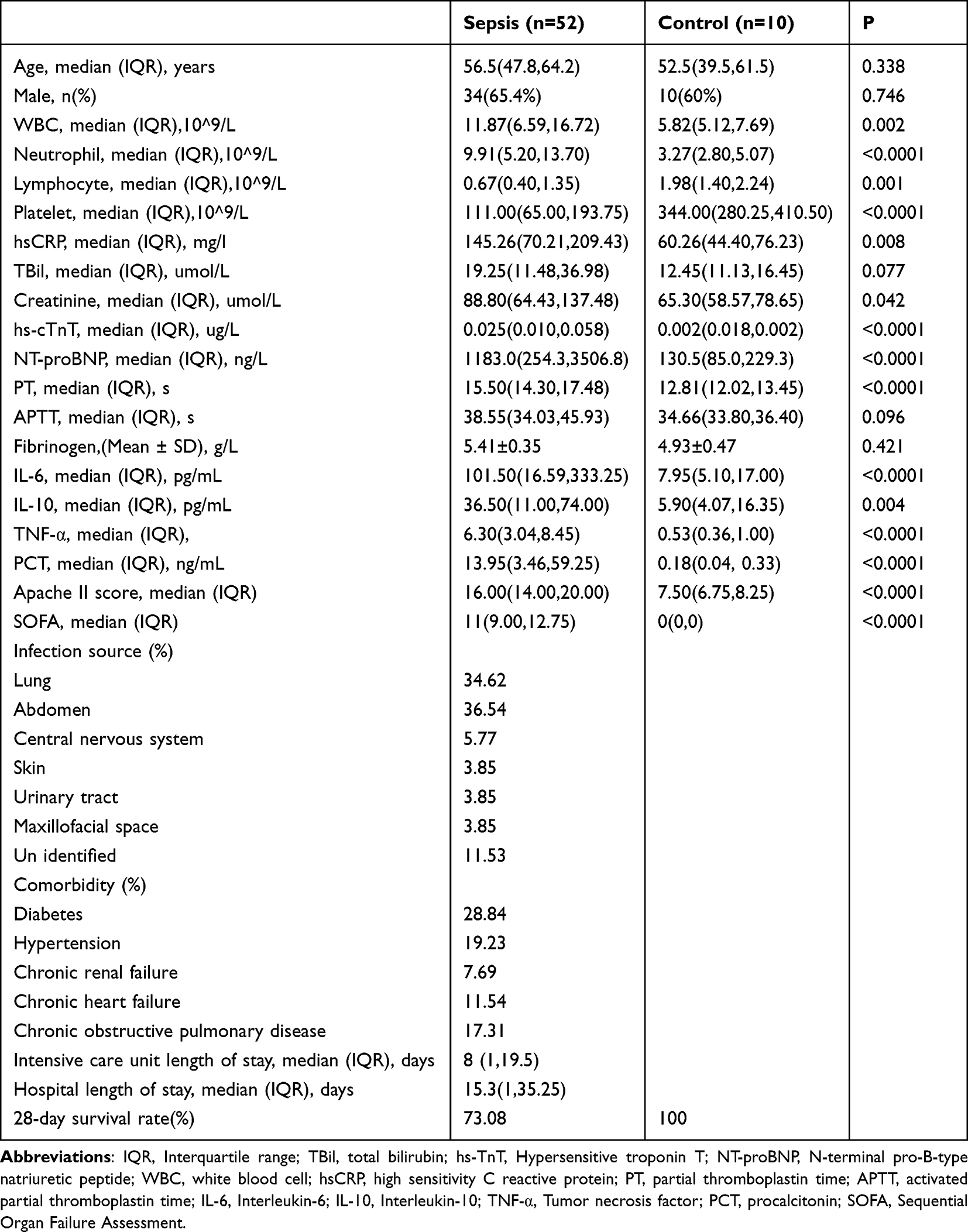 |
Table 1 Baseline Characteristics of Control and Patients with Sepsis |
DIA Mass Spectrometry and Quality Control
We randomly selected 22 and 10 peripheral blood samples from the sepsis patients and controls, respectively. The 32 samples were collected by a Q-EX Active HF (Thermo Fisher Scientific, San Jose, CA) instrument in DIA mode. A total of 7699 peptides and 979 proteins were quantified using MSstats software. The data quality was evaluated using the intra-group variation coefficient and principal component analysis. Then, based on the spectrum library constructed by the traditional data-dependent acquisition (DDA) mode, the ratio and P-value of the protein expression changes in the 32 samples were identified and quantified using the mProphet algorithm.
