Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Exploring the Potential of CSTF1 as a Prognostic Biomarker in Hepatocellular Carcinoma and Its Correlation with Immune Infiltration
Authors Aimaiti M, Maimaitituxun D, Yilihaer X, Kuerban T, Zhu J, Ainiwaer M, Jia Z, Abudourousuli A
Received 16 July 2025
Accepted for publication 26 November 2025
Published 11 December 2025 Volume 2025:12 Pages 2693—2707
DOI https://doi.org/10.2147/JHC.S552710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
Maimaitiming Aimaiti,1,* Dilimulati Maimaitituxun,2,* Xiaokaiti Yilihaer,2 Talifujiang Kuerban,3 Junling Zhu,4 Mieradilijiang Ainiwaer,5 Zhiqiang Jia,3 Ainiwaerjiang Abudourousuli4,6,7
1Department of Vascular and Endovascular Surgery, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China; 2Department of Surgical Oncology, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China; 3Department of Tumor Internal Medicine, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China; 4Department of Pathology, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China; 5Department of General Surgery, Xinjiang Kashi Uygur Medical Hospital, Xinjiang, Kashi, People’s Republic of China; 6Kashi Prefecture Cancer Research Institute, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China; 7Institute of Etiology and Metabolic Diseases in Pamir Plateau Area, Kashi University, Xinjinag, Kashi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiqiang Jia, Department of Tumor Internal Medicine, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China, Email [email protected] Ainiwaerjiang Abudourousuli, Department of Pathology, The First People’s Hospital of Kashi Prefecture, Xinjiang, Kashi, People’s Republic of China, Email [email protected]
Background: Hepatocellular carcinoma (HCC) is a aggressive cancer associated with high morbidity and mortality globally. Reliable biomarkers are urgently needed to enhance diagnostic accuracy and survival outcomes in patients with HCC. This study aimed to evaluate the prognostic value of cleavage stimulation factor subunit 1 (CSTF1) in HCC.
Methods: CSTF1 expression in different cancer types, including HCC, was analyzed using data from The Cancer Genome Atlas. Immunohistochemistry was performed to assess CSTF1 expression in clinical samples. Logistic regression analyses were used to evaluate associations between CSTF1 expression and the clinical characteristics of patients with HCC. Furthermore, Gene Ontology, Kyoto Encyclopedia of Genes and Genomes, and gene set enrichment analysis (GSEA) were performed to identify signaling pathways and biological functions linked to differentially expressed genes. The prognostic significance of CSTF1 in HCC was assessed via the Kaplan-Meier method and Cox univariate and multivariate analyses. Immune cell infiltration was investigated through single-sample GSEA and the CIBERSORT algorithm. Three nomograms were constructed to predict overall survival (OS), disease-specific survival (DSS), and progression free interval (PFI) rates at 1, 3, and 5 years after diagnosis.
Results: CSTF1 expression was elevated in HCC cases and closely correlated with multiple clinical features. Elevated CSTF1 expression was strongly associated with various cancer-related pathways and the immune microenvironment. The Kaplan-Meier analysis revealed that elevated CSTF1 expression predicts poorer prognostic outcomes in individuals with HCC. CSTF1 hypermethylation was also related to poor patient outcomes. The constructed nomograms for OS, DSS, and PFI achieved concordance indices of 0.631, 0.719 and 0.787, respectively.
Conclusion: These findings suggest that CSTF1 can serve as a novel prognostic biomarker for HCC. Evidence from immunohistochemistry and bioinformatics analyses supports CSTF1 as a prognostic indicator and a potential therapeutic target. This discovery could enhance diagnostic precision and improve survival outcomes for patients with HCC.
Keywords: hepatocellular carcinoma, CSTF1, prognostic biomarker, immunodulation, tumor microenvironment
Introduction
Hepatocellular carcinoma (HCC) is a major global health concern characterized by high incidence and mortality rates, imposing heavy burdens on patients and healthcare systems alike.1,2 Over 800,000 cases are reported annually worldwide, and China accounts for more than 400,000 new cases, underscoring the substantial health burden in the region.3,4 The 5-year survival rate among patients with HCC is approximately 20%.5 The complexity of HCC arises from various risk factors, including chronic hepatic inflammation, alcohol abuse, and metabolic disorders, which contribute to poor prognostic outcomes.6–8 Current diagnostic and therapeutic approaches, such as imaging techniques, liver transplantation, chemotherapy, and targeted therapy, have shown limited efficacy in advanced stages and variable treatment responses, often resulting in poor patient outcomes.9,10 Despite advances in targeted therapies and immunotherapy, the pronounced heterogeneity of HCC contributes to hinder treatment success, highlighting critical gaps in our current understanding of this malignancy.11 Consequently, identifying novel biomarkers is crucial to improve prognostic precision and guiding personalized therapeutic strategies for better management of HCC.
Emerging evidence identifies RNA binding proteins as master regulators of cancer-immune crosstalk.12 Among these, cleavage stimulation factor 1 (CSTF1) plays an essential role in RNA processing, particularly in the regulation of polyadenylation and its alternative processes.13 Previous research has shown that CSTF1 is strongly associated with the onset and progression of various diseases.14 For example, CSTF1 expression was notably elevated in patients with advanced Alzheimer’s disease, suggesting its involvement in neurodegenerative molecular mechanisms.15 Similarly, in abdominal aortic aneurysms, CSTF1 was shown to regulate cell-mediated immune processing, reinforcing its importance as a regulatory factor.16 Furthermore, CRISPR-based studies on transcription and 3′ end processing of the human U2 snRNA, identified CSTF1 among the key regulatory components.17 These findings indicate that CSTF1 not only participates in snRNA gene expression, but may also influence other RNA processing pathways.18 However, its biological function in HCC remains unclear, and further investigation may elucidate CSTF1’s role in HCC onset and progression.
In this study, we applied bioinformatics analyses using the Cancer Genome Atlas (TCGA) datasets and conducted immunohistochemistry to validate CSTF1 expression in clinical HCC samples. Our results demonstrate elevated CSTF1 expression in HCC—along with strong associations between CSTF1 levels, cancer-related signaling pathways, and the immune microenvironment—underscoring its relevance in HCC. These findings highlight CSTF1’s potential as a prognostic biomarker and possible role in guiding therapeutic strategies to enhance HCC clinical management. Overall, as a key RNA-processing regulator, CSTF1 warrants further investigation to provide new insights and approaches for HCC diagnosis and treatment.
Materials and Methods
Data Collection
Transcriptomic profiles (RNA-seq FPKM values) and clinicopathological data for 374 HCC cases, including 50 cases with paired adjacent tissues, were obtained from TCGA-LIHC cohort (https://portal.gdc.cancer.gov/). The dataset included clinical variables such as age, sex, TNM stage, pathological stage, adjacent tissue lymphocyte infiltration, vascular invasion, and alpha-fetoprotein levels. All methodologies adhered to the ethical standards of the Declaration of Helsinki, amended in 2013, ensuring the responsible use of the data. The design, experiment, and research involving human data in this study have total ethical approval granted by the Ethics Committee of the First People’s Hospital of Kashi Prefecture.
Tissue Microarray
The HCC tissue microarray was supplied by Shanghai Zhouli Bio. Co., Ltd. (ZL-LivHCC962), with ethical approval provided (approval number: LLSM-15-01-250227). It included 48 histologically confirmed HCC specimens and 48 adjacent noncancerous tissues, enabling detailed evaluation of CSTF1 expression across cancer microenvironments.
