")
Back to Journals » Vascular Health and Risk Management » Volume 18
Screening for Atrial Fibrillation by Village Doctors in Rural Areas of China: The Jiangsu Province Rural Community AF Project
Authors Li M, Shi J, Chu M, Shen Y, Zhang S, Sun X , Zhang H, Yan Q, Gong J, Lip GYH, Chen M
Received 19 June 2022
Accepted for publication 5 September 2022
Published 15 September 2022 Volume 2022:18 Pages 757—766
DOI https://doi.org/10.2147/VHRM.S379182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Mirna N Chahine
Mingfang Li,1 Jiaojiao Shi,1 Ming Chu,1 Youmei Shen,1 Shimeng Zhang,1 Xingxing Sun,1 Hengli Zhang,1 Qing Yan,1 Jinlong Gong,2 Gregory YH Lip,3,4 Minglong Chen1,5
1Division of Cardiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 2Division of Cardiology, Jiangdu People’s Hospital, Yangzhou, People’s Republic of China; 3Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart & Chest Hospital, Liverpool, UK; 4Department of Clinical Medicine, Aalborg University, Aalborg, Denmark; 5Division of Cardiology, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China
Correspondence: Minglong Chen, Division of Cardiology, the First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Tel +86-25-68303115, Fax +86-25-6813-6479, Email [email protected]
Abstract: China has a large population of elderly in rural areas. Village doctors are acting as health-care gatekeepers for the rural elderly in China and are encouraged to provide more long-term care for patients with chronic diseases such as atrial fibrillation (AF). The data of AF registries from the rural elderly are limited. The present registry aims to provide contemporary data on the current AF-related health status of the rural elderly and the gaps in management of AF by village doctors. This study has two phases. The first phase is a cross-sectional study of AF screening in two rural towns of eastern China. All the residents aged ≥ 65 years are eligible and will be invited to attend a government-led health examination or an in-house AF screening program. The AF detection rate, the awareness of AF and the usage of oral anticoagulants and smartphones by AF patients, and the ability to diagnose and manage AF by village doctors will be assessed. Participants with AF detected in the first phase are eligible for the second phase. A variety of modes of intensified education will be provided to all AF patients and their family members to enrich their AF-related knowledge. Their village doctors will be offered a lecture-based training program focusing on Atrial fibrillation Better Care (ABC) pathway. Follow-up will be conducted for 1 year. The primary endpoint is the composite of all stroke and all-cause mortality. The first phase of AF screening was conducted between April 2019 and June 2019, and 18,712 participants with the mean age of 73.1± 5.8 years were enrolled. The second phase that includes 810 patients with AF, started on 1 May 2019. This study will provide a perspective of primary care system and would indirectly reflect the current status of chronic disease care in rural China.
Keywords: atrial fibrillation, elderly, village doctors, rural China
Introduction
Rural China has been recognized as an ageing society since the 21st century. In 2020, China has a population of over 500 million (36.11%) in rural areas.1 The proportion of elderly people (age ≥65 years old) relative to the total population was 9.6% in 2005 and is projected to be 15% by 2020, which rises further to 21% by 2030 in rural areas of China.2 In addition to the rural-to-urban migration of young adults for higher income earning opportunities, better living and health-care condition, a declining birth rate, and longer life expectancy have all contributed to the accelerated process of population ageing in rural China.
