")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Promising Novel Biomarkers for Hepatocellular Carcinoma: Diagnostic and Prognostic Insights
Received 1 April 2023
Accepted for publication 7 July 2023
Published 18 July 2023 Volume 2023:10 Pages 1105—1127
DOI https://doi.org/10.2147/JHC.S341195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Gerber
James Yu,1 Robin Park,1 Richard Kim2
1Division of Hematology and Medical Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA; 2Department of Gastrointestinal Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA
Correspondence: Richard Kim, Department of Gastrointestinal Oncology, H. Lee Moffitt Cancer Center and Research Institute, CSB 8TH 8173, 12902 USF Magnolia Drive, Tampa, FL, 33612, USA, Tel +1 813 745 1813, Fax +1 813 449 6749, Email [email protected]
Abstract: The systemic therapy landscape for hepatocellular carcinoma is rapidly evolving, as the recent approvals of checkpoint inhibitor-based regimens such as atezolizumab–bevacizumab and durvalumab–tremelimumab in advanced disease have led to an expanding therapeutic armamentarium. The development of biomarkers, however, has not kept up with the approvals of new agents. Nevertheless, biomarker research for hepatocellular carcinoma has recently been growing at a rapid pace. The most active areas of research are biomarkers for early detection and screening, accurate prognostication, and detection of minimal residual disease following curative intent therapies, and, perhaps most importantly, predictive markers to guide selection and sequencing of the individual agents, including tyrosine kinase inhibitors and immunotherapy. In this review, we briefly summarize the recent developments in systemic therapeutics for hepatocellular carcinoma, introduce the key completed and ongoing prospective and retrospective studies evaluating diagnostic, prognostic, and predictive biomarkers with high clinical relevance, highlight several potentially important areas of future research, and share our insights for each biomarker.
Keywords: hepatocellular carcinoma, diagnostic biomarker, prognostic biomarker, predictive biomarker, novel biomarker
Introduction
Hepatocellular carcinoma (HCC) is the most common liver primary cancer and the second leading cause of cancer-associated death worldwide.1 Although there are established HCC surveillance systems, more than 50% of HCC patients present with advanced disease, which limits them from receiving curative treatment such as surgical resection or liver transplantation (LT).2,3 Alpha-fetoprotein (AFP) is the most widely used biomarker for HCC surveillance, in conjunction with ultrasound (US).4,5 However, the exact role of AFP in surveillance is somewhat controversial. No other biomarkers have been incorporated into daily practice for HCC surveillance in the major guidelines.4,5 There is an unmet need for the development of biomarkers for the early detection of HCC.
Since 2008, there have been remarkable improvements in novel systemic therapy for HCC. During this period, more than a dozen therapies, predominantly tyrosine kinase inhibitors (TKIs), anti-angiogenesis agents, and immune checkpoint inhibitors (CPIs), have been approved as first or later-line therapies, and have significantly extended survival in advanced HCC. However, only around 27% of HCC patients respond to the atezolizumab–bevacizumab combination, which is one of the standard first-line therapies for HCC at the time of publication.6 Also, emerging data have indicated that the clinical benefit of HCC from CPIs and TKIs may be dependent on the etiology of HCC.7–9 These heterogeneous responses to each treatment imply that finding novel predictive biomarkers could potentially elucidate which subgroup of HCC can achieve maximal clinical benefit from specific novel therapies.
Along with this dynamic development of new agents in HCC, a huge number of studies have been performed that propose potential predictive biomarkers for each novel agent. However, except for AFP for ramucirumab, most of those proposed biomarkers have not been used in clinical practice.10 Therefore, there is an unmet necessity to develop and verify better predictive biomarkers for each novel therapy.
In recent years, there have been an emerging developments in omics technology, such as cell-free DNA (cfDNA), including circulating tumor DNA (ctDNA), micro-RNA (miRNA), and circulating tumor cells (CTCs), which can potentially lead to novel diagnostic, prognostic, and predictive biomarkers in HCC. In this review, we discuss the current evidence on early diagnostic, prognostic, and predictive HCC biomarkers, share our insights, and present a comparative discussion for each novel biomarker.
Biomarkers for Hepatocellular Carcinoma Surveillance and Early Detection
Phase of Cancer Biomarkers for HCC Early Detection
The Early Detection Research Network (EDRN) proposed five phases of biomarker development for early cancer detection that have been widely used in the field.11 In 2021, the International Liver Cancer Association (ILCA) suggested modified EDRN biomarker phases tailored to HCC.12 Phase 1 is an exploratory study to find potential biomarkers in preclinical settings. It is usually performed by comparing tumor versus non-tumor tissue with tools detecting protein or gene expression. Phase 2 is the development of a clinical assay by comparing specimens from human subjects with versus without tumors. It is performed in a clinical setting, such as a case–control study after case subjects have been diagnosed with cancer. Phase 3 is a retrospective longitudinal study to evaluate the biomarkers’ early detection ability. It compares subjects who have versus subjects who have not developed cancer, using clinical assays from multiple timelines. Phase 4 is a prospective screening study to evaluate biomarkers as a screening tool in the target population. Phase 5 is a controlled study, ideally a randomized controlled trial (RCT), accompanied by therapeutic intervention if needed, with a positive screening test to evaluate the mortality benefit of the biomarker screening. Outcome measures from each phase are described in Table 1. Outcomes from novel biomarkers for early HCC detection can be compared to those of established surveillance tools such as AFP with or without US.12
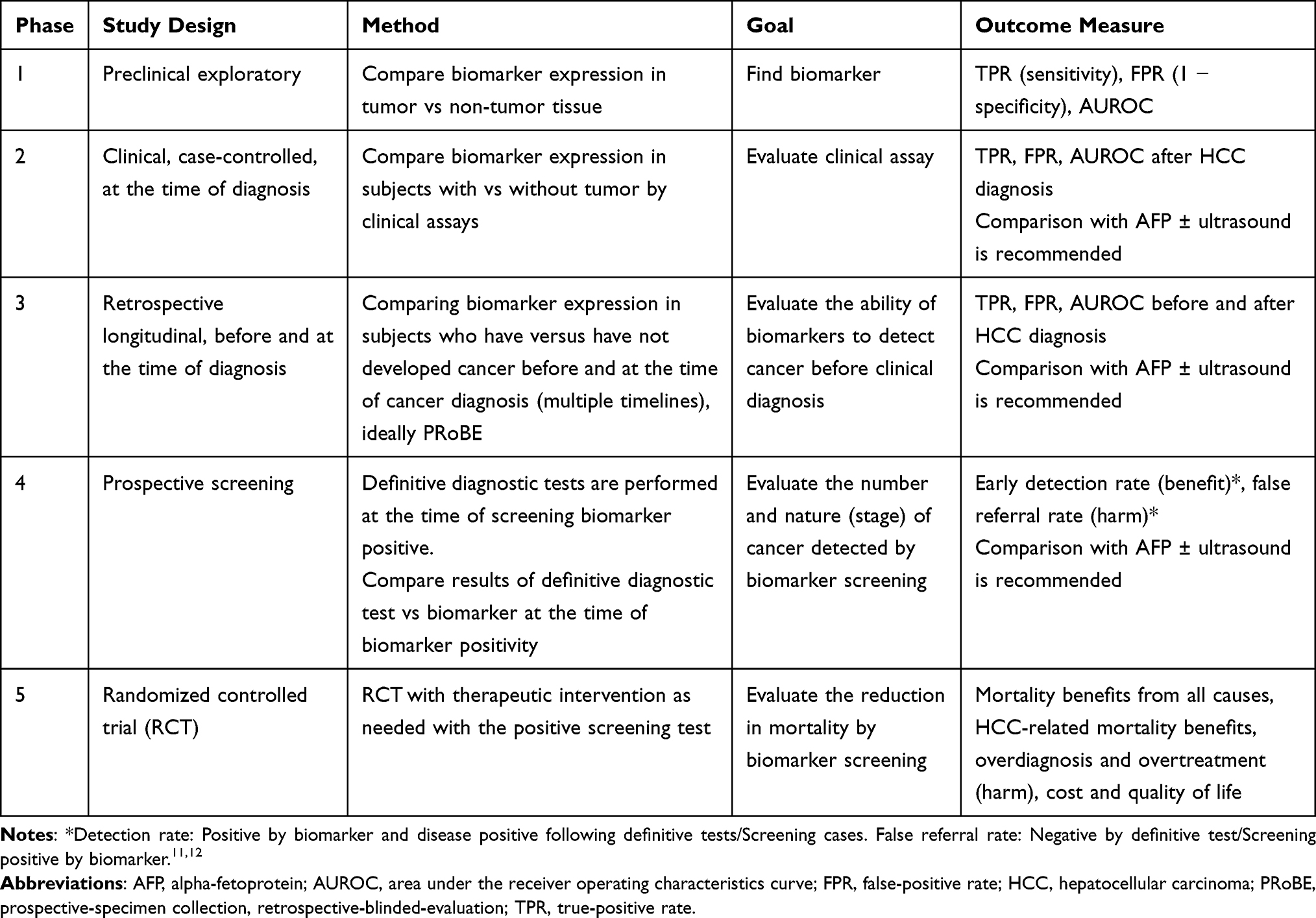 |
Table 1 Phases of Cancer Biomarker Development for Early Detection of HCC |
Although not all biomarker studies for early cancer detection fit the EDRN and ILCA models, this framework provides an estimation of the scientific evidence from each biomarker study in HCC. In this review, we will estimate diagnostic biomarkers based on this five-phase structure.
AFP, AFP-L3, DCP
Biannual abdominal US has been the standard screening tool for HCC surveillance in at-risk populations following major international guidelines.4,5,13 US is known to have a high sensitivity for detecting any stage of HCC, but a relatively low sensitivity for early-stage HCC.14–16 For example, in a meta-analysis with six prospective studies for any-stage HCC and 13 studies for early HCC, US had a high sensitivity of 94% for any-stage HCC but only 63% sensitivity for early-stage HCC.15 Given this limited detection capacity for early-stage HCC with US, there is an unmet need for biomarkers for the early detection of HCC.
AFP is a plasma glycoprotein normally produced by the fetal liver and embryonic yolk sac during embryogenesis, and has historically been used as an HCC biomarker.17–19 However, serum AFP is also known to be elevated in other clinical conditions, including intrahepatic cholangiocarcinoma, gastric cancer, germ cell tumors, acute hepatitis, and chronic liver disease.20–24 Despite this controversy and the potential non-specificity of AFP as an HCC biomarker, it has been the most studied biomarker as a surveillance tool in HCC.
Two large population-based meta-analysis studies assessed the value of adding AFP to US for HCC surveillance.15,25 The first meta-analysis, by Singal et al, including 13 prospective studies, revealed no additional sensitivity benefit of adding AFP to US for early HCC detection (63% vs 69%),15 whereas later meta-analysis by Tzartzeva et al, including 32 studies (23 prospective, nine retrospective), showed higher sensitivities for both early (63% vs 45%) and any stage (97% vs 78%) HCC detection in AFP with US compared to US alone.25 It is important to note that the later study observed a wide variation of US performance, which could potentially overestimate the detection value of AFP compared to expert-performed US alone.24,25 Two phase 5 RCTs with AFP for HCC surveillance were carried out in China in the 1990s.26,27 One study evaluated biannual AFP plus US surveillance compared to non-surveillance, and showed a significant 36% relative and 0.05% absolute risk reduction.26 The other RCT, with biannual AFP without US for HCC surveillance, did not show a mortality benefit compared to non-surveillance.27 These RCTs were not specifically designed for evaluating the addition of AFP to US, and focused on HBV hepatitis patients regardless of cirrhosis status.26,27 Therefore, proper evaluation of the value of adding AFP to US for early HCC detection in cirrhosis populations is limited.
