Back to Journals » International Journal of General Medicine » Volume 19
Hematoma Capsule Spanning the Sylvian Fissure and Non-Blocking the Middle Meningeal Artery During Surgery Are Associated With Postoperative Recurrence of Chronic Subdural Hematoma
Received 15 September 2025
Accepted for publication 20 December 2025
Published 8 January 2026 Volume 2026:19 567757
DOI https://doi.org/10.2147/IJGM.S567757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Redoy Ranjan
Sen He,1 Fang Xue,1 Mingli Wei2
1Department of Neurosurgery, West China Hospital of Sichuan University-Ziyang Hospital & Ziyang Central Hospital, Ziyang, Sichuan, 641300, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, West China Hospital of Sichuan University-Ziyang Hospital & Ziyang Central Hospital, Ziyang, Sichuan, 641300, People’s Republic of China
Correspondence: Mingli Wei, Department of Respiratory and Critical Care Medicine, West China Hospital of Sichuan University-Ziyang Hospital & Ziyang Central Hospital, No. 66, Rende west Road, Yanjiang District, Ziyang, Sichuan, 641300, People’s Republic of China, Email [email protected]
Background: Despite advances in surgical techniques, recurrence after chronic subdural hematoma (CSDH) evacuation remains common. With the aging of the population, the incidence rate is still rising. Most patients require surgical treatment, but postoperative hematoma recurrence remains an important factor affecting patient prognosis.
Objective: This study aimed to identify factors influencing recurrence following neuroendoscopic-assisted drainage.
Methods: CSDH patients who underwent neuroendoscopy-assisted hematoma drainage(NEAHD) via a single burr-hole craniostomy between January 2021 and August 2024 were categorized based on the presence or absence of postoperative hematoma recurrence. Binary logistic regression analysis was performed on the variables that showed statistically significant inter-group differences in univariate analyses.
Results: In total, 121 patients with CSDH were included. The recurrence group consisted of 17 patients (14.05%). Gender, age, smoking, alcoholism, hypertension or diabetes, perioperative use of statins, hematoma thickness, midline deviation distance, and direction, depth, and retention time of the drainage tube were not associated with hematoma recurrence. In contrast, hematoma capsule spanning the Sylvian fissure (P < 0.001; OR = 12.504; 95% CI, 3.091– 50.583) and non-blocking the main trunk or major branches of the middle meningeal artery (MMA) (P = 0.006; OR = 9.955; 95% CI, 1.911– 51.848) were the independent risk factors for hematoma recurrence after NEAHD surgery.
Conclusion: Spanning of the hematoma capsule over the Sylvian fissure and absence of intraoperative occlusion of the middle meningeal artery are independent risk factors for recurrence. These features should be considered when planning surgical strategies for CSDH.
Keywords: chronic subdural hematoma, neuroendoscopy, surgery, prognosis, recurrence
Introduction
Chronic subdural hematoma (CSDH) is a common neurosurgical disease.1 It refers to an abnormal accumulation of bloody components between the surface of the brain and the dura mater.2 Its incidence rate is about 20.6/100,000 people/year. It is more common in the elderly; among people aged over 80 years, its incidence rate can reach 127/100,000 people/year.3–5 With the aging of the population and the increasing use of antithrombotic drugs, the incidence rate of CSDH and the number of surgeries are rising steadily.1,6,7 CSDH not only affects the quality of life and survival time of patients, but also imposes a heavy burden on families and society.
At present, it is believed that the cascade of bleeding and inflammation caused by trauma is an important cause of the formation of CSDH.8 Patients with CSDH may present with clinical manifestations such as headache, dizziness, nausea, vomiting, hemiplegia, and cognitive impairment. Diagnosis can be made by combining imaging examinations. The treatment plan includes surgical and nonsurgical treatment.9 For CSDH with small lesion volume, insignificant space-occupying effect, and mild clinical discomfort symptoms, drug therapy can be used.10–12 However, for CSDH with obvious symptoms or occupying effects, surgical treatment is required.13 Given its advantages in terms of safety, minimal damage, and rapid relief of occupying effects, burr-hole evacuation is the preferred surgical procedure for CSDH patients.14 However, considering its high postoperative hematoma recurrence rate of 37.3%, it is currently mainly used to treat patients with uniform hematoma density, inorganic structure, and no obvious separation.14–18
Endoscopic CSDH clearance and middle meningeal artery (MMA) embolization have gradually been applied in clinical practice and have become current hot topics.1,19–24 Nevertheless, there is still controversy over the ability of MMA embolization to reduce the risk of postoperative hematoma recurrence in CSDH patients.20–22,25,26 Thus, more high-quality evidence is needed to support the safety of MMA embolization for CSDH treatment.1,21,27 Neuroendoscopy has several advantages, such as minimal trauma and good field of view. Neuroendoscopy-assisted hematoma-removal surgery can remove the capsule, septa, and blood clots of the hematoma, with sufficient exposure and good field of view. It has become a commonly used surgical procedure for treating CSDH with complex conditions such as septa, capsules, and blood clots. Compared with burr-hole evacuation, neuroendoscopy-assisted hematoma removal can reduce the risk of postoperative hematoma recurrence in CSDH patients.23,24,28,29 However, some patients still experience hematoma recurrence after neuroendoscopy-assisted hematoma-removal surgery, so recurrence remains a major issue that needs to be urgently addressed.30,31 Therefore, further exploration of the factors related to the recurrence of CSDH after neuroendoscopy-assisted hematoma-removal surgery is of great significance for improving the efficacy and prognosis.4,32
Previous studies have reported that male gender, older age, drinking, diabetes, high density (mixed density) of hematoma on computed tomography (CT), presence of hematoma septum or capsule (thickened intima), hematoma thickness greater than 2 cm, and pneumocephalus are risk factors for postoperative recurrence(POR).17,33–39 However, these studies have not specifically discussed the factors influencing hematoma recurrence after endoscopy-assisted treatment of CSDH. Because neuroendoscopy-assisted hematoma-clearance surgery can completely remove solid components and separate the hematoma cavity during surgery, it may reduce the risk of hematoma recurrence in these patients after surgery. However, patients undergoing such surgery may be at a higher risk of hematoma encapsulation, which increases the risk of recurrence. The specific influencing factors are not yet clear. Thus, this study investigated factors influencing CSDH recurrence following NEAHD using regression analysis of data from 121 patients.