Immunohistochemistry and Assessment
Tumor specimens were fixed in 10% formalin, embedded in paraffin, and sectioned into 4–6-µm slices, which were mounted on charged slides. Following deparaffinization and rehydration, antigen retrieval was performed using microwave treatment in citrate buffer (pH 6.0) to optimize antibody binding. Sections were incubated overnight at 4°C with rabbit monoclonal anti-CSTF1 antibody (ABclonal, AB-2766657) diluted at 1:100, followed by incubation with a secondary antibody at room temperature for 30 min. DAB substrate staining and counterstaining with modified Mayer’s hematoxylin (5 min) enhanced CSTF1 visualization in the tissue microarray. Two independent pathologists, blinded to the study, evaluated the slides according to the 2022 WHO classification of HCC.19 A four-tier immunohistochemical scoring system was applied: 0 (negative, <1% positivity), 1+ (focal weak staining, 1–25%), 2+ (moderate multifocal, 26–50%), and 3+ (strong diffuse, >50%). Cohen’s kappa test was employed to assess interobserver agreement and validate scoring consistency.
Functional Enrichment Analysis
Based on average CSTF1 expression, TCGA-HCC data were stratified into high and low CSTF1 expression groups. Differentially expressed gene (DEG) analysis was performed using the limma package in R, applying a padj < 0.05 and |log2FC| > 1.5 threshold. Associations between CSTF1 expression and the 10 most significant DEGs were assessed via Spearman correlation test. Functional enrichment analyses of the DEGs, including Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) assessments, were conducted using the R package GOplot (v1.0.2). Gene set enrichment analysis (GSEA) was executed using the MSigDB v6.2 dataset obtained from the GSEA portal (http://software.broadinstitute.org/gsea/index.jsp). The clusterProfiler (v3.6.0) R package was also employed to facilitate GSEA. Comparisons between the high and low CSTF1 expression groups were iterated 10,000 times using c5.all.v7.0.symbols.gmt (GO) as the reference. Significant enrichment was defined by a false discovery rate q-value < 0.25 and padj < 0.05.
DNA Methylation and Mutation Analysis
The prognostic relevance of CSTF1 methylation levels was assessed through the MethSurv database, an online platform designed for multivariable survival analysis using DNA methylation data. Additionally, the genomic alternation profiles of CSTF1 were analyzed through the cBioPortal database (http://www.cbioportal.org/).
Survival Analysis
Survival outcomes were analyzed using the Kaplan–Meier method and Log rank test to compare survival curves among groups. Univariate and multivariate Cox regression analyses were conducted to determine the impact of clinical variables on patient outcomes. Prognostic factors with p < 0.05 in univariate analysis were included in multivariate analysis.
Analysis of Immune Cell Infiltration
Immune cell infiltration in HCC was analyzed using single-sample (ssGSEA) and CIBERSORT in the GSVA (v3.6) R package (http://www.bioconductor.org/packages/release/bioc/html/GSVA.html). This approach enabled the quantification of infiltration levels for 24 immune cell types based on gene expression data. Associations between CSTF1 expression and immune cell infiltration were tested via Spearman correlation and Wilcoxon rank-sum tests.
Development and Verification of the Nomograms
Three nomograms were constructed using independent prognostic variables identified by multivariate Cox regression analysis. Calibration plots were generated to evaluate nomogram performance, and the concordance index (C-index) quantified discriminative ability. The nomograms and calibration plots were generated using the R package RMS, with predictive accuracy evaluated via time-dependent receiver operating characteristic (ROC) curve analysis through the timeROC package.
Statistical Analysis
All statistical analyses were performed in R (v3.6.3). Associations between clinical pathological characteristics and CSTF1 expression were assessed through Wilcoxon rank-sum, chi-square, Fisher’s exact, and logistic regression tests. Survival rates in patients from TCGA were determined using the Kaplan–Meier method. Univariate and multivariate Cox proportional hazards models were constructed to evaluate relationships between clinical and genetic factors and overall survival (OS). P < 0.05 was considered statistically significant.
