")
Back to Journals » Journal of Pain Research » Volume 15
Effect of Exercise Interventions on Health-Related Quality of Life in Patients with Fibromyalgia Syndrome: A Systematic Review and Network Meta-Analysis
Authors Zhang KD, Wang LY, Zhang ZH , Zhang DX, Lin XW, Meng T, Qi F
Received 11 August 2022
Accepted for publication 12 November 2022
Published 22 November 2022 Volume 2022:15 Pages 3639—3656
DOI https://doi.org/10.2147/JPR.S384215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Kang-Da Zhang,1 Lin-Yu Wang,1 Zhi-Hua Zhang,1 Dan-Xu Zhang,1 Xiao-Wen Lin,2 Tao Meng,1 Feng Qi1
1Department of Anesthesiology, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 2Department of Pain Management, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, People’s Republic of China
Correspondence: Tao Meng; Feng Qi, Department of Anesthesiology, Qilu Hospital of Shandong University, No.107 Wenhua Xilu, Jinan, Shandong, 250012, People’s Republic of China, Email [email protected]; [email protected]
Objective: Several guidelines highlight the beneficial impact of exercise on the management of symptoms and health-related quality of life (HRQOL) in patients with fibromyalgia syndrome (FMS). However, few analyses have compared different types of exercise. We, therefore, intent to compare the effects of different exercise types on improving the overall HRQOL and typical symptoms in patients with FMS.
Methods: Medline, Embase, the Cochrane Register of Clinical Trials, and NIH ClinicalTrials.gov were searched from inception to April 21, 2022. Randomized clinical trials (RCTs) were included to assess the impact of exercise intervention on health parameters in adult FMS patients. Data were extracted independently and a frequentist network meta-analyses (NMA) was performed to rank the effects of interventions according to P-scores. The NMA evidence certainty was assessed using the method recommended by Grading of Recommendations Assessment, Development, and Evaluation Working Group.
Results: A total of 57 RCTs were identified, including 3319 participants, involving 9 interventions (7 types of exercise, 2 controls). Of all treatments compared with usual care in efficacy outcomes, Mind-body exercise was associated with the best HRQOL (SMD, − 12.12; 95% CI, − 15.79 to − 8.45). On the other characteristic symptom dimensions, based on moderate quality evidence, sensorimotor training was associated with minimal pain scores compared with usual care (SMD, − 1.81; 95% CI, − 2.81 to − 0.82), whole body vibration therapy was most promising for improving sleep quality (SMD, − 6.95; 95% CI, − 10.03 to − 3.87), pool-based aerobic exercise was most likely to ease anxiety (SMD, − 4.83; 95% CI, − 7.47 to − 2.19), and whole body vibration was most likely to improve depression (SMD, − 10.44; 95% CI, − 22.00 to 1.12).
Conclusion: Mind-body exercise seems to be the most effective exercise to improve the overall HRQOL of patients with FMS. But at the same time, clinicians still need to develop individualized exercise plans for patients according to their symptoms and accessibility.
Keywords: fibromyalgia syndrome, exercise, quality of life, systematic review, network meta-analysis
Introduction
Fibromyalgia syndrome (FMS) is a chronic, painful, non-articular rheumatism characterized by widespread musculoskeletal pain, fatigue, and sleep disturbances, and is considered the third most frequent musculoskeletal condition.1,2 Fatigue, sleep disturbances, mood abnormalities and other somatic symptoms are also common, all of which have a significant impact on health-related quality of life (HRQOL). The prevalence of the disease in Europe is conservatively estimated at 4.7% or more, with a female: male ratio of 3:1.1,3 Until now, FMS is understood to be a mysterious syndrome of unknown cause. In recent years, functional Magnetic Resonance Imaging (fMRI) found that FMS patients pain associated neuropeptides and neurotransmitter levels (substance P, brain-derived neurotrophic factor, glutamine and dopamine) not only changed, brain morphology and pain receptors have been reconstructed, show the pain-processing areas of the brain neuron activity increased.2 These changes seem to explain the multiple symptoms and hyperalgesia seen in FMS patients.
FMS can be lifelong, and medical therapy is of limited value due to the diversity of pathogenesis and concerns about side effects.4–7 In the long term, FMS is best managed as a chronic condition, with non-pharmacological therapies as the primary treatment and medications as an adjunct to symptom relief. In Recent guidelines from the European League Against Rheumatism (EULAR)’s recommendations for fibromyalgia management, the importance of using non-pharmacological measures first was stressed, with exercise being the only “strong” recommendation.2,8 Early research supports aerobic and strength training to improve fitness and optimize health and well-being. However, there are still some patients with FMS who cannot tolerate aerobic exercise, with poor muscle strength and flexibility.9,10 Other forms of exercise (such as tai chi, yoga, vibration techniques) and lifestyle physical activities have also been introduced.11 It is important to determine the most effective type of exercise (aerobic, resistance, stretching, sensorimotor training, mind-body exercise, etc.).12 A review of the last 32 years (1990–2022) of research on this question shows that there is a strong interest in answering it.
Although a previous traditional paired meta-analysis involving 35 randomized clinical trials (RCTs) assessed the efficacy of several types of exercise versus control arm, the rough or fuzzy classification of exercise interventions led to considerable heterogeneity in the assessment of exercise intervention outcomes, which reduced the quality of the evidence.13 The authors did not consider placebo (or sham exercise) effects when selecting control measures. In addition, traditional meta-analyses cannot clearly rank different classes of interventions based on efficacy outcomes. Based on the above unresolved issues, this study aims to adopt more stringent exercise classification measures, determine the best physical exercise types for FMS patients’ overall HRQOL and common symptoms, and guide clinical practice. Network meta-analysis (NMA) combines all direct and indirect evidence from RCTs to compare multiple treatment options simultaneously and rank them by effect size (ES), helping to update the evidence on exercise options for patients with FMS.14 Therefore, the aim of this NMA was to assess which types of physical exercise have the greatest positive impact on HRQOL and other typical symptoms in adults with FMS.
Methods
Protocol and Registration
This systematic review and NMA were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement and its extension for network meta-analyses (PRISMA-NMA),15,16 (Supplementary Appendix 1). The study was registered on the International Prospective Register of Systematic Reviews (PROSPERO) on May 16, 2022 (Registration number CRD42022330588).
Search Strategy and Study Selection
The retrieval strategy was jointly formulated by two authors (Z.-H.Z. and L.-Y.W.), which mainly used the combination of Medical Subject Headings (MeSH) and free text, then combined the retrieval words through logical characters “OR” and “AND” to conduct literature retrieval (Supplementary Table 1). Specific search strategies are provided in the supplementary document. We then independently searched PubMed, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to April 21, 2022 for all articles expressed in English. In addition, we manually searched unpublished studies at NIH ClinicalTrials.gov (www.clinicaltrials.gov). All citations retrieved were downloaded and imported into EndNote for management and subsequent screening. The titles and abstracts that met the requirements were screened independently by two investigators (D.-X.Z. and K.-D.Z.). Any differences will be resolved through consultation or by seeking a third party (T.M.). Then, the full text of potential articles was reviewed according to the inclusion and exclusion criteria of the study.
The following eligibility criteria have been designed in accordance with the PICOS framework: (i) Adults diagnosed with FMS according to the American College of Rheumatology (ACR) classification criteria. (ii) Studies focusing on the comparison of two different exercise treatments, or the exercise group versus the control group. Waiting list or treatment as usual are identified as Non-intervention control (NC). As active controls (AC), health education, relaxation, and sham exercise can be presented alone as a control group. Multidisciplinary treatment with active controls combined with exercise was not considered in this study. (iii) Studies with comparable baseline data between groups and available quantitative outcome data after exercise interventions. (iv) The study design is a RCT.
Studies are excluded if they involve the following characteristics: (i) The study population was not exclusively FMS patients (eg, chronic widespread pain). (ii) Studies focused on drug therapy. (iii) Studies involving other non-pharmacological therapies, such as balneotherapy, cognitive behavioral therapy, neuroregulatory therapy, multidisciplinary therapy, acupuncture, etc. (iv) Studies combining different pharmacological and non-pharmacological regimens. (v) Studies comparing the effects of different intensities or frequencies of the same exercise program. (vi) Studies that focused on different combinations of exercises.