Materials and Methods
This study was a retrospective analysis, and the research protocol was approved by the Ethics Committee of Ziyang Hospital, West China Hospital, Sichuan University (Approval No. 2024199). The requirement for informed consent was waived due to the retrospective design. For this study, we screened all CSDH patients who had received treatment at the Neurosurgery Department of Ziyang Hospital, West China Hospital of Sichuan University from January 2021 to August 2024, and obtained written consent from the subjects themselves or their families.
Inclusion and Exclusion Criteria
All of the CSDH patients enrolled in this study met the following criteria: age ≥ 18 years; unilateral or bilateral CSDH on cranial CT or head magnetic resonance (MR) imaging; presence of septa, high density, or uneven density (signal) within the hematoma; a midline shift of more than 1 cm, or clinical symptoms such as headache, vomiting, limb weakness, or numbness; patients who have received general anesthesia; patients who underwent NEAHD via a single burr-hole craniostomy. The exclusion criteria were as follows: Patients with bilateral CSDH who underwent surgical treatment on one side within 6 months of receiving surgical treatment on the other side for CSDH; Patients with incomplete information; subdural hematoma caused by cerebrovascular diseases such as intracranial aneurysm, intracranial vascular malformation, moyamoya disease, or subarachnoid hemorrhage; subdural hemorrhage caused by intracranial tumors; and surgical contraindications, such as coagulation dysfunction and cardiac or pulmonary dysfunction.
Data Collection
We collected data on clinical characteristics of each subject who met the eligibility criteria, including demographic data, medical history, imaging features of hematoma (thickness, septa, midline shift, and capsule distribution), treatment status (bone window size; occlusion of the frontal and parietal branches of the MMA; direction, depth, and duration of retention of the drainage tube; and post operative use of statins). Patients underwent head CT or MR scans at 1, 3, and 6 months after surgery, and whether the hematoma recurred within 180 days after surgery. A total of 143 patients met the inclusion criteria, but 22 were excluded due to factors such as loss to follow-up or contralateral reoperation, etc. The thickness and midline displacement distance of the hematoma were measured by the maximum thickness layer and the maximum displacement layer of the hematoma in the horizontal plane, respectively (Figure 1A). We also recorded the distribution of the capsule and whether it spanned the Sylvian fissure (Figure 1A). CT and MR images of the hematoma showed cord-like density or signal within the hematoma (Figure 1A–E). The size of the bone window was recorded as the product of the maximum longitudinal diameter and the maximum transverse diameter of the bone window (Figure 1F). The occlusion of the frontal or parietal branch of the MMA was also noted. After surgery, thin-layer CT imaging of the patient’s head was performed to display the main branches of the MMA and record whether the bone flap contained the main trunk or branches of the frontal or parietal branch of the MMA (Figure 1F). Hematoma recurrence is defined as the reoccurrence or re-increase of hematoma at the original hematoma site, confirmed by head CT or MR within 180 days after surgery, with the hematoma volume reaching or exceeding 30% of the pre-operative volume, or with the midline shift caused by the hematoma being no less than half of the pre-operative value, accompanied by neurological symptoms or signs related to hematoma, such as hemiplegia, apathy, and drowsiness, requiring surgical treatment. CT and MR are both non enhanced scans. CT scanning equipment: GE LightSpeed VCT 64 row spiral CT machine; Scanning layer thickness: 5mm; scanning conditions: 120kVp, 200mA; Brain window (width 80 HU, level 40 HU) and bone window (width 2000–4000 HU, level 400–700 HU) settings were used for image review. MR scanning equipment: Siemens Magnetom Skyra 1.5T MRI System; Scanning sequence: T1 weighted imaging (T1WI), T2 weighted imaging (T2WI), fluid attenuated inversion recovery sequence (FLAIR); Scanning layer thickness: 1mm; Two neuroradiologists who were blinded to the clinical outcomes jointly evaluated the above imaging data, and reached a consensus through discussion in case of disagreement. Depending on whether or not they experienced hematoma recurrence after surgery, the patients were divided into the recurrence group and the non-recurrence group (Figure 1).