Results
CSTF1 is Significantly Overexpressed in HCC
We performed a pancancer analysis to evaluate CSTF1 expression levels across various cancer types using TCGA data (Figure 1A). CSTF1 expression was further examined in 16 cancers and their adjacent noncancerous tissues (Figure 1B). Results indicated that CSTF1 is significantly overexpressed in several cancers, including HCC. Analysis of TCGA-HCC samples, comprising 374 tumor and 50 adjacent noncancerous tissues, confirmed elevated CSTF1 expression in HCC (Figure 1C). Validation using 50 paired HCC samples produced similar results (Figure 1D). ROC curve analysis yielded an area under the curve (AUC) of 0.878 (Figure 1E). Immunohistochemical analysis also confirmed significant CSTF1 overexpression in HCC (Supplementary Figure 1A; Figure 1F–H). Adjacent noncancerous tissues displayed minimal punctate cytoplasmic staining, whereas HCC tissues exhibited diffuse cytoplasmic localization with limited nuclear or membranous staining (Supplementary Figure 1B and C). Collectively, these findings indicate that CSTF1 is significantly overexpressed in HCC.
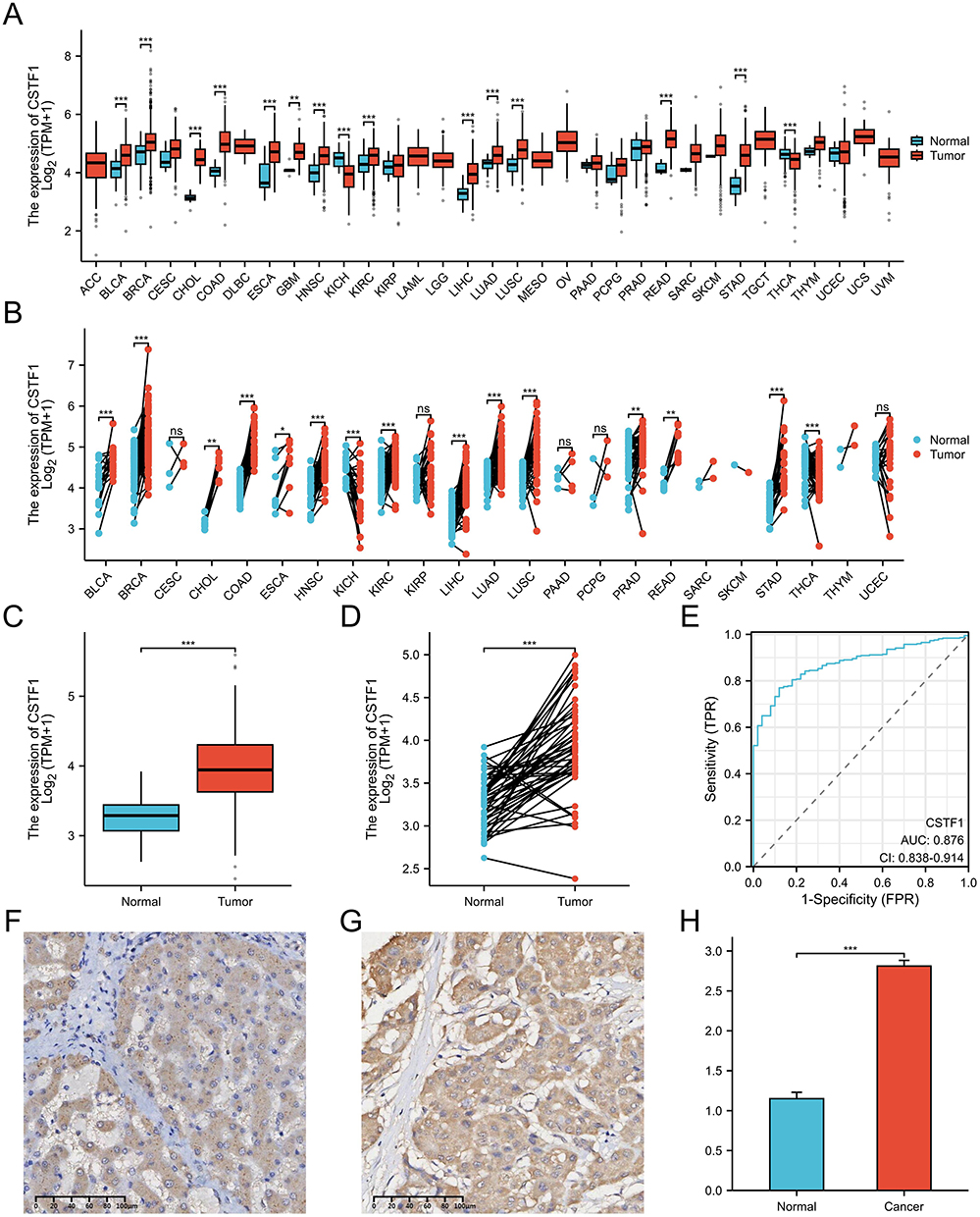 |
Figure 1 CSTF1 is overexpressed in HCC. (A) CSTF1 expression across various cancer types. (B) Comparison of CSTF1 expression in 16 paired cancer types. (C) CSTF1 expression in the TCGA-HCC dataset. (D) Comparison of CSTF1 expression between 50 HCC and adjacent noncancerous tissues. (E) ROC curve analysis of CSTF1 in HCC. (F) CSTF1 expression in adjacent noncancerous tissues (scale bar: 100 μm). (G) CSTF1 expression in HCC tissues (scale bar: 100 μm). (H) Statistical analysis of immunohistochemistry results (*P<0.05, **P<0.01, ***P<0.001). |
CSTF1 Expression is Associated with Various Clinical Features of HCC
The clinical characteristics of patients with HCC are summarized in Supplemental Table 1. We analyzed correlations between CSTF1 expression and various clinicopathological features. CSTF1 expression showed strong correlations with pathologic stage, pathologic T stage, weight, body mass index (BMI), and histological grade (Figure 2A–E). Logistic regression analysis confirmed the correlations between CSTF1 expression and two clinical variables (Table 1): patient weight (p = 0.032) and histological grade (p = 0.023). Analysis of the HCC tissue microarray also revealed associations between CSTF1 expression and pathologic T stage, as well as positive correlations with CD34 (R = 0.665, p < 0.001) and Ki-67 (R = 0.798, p < 0.001) expression (Supplementary Figure 1E–G). These findings show that CSTF1 expression is significantly associated with the clinical characteristics of patients with HCC.
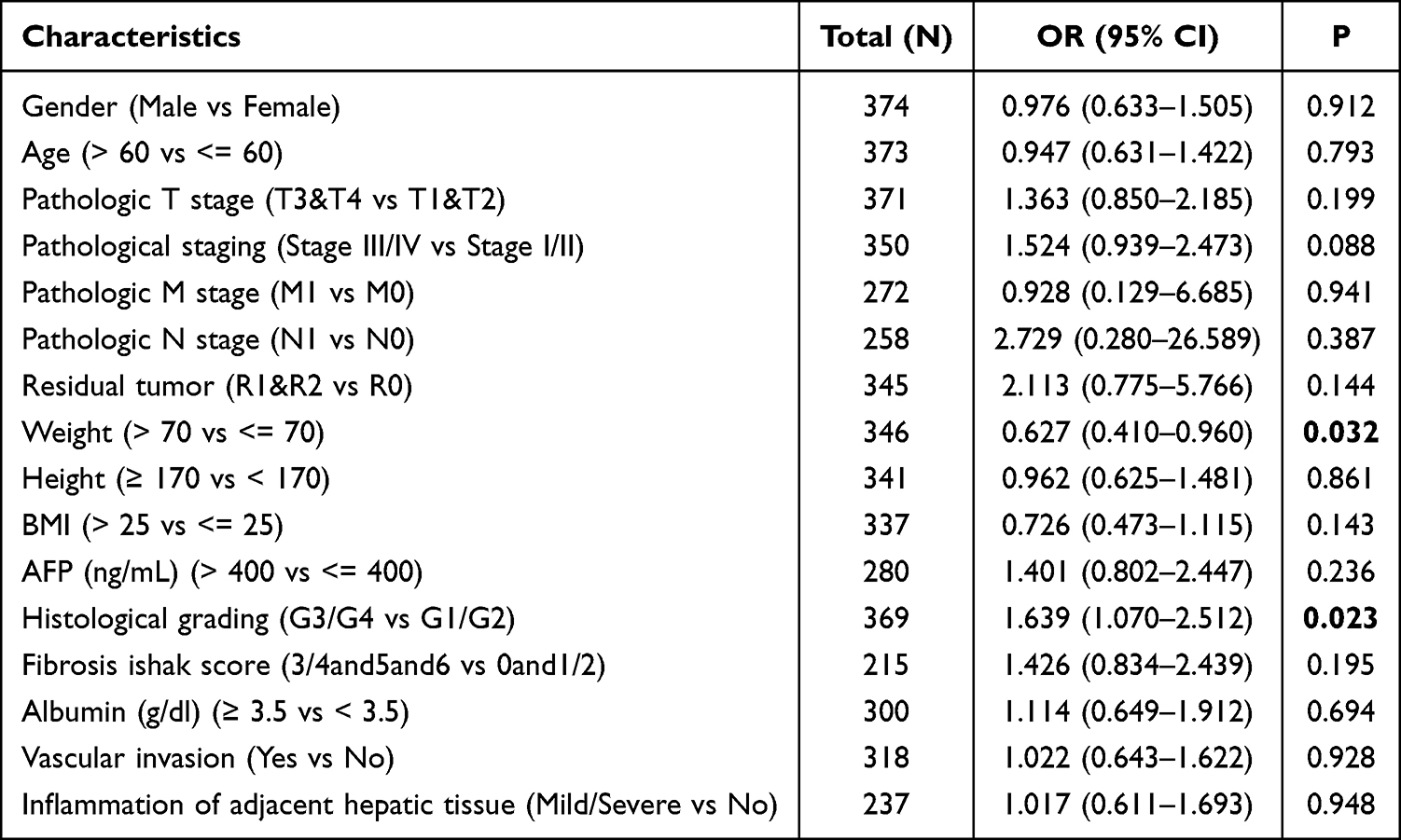 |
Table 1 Logistic Regression Analysis of CSTF1 in HCC |
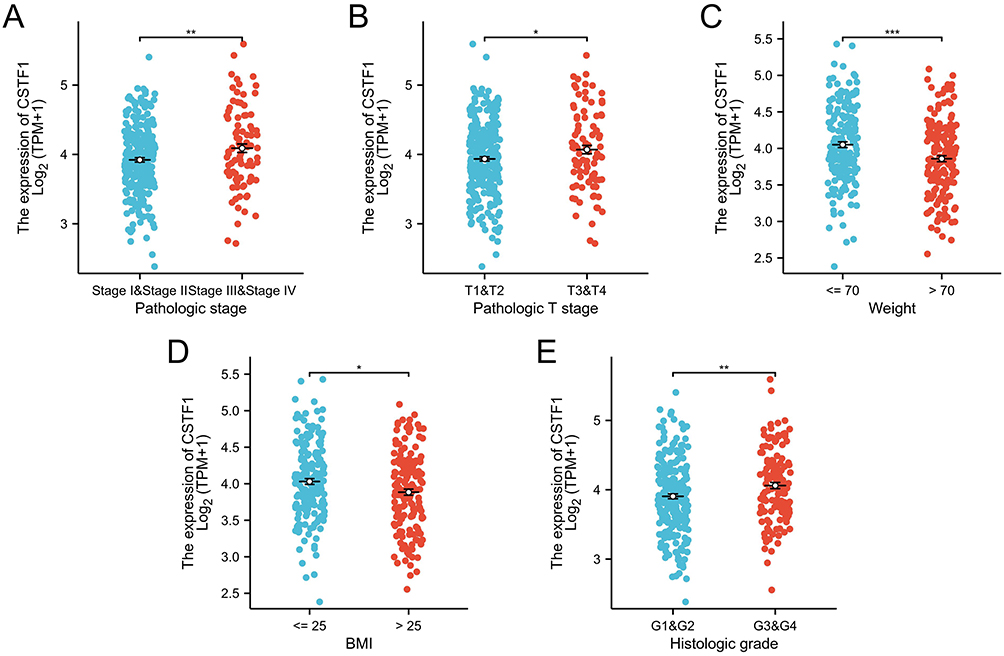 |
Figure 2 Association between CSTF1 expression levels and clinical features of HCC. (A) Pathologic stage. (B) Pathologic T stage. (C) Weight. (D) BMI. (E) Histologic grade (*P<0.05, **P<0.01, ***P<0.001). |
Functional Enrichment Analysis of CSTF1-Related DEGs in HCC
In total, 401 genes displayed differential expression levels between the CSTF1 high and low expression groups. Among these, 286 (71.4%) were upregulated and 115 (28.6%) were downregulated, based on padj < 0.05 and |log2-FC| > 1.5 (Figure 3A). Relationships between CSTF1 and the top 10 DEGs (WIF1, HMGA2, CHP2, WNT7B, SAA2, OLIG3, PEBP4, SAA1, KLK3, and HAMP) are presented in Figure 3B. Enrichment analysis demonstrated notable enrichment of the DEGs in several GO biological processes, cellular components, and molecular functions as well as in KEGG signaling pathways. These included response to copper ion stress, cell body membrane, receptor–ligand activity, and neuroactive ligand–receptor interactions (Figure 3C–F). These findings emphasize the unique gene expression profiles linked to CSTF1 levels, indicating that the identified DEGs are involved in biological processes relevant to HCC.