DEG Screening and Functional Enrichment
Differential proteins between the control and sepsis groups were screened using P < 0.05 and |log2 fold change (FC) |≥ 2. The differential proteins were imported into the STRING database (https://cn.string-db.org/) and enriched for the main biological functions and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathways using false discovery rate (FDR) < 0.05 as the inclusion threshold.
ELISA
Plasma samples were collected from the sepsis group (n = 52) and control group (n = 10) for ELISA. The protein content in the samples was determined using the double antibody sandwich method. The sample was coated with a purified specific antibody to yield a solid-phase antibody. Then, the sample was sequentially added to the coated wells and combined with horseradish peroxidase (HRP)-labeled detection antibody to form an antibody–antigen–enzyme-labeled antibody complex, washed, and washed with the substrate TMB to develop the color. The depth of color positively correlated with the protein content of the sample. The absorbance (optical density [OD]) was measured at 450 nm using an enzyme marker, and the protein content in the sample was calculated from a standard curve. The data were analyzed using GraphPad Prism 9 (GraphPad Inc., La Jolla, CA). Differences between groups were analyzed using an independent samples t-test. P < 0.05 was considered statistically significant.
Survival Curve
The participants were divided into high- and low-expression groups based on the plasma concentration of SPINK1 protein. The mapping analysis was conducted using GraphPad Prism 9, and the Log rank test was used for statistics. P < 0.05 was defined as statistically significant.
Statistical Method
Numerical variables were described using the median (interquartile range) or the mean ± standard deviation. The Mann–Whitney U nonparametric test was used for non-normally distributed data, and the unpaired t-test was used for normally distributed data. Categorical variables were compared using the chi-square test. Survival curves were tested using the Log rank test. Diagnostic indicator efficiency (sensitivity and specificity) was evaluated using receiver operating characteristic (ROC) analysis and logistic regression. The strength of the relationship between two quantitative variables was evaluated using Spearman correlation test. P < 0.05 was considered significant. IBM SPSS Statistics 22 and GraphPad Prism 9 were used to analyze the data and construct graphs.
Results
SPINK1 Protein Was Highly Expressed in the Plasma of Sepsis Patients
From January 2019 to December 2022, this study screened 52 sepsis patients and 10 healthy controls. Twenty-two sepsis patients and 10 controls were randomly selected for DIA mass spectrometry analysis, and Figure 1 depicts the process. The data underwent principal component analysis, and the results were visualized using ggplot2. The control and sepsis groups had good inter-group differentiation (Figure 2A). After quality control, the data underwent bioinformatics analysis, and 78 differential proteins were screened out, of which 72 were upregulated, and six were downregulated (Figure 2B). Supplement 1 lists all differentially expressed proteins. The differential proteins were analyzed using Gene Ontology (GO) and KEGG. GO enriched 16 cellular components (CC), 11 biological processes (BP), one molecular function (MF), and one KEGG pathway (Figure 2C). The differential proteins were mainly in extracellular space, vesicles, and secretory granules, and their molecular functions were mainly combined with signal receptors. The protein’s biological functions were mainly stress, defense, inflammatory, humoral immune responses, and leukocyte–cell adhesion. The main enrichment pathway was N-glycan biosynthesis. The DIA analysis demonstrated that SPINK1 protein was elevated in sepsis patients and was in the extracellular space, extracellular region, exosomes, and vesicles (Supplement 1). The DIA results were verified by measuring the SPINK1 protein concentration of all collected plasma samples using ELISA. The patients’ demographic characteristics, inflammatory markers, organ function indicators, lactic acid, SOFA score, APACHE II score, infection source, comorbidities, and 28-day survival rate were also collected. Table 1 presents the specific clinical features. The sepsis group had significantly increased inflammatory markers, different degrees of organ damage, significantly increased SOFA and APACHE II scores, and a survival rate of ~73.08% (Table 1). The ELISA results revealed that SPINK1 expression was 48.53 ± 6.48 ng/mL in the control group and 107.76 ± 5.93 nmol/L in the sepsis group. The sepsis group had significantly elevated SPINK1 expression compared with the control group (Figure 2D, P < 0.0001).