Classification of the Interventions and Outcomes
Referring to the classification methods of Luan et al, Gutiérrez et al, we divided physical exercise intervention into the following 6 categories17,18 Aerobic exercises (exercise designed to increase energy expenditure and increase heart rate, including endurance training, cycling, brisk walking, etc.), Mind-body exercises (MBE, a form of exercise that combines movement, concentration, and breath control while simultaneously taking care of the mental and physical. Including yoga, Pilates, tai Chi and so on), Strength or resistance exercises (SRE, exercises designed to increase muscle mass and strength include strength training and personalized load training), Stretching exercises (STE, a form of exercise designed to increase muscle elasticity and achieve comfortable muscle tone, including flexibility training), Sensorimotor training (SME, activities designed to increase the body’s stability to produce balanced balance, including dance, balance training, and Exergames, can also add appropriate stretching, strength, and aerobic exercise, as well as stress reduction interventions), and Whole body vibration (WBV, a therapy that uses vibrations of a specific frequency and amplitude to cause muscle contractions and nerve stimulation). In fact, almost all aerobic exercise programs include four stages: (i) warm-up, (ii) Main aerobic exercise and Endurance training, (iii) Stretching and (iv) Relaxation. Since aquatic exercises are different from regular land-based exercises, we further subdivide aerobic exercises into Land-based aerobic exercises (LAE) and Pool-based aerobic exercises (PAE) (Supplementary Table 2).
The primary outcome is FMS patients’ HRQOL after exercise intervention, as measured by Fibromyalgia Impact Questionnaire (FIQ) or its revised version (FIQR), the reliability of which has been fully validated in previous studies.19,20 The secondary outcomes are pain, sleep, anxiety, and depression measured after the exercise intervention, with the Visual Analogue Scale (VAS), Pittsburgh Sleep Quality Index (HSQI), Hospital Anxiety and Depression Scale (HADS), and Beck Depression Inventory (BDI) selected as the default scales, respectively. If an alternative scale is used in a study, the measurement results of that alternative scale are adopted (Supplementary Table 3).
Data Extraction
Before information extraction, all authors jointly developed a standardized information extraction table. Information to be extracted includes study name (first author and publication year), study design (randomization, allocation concealment, blinding, etc.), patient characteristics (mean age and proportion of females), intervention details (duration and frequency), and results (outcome measurements, FIQ, FIQR, pain, sleep, anxiety, and depression). The information was then extracted independently by the two authors (K.-D.Z. and L.-Y.W.) and cross-checked by another reviewer (X.-W.L.). Following Migliorini et al, we only considered reporting quantitative data after exercise therapy for FMS.21 As continuous data, we extracted the mean and standard deviation (SD) of each target outcome at the end of the treatment period. If SD is not available, we imputed them based on standard error (SE), confidence interval (CI), median combine with Interquartile Range (IQR).22–24 Whenever available we used results from intention-to-treat (ITT) analyses. Otherwise, report the results of per-protocol (PP) analysis. All data are consolidated in Microsoft Excel 2019 (Microsoft Corp) in a contrast-based format.
Risk of Bias and Quality Assessment
The risk of bias of all included RCTs was assessed independently by two researchers (K.-D.Z. and D.-X.Z.) following the Revised Cochrane risk-of-bias tool for randomized trials (ROB2),25 Any differences will be resolved through consultation or by seeking a third party (T.M.). ROB2 sets up 5 evaluation domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. The risk of bias in each domain can be divided into 3 levels: low risk of bias, some concerns and high risk of bias. In addition, two of us (K.-D.Z. and F.-Q.) independently graded the NMA evidence certainty using a four-step method recommended by Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group.26 The methodology was updated in 2019 to eliminate imprecision in grading the quality of direct evidence for each comparison group.27 Arbitration by the third author (F.-Q.), if necessary. Based on evidence assessment, we applied GRADE’s recommended informative statements (“probably or likely”, “may”) to convey our confidence in the effect estimates.28
Statistical Analysis
More information on the detailed statistical principles of NMA can be found in a previously published review.29 This manuscript only gives a brief description of the relevant analytical steps involved in this study.
ES is a measure of the size of the effect produced by the intervention. All outcomes are continuous data, so we summarize the ES of the interventions using the Cohen’s d standardized mean differences (SMDs) with 95% CI. For the outcomes of FIQ (or FIQR), pain, sleep, anxiety, and depression severity after intervention, we chose to apply a random-effects models rather than fixed-effects models because we acknowledge that the included studies are partially heterogeneous.
To integrate all direct and indirect evidence, we conducted NMA within a frequentist framework using the statistical package netmeta in R software version 3.6.3 (R Foundation for Statistical Computing), which is a graph-theoretical model for NMA.30 As long as the heterogeneity is moderate, the estimation bias of this model is lower than that of other methods, which is facilitate clinicians’ decision-making process.31 A network geometry graph was drawn to assess the strength of the available evidence, with the size of the nodes proportional to the participants involved in the intervention and the thickness of the lines connecting the nodes proportional to the number of trials directly compared. We ranked the efficacy outcomes of various treatments with reference to the P-score, which is similar to the surface under the cumulative ranking curve (SUCRA).32 P-score ranges from 0 to 1, and interventions with high P-score have better overall efficacy than those with low P-score.
Homogeneity, transitivity and consistency assumptions are three basic assumptions that are often involved in indirect comparison and NMA.33 In our study, we explored the transitivity assumption by assessing the characteristics of participants and whether there were significant differences in the intensity and frequency of interventions. I2 statistics were calculated to analyze statistical heterogeneity of the network. In addition, τ2 statistics were calculated to further determine the size and clinical relevance of heterogeneity.34 To express global inconsistency between studies, the Cochrane Q statistic was applied.35 For NMA with closed loop, local inconsistency was assessed by checking whether direct comparison results were consistent with indirect comparison results, which can be investigated by node-splitting technique with the netsplit command.30 P values less than 0.05 were considered statistically significant (two-tailed). The possibility of publication bias was explored by comparing-adjusted funnel plots and Egger test. If scattered points are evenly distributed on both sides of the point estimate line and the P value of Egger test is greater than 0.05, it may indicate that there is no publication bias. Data were analyzed in June 2022.
Results
Study Selection and Characteristics
Figure 1 shows the process of study screening and exclusion. A total of 57 RCTs (Supplementary Appendix 2) were eligible, involving 3319 patients. Data from only 2961 patients were analyzed after exclusion of loss of follow-up and contributed to the NMA. The characteristics of all included RCTs are summarized in Table 1. Three studies had 3 arms (2 interventions and 1 control). The ACR 1990 and ACR 2010 criteria have been widely used in the research and clinical application of FMS. Overall, the trials were published between 1996 and 2021, 93.8% of participants were women, and the average age of participants ranged from 35 to 59.3 years. Twenty-five trials evaluated LAE (772 patients), 11 trials PAE (303 patients), 9 trials SME (260 patients), 10 trials MBE (348 patients), 10 trials STE (316 patients), 10 trials SRE (303 patients), and 3 trials WBV (78 patients). Thirty-five trials evaluated NC (776 patients), and four trials evaluated AC (163 patients). The intervention duration of 40 trials (70.2%) was between 8 and 16 weeks, and the recommended frequency of exercise was 2–3 times per week for 50 trials (87.7%). Eighteen trials (31.6%) reported analyses according to the ITT principle.