 |
Figure 3 Identification and functional enrichment analysis of CSTF1-related DEGs. (A) Volcano plot of DEGs. (B) Heatmap showing correlations among the top 10 DEGs and CSTF1. (C) GO biological process (BP) term analysis. (D) GO cellular component (CC) term analysis. (E) GO molecular function (MF) term analysis. (F) KEGG pathway analysis (*P<0.05, **P<0.01, ***P<0.001). |
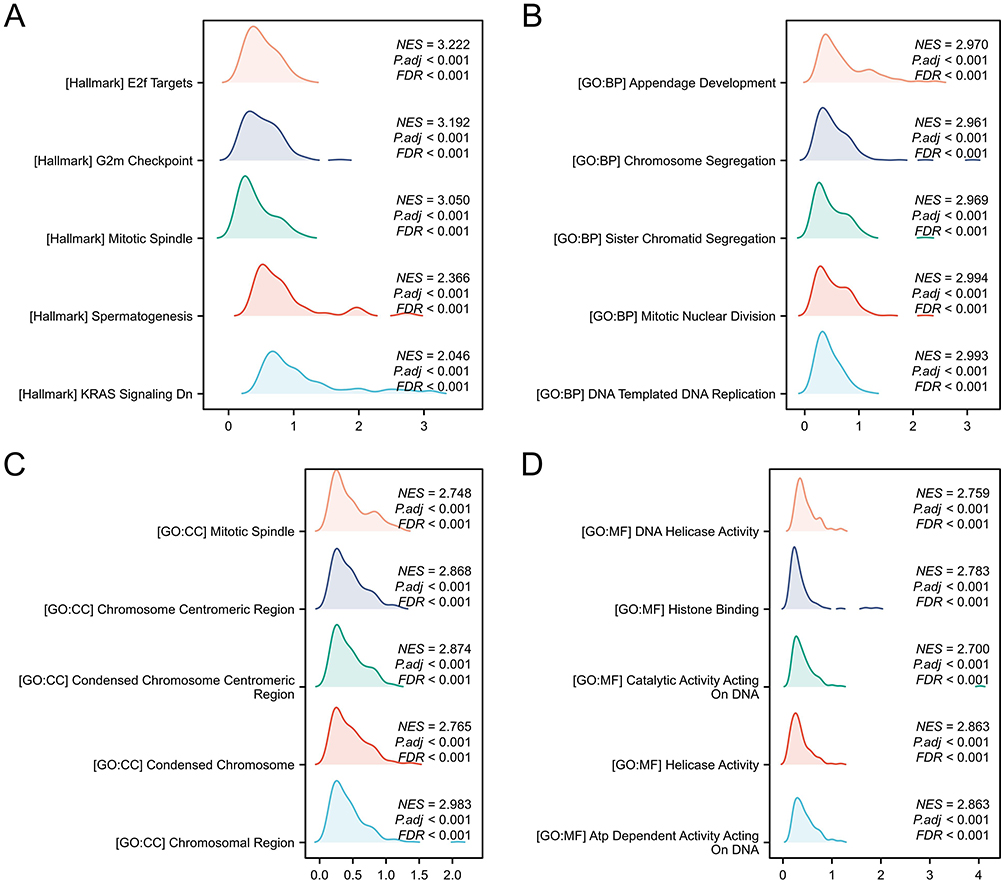 |
Figure 4 GSEA of CSTF1-associated genes. (A) Hallmark gene sets. (B) GO BP term gene sets. (C) The GO CC term gene sets. (D) The GO MF term gene sets. |
GSEA of CSTF1-Related DEGs in HCC
We conducted GSEA analysis to further assess CSTF1-related biological functions in HCC. Analysis of hallmark gene sets identified enrichment in E2F targets, G2M checkpoints, mitotic spindle formation, spermatogenesis, and KRAS signaling (Figure 4A). Biological processes included appendage development, chromosome segregation, sister chromatid segregation, mitotic nuclear division, and DNA-templated DNA replication (Figure 4B). Enriched cellular components comprised the mitotic spindle, chromosome centrometre region, condensed chromosome region, and chromosomal region (Figure 4C). Molecular function enrichment included DNA helicase activity, histone binding, catalytic activity acting on DNA, and ATP-dependent activity acting on DNA (Figure 4D). These findings emphasize the distinct gene expression profiles linked to CSTF1 and the involvement of DEGs in key HCC-associated molecular pathways.
Analyses of CSTF1 Methylation and Mutation in HCC
To investigate the epigenetic regulation of CSTF1, the correlations between CSTF1 expression and methylation status were analyzed using the MethSurv dataset (Figure 5A). Five methylation sites—cg19818007, cg13008301, cg05002314, cg10922808, and cg23597562—were identified as markers of poor prognosis in patients with HCC (Figure 5B–F). Hypomethylation at these sites suggests reduced regulatory control of CSTF1 expression, potentially contributing to tumorigenesis and poor prognosis outcomes. Mutation analysis using the cBioportal database (Supplementary Figure 2A) revealed a 1% CSTF1 mutation rate in HCC, with variable mutation patterns across datasets (Supplementary Figure 2B). No clear correlations were observed between CSTF1 mutation status and patient prognostic outcomes (Supplementary Figure 2C–E). These results indicate that CSTF1 methylation status may play an important role in HCC progression and prognosis.