 |
Figure 1 Experimental flow chart of this study. |
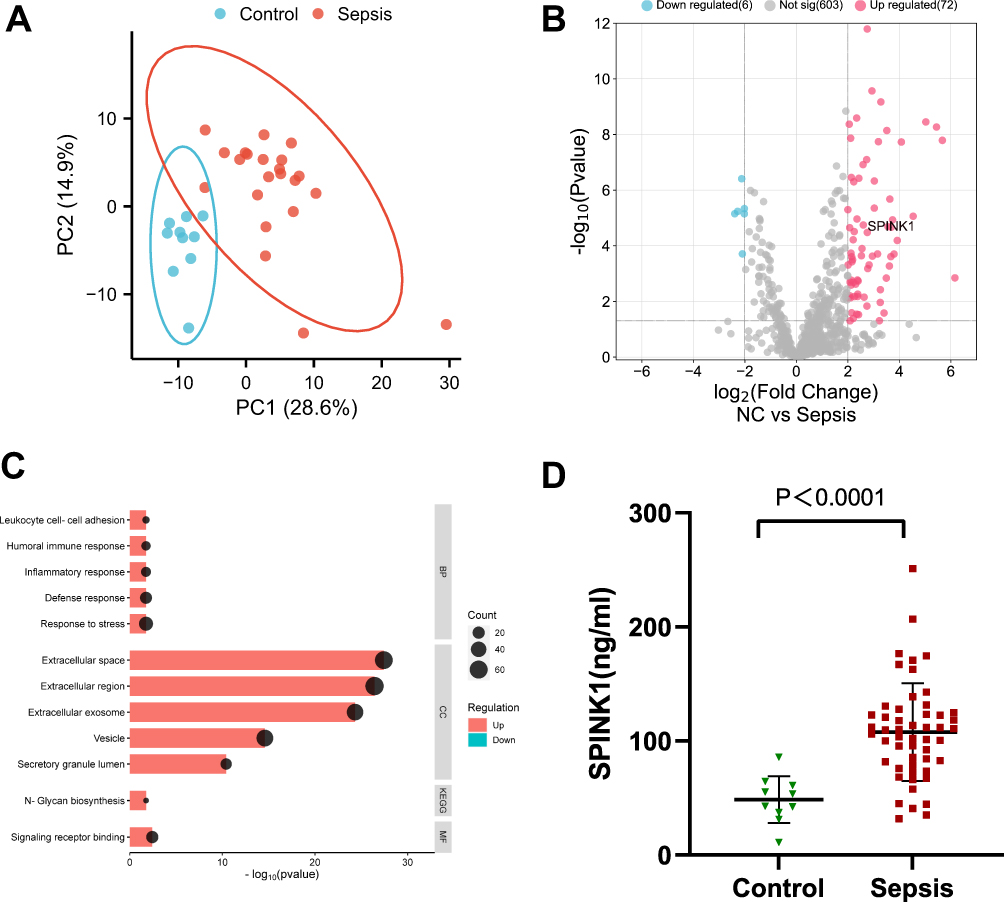 |
Figure 2 SPINK1 is highly expressed in patients with sepsis. (A) PCA shows that the two groups are distinguishable and there were no outliers. (B)Volcano plot showing up-regulated (red) and down-regulated (blue) proteins screened by differential analysis, with the logarithm of the difference multiplicity (log2) as the horizontal coordinate and the negative logarithm of the p-value (log10) as the vertical coordinate (fold-change ≥2.0, P value<0.05). Compared with the normal group, 78 differential proteins were screened, of which 6 were down-regulated and 72 were up-regulated, Among them, SPINK1 is highly expressed in sepsis patients. (C) In the GO enrichment results of different proteins, red represents the up-regulated pathway, blue represents the down-regulated pathway, and the size of the dots represents the number of proteins in different items. (D) ELISA results showed that the expression of SPINK1 in the sepsis group was significantly higher than that in the normal group, the differences were statistically significant (P<0.0001). |
SPINK1 Combined with PCT Has a High Diagnostic Value for Sepsis
The PCT level in the sepsis patients and controls was 13.95 ng/mL (3.46, 59.25) and 0.18 ng/mL (0.04, 0.33), respectively (Figure 3A, P < 0.0001). The ability of biomarkers to classify disease states is evaluated using the ROC curve, and a larger area under the ROC curve (AUC) indicates higher diagnostic accuracy. Statistical analysis of the clinical data of 62 patients determined that the AUC of SPINK1 and PCT was 0.9096 and 0.9529, respectively. Combining SPINK1 and PCT to diagnose sepsis yielded an AUC of 1. Youden’s index (sensitivity+specificity-1) is a summary statistic of the ROC curve that defines the potential effectiveness of biomarkers. The maximum Youden’s index determines the best diagnostic cut point.16 In the present study, the optimal critical value of SPINK1 was 65.4101 ng/mL, sensitivity was 88.5%, and specificity was 90%. The optimal critical value of PCT was 0.575 ng/mL, sensitivity was 90.4%, and specificity was 100%. SPINK1 combined with PCT for diagnosing sepsis demonstrated up to 98.1% sensitivity and 100% specificity (Figure 3B and Table 2).
