Back to Journals » Clinical Interventions in Aging » Volume 21
Exercise, Ethnicity, and Quality of Life in Older Adults with Persistent Nonvalvular Atrial Fibrillation: A Multicenter Cross-Sectional Study
Authors Xu Y ![]() , Zhao X, Zheng X, Shi S, Lv F, Dong R, Liu K
, Zhao X, Zheng X, Shi S, Lv F, Dong R, Liu K
Received 27 January 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:21 599331
DOI https://doi.org/10.2147/CIA.S599331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Yankai Xu,1– 3,* Xia Zhao,2,3,* Xin Zheng,3,4,* Shilin Shi,5 Fuqiang Lv,1– 3 Runtian Dong,1– 3 Kejian Liu3,4
1Department of General Medicine, The First Affiliated Hospital of Shihezi University, Shihezi City, Xinjiang, People’s Republic of China; 2Clinical College of Shihezi University, Shihezi City, Xinjiang, People’s Republic of China; 3Key Laboratory of Central Asian High Disease Prevention and Control, National Health Commission, Shihezi City, People’s Republic of China; 4Department of Cardiology, First Affiliated Hospital of Shihezi University, Shihezi City, Xinjiang, People’s Republic of China; 5Department of Cardiology, Shihezi People’s Hospital, Shihezi City, Xinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kejian Liu, Email [email protected]
Purpose: This study assessed quality of life and its determinants, including age and ethnicity, among elderly patients with persistent nonvalvular atrial fibrillation (NVAF) in Xinjiang, aiming to provide clinical evidence for targeted interventions.
Patients and Methods: A multicenter cross-sectional study enrolled 123 patients (≥ 65 years old) with persistent NVAF. QoL was evaluated using the EQ-5D-5L scale. Ordered logistic regression identified predictors of five EQ-5D-5L dimensions of QoL.
Results: The median EQ-5D-5L utility score was 0.654. Ordered logistic regression analysis revealed that age≥ 75 years was significantly associated with poorer QoL in the domains of mobility (OR=6.30, 95% CI: 2.49– 15.94), self-care (OR=10.73, 95% CI: 3.87– 29.70), daily activities (OR=9.23, 95% CI: 1.82– 46.94), and pain/discomfort (OR=3.51, 95% CI: 1.40– 8.79). Ethnic minority status was a protective factor for self-care (OR=0.25, 95% CI: 0.08– 0.81), pain/discomfort (OR=0.30, 95% CI: 0.12– 0.71), and anxiety/depression (OR=0.13, 95% CI: 0.05– 0.35). Regular exercise (≥ 90 minutes/week) reduced the risks of self-care (OR=0.15, 95% CI: 0.03– 0.87) and daily activities (OR=0.10, 95% CI: 0.01– 0.81). Female sex was protective for pain/discomfort (OR=0.31, 95% CI: 0.13– 0.73) and anxiety/depression (OR=0.17, 95% CI: 0.06– 0.45). Conversely, regular medication use was unexpectedly associated with increased anxiety/depression risk (OR=9.47, 95% CI: 1.46– 61.46).
Conclusion: Age, ethnicity, and physical activity impact QoL in elderly NVAF patients. These findings support the need for age-specific and culturally tailored interventions, including structured exercise programs and personalized care strategies.
Keywords: atrial fibrillation, elderly, quality of life, ethnic disparities, exercise
Introduction
Atrial fibrillation (AF) is usually the most common sustained arrhythmia and associated by increased atrial remodeling characterized by profound structural, electrical, and functional changes, which can cause disability, thromboembolic events, or death, while also imposing a substantial burden on patients’ physical and psychological well-being.1 According to statistics, the global incidence of atrial fibrillation has increased by 33% in the past 20 years,2 and it is expected that by 2050, the global growth rate of this disease will exceed 60%, with low- and middle-income countries facing disproportionate impacts due to healthcare disparities. In China, the AF epidemic is accelerating, with approximately 9 million elderly patients currently affected, posing significant challenges for public health systems.3 Persistent nonvalvular atrial fibrillation (NVAF), defined as AF lasting more than seven days in the absence of significant valvular pathology, represents a distinct clinical entity with unique management challenges.4
Although the impact of AF on morbidity and mortality is well-documented, evidence specifically addressing quality of life (QoL) in elderly patients with persistent NVAF—particularly within multi-ethnic contexts—remains limited.5 In Xinjiang, a multi-ethnic region with diverse lifestyles and healthcare access, the prevalence of AF in the elderly was 2.56%, much higher than the national average (1.83%).6 This disparity may reflect regional differences in diet, genetic predispositions, or uneven healthcare resources, underscoring the need for localized studies.