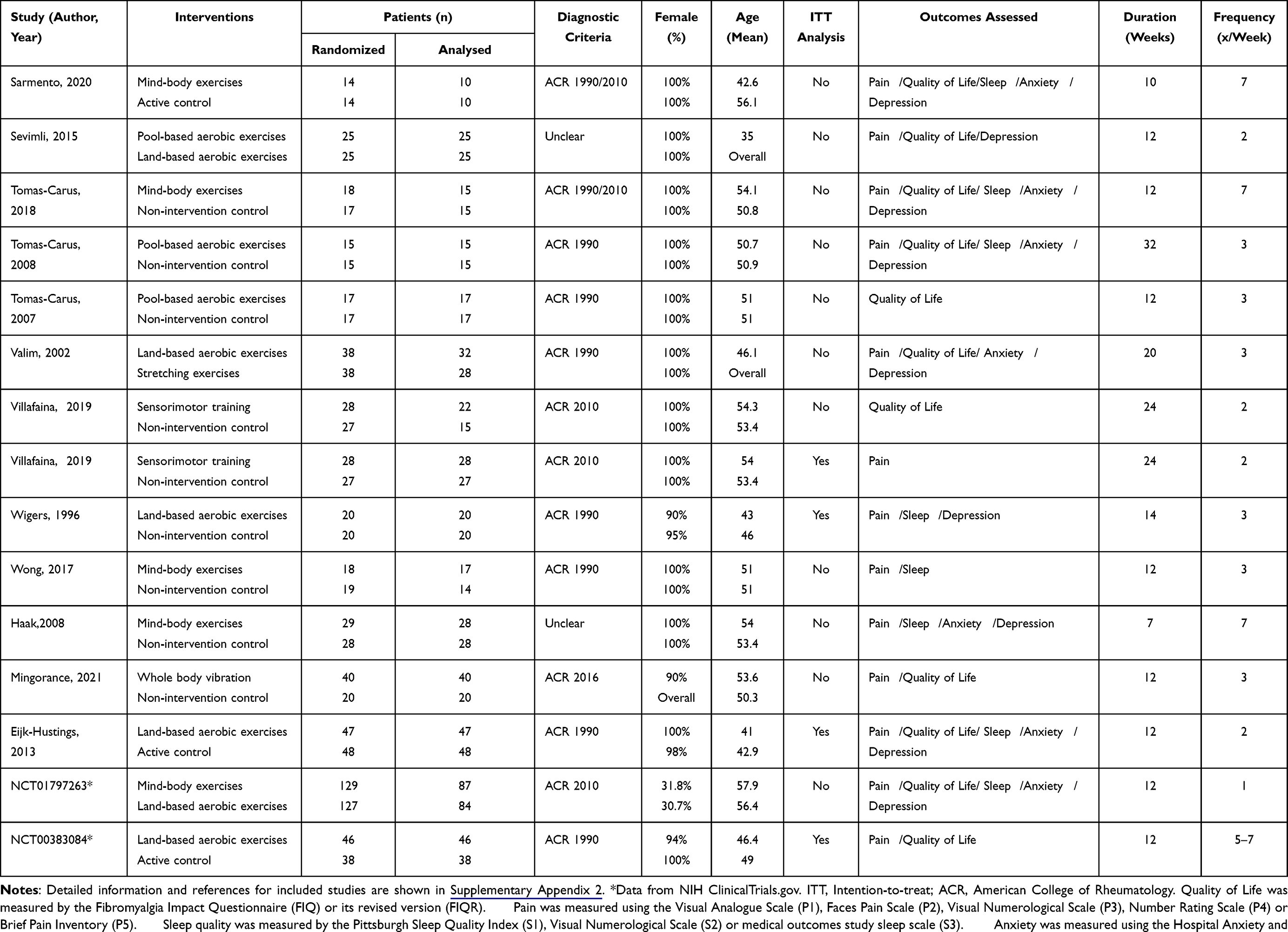 |
Table 1 Characteristics of Included Studies |
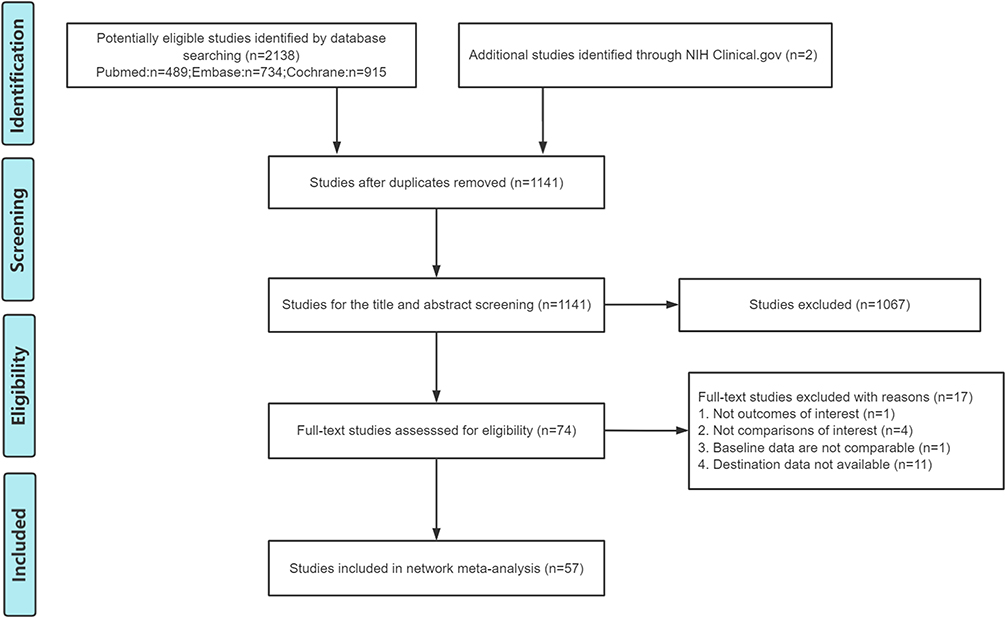 |
Figure 1 Flow diagram of the literature search and study. |
These studies showed significant heterogeneity in post-intervention follow-up in terms of outcomes based on HRQOL, pain, sleep, and depression, ranging from I2= 64.3% to 91.3%; τ2 = 0.5793 to 20.3430 (Supplementary Table 4). For Anxiety, only mild heterogeneity was observed (I2=38.4%, τ2 =1.0901). After reading and comparing the original literature, the follow-up time of different treatment strategies and different evaluation scales of the same outcome explained the source of these heterogeneity, so random effect model combined with ES was used for analysis.
Risk of Bias of Included Studies and Certainty of Evidence
The risk of bias for each trial assessed with the ROB2 tool is listed in Supplementary Figure 1. Overall, 16 trials (28.1%) were considered to have a low risk of bias in all domains, 30 studies (52.6%) were assessed as having some concerns, and 11 trials (19.3%) were assessed as high risk of bias. Specifically, 2 trials were judged to have a high risk of bias for inadequate randomization (the grouping of patients depends on the order of inclusion in the study). For missing outcome data, 6 trials were considered to have a high risk of bias (a possibility that the true outcome may be affected by large missing data or large difference in missing reasons between groups). For measurement of the outcome, 4 trials were judged to have a high risk of bias (measurement of outcome may be affected by the evaluator’s lack of blinding). The certainty of direct evidence assessment is shown in Supplementary Table 5. For indirectness, we focused on whether patient clinical characteristics, duration of intervention, or exercise frequency were transferable between studies. In theory, there should be an indirection between any two relevant trials, and only significant indirection would be considered for downgrade. The certainty of NMA evidence assessment by GRADE system is shown in Supplementary Table 6.
HRQOL
Among the FMS population, the network of treatment comparisons for HRQOL included 48 RCTs (2 arms n=46 and 3 arms n=2), 9 interventions and 2546 patients (Figure 2A). NC was the most closely linked intervention. The exercise pattern with the highest probability of being the best is MBE (Figure 3 and Supplementary Figure 2A). For all treatments compared with NC, MBE was associated with the lowest FIQ score (SMD, −12.12; 95% CI, −15.79 to −8.45; P-score, 0.974), followed by WBV (SMD, −9.23; 95% CI, −14.08 to −4.39; P-score, 0.816), SRE (SMD,-7.19; 95% CI, −11.29 to −3.09; P-score, 0.685), LAE (SMD, −6.49; 95% CI, −8.98 to −4.01; P-score, 0.619), PAE (SMD, −6.48; 95% CI, −9.14 to −3.83; P-score, 0.615), STE (SMD, −3.78; 95% CI, −7.31 to −0.26; P-score, 0.340) and SME (SMD, −3.04; 95% CI, −5.87 to −0.20; P-score, 0.287) (Figures 2B and 3). In the netsplit analysis, we identified 4 inconsistent comparisons, indicating divergence between indirect and direct evidence of LAE vs MBE, LAE vs PAE, NC vs PAE, and SME vs STE (Supplementary Figure 3A). Comparison-adjusted funnel plots and Egger test were performed for the primary outcome, HRQOL. The results showed that the left and right sides of the funnel plot were roughly symmetrical and the P value of Egger test was 0.36, that is, publication bias was unlikely to exist (Figure 2C).