 |
Figure 1 Chronic subdural hematoma (CSDH) on the right side. (A) Computed tomography (CT) horizontal images show high-density shadows on the inner and outer edges of the hematoma before and after transverse rupture, with mixed high-density and low-density shadows inside the hematoma dominated by equi-density shadows, and the midline structure shifting toward the opposite side; (B) The CT sagittal view shows high-density shadows in the anterior, posterior, and lower edge of the hematoma capsule, with high-density septa and low-density shadows inside the hematoma cavity dominated by iso-density shadows; (C) CT coronal view shows a high-density shadow around the edge of the hematoma capsule, a low-density shadow above the hematoma, and an iso-density shadow below, with local brain tissue being compressed; (D) MRI T1 shows a “crescent-shaped” high-signal shadow below the dura mater with low-signal streaks; (E), MRI T2 shows a slightly high-signal shadow below the dura mater with a clear boundary with brain tissue, separated internally by a cord-like low-signal shadow; (F) Postoperative skull CT three-dimensional imaging shows a bone flap size of approximately 1.77 cm × 2.91 cm, covering the main branches of the frontal or parietal branch of the MMA. |
Patient Surgical Methods
Anesthesia methods: All patients received general anesthesia with endotracheal intubation performed by the same anesthesia team. Continuous monitoring of vital signs and blood oxygen saturation during surgery. Resuscitate the patient after the surgery and remove the endotracheal tube.
Surgical methods: All patients underwent surgery performed by the same neurosurgeon team. Intraoperative navigation equipment was not used during the surgery.the patients were placed in a supine position with their head slightly above their feet. A straight, 5-cm-long incision was made at the top of the temporal region, with the center of the incision located on the surface projection of the hematoma center. A burr hole (approximately 1 cm in diameter) was created using a skull drill. If the MMA was visualized beneath the burr hole, it was first occluded using bipolar electrocoagulation and then divided. The dura mater was cut open in a “cross” shape, the hematoma was slowly released, and a 0° neuroendoscope (STORZ) was inserted into the hematoma cavity through the bone window to observe whether there were residual blood clots, septa, or other complications. If there was a large amount of residual hematoma that could not be washed away or the hematoma cavity was well-separated, a milling cutter was used to open the skull through the burr hole, forming a bone window with a diameter of approximately 3 cm. The size of the bone window was not predetermined but was adjusted intraoperatively. A milling cutter was used to expand the initial burr-hole into a larger bone window only when necessary to achieve adequate endoscopic access and maneuverability, such as in cases with extensive fibrous septations or a tight, restrictive hematoma capsule. If the MMA was identified beneath the bone window, it was first occluded using bipolar electrocoagulation, then divided, before proceeding to incise the dura mater. A suction device was used under the neuroendoscope to remove the residual hematoma, and micro scissors and suction devices were used to endoscopically managed the separation. After confirming that there was no active bleeding in the surgical area, the area was repeatedly rinsed with 37°C warm saline solution, and a drainage tube was placed at the lowest point of the hematoma cavity. The dura mater was sutured, and the fixed bone flap was repositioned. The scalp was sutured layer by layer, and the surgery was concluded.
Postoperative managements: After the patient’s postoperative consciousness is restored, they will be sent back to the ward and receive the same treatment measures. The management measures for drainage tubes are as follows: the drainage tube approximately 10 cm below the interventricular foramen for drainage, the drainage tube was removed within 24 hours when the drainage volume was less than 30 mL or on the 5th day after surgery.
Statistical Methods
IBM SPSS software 22.0 was used for statistical analysis. Count data were presented as n (%), and inter-group associations were based on the chi-square test or Fisher’s exact probability method. Continuous variables were presented as mean ± standard deviation. The normality of continuous variables was assessed using the Shapiro–Wilk test. Based on this assessment, independent samples t-test was used for normally distributed data. Variables with P-values < 0.05 in the univariable analysis of hematoma recurrence were included as the independent influencing factors in the binary logistic regression analysis. P-values < 0.05 indicated a statistically significant. The interobserver consistency in the assessment of imaging data was evaluated using Cohen’s kappa (κ) statistic.
Results
A total of 121 patients were included in the study. There were 96(79.3%) males and 25(20.7%) females, The ratio of males to females is approximately 3.8:1, with a minimum age of 39 years and a maximum age of 86 years, and an average age of 67.4 ± 8.2 years. There were 104(85.95%) patients in the non-recurrence group and 17 (14.05%)patients in the recurrence group, with a recurrence rate of 14.05%. Among the 35 patients who only received endoscopic assisted treatment after drilling, 7 (20%) experienced recurrence, and among the 86 patients who underwent neuroendoscopic assisted treatment with milling cutters to enlarge the bone window, 10 (11.6%) experienced recurrence. There was no statistically significant difference in the postoperative hematoma recurrence rate between these two different surgical procedures (χ2=1.444, p=0.255), however, there was a statistically significant difference in the duration of surgery (t=4.889, p=0.015). The interobserver agreement between the two neuroradiologists for assessing imaging data was excellent (Cohen’s κ = 0.68).
Univariate Analyses
The results of the univariate analyses (Tables 1 and 2) showed that there were association inter-group in whether hematoma capsule spanned the Sylvian fissure, the presence of septa in the hematoma cavity, and the lack of the main trunk or major branches of the MMA under the bone flap of the bone window, while there were no association in other indicators.