The European Quality of Life Scale (EQ-5D-5L) is a standardized scale validated across cultures to describe and evaluate the health status of patients with chronic diseases from the five dimensions of mobility, self-care, daily activities, pain/discomfort and anxiety/depression.7,8 Furthermore, while factors such as age, comorbidities, and treatment adherence have been widely examined in NVAF, the influence of ethnicity and lifestyle factors—such as physical activity—on QoL in NVAF patients warrants further exploration.9,10 In this study, EQ-5D-5L scale (Chinese version) was used to evaluate elderly patients with persistent atrial fibrillation in some areas of Xinjiang, a region where ethnic diversity and socioeconomic factors may modulate QoL differently than in homogeneous populations. And the factors associated with QoL were also analyzed, so as to provide clinical data that can inform the development of practical, actionable interventions for the management of elderly patients with persistent NVAF in Xinjiang.
Material and Methods
Study Design and Participants
The study was approved by the Ethics Committee of the First Affiliated Hospital of Shihezi University (Approval KJ2023-176-01). All participants were informed about the study protocol and provided written informed consent to participate in the study. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
This is a cross-sectional study, so only associations rather than causal relationships could be identified between exercise, ethnicity and QoL. From October 2023 to November 2024, field investigation was conducted in elderly patients with persistent nonvalvular atrial fibrillation admitted to four hospitals in Yanqi, Tumshuk, Kashgar and Shihezi, Xinjiang. Shihezi was chosen as it has the largest Han population in Xinjiang, while Kashgar represents the region with the highest Uyghur population concentration. Additionally, Yanqi and Tumshuk were included as they constitute the largest agricultural divisions in southern Xinjiang under the Xinjiang Production and Construction Corps system. This strategic selection ensured comprehensive geographic, ethnic, and socioeconomic representation across Xinjiang’s diverse population.
Inclusion criteria: (1) aged ≥65 years, with clear consciousness and normal communication ability; (2) Electrocardiogram or 24 h Holter electrocardiogram suggested atrial fibrillation; (3) persistent nonvalvular atrial fibrillation (Diagnostic criteria: Persistent atrial fibrillation was diagnosed according to Atrial Fibrillation Diagnosis and Treatment (2023)8); (4) Obtain the informed consent of the patient and sign the informed consent.
Exclusion criteria: (1) Valvular AF or status post heart valve replacement; (2) Heart dysfunction, NYHA grade III or above (Patients with NYHA functional class ≥ III heart failure were excluded because severe heart failure independently severely impairs quality of life and may confound the observed associations between AF and QoL); (3) Malignant tumors and life expectancy less than 1 year; (4) Severe hepatic and renal insufficiency [ALT (alanine aminotransferase) > 120U/L; eGFR < 15mL/(min*1.73m2)]; (5) In the acute stage of the disease treatment; (6) Has done or is undergoing drug weight loss or surgical weight loss; (7) Suffering from mental or mental illness; (8) Follow-up data were incomplete.
Sampling method: The continuous sampling method was used to select patients who met the inclusion and exclusion criteria.
Outcome Measurements
Data were collected at baseline including: general demographic information such as gender, age, ethnicity, and comorbidities, while documenting height, weight (and calculating BMI), medication, diet and exercise. Medication adherence was categorized into three groups: no medication use, regular medication use, and irregular medication use. Regular medication use was defined as taking prescribed drugs daily at each meal in strict accordance with medical instructions. Dietary quality was assessed using the Life’s Essential 8 (LE8) diet score, which rates eating habits based on the number of healthy dietary components met (eg, a score of 100 for meeting 8 items, 80 for 6–7 items, 50 for 4–5 items, 25 for 2–3 items, and 0 for fewer than 2 items).11,12 Physical exercise was classified as no exercise, occasional exercise (<90 minutes/week), or regular exercise (≥90 minutes/week).
The EQ-5D-5L scale was used,13 which included 5 dimensions of mobility, self-care, daily activities, pain/discomfort, and anxiety/depression. Each dimension is divided into five levels: no difficulty, little difficulty, moderate difficulty, severe difficulty, and very severe difficulty. The EQ-5D-5L score is calculated based on the utility value scoring systemdeveloped by the Chinese population.8 The closer the score is to 1, the higher the quality of life score is. The investigators were trained to ask questions according to the contents of the EQ-5D-5L scale and fill in the questionnaire according to the answers of the patients.
The investigators in this study are all post-graduate students and ethnic minority investigators who have received unified training. They ask questions of patients in plain language, and appoint special personnel to check and retrieve questionnaires, and fill in the gaps or omissions in time. All researchers did not interfere with the subjects’ responses.
Sample Size
Sample size was calculated using power analysis (80% statistical power, α=0.05) based on effect sizes from previous studies on AF and QoL.14 The minimum sample size required was 100; we finally enrolled 123 patients to ensure adequate statistical power and compensate for potential data loss.