Elderly people living in rural areas remain vulnerable due to their low educational attainment, low awareness of treatable conditions and health knowledge, insufficient family-based care as a result of the migration of their adult children, and low pension coverage.3–5 The ageing society in rural areas puts increasing stress on health-care structures. The Chinese government has recently attached great importance to the “left behind” neglected elderly in rural China. For instance, the New Rural Cooperative Medical Scheme was put into effect in 2003, aiming to improve rural primary care and preventive healthcare to rural residents in China.6 Nevertheless, the rural elderly population is still characterized by unsatisfactory health status and limited access to good quality healthcare, partly because the reimbursement rates of the scheme remains relatively low.7 In addition, effective mechanisms to coordinate health institutions to ensure continuity of care have not been properly established.8
Most of the rural elderly in China access their preventive healthcare and primary medical care mainly through village doctors for decades. To this day, these village doctors still act as health-care gatekeepers for the rural elderly, and they are particularly important for those rural elderly who are often unable to access upper-tier health-care centers due to long travel time.9 To improve the quality of village doctors, a series of national policies have been established since 1990. Particularly, the “Village Doctors Practitioners Regulation” was issued by the State Council in 2003, providing the first relevant national regulation that outlined the legal obligations of village doctors, and the training and practice requirement for them.10
Along with the population ageing, fast urbanization, and rapid lifestyle changes, an epidemiological transition has been observed in rural China. Non-communicable chronic disease (NCD) has overcome communicable diseases to become the major disease burden and accounted for most of deaths in rural China.11 Thus, Chinese government has been encouraging village doctors to provide more long-term care for patients with chronic diseases among the rural elderly.10 However, most village doctors face critical challenges, including their increasing age, gender imbalance, a lack of standard medical training, inferior social positions, low salaries, and poor working conditions.7,12 Studies focusing on the capacity of village doctors to deliver long-term chronic disease care are extremely limited.
Atrial fibrillation (AF), the most common cardiac arrhythmia is associated with increased risk of mortality and morbidity, particularly from thromboembolism and heart failure, thus conferring a significant burden to patients, their families and the social economy.13 Previous epidemiological data in China showed that the prevalence of AF in elderly ≥65 years old varied from 2.4% to 5.4%.14 Although China has already reported a number of AF registries,14–19 the data from rural elderly population are very limited.
The present Jiangsu Province Rural Community AF project consists of a cross-sectional study of AF screening in rural elderly and a prospective observational registry of elderly patients with AF in rural China. We aim to provide contemporary data on the current health status of the rural elderly and the current gaps in awareness and management of AF by village doctors.
Materials and Methods
This study has two phases. The first phase is a cross-sectional study of AF screening focusing on the elderly in rural China. The second phase is a prospective observational registry of elderly patients with AF in rural China. This study is conducted in accordance with the Declaration of Helsinki.
The First Phase of This Study
The first phase of this present study is a cross-sectional study conducted in Daqiao Town and Xiaoji Town, Jiangdu District, Yangzhou City, Jiangsu Province. The study area is a well-developed rural region in eastern China (Figure 1). This first phase has two steps (Figure 2). All the permanent residents aged 65 years or above in these two towns are eligible and will be invited to participate in the first step, which is primary medical center-based government-led health examination. Those who refuse to participate the first step will then be invited to participate for the second step, which is a village clinic-based in-house AF screening program developed by a panel of AF specialists, and conducted with the assistance of village doctors. Posters and leaflets used to invite participants will be placed around the villages by the village leaders two weeks before this study.