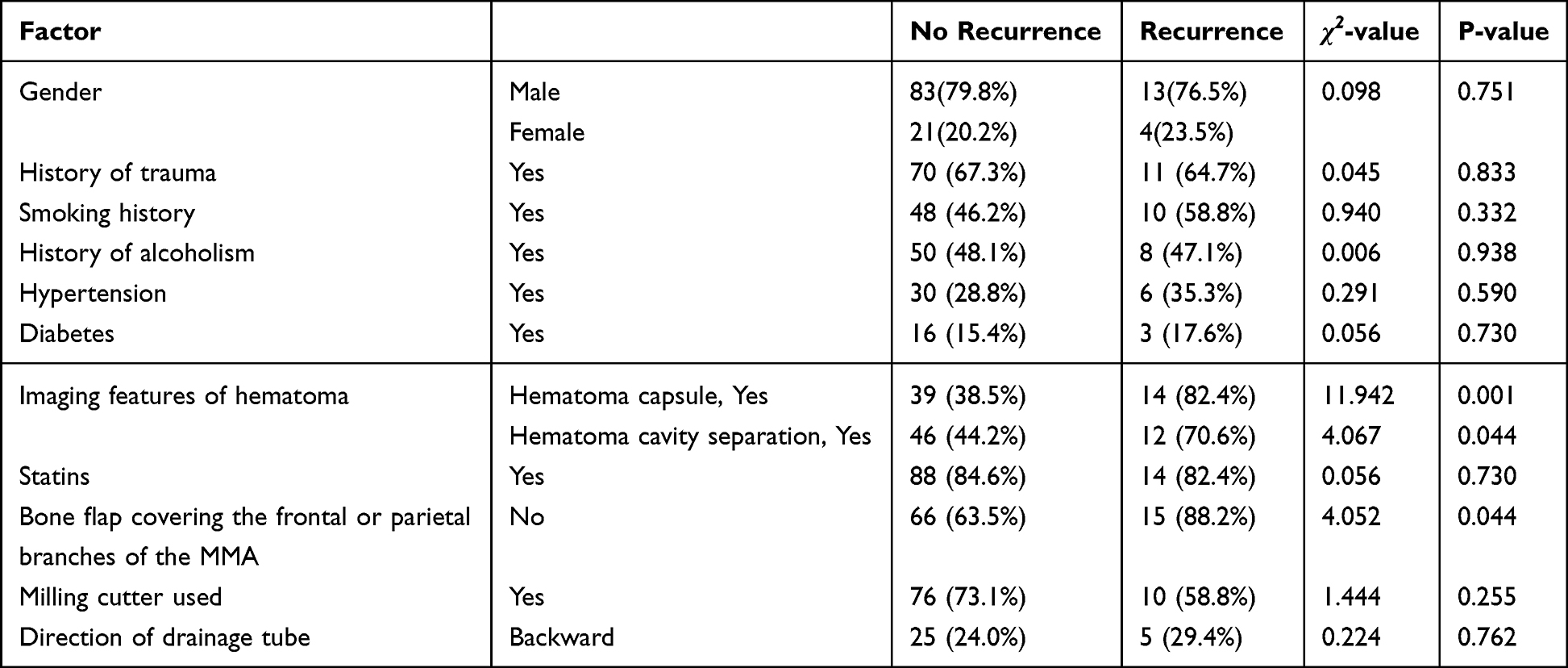 |
Table 1 Univariable Analysis of Factors Influencing Hematoma Recurrence After Neuroendoscope-Assisted Chronic Subdural Hematoma Drainage(Chi Square Test) |
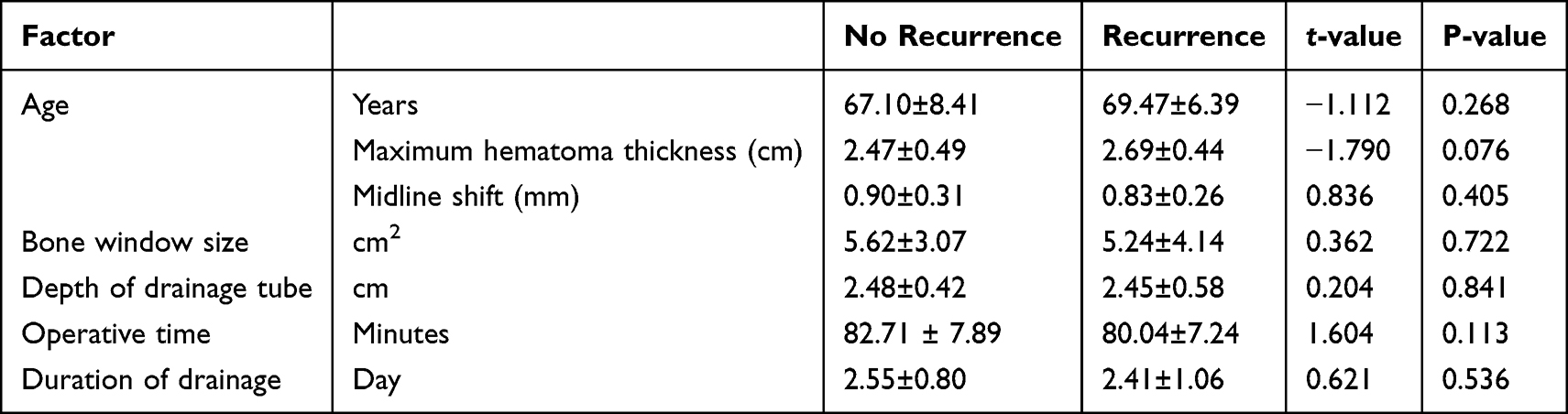 |
Table 2 Univariable Analysis of Factors Influencing Hematoma Recurrence After Neuroendoscope-Assisted Chronic Subdural Hematoma Drainage(T-Test) |
Multivariate Analysis
Multivariate binary logistic regression analysis was performed to determine the factors affecting POR of CSDH. Specifically, the POR of CSDH was selected as the dependent variable, while the significant factors from the univariate analyses were included as the independent variables. The final logistic regression model demonstrated good fit, as indicated by a non-significant Hosmer-Lemeshow test (χ2 =0.687, p =0.995). The results showed that hematoma capsule spanning the Sylvian fissure and the bone flap of the bone window that did not include the main trunk or the frontal or parietal branch of the MMA were the independent risk factors for POR of CSDH (Table 3).