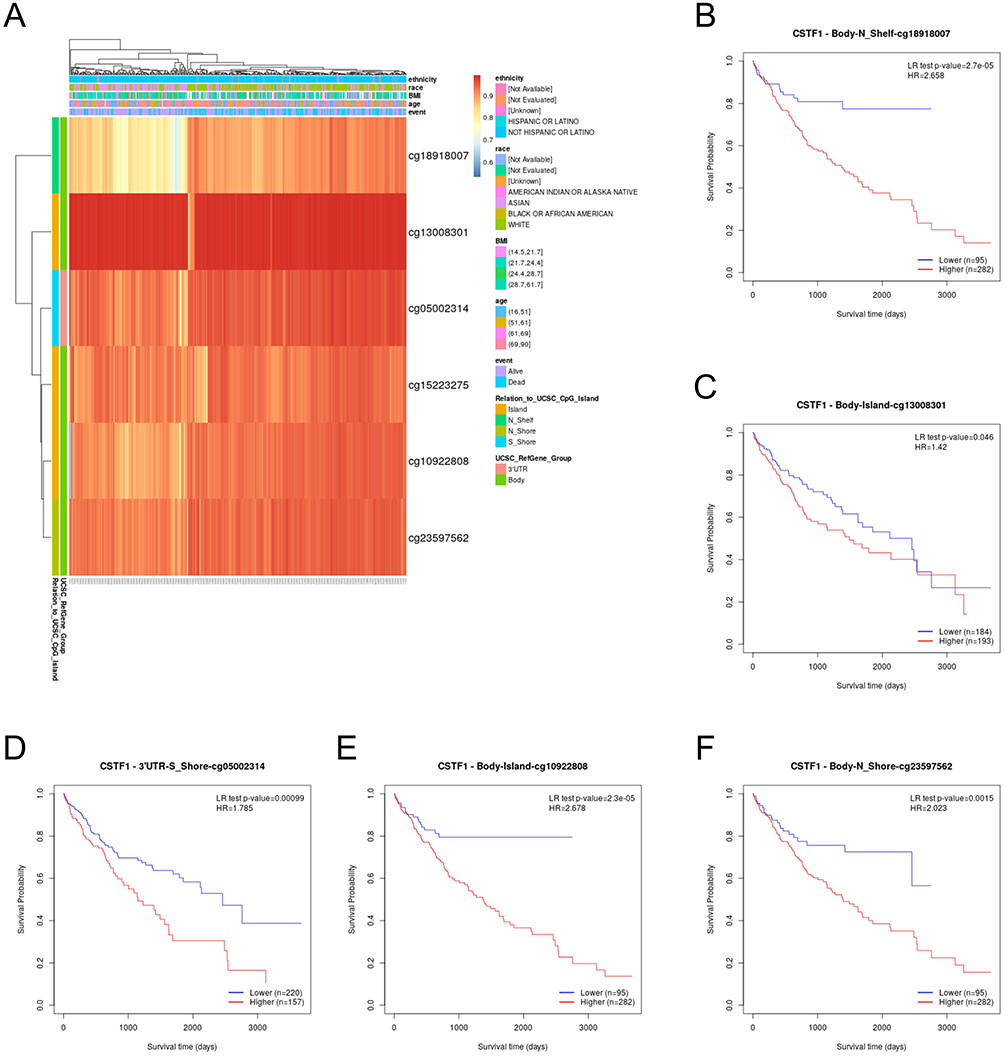 |
Figure 5 Methylation analysis and prognostic correlations of CSTF1 in HCC. (A) Correlation between CSTF1 expression and methylation levels. (B–F) Kaplan–Meier analyses of five CSTF1 methylation loci. |
Associations Between CSTF1 Expression Levels and Immune Cell Infiltration
HCC is known for its strong immunogenicity, closely linked to viral infections and a proinflammatory microenvironment.20 To explore the relationship between CSTF1 expression and immune cell infiltration, we conducted ssGSEA and assessed correlations using Spearman’s test (Figure 6A). Analysis revealed significant negative correlations between CSTF1 expression and the infiltration levels of cytotoxic cells, dendritic cells (DCs), and B cells (p < 0.001; Figure 6B–G). These immune cell populations are essential for antitumor immunity, and their reduced abundance suggests that elevated CSTF1 expression suppresses immune surveillance in HCC. Conversely, CSTF1 expression showed positive correlations with infiltration levels of T helper (TH and TH2) cells and central memory T cells (p < 0.001; Supplementary Figure 3). Immune cell infiltration was also analyzed using CIBERSORT (Supplementary Figure 4A). Results revealed negative associations between CSTF1 and regulatory T cells and positive associations with activated DCs and monocytes (Supplementary Figure 4B–D). These findings indicate that CSTF1 may modulate the tumor microenvironment by suppressing cytotoxic immune cell populations while promoting those involved in immune tolerance, thereby facilitating immune evasion and tumor progression in HCC.
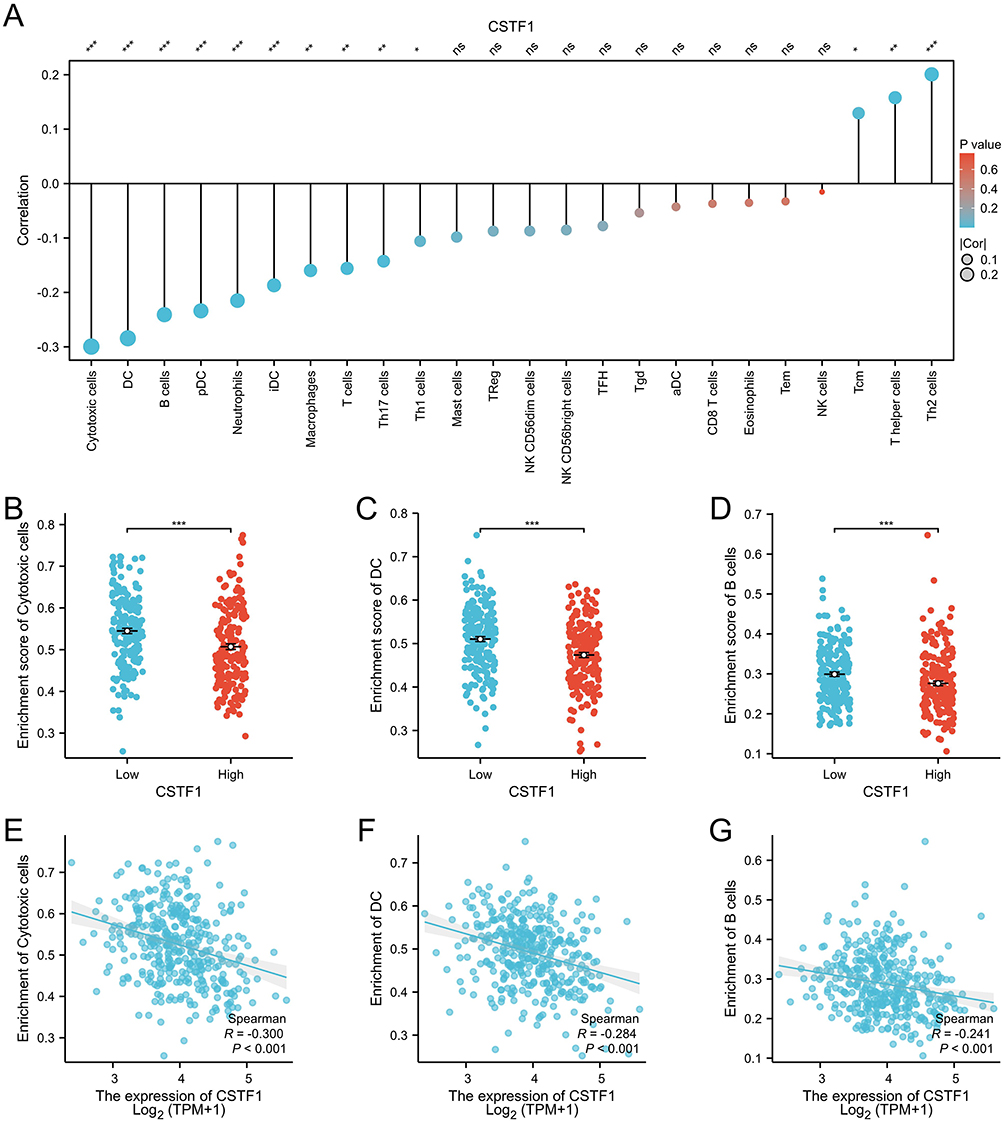 |
Figure 6 CSTF1 expression associated with immune cell infiltration in the tumor microenvironment. (A) Relationships between CSTF1 expression and immune cell types. (B) Differences in cytotoxic cell infiltration between the high and low CSTF1 expression groups. (C) Correlation between CSTF1 expression and DCs. (D) Differences in B-cell infiltration levels between the high and low CSTF1 expression groups. (E) Correlation between CSTF1 expression and cytotoxic cells. (F) Correlation between CSTF1 expression and DCs. (G) Correlation between CSTF1 expression and B cells (*P<0.05, **P<0.01, ***P<0.001). |
Prognostic Implications of CSTF1 Expression in HCC Patients
The prognostic value of CSTF1 expression was investigated using Kaplan–Meier survival curves. Elevated CSTF1 expression was significantly correlated with reduced OS (p = 0.008), DSS (p = 0.011), and PFI (p = 0.007; Figure 7A–C). These findings suggest that elevated CSTF1 expression contributes to more aggressive tumor behavior and poorer outcomes in HCC cases. To examine the broader impact of CSTF1 expression across cancers, we analyzed its association with OS in other malignancies. High CSTF1 expression was similarly correlated with poor survival outcomes in patients with adrenocortical carcinoma, kidney renal cell carcinoma, and endometrial carcinoma (Supplementary Figure 5A–C). However, ROC curve analyses indicated only moderate predictive performance in these cancers, with AUC values of 0.5–0.7 (Supplementary Figure 5D and E). These differences highlight CSTF1’s stronger prognostic relevance in HCC. Additionally, survival analysis stratified by clinicopathological variables showed that elevated CSTF1 expression consistently predicted poorer outcomes across several patient subgroups, including age > 60 years, sex, weight < 70 kg, pathological stage III and IV, pathological T stage T3 and T4, pathological M stage M0, pathologic N stage N0, BMI < 25, and fibrosis Ishak scores of 3/4 and 5/6 (p < 0.05; Supplementary Figure 6A–I). These findings reinforce CSTF1’s role as a key prognostic biomarker across clinical contexts in HCC.
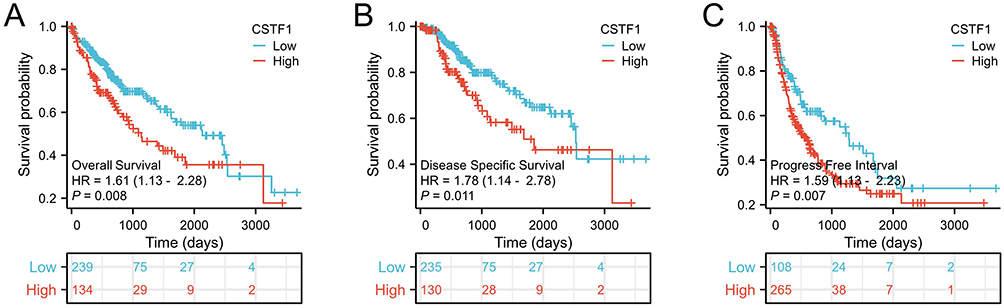 |
Figure 7 CSTF1 expression linked to reduced survival rates in patients with HCC. (A) OS, (B) DSI. (C) PFI. |