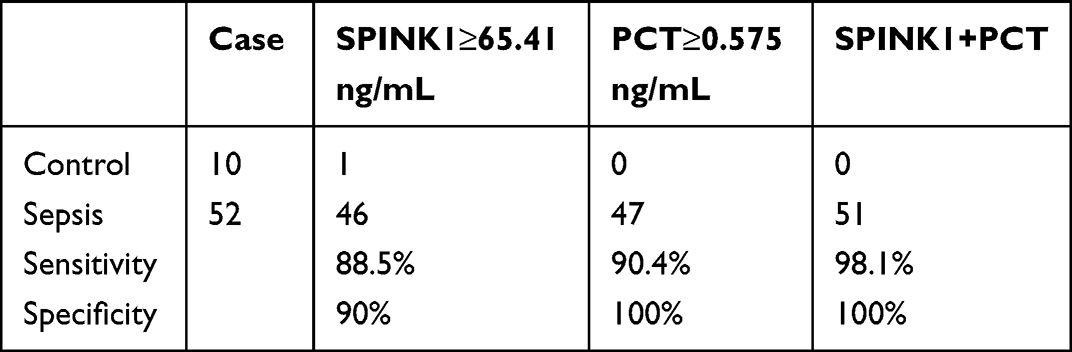 |
Table 2 Sensitivity and Specificity of SPINK1, PCT and SPINK1 Combined with PCT in the Diagnosis of Sepsis |
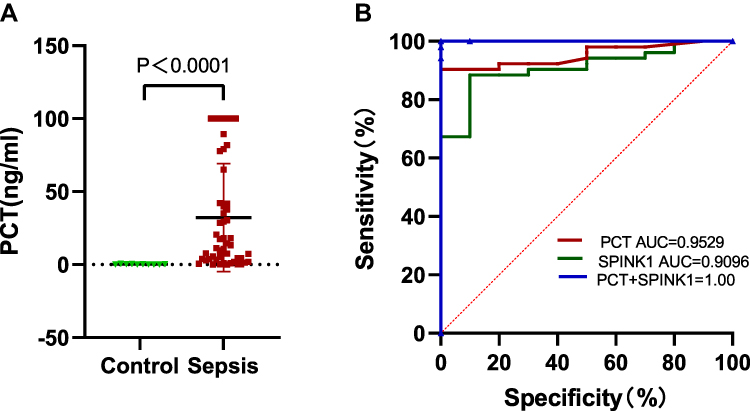 |
Figure 3 SPINK1 and PCT have high diagnostic efficiency for sepsis. (A)The PCT in sepsis group was significantly higher than that in normal group, and the difference was statistically significant (P<0.0001). (B) The true positive rate (sensitivity) and false positive rate (specificity) of SPINK1, PCT and SPINK1 combined with PCT at different possible cutting points were used to plot the ROC curve. The area under the ROC curve is calculated to represent the AUC value. |
SPINK1 Was Associated with the SOFA and APACHE II Scores and the 28-Day Survival Rate in Sepsis Patients
In this study, SPINK1 was correlated with the data on sex and age, inflammation indexes, bilirubin, creatinine, troponin, clotting time, lactate, and APACHE II scores (Table 1), and there was a weak correlation with the SOFA and APACHE II scores. SPINK1 expression positively correlated with the SOFA score (r = 3497, P = 0.0053) (Figure 4A) and the APACHE II score (r = 3223, P = 0.0106) (Figure 4B). Additionally, the survival analysis revealed that high SPINK1 expression negatively correlated with 28-day survival (P = 0.0149) (Figure 4C).