Statistical Analysis
SPSS 25.0 (IBM Corp., Armonk, NY, USA) was used to analyze the data. The number of use cases of categorical variables (percentage) [n(%)] was described. Continuous variables were assessed for normality and presented as mean±standard deviation if normal distribution and median (quart range)[M(P25-P75)] if skewed distribution. An ordered logistic regression model was applied to assess associations between variables and QoL dimensions. Odds ratios (OR) with 95% confidence intervals (CI) were reported. P< 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 123 elderly patients with persistent NVAF were included, comprising 71 males (57.7%) and 52 females (42.3%). More than half of the participants (n = 63, 51.2%) were aged ≥75 years. Patients younger than 75 years exhibited significantly higher EQ-5D-5L utility scores compared with those aged ≥75 years [0.713 (0.658–0.782) vs. 0.585 (0.379–0.654), P < 0.001]. Han patients accounted for 64.2% (n = 79), while ethnic minority patients constituted 35.8% (n = 44); notably, minority patients reported better quality of life scores than their Han counterparts [0.702 (0.635–0.782) vs. 0.585 (0.471–0.713), P < 0.001].
With respect to BMI, 40.7% of participants had values within the normal range (18.5–24.0 kg/m2). However, no significant differences in QoL were observed across BMI categories (P = 0.140). Multimorbidity was prevalent, with 78 patients (63.4%) presenting with two or more chronic conditions. Hypertension (60.2%), coronary heart disease (68.3%), diabetes (21.1%), and heart failure (46.3%) were the most frequent comorbidities, yet none of these conditions showed a statistically significant association with EQ-5D-5L scores (all P > 0.05). Detailed baseline data are summarized in Table 1.
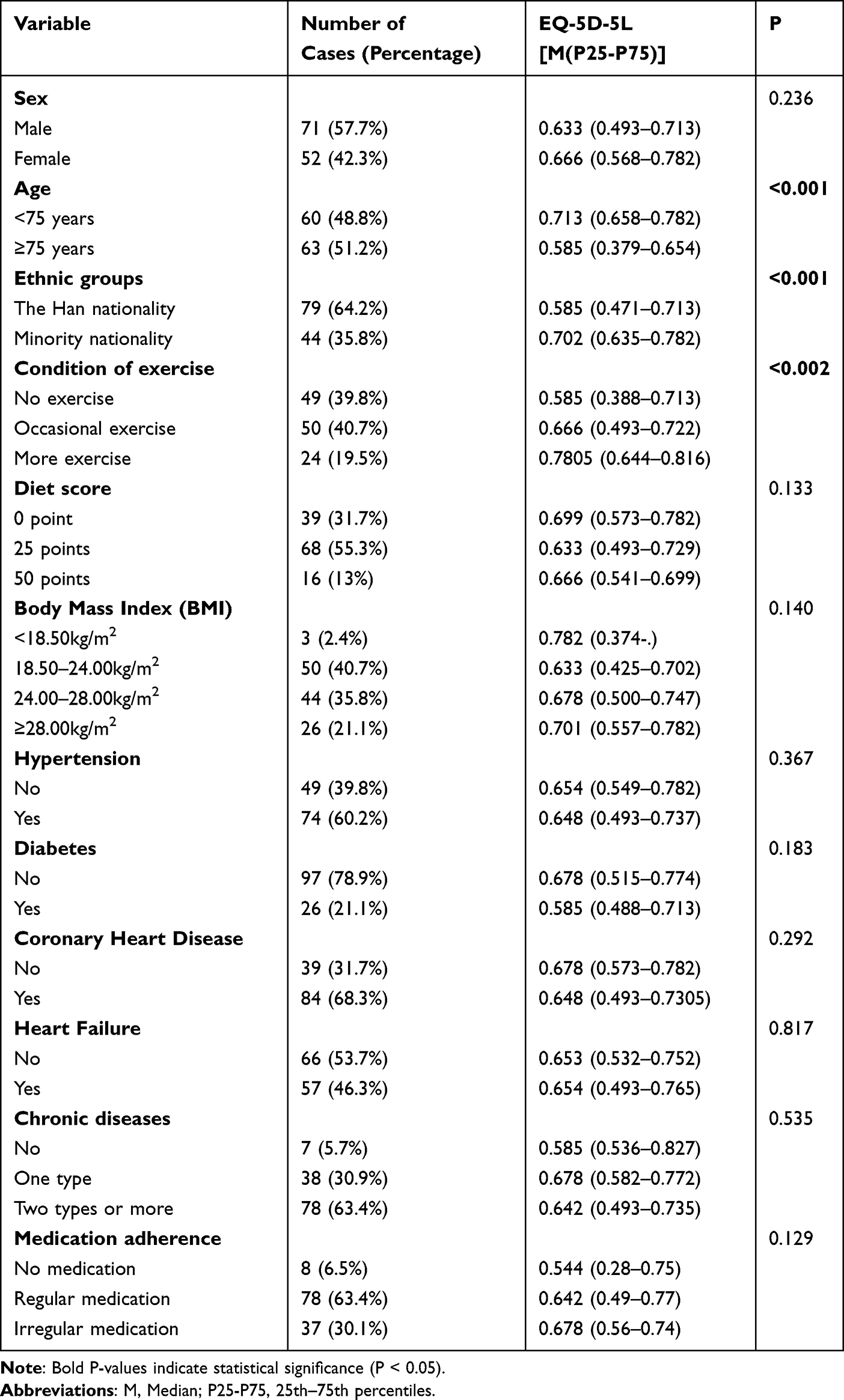 |
Table 1 Baseline Characteristics and EQ-5D-5L Scores of Elderly AF Patients (N=123) |
Quality of Life of Patients with Different Behavioral Habits
According to their weekly exercise duration, 49 patients (39.8%) reported no exercise, 50 (40.7%) engaged in occasional exercise, and 24 (19.5%) participated in regular exercise (≥90 minutes/week). There were significant differences in the quality of life scores of elderly patients with atrial fibrillation in different exercise conditions (P<0.05, Table 1).