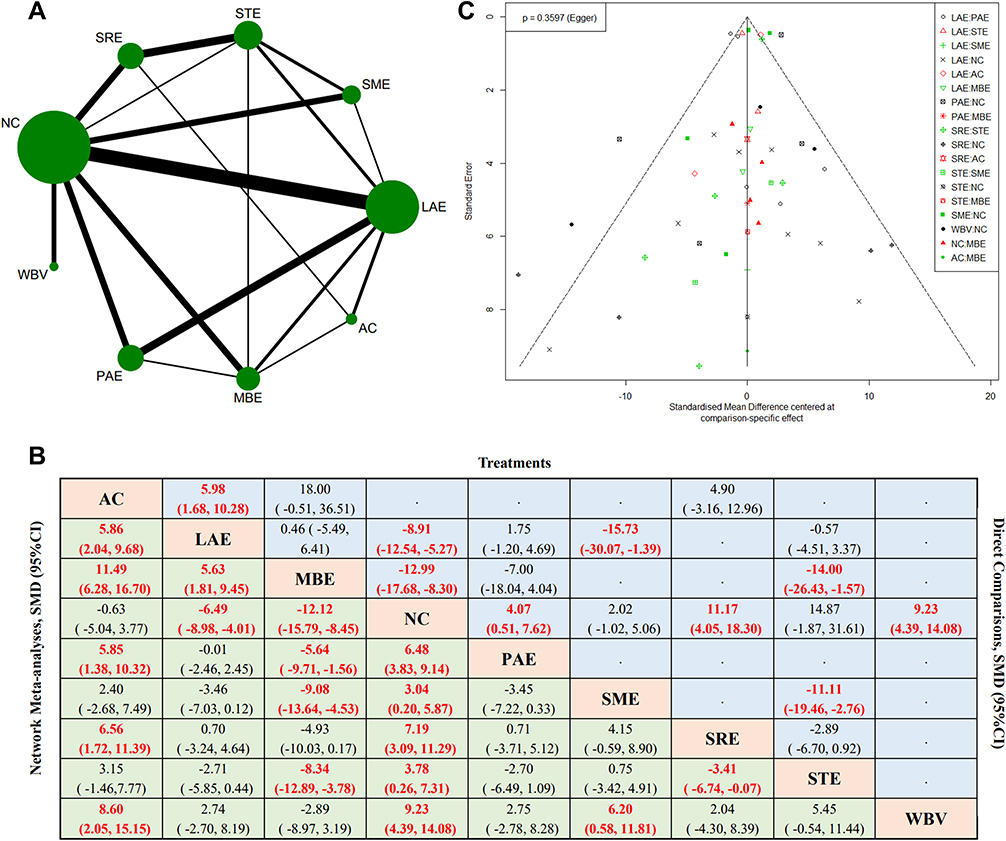 |
Figure 2 HRQOL. (A). Network plot of treatment comparisons. The width of the line represents the number of RCTs per pairwise comparison, and the size of each node is proportional to the number of sample size. (B). Network meta-analysis Estimates of HRQOL. Effect sizes presented on the upper triangle are direct comparisons (head-to-head studies) between the row and columns; the effect sizes on the lower triangle are network meta-analyses between the column and the row. Meta-analysis use SMD and 95% CI to assess the improvement in quality of life of the intervention. (C). Comparing-adjusted funnel plot. Abbreviations: MBE, Mind-body exercises; SRE, Strength or resistance exercises; STE, Stretching exercises; SME, Sensorimotor training; WBV, Whole body vibration; LAE, Land-based aerobic exercises; PAE, Poor-based aerobic exercises; NC, Non-intervention control; AC, Active control; SMD, standardized mean differences; CI, confidence interval. |
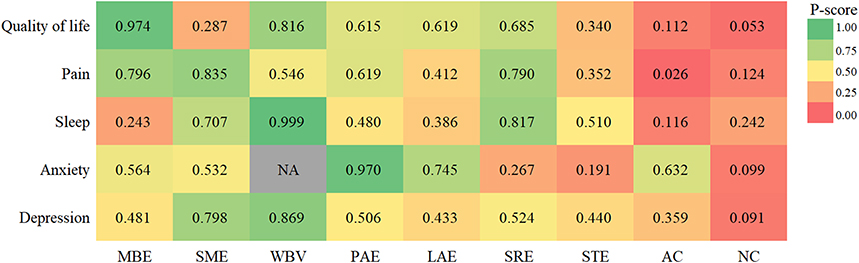 |
Figure 3 Heat map of exercise interventions ranked according to improve Health-Related Quality of Life (HRQOL), pain, sleep, anxiety and depression. Abbreviations: MBE, Mind-body exercises; SRE, Strength or resistance exercises; STE, Stretching exercises; SME, Sensorimotor training; WBV, Whole body vibration; LAE, Land-based aerobic exercises; PAE, Poor-based aerobic exercises; NC, Non-intervention control; AC, Active control. |
Pain
Among the FMS population, the network of treatment comparisons for Pain included 42 RCTs (2 arms n=40 and 3 arms n=2), 9 interventions and 2266 patients (Supplementary Figure 4A). The best exercise pattern for relieving pain symptoms is probably SME (Figure 3 and Supplementary Figure 2B). After exercise intervention, patients in the SME group had the most significant reduction in pain scores compared with NC (SMD, −1.81; 95% CI, −2.81 to −0.82; P-score, 0.835), followed by MBE (SMD, −1.65; 95% CI, −2.26 to −1.05; P-score, 0.796), SRE (SMD, −1.73; 95% CI, −3.00 to −0.47; P-score, 0.790), PAE (SMD, −1.28; 95% CI, −2.08 to −0.48; P-score, 0.619), WBV (SMD, −1.12; 95% CI, −2.38 to 0.14; P-score, 0.546), LAE (SMD, −0.87; 95% CI, −1.53 to −0.21; P-score, 0.412), and STE (SMD, −0.69; 95% CI, −1.66 to 0.27; P-score, 0.352) (Figures 3, 4A and Supplementary Table 7A). In the netsplit analysis, we identified only 2 inconsistent comparisons, indicating divergence between indirect and direct evidence of AC vs LAE and AC vs SRE (Supplementary Figure 3B). The asymmetrical funnel plot and Egger test (P =0.0042) suggest that the trails with favorable therapeutic effects were more likely to be published (Supplementary Figure 5A).
 |
Figure 4 Forest plot of network meta-analysis results. (A). Pain. (B). Sleep. (C). Anxiety. (D). Depression. Comparisons are based on SMD and 95% CI in all outcomes. Abbreviations: MBE, Mind-body exercises; SRE, Strength or resistance exercises; STE, Stretching exercises; SME, Sensorimotor training; WBV, Whole body vibration; LAE, Land-based aerobic exercises; PAE, Poor-based aerobic exercises; NC, Non-intervention control; AC, Active control; SMD, standardized mean differences; CI, confidence interval. |
Sleep
For sleep, 21 trials (2 arms n=20 and 3 arms n=1) compared 9 different interventions involving 1057 patients (Supplementary Figure 4B). In the efficacy ranking results, WBV was determined to be the best (P-score, 0.999), followed by SRE (P-score, 0.817) (Figure 3 and Supplementary Figure 2C). The advantage of WBV in improving sleep quality was significant, even when compared with SRE (SMD, −4.57; 95% CI, −8.00 to −1.13) (Supplementary Table 7B). No local inconsistencies were observed in the network (Supplementary Figure 3C). A roughly symmetrical comparison adjustment funnel plot and Egger test result (P =0.8475) suggest that publication bias is unlikely to exist (Supplementary Figure 5B).
Anxiety
For anxiety, 20 trials (2 arms n=19 and 3 arms n=1) compared 8 different interventions involving 1091 patients (Supplementary Figure 4C). No data related to WBV were reported. Compared with NC, 4 exercise patterns significantly improved anxiety in FMS patients, namely PAE (SMD, −4.83; 95% CI, −7.47 to 2.19; P-score, 0.970), LAE (SMD, −2.87; 95% CI, −4.51 to −1.24; P-score, 0.745), MBE (SMD, −2.13; 95% CI, −3.60 to −0.66; P-score, 0.564) and SME (SMD, −1.90; 95% CI, −3.68 to −0.12; P-score, 0.532) (Figures 3, 4C and Supplementary Table 7C). Ranking identified that PAE was probably the best, and interestingly, the AC group also showed satisfactory results (Figure 3 and Supplementary Figure 2D). There was no measurable local inconsistency within the network (Supplementary Figure 3D). Based on the comparison-adjusted funnel plot, we believe that the probability of publication bias is low (Supplementary Figure 5C).
Depression
For anxiety, 31 trials (2 arms n=29 and 3 arms n=2) compared 9 different interventions involving 1572 patients (Supplementary Figure 4D). Based on interval estimates of direct and indirect comparisons, no treatment appeared to be superior to the others, except that SME (SMD, −6.33; 95% CI, −10.81 to −1.84) was significantly superior to NC (Figure 4D and Supplementary Table 7D). The exercise modality that has the highest probability of being the best is WBV (Figure 3 and Supplementary Figure 2E). In the netsplit analysis, no local inconsistencies were observed in the network (Supplementary Figure 3E). A roughly symmetrical comparison adjustment funnel plot and Egger test result (P =0.7886) suggest that publication bias is unlikely to exist (Supplementary Figure 5D).
Discussion
Exercise therapy conforms to the new medical model and has become one of the most popular rehabilitation medical means for patients with FMS. This NMA is a timely addition to previous literature and tends to form a unified decision. In summary, our results indicate that MBE, including yoga and tai chi, is associated with lower FIQ (or FIQR) scores in patients with FMS compared with treatment as usual, contributing to reduced symptom severity and enhance overall quality of life. Based on moderate-quality evidence, appropriate SME, including dance, is recommended for patients with FMS whose core symptoms are pain. Regarding FMS patients with recent sleep disorders such as severe insomnia and dreaminess, WBV therapy is a type of exercise intervention worth promoting based on moderate-quality evidence. Aerobic exercise, particularly PAE, may be associated with significant improvements in anxiety based on moderate-quality evidence. In addition, the outcomes of depressive mood improvement were similar for all exercise modality, except for SME compared with NC.
To our knowledge, this is the first NMA to combine all exercise interventions in FMS. We evaluated SMD as our treatment outcome in HRQOL, pain, sleep, anxiety and depression. In this study, we also conducted hypothesis testing and evaluated the quality of the evidence. Of course, under this model, we assume that the relative therapeutic effects of two or more interventions in different studies are derived from a common distribution. This assumption may limit the accuracy of conclusions because the population is not homogeneous, but the NMA comparison of multiple interventions simultaneously is important to develop exercise strategies for FMS patients with different typical symptoms. In the meantime, our results may still help guide clinicians and patients in their choice of exercise therapy that is most appropriate for the individual.