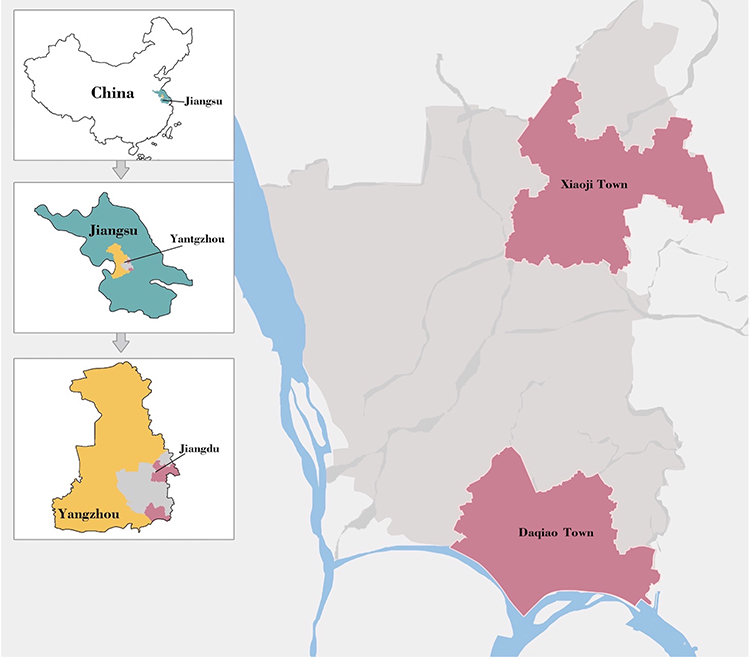 |
Figure 1 Geographical location of the study. Residents aged 65 and above were recruited from Daqiao Town and Xiaoji Town in Jiangdu, Yangzhou City, Eastern China. |
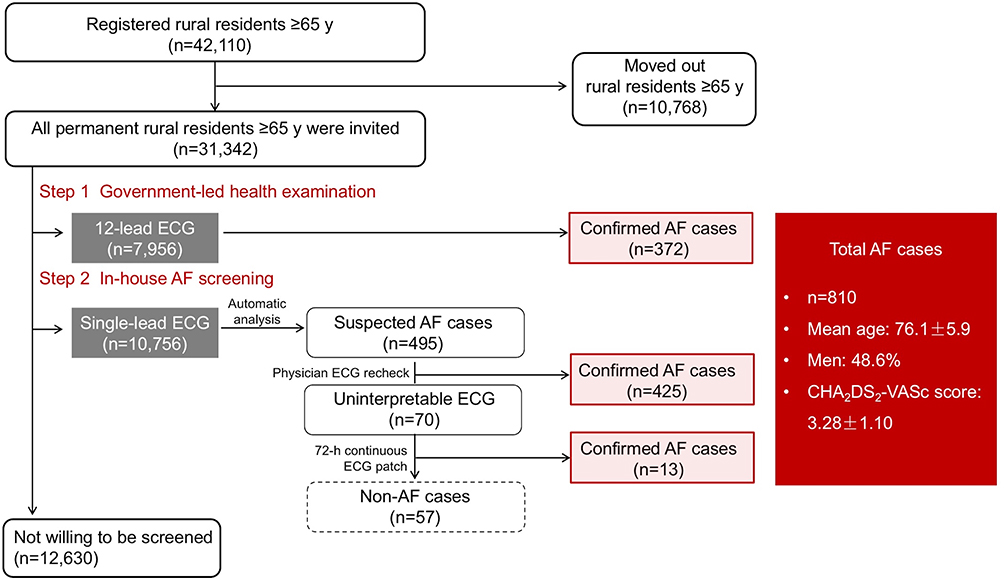 |
Figure 2 The flow chart of the first phase of this study. Abbreviations: AF, atrial fibrillation; ECG, electrocardiograph. |
ECG Acquisition and Analysis
In the first step, a 12-lead electrocardiogram (ECG, CardiMax FX-8322, Fukuda Denshi, Japan) will be used. In order to confirm the diagnosis of AF, the ECG strips will be interpreted by two independent AF specialists. In the second step, a mobile single-lead ECG monitor device consisting of a smartphone software application and a handheld hardware component with two electrodes (SnapECG E-U08/E-A08, Xijian Information Technology Co., Ltd., Nanjing, China) will be used. To undergo an ECG test, participants will be instructed to place each of their thumbs on each electrode of the hardware component. A 30-second lead I ECG will be recorded for every participant. The SnapECG has an automated algorithm to interpret the ECG strips. According to our previous study, this algorithm has a sensitivity of 86.2%, an accuracy of 92.6%, and a negative predictive value of 86.2% for the diagnosis of atrial arrhythmia.20 If AF is suspected after the automated analysis, the original single-lead ECG strip will be reviewed by two independent AF specialists to confirm the diagnosis of AF. Participants who have uninterpretable ECGs will be then advised to undergo a 72-hour continuous ECG patch (ECG-SNI-B, Zhengxin Medical Technology Co., Ltd., Shandong, China).