Dietary quality, as assessed by the LE8 scoring system, did not show significant associations with QoL (P=0.133). Similarly, no significant differences were identified in relation to medication adherence, although a trend toward lower QoL scores was noted in patients reporting no medication use (median 0.544).
EQ-5D-5L Dimensions
The results showed that the proportion of elderly patients with persistent AF in the five dimensions of mobility, self-care, daily activities, pain/discomfort and anxiety/depression were 82.9%, 45.5%, 88.6%, 100.0% and 100.0%, respectively. Specifically, 52.8% experienced moderate pain/discomfort and an equal proportion reported moderate anxiety/depression, while 13.0% and 6.5% had severe difficulties in these two dimensions, respectively. In contrast, 54.5% reported no difficulties with self-care, although 39.0% experienced some level of impairment. Mild limitations were also common in mobility (53.7%) and daily activities (81.3%) (Figure 1).
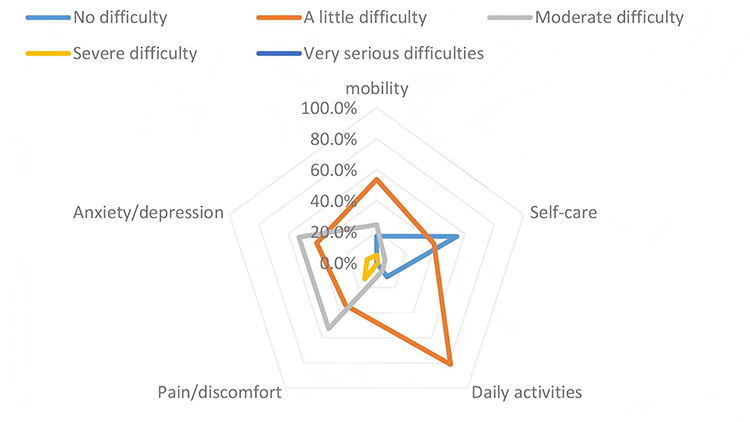 |
Figure 1 EQ-5D-5L limited proportion of each dimension. |
Ordered Logistic Regression Analysis of Quality of Life Score
In the ordered logistic regression analysis, the dependent variable was the five dimensions of the EQ-5D-5L scale (mobility, self-care, usual activities of daily living, pain/discomfort, anxiety/depression), and each dimension was scored on a scale ranging from no difficulty (0 points) to extreme difficulty (5 points) as an ordered outcome variable.
Supplementary univariate regression analysis confirmed that advanced age (≥75 years) markedly increased risks of impaired mobility, self-care, daily activities, and pain/discomfort, while ethnic minority status and regular exercise consistently demonstrated protective effects across several QoL dimensions. These results highlight age, ethnicity, and physical activity as primary determinants of QoL among elderly NVAF patients (Supplementary Table S1).
Ordered logistic regression identified age ≥75 years (advanced age) was an independent risk factor of poorer outcomes in mobility (OR: 6.30, 95% CI: 2.49–15.94), self-care (OR: 10.73, 95% CI: 3.87–29.70), and daily activity (OR: 9.23, 95% CI: 1.82–46.94). Compared with Han, ethnic minorities were protective factors in the dimensions of self-care (OR: 0.25, 95% CI: 0.08–0.81), pain/discomfort (OR: 0.30, 95% CI: 0.12–0.71) and anxiety/depression (OR: 0.13, 95% CI: 0.05–0.35). Female sex was protective for pain/discomfort (OR: 0.31, 95% CI: 0.13–0.73) and anxiety/depression (OR: 0.17, 95% CI: 0.06–0.45). Higher physical activity (≥90 min/week) was associated with some protective effects on the self-care (OR: 0.15, 95% CI: 0.03–0.87) and daily activity (OR: 0.10, 95% CI: 0.01–0.81) dimensions (Table 2).