As the performance of AFP for HCC surveillance is suboptimal, many other biomarkers have been studied. Among them, AFP-L3 and des-gamma-carboxyprothrombin (DCP) have gained attention. AFP can be classified into three groups according to its binding capacity to lens culinaris agglutinin (LCA), from AFP-L1 (non-binding) to AFP-L3 (LCA-reactive).28,29 Compared to AFP, AFP-L3 is known to be exclusively secreted in HCC cells in the early stages, so it has been proposed as a more specific biomarker for HCC.24,28,29 DCP, also known as prothrombin, induced by vitamin K absence/antagonist-II (PIVKA-II), is an abnormal prothrombin molecule due to an acquired defect in -translational carboxylation, which can stem from oncogenesis and HCC progression.29–31
Initially, AFP-L3 and DCP were proposed as possible superior biomarkers to AFP for HCC surveillance, but later studies revealed mixed results.32–34 Accordingly, AFP-L3 and DCP have been proposed to be combined with AFP to increase its HCC detection capacity. For example, the GALAD score, a statistical model combining gender, age, AFP, DCP, and AFP-L3, was suggested in 2014.35 Later, a phase 2 study evaluated the GALAD score in patients with cirrhosis or chronic hepatitis B.36 In this study, GALAD showed a larger area under the receiver operating characteristics curve (AUROC) compared to US for any-stage (0.95 vs 0.82, p<0.01) and early-stage (0.92 vs 0.82, p<0.01) HCC.36 This study also suggested another statistical model combining GALAD and US, titled the GALADUS score, which showed improved HCC detection performance, with AUROC of 0.98 and 0.97 in any- and early-stage HCC, respectively.36 Two phase 3 studies published in 2022 evaluated GALAD and each of three biomarkers. In both studies, there were no significant differences in AUROC between GALAD and AFP alone, but GALAD showed higher sensitivity with compromising specificity compared to AFP, regardless of timeline or HCC stage.37,38 With fixed specificity at 90%, GALAD increased the sensitivity compared to AFP alone by 9–20 percentage points at 6 months before HCC diagnosis in any-stage disease, but mixed results were observed for early-stage disease.37,38 Neither study compared those biomarkers to US. An interim report from a phase 5 RCT showed that adding AFP, AFP-L3, and DCP to US improved the sensitivity of HCC detection compared to US alone with compromising specificity, although HCC cases during the follow-up were small (n=20) at the time of the report.36,39,40 Except for these interim data, there are limited phase 4 and 5 data for AFP-L3, DCP, GALAD, and GALADUS.
Many other candidates, such as aldo-keto reductase family 1 member B10 (AKR1B10), Dickkopf-1 (DKK1), Golgi protein 73 (Gp-73), glypican-3, and osteopontin (OPN), have been proposed as potential biomarkers for HCC surveillance.24,40–44 However, most of those proposals are based on phase 1–2 studies, and phase 3 or later data for those biomarkers are insufficient to date.
None of the three major international HCC guidelines recommends biomarkers, except for AFP for HCC surveillance, which is also controversial, with the recommendations varying between guidelines, given limited evidence.4,5,13 Further verification is warranted, with later-phase biomarker studies, for the above biomarkers to be incorporated in daily practice. Also, possible harm from false-positive cases, such as additional costs, tests, or patient anxiety, should be considered to comprehensively estimate the value of these biomarkers.
Liquid Biopsy: ctDNA, CTCs, miRNA
Liver biopsy is invasive, with a risk of tumor seeding and bleeding. Also, the intratumoral and intertumoral heterogeneity of HCC limits single-specimen biopsy in fully reflecting the entire HCC tumors.45,46 Liquid biopsy, which is minimally invasive, can potentially be used in cancer screening, recurrence monitoring, estimating prognosis and treatment response, and identifying treatment resistance mechanisms.47,48 In a liquid biopsy, samples of body fluids, such as blood, are collected, and genomic and proteomic information is obtained about the primary tumor.47,48 Liquid biopsy encompasses CTCs, circulating tumor nucleic acids (ctDNA and miRNA), and extracellular vehicles.46–48 A variety of studies have proposed novel biomarkers for HCC using these liquid biopsy techniques. Among them, ctDNA, CTCs, and miRNA have been actively investigated in HCC. Developments in liquid biopsy for HCC have focused on the detection of early-stage or recurrent disease, prognostic, and predictive biomarkers. The diagnostic insights of liquid biopsy is discussed in this section, and the prognostic and predictive insights of liquid biopsy are discussed later.
ctDNA
There are multiple cancer genetic targets in ctDNA, including copy number variations (CNV), gene methylation, fusion, integrity, and DNA mutation.49 Of these, gene methylation and gene mutations are the two most studied in HCC. Aberrant DNA methylation has been proposed as playing an important role in early carcinogenesis, including in HCC, and investigated for early HCC detection.50,51 In contrast, gene mutation has been more investigated as a biomarker for disease monitoring, prognostication, and treatment response, as described in a later section.
Several ctDNA methylation profiling platforms, including Epigenomics AG, ExactSciences, and Laboratory for Advanced Medicine (LAM), have received FDA breakthrough and/or CE mark approval and have been investigated for HCC surveillance. In a phase 2 trial with HCC cases and cirrhosis controls, Epigenomics AG single-target SEPT9 platform showed a sensitivity of 76.7% at 97% specificity.52 Another phase 2 trial with the Epigenomics AG platform in a large population of 530 target participants is underway in France (NCT03311152).
In a phase 2 study, Chalasani et al developed an algorithm by combining the ExactSciences Oncoguard® Liver panel of three methylated markers (HOXA1, TSPYL5, and B3GALT6) with AFP and sex, which revealed 88% sensitivity at 87% specificity for any-stage HCC.53 In another phase 2 study, the same authors developed a new multi-target panel with four methylation markers (HOXA1, EMX1, TSPYL5, and B3GALT6) and two protein markers (AFP and AFP-L3), which showed higher sensitivity of 71% than the GALAD score of 41% and an AFP of 45% at fixed 90% specificity for early-stage HCC.54
The LAM-IvyGene DNA methylation panel was developed based on a large population-based phase 2 study in China.55 This IvyGene methylation platform also demonstrated promising capacity in another phase 2 study, with sensitivity of 95% at 97.5% specificity in any-stage HCC.56 A phase 4 prospective study with this LAM-IvyGene ctDNA methylation platform is underway in the USA (NCT03694600). Notably, each ctDNA methylation platform uses different epigenetic factors for HCC surveillance.
CTCs
CellSearch is an FDA-approved CTC platform based on EpCAM-based enrichment and immunofluorescent detection.57 A phase 2 study with metastatic HCC cases and non-malignant liver disease controls, CellSearch, showed 35% sensitivity and 100% specificity with a cut-off of ≥2 CTCs per 7.5 mL whole blood.58 In another phase 2 study with any-stage HCC cases and non-malignant liver cirrhosis controls, CellSearch showed 30.5% sensitivity and 94.7% specificity with a cut-off ≥1 CTCs per 7.5 mL.59 If the cut-off was increased to ≥2 CTCs per 7.5 mL, sensitivity was significantly decreased to 15.3% with 100% specificity.59
Dozens of other phase 1/2 biomarker studies have been performed and many different CTC clinical assays have been proposed as biomarkers for the early detection of HCC. For example, a phase 1/2 study, which developed an optimized EpCAM mRNA-based CTC platform in a preclinical setting followed by a phase 2 case–control study, revealed an AUROC of 0.70 with sensitivity of 42.6% at 96.7% specificity with a cut-off of ≥2 CTCs per 5 mL whole blood.60 Combined with AFP, the diagnostic capacity of CTCs was improved to an AUROC of 0.86 with a sensitivity of 73.0% at 93.4% specificity.60 Two meta-analyses which combined phase 2 data from heterogeneous CTC assays with different cut-off values showed sensitivities of 0.60–0.67 and specificities of 0.95–0.98 for HCC diagnosis.61,62
EpCAM-based CTC showed limited detection capacity in phase 2 studies compared to AFP or other protein-based biomarkers. Also, it is known that only around 30–40% of HCCs express EpCAM, which limits their use as a biomarker for HCC surveillance.48 However, the addition of CTC markers, such as GPC3, vimentin, twist, and cadherin, has been proposed for HCC surveillance.46,63,64
miRNA
Several phase 1 and 2 studies have proposed miRNA as a biomarker for HCC surveillance, but the miRNA from each study is heterogeneous.24,65,66 Notably, a three-stage miRNA study was performed in China.67 This initially identified a seven-miRNA classifier (Cmi) (miR-29a, 29c, 133a, 143, 145, 192, and 505) in phase 1. In the phase 2 stage, the Cmi showed higher sensitivity (70.4–85.7% vs 40.7–69.4%) with similar specificity (80.0–91.1% vs 84.9–100%) compared to AFP at the time of HCC diagnosis. Following the phase 3 nested case–control stage, Cmi showed much higher sensitivity and larger AUROC compared to AFP at 12, 9, 6, and 3 months before HCC diagnosis, with mildly compromised specificity.67
Prognostic Biomarkers for Hepatocellular Carcinoma
AFP
AFP has been extensively investigated and has demonstrated high-level evidence as a prognostic biomarker in different stages of HCC.12,24,68,69 In France, an AFP-based statistical model for post-transplant HCC recurrence prediction was developed in a retrospective cohort study.68 This model was validated in a following prospective cohort study, which predicted overall survival (OS) and relapse-free survival (RFS) regardless of Milan criteria.68 Many countries incorporate AFP as part of their criteria for LT candidacy.12,24 In subset analyses from the historic SHARP RCT cohort, increased AFP showed worse OS and time to progression, but sorafenib showed survival benefit regardless of AFP level.70 The authors concluded that AFP has a prognostic but not a predictive value for OS.70 A pooled analysis from two historic sorafenib RCTs, the SHARP and the Asia-Pacific trial, found high AFP (>200 ng/mL) to be an independent factor for worse OS but not a predictive marker for sorafenib.71
The following major phase 3 HCC RCTs, such as IMbrave150 and RESORCE trials, included AFP as a stratification factor.6,72 Furthermore, an AFP-driven trial was performed with ramucirumab, as shown below (Ramucirumab section).10 There has been controversy regarding the cut-off for AFP as a prognostic biomarker, but 100, 200, 400, and 1000 ng/mL have been commonly used.24 One noteworthy limitation of AFP as an HCC prognostic biomarker is that a limited number of HCC patients have elevated AFP, and, in particular, only around 10% of early-stage HCC is known to elevate AFP.12,73
AFP-L3, DCP, BALAD
Multiple retrospective studies have demonstrated the prognostic value of AFP-L3 and DCP in different stages of HCC. Several retrospective studies with curative hepatectomy patients found AFP-3 and DCP to be independent risk factors for recurrence and survival.24,74,75 In Japan, several retrospective studies with transplant recipients for HCC showed DCP to be an independent risk factor for recurrence and survival.76–78 DCP has been proposed as a selection criterion for LT candidacy by several societies.24,76,78 In a prospective study including patients withunresectable HCC, with limited population size (n=99), AFP-L3, but not DCP, showed a significant relationship to patient outcome.79
BALAD and BALAD2 scores, which combine three biomarkers (AFP, AFP-L3, DCP) and two liver function markers (albumin and bilirubin), were suggested as HCC prognosis systems based on retrospective analyses from large population data sets in Japan and the UK.80,81 BALAD and BALAD2 were validated by multiple observational studies from different countries, which demonstrated their promising prognostic capacity,82–84 but the comparison of the prognostication performance of these serum-based scoring systems compared to other commonly used staging systems, such as Barcelona Clinic Liver Cancer (BCLC) staging, is limited. One relatively small population-based retrospective study with 148 HCC patients revealed comparable performance among BALAD, BALAD2, and BCLC.84 An important limitation of these serology-based scoring systems is that they do not include the tumor burden or imaging features, which are the key components for treatment decisions such as resection, transplantation, and liver-directed locoregional therapy. Thus, they are not routinely used in daily practice.