Due to the lack of high-quality RCTs of drug effectiveness, recommended guidelines for the treatment of FMS rely heavily on low-quality evidence and expert consensus,36 leaving pharmacological management complex and evidence deficient. Exercise has beneficial clinical effects for most musculoskeletal conditions, including FMS, according to Hagen et al, who have empirical evidence.37 Recent guidelines from EULAR (2016), the Canadian Pain Society (2012) and the Association of the Scientific Medical Societies in Germany (AWMF) (2012) all emphasize non-pharmacological treatment as the first-line treatment for FMS, with exercise therapy being given the highest level of recommendation.8,38,39 As the low risk of side effects and the general health benefits of exercise, most of the types of exercise in our research confirmed this consensus. Besides, more novel is that the pattern of movement needs to vary from person to person, depending on the characteristics of the symptoms.
For aerobic exercise, it is recommended that the intensity of exercise be moderate. Some studies adjusted the intensity according to the target heart rate,40–45 while others determined the intensity of exercise in patients with FMS according to the Borg’s rating of perceived exertion.46–49 Moreover, in the Bidonde et al study, almost all forms of aerobic exercise, regardless of intensity, were well tolerated by the subjects and produced positive effects.50 Our NMA concluded that PAE proved to be as effective as LAE in improving overall HRQOL, while PAE appeared to perform better than LAE at the level of specific symptoms. We consider that the pool environment is directly related to the present results, with water having a direct relaxant effect on the muscles.51 Low speed exercise in water can reduce the impact on joints, induce oxygen free radical scavenging, and improve microcirculation.52 However, due to the scarcity of studies and the width of the CI, conclusions could not be drawn with greater confidence.
Although aerobic exercise is currently the most commonly used non-pharmacological treatment for patients with FMS, the fluctuation of symptoms makes it difficult for many patients to carry out and adhere to an exercise program.12 In the study by Wang et al, participants assigned to psychosomatic therapy had higher attendance compared to aerobic exercise.53 In addition, tai chi showed greater benefits on HRQOL at the same intensity and duration (24 weeks, twice a week). Of note, 24 weeks of tai chi resulted in greater clinical improvement than 12 weeks of tai chi. For the superiority of MBE over aerobic exercise in HRQOL, we found that both traditional paired meta-analyses and NMA showed lower SMDs in favor of MBE. However, due to low power, the results were not statistically significant in paired meta-analyses. This is because NMA, which combines direct and indirect evidence, has the advantage of achieving more accurate estimates of treatment benefit than pairwise meta-analyses. fMRI has shown that MBE can improve the connectivity of medial hypothalamus with thalamus and amygdala in patients with FMS, thereby affecting neuroendocrine and immune functions.54 MBE can also reduce peripheral nociceptive inputs to central pain pathways, ultimately breaking the “pain cycle”55 In the long run, fibromyalgia patients may better accept MBE.
For WBV, the encouraging result was its excellent performance in improving biorhythm-related symptoms (ie, sleep quality and depressive mood). A previous study suggested a possible link between improved subjective sleep outcomes and reduced depression and restoration of plasma brain-derived neurotrophic factor (BDNF) levels in FMS patients after WBV intervention.56 Although the study design and analysis do not allow us to make causal inferences about the relationship between BDNF and the outcome variables.
SME, including dancing and exergames, requires the integration of sensory information from multiple channels (auditory, vestibular, visual, somatosensory), which is conducive to enhancing human stability, coordination and balance.57,58 Compared to aerobic exercise, SME also has a pleasurable element, which may have a positive impact on mental health, reducing depression and raising pain thresholds.59 Such speculation seems to be consistent with our results, which showed that SME performed well in reducing depression scores and ameliorating pain. However, SME did not rank high in reducing FIQ (FIQR) scores. Notably, with the exception of STE, the lack of direct comparisons of SME with other forms of exercise leads to an over-reliance on indirect comparisons for the results of NMA (Table 1). This reduces the credibility (ie evidence quality) of the SME’s impact on HRQOL in view of non-transitivity considerations.
Regarding SRE, this NMA demonstrated a favourable effect on all the results analyzed, although there was non-significant positive effect on psychiatric symptoms. Whereas a previous systematic review by Busch et al cautioned against limited evidence of SRE for depression,60 Vilarino et al emphasized that this type of exercise enhanced psychological health.61 The contradictions may arise from the differences in the included literature. More and higher quality studies are needed in the future to confirm the therapeutic value of SRE.
For STE, this study showed no statistically significant effects on all secondary outcomes of interest, with the exception of HRQOL. STE is beneficial for reducing muscle stiffness and reducing muscle and joint viscosity, and are often used as part of the preparation for other forms of exercise. Therefore, some stretching of the extremities and trunk muscles prior to the formal exercise program is considered a helpful supplement.62
Our study was based on an extensive literature search and we assumed that vital trials were unlikely to be missed. We hope to ensure the integrity of the network as much as possible, but due to the quality of the data currently available, there is non-negligible heterogeneity in some outcomes. Even if we stepwise restrict the inclusion criteria, we believe it is unlikely to eliminate this problem and will lead to a reduction in the number of interventions available. The actual heterogeneity comes mostly from clinical heterogeneity. There was considerable heterogeneity in the characteristics of the intervention (specific exercise details, intensity, frequency, and duration) between studies, and different measures of pain, sleep, anxiety, and depression were applied across studies. HRQOL, the primary outcome of the unified FIQ or FIQR assessment, is not affected by this warning. Universality may also be hampered by the way in which specific forms of movement are classified. Kundakci et al reported that aerobic exercise and STE showed improvement in FIQ, while MBE did not increase FIQ.13 Their findings, however, were based on direct evidence rather than indirect evidence, and the classification of exercise was not specific enough. It may also be related to the larger number of studies (48 vs 28) and overall sample size (2546 vs 1487) in the current study.
There were some limitations to our study. First, we did not consider the characteristics of various exercise intervention, such as intensity, frequency and duration, which varied widely from study to study, making subgroup analysis difficult. But to flesh out the results, we analyzed overall HRQOL as well as other specific dimensions, such as pain, sleep, anxiety, and depression, that might be confounding factors in the effect of exercise on HRQOL. Second, regarding baseline characteristics, we assessed only age and sex. However, due to lack of data, other baseline characteristics were not evaluated, particularly the severity of FMS between studies, which may lead to bias. Third, there is no consensus on the optimal follow-up period for the long-term effects of exercise interventions. Since there may be some differences between the outcome at the end of treatment and the outcome of long-term follow-up, this study only focuses on the outcome at the end of treatment and establishes treatment recommendations based on short-term data only. Fourth, the tools used to assess efficacy vary from study to study, which may influence the pooled conclusions. Future research should specify the most appropriate, reliable and effective scores to avoid data fragmentation between them. Fifthly, there are some limitations in using P-value to estimate the rank probability of comparative efficacy between different interventions, and the results need to be carefully interpreted. Sixth, due to the heterogeneity of the study, only the results under the random-effect model were reserved, and additional large-scale RCTs with high methodological quality still need to be carried out and supplemented. Seventh, some small sample size studies included in the study may help determine heterogeneity, and caution is needed in interpreting our results.
Conclusion
Despite limited evidence, exercise interventions have clear benefits for patients with FMS, and the size of the effect varies depending on the type of exercise and the outcome of interest. Given the evidence currently available, MBE seems most promising for improving overall HRQOL in patients with FMS. SME was most promising for relieving pain, WBV for improving sleep, aerobic exercise for relieving anxiety and WBV for improving depression. This study can be used as a reference for clinicians to prescribe personalized exercise for FMS patients, that is, the choice in terms of exercise recommendations should be informed by evidence, but other factors such as barriers to engagement and accessibility also have to be recognized. In the future, further studies are needed to confirm the reliability of the conclusions of this study. In addition, it is important to determine the most appropriate exercise variables (intensity, frequency and duration) to achieve the best results for quality of life.
Abbreviations
FMS, fibromyalgia syndrome; HRQOL, health-related quality of life; RCTs, Randomized clinical trials; NMA, network meta-analyses; functional Magnetic Resonance Imaging (fMRI); EULAR, the European League Against Rheumatism; ES, effect size; MeSH, Medical Subject Headings; MBE, Mind-body exercises; SRE, Strength or resistance exercises; STE, Stretching exercises; SME, Sensorimotor training; WBV, Whole body vibration; LAE, Land-based aerobic exercises; PAE, Poor-based aerobic exercises; NC, Non-intervention control ;AC, active control; FIQ, Fibromyalgia Impact Questionnaire; FIQR, Revised Fibromyalgia Impact Questionnaire; ACR, American College of Rheumatology; SE, standard error; CI, confidence interval; ITT, intention-to-treat; SMDs, standardized mean differences; SUCRA, the surface under the cumulative ranking curve; AWMF, the Association of the Scientific Medical Societies in Germany; BDNF, brain-derived neurotrophic factor; PICOS, participants, interventions, comparisons, outcomes, and study design; PRISMA, the Preferred Reporting Items for Systematic Reviews and Meta-Analysis; PROSPERO, the International Prospective Register of Systematic Reviews.