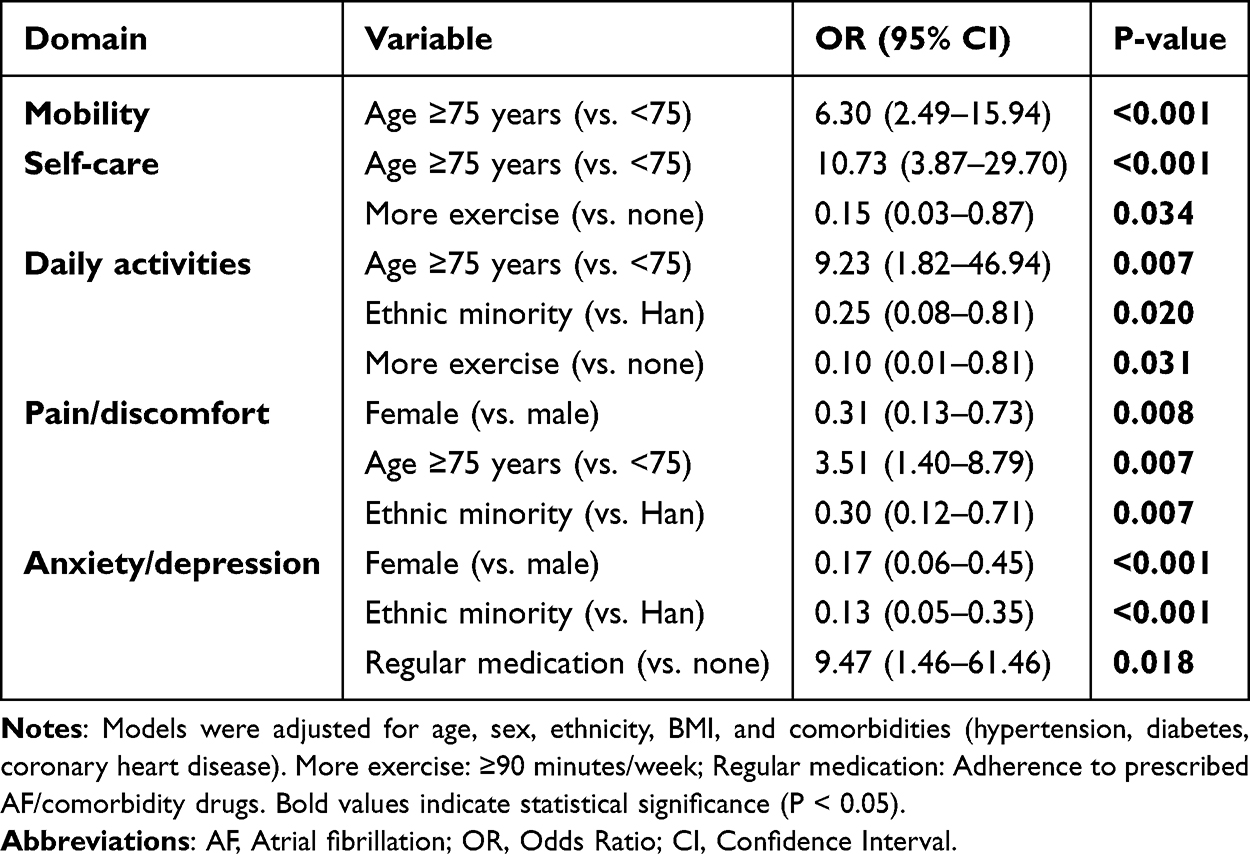 |
Table 2 Multivariable Ordered Logistic Regression Analysis of EQ-5D-5L Domains in Elderly AF Patients |
Discussion
Elderly patients with persistent NVAF commonly experience physiological decline and increased comorbidities (such as hypertension, diabetes, etc). Long-standing atrial arrhythmia may exacerbate ventricular dysfunction, imposing further cardiac burden and limiting mobility, self-care, and daily activities, ultimately diminishing quality of life. In this study, both univariate and multivariate analyses were conducted across the five EQ-5D-5L dimensions. These findings highlight the substantial roles of age, ethnicity and physical activity in determining health-related QoL among elderly patients with NVAF in Xinjiang.