Prognostic and Predictive Biomarkers for Advanced HCC from Major Clinical Trials
In 2021, the ILCA suggested a scientific evidence level-based system of prognostic and predictive biomarkers by study design: case–control from a convenience sample (level 3), retrospective cohort (level 2b), prospective cohort (level 2a), archived samples from an RCT (level 2a), and RCT (level 1), with well-conducted archived samples from RCT studies also rated level 1.12 A variety of studies have suggested many prognostic and predictive biomarkers in HCC, with different designs in the heterogeneous HCC population. To date, except for ramucirumab from the REACH-2 trial, none of the suggested biomarkers hasbeen derived from biomarker-driven RCTs. This section focuses on prognostic and predictive biomarkers derived from high-level studies such as exploratory studies from RCTs or major clinical trials. Table 2 and Table 3 summarize the suggested biomarkers from major clinical trials on HCC.
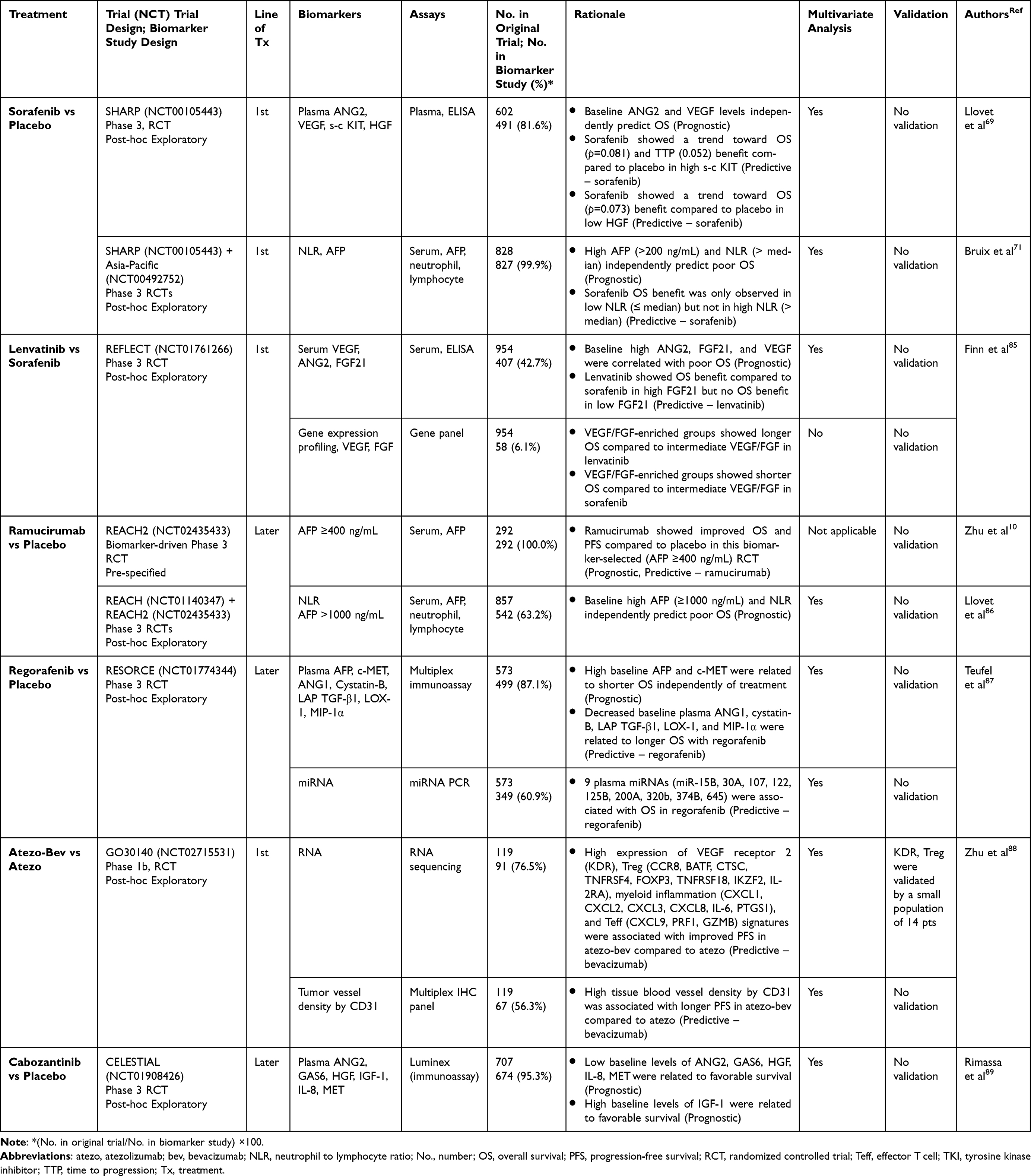 |
Table 2 Summary of Proposed Prognostic and Predictive Biomarkers for TKIs and Anti-Angiogenesis Agents by Biomarker Studies from Major Clinical Trials |
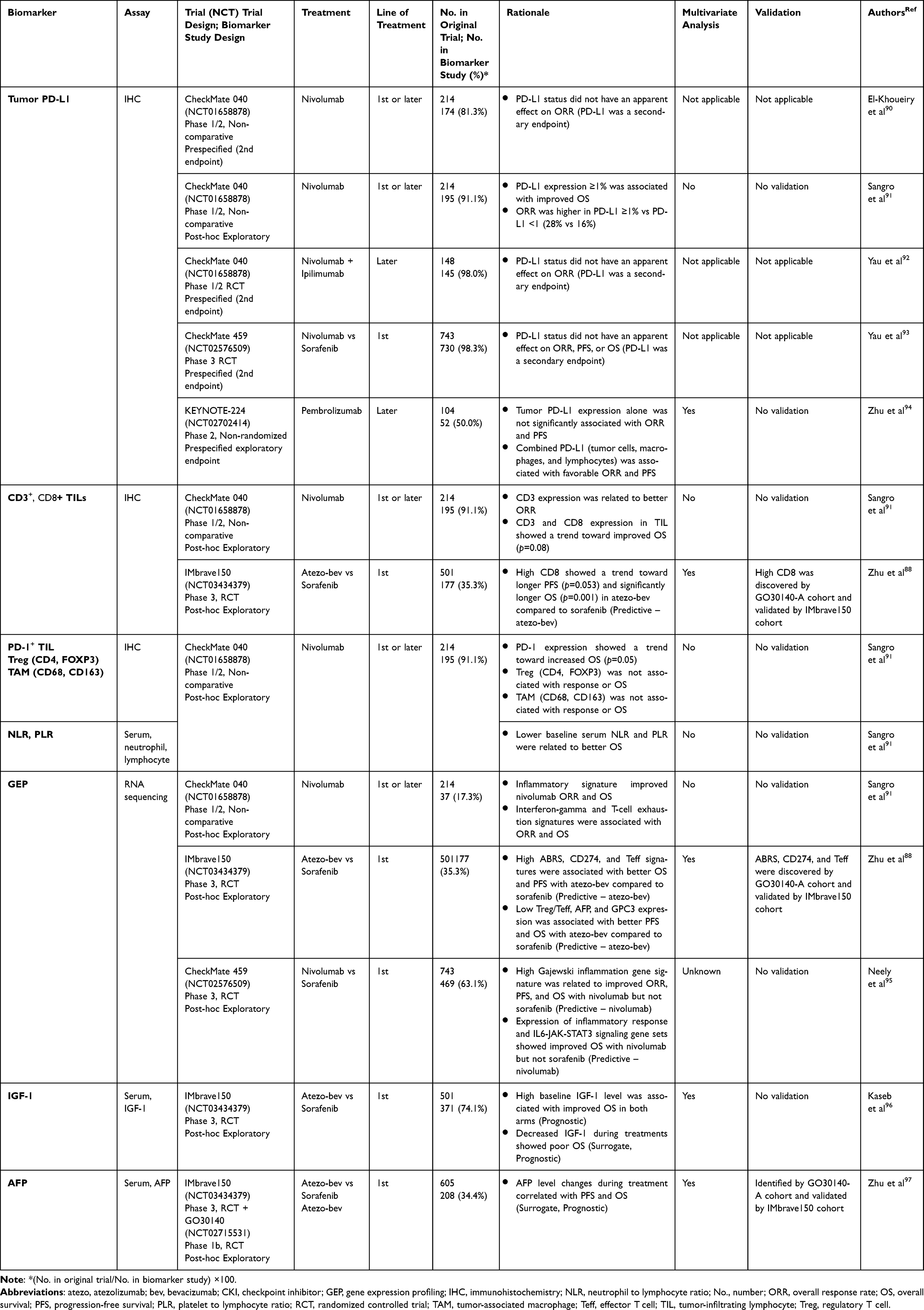 |
Table 3 Summary of Proposed Prognostic and Predictive Biomarkers for CPIs by Biomarker Studies from Major Clinical Trials |
Prognostic and Predictive Biomarkers for TKIs and Anti-Angiogenesis Therapy
Sorafenib
Based on the historic phase 3 SHARP trial, sorafenib became the standard first-line systemic therapy for advanced HCC in 2008, and was also verified in an Asian population by the Asia-Pacific trial.98,99 The following biomarker study from the SHARP trial cohort investigated 10 plasma markers: angiopoietin 2 (ANG2), EGF, bFGF, VEGF, sVEGFR-2, sVEGFR-3, hepatocyte growth factor (HGF), s-c KIT, insulin-like growth factor-1 (IGF-2), and circulating Ras.69 Among these, baseline ANG2 and VEGF levels showed value as prognostic biomarkers, independently predicting survival in both the sorafenib and placebo arms. Also, baseline high s-c KIT and low HGF levels showed a trend toward survival benefit in the sorafenib compared to placebo arm, which suggests that they could be used as potential predictive biomarkers for sorafenib.69 Another sorafenib biomarker study with analyses from a combined SHARP and Asia-Pacific pool revealed high AFP and neutrophil to lymphocyte ratio (NLR) as prognostic biomarkers for poor OS.71 Also, sorafenib showed OS benefit compared to placebo in the low-NLR but not the high-NLR subgroup, and NLR was suggested as a potential predictive biomarker for sorafenib.71
Lenvatinib
In the phase 3 REFLECT trial, lenvatinib showed non-inferior OS outcome compared to sorafenib and became a first-line therapy option for advanced HCC in 2018.100 A following biomarker study explored five serum biomarkers (VEGF, ANG2, FGF19, FGF21, and FGF23) and gene expression profiling (GEP), with 407 cases for serum and only 58 cases for GEP analyses.85 Higher baseline VEGF, ANG2, and FGF21 levels were associated with poor OS in both arms and were suggested as prognostic biomarkers. Also, OS was longer with lenvatinib compared to sorafenib in high baseline FGF21, which was not observed in low FGF21, so high FGF21 was suggested as a potential predictive biomarker for lenvatinib.85 The VEGF/FGF-enriched group by GEP showed improved OS in lenvatinib but shorter OS in sorafenib compared to the intermediate VEGF/FGF group. Also, in transcriptional regulation analyses, Wnt and DNA-repair pathways were associated with survival outcomes in the lenvatinib arm.85 However, any interpretations from this GEP analysis should be made with caution, given the small sample size of 58 cases.