 |
Figure 4 SPINK1 was associated with the SOFA and APACHE II scores and the 28-day survival rate in sepsis patients. (A)Positive correlation between SPINK1 and Sofa score in sepsis patients (r=0.3497, P=0.0053). (B) Positive correlation SPINK1 and Apache II score in sepsis patients (r=0.322, P=0.0106). (C) SPINK1 survival analysis based on clinical data showed a negative correlation between SPINK1 and patient survival (P=0.0149). |
Discussion
sepsisThe 2016 Save Sepsis campaign redefined sepsis,17 and sepsis diagnosis and treatment have greatly advanced. However, the morbidity and mortality rates of sepsis and septic shock remain high, and early identification and appropriate management of sepsis patients improves prognosis. Nevertheless, the current early screening tools are all subject to limitations,1 and there is an urgent need to identify higher-sensitivity and -specificity biomarkers, which would improve sepsis diagnosis. In the present study, the peripheral blood plasma of healthy controls and sepsis patients underwent DIA analysis, which revealed that SPINK1 protein expression might be increased in sepsis patients. This result was verified by expanding the samples and detecting SPINK1 levels in the patients’ plasma using ELISA. The ELISA confirmed that SPINK1 was highly expressed in sepsis patients.
SPINK1 is a serine protease inhibitor family member. Under physiological conditions, SPINK1 is secreted by pancreatic follicular cells and is the first line of defense against premature trypsinogen activation in the pancreatic follicles and ducts. SPINK1 is also a potent inhibitor of trypsin 1 and 2,18 which regulate tissue repair, gastroprotection, and normal pancreatic development.19 In the present study, we determined that SPINK1 has high sensitivity and specificity for diagnosing sepsis. The literature review revealed that SPINK1 is abnormally expressed in various tumors, such as liver, breast, ovarian, lung, pancreatic, and renal cancers, and correlates with their overall survival rates.20 SPINK1 is upregulated in several tumors at the transcriptome level, such as hepatocellular carcinoma21 and prostate cancer.22 However, the previous transcriptomic sequencing results of sepsis patients and healthy controls by our group did not reveal SPINK1 expression at the transcriptome level. Additionally, analysis of the Gene Expression Omnibus (GEO) data sets GSE54514, GSE67652, GSE69528, GSE28750, and GSE95233 revealed that SPINK1 was only expressed in GSE28750 and GSE95233. Single gene meta-analysis revealed no statistically significant difference in SPINK1 between the two data sets (Figure S1), suggesting that elevated SPINK1 protein expression in sepsis plasma might demonstrate specificity. As it is unclear whether SPINK1 is expressed at the protein level in the plasma of patients with tumors, it is unclear whether it is specific in sepsis. A meta-analysis of 3244 patients suggested that PCT had a composite sensitivity of 77% and specificity of 79% for sepsis in critically ill patients,1 suggesting that PCT has a predictive role in ICU sepsis but with limited utility.8 In this study, ROC curves plotted for PCT indicated high sensitivity and specificity. Our results differed significantly from those of this meta-analysis, which was likely related to the small sample size and single-center nature of this study. The diagnostic efficacy of sepsis was improved by combining SPINK1 with PCT to diagnose patients. The combined analysis significantly improved the sepsis diagnostic sensitivity and specificity.
In 1994, the European Society of Critical Care Medicine formally developed the SOFA score in Paris,23 which assigns values to the severity of central nervous system, cardiovascular, respiratory, hepatic, renal, and coagulation and is widely used for assessing sepsis-associated organ failure. The SOFA score was formally used to diagnose sepsis instead of the SIRS score in 2016, and studies on the SOFA score have increased while finding that its use is delayed and lacks sensitivity and assessment complexity in diagnosing sepsis.24. However, the SOFA score is superior to SIRS, qSOFA, and National Early Warning Score (NEWS) for predicting in-hospital mortality in sepsis patients and can be used as a screening tool to predict 28/30-day mortality in patients with sepsis in low-income countries.25 The APACHE II score proposed by Knaus et al in 1985 consists of three components: an acute physiologic score, an age score, and a chronic health score.26 The APACHE II score is a widely used tool for assessing illness severity and the risk of death in ICU patients, where higher scores are associated with higher mortality.27 Our results demonstrated a weak positive correlation between SPINK1 and the SOFA and APACHE II scores. High SPINK1 expression negatively correlated with the 28-day survival rate of sepsis patients. However, our study was subject to the following limitations: the number of sequencing samples was low, and there might have been false positives. The limited number of populations using ELISA validation for sepsis plasma and the single-center nature of the study renders it susceptible to bias. We will conduct a cohort study to increase the sample size and conduct a multi-center study for validation.