Our analysis demonstrated that patients aged ≥75 years exhibited a significantly higher risk of impairment with regard to mobility, self-care, and activities of daily living. These observations align with previous studies showing that advanced age intensifies the clinical burden of AF, likely due to reduced physiological reserve and greater multimorbidity.15,16 Compared with younger patients with atrial fibrillation, elderly patients with NVAF have poor cardiac reserve function and are more prone to co-morbidity, and the risk of complications can be increased by 2–3 times. The pronounced impact of age on pain/discomfort (OR: 3.51) may further reflect degenerative conditions (eg, osteoarthritis) and underrecognized undertreatment of non-cardiac symptoms in geriatric AF populations. These physical limitations often translate into reduced endurance, chest tightness, and difficulty performing daily tasks, which in turn restrict social participation and gradually erode overall QoL. Therefore, targeted interventions to support basic functional abilities in older adults are essential to mitigate the gap in quality of life between high-aged and younger NVAF patients.
In the dimensions of self-care, daily activities, pain/discomfort, and anxiety/depression, univariate analysis showed protective effects of ethnic minorities across multiple QoL dimensions, and these effects remained significant for pain/discomfort (P=0.007) and anxiety/depression (P<0.001) in multivariate analysis. This suggests that while ethnicity itself may contribute to QoL differences, other interrelated sociocultural and behavioral factors play a mediating role. Similar patterns have been observed in European populations, where racial and ethnic disparities in cardiovascular outcomes persist even after accounting for socioeconomic status, underscoring the complex interplay of biological, cultural, and environmental influences.17
This difference may be related to the behavior of different ethnic groups (most ethnic minorities are nomads), cultural background (religious beliefs, etc), and so on. Many ethnic minority groups in Xinjiang (eg, Kazakh, Uyghur) traditionally live in tight-knit, multigenerational households, fostering strong familial and communal support networks,13 and ethnic minorities are more inclined to live in compact communities to provide family support and care. Such social cohesion has been linked to better mental health and functional independence in elderly populations, potentially buffering against anxiety/depression and self-care limitations. Ethnic minorities in China have different cultural diversity, such as Uygur medicine and Tibetan medicine, which have certain advantages in pain18 and reduce pain perception through analgesia, but it needs further analysis. Eating a diet that does not eat raw meat or dried fruits11 has a certain protective effect on the cardiovascular system and has a certain positive significance in the relief of symptoms, thereby reducing the occurrence of pain and anxiety/depression. Interventions for multi-ethnic populations should incorporate these cultural assets—for example, leveraging extended family support networks and integrating ethnic traditional activities, such as Uyghur dance, into exercise prescriptions—to enhance engagement, mental well-being, and functional outcomes.
Multivariable analysis revealed that regular exercise (≥90 minutes/week) was associated with significant improvements across multiple QoL dimensions. While univariate analysis suggested beneficial effects of exercise on pain/discomfort and anxiety/depression, these associations were no longer statistically significant in multivariable models, likely due to confounding factors, though the potential benefits of physical activity cannot be excluded. The results of this study are consistent with the ESC Guideline 2023, which recommends weekly exercise for patients with atrial fibrillation, suggesting that elderly patients should be advised to do moderate amounts of physical exercise, such as tai chi, etc.19 The mechanisms underlying these improvements are multifaceted. First, exercise enhances cardiovascular and metabolic function, mitigating AF-related symptoms like fatigue and palpitations. Second, it counteracts age-related muscle atrophy and balance decline, thereby preserving functional independence.20,21 Exercise can not only improve heart and lung function, but also promote the release of endorphins, elevate mood, and reduce anxiety and depression symptoms.22 Exercise is also known to enhance mood through endorphin release and to alleviate psychological distress by promoting social interaction and participation. Although evidence for exercise specifically in persistent NVAF remains limited, these results support the inclusion of structured exercise as a core component of individualized interventions for elderly patients, with Tai Chi or Baduanjin23 representing practical options with low cardiac burden and demonstrated benefits for cardiac rehabilitation. These benefits may relate to cultural and social support factors observed in these groups, which were not directly measured and require further research.
Female sex was identified as an independent protective factor against pain/discomfort and anxiety/depression, which may be associated with more sensitive symptom perception and more proactive healthcare-seeking behavior among women.
Hypertension, diabetes mellitus, and heart failure exhibited no significant association with QoL scores. This finding may be attributable to adequate management of disease-related symptoms or the predominant influences of age, ethnicity, and physical activity within the study population.
Regular medication use is associated with an increased risk of anxiety/depression symptoms. This phenomenon may be related to the severity of the disease, side effects of the drugs, or the complexity of the medication regimen, and no classification and comparison of drug types have been conducted; in clinical applications, specific circumstances such as the patient’s income level and accessibility of medical care should also be taken into consideration.