Ramucirumab
Ramucirumab is the first and only medicine to have been verified by a biomarker-driven phase 3 RCT in HCC. The phase 3 REACH trial evaluated ramucirumab compared to placebo as the second or later line in advanced HCC, and the trial did not meet the primary endpoint of OS.101 However, in the subgroup analysis, high baseline AFP (≥400 ng/mL) showed OS benefit in the ramucirumab compared to the placebo arm.101 The following biomarker-driven phase 3 REACH-2 trial with the same design that only included baseline AFP ≥400 ng/mL revealed a significant OS benefit for ramucirumab compared to placebo.10 Therefore, AFP showed both prognostic and predictive value in HCC with ramucirumab.102 The following biomarker study from the REACH and REACH-2 pool revealed AFP >1000 ng/mL and high baseline NLR to be prognostic biomarkers in HCC but not predictive biomarkers for ramucirumab.86
Regorafenib
The phase 3 RESORCE trial evaluated regorafenib as the second line therapy after sorafenib compared to placebo in HCC, which met the primary endpoint of OS benefit.72 The following exploratory biomarker study with the RESORCE pool revealed five proteins (ANG1, Cystatin-B, LAP TGF-β1, LOX-1, and MIP-1α) and nine miRNAs (miR-15b, 30a, 107, 122, 125B, 200a, 320, and 374b) as potential predictive biomarkers for improved OS with regorafenib compared with placebo.87 Tumor immune profiling did not reveal any survival difference. High AFP and c-MET showed value as prognostic biomarkers for poor survival outcomes in HCC, but not as predictive biomarkers for regorafenib.87
Bevacizumab
The phase 1b GO30140 trial randomized group-F compared atezolizumab with versus without bevacizumab. The following exploratory biomarker analysis with 91 cases showed high expression of VEGF receptor 2 (KDR), regulatory T cells (Tregs), myeloid inflammation, and T-effector signatures (CXCL9, PRF1, and GZMB) associated with improved progression-free survival (PFS) for the combination compared to atezolizumab alone, which suggests them as potential predictive biomarkers for bevacizumab.88 Also, high tissue blood vessel density measured by CD31 digital readouts from a multiplex immunohistochemistry (IHC) panel was associated with longer PFS in combination compared to atezolizumab monotherapy, which implies that CD31 is a potential predictive biomarker for adding bevacizumab to atezolizumab.88
Cabozantinib
The phase 3 CELESTIAL trial investigated cabozantinib as the second or later-line therapy after sorafenib compared to placebo in HCC, and showed significant OS and PFS benefits of cabozantinib compared to placebo.103 A following exploratory biomarker study with the CELESTIAL pool evaluated plasma markers. High IGF-1 and low ANG2, GAS6, HGH, IL-8, and MET baseline levels were related to favorable OS and PFS, and were suggested as prognostic biomarkers in previously treated advanced HCC.89 No potential predictive biomarker for cabozantinib was identified from the study.89 The phase 3 COSMIC-312 trial evaluated cabozantinib–atezolizumab combination compared to sorafenib as the first line in advanced HCC, and did not meet one of the dual primary endpoints of OS benefit.104 The following exploratory biomarker study is underway.104
Prognostic and Predictive Biomarkers for Immune Checkpoint Inhibitors
Tumor PD-L1 Expression
Initially, the CheckMate 040 phase 1/2 non-comparative study in advanced HCC evaluated the response to nivolumab by tumor PD-L1 expression as a secondary endpoint.90 The study showed that tumor PD-L1 expression is not apparently associated with the response to nivolumab.90 In the following biomarker analysis from the CheckMate 040 pool, tumor PD-L1 expression was associated with improved OS.91 However, given that responses occurred in PD-L1-negative patients, and significant target lesion size shrinkages were observed regardless of PD-L1 status, the authors concluded that PD-L1 was not an ideal predictive biomarker for nivolumab.91 In addition, the nivolumab plus ipilimumab cohort from the CheckMate 040 study revealed that PD-L1 expression was not associated with response rates.92 More recently, the CheckMate 459 phase 3 RCT compared first line nivolumab to sorafenib and evaluated anti-tumor efficacy by PD-L1 expression as a secondary endpoint.93 Positive PD-L1 showed a higher nivolumab response, but it was not significant, and PD-L1 expression was not related to PFS and OS.93 Biomarker analyses from the phase 2 KEYNOTE-224 trial pool with a relatively small subset of 52 cases revealed that positive combined PD-L1 (tumor cells, macrophages, and lymphocytes) was associated with a favorable pembrolizumab response and PFS, but tumor PD-L1 expression alone was not significantly associated with response and PFS.94 In summary, PD-L1 expression in HCC has not shown a strong enough signal as a predictive biomarker for CPIs to drive clinical decisions.
Immune- and Inflammation-Related Markers: T-Cell Subsets (CD3, CD4, CD8, FOXP3), PD-1, Macrophages (CD68, CD163), NLR, and PLR
The exploratory biomarker study from CheckMate 040 evaluated multiple immune cells and inflammation-related markers as potential predictive biomarkers for nivolumab. In the study, CD3 and CD8 expression in tumor-infiltrating T cells showed a trend toward improved OS (p=0.08).91 CD3 expression was also related to better nivolumab response (p=0.03). PD-1 expression, which is known as the T-cell exhaustion marker, was related to better nivolumab response and showed a trend toward longer OS (p=0.05).91,105 Also, lower serum NLR and platelet to lymphocyte ratio (PLR) were associated with improved OS.91 Regulatory T-cell markers such as CD4 and FOXP3 or tumor-associated macrophage markers such as CD68 and CD163 appear unrelated to either response or OS.91,106
In an exploratory biomarker study from the phase 3 IMbrave150 trial, patients with high CD8 expression in tumor-infiltrating T cells were associated with improved OS in the atezolizumab–bevacizumab combination compared to the sorafenib arm.88 There was no significant difference in survival outcome between the combination arm and the sorafenib arm in low CD8 expression, which implies that high intratumoral CD8+ T cells are a potential predictive biomarker for atezolizumab plus bevacizumab.88
Gene Expression Profiling
Several studies have investigated tumor cell GEP such as RNA sequencing as a potential biomarker for CPIs in HCC. The biomarker study from the CheckMate 040 pool performed RNA sequencing in 37 cases and revealed that the four-gene inflammatory signature with CD274 (PD-L1 messenger RNA), CD8A, LAG3, and STAT1) was associated with improved nivolumab response and OS.91 Also, the six-gene interferon-gamma signature (CXCL10, CXCL9, HLA-DRA, IDO1, IFNG, and STAT) and the T-cell exhaustion signature (CD274, CD276, CD8A, LAG3, PDCD1LG2, and TIGIT) were associated with ORR and OS.91 In the biomarker study from the phase 2 single-arm pembrolizumab trial in South Korea, GEP by RNA sequencing showed that the T-cell receptor (TCR) signaling pathway was significantly enriched in responders compared to non-responders.107 In contrast, non-responders showed higher expression of neutrophil gene markers compared to responders.107
In a study from the IMbrave150 pool, high expression of ABRS, CD274, and T-effector (Teff) signatures was associated with better OS and PFS with the atezolizumab–bevacizumab combination compared to sorafenib.88 Survival was not significantly different between groups with low expression of ABRS, CD274, and Teff, implying that pre-existing immunity by those GEP markers can be a positive predictive biomarker for atezolizumab–bevacizumab combination.88 In contrast, lower expression of Treg/Teff ratio, AFP, and glypican 3 (GPC3) were associated with better PFS and OS in the combination compared to sorafenib. No survival differences between groups were observed with high expression of AFP, GPC3, and Treg/Teff ratio, suggesting these as negative predictive biomarkers for atezolizumab–bevacizumab.88
In another exploratory biomarker analysis from the CheckMate 459 cohort with 469 cases of whole transcriptome RNA sequencing, a high Gajewski inflammation gene signature score was related to improved response, PFS, and OS in the nivolumab but not the sorafenib arm.95 Also, in gene set enrichment analysis, expression of inflammatory response and IL6-JAK-STAT3 signaling gene sets showed improved OS in the nivolumab but not the sorafenib arm.95 A biomarker study including RNA sequencing from the ORIENT-32 phase 2–3 RCT with a sintilimab (anti-PD-L1) and bevacizumab biosimilar combination is underway in China, but no interim data are available to date.108
AFP, IGF-1
Serum IGF-1 and AFP levels were suggested as surrogate and/or prognostic biomarkers by the exploratory studies from the IMbrave150 and GO30140 cohorts.96,97 As the liver synthesizes the majority of IGF-1, IGF-1 has been proposed as a liver synthetic function marker.109 A biomarker study from the IMbrave150 pool showed that high baseline IGF-1 level is associated with improved OS in both the atezolizumab–bevacizumab and sorafenib arms, and it was suggested as a prognostic but not predictive biomarker.96 Also, patients with decreased IGF-1 during treatment showed poor OS compared to stable IGF-1 in both the combination and sorafenib arms, which suggests IGF-1 as a surrogate marker for survival for both treatments. Notably, relatively few patients had decreased IGF-1 (32 cases in atezolizumab–bevacizumab and 14 cases in sorafenib) during treatment, so interpretation from the findings should be done with caution.96
An exploratory two-step biomarker study was performed for atezolizumab–bevacizumab combination, identifying the optional AFP cut-off from the GO30140 pool, with 58 cases followed by validating the optimized AFP cut-off in the IMbrave150 pool, with 150 cases.97 AFP decreases of ≥75% and increases of ≤10% from baseline at 6 weeks of treatment were identified as response and disease control, respectively. Both AFP cut-offs predicted longer OS and PFS, which suggests that AFP response could be a surrogate biomarker for atezolizumab–bevacizumab in HCC.97 Notably, both AFP and IGF-1 levels are easily accessible tests that can be used in daily practice.
Prognostic and Predictive Insights of Liquid Biopsy in HCC
ctDNA
Several observational studies have suggested ctDNA as a potential prognostic biomarker in HCC patients who have undergone curative treatment. In a retrospective cohort study with 81 HCC patients who received curative hepatectomy, ctDNA by four hotspot mutations was evaluated as a potential predictive biomarker.110 Preoperative positive ctDNA was associated with shorter DFS (16.6 vs 35.3 months, p<0.001) and OS (22.5 vs 40.0 months, p<0.001) compared to negative ctDNA.110 Increased mutant allele frequency (MAF) from pre- to post-hepatectomy correlated with higher disease recurrence.110 The following multivariable analyses revealed both pre-hepatectomy positive ctDNA and increased MAF after hepatectomy as independent risk factors for post-hepatectomy recurrence.110 Similarly, in another observational study with 97 HCC patients who underwent curative resection, post-resection positive ctDNA by a 1021-gene panel showed higher recurrence (100% vs 15.8%) and shorter DFS (5 months vs not reached) compared to the ctDNA negative group.111 In a pilot study with 74 HCC patients who underwent LT, ctDNA positivity by the fingerprint method was related to a higher recurrence rate (31.7% vs 11.5%) and shorter recurrence-free survival (HR=3.25, p=0.019).112 Another observational study with 45 LT recipients for HCC showed that detectable ctDNA before LT is related to increased recurrence (48.6% vs 0%) and shorter disease-free survival (12.8 months vs not reached).113 In a prospective study with 41 LT recipients for HCC, the pre- and post-LT ctDNA positivities by mutation-based methods were both related to shorter RFS.114
The prognostic value of ctDNA has also been investigated in advanced HCC. In an observational study by Kim et al with 107 HCC patients, including around 35% with advanced stage disease, the MLH1 single-nucleotide variant in ctDNA was associated with shorter OS in advanced HCC.115 In a large observational study by Xu et al with 1098 HCC patients, including advanced stage, positive ctDNA with eight methylation markers was independently related to shorter OS.55 An exploratory biomarker study with personalized ctDNA assays by the Signatera platform was performed using the GO30140 trial atezolizumab–bevacizumab cohort with advanced HCC.116 ctDNA was positive in 96% (45/47) of patients. The post-treatment ctDNA clearance group showed longer PFS compared to the not-cleared group (not reached vs 6.5 months), which illustrates positive ctDNA as a potential adverse prognostic biomarker and surrogate biomarker for treatment response and disease progression.116 Notably, each study used different biomarkers and methods in the boundary of ctDNA, which raises concerns over reliability.