Creation and Assessment of Prognostic Nomograms
To provide clinicians with reliable and individualized prognostic tools for HCC, we developed three nomograms incorporating independent prognostic factors, particularly tumor status. These nomograms assigned higher total points to factors associated with poorer survival, thus visually illustrating risk based on clinical and molecular features. Calibration curves revealed strong agreement between predicted rates and observed OS rates, with a C-index of 0.631 [95% confidence interval (CI) = 0.599–0.663; Figure 8A and B]; DSS, with a C-index of 0.719 (95% CI = 0.687–0.752; Figure 8C and D); and PFI, with a C-index of 0.787 (95% CI = 0.770–0.805; Figure 8E and F). By integrating predictors into a composite score, these nomograms may help optimize treatment planning and guide personalized follow-up strategies for patients with HCC. Cox univariate analysis identified pathologic stage, pathologic T stage (p < 0.001), tumor status (p < 0.001), and CSTF1 expression (p = 0.007) as significant OS predictors (Supplementary Table 2). Cox univariate–multivariate analysis was also performed for DSS and PFI, as shown in Supplementary Tables 3 and 4. Overall, these results suggest that CSTF1 functions as a risk marker, with its prognostic influence likely mediated by tumor status and progression.
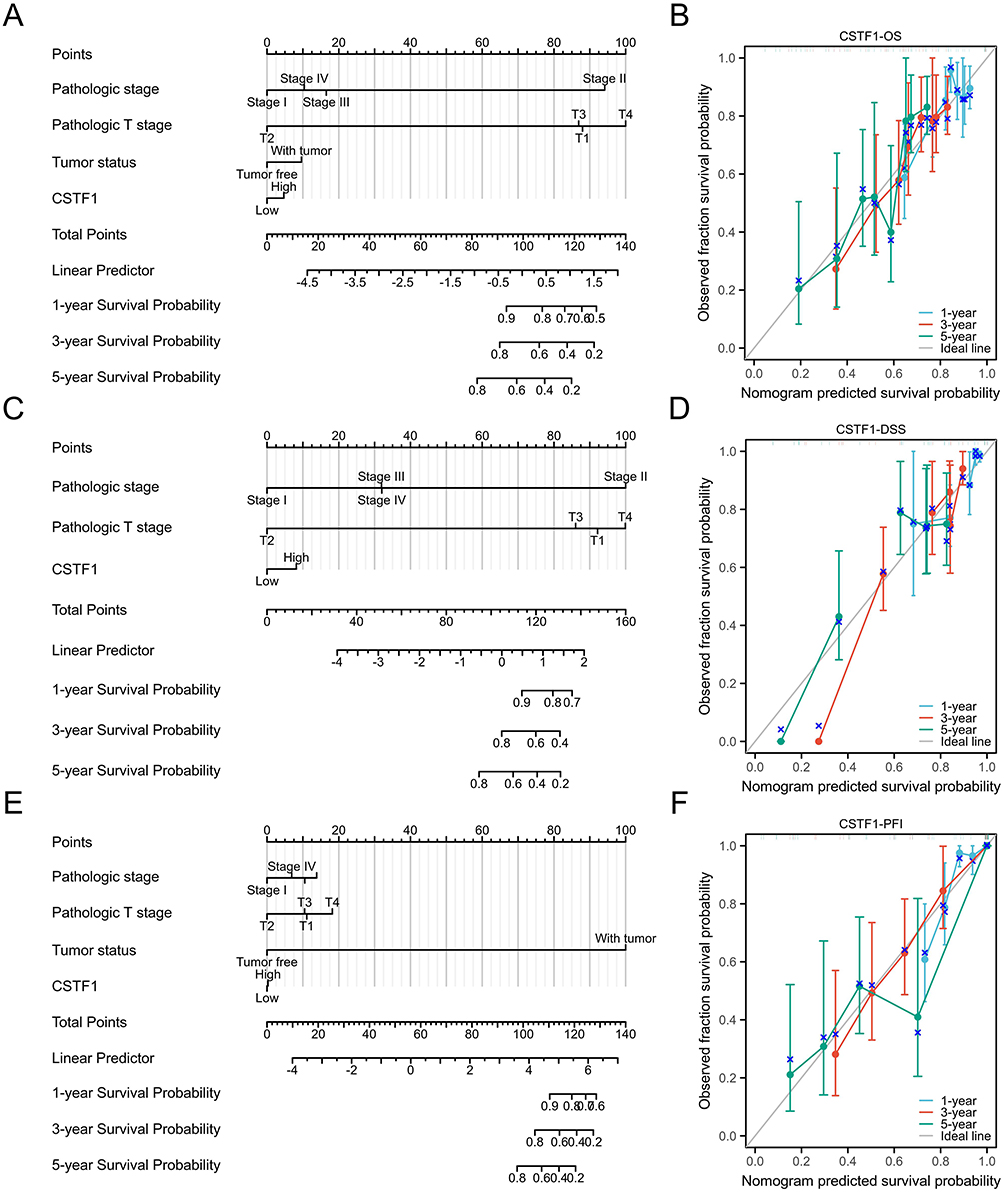 |
Figure 8 Nomograms and calibration curves predicting HCC survival rates at 1, 3, and 5 years. (A) Nomogram predicting 1-, 3-, and 5-year OS in patients with HCC. (B) Calibration curve of the OS nomogram. (C) Nomogram for predicting 1-, 3-, and 5-year DSS in patients with HCC. (D) Calibration curve of the DSS nomogram. (E) Nomogram predicting 1-, 3-, and 5-year PFI in patients with HCC. (F) Calibration curve of the PFI nomogram. |
Discussion
Hepatocellular carcinoma (HCC), an aggressive and highly malignant tumor, exhibits alarmingly high global mortality rates, posing a major public health concern.21 The development of HCC is linked to multiple factors, including chronic viral hepatitis, liver cirrhosis, and metabolic syndrome.22 Current treatment strategies for HCC, although beneficial to some extent, have substantial limitations, particularly in advanced-stage cases, where therapeutic options become increasingly scarce and less effective.23 This situation underscores the urgent need to identify novel biomarkers that enhance prognostic precision and improve patient survival.24
As a key regulator of RNA processing, particularly in polyadenylation and alternative polyadenylation, interest in CSTF1 has increased across various diseases.25 Elevated CSTF1 expression has been observed in the peripheral blood of patients with advanced Alzheimer’s disease—where it showed a positive correlation with regulatory factors such as CPSF1, WDR33, and CPSF6—indicating its potential involvement in neurodegenerative diseases.26 Furthermore, research has highlighted the role of CSTF1 in abdominal aortic aneurysm progression, showing that it modulates cell-mediated immune responses by regulating miRNA and lncRNA networks.27 These findings indicate that CSTF1 extends beyond post-transcriptional modification to broader biological functions. However, the mechanisms underlying CSTF1-related activity in HCC and other cancers remain unclear. The current study aimed to identify potential biomarkers for HCC using bioinformatics analyses of TCGA data and clinical validation via immunohistochemistry. Our findings demonstrate significantly increased CSTF1 gene expression in patients with HCC (p < 0.01), suggesting that CSTF1 overexpression contributes to disease development and pathogenesis.