The findings of this study have several practical implications for the management of elderly NVAF patients. First, for patients aged ≥75 years, individualized functional training—such as balance exercises and hand grip training—should be implemented at least three times per week to improve mobility and self-care capacity. Second, in multi-ethnic populations, care strategies should be adapted to cultural characteristics, including leveraging extended family support networks and incorporating ethnic traditional physical activities, such as Uyghur dance, into exercise prescriptions. Third, exercise interventions for elderly NVAF patients should focus on moderate-intensity activities, approximately 30 minutes per session, three times per week, with Tai Chi or Baduanjin preferred due to their low cardiac burden and suitability for older adults. Integrating these targeted strategies may help preserve functional independence, reduce physical limitations, and improve overall quality of life in this vulnerable population.
This study has limitations. First, the cross-sectional design restricts causal inference, and QoL was assessed at a single time point. Second, the sample size, although adequately powered, may still limit generalizability to broader populations. Third, unmeasured confounding factors, such as socioeconomic status and healthcare accessibility, could influence the observed associations. Fourth, this study did not use specific exercise assessment scales such as EHRA score, PASE or 6-Minute Walk Test; exercise was classified by weekly duration, which is a limitation of this study. Despite these limitations, the study provides novel insights into QoL determinants in a multi-ethnic elderly population with NVAF.
Conclusion
In summary, ethnicity, exercise, medication, etc, can be used as influencing factors to affect the quality of life of elderly patients with persistent NVAF. In clinical practice, comprehensive management of elderly NVAF patients should not only focus on symptom control but also emphasize physical activity, social support, and culturally tailored care strategies. Personalized interventions that integrate medical, behavioral, and cultural dimensions may offer the greatest potential to preserve functional independence and improve QoL in this vulnerable population.
Data Sharing Statement
The data underlying this article are available in the article and in its online supplementary material.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the First Affiliated Hospital of Shihezi University (Approval KJ2023-176-01). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Cardiovascular Specialist Alliance of Xinjiang Production and Construction Corps for “Construction and Regional Demonstration of atrial fibrillation Prevention and Control System in Southern Xinjiang (2023AB018-12). Young and Middle-aged Backbone Training Project of “Tianshan Talents” for High-level Medical and Health Personnel in 2024 (CZ001216).
Disclosure
The authors declare that they have no competing interests.
References
1. Yang R, M Liuc, Liao XY. Exploration and consideration on collaborative approach of comprehensive management of atrial fibrillation in tertiary general hospitals and community hospitals. Chin J Gen Med. 2021;24(1):36–9.
2. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16(2):217–221. doi:10.1177/1747493019897870
3. Wang Y, Guo Y, Qin M, et al. 2024 Chinese Expert Consensus Guidelines on the Diagnosis and Treatment of Atrial Fibrillation in the Elderly, Endorsed by Geriatric Society of Chinese Medical Association (Cardiovascular Group) and Chinese Society of Geriatric Health Medicine (Cardiovascular Branch): executive Summary. Thrombosis Haemostasis. 2024;124(10):897–911. doi:10.1055/a-2325-5923
4. Xia Y, Jiang J, Fan F, et al. Prevalence, characteristics, and treatment strategy of different types of heart failure in patients with nonvalvular atrial fibrillation. J Am Heart Assoc. 2024;13(19):e033941. doi:10.1161/jaha.123.033941
5. Gabilondo M, Loza J, Pereda A, et al. Quality of life in patients with nonvalvular atrial fibrillation treated with oral anticoagulants. Hematology. 2021;26(1):277–283. doi:10.1080/16078454.2021.1892329
6. Shi S, Tang Y, Zhao Q, et al. Prevalence and risk of atrial fibrillation in China: a national cross-sectional epidemiological study. Lancet Reg Health Western Pacific. 2022;23:100439. doi:10.1016/j.lanwpc.2022.100439
7. Thompson AJ, Turner AJ. A Comparison of the EQ-5D-3L and EQ-5D-5L. PharmacoEconomics. 2020;38(6):575–591. doi:10.1007/s40273-020-00893-8
8. N Luo, G Liu, Li M. Estimating an EQ-5D-5L value set for China. Value Health. 2017;20(4):662–669. doi:10.1016/j.jval.2016.11.016
9. Varona JF, Seguí-Ripoll JM, Lozano-Duran C, et al. Health-related quality of life in nonvalvular atrial fibrillation patients with controlled or uncontrolled anticoagulation status. Health Qual Life Outcomes. 2020;18(1):383. doi:10.1186/s12955-020-01563-1
10. Atreja N, Johannesen K, Subash R, et al. US cost-effectiveness analysis of apixaban compared with warfarin, dabigatran and rivaroxaban for nonvalvular atrial fibrillation, focusing on equal value of life years and health years in total. J Comparative Effect Res. 2025;14(1):e240163. doi:10.57264/cer-2024-0163
11. Lloyd-Jones DM, Allen NB, Anderson CAM, et al. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation. 2022;146(5):e18–e43. doi:10.1161/cir.0000000000001078
12. Mellen PB, Gao SK, Vitolins MZ, Goff DC Jr. Deteriorating dietary habits among adults with hypertension: DASH dietary accordance, NHANES 1988-1994 and 1999-2004. Arch Internal Med. 2008;168(3):308–314. doi:10.1001/archinternmed.2007.119
13. The EuroQol Group. EuroQol: a new facility for the measurement of health-related quality of life. Health Policy. 1990;16(3):199–208. doi:10.1016/0168-8510(90)90421-9.