ctDNA has also demonstrated its potential value to discover predictive biomarkers in HCC. In a pilot study by von Felden et al, HCC patients with PI3K/MTOR pathway mutations had significantly poorer PFS than those without these mutations after TKIs (2.1 vs 3.7 months, p<0.001), but not after CPIs.117 This analysis is from a small subset of 22 patients, so interpretation should be made with caution, but this finding implies that predictive biomarkers can be potentially identified from analyses of ctDNA gene mutations in HCC.
miRNA
An exploratory biomarker study from the RESORCE study suggested nine miRNAs as potential predictive biomarkers for regorafenib, as mentioned above (Regorafenib section).87 Other than this, multiple studies have shown the possible prognostic value of miRNAs in HCC. Upregulation of miR-32-5p, miR-92a, miR-221, miR-224, miR-487a, and miR-665, and downregulation of miR-125b, miR-296, miR-638, miR-940, and miR-718 were associated with poor survival outcomes.118,119 However, those proposals are based on observational studies with relatively small populations in heterogeneous clinical settings. Notably, even with these multiple observation studies, almost none of these miRNAs have demonstrated their prognostic value in two or more studies, and most of the proposal is based on a single observational study. In addition, the comprehensive understanding of biological mechanisms and the role of each miRNA in HCC is still unclear, which limits the clinical utility of miRNAs in HCC diagnosis and treatment.119
CTCs
In an observational study with 49 HCC patients who underwent curative resection, an elevated preoperative EpCAM CTC level was associated with a higher recurrence rate.120 However, as mentioned above (Liquid Biopsy: ctDNA, CTCs, miRNA; CTCs section), EpCAM is known to express only a small proportion (30–40%) of HCC cells, and other markers such as mesenchymal CTCs have also been investigated.48 In a prospective cohort study with 62 HCC patients who underwent curative resection, postoperative mesenchymal CTC positivity was associated with higher recurrence and shorter DFS.121 This prognostic value of mesenchymal CTC in post-resection HCC patients was also consistently observed in several other observational studies.46,64,122
Thus, liquid biopsy with ctDNA, miRNA, and CTCs has shown potential in providing prognostic and predictive biomarkers for HCC, particularly ctDNA. However, most of the evidence is based on observational studies, and data from major RCT exploratory biomarker studies are insufficient at present.
Comparative Discussion on Proposed Novel Biomarkers in HCC
In regard to liquid biopsy for the early detection of HCC, the EpCAM-based CTC approach revealed lower sensitivity outcomes than the ctDNA or miRNA approach, probably owing to limited EpCAM expression in HCC.48 Many different miRNAs were proposed as biomarkers from each phase 1 and 2 study, but these are heterogeneous. Therefore, further validation is needed from other cohorts, and a better biological understanding is also needed to supply the rationale for miRNA as an early detection tool in HCC. Currently, ctDNA seems to have the most scientific evidence for HCC early detection using liquid biopsy, with several ctDNA methylation-based platforms showing promising detection capacity for HCC in multiple phase 2 studies, but further verification with phase 3 or later studies is needed to prove its early detection capacity before it can be used for clinical diagnosis in HCC.
To evaluate and compare the scientific rationale of each suggested prognostic and predictive biomarker, we evaluated the design, sample size, presence of multivariate analyses, and validation from each biomarker study (Table 2 and 3).123 Several potential prognostic biomarkers were identified from independent cohorts, including AFP from five,10,71,86,87,97 ANG2 from three,69,85,89 and NLR,71,86 VEGF,69,85 and IGF-189,96 from two different phase 3 RCT cohorts. These reproduced results from different studies potentially make AFP, ANG2, NLR, VEGF, and IGF-1 more reliable prognostic biomarkers than other suggested markers from a sole study cohort. Notably, the sample sizes for tissue-based biomarkers such as IHC or RNA sequencing are significantly smaller than those for blood-based biomarkers; this is likely to stem from limited tumor tissue collection, as a definitive diagnosis of HCC can be made by radiologic evaluation alone, without histologic confirmation. For example, sample size ranges for tissue biomarkers were 58–91, compared to blood biomarkers with ranges of 292–827 in TKI and anti-angiogenesis agent biomarker studies from major clinical trials (Table 2). Looking at the accumulated evidence so far, this limited sample size makes the suggested tissue-based markers (IHC and RNA sequencing) less reliable, with poorer precision and power compared to the blood-based biomarkers suggested from larger samples. Only a few biomarker studies performed validation. Zhu et al identified potential predictive biomarkers from the discovery GO30140-A cohort (n=90) and validated these markers in the IMbrave150 phase 3 RCT cohort (n=177).88 Hence, predictive biomarkers suggested from this study, such as high CD8 and RNA sequencing (ABRS, CD274, Teff, Treg/Teff, AFP, and GPC3 expression), would potentially be more reproducible and accurate compared to others without validation. In contrast, inflammatory, interferon-gamma, and T-cell exhaustion signatures suggested by the exploratory CheckMate 040 study have weaker evidence compared to other suggested RNA-sequencing biomarkers for CPIs in HCC at the time of publication, as they were suggested from an early-phase, non-comparative population without validation or multivariate analyses.
Future Directions
Although multiple candidate diagnostic biomarkers for the early detection of HCC have been proposed, including from liquid biopsy platforms, few have been used in daily practice because of the insufficiency of verification from well-designed phase 3–5 studies. Ideally, phase 4 and 5 studies can provide strong scientific evidence for early detection biomarkers, but realistically, they require excessive resources with long-term follow-up. Most importantly, ethical issues are inevitable, such as potential harm from false-positive cases in phase 4 and a non-surveillance comparison group in phase 5 studies. So, a large population-based well-designed phase 3 study may be an alternative to find promising biomarkers for the early detection of HCC. The NCI EDRN has launched the Hepatocellular carcinoma Early Detection Strategy study, with 1482 LC participants, with longitudinal data and biospecimen collection.124 Also, the Texas Hepatocellular Carcinoma Consortium Cohort Study has enrolled LC patients with a target of 5000 participants for biomarker evaluation with a prospective specimen collection, retrospective blinded evaluation (PRoBE) phase 3 design.125 These large cohorts can potentially provide well-designed phase 3 validation of candidate novel biomarkers, such as ctDNA, miRNA, and CTC, which were suggested by phase 1–2 studies.126 Notably, a phase 4 prospective screening study with the ctDNA LAM DNA methylation platform is underway (NCT03694600). The target enrollment is 1600 participants, with the primary endpoint as sensitivity and specificity of ctDNA compared to US. Cost can be another important hurdle that should be overcome for liquid biopsy-based biomarkers to be used in clinical practice as HCC surveillance tools, as their cost is relatively high compared to protein-based biomarkers.
BALAD and BALAD2 scores showed potential prognostic value, but their current utility in daily practice is limited. An algorithm or scoring system which incorporates BALAD components with tumor burden features can be considered to promote its clinical utility. Also, further validation of the prognostic value of AFP-L3, DCP, and their combination with AFP is needed with prospective studies, ideally compared to BCLC or other major HCC staging systems.
In advanced HCC, multiple candidate prognostic and predictive biomarkers have been proposed from exploratory studies from major clinical trial pools. Also, further candidate biomarkers are expected to be presented from exploratory biomarker studies from major HCC RCTs, including HIMALAYA, COSMIC-312, and ORIENT-32. Although biomarker studies from RCT samples can provide stronger evidence compared to those from observational studies, given the nature of retrospective analyses, and that the study is not powered to each biomarker, their utility in clinical practice is limited. Ultimately, biomarker-driven RCTs such as the REACH2 ramucirumab trial with AFP will be warranted for these candidate novel predictive and/or prognostic biomarkers to be used to drive clinical decisions in daily practice.
Arguably, one of the most pressing, unresolved issues in advanced HCC management is the optimal sequencing of systemic therapies, namely, between TKI and CPI-based regimens. Furthermore, no prospective head-to-head comparative studies of efficacy exist among the various first line regimens, including atezolizumab–bevacizumab, durvalumab–tremelimumab, lenvatinib, and sorafenib, except between sorafenib and lenvatinib in REFLECT. Nonetheless, large, multicenter retrospective cohort studies have been invaluable in highlighting potential biomarkers that may influence this crucial decision. A preclinical study by Pfister et al suggests that HCC arising from NASH is characterized by the presence of exhausted CD8+ T cells and impaired immune surveillance, which contribute toward resistance against anti-PD-1 inhibitors.7 This mechanistic finding is supported by several retrospective cohort studies and meta-analyses showing that NASH-driven HCC patients have worse outcomes compared to those with non-NASH-driven HCC when treated with anti-PD-1 or L1 inhibitors.7,127 Furthermore, in NASH-driven HCC patients, lenvatinib was associated with superior outcomes compared to atezolizumab–bevacizumab in a multicenter propensity-matched analysis.128 Other studies have suggested that the clinical benefit with sorafenib can be greater in HCV-driven HCC compared to HCC driven by other etiology.8,9 Thus, the underlying HCC etiology, namely, NASH versus non-NASH or viral hepatitis, may be a potential marker of response to CPI versus TKI. In an observational study by Fang et al, HCC with vessels that encapsulate tumor clusters (VETC) by IHC demonstrated significant survival benefits from sorafenib, but no survival benefits were demonstrated from sorafenib in HCC without this vascular pattern, and VETC was suggested as a potential predictive biomarker for sorafenib.129 Nonetheless, further validation of these findings is warranted in larger prospective studies given the biases inherent to observational studies.
Unlike most other solid tumors, the definitive diagnosis of HCC can be made with radiologic evaluation without histologic confirmation. This limits investigators being able to justify tumor tissue collection before treatment, which can be a major limitation to investigating potential biomarkers and also performing biomarker-driven RCTs. This limitation is well demonstrated in the exploratory biomarker studies from REFLECT (407 cases available for serum and only 58 cases for tumor tissue biomarker analyses) and RESORCE (499 cases for plasma and only 46 cases for tumor tissue biomarkers).85,87 Liquid biopsy with CTCs and ctDNA can potentially substitute part of the tissue biopsy role, but studies validating a strong correlation between tumor tissue and liquid biopsy of that particular candidate predictive marker should precede this.
ctDNA analysis has demonstrated a promising potential to detect measurable residual disease (MRD) for other solid tumors after curative treatment.130 For example, MRD measured by ctDNA with Signatera after curative resection showed promise in predicting disease recurrence in other solid tumors in RCTs or exploratory biomarker tests from RCT cohorts.131,132 Accordingly, emerging data from liquid biopsies such as ctDNA and CTC have been showing a promising prediction of the recurrence risk in HCC with post-curative treatment. The use of ctDNA in the adjuvant setting following curative intent local therapies such as radiofrequency ablation (RFA) or liver resection is an area of active research. The phase 2 single-arm NIVOLVE study, conducted in Japan, studied the role of ctDNA as part of an exploratory analysis in patients treated with up to 16 cycles of adjuvant nivolumab after RFA or resection.133 The results showed ctDNA-positive patients tended to have shorter RFS compared to patients who were ctDNA negative (26.3 months vs not reached).133 Another single-arm phase 2 study, conducted in China, evaluated the role of ctDNA after perioperative camrelizumab (anti-PD-1 inhibitor) plus apatinib (VEGF-TKI), and similarly showed shorter RFS in ctDNA-positive versus ctDNA-negative patients (205 days vs not reached).134 Although the small sample sizes of these studies warrant caution in interpretation, the results merit close attention and validation in larger prospective studies. Other ctDNA-driven therapeutic studies evaluating post-curative therapy with gastrointestinal cancers, including HCC, are underway (NCT05482516). Patients with MRD positivity by Signatera ctDNA will receive atezolizumab–bevacizumab, and the ctDNA response to the therapy is planned to be evaluated. Also, Natera announced a new biomarker-driven trial, the Observational Study of Signatera in Liver Cancer (SIGNAL), in September 2020.135 The purpose of the SIGNAL study is to identify MRD by ctDNA after LT and evaluate the correlation with disease recurrence. Of note, the importance of ongoing ctDNA studies in the adjuvant setting is underscored by the IMBrave050 study (NCT04102098), the pivotal phase 3 trial evaluating adjuvant atezolizumab–bevacizumab in the post-resection adjuvant setting for early-stage HCC patients at high risk of recurrence.136 The study met its primary endpoint of RFS determined by an independent review facility with a hazard ratio of 0.72 (p=0.012).136 Indeed, the results of the study have the potential to shift the paradigm of early stage as well as advanced HCC management, and determination of the role of ctDNA in risk stratification of future adjuvant therapies is likely to be a growing area of research.