The elevated CSTF1 expression observed in HCC implies its potential involvement in tumorigenesis through the modulation of key oncogenic pathways. Our study also reveals close correlations between CSTF1 expression and activation of multiple cancer-related pathways, including responses to copper ion stress, receptor–ligand activity, E2F targets, and G2M checkpoints. Elucidating CSTF1’s precise regulatory role in these pathways could provide valuable insights into the biological mechanisms underlying HCC progression and prognosis.
Research on triple-negative gastrointestinal stromal tumors has revealed that CSTF1 may cooperate with other driver mutations to influence tumor development.28 These mutations include alterations in the RAS/RAF/MAPK pathway and mutations in genes such as TP53 and FGFR.29 In the present study, we identified five methylation sites in the CSTF1 promoter region that could affect HCC patient prognosis; however, mutation analyses showed no clear associations between CSTF1 mutation rates and patient outcomes.
Previous studies have demonstrated that the tumor microenvironment significantly impacts cancer progression and clinical outcomes.30 Our analysis identified a strong association between CSTF1 expression and the immune microenvironment in HCC, particularly regarding cytotoxic cells, DCs, and B cells (p < 0.05). Assessing CSTF1 expression within diverse immune microenvironments and its prognostic impact could yield important insights for personalized therapies. The link between CSTF1 and immune regulation is particularly noteworthy as it underscores that CSTF1 may shape immune responses in HCC. Consequently, identifying CSTF1 as a modulator of tumor–immune interactions could advance the development of improved immunotherapeutic strategies for HCC management.
This study also found a significant association between CSTF1 expression and patient survival, with high CSTF1 levels correlating with reduced survival outcomes (p < 0.01). Moreover, analyses across HCC subtypes revealed that CSTF1 expression affects multiple patient subgroups. Additional research is required to clarify how CSTF1 affects survival and to determine its value as an independent prognostic predictor. Examining CSTF1 expression across different survival groups may provide valuable information for clinical decision-making.
The limitations of this study include the reliance on bioinformatics analysis based on TCGA data without in vitro or in vivo validation. Although clinical validation was performed, the sample size remained small. Despite these limitations, our findings indicate that high CSTF1 expression in HCC is significantly associated with poor prognosis, supporting CSTF1’s potential as a prognostic biomarker. Future research should incorporate biological validation, expand patient cohorts, and conduct further clinical analyses to confirm CSTF1’s role and clinical applicability in HCC.
Conclusion
These results support the hypothesis that CSTF1 functions as a novel prognostic indicator and a promising molecular target for therapeutic intervention in HCC. Further studies should confirm these observations and elucidate the mechanistic pathways though which CSTF1 contributes to HCC progression.
Acknowledgments
We would like to thank the editor, the reviewers and general staff of the journal of hepatocellular carcinoma.
Funding
Sponsored by the Natural Science Foundation of Xinjiang Uygur Autonomous Region, number 2023D01F12. The State Key Laboratory of Pathogenesis, Prevention, Treatment of Central Asian High Incidence Diseases Fund, number SKL-HIDCA-2024-KY3. Kashgar Prefecture Science and Technology Plan Program, number KS2024022. Open research grant from the Institute of Etiology and Metabolic Diseases in Pamir Plateau Area, Kashi University, number: YXY2025ZD05. “Tianshan Talent” high level Medical and Health Personnel Training Program, number: TSYC202401B223. Xinjiang Uygur Autonomous Region Health Science and Technology Program, number: 2025001CGZHYDXM653124504.
Disclosure
The authors declare that they have no competing interests in this paper.