14. Abed HS, Wittert GA, Leong DP, et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310(19):2050–2060. doi:10.1001/jama.2013.280521
15. Haller PM, Jarolim P, Palazzolo MG, et al. Heart failure risk assessment using biomarkers in patients with atrial fibrillation: analysis from COMBINE-AF. J Ame College Cardiol. 2024;84(16):1528–1540. doi:10.1016/j.jacc.2024.07.023
16. Marzo RR, Khanal P, Shrestha S, Mohan D, Myint PK, Su TT. Determinants of active aging and quality of life among older adults: systematic review. Front Public Health. 2023;11:1193789. doi:10.3389/fpubh.2023.1193789
17. Khan MS, Shahid I, Bennis A, Rakisheva A, Metra M, Butler J. Global epidemiology of heart failure. Nat Rev Cardiol. 2024;21(10):717–734. doi:10.1038/s41569-024-01046-6
18. Tursun H, Wang C, Abibra A, Baqhsara. Uyghur medicine treatment of chronic pain and advances in modern research. ChinMed. 2026;15(2):116–123. doi:10.12677/tcm.2026.152083
19. Liu T, Chan AW, Liu YH, Taylor-Piliae RE. Effects of Tai Chi-based cardiac rehabilitation on aerobic endurance, psychosocial well-being, and cardiovascular risk reduction among patients with coronary heart disease: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2018;17(4):368–383. doi:10.1177/1474515117749592
20. Kang J, Ratamess NA, Faigenbaum AD, et al. Time-of-day effects of exercise on cardiorespiratory responses and endurance performance-a systematic review and meta-analysis. J Strength Condition Res. 2023;37(10):2080–2090. doi:10.1519/jsc.0000000000004497
21. Yu J, Chun B, Lee D, Rokni L. Effect of baduanjin exercise on metabolic syndrome risk: a systematic review and meta-analysis of randomized controlled trials. Iran J Public Health. 2023;52(5):880–891. doi:10.18502/ijph.v52i5.12705
22. Hossain MN, Lee J, Choi H, Kwak YS, Kim J. The impact of exercise on depression: how moving makes your brain and body feel better. Phys Activity Nutr. 2024;28(2):43–51. doi:10.20463/pan.2024.0015
23. Gao R, Greiner C, Ryuno H, Zhang X. Effects of Tai Chi on physical performance, sleep, and quality of life in older adults with mild to moderate cognitive impairment. BMC Complement Med Therap. 2024;24(1):423. doi:10.1186/s12906-024-04705-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Screening for Atrial Fibrillation by Village Doctors in Rural Areas of China: The Jiangsu Province Rural Community AF Project
Li M, Shi J, Chu M, Shen Y, Zhang S, Sun X, Zhang H, Yan Q, Gong J, Lip GYH, Chen M
Vascular Health and Risk Management 2022, 18:757-766
Published Date: 15 September 2022
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Zhang KD, Wang LY, Zhang ZH, Zhang DX, Lin XW, Meng T, Qi F
Journal of Pain Research 2022, 15:3639-3656
Published Date: 22 November 2022
Adherence to Atrial Fibrillation Better Care (ABC) Pathway Management of Chinese Community Elderly Patients with Atrial Fibrillation: A Cross-Sectional Study
Zhang X, Huang J, Weng F, Wen Y, Wang X, Jiang J, Xue Y, Li K
Patient Preference and Adherence 2023, 17:1813-1823
Published Date: 25 July 2023
Prognosis of Older Adult Patients Suffering from Atrial Fibrillation and Hypokalemia
Wang XD, Wang Y, Liu J, Yao JW, Zhang J, Zhang YN
Clinical Interventions in Aging 2023, 18:1363-1371
Published Date: 17 August 2023
How Do Exercise, Sleep and Depression Affect Disease Scores and Quality of Life in Primary Sjögren’s Syndrome Patients?
Tastekin F, Karatas E, Aydin O, Yargucu Zihni F, Kabasakal Y, Barutcuoglu B, Karabulut G
International Journal of General Medicine 2024, 17:2981-2991
Published Date: 9 July 2024