Funding
This work was supported by the National Natural Science Foundation of China [grant numbers 81672250]; the National Natural Science Foundation of China [grant numbers 81900394]; Shandong Province Natural Science Foundation [grant numbers ZR2017BH022]; China Postdoctoral Science Foundation [grant numbers 2019M652395]; and the Fundamental Research Funding of Shandong University.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Sarzi-Puttini P, Giorgi V, Marotto D, Atzeni F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020;16(11):645–660. doi:10.1038/s41584-020-00506-w
2. Bair MJ, Krebs EE. Fibromyalgia. Ann Intern Med. 2020;172(5):Itc33–itc48. doi:10.7326/AITC202003030
3. Queiroz LP. Worldwide epidemiology of fibromyalgia. Curr Pain Headache Rep. 2013;17(8):356. doi:10.1007/s11916-013-0356-5
4. Farag HM, Yunusa I, Goswami H, Sultan I, Doucette JA, Eguale T. Comparison of amitriptyline and US food and drug administration-approved treatments for fibromyalgia: a systematic review and network meta-analysis. JAMA Network Open. 2022;5(5):e2212939. doi:10.1001/jamanetworkopen.2022.12939
5. Chappell AS, Littlejohn G, Kajdasz DK, Scheinberg M, D’Souza DN, Moldofsky H. A 1-year safety and efficacy study of duloxetine in patients with fibromyalgia. Clin J Pain. 2009;25(5):365–375. doi:10.1097/AJP.0b013e31819be587
6. Häuser W, Bernardy K, Uçeyler N, Sommer C. Treatment of fibromyalgia syndrome with gabapentin and pregabalin--a meta-analysis of randomized controlled trials. Pain. 2009;145(1–2):69–81. doi:10.1016/j.pain.2009.05.014
7. Eguale T, Buckeridge DL, Verma A, et al. Association of off-label drug use and adverse drug events in an adult population. JAMA Intern Med. 2016;176(1):55–63. doi:10.1001/jamainternmed.2015.6058
8. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis. 2017;76(2):318–328. doi:10.1136/annrheumdis-2016-209724
9. Jones KD, Liptan GL. Exercise interventions in fibromyalgia: clinical applications from the evidence. Rheum Dis Clin North Am. 2009;35(2):373–391. doi:10.1016/j.rdc.2009.05.004
10. Häuser W, Klose P, Langhorst J, et al. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: a systematic review and meta-analysis of randomised controlled trials. Arthritis Res Ther. 2010;12(3):R79. doi:10.1186/ar3002
11. Wang C, Schmid CH, Rones R, et al. A randomized trial of tai chi for fibromyalgia. N Engl J Med. 2010;363(8):743–754. doi:10.1056/NEJMoa0912611
12. Busch AJ, Webber SC, Brachaniec M, et al. Exercise therapy for fibromyalgia. Curr Pain Headache Rep. 2011;15(5):358–367. doi:10.1007/s11916-011-0214-2
13. Kundakci B, Kaur J, Goh SL, et al. Efficacy of nonpharmacological interventions for individual features of fibromyalgia: a systematic review and meta-analysis of randomised controlled trials. Pain. 2021;163(8):1432–1445. doi:10.1097/j.pain.0000000000002500
14. Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Intern Emerg Med. 2017;12(1):103–111. doi:10.1007/s11739-016-1583-7
15. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
16. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/M14-2385
17. Luan X, Tian X, Zhang H, et al. Exercise as a prescription for patients with various diseases. J Sport Health Sci. 2019;8(5):422–441. doi:10.1016/j.jshs.2019.04.002
18. Reina-Gutiérrez S, Cavero-Redondo I, Martínez-Vizcaíno V, et al. The type of exercise most beneficial for quality of life in people with multiple sclerosis: a network meta-analysis. Ann Phys Rehabil Med. 2021;65(3):101578. doi:10.1016/j.rehab.2021.101578
19. Burckhardt CS, Clark SR, Bennett RM. The fibromyalgia impact questionnaire: development and validation. J Rheumatol. 1991;18(5):728–733.
20. Bennett RM, Friend R, Jones KD, Ward R, Han BK, Ross RL. The revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. 2009;11(4):R120. doi:10.1186/ar2783
21. Migliorini F, Maffulli N, Eschweiler J, Knobe M, Tingart M, Colarossi G. Pharmacological management of fibromyalgia: a Bayesian network meta-analysis. Expert Rev Clin Pharmacol. 2022;15(2):205–214. doi:10.1080/17512433.2022.2044792
22. Higgins JPT LT, Deeks JJ. Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JPT, Thomas J, Chandler J, et al., editors. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022). Cochrane; 2022. Available from: www.trainingcochraneorg/handbook.
23. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
24. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
25. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
26. A GRADE Working. Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2015;350:h3326. doi:10.1136/bmj.h3326
27. Brignardello-Petersen R, Murad MH, Walter SD, et al. GRADE approach to rate the certainty from a network meta-analysis: avoiding spurious judgments of imprecision in sparse networks. J Clin Epidemiol. 2019;105:60–67. doi:10.1016/j.jclinepi.2018.08.022
28. Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. 2020;119:126–135. doi:10.1016/j.jclinepi.2019.10.014
29. PLOS ONE Staff. Correction: network meta-analysis using R: a review of currently available automated packages. PLoS One. 2015;10(4):e0123364. doi:10.1371/journal.pone.0123364
30. Shim SR, Kim SJ, Lee J, Rücker G. Network meta-analysis: application and practice using R software. Epidemiol Health. 2019;41:e2019013. doi:10.4178/epih.e2019013
31. Steeb T, Wessely A, Petzold A, et al. Evaluation of long-term clearance rates of interventions for actinic keratosis: a systematic review and network meta-analysis. JAMA dermatol. 2021;157(9):1066–1077. doi:10.1001/jamadermatol.2021.2779
32. Rücker G, Schwarzer G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol. 2015;15:58. doi:10.1186/s12874-015-0060-8
33. Song F, Loke YK, Walsh T, Glenny AM, Eastwood AJ, Altman DG. Methodological problems in the use of indirect comparisons for evaluating healthcare interventions: survey of published systematic reviews. BMJ. 2009;338:b1147. doi:10.1136/bmj.b1147
34. Álvarez-Bueno C, Deeks JJ, Cavero-Redondo I, et al. Effect of exercise on motor symptoms in patients with parkinson’s disease: a network meta-analysis. J Geriatric Phys Ther. 2021. doi:10.1519/JPT.0000000000000322
35. Jackson D, Barrett JK, Rice S, White IR, Higgins JP. A design-by-treatment interaction model for network meta-analysis with random inconsistency effects. Stat Med. 2014;33(21):3639–3654. doi:10.1002/sim.6188
36. Kia S, Choy E. Update on treatment guideline in fibromyalgia syndrome with focus on pharmacology. Biomedicines. 2017;5(2):20. doi:10.3390/biomedicines5020020
37. Hagen KB, Dagfinrud H, Moe RH, et al. Exercise therapy for bone and muscle health: an overview of systematic reviews. BMC Med. 2012;10:167. doi:10.1186/1741-7015-10-167
38. Fitzcharles MA, Ste-Marie PA, Goldenberg DL, et al. 2012 Canadian guidelines for the diagnosis and management of fibromyalgia syndrome: executive summary. Pain Res Manag. 2013;18(3):119–126. doi:10.1155/2013/918216
39. Sommer C, Häuser W, Alten R, et al. Medikamentöse Therapie des Fibromyalgiesyndroms, Systematische Übersicht und Metaanalyse[Drug therapy of fibromyalgia syndrome. Systematic review, meta-analysis and guideline]. Schmerz. 2012;26(3):297–310. German. doi:10.1007/s00482-012-1172-2
40. Assis MR, Silva LE, Alves AM, et al. A randomized controlled trial of deep water running: clinical effectiveness of aquatic exercise to treat fibromyalgia. Arthritis Rheum. 2006;55(1):57–65. doi:10.1002/art.21693
41. Etnier JL, Karper WB, Gapin JI, Barella LA, Chang YK, Murphy KJ. Exercise, fibromyalgia, and fibrofog: a pilot study. J Phys Act Health. 2009;6(2):239–246. doi:10.1123/jpah.6.2.239
42. Fernandes G, Jennings F, Nery Cabral MV, Pirozzi Buosi AL, Natour J. Swimming improves pain and functional capacity of patients with fibromyalgia: a randomized controlled trial. Arch Phys Med Rehabil. 2016;97(8):1269–1275. doi:10.1016/j.apmr.2016.01.026
43. García-Martínez AM, De Paz JA, Márquez S. Effects of an exercise programme on self-esteem, self-concept and quality of life in women with fibromyalgia: a randomized controlled trial. Rheumatol Int. 2012;32(7):1869–1876. doi:10.1007/s00296-011-1892-0
44. Munguía-Izquierdo D, Legaz-Arrese A. Exercise in warm water decreases pain and improves cognitive function in middle-aged women with fibromyalgia. Clin Exp Rheumatol. 2007;25(6):823–830.