AF is diagnosed if any following criterion are met: (i) AF pattern in 12-lead ECG screening (absolutely irregular RR intervals without discernible and distinct P waves); (ii) AF pattern lasting over 30s in single-lead ECG; or (iii) AF episodes (a minimum of 2 similar episodes lasting over 10s in 72-hour continuous ECG patch).
Data Collection and Measurement
Every enrolled participant will undergo a face-to-face interview using a standardized questionnaire. The following information will be obtained for every participant: the demographic characteristics (age and sex) and prior history of cardiovascular comorbidities including hypertension, diabetes mellitus, previous stroke or transient ischemic attack (TIA), coronary artery disease (CAD) or peripheral artery disease (PAD), and congestive heart failure. CHA2DS2-VASc score will be calculated. In addition, resting blood pressure and fasting blood glucose level will be measured.
For patients with confirmed AF, an additional brief survey will be conducted. Information on their highest education level, the awareness of AF, use of oral anticoagulants, and use of smartphone (the type of mobile phone used and the purpose of using a smartphone) in these patients will be obtained.
All the village doctors in Daqiao Town and Xiaoji Town will also be invited to participate a questionnaire survey. Data are collected regarding the age, sex, full-time practicing, practicing experience, highest education, type of medical education, qualification, professional title, and frequency of medical training received during their clinical practice. In addition, numbers of village doctors in every village clinic as well as distance from the village clinic to township central hospitals will be investigated. Furthermore, the ability to diagnose and treat AF by village doctors will be estimated using this self-report questionnaire. The information of numbers of villagers served per village clinic and village doctors per 1000 population will be provided by Health Commission of Jiangdu District.
Statistical Analysis
Categorical variables will be presented as numbers and percentages, and groups with or without AF detected will be compared using χ2 tests. Continuous variables will be presented as mean± standard deviation (SD) or medians and interquartile ranges (IQRs), and groups will be compared using the t tests or Wilcoxon rank sum tests if the data are not normally distributed. Multivariable logistic regression will be performed to identify the association between AF and existing risk factors. Variables with a P value <0.05 in univariate analysis will be included in the multivariable logistic regression model. The odds ratios (ORs) and corresponding 95% confidence intervals (CIs) will be calculated to assess the association. SPSS software version 26.0 (IBM Corporation, New York, America) will be used for all the statistical analyses. All statistical tests will be 2-sided, and a P-value <0.05 will be considered to be statistically significant.
The Second Phase of This Study
This second phase of this present study is a prospective observational registry. Participants with AF detected in the first phase are eligible for the second phase. All the enrolled patients should understand and consent to participate in the study. Figure 3 shows the study flow chart of the second phase.
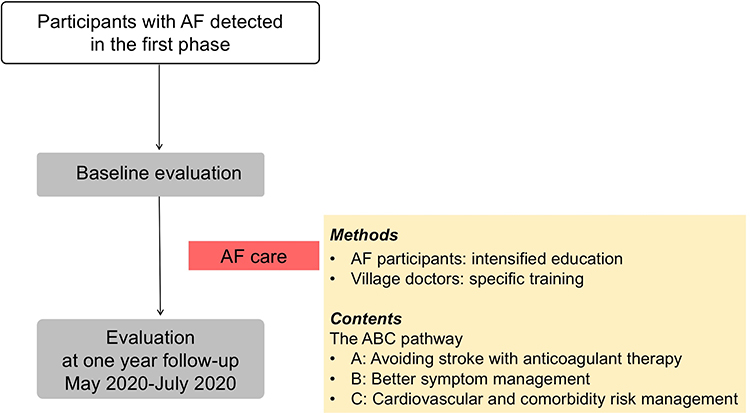 |
Figure 3 The flow chart of the second phase of this study. Abbreviations: AF, atrial fibrillation; ABC pathway, Atrial fibrillation Better Care pathway. |
Intensified Education Targeting AF Patients and Their Family Members
After enrollment, AF patients and their family members will receive intensified education. The main objective is to increase awareness of AF and knowledge related to prevention and treatment of AF. The key points of the intensified education are as follows: what AF is; the main complications that AF may lead to; risk factors that can facilitate incident AF; the relationship of AF and stroke; the importance of taking OACs; and the possible bleeding complications associated with OACs. This intensified education will involve the use of educational videos dubbed in local dialect, a monograph consisting of AF-related knowledge, information brochure about AF, and popular science articles pushed on our WeChat public account. The Wechat application is a social media and instant messaging tool mainly for the adult children of the rural elderly.