 |
Table 3 Multivariable Analysis of Hematoma Recurrence After Neuroendoscopic Assisted Drainage for Chronic Subdural Hematoma |
Discussion
To the best of our knowledge, We reported for the first time that the distribution of the hematoma capsule across the Sylvian fissure pool and non-blocking the MMA during surgery were the risk factors for POR of CSDH. Although there have been previous studies on the factors influencing POR of CSDH, these studies did not specifically focus on NEAHD and specific CSDH patients.17,33,34,40,41 In this study, the overall recurrence rate was 14.05%, which is consistent with previously reported recurrence rates of 10%–20%.5 Due to the differences in the details and adaptability of patients undergoing NEAHD surgery compared with other surgical methods, the factors affecting POR may not be entirely consistent.
First, NEAHD can endoscopically managed solid components and partition the hematoma cavity under direct visualization. This eliminates the previously reported hematoma cavity separation as a risk factor for POR in CSDH.33,36 In theory, this should reduce the risk of recurrence for patients. In this study, inter-group comparisons revealed that the presence of hematoma compartment separation was a significant risk factor for postoperative hematoma recurrence (P = 0.044), but the significance was lost in the multivariate analysis (P = 0.058; 95% CI, 0.960–11.751). This may be due to the lack of medical treatment for the separation of hematoma cavities duringtwist drill evacuation or burr-hole evacuation, which could affect the POR of hematoma. However, in NEAHD surgery, the separation of hematoma cavities was appropriately treated in all patients. Thus, the separation of hematoma cavities in these patients no longer existed after surgery and had no effect on hematoma recurrence.
Second, NEAHD often requires drilling larger holes in the skull or milling a small bone flap with a milling cutter. This may increase the possibility of postoperative intracranial gas accumulation, which means that the risk of POR may increase.40 Yet, larger bone pores or flaps are beneficial for residual hematoma or exudate to flow out through the bone window and be absorbed by soft tissues such as the temporal muscle in the head, which plays a role in subperiosteal drainage.42 In this study, we compared the size of the bone window formed during surgery between the two groups of patients and found no significant difference between them. The inter-group comparison (P = 0.722) did not indicate that the size of the bone window had an impact on POR. Interestingly, we found significant inter-group differences in terms of whether the bone flaps formed by milling cutters crossed the main trunk or major branches of the MMA. Among the 17 patients in the recurrence group, 15 patients (88.2%) had bone flaps that did not cover the aforementioned arteries, while in the non-recurrence group, the proportion was 63.5%. The inter-group difference was statistically significant (P = 0.044), even after multivariate analysis (P = 0.006; OR = 9.955; 95% CI, 1.911–51.848). The difference between the two groups of patients suggests the absence of the bone window spanning the main trunk or major branches of the MMA as a associated factor for POR. The reason for this difference may be as follows: when the MMA branches were below the bone flap, intraoperative hemostasis and electrocoagulation were performed on these arteries when cutting open the meninges, causing their occlusion and playing a role similar to interventional embolization. Interventional embolization treatment for CSDH is achieved by embolization of the MMA under interventional surgery, resulting in occlusion of the MMA.1,22,43 After surgery, the blood supply to the meninges in these vascular supply areas is significantly reduced or even completely eliminated, thereby reducing or blocking the blood supply to the hematoma capsule in the corresponding area and consequently reducing recurrence. Consequently, we recommend that in surgical planning for CSDH patients undergoing NEAHD, the bone window be designed to cover the main trunk or major branches of the MMA, with intraoperative blocking performed. To our knowledge, there is currently no literature reporting this strategy.
Third, in this study, we observed a significant difference in the spatial characteristics of the hematoma capsule between the two groups of patients (P < 0.001; OR = 12.504; 95% CI, 3.091–50.583). Namely, the recurrence group had a greater proportion of cases with hematoma capsule spanning the Sylvian fissure (82.4%) compared with the non-recurrence group (38.5%). This finding is similar to previous reports that the capsule is a risk factor for postoperative hematoma recurrence in CSDH patients.18,33,34,36 However, our study further described which form of capsule was more likely to cause postoperative hematoma recurrence. Specifically, when performing surgical treatment for CSDH patients with hematoma capsule spanning the Sylvian fissure, the risk of POR should be fully considered, and NEAHD should be carefully selected. Further research is needed to determine the optimal surgical plan for such patients.