45. Sañudo B, Carrasco L, de Hoyo M, Figueroa A, Saxton JM. Vagal modulation and symptomatology following a 6-month aerobic exercise program for women with fibromyalgia. Clin Exp Rheumatol. 2015;33(1 Suppl 88):S41–S45.
46. Hernando-Garijo I, Ceballos-Laita L, Mingo-Gómez MT, et al. Immediate effects of a telerehabilitation program based on aerobic exercise in women with fibromyalgia. Int J Environ Res Public Health. 2021;18(4):2075. doi:10.3390/ijerph18042075
47. Izquierdo-Alventosa R, Inglés M, Cortés-Amador S, et al. Low-intensity physical exercise improves pain catastrophizing and other psychological and physical aspects in women with fibromyalgia: a randomized controlled trial. Int J Environ Res Public Health. 2020;17(10):3634. doi:10.3390/ijerph17103634
48. Izquierdo-Alventosa R, Inglés M, Cortés-Amador S, et al. Comparative study of the effectiveness of a low-pressure hyperbaric oxygen treatment and physical exercise in women with fibromyalgia: randomized clinical trial. Ther Adv Musculoskelet Dis. 2020;12:1759720x20930493. doi:10.1177/1759720X20930493
49. Izquierdo-Alventosa R, Inglés M, Cortés-Amador S, Gimeno-Mallench L, Sempere-Rubio N, Serra-Añó P. Effectiveness of high-frequency transcranial magnetic stimulation and physical exercise in women with fibromyalgia: a randomized controlled trial. Phys Ther. 2021;101(10). doi:10.1093/ptj/pzab159
50. Bidonde J, Busch AJ, Bath B, Milosavljevic S. Exercise for adults with fibromyalgia: an umbrella systematic review with synthesis of best evidence. Curr Rheumatol Rev. 2014;10(1):45–79. doi:10.2174/1573403X10666140914155304
51. Mannerkorpi K, Hernelid C. Leisure time physical activity instrument and physical activity at home and work instrument. Development, face validity, construct validity and test-retest reliability for subjects with fibromyalgia. Disabil Rehabil. 2005;27(12):695–701. doi:10.1080/09638280400009063
52. Torres-Ronda L, Del Alcázar XS. The properties of water and their applications for training. J Hum Kinet. 2014;44:237–248. doi:10.2478/hukin-2014-0129
53. Wang C, Schmid CH, Fielding RA, et al. Effect of tai chi versus aerobic exercise for fibromyalgia: comparative effectiveness randomized controlled trial. BMJ. 2018;360:k851. doi:10.1136/bmj.k851
54. Kong J, Huang Y, Liu J, et al. Altered functional connectivity between hypothalamus and limbic system in fibromyalgia. Mol Brain. 2021;14(1):17. doi:10.1186/s13041-020-00705-2
55. Yocum DE, Castro WL, Cornett M. Exercise, education, and behavioral modification as alternative therapy for pain and stress in rheumatic disease. Rheum Dis Clin North Am. 2000;26(1):145–159, x–xi. doi:10.1016/S0889-857X(05)70128-9
56. Ribeiro VGC, Lacerda ACR, Santos JM, et al. Efficacy of whole-body vibration training on brain-derived neurotrophic factor, clinical and functional outcomes, and quality of life in women with fibromyalgia syndrome: a randomized controlled trial. J Healthc Eng. 2021;2021:7593802. doi:10.1155/2021/7593802
57. Collado-Mateo D, Dominguez-Muñoz FJ, Adsuar JC, Merellano-Navarro E, Gusi N. Exergames for women with fibromyalgia: a randomised controlled trial to evaluate the effects on mobility skills, balance and fear of falling. PeerJ. 2017;5:e3211. doi:10.7717/peerj.3211
58. Rehfeld K, Müller P, Aye N, et al. Dancing or fitness sport? The effects of two training programs on hippocampal plasticity and balance abilities in healthy seniors. Front Hum Neurosci. 2017;11:305. doi:10.3389/fnhum.2017.00305
59. Vendramin B, Bergamin M, Gobbo S, et al. Health benefits of zumba fitness training: a systematic review. PM R. 2016;8(12):1181–1200. doi:10.1016/j.pmrj.2016.06.010
60. Busch AJ, Schachter CL, Overend TJ, Peloso PM, Barber KA. Exercise for fibromyalgia: a systematic review. J Rheumatol. 2008;35(6):1130–1144.
61. Vilarino GT, Andreato LV, de Souza LC, Branco JHL, Andrade A. Effects of resistance training on the mental health of patients with fibromyalgia: a systematic review. Clin Rheumatol. 2021;40(11):4417–4425. doi:10.1007/s10067-021-05738-z
62. Gómez-Hernández M, Gallego-Izquierdo T, Martínez-Merinero P, et al. Benefits of adding stretching to a moderate-intensity aerobic exercise programme in women with fibromyalgia: a randomized controlled trial. Clin Rehabil. 2020;34(2):242–251. doi:10.1177/0269215519893107
63. De Medeiros SA, De Almeida Silva HJ, Do Nascimento RM, Da Silva Maia JB, De Almeida Lins CA, De Souza MC. Mat Pilates is as effective as aquatic aerobic exercise in treating women with fibromyalgia: a clinical, randomized and blind trial. Adv Rheumatol. 2020;60(1). doi:10.1186/s42358-020-0124-2
64. Gavi MBRO, Vassalo DV, Amaral FT, et al. Strengthening exercises improve symptoms and quality of life but do not change autonomic modulation in fibromyalgia: a randomized clinical trial. PLoS One. 2014;9(3):e90767. doi:10.1371/journal.pone.0090767
65. Glasgow A, Stone TM, Kingsley JD. Resistance exercise training on disease impact, pain catastrophizing and autonomic modulation in women with fibromyalgia. Int J Exerc Sci. 2017;10(8):1184–1195.
66. Acosta-Gallego A, Ruiz-Montero PJ, Castillo-Rodríguez A. Land- and pool-based intervention in female fibromyalgia patients: a randomized-controlled trial. Turkish J Phys Med Rehabilitat. 2018;64(4):337–343. doi:10.5606/tftrd.2018.2314
67. Altan L, Korkmaz N, Bingol Ü, Gunay B. Effect of pilates training on people with fibromyalgia syndrome: a pilot study. Arch Phys Med Rehabil. 2009;90(12):1983–1988. doi:10.1016/j.apmr.2009.06.021
68. Andrade A, Sieczkowska SM, Vilarino GT. Resistance training improves quality of life and associated factors in patients with fibromyalgia syndrome. PM R. 2019;11(7):703–709. doi:10.1016/j.pmrj.2018.09.032
69. Andrade A, Torres Vilarino G, Guimarães Bevilacqua G. What is the effect of strength training on pain and sleep in patients with fibromyalgia? Am J Phys Med Rehabil. 2017;96(12):
70. Andrade CP, Zamunér AR, Forti M, Tamburús NY, Silva E. Effects of aquatic training and detraining on women with fibromyalgia: controlled randomized clinical trial. Eur J Phys Rehabil Med. 2019;55(1):79–88. doi:10.23736/S1973-9087.18.05041-4
71. Arakaki JS, Jennings F, Estrela GQ, Cruz Martinelli VDG, Natour J. Strengthening exercises using Swiss ball improve pain, health status, quality of life and muscle strength in patients with fibromyalgia: a randomized controlled trial. Reumatismo. 2021;73(1):15–23. doi:10.4081/reumatismo.2021.1357
72. Assumpção A, Matsutani LA, Yuan SL, et al. Muscle stretching exercises and resistance training in fibromyalgia: which is better? A three-arm randomized controlled trial. Eur J Phys Rehabil Med. 2018;54(5):663–670. doi:10.23736/S1973-9087.17.04876-6
73. Baptista AS, Villela AL, Jones A, Natour J. Effectiveness of dance in patients with fibromyalgia: a randomised, single-blind, controlled study. Clin Exp Rheumatol. 2012;30(SUPPL.74):S18–S23.
74. Bongi SM, Di Felice C, Del Rosso A, et al. The efficacy of the Rességuier method in the treatment of fibromyalgia syndrome: a randomised controlled trial. Clin Exp Rheumatol. 2010;28(6SUPPL. 63):S46–S50.