In order to encourage interactions with village doctors, patients and their family members will be invited to participate group discussion sessions organized in village clinics. All the patients will encourage to have a visit to their village clinics every month. The feedback is assessed by identifying patients for not using (or stopping) oral anticoagulation and their possible reasons for withholding therapy.
Specific Training to Village Doctors Regarding AF Management
Village doctors will be provided with a specific training program regarding AF management by AF specialists. The main objective of the training program targeting village doctors is to increase their knowledge of integrated care for patients with AF using the guideline-recommended Atrial fibrillation Better Care (ABC) pathway,21–23 whereby adherence to this holistic management approach has been associated with improved clinical outcomes.24,25 In this program, a series of lectures will be provided by AF specialists. In the end, AF specialists will provide education directed towards specific knowledge gaps in every individual village doctor based on his or her prior knowledge evaluation. In addition, all the teaching materials are available via a special developed online education platform. Feedback from village doctors will be assessed by evaluating if their knowledge level is improved after the specific training. In addition, the difference of this knowledge level between village doctors who participated our registry and those without participation will be evaluated.
Compliance of the ABC Pathway Components
The A, B, and C components of the ABC pathway are defined as follows, based on the ESC Guidelines:22 The “A” criterion refers to “Avoid stroke” or “Anticoagulation”, and is defined by the quality of anticoagulation. “A criterion compliant” means that either appropriate Non-vitamin K antagonist oral anticoagulation (NOAC) is used, or alternatively, warfarin is used with the time in therapeutic range (TTR) ≥65%. The TTR will be calculated with the method by Rosendaal et al.26 Patients who do not receive NOAC or have a TTR <65% with warfarin will be considered as “A non-compliant”.
The “B” criterion stands for “Better symptoms control”, based on the presence of symptoms, classified by the European Heart Rhythm Association (EHRA) symptom scale.27 Patients with EHRA score of I (no symptoms) or II (mild symptoms without affecting normal daily activity) have good control of AF symptoms and will be considered as “B compliant”. Patients with EHRA score of III (severe symptoms with normal daily activity affected) or IV (disabling symptoms with normal daily activity discontinued) will be considered as “B non-compliant”, which means that the treatment to control symptoms is insufficient.
“C” stands for “cardiovascular risk and other comorbidity optimization”. Cardiovascular risk factors and comorbidities, eg, hypertension, diabetes mellitus, heart failure, and coronary artery disease and ischemic stroke, are defined in accordance with international guidelines.28–31 “C compliant” means that all considered risk factors have been well controlled or be properly treated. Uncontrolled risk factors include high blood pressure (≥160/90 mmHg), high level of fasting blood glucose (≥7.0 mmol/L), obesity (BMI ≥30 kg/m2), current smoking, and current alcohol drinking. Patients who met all the three criteria for integrated care will be defined as the “ABC compliant” group, otherwise the patients will be considered as the “Non-ABC compliant” group.
Evaluation and Study Outcomes
Patients will be evaluated at baseline as described in the section of the first phase. Follow-up will be performed at 12 months. The primary endpoint in this prospective cohort study is the composite of all stroke and all-cause mortality. The secondary endpoints are all stroke, all-cause mortality, cardiovascular death, and the number of patients with ABC pathway criteria fulfilled. All stroke is defined as ischemic/hemorrhagic stroke or TIA. The cause of death will be evaluated according to the death certification provided by Health Commission of Jiangdu District. Cardiac deaths include deaths caused by myocardial infarction, sudden cardiac death, heart failure, stroke, cardiovascular procedures, cardiovascular hemorrhage, and deaths resulting from other cardiovascular causes. The AF-related knowledge level in village doctors will also be evaluated.