Conclusion
With emerging developments in omics technologies, a variety of novel biomarkers for HCC have been proposed. To date, nearly all of those suggested novel biomarkers for early HCC detection are from early phase studies. Findings from ongoing large-population-based phase 3 or phase 4 studies may provide verification for promising biomarkers for early HCC diagnosis among the candidates. Similarly, the majority of suggested novel prognostic and predictive biomarkers for advanced HCC come from exploratory studies from RCT cohorts. Ultimately, biomarker-driven RCTs will be warranted before these suggested prognostic and predictive markers are used to drive clinical practice.
Abbreviations
AFP, alpha-fetoprotein; ANG2, angiopoietin 2; AUROC, area under the receiver operating characteristics curve; BCLC, Barcelona Clinic Liver Cancer; cfDNA, cell-free DNA; CPI, checkpoint inhibitor; CTC, circulating tumor cell; ctDNA, circulating tumor DNA; DCP, des-gamma-carboxyprothrombin; EDRN, Early Detection Research Network; GEP, gene expression profiling; HCC, hepatocellular carcinoma; HGF, hepatocyte growth factor; IHC, immunohistochemistry; ILCA, International Liver Cancer Association; LCA, lens culinaris agglutinin; LT, liver transplantation; miRNA, micro-RNA; MRD, measurable residual disease; NLR, neutrophil to lymphocyte ratio; OS, overall survival; PFS, progression-free survival; PLR, platelet to lymphocyte ratio; PRoBE, prospective specimen collection, retrospective blinded evaluation; RCT, randomized controlled trial; RFS, relapse-free survival; Teff, effector T cell; Treg, regulatory T cell; US, ultrasound.
Acknowledgments
There are no funding sources.
Disclosure
Dr Richard Kim reports personal fees from Incyte, Pfizer, Ipsen, Eisai, Exelixis, Taiho, and Servier, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Colagrande S, Inghilesi AL, Aburas S, Taliani GG, Nardi C, Marra F. Challenges of advanced hepatocellular carcinoma. World J Gastroenterol. 2016;22(34):7645–7659. doi:10.3748/wjg.v22.i34.7645
3. Ronot M, Bouattour M, Wassermann J, et al. Alternative response criteria (Choi, European Association for the study of the liver, and modified Response Evaluation Criteria in Solid Tumors [RECIST]) versus RECIST 1.1 in patients with advanced hepatocellular carcinoma treated with sorafenib. Oncologist. 2014;19(4):394–402. doi:10.1634/theoncologist.2013-0114
4. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
5. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
6. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
7. Pfister D, Nunez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592(7854). doi:10.1038/s41586-021-03362-0
8. Bruix J, Raoul JL, Sherman M, et al. Efficacy and safety of sorafenib in patients with advanced hepatocellular carcinoma: subanalyses of a phase III trial. J Hepatol. 2012;57(4):821–829. doi:10.1016/j.jhep.2012.06.014
9. Jackson R, Psarelli EE, Berhane S, Khan H, Johnson PJ. Impact of viral status on survival in patients receiving sorafenib for advanced hepatocellular cancer: a meta-analysis of randomized phase III trials. J Clin Oncol. 2017;35(6):622–628. doi:10.1200/JCO.2016.69.5197
10. Zhu AX, Kang YK, Yen CJ, et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(2):282–296. doi:10.1016/S1470-2045(18)30937-9
11. Pepe MS, Etzioni R, Feng Z, et al. Phases of biomarker development for early detection of cancer. JNCI. 2001;93(14):1054–1061. doi:10.1093/jnci/93.14.1054
12. Singal AG, Hoshida Y, Pinato DJ, et al. International Liver Cancer Association (ILCA) white paper on biomarker development for hepatocellular carcinoma. Gastroenterology. 2021;160(7):2572–2584. doi:10.1053/j.gastro.2021.01.233
13. Omata M, Cheng AL, Kokudo N, et al. Asia–Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11(4):317–370. doi:10.1007/s12072-017-9799-9
14. Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Med. 2014;11(4):e1001624. doi:10.1371/journal.pmed.1001624
15. Singal A, Volk ML, Waljee A, et al. Meta-analysis: surveillance with ultrasound for early-stage hepatocellular carcinoma in patients with cirrhosis. Aliment Pharmacol Ther. 2009;30(1):37–47. doi:10.1111/j.1365-2036.2009.04014.x
16. Colli A, Fraquelli M, Casazza G, et al. Accuracy of ultrasonography, spiral CT, magnetic resonance, and alpha-fetoprotein in diagnosing hepatocellular carcinoma: a systematic review. Am J Gastroenterol. 2006;101(3):513–523. doi:10.1111/j.1572-0241.2006.00467.x
17. Kim JU, Shariff MIF, Crossey MME, et al. Hepatocellular carcinoma: review of disease and tumor biomarkers. World J Hepatol. 2016;8(10):471–484. doi:10.4254/wjh.v8.i10.471
18. Bader D, Riskin A, Vafsi O, et al. Alpha-fetoprotein in the early neonatal period—a large study and review of the literature. Clin Chim Acta. 2004;349(1):15–23. doi:10.1016/j.cccn.2004.06.020
19. Mizejewski GJ. Alpha-fetoprotein structure and function: relevance to isoforms, epitopes, and conformational variants. Exp Biol Med. 2001;226(5):377–408. doi:10.1177/153537020122600503
20. Wong RJ, Ahmed A, Gish RG. Elevated alpha-fetoprotein: differential diagnosis - hepatocellular carcinoma and other disorders. Clin Liver Dis. 2015;19(2):309–323. doi:10.1016/j.cld.2015.01.005
21. Shen WF, Zhong W, Xu F, et al. Clinicopathological and prognostic analysis of 429 patients with intrahepatic cholangiocarcinoma. World J Gastroenterol. 2009;15(47):5976–5982. doi:10.3748/wjg.15.5976
22. Adachi Y, Tsuchihashi J, Shiraishi N, Yasuda K, Etoh T, Kitano S. AFP-producing gastric carcinoma: multivariate analysis of prognostic factors in 270 patients. Oncology. 2003;65(2):95–101. doi:10.1159/000072332
23. Di Bisceglie AM, Sterling RK, Chung RT, et al. Serum alpha-fetoprotein levels in patients with advanced hepatitis C: results from the HALT-C trial. J Hepatol. 2005;43(3):434–441. doi:10.1016/j.jhep.2005.03.019
24. Piñero F, Dirchwolf M, Pessôa MG. Biomarkers in hepatocellular carcinoma: diagnosis, prognosis and treatment response assessment. Cells. 2020;9(6):E1370. doi:10.3390/cells9061370
25. Tzartzeva K, Obi J, Rich NE, et al. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: a meta-analysis. Gastroenterology. 2018;154(6):1706–1718.e1. doi:10.1053/j.gastro.2018.01.064
26. Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol. 2004;130(7):417–422. doi:10.1007/s00432-004-0552-0
27. Chen JG, Parkin DM, Chen QG, et al. Screening for liver cancer: results of a randomised controlled trial in Qidong, China. J Med Screen. 2003;10(4):204–209. doi:10.1258/096914103771773320
28. Taketa K, Sekiya C, Namiki M, et al. Lectin-reactive profiles of alpha-fetoprotein characterizing hepatocellular carcinoma and related conditions. Gastroenterology. 1990;99(2):508–518. doi:10.1016/0016-5085(90)91034-4
29. Hanif H, Ali MJ, Susheela AT, et al. Update on the applications and limitations of alpha-fetoprotein for hepatocellular carcinoma. World J Gastroenterol. 2022;28(2):216–229. doi:10.3748/wjg.v28.i2.216
30. Marrero JA, Su GL, Wei W, et al. Des-gamma carboxyprothrombin can differentiate hepatocellular carcinoma from nonmalignant chronic liver disease in American patients. Hepatology. 2003;37(5):1114–1121. doi:10.1053/jhep.2003.50195
31. Yu R, Tan Z, Xiang X, Dan Y, Deng G. Effectiveness of PIVKA-II in the detection of hepatocellular carcinoma based on real-world clinical data. BMC Cancer. 2017;17(1):608. doi:10.1186/s12885-017-3609-6
32. Shiraki K, Takase K, Tameda Y, Hamada M, Kosaka Y, Nakano T. A clinical study of lectin-reactive alpha-fetoprotein as an early indicator of hepatocellular carcinoma in the follow-up of cirrhotic patients. Hepatology. 1995;22(3):802–807. doi:10.1002/hep.1840220317
33. Lok AS, Sterling RK, Everhart JE, et al. Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma. Gastroenterology. 2010;138(2):493–502. doi:10.1053/j.gastro.2009.10.031
34. Choi J, Kim GA, Han S, Lee W, Chun S, Lim YS. Longitudinal assessment of three serum biomarkers to detect very early-stage hepatocellular carcinoma. Hepatology. 2019;69(5):1983–1994. doi:10.1002/hep.30233
35. Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev. 2014;23(1):144–153. doi:10.1158/1055-9965.EPI-13-0870
36. Yang JD, Addissie BD, Mara KC, et al. GALAD score for hepatocellular carcinoma detection in comparison with liver ultrasound and proposal of GALADUS score. Cancer Epidemiol Biomarkers Prev. 2019;28(3):531–538. doi:10.1158/1055-9965.EPI-18-0281
37. Singal AG, Tayob N, Mehta A, et al. GALAD demonstrates high sensitivity for HCC surveillance in a cohort of patients with cirrhosis. Hepatology. 2022;75(3):541–549. doi:10.1002/hep.32185
38. Tayob N, Kanwal F, Alsarraj A, Hernaez R, El-Serag HB. The performance of AFP, AFP-3, DCP as biomarkers for detection of Hepatocellular Carcinoma (HCC): a phase 3 biomarker study in the United States. Clin Gastroenterol Hepatol. 2022;S1542–3565(22)00106–9. doi:10.1016/j.cgh.2022.01.047
39. Sherman M, Feld J, Yamada H, Mori Y, Janssen H. A randomized controlled trial of US vs US + biomarkers for the diagnosis of hepatocellular carcinoma: an interim report. J Hepatol. 2017;1:S13. doi:10.1016/S0168-8278(17)30288-X
40. Debes JD, Romagnoli PA, Prieto J, et al. Serum biomarkers for the prediction of hepatocellular carcinoma. Cancers. 2021;13(7):1681. doi:10.3390/cancers13071681
41. Ye X, Li C, Zu X, et al. A large-scale multicenter study validates aldo-keto reductase family 1 member B10 as a prevalent serum marker for detection of hepatocellular carcinoma. Hepatology. 2019;69(6):2489–2501. doi:10.1002/hep.30519
42. Shen Q, Fan J, Yang XR, et al. Serum DKK1 as a protein biomarker for the diagnosis of hepatocellular carcinoma: a large-scale, multicentre study. Lancet Oncol. 2012;13(8):817–826. doi:10.1016/S1470-2045(12)70233-4
43. Xu D, Su C, Sun L, Gao Y, Li Y. Performance of serum glypican 3 in diagnosis of hepatocellular carcinoma: a meta-analysis. Ann Hepatol. 2019;18(1):58–67. doi:10.5604/01.3001.0012.7863