75. Britto A, Rodrigues V, Dos Santos AM, et al. Effects of water- and land-based exercises on quality of life and physical aspects in women with fibromyalgia: a randomized clinical trial. Musculoskeletal Care. 2020;18(4):459–466. doi:10.1002/msc.1481
76. Carson JW, Carson KM, Jones KD, Bennett RM, Wright CL, Mist SD. A pilot randomized controlled trial of the Yoga of Awareness program in the management of fibromyalgia. Pain. 2010;151(2):530–539. doi:10.1016/j.pain.2010.08.020
77. Carvalho MS, Carvalho LC, Menezes FDS, Frazin A, Gomes EDC, Iunes DH. Effects of exergames in women with fibromyalgia: a randomized controlled study. Games Health J. 2020;9(5):358–367. doi:10.1089/g4h.2019.0108
78. Collado-Mateo D, Dominguez-Muñoz FJ, Adsuar JC, Garcia-Gordillo MA, Gusi N. Effects of exergames on quality of life, pain, and disease effect in women with fibromyalgia: a randomized controlled trial. Arch Phys Med Rehabil. 2017;98(9):1725–1731. doi:10.1016/j.apmr.2017.02.011
79. Duruturk N, Tuzun EH, Culhaoglu B. Is balance exercise training as effective as aerobic exercise training in fibromyalgia syndrome? Rheumatol Int. 2014;35(5):845–854. doi:10.1007/s00296-014-3159-z
80. Demir-Göçmen D, Altan L, Korkmaz N, Arabacı R. Effect of supervised exercise program including balance exercises on the balance status and clinical signs in patients with fibromyalgia. Rheumatol Int. 2013;33(3):743–750. doi:10.1007/s00296-012-2444-y
81. Espí-López GV, Inglés M, Ruescas-Nicolau MA, Moreno-Segura N. Effect of low-impact aerobic exercise combined with music therapy on patients with fibromyalgia. A pilot study. Complement Ther Med. 2016;28:1–7. doi:10.1016/j.ctim.2016.07.003
82. Evcik D, Yigit I, Pusak H, Kavuncu V. Effectiveness of aquatic therapy in the treatment of fibromyalgia syndrome: a randomized controlled open study. Rheumatol Int. 2008;28(9):885–890. doi:10.1007/s00296-008-0538-3
83. Garrido-Ardila EM, González-López-Arza MV, Jiménez-Palomares M, García-Nogales A, Rodríguez-Mansilla J. Effectiveness of acupuncture vs. core stability training in balance and functional capacity of women with fibromyalgia: a randomized controlled trial. Clin Rehabil. 2020;34(5):630–645. doi:10.1177/0269215520911992
84. Larsson A, Palstam A, Löfgren M, et al. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia-a randomized controlled trial. Arthritis Res Ther. 2015;17(1). doi:10.1186/s13075-015-0679-1
85. Jones KD, Burckhardt CS, Clark SR, Bennett RM, Potempa KM. A randomized controlled trial of muscle strengthening versus flexibility training in fibromyalgia. J Rheumatol. 2002;29(5):1041–1048.
86. Kingsley JD, Panton LB, Toole T, Sirithienthad P, Mathis R, McMillan V. The effects of a 12-week strength-training program on strength and functionality in women with fibromyalgia. Arch Phys Med Rehabil. 2005;86(9):1713–1721. doi:10.1016/j.apmr.2005.04.014
87. Norouzi E, Hosseini F, Vaezmosavi M, Gerber M, Pühse U, Brand S. Zumba dancing and aerobic exercise can improve working memory, motor function, and depressive symptoms in female patients with Fibromyalgia. Eur J Sport Sci. 2020;20(7):981–991. doi:10.1080/17461391.2019.1683610
88. Olivares PR, Gusi N, Parraca JA, Adsuar JC, Del Pozo-Cruz B. Tilting whole body vibration improves quality of life in women with fibromyalgia: a randomized controlled trial. J Altern Complement Med. 2011;17(8):723–728. doi:10.1089/acm.2010.0296
89. Park HK, Song MK, Kim DJ, Choi IS, Han JY. Comparison of core muscle strengthening exercise and stretching exercise in middle-aged women with fibromyalgia A randomized, single-blind, controlled study. Medicine. 2021;100(50):E27854. doi:10.1097/MD.0000000000027854
90. Richards SCM, Scott DL. Prescribed exercise in people with fibromyalgia: parallel group randomised controlled trial. Br Med J. 2002;325(7357):185–187. doi:10.1136/bmj.325.7357.185
91. Rodríguez-Mansilla J, Mejías-Gil A, Garrido-Ardila EM, Jiménez-Palomares M, Montanero-Fernández J, González-López-arza MV. Effects of non-pharmacological treatment on pain, flexibility, balance and quality of life in women with fibromyalgia: a randomised clinical trial. J Clin Med. 2021;10(17):3826. doi:10.3390/jcm10173826
92. Sañudo B, Carrasco L, de Hoyo M, McVeigh JG. Effects of exercise training and detraining in patients with fibromyalgia syndrome: a 3-yr longitudinal study. Am J Phys Med Rehabil. 2012;91(7):561–569; quiz 570–573. doi:10.1097/PHM.0b013e31824faa03
93. Sañudo B, Galiano D, Carrasco L, de Hoyo M, McVeigh JG. Effects of a prolonged exercise program on key health outcomes in women with fibromyalgia: a randomized controlled trial. J Rehabilitat Med. 2011;43(6):521–526. doi:10.2340/16501977-0814
94. Sarmento CVM, Moon S, Pfeifer T, et al. The therapeutic efficacy of Qigong exercise on the main symptoms of fibromyalgia: a pilot randomized clinical trial. Integr Med Res. 2020;9(4):100416. doi:10.1016/j.imr.2020.100416
95. Sevimli D, Kozanoglu E, Guzel R, Doganay A. The effects of aquatic, isometric strength-stretching and aerobic exercise on physical and psychological parameters of female patients with fibromyalgia syndrome. J Phys Ther Sci. 2015;27(6):1781–1786. doi:10.1589/jpts.27.1781
96. Tomas-Carus P, Branco JC, Raimundo A, Parraca JA, Batalha N, Biehl-Printes C. Breathing exercises must be a real and effective intervention to consider in women with fibromyalgia: a pilot randomized controlled trial. J Altern Complement Med. 2018;24(8):825–832. doi:10.1089/acm.2017.0335
97. Tomas-Carus P, Gusi N, Häkkinen A, Häkkinen K, Leal A, Ortega-Alonso A. Eight months of physical training in warm water improves physical and mental health in women with fibromyalgia: a randomized controlled trial. J Rehabilitat Med. 2008;40(4):248–252. doi:10.2340/16501977-0168
98. Tomas-Carus P, Häkkinen A, Gusi N, Leal A, Häkkinen K, Ortega-Alonso A. Aquatic training and detraining on fitness and quality of life in fibromyalgia. Med Sci Sports Exerc. 2007;39(7):1044–1050. doi:10.1249/01.mss.0b0138059aec4
99. Valim V, Oliveira L, Suda A, et al. Aerobic fitness effects in fibromyalgia. J Rheumatol. 2003;30(5):1060–1069.
100. Villafaina S, Borrega-mouquinho Y, Fuentes-garcía JP, Collado-mateo D, Gusi N. Effect of exergame training and detraining on lower-body strength, agility, and cardiorespiratory fitness in women with fibromyalgia: single-blinded randomized controlled trial. Int J Environ Res Public Health. 2020;17(1):161.
101. Villafaina S, Collado-Mateo D, Domínguez-Muñoz FJ, Fuentes-García JP, Gusi N. Benefits of 24-week exergame intervention on health-related quality of life and pain in women with fibromyalgia: a single-blind, randomized controlled trial. Games Health J. 2019;8(6):380–386. doi:10.1089/g4h.2019.0023
102. Horven Wigers S, Stiles TC, Vogel PA. Effects of aerobic exercise versus stress management treatment in fibromyalgia. Scand J Rheumatol. 1996;25(2):77–86. doi:10.3109/03009749609069212
103. Wong A, Figueroa A, Sanchez-Gonzalez MA, Son WM, Chernykh O, Park SY. Effectiveness of tai chi on cardiac autonomic function and symptomatology in women with fibromyalgia: a randomized controlled trial. J Aging Phys Act. 2018;26(2):214–221. doi:10.1123/japa.2017-0038
104. Haak T, Scott B. The effect of Qigong on fibromyalgia (FMS): a controlled randomized study. Disabil Rehabil. 2008;30(8):625–633. doi:10.1080/09638280701400540
105. Mingorance JA, Montoya P, Miranda JGV, Riquelme I. A comparison of the effect of two types of whole body vibration platforms on fibromyalgia. A randomized controlled trial. Int J Environ Res Public Health. 2021;18(6):1–14. doi:10.3390/ijerph18063007
106. Van Eijk-Hustings Y, Kroese M, Tan F, Boonen A, Bessems-Beks M, Landewé R. Challenges in demonstrating the effectiveness of multidisciplinary treatment on quality of life, participation and health care utilisation in patients with fibromyalgia: a randomised controlled trial. Clin Rheumatol. 2013;32(2):199–209. doi:10.1007/s10067-012-2100-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.