Statistical Analysis
The general statistical analysis plan is consistent with what is described in the section of the first phase. In the second phase of the present study, the major analysis will compare the incidence rate of outcome events between participants with and without AF detected in this local area. In addition, the incidence rate will be compared between the “ABC” group vs the “Non-ABC” group among AF patients. The cumulative incidence of the outcome events will be estimated using a Kaplan–Meier curve and compared with the Log rank test. A cox proportional hazards regression analysis will be performed to analyze the association between the group considered and the study outcomes. The hazard ratio (HR) and 95% CI will be used to express the association. All multivariable regression models will be adjusted for age, gender, and other major cardiovascular risk factors. The secondary analysis will compare the annual risk of ischemic stroke between AF patient in this registry and CHA2DS2-VASc score-matched non-anticoagulated patients without using any form of anticoagulation in published literature.32 The relative risk reductions will be determined.
Sample Size and Power Calculations
Considering that this is a fully observational study, a formal sample size has not been determined. Especially in the first phase of the cross-sectional AF screening study, the aim was to recruit as many participants as possible in the rural areas.
Patient and Public Involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Study Setting and Site Selection
Daqiao town and Xiaoji town in Jiangdu District, Yangzhou city are selected as our study sites. This rural area is relatively more well-developed compared to other rural area in China. This study is conducted with the help of local government and Health Commission of Jiangdu District. Patient evaluation and follow-up are performed in the local village clinics.
Data Management
All the data will be collected locally and gathered to the central research database. Data management for this registry will be performed by an independent third party, which is EnChannel Information Technology Co. Ltd. This independent third-party audit will mainly focus on the rights, health and safety of the participants. The study sites are required to conduct the study according to protocol, with all the requirements met by the site staff and facility.
The Status of the Study
The study protocol V.2.0 dated 1 Mar 2019 was approved by the Institutional Review Board of Jiangdu People’s Hospital (Approval number: YJRY-K-2019-01). The first phase of AF screening was conducted between 1 April 2019 and 30 June 2019, and a total of 18,712 participants with the mean age of 73.1±5.8 years were enrolled in the first phase. In the second phase, the recruitment of participants started on 1 May 2019. Follow-up of patients was completed in July 2020. Database cleaning is currently in progress, and data analysis is expected to be performed in August 2022.
Discussion
The Jiangsu Province Rural Community AF project is a two-phase observational study which will update our understanding of AF management among elderly population in rural China. It will also provide a perspective of primary care system and would also indirectly reflect the current status of chronic disease care in rural China.
The ESC Guidelines for the AF management puts great emphasis on the role of health education on AF management and stresses the importance of patient-centered integrated care.22 The guidelines point out that the tailored patient education should be recommended for all phases of AF management (Class I), which would be favorable for lifestyle change and self-management of AF patients (Class IIa). Meanwhile, teamwork comprising not only the specialized cardiologist, but also general physicians and the advanced technology tools for knowledge transmission are highlighted for AF integrated care management.
A large nationwide community-based survey in China has demonstrated the low awareness of AF and the large treatment gap.14 More than one-third of the patients with AF were unaware of their condition, and only 6% of patients with high-risk AF received anticoagulation therapy.14 The ChiOTEAF registry recently reported that even in the era of NOACs, only 44.7% of all eligible elderly Chinese patients with AF were prescribed with guideline-directed anticoagulation.18 In addition, assessment of quality measures and clinical performance indicators revealed the gaps in AF care among Chinese patients in the ChiOTEAF registry.18 Of note, the AF population in these studies were mainly from large cities, medium-sized urban areas, or an urban-rural mixture. Indeed, data on the rural elderly with AF in China remain under-represented in the literature. Given that AF is a serious public health problem and the rural elderly is a “left behind” neglected population in China, we estimate that the outlook for the management of AF in rural elderly is less positive. Therefore, it is important that a more specific integrated or holistic approach to AF management for rural elderly should be implemented.