44. Z S, L M, Z X, et al. The diagnostic value of the combination of Golgi protein 73, glypican-3 and alpha-fetoprotein in hepatocellular carcinoma: a diagnostic meta-analysis. Ann Transl Med. 2020;8(8). doi:10.21037/atm.2020.02.89
45. Liu J, Dang H, Wang XW. The significance of intertumor and intratumor heterogeneity in liver cancer. Exp Mol Med. 2018;50(1):e416–e416. doi:10.1038/emm.2017.165
46. Ahn JC, Teng PC, Chen PJ, et al. Detection of circulating tumor cells and their implications as a biomarker for diagnosis, prognostication, and therapeutic monitoring in hepatocellular carcinoma. Hepatology. 2021;73(1):422–436. doi:10.1002/hep.31165
47. Wu J, Hu S, Zhang L, et al. Tumor circulome in the liquid biopsies for cancer diagnosis and prognosis. Theranostics. 2020;10(10):4544–4556. doi:10.7150/thno.40532
48. Ye Q, Ling S, Zheng S, Xu X. Liquid biopsy in hepatocellular carcinoma: circulating tumor cells and circulating tumor DNA. Mol Cancer. 2019;18(1):114. doi:10.1186/s12943-019-1043-x
49. Wu X, Li J, Gassa A, et al. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int J Biol Sci. 2020;16(9):1551–1562. doi:10.7150/ijbs.44024
50. Tran NH, Kisiel J, Roberts LR. Using cell-free DNA for HCC surveillance and prognosis. JHEP Rep. 2021;3(4):100304. doi:10.1016/j.jhepr.2021.100304
51. Yang B, Guo M, Herman JG, Clark DP. Aberrant promoter methylation profiles of tumor suppressor genes in hepatocellular carcinoma. Am J Pathol. 2003;163(3):1101–1107. doi:10.1016/S0002-9440(10)63469-4
52. Lewin J, Kottwitz D, Aoyama J, et al. Plasma cell free DNA methylation markers for hepatocellular carcinoma surveillance in patients with cirrhosis: a case control study. BMC Gastroenterol. 2021;21:136. doi:10.1186/s12876-021-01714-8
53. Chalasani NP, Porter K, Bhattacharya A, et al. Validation of a novel multitarget blood test shows high sensitivity to detect early stage hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2022;20(1):173–182.e7. doi:10.1016/j.cgh.2021.08.010
54. Chalasani NP, Ramasubramanian TS, Bhattacharya A, et al. A novel blood-based panel of methylated DNA and protein markers for detection of early-stage hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2021;19(12):2597–2605.e4. doi:10.1016/j.cgh.2020.08.065
55. Xu RH, Wei W, Krawczyk M, et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat Mater. 2017;16(11):1155–1161. doi:10.1038/nmat4997
56. Roy D, Taggart D, Zheng L, et al. Abstract 837: circulating cell-free DNA methylation assay: towards early detection of multiple cancer types. Cancer Res. 2019;79(13_Supplement):837. doi:10.1158/1538-7445.AM2019-837
57. Alix-Panabières C, Pantel K. Circulating tumor cells: liquid biopsy of cancer. Clin Chem. 2013;59(1):110–118. doi:10.1373/clinchem.2012.194258
58. Kelley RK, Magbanua MJM, Butler TM, et al. Circulating tumor cells in hepatocellular carcinoma: a pilot study of detection, enumeration, and next-generation sequencing in cases and controls. BMC Cancer. 2015;15(1):206. doi:10.1186/s12885-015-1195-z
59. Schulze K, Gasch C, Staufer K, et al. Presence of EpCAM-positive circulating tumor cells as biomarker for systemic disease strongly correlates to survival in patients with hepatocellular carcinoma. Int J Cancer. 2013;133(9):2165–2171. doi:10.1002/ijc.28230
60. Guo W, Yang XR, Sun YF, et al. Clinical significance of EpCAM mRNA-positive circulating tumor cells in hepatocellular carcinoma by an optimized negative enrichment and qRT-PCR–based platform. Clin Cancer Res. 2014;20(18):4794–4805. doi:10.1158/1078-0432.CCR-14-0251
61. Sun C, Liao W, Deng Z, et al. The diagnostic value of assays for circulating tumor cells in hepatocellular carcinoma. Medicine. 2017;96(29):e7513. doi:10.1097/MD.0000000000007513
62. Cui K, Ou Y, Shen Y, Li S, Sun Z. Clinical value of circulating tumor cells for the diagnosis and prognosis of hepatocellular carcinoma (HCC). Medicine. 2020;99(40):e22242. doi:10.1097/MD.0000000000022242
63. Court CM, Hou S, Winograd P, et al. A novel multimarker assay for the phenotypic profiling of circulating tumor cells in hepatocellular carcinoma. Liver Transplant. 2018;24(7):946–960. doi:10.1002/lt.25062
64. Qi LN, Xiang BD, Wu FX, et al. Circulating tumor cells undergoing EMT provide a metric for diagnosis and prognosis of patients with hepatocellular carcinoma. Cancer Res. 2018;78(16):4731–4744. doi:10.1158/0008-5472.CAN-17-2459
65. Shi KQ, Lin Z, Chen XJ, et al. Hepatocellular carcinoma associated microRNA expression signature: integrated bioinformatics analysis, experimental validation and clinical significance. Oncotarget. 2015;6(28):25093–25108. doi:10.18632/oncotarget.4437
66. Zekri ARN, Youssef ASED, El-Desouky ED, et al. Serum microRNA panels as potential biomarkers for early detection of hepatocellular carcinoma on top of HCV infection. Tumor Biol. 2016;37(9):12273–12286. doi:10.1007/s13277-016-5097-8
67. Lin XJ, Chong Y, Guo ZW, et al. A serum microRNA classifier for early detection of hepatocellular carcinoma: a multicentre, retrospective, longitudinal biomarker identification study with a nested case-control study. Lancet Oncol. 2015;16(7):804–815. doi:10.1016/S1470-2045(15)00048-0
68. Duvoux C, Roudot-Thoraval F, Decaens T, et al. Liver transplantation for hepatocellular carcinoma: a model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology. 2012;143(4):986–994.e3; quiz e14–15. doi:10.1053/j.gastro.2012.05.052
69. Llovet JM, Peña CEA, Lathia CD, et al. Plasma biomarkers as predictors of outcome in patients with advanced hepatocellular carcinoma. Clin Cancer Res. 2012;18(8):2290–2300. doi:10.1158/1078-0432.CCR-11-2175
70. Raoul JL, Bruix J, Greten TF, et al. Relationship between baseline hepatic status and outcome, and effect of sorafenib on liver function: SHARP trial subanalyses. J Hepatol. 2012;56(5):1080–1088. doi:10.1016/j.jhep.2011.12.009
71. Bruix J, Cheng AL, Meinhardt G, Nakajima K, De Sanctis Y, Llovet J. Prognostic factors and predictors of sorafenib benefit in patients with hepatocellular carcinoma: analysis of two phase III studies. J Hepatol. 2017;67(5):999–1008. doi:10.1016/j.jhep.2017.06.026
72. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
73. Montal R, Andreu-Oller C, Bassaganyas L, et al. Molecular portrait of high alpha-fetoprotein in hepatocellular carcinoma: implications for biomarker-driven clinical trials. Br J Cancer. 2019;121(4):340–343. doi:10.1038/s41416-019-0513-7
74. Saito Y, Shimada M, Utsunomiya T, et al. Prediction of recurrence of hepatocellular carcinoma after curative hepatectomy using preoperative Lens culinaris agglutinin-reactive fraction of alpha-fetoprotein. Hepatol Res. 2012;42(9):887–894. doi:10.1111/j.1872-034X.2012.01004.x
75. Kiriyama S, Uchiyama K, Ueno M, et al. Triple positive tumor markers for hepatocellular carcinoma are useful predictors of poor survival. Ann Surg. 2011;254(6):984–991. doi:10.1097/SLA.0b013e3182215016
76. Fujiki M, Takada Y, Ogura Y, et al. Significance of des-gamma-carboxy prothrombin in selection criteria for living donor liver transplantation for hepatocellular carcinoma. Am J Transplant. 2009;9(10):2362–2371. doi:10.1111/j.1600-6143.2009.02783.x
77. Shindoh J, Sugawara Y, Nagata R, et al. Evaluation methods for pretransplant oncologic markers and their prognostic impacts in patient undergoing living donor liver transplantation for hepatocellular carcinoma. Transpl Int. 2014;27(4):391–398. doi:10.1111/tri.12274
78. Taketomi A, Sanefuji K, Soejima Y, et al. Impact of des-gamma-carboxy prothrombin and tumor size on the recurrence of hepatocellular carcinoma after living donor liver transplantation. Transplantation. 2009;87(4):531–537. doi:10.1097/TP.0b013e3181943bee
79. Carr BI, Kanke F, Wise M, Satomura S. Clinical evaluation of lens culinaris agglutinin-reactive α-fetoprotein and des-γ-carboxy prothrombin in histologically proven hepatocellular carcinoma in the United States. Dig Dis Sci. 2007;52(3):776–782. doi:10.1007/s10620-006-9541-2
80. Toyoda H, Kumada T, Osaki Y, et al. Staging hepatocellular carcinoma by a novel scoring system (BALAD score) based on serum markers. Clin Gastroenterol Hepatol. 2006;4(12):1528–1536. doi:10.1016/j.cgh.2006.09.021
81. Fox R, Berhane S, Teng M, et al. Biomarker-based prognosis in hepatocellular carcinoma: validation and extension of the BALAD model. Br J Cancer. 2014;110(8):2090–2098. doi:10.1038/bjc.2014.130
82. Toyoda H, Tada T, Johnson PJ, et al. Validation of serological models for staging and prognostication of HCC in patients from a Japanese nationwide survey. J Gastroenterol. 2017;52(10):1112–1121. doi:10.1007/s00535-017-1321-6
83. Berhane S, Toyoda H, Tada T, et al. Role of the GALAD and BALAD-2 serologic models in diagnosis of hepatocellular carcinoma and prediction of survival in patients. Clin Gastroenterol Hepatol. 2016;14(6):875–886.e6. doi:10.1016/j.cgh.2015.12.042
84. Wongjarupong N, Negron-Ocasio GM, Mara KC, et al. BALAD and BALAD-2 predict survival of hepatocellular carcinoma patients: a North American cohort study. HPB. 2021;23(5):762–769. doi:10.1016/j.hpb.2020.09.014
85. Finn RS, Kudo M, Cheng AL, et al. Pharmacodynamic biomarkers predictive of survival benefit with lenvatinib in unresectable hepatocellular carcinoma: from the phase III REFLECT study. Clin Cancer Res. 2021;27(17):4848–4858. doi:10.1158/1078-0432.CCR-20-4219
86. Llovet JM, Singal AG, Villanueva A, et al. Prognostic and predictive factors in patients with advanced HCC and elevated alpha-fetoprotein treated with ramucirumab in two randomized phase III trials. Clin Cancer Res. 2022;28(11):2297–2305. doi:10.1158/1078-0432.CCR-21-4000
87. Teufel M, Seidel H, Köchert K, et al. Biomarkers associated with response to regorafenib in patients with hepatocellular carcinoma. Gastroenterology. 2019;156(6):1731–1741. doi:10.1053/j.gastro.2019.01.261
88. Zhu AX, Abbas AR, de Galarreta MR, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat Med. 2022;28(8):1599–1611. doi:10.1038/s41591-022-01868-2