Conclusion
SPINK1 protein expression was increased in the plasma of sepsis patients, and combining it with PCT might have a high diagnostic value for sepsis. SPINK1 was associated with the SOFA and APACHE II scores and the 28-day survival rate in sepsis patients.
Data Sharing Statement
All data and materials were in full compliance with the journal’s policy. And the data were obtained in emergency intensive care unit, the Affiliated Hospital, Southwest Medical University. The datasets used and during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Affiliated Hospital of Southwest Medical University (Ethics Nos. ky2018029 and ky2022094), and each specimen was signed by the patient or family members for consent, and the clinical trial registration numbers were: ChiCTR1900021261 and ChiCTR2200057401, This study was performed in accordance with the ethical standards in the 1964 Declaration of Helsinki.
Acknowledgments
Thanks to the medical staff of Emergency Medicine Department of Affiliated Hospital of Southwest Medical University for their assistance in collecting clinical samples.
Funding
The Southwest Medical University research project, Grant/Award Number: 2021ZKQN092, Clinical key specialty construction project of Sichuan Province and Sichuan Science and Technology Program (Number: 2022YFS0632) supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
2. Schorr C, Odden A, Evans L, et al. Implementation of a multicenter performance improvement program for early detection and treatment of severe sepsis in general medical-surgical wards. J Hosp Med. 2016;11 Suppl 1:S32–S39. doi:10.1002/jhm.2656
3. Alberto L, Marshall AP, Walker R, Aitken LM. Screening for sepsis in general hospitalized patients: a systematic review. J Hosp Infect. 2017;96(4):305–315. doi:10.1016/j.jhin.2017.05.005
4. Bhattacharjee P, Edelson DP, Churpek MM. Identifying patients with sepsis on the hospital wards. Chest. 2017;151(4):898–907. doi:10.1016/j.chest.2016.06.020
5. Nishibori M, Wake H, Morimatsu H. Histidine-rich glycoprotein as an excellent biomarker for sepsis and beyond. Crit Care. 2018;22(1):209. doi:10.1186/s13054-018-2127-5
6. Barichello T, Generoso JS, Singer M, Dal-Pizzol F. Biomarkers for sepsis: more than just fever and leukocytosis-A narrative review. Crit Care. 2022;26(1):14. doi:10.1186/s13054-021-03862-5
7. El-Khazragy N, Mohamed NM, Mostafa MF, et al. miRNAs: novel noninvasive biomarkers as diagnostic and prognostic tools in neonatal sepsis. Diagn Microbiol Infect Dis. 2023;107(3):116053. doi:10.1016/j.diagmicrobio.2023.116053
8. Povoa P, Coelho L, Dal-Pizzol F, et al. How to use biomarkers of infection or sepsis at the bedside: guide to clinicians. Intensive Care Med. 2023;49(2):142–153. doi:10.1007/s00134-022-06956-y
9. Kennis B, Ali A, Lasoff D, Sweeney DA, Wardi G. The diagnostic utility of procalcitonin is limited in the setting of methamphetamine toxicity. Am J Emerg Med. 2022;54:36–40. doi:10.1016/j.ajem.2022.01.049
10. Essmann L, Wirz Y, Gregoriano C, Schuetz P. One biomarker does not fit all: tailoring anti-infective therapy through utilization of procalcitonin and other specific biomarkers. Expert Rev Mol Diagn. 2023;2023:1–14.