The first phase of our observational study was the two-step AF screening program, where we will address the knowledge gap in AF prevalence in rural elderly in China. This disadvantaged and vulnerable population is likely to refuse to participate the first step of government-led health examination, even though it was free for service. The travel difficulties faced by rural elderly may limit their spatial accessibility of health services. Therefore, we also performed a second step, ie, in-house screening with the assistance of village doctors. It would hopefully be more convenient and acceptable for the rural elderly to be examined at home or close to their home.
Health education has already been announced as one category of the basic public health services provided for urban and rural residents.33 Telemedicine is being encouraged to facilitate patient health-related education. In the present study, we will also investigate the rate of smartphone use in rural elderly, and the data will provide rationale whether implementing telemedicine through smartphones among rural elderly in China is feasible.
The ability of AF management by village doctors will be evaluated in the present study. Health care delivery system in rural China has three tiers including county hospitals as the bellwether, and township central hospitals and village clinics as the basis.34 Village doctors are the front-line basic health-care providers in the first tier. The heavy workload of primary care can cause village doctors to lose their job motivation and satisfaction, which may lead to job burnout.35 Indeed, with the rapidly ageing population, the estimated NCD burden is 82% of the total disease and keeps growing.36
A series of studies have demonstrated the beneficial effect of education on AF management. In IMPACT-AF trial, the impact of a multifaceted educational intervention on the use of OAC in 2281 patients with AF was assessed.37 After one-year follow up, compliance to OAC usage increased in the intervention group from 68% to 80%, compared to only 3% increase in patients under usual care. A reduction in stroke (HR 0.48, 95% CI 0.23–0.99) between the two groups was also observed although the composite endpoint had no significant difference. In the second phase of the present study, we intend to examine whether intensified education strategy for rural elderly patients and specific training program for village doctors can provide better clinical outcome and more efficient integrated management reflected by the ABC pathway compliance in this vulnerable population.
Limitations
Our study certainly has its limitations. The population was not selected from several representative areas in China, but a rural area from a well-developed region; however, it provides a deep perspective of the current public healthcare system in rural China. Problems exposed in this study should be common in other areas, if not more. The present study also could not cover all the eligible elderly in the study area, but this is determined by the nature of this special population.
Conclusion
The Jiangsu Province Rural Community Atrial Fibrillation project is a large prospective observational study in the rural setting of China, which area was under-presented in previous studies. This project specifically focuses on AF screening and management among elderly population and will provide a deep perspective of primary care system in rural China.
Data Sharing Statement
No additional data are available.
Ethics Approval and Informed Consent
Ethics approval was granted by Institutional Review Board of Jiangdu People’s Hospital (approval no. YJRY-K-2019-01). The (inter)national research presentations, peer-reviewed publications and media coverage of the research will be used for dissemination of the results. Informed consent will be obtained from all enrolled participants.
Acknowledgments
Steering committee members: Minglong Chen, MD (The First Affiliated Hospital of Nanjing Medical University and the Affiliated Hospital of Xuzhou Medical University (Chair)); Yiyang Zhan, MD (The First Affiliated Hospital of Nanjing Medical University); Zhirong Wang, MD (The Affiliated Hospital of Xuzhou Medical University); Jinlong Gong, MD (Jiangdu People’s Hospital).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The Clinical Medicine Expert Team Project of Xuzhou, China (ID: 2019208002) and the Key Clinical Study Project of Jiangsu Province, China (ID: BE2017750).
Disclosure
All the authors have nothing to declare except for GYHL and MLC. GYHL is a consultant and speaker for Boehringer Ingelheim, BMS/Pfizer and Daiichi-Sankyo. MLC reports receiving lecture fee from Biosense Webster, St. Jude Medical, Medtronic, Bayer and Boehringer Ingelheim; also reports grants from The Clinical Medicine Expert Team Project of Xuzhou, grants from The Key Clinical Study Project of Jiangsu Province, during the conduct of the study. No fees are received personally.