Fourth, in this study, there were no significant inter-group differences in gender, age, smoking, alcoholism, hypertension or diabetes, perioperative use of statins, hematoma thickness, midline deviation distance, and drainage tube direction, depth, and retention time. These findings disagree with previous reports.33,39,41 In addition to the differences in patient disease factors and surgical methods, we used t tests for continuous variables such as age, hematoma thickness, midline offset distance, and drainage tube depth and retention time. We only conducted binary analysis on the use of statins and drainage tube direction during the perioperative period. If we convert continuous variables into categorical variables or further collect data on the relationship between statin dosage and weight, drainage tube direction, and hematoma center and position, we may obtain different results. Still, these changes would only alter the role of the factors we are currently discussing, and the previously obtained results would remain unaffected.
This study has some limitations. First, this was a single-center retrospective study, which may not represent diverse populations across different geographic regions or healthcare systems, such as the operational details and proficiency of different surgeons, patient race and lifestyle, which may have affected the obtained results, potentially limiting the applicability of our results to broader populations. Second, We reliance on electronic health records for inclusion/exclusion, it may have introduced selection bias. Specifically, patients who did not complete follow-up visits after discharge, patients who died within 6 months after surgery, and patients who refused surgical intervention were excluded from the study. These patients might differ systematically from those retained, potentially skewing outcome estimates. Third, the sample size of this study was relatively small, especially in the recurrence group. Fourth, a major limitation of this study is the potential confounding effect of surgical heterogeneity, particularly regarding the decision to perform bone-window expansion. While this reflects real-world clinical practice, it represents a source of potential bias that must be considered when interpreting the results. Therefore, further multicenter prospective randomized controlled trials are needed to clarify the factors influencing hematoma recurrence after NEAHD in the treatment of CSDH. Critically, the proposed mechanism of MMA occlusion requires confirmation in future prospective studies that incorporate preoperative and postoperative vascular imaging (eg, CTA) to directly verify hemodynamic changes.
Conclusion
The hematoma capsule spanning the Sylvian fissure and non-blocking the main trunk or major branches of the MMA during surgery are associated with hematoma recurrence after NEAHD for CSDH treatment.
When formulating treatment plans for CSDH patients, it is necessary to fully consider the associated factors of POR. If choosing to perform NEAHD surgery, the bone window designed for the surgical approach could potentially cover the hematoma capsule spanning the Sylvian fissure and the main trunk (or major branches) of the MMA, destroy this capsule and occlude these vasculars during surgery to reduce the risk of postoperative hematoma recurrence.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study is a retrospective analysis, and the research protocol has been approved by the Ethics Committee of Ziyang Hospital, West China Hospital, Sichuan University (Approval No.2024199). The study screened all CSDH patients who received treatment in the Neurosurgery Department of Ziyang Hospital, West China Hospital of Sichuan University from January 2021 to February 2025, and obtained written consent from the subjects themselves or their families.
Consent for Publication
The written informed consent was obtained from the subjects themselves or their families.
Acknowledgments
Thanks for the support from Health Commission of Sichuan Province Medical Science and Technology Program (NO.24WSXT094).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Health Commission of Sichuan Province Medical Science and Technology Program (No. 24WSXT094) and the Ziyang Medical Research Project (No. 2025035).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Fiorella D, Monteith SJ, Hanel R, et al. Embolization of the middle meningeal artery for chronic subdural hematoma. N Engl J Med. 2025;392(9):855–10. doi:10.1056/NEJMoa2409845
2. Shibahashi K, Ohbe H, Yasunaga H. Artificial cerebrospinal fluid use during burr-hole surgery and reoperation rate in patients with chronic subdural hematoma: an analysis using a nationwide inpatient database. Acta neurochirurgica. 2023;165(5):1289–1296. doi:10.1007/s00701-023-05570-1
3. Hamou HA, Clusmann H, Schulz JB, Wiesmann M, Altiok E, Höllig A. Chronic Subdural Hematoma. Deutsches Arzteblatt International. 2022;119(12):208–213. doi:10.3238/arztebl.m2022.0144