References
1. Sankar K, Gong J, Osipov A, et al. Recent advances in the management of hepatocellular carcinoma. Clin Mol Hepatol. 2023;30(1):1–15. doi:10.3350/cmh.2023.0125
2. Chen T, Hsiao S, Chen Y, et al. Increased prevalence but decreased survival of nonviral hepatocellular carcinoma compared to viral hepatocellular carcinoma in recent ten years. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-59668-2
3. Zheng S, Chan SW, Liu F, et al. Hepatocellular carcinoma: current drug therapeutic status, advances and challenges. Cancers. 2024;16(8):1582. doi:10.3390/cancers16081582
4. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
5. Luo X, He X, Zhang X, et al. Hepatocellular carcinoma: signaling pathways, targeted therapy, and immunotherapy. MedComm. 2024;5(2). doi:10.1002/mco2.474
6. Fu Y, Maccioni L, Wang XW, Greten TF, Gao B. Alcohol-associated liver cancer. Hepatology. 2024;80(6):1462–1479. doi:10.1097/HEP.0000000000000890
7. Ayares G, Idalsoaga F, Díaz LA, Arnold J, Arab JP. Current medical treatment for alcohol-associated liver disease. J Clin Exp Hepatol. 2022;12(5):1333–1348. doi:10.1016/j.jceh.2022.02.001
8. Provera A, Vecchio C, Sheferaw AN, et al. From masld to hcc: what’s in the middle? Heliyon. 2024;10(15):e35338. doi:10.1016/j.heliyon.2024.e35338
9. Tang J, Zhao D. Current status of liver transplantation for human immunodeficiency virus-infected patients in mainland China. World J Gastroenterol. 2024;30(14):1958–1962. doi:10.3748/wjg.v30.i14.1958
10. Oura K, Morishita A, Tani J, Masaki T. Tumor immune microenvironment and immunosuppressive therapy in hepatocellular carcinoma: a review. Int J Mol Sci. 2021;22(11):5801. doi:10.3390/ijms22115801
11. Childs A, Aidoo-Micah G, Maini MK, Meyer T. Immunotherapy for hepatocellular carcinoma. JHEP Rep. 2024;6(10):101130. doi:10.1016/j.jhepr.2024.101130
12. Jungfleisch J, Gebauer F. Rna-binding proteins as therapeutic targets in cancer. RNA Biol. 2025;22(1):1–8. doi:10.1080/15476286.2025.2470511
13. Grozdanov PN, Li J, Yu P, Yan W, Macdonald CC. Cstf2t regulates expression of histones and histone‐like proteins in male germ cells. Andrology. 2018;6(4):605–615. doi:10.1111/andr.12488
14. Ren F, Zhang N, Zhang L, Miller E, Pu JJ. Alternative polyadenylation: a new frontier in post transcriptional regulation. Biomark Res. 2020;8(1). doi:10.1186/s40364-020-00249-6
15. Garofalo M, Pandini C, Bordoni M, et al. Alzheimer’s, Parkinson’s disease and amyotrophic lateral sclerosis gene expression patterns divergence reveals different grade of rna metabolism involvement. Int J Mol Sci. 2020;21(24):9500. doi:10.3390/ijms21249500
16. Zhang H, Bian C, Tu S, et al. Construction of the circrna-mirna-mrna regulatory network of an abdominal aortic aneurysm to explore its potential pathogenesis. Dis Markers. 2021;2021:1–17. doi:10.1155/2021/9916881
17. Guiro J, Fagbemi M, Tellier M, et al. Capture of the human u2 snrna genes expands the repertoire of associated factors. Biomolecules. 2022;12(5):704. doi:10.3390/biom12050704
18. Shankarling GS, Macdonald CC. Polyadenylation site-specific differences in the activity of the neuronal βcstf-64 protein in pc-12 cells. Gene. 2013;529(2):220–227. doi:10.1016/j.gene.2013.08.007
19. Kim H, Jang M, Park YN. Histopathological variants of hepatocellular carcinomas: an update according to the 5th edition of the who classification of digestive system tumors. J Liver Cancer. 2020;20(1):17–24. doi:10.17998/jlc.20.1.17
20. Fu Y, Guo X, Sun L, et al. Exploring the role of the immune microenvironment in hepatocellular carcinoma: implications for immunotherapy and drug resistance. Elife. 2024:13. doi:10.7554/eLife.95009
21. Huang W, You L, Yang S, Liu D, Liu M, Fan X. S-1 for treatment of advanced hepatocellular carcinoma: a systematic review of the literature. Contemp Oncol. 2017;21(1):16–20. doi:10.5114/wo.2017.66653
22. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol. 2019;16(10):589–604. doi:10.1038/s41575-019-0186-y
23. Singal A, Ravi S. Regorafenib: an evidence-based review of its potential in patients with advanced liver cancer. Core Evidence. 2014;81. doi:10.2147/CE.S48626
24. Kapoor A, Bayat Mokhtari R, Sonti SS, et al. Circulatory agrin serves as a prognostic indicator for hepatocellular carcinoma. Cancers. 2024;16(15):2719. doi:10.3390/cancers16152719
25. Monarez RR, Macdonald CC, Dass B. Polyadenylation proteins cstf-64 and τcstf-64 exhibit differential binding affinities for rna polymers. Biochem J. 2007;401(3):651–658. doi:10.1042/BJ20061097
26. Patel R, Brophy C, Hickling M, Neve J, Furger A. Alternative cleavage and polyadenylation of genes associated with protein turnover and mitochondrial function are deregulated in Parkinson’s, Alzheimer’s and als disease. BMC Med Genomics. 2019;12(1). doi:10.1186/s12920-019-0509-4
27. Wu Z, Yu W, Luo J, et al. Comprehensive transcriptomic analysis unveils macrophage-associated genes for establishing an abdominal aortic aneurysm diagnostic model and molecular therapeutic framework. Eur J Med Res. 2024;29(1). doi:10.1186/s40001-024-01900-w
28. Denu RA, Joseph CP, Urquiola ES, et al. Utility of clinical next generation sequencing tests in kit/pdgfra/sdh wild-type gastrointestinal stromal tumors. Cancers. 2024;16(9):1707. doi:10.3390/cancers16091707
29. Tornesello ML, Buonaguro L, Izzo F, Buonaguro FM. Molecular alterations in hepatocellular carcinoma associated with hepatitis b and hepatitis c infections. Oncotarget. 2016;7(18):25087–25102. doi:10.18632/oncotarget.7837
30. Xiao Y, Yu D. Tumor microenvironment as a therapeutic target in cancer. Pharmacol Ther. 2021;221:107753. doi:10.1016/j.pharmthera.2020.107753
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decaprenyl Diphosphate Synthase Subunit 1 (PDSS1): A Potential Prognostic Biomarker and Immunotherapy-Target for Hepatocellular Carcinoma
Yang Y, Li J, Tang M, Nie B, Huang W
Cancer Management and Research 2022, 14:1627-1639
Published Date: 3 May 2022
Overexpression of TREM1 is Associated with the Immune-Suppressive Microenvironment and Unfavorable Prognosis in Pan-Cancer
Zhou X, Lin K, Fu L, Liu F, Lin H, Chen Y, Zhuang B, Liang H, Deng Q, Wang Z, Chen W, Luo J, Cao J, Li P
Journal of Inflammation Research 2023, 16:1375-1391
Published Date: 27 March 2023
Promising Novel Biomarkers for Hepatocellular Carcinoma: Diagnostic and Prognostic Insights
Yu J, Park R, Kim R
Journal of Hepatocellular Carcinoma 2023, 10:1105-1127
Published Date: 18 July 2023
Development and Validation of a Propionate Metabolism-Related Gene Signature for Prognostic Prediction of Hepatocellular Carcinoma
Xiao J, Wang J, Zhou C, Luo J
Journal of Hepatocellular Carcinoma 2023, 10:1673-1687
Published Date: 2 October 2023
Chronic Inflammatory and Immune Microenvironment Promote Hepatocellular Carcinoma Evolution
Chen S, Zhang L, Chen Y, Zhang X, Ma Y
Journal of Inflammation Research 2023, 16:5287-5298
Published Date: 15 November 2023