References
1. China’s urban residents up to 63.89% of total population; 2021. Available from: http://english.www.gov.cn/archive/statistics/202105/11/content_WS609a1853c6d0df57f98d9558.html.
2. Cai F, Giles J, O’Keefe P, Wang D. The elderly and old age support in Rural China: challenges and prospects. The World Bank; 2012.
3. Yuan F, Qian D, Huang C, et al. Analysis of awareness of health knowledge among rural residents in Western China. BMC Public Health. 2015;15(1):55. doi:10.1186/s12889-015-1393-2
4. Liu Z, Albanese E, Li S, et al. Chronic disease prevalence and care among the elderly in urban and rural Beijing, China - a 10/66 Dementia research group cross-sectional survey. BMC Public Health. 2009;9(1):394. doi:10.1186/1471-2458-9-394
5. John G, Dewen W, Changbao Z. Can China’s rural elderly count on support from adult children? Implications of rural-to-urban migration. J Popul Ageing. 2010;3:183–204. doi:10.1007/s12062-011-9036-6
6. Watts J. China’s rural health reforms tackle entrenched inequalities. Lancet. 2006;367(9522):1564–1565. doi:10.1016/S0140-6736(06)68675-3
7. Han J, Wu M-C, Yang T. Challenge of China’s rural health. BMJ. 2016;353:i2003. doi:10.1136/bmj.i2003
8. Meng Q, Mills A, Wang L, Han Q. What can we learn from China’s health system reform? BMJ. 2019;365:l2349. doi:10.1136/bmj.l2349
9. Babiarz KS, Yi H, Luo R. Meeting the health-care needs of the rural elderly: the unique role of village doctors. China World Econ. 2013;21(3):44–60. doi:10.1111/j.1749-124X.2013.12021.x
10. The guideline for improving the village doctors by state council; 2021. Available from: http://www.gov.cn/zwgk/2011-07/14/content_1906244.htm.
11. Yang G, Wang Y, Zeng Y, et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. 2013;381(9882):1987–2015. doi:10.1016/S0140-6736(13)61097-1
12. Xu H, Zhang W, Zhang X, et al. Longitudinal study of rural health workforce in five counties in China: research design and baseline description. Hum Resour Health. 2013;11(1):17. doi:10.1186/1478-4491-11-17
13. Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129(8):837–847. doi:10.1161/CIRCULATIONAHA.113.005119
14. Du X, Guo L, Xia S, et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart. 2021;107(7):535–541. doi:10.1136/heartjnl-2020-317915
15. Chen Y, Huang Q-F, Sheng C-S, et al. Detection rate and treatment gap for atrial fibrillation identified through screening in community health centers in China (AF-CATCH): a prospective multicenter study. PLoS Med. 2020;17(7):e1003146. doi:10.1371/journal.pmed.1003146
16. Wang Z, Chen Z, Wang X, et al. The disease burden of atrial fibrillation in China from a national cross-sectional survey. Am J Cardiol. 2018;122(5):793–798. doi:10.1016/j.amjcard.2018.05.015
17. Zhou Z, Hu D. An epidemiological study on the prevalence of atrial fibrillation in the Chinese population of Mainland China. J Epidemiol. 2008;18(5):209–216. doi:10.2188/jea.JE2008021
18. Guo Y, Kotalczyk A, Imberti JF, Wang Y, Lip GYH. Poor adherence to guideline-directed anticoagulation in elderly Chinese patients with atrial fibrillation. A report from the optimal thromboprophylaxis in Elderly Chinese Patients with Atrial Fibrillation (ChiOTEAF) registry. Eur Heart J Qual Care Clin Outcomes. 2021. doi:10.1093/ehjqcco/qcab054
19. Wang X, Fu Q, Song F, et al. Prevalence of atrial fibrillation in different socioeconomic regions of