4. Uno M, Toi H, Hirai S. Chronic subdural hematoma in elderly patients: is this disease benign? Neurologia medico-chirurgica. 2017;57(8):402–409. doi:10.2176/nmc.ra.2016-0337
5. Feghali J, Yang W, Huang J. Updates in chronic subdural hematoma: epidemiology, etiology, pathogenesis, treatment, and outcome. World Neurosurg. 2020;141:339–345. doi:10.1016/j.wneu.2020.06.140
6. Rauhala M, Luoto TM, Huhtala H, et al. The incidence of chronic subdural hematomas from 1990 to 2015 in a defined Finnish population. J Neurosurg. 2020;132(4):1147–1157. doi:10.3171/2018.12.Jns183035
7. Gaist D, García Rodríguez LA, Hellfritzsch M, et al. Association of antithrombotic drug use with subdural hematoma risk. JAMA. 2017;317(8):836–846. doi:10.1001/jama.2017.0639
8. Edlmann E, Giorgi-Coll S, Whitfield PC, Carpenter KLH, Hutchinson PJ. Pathophysiology of chronic subdural haematoma: inflammation, angiogenesis and implications for pharmacotherapy. J Neuroinflamm. 2017;14(1):108. doi:10.1186/s12974-017-0881-y
9. Kim KH, Lee Y. Medical management of chronic subdural hematoma. Korean J Neurotrauma. 2023;19(3):288–297. doi:10.13004/kjnt.2023.19.e47
10. Miah IP, Holl DC, Blaauw J, et al. Dexamethasone versus surgery for chronic subdural hematoma. N Engl J Med. 2023;388(24):2230–2240. doi:10.1056/NEJMoa2216767
11. Jiang R, Zhao S, Wang R, et al. Safety and efficacy of atorvastatin for chronic subdural hematoma in chinese patients: a randomized clinicaltrial. JAMA Neurol. 2018;75(11):1338–1346. doi:10.1001/jamaneurol.2018.2030
12. Foppen M, Lodewijkx R, Bandral HV, et al. Factors associated with success of conservative therapy in chronic subdural hematoma: a single-center retrospective analysis. J Neurol. 2024;271(6):3586–3594. doi:10.1007/s00415-024-12307-2
13. Chen H, Zhang Y, Luo B, Tang H, Shang B, Song X. Efficacy of minimally invasive soft-channel drainage for chronic subdural hematoma utilizing 3D slicer: a retrospective comparative analysis. Neurosurg Rev. 2024;48(1):1. doi:10.1007/s10143-024-03147-9
14. Raj R, Tommiska P, Koivisto T, et al. Burr-hole drainage with or without irrigation for chronic subdural haematoma (FINISH): a Finnish, nationwide, parallel-group, multicentre, randomised, controlled, non-inferiority trial. Lancet. 2024;403(10446):2798–2806. doi:10.1016/s0140-6736(24)00686-x
15. Guo S, Gao W, Cheng W, Liang C, Wu A. Endoscope-assisted surgery vs. Burr-Hole craniostomy for the treatment of chronic subdural hematoma: a systemic review and meta-analysis. Front Neurol. 2020;11(540911). doi:10.3389/fneur.2020.540911
16. Santarius T, Kirkpatrick PJ, Ganesan D, et al. Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet. 2009;374(9695):1067–1073. doi:10.1016/s0140-6736(09)61115-6
17. Miah IP, Tank Y, Rosendaal FR, et al. Radiological prognostic factors of chronic subdural hematoma recurrence: a systematic review and meta-analysis. Neuroradiology. 2021;63(1):27–40. doi:10.1007/s00234-020-02558-x
18. Peters DR, Parish J, Monk S, et al. Surgical treatment for chronic subdural hematoma in the elderly: a retrospective analysis. World Neurosurg. 2023;18(100183). doi:10.1016/j.wnsx.2023.100183
19. Kan P, Fiorella D, Dabus G, et al. ARISE I consensus statement on the management of chronic subdural hematoma. Stroke. 2024;55(5):1438–1448. doi:10.1161/strokeaha.123.044129
20. Liu J, Ni W, Zuo Q, et al. Middle meningeal artery embolization for nonacute subdural hematoma. N Engl J Med. 2024;391(20):1901–1912. doi:10.1056/NEJMoa2401201
21. Davies JM, Knopman J, Mokin M, et al. Adjunctive middle meningeal artery embolization for subdural hematoma. N Engl J Med. 2024;391(20):1890–1900. doi:10.1056/NEJMoa2313472
22. Schmolling ÁH, Pérez-García C, Trejo C, et al. Middle meningeal artery embolization for management of chronic subdural hematoma. Radiographic. 2024;44(4):e230158. doi:10.1148/rg.230158
23. Ma B, Song H, Lin W. Efficacy and prognosis of neuroendoscopy-assisted surgery for chronic subdural hematoma. Pak J Med Sci. 2023;39(2):578–582. doi:10.12669/pjms.39.2.6642
24. Wu L, Guo X, Ou Y, et al. Efficacy analysis of neuroendoscopy-assisted burr-hole evacuation for chronic subdural hematoma: a systematic review and meta-analysis. Neurosurg Rev. 2023;46(1):98. doi:10.1007/s10143-023-02007-2
25. Shotar E, Mathon B, Salle H, et al. Meningeal embolization for preventing chronic subdural hematoma recurrence after surgery: the EMPROTECT randomized clinical trial. JAMA. 2025;334(2):127–135. doi:10.1001/jama.2025.7583
26. Bastianon Santiago R, Dengri C, Kaye B, et al. Natural history of chronic subdural hematoma following middle meningeal artery embolization: a retrospective analysis. World Neurosurg. 2025;194(123501):123501. doi:10.1016/j.wneu.2024.11.084
27. Martinez-Perez R, Rayo N, Tsimpas A. Endovascular embolisation of the middle meningeal artery to treat chronic subdural haematomas: effectiveness, safety, and the current controversy. A systematic review. Neurologia. 2023;38(2):124–130. doi:10.1016/j.nrleng.2020.04.016
28. Fang H, Zhang Z, Liu Y, et al. Rigid neuroendoscopy assisted hematoma resection reduces the recurrence rate of chronic subdural hematoma with mixed density: a retrospective analytic cohort study. Front Surg. 2022;9(789118). doi:10.3389/fsurg.2022.789118