11. Mun DG, Renuse S, Saraswat M, et al. PASS-DIA: a data-independent acquisition approach for discovery studies. Anal Chem. 2020;92(21):14466–14475. doi:10.1021/acs.analchem.0c02513
12. Luo M, Zhang Q, Hu Y, Sun C, Sheng Y, Deng C. LGALS3BP: a potential plasma biomarker associated with diagnosis and prognosis in patients with sepsis. Infect Drug Resist. 2021;14:2863–2871. doi:10.2147/IDR.S316402
13. Wang C, Li Y, Li S, Chen M, Hu Y. Proteomics combined with RNA sequencing to screen biomarkers of sepsis. Infect Drug Resist. 2022;15:5575–5587. doi:10.2147/IDR.S380137
14. Kazal LA, Spicer DS, Brahinsky RA. Isolation of a crystalline trypsin inhibitor-anticoagulant protein from pancreas. J Am Chem Soc. 1948;70(9):3034–3040. doi:10.1021/ja01189a060
15. Lin TC. Functional roles of SPINK1 in cancers. Int J Mol Sci. 2021;22(8):1.
16. Ruopp MD, Perkins NJ, Whitcomb BW, Schisterman EF. Youden index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom J. 2008;50(3):419–430. doi:10.1002/bimj.200710415
17. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
18. Sahin-Toth M. Human mesotrypsin defies natural trypsin inhibitors: from passive resistance to active destruction. Protein Pept Lett. 2005;12(5):457–464. doi:10.2174/0929866054395356
19. Itkonen O, Stenman UH. TATI as a biomarker. Clin Chim Acta. 2014;431:260–269. doi:10.1016/j.cca.2014.02.014
20. Liao C, Wang Q, An J, et al. SPINKs in tumors: potential therapeutic targets. Front Oncol. 2022;12:833741. doi:10.3389/fonc.2022.833741
21. Jia J, Ga L, Liu Y, et al. Serine protease inhibitor kazal type 1, a potential biomarker for the early detection, targeting, and prediction of response to immune checkpoint blockade therapies in hepatocellular carcinoma. Front Immunol. 2022;13:923031. doi:10.3389/fimmu.2022.923031
22. Stevens C, Hightower A, Buxbaum SG, Falzarano SM, Rhie SK. Genomic, epigenomic, and transcriptomic signatures of prostate cancer between African American and European American patients. Front Oncol. 2023;13:1079037. doi:10.3389/fonc.2023.1079037
23. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
24. Wang X, Guo Z, Chai Y, et al. Application prospect of the SOFA score and related modification research progress in sepsis. J Clin Med. 2023;12(10):1.
25. Qiu X, Lei YP, Zhou RX. SIRS, SOFA, qSOFA, and NEWS in the diagnosis of sepsis and prediction of adverse outcomes: a systematic review and meta-analysis. Expert Rev Anti Infect Ther. 2023;21(8):891–900. doi:10.1080/14787210.2023.2237192
26. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
27. Baldira J, Ruiz-Rodriguez JC, Ruiz-Sanmartin A, et al. Use of Biomarkers to improve 28-day mortality stratification in patients with sepsis and SOFA </= 6. Biomedicines. 2023;11(8). doi:10.3390/biomedicines11082149
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identifying Potential Effective Diagnostic and Prognostic Biomarkers in Sepsis by Bioinformatics Analysis and Validation
Huang X, Tan J, Chen X, Zhao L
International Journal of General Medicine 2022, 15:6055-6071
Published Date: 6 July 2022
Impaired Circulating Antibody-Secreting Cells Generation Predicts the Dismal Outcome in the Elderly Septic Shock Patients
Xu H, Li T, Zhang X, Li H, Lv D, Wang Y, Huo F, Bai J, Wang C
Journal of Inflammation Research 2022, 15:5293-5308
Published Date: 13 September 2022
Integrated Analysis Identified TGFBI as a Biomarker of Disease Severity and Prognosis Correlated with Immune Infiltrates in Patients with Sepsis
Shi M, Wei Y, Guo R, Luo F
Journal of Inflammation Research 2024, 17:2285-2298
Published Date: 15 April 2024
PCT/ALB Ratio in Initial Three days for the Prediction of Secondary Infection in Septic Patients
Zhang C, Huang G, Li H, Zhang T, Jian M, Huang C, Zhang Y, Wang Z, Hou X, Xia Y, Jiang W
Infection and Drug Resistance 2025, 18:625-633
Published Date: 1 February 2025
Neutrophil Extracellular Traps in Sepsis and Sepsis-Related Organ Dysfunction
Yan W, Xu X, Li X, Ma Y, Guo L, Yang J, Jin Z, Zhang J, Li T
ImmunoTargets and Therapy 2025, 14:1373-1393
Published Date: 27 November 2025