89. Rimassa L, Kelley RK, Meyer T, et al. Outcomes based on plasma biomarkers for the phase 3 CELESTIAL trial of cabozantinib versus placebo in advanced hepatocellular carcinoma. Liver Cancer. 2022;11(1):38–47. doi:10.1159/000519867
90. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
91. Sangro B, Melero I, Wadhawan S, et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J Hepatol. 2020;73(6):1460–1469. doi:10.1016/j.jhep.2020.07.026
92. Yau T, Kang YK, Kim TY, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564. doi:10.1001/jamaoncol.2020.4564
93. Yau T, Park JW, Finn RS, et al. Nivolumab versus sorafenib in advanced hepatocellular carcinoma (CheckMate 459): a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2022;23(1):77–90. doi:10.1016/S1470-2045(21)00604-5
94. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
95. Neely J, Yao J, Kudo M, et al. Abstract 2145: genomic and transcriptomic analyses related to the clinical efficacy of first-line nivolumab in advanced hepatocellular carcinoma from the phase 3 CheckMate 459 trial. Cancer Res. 2022;82(12_Supplement):2145. doi:10.1158/1538-7445.AM2022-2145
96. Kaseb AO, Guan Y, Gok Yavuz B, et al. Serum IGF-1 scores and clinical outcomes in the phase III imbrave150 study of atezolizumab plus bevacizumab versus sorafenib in patients with unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2022;9:1065–1079. doi:10.2147/JHC.S369951
97. Zhu AX, Dayyani F, Yen CJ, et al. Alpha-fetoprotein as a potential surrogate biomarker for atezolizumab + bevacizumab treatment of hepatocellular carcinoma. Clin Cancer Res. 2022;28(16):3537–3545. doi:10.1158/1078-0432.CCR-21-3275
98. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
99. Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. doi:10.1016/S1470-2045(08)70285-7
100. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
101. Zhu AX, Park JO, Ryoo BY, et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): a randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015;16(7):859–870. doi:10.1016/S1470-2045(15)00050-9
102. Boilève A, Hilmi M, Delaye M, Tijeras-Raballand A, Neuzillet C. Biomarkers in hepatobiliary cancers: what is useful in clinical practice? Cancers. 2021;13(11):2708. doi:10.3390/cancers13112708
103. Abou-Alfa GK, Meyer T, Cheng AL, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
104. Kelley RK, Rimassa L, Cheng AL, et al. Cabozantinib plus atezolizumab versus sorafenib for advanced hepatocellular carcinoma (COSMIC-312): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2022;23(8):995–1008. doi:10.1016/S1470-2045(22)00326-6
105. Wei F, Zhong S, Ma Z, et al. Strength of PD-1 signaling differentially affects T-cell effector functions. Proc Natl Acad Sci USA. 2013;110(27):E2480–E2489. doi:10.1073/pnas.1305394110
106. Elliott LA, Doherty GA, Sheahan K, Ryan EJ. Human tumor-infiltrating myeloid cells: phenotypic and functional diversity. Front Immunol. 2017;8:86. doi:10.3389/fimmu.2017.00086
107. Hong JY, Cho HJ, Sa JK, et al. Hepatocellular carcinoma patients with high circulating cytotoxic T cells and intra-tumoral immune signature benefit from pembrolizumab: results from a single-arm phase 2 trial. Genome Med. 2022;14(1):1. doi:10.1186/s13073-021-00995-8
108. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
109. Abdel-Wahab R, Shehata S, Hassan MM, et al. Type I insulin-like growth factor as a liver reserve assessment tool in hepatocellular carcinoma. J Hepatocell Carcinoma. 2015;2:131–142. doi:10.2147/JHC.S81309
110. Wang J, Huang A, Wang YP, et al. Circulating tumor DNA correlates with microvascular invasion and predicts tumor recurrence of hepatocellular carcinoma. Ann Transl Med. 2020;8(5):237. doi:10.21037/atm.2019.12.154
111. Zhou L, Xu Y, Wang D, et al. Perioperative circulating tumor DNA analysis to predict patient prognosis in liver cancer. JCO. 2020;38(15_suppl):4593. doi:10.1200/JCO.2020.38.15_suppl.4593
112. Huang A, Guo DZ, Zhang X, et al. Application of circulating tumor DNA for prediction and surveillance of tumor recurrence after liver transplantation: a pilot study. JCO. 2022;40(16_suppl):e16149–e16149. doi:10.1200/JCO.2022.40.16_suppl.e16149
113. Jiang N, Zeng X, Tang J, et al. Circulating tumor DNA is a potential prognostic risk factor of recurrence in patients with hepatocellular carcinoma treated by liver transplantation. JCO. 2022;40(16_suppl):e16196–e16196. doi:10.1200/JCO.2022.40.16_suppl.e16196
114. Zhu GQ, Liu WR, Tang Z, et al. Serial circulating tumor DNA to predict early recurrence in patients with hepatocellular carcinoma: a prospective study. Mol Oncol. 2022;16(2):549–561. doi:10.1002/1878-0261.13105
115. Kim SS, Eun JW, Choi JH, et al. MLH1 single-nucleotide variant in circulating tumor DNA predicts overall survival of patients with hepatocellular carcinoma. Sci Rep. 2020;10(1):17862. doi:10.1038/s41598-020-74494-y
116. Hsu CH, Lu S, Abbas A, et al. Longitudinal and personalized detection of circulating tumor DNA (ctDNA) for monitoring efficacy of atezolizumab plus bevacizumab in patients with unresectable hepatocellular carcinoma (HCC). JCO. 2020;38(15_suppl):3531. doi:10.1200/JCO.2020.38.15_suppl.3531
117. von Felden J, Craig AJ, Garcia-Lezana T, et al. Mutations in circulating tumor DNA predict primary resistance to systemic therapies in advanced hepatocellular carcinoma. Oncogene. 2021;40(1):140–151. doi:10.1038/s41388-020-01519-1
118. Morishita A, Oura K, Tadokoro T, Fujita K, Tani J, Masaki T. MicroRNAs in the pathogenesis of hepatocellular carcinoma: a review. Cancers. 2021;13(3):514. doi:10.3390/cancers13030514
119. Sorop A, Constantinescu D, Cojocaru F, Dinischiotu A, Cucu D, Dima SO. Exosomal microRNAs as biomarkers and therapeutic targets for hepatocellular carcinoma. Int J Mol Sci. 2021;22(9):4997. doi:10.3390/ijms22094997
120. Zhou Y, Wang B, Wu J, et al. Association of preoperative EpCAM circulating tumor cells and peripheral treg cell levels with early recurrence of hepatocellular carcinoma following radical hepatic resection. BMC Cancer. 2016;16:506. doi:10.1186/s12885-016-2526-4
121. Wang Z, Luo L, Cheng Y, et al. Correlation between postoperative early recurrence of hepatocellular carcinoma and mesenchymal circulating tumor cells in peripheral blood. J Gastrointest Surg. 2018;22(4):633–639. doi:10.1007/s11605-017-3619-3
122. Ou H, Huang Y, Xiang L, et al. Circulating tumor cell phenotype indicates poor survival and recurrence after surgery for hepatocellular carcinoma. Dig Dis Sci. 2018;63(9):2373–2380. doi:10.1007/s10620-018-5124-2
123. Altman DG, McShane LM, Sauerbrei W, Taube SE. Reporting recommendations for tumor marker prognostic studies (REMARK): explanation and elaboration. BMC Med. 2012;10(1):51. doi:10.1186/1741-7015-10-51
124. Borges KA, Dai J, Parikh ND, et al. Rationale and design of the hepatocellular carcinoma early detection strategy study: a multi-center longitudinal initiative of the national cancer institute’s early detection research network. Contemp Clin Trials. 2019;76:49–54. doi:10.1016/j.cct.2018.11.008
125. Feng Z, Marrero JA, Khaderi S, et al. Design of the Texas hepatocellular carcinoma consortium cohort study. Am J Gastroenterol. 2019;114(3):530–532. doi:10.14309/ajg.0000000000000068
126. Tsuchiya N, Sawada Y, Endo I, Saito K, Uemura Y, Nakatsura T. Biomarkers for the early diagnosis of hepatocellular carcinoma. World J Gastroenterol. 2015;21(37):10573–10583. doi:10.3748/wjg.v21.i37.10573
127. Kim BK, Cheon J, Kim H, et al. Atezolizumab/bevacizumab vs. lenvatinib as first-line therapy for unresectable hepatocellular carcinoma: a real-world, multi-center study. Cancers. 2022;14(7):1747. doi:10.3390/cancers14071747
128. Rimini M, Rimassa L, Ueshima K, et al. Atezolizumab plus bevacizumab versus lenvatinib or sorafenib in non-viral unresectable hepatocellular carcinoma: an international propensity score matching analysis. ESMO Open. 2022;7(6):100591. doi:10.1016/j.esmoop.2022.100591
129. Fang JH, Xu L, Shang LR, et al. Vessels That Encapsulate Tumor Clusters (VETC) pattern is a predictor of sorafenib benefit in patients with hepatocellular carcinoma. Hepatology. 2019;70(3):824–839. doi:10.1002/hep.30366
130. Chin RI, Chen K, Usmani A, et al. Detection of solid tumor Molecular Residual Disease (MRD) using Circulating Tumor DNA (ctDNA). Mol Diagn Ther. 2019;23(3):311–331. doi:10.1007/s40291-019-00390-5
131. Tie J, Wang Y, Tomasetti C, et al. Circulating tumor DNA analysis detects minimal residual disease and predicts recurrence in patients with stage II colon cancer. Sci Transl Med. 2016;8(346):346ra92. doi:10.1126/scitranslmed.aaf6219
132. Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021;595(7867):432–437. doi:10.1038/s41586-021-03642-9
133. Kudo M, Ueshima K, Nakahira S, et al. Final results of adjuvant nivolumab for hepatocellular carcinoma (HCC) after surgical resection (SR) or radiofrequency ablation (RFA) (NIVOLVE): a phase 2 prospective multicenter single-arm trial and exploratory biomarker analysis. JCO. 2022;40(4_suppl):416. doi:10.1200/JCO.2022.40.4_suppl.416
134. Xia Y, Tang W, Qian X, et al. Efficacy and safety of camrelizumab plus apatinib during the perioperative period in resectable hepatocellular carcinoma: a single-arm, open label, phase II clinical trial. J Immunother Cancer. 2022;10(4):e004656. doi:10.1136/jitc-2022-004656
135. Natera. Natera launches initiative to transform the management of cancer patients in organ transplantation; 2020. Available from: https://www.natera.com/company/news/natera-launches-initiative-to-transform-the-management-of-cancer-patients-in-organ-transplantation-2/.
136. Chow P, Chen M, Cheng AL, et al. Abstract CT003: iMbrave050: phase 3 study of adjuvant atezolizumab + bevacizumab versus active surveillance in patients with hepatocellular carcinoma (HCC) at high risk of disease recurrence following resection or ablation. Cancer Res. 2023;83(8_Supplement):CT003. doi:10.1158/1538-7445.AM2023-CT003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.