29. Liu HQ, Bai X, Xiong FL, Gao MM, Zhang HB, Liu BH. Efficacy of neuroendoscopy-assisted surgery in the treatment of chronic subdural hematoma: a meta-analysis. Chin Neurosurg J. 2024;10(1):28. doi:10.1186/s41016-024-00380-5
30. Zhong D, Cheng H, Xian Z, et al. Advances in pathogenic mechanisms, diagnostic methods, surgical and non-surgical treatment, and potential recurrence factors of chronic Subdural Hematoma: a review. Clin Neurol Neurosurg. 2024;242(108323):108323. doi:10.1016/j.clineuro.2024.108323
31. Hirata K, Fujita K, Ishikawa E, Matsumaru Y. The efficacy and safety of the internal medication therapy of the triple drugs for chronic subdural hematoma: retrospective analysis. Clin Neurol Neurosurg. 2024;244(108434):108434. doi:10.1016/j.clineuro.2024.108434
32. Hounkpatin S, Stierer M, Frechon P, et al. Comparative analysis of surgical techniques in the management of chronic subdural hematomas and risk factors for poor outcomes. Neurosurg Rev. 2024;47(1):254. doi:10.1007/s10143-024-02493-y
33. Maroufi SF, Farahbakhsh F, Macdonald RL, Khoshnevisan A. Risk factors for recurrence of chronic subdural hematoma after surgical evacuation: a systematic review and meta-analysis. Neurosurg Rev. 2023;46(1):270. doi:10.1007/s10143-023-02175-1
34. Liu LX, Cao XD, Ren YM, Zhou LX, Yang CH. Risk factors for recurrence of chronic subdural hematoma: a single center experience. World Neurosurg. 2019;132:e506–e513. doi:10.1016/j.wneu.2019.08.089
35. Ito S, Higuchi K. Subdural air increases postoperative recurrence of chronic subdural hematoma after initial burr-hole surgery only in the very elderly: a pilot study. World Neurosurg. 2021;156(e25–e29. doi:10.1016/j.wneu.2021.07.143
36. Liu H, Yan R, Xie F, Richard SA. Hematoma cavity separation and neomembrane thickness are potential triggers of recurrence of chronic subdural hematoma. BMC Surgery. 2022;22(1):236. doi:10.1186/s12893-022-01687-9
37. Andersen-Ranberg NC, Debrabant B, Poulsen FR, Bergholt B, Hundsholt T, Fugleholm K. The Danish chronic subdural hematoma study-predicting recurrence of chronic subdural hematoma. Acta neurochirurgica. 2019;161(5):885–894. doi:10.1007/s00701-019-03858-9
38. Hubbard ZS, Al Kasab S, Porto GB, Spiotta A. Chronic subdural hematoma recurrence due to contralateral neovascularization following middle meningeal artery embolization. Intervent Neuroradiol. 2022;28(6):639–643. doi:10.1177/15910199211065197
39. Zhang J, Gao A, Meng X, et al. Prediction model for poor short-term prognosis in patients with chronic subdural hematoma after burr hole drainage: a retrospective cohort study. Neurosurg Rev. 2024;47(1):633. doi:10.1007/s10143-024-02752-y
40. Alenezi H, Lampmann T, Asoglu H, et al. Postoperative pneumocephalus as a predictor of chronic subdural hematoma recurrence: a retrospective cohort analysis. Eur J Trauma Emerg Surg. 2025;51(1):263. doi:10.1007/s00068-025-02939-y
41. Han MH, Ryu JI, Kim CH, Kim JM, Cheong JH, Yi HJ. Predictive factors for recurrence and clinical outcomes in patients with chronic subdural hematoma. J Neurosurg. 2017;127(5):1117–1125. doi:10.3171/2016.8.Jns16867
42. Hwang Y, Choi S, Kim YS, et al. Comparative analysis of safety and efficacy in subperiosteal versus subdural drainage after burr-hole trephination for chronic subdural hematoma. Clin Neurol Neurosurg. 2022;212(107068):107068. doi:10.1016/j.clineuro.2021.107068
43. Salem MM, Kuybu O, Nguyen Hoang A, et al. Middle meningeal artery embolization for chronic subdural hematoma: predictors of clinical and radiographic failure from 636 embolizations. Radiology. 2023;307(4):e222045. doi:10.1148/radiol.222045
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Fibrinogen/Albumin Ratio Index as an Independent Prognostic Biomarker for Patients with Combined Hepatocellular Cholangiocarcinoma After Surgery
Xu J, Li S, Feng Y, Zhang J, Peng Y, Wang X, Wang H
Cancer Management and Research 2022, 14:1795-1806
Published Date: 23 May 2022
Associations Between Morphological Phenotypes of COPD and Clinical Characteristics in Surgically Resected Patients with COPD and Concomitant Lung Cancer
Suzuki Y, Kitaguchi Y, Ueno F, Droma Y, Goto N, Kinjo T, Wada Y, Yasuo M, Hanaoka M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1443-1452
Published Date: 21 June 2022
Recurrent Hepatocellular Carcinoma: Patterns, Detection, Staging and Treatment
Papaconstantinou D, Tsilimigras DI, Pawlik TM
Journal of Hepatocellular Carcinoma 2022, 9:947-957
Published Date: 3 September 2022
Non-Locatable Internal Opening in Anal Fistula Associated with Acute Abscess and Its Definitive Management by Garg Protocol
Yagnik VD, Kaur B, Dawka S, Sohal A, Menon GR, Garg P
Clinical and Experimental Gastroenterology 2022, 15:189-198
Published Date: 26 September 2022
Analysis of Pathogenic Bacteria Distribution and Related Factors in Recurrent Acute Cholangitis
Li K, Hu X, Lu Q, Zhang H, Zhou J, Tian S, Zhou F
Infection and Drug Resistance 2023, 16:4729-4740
Published Date: 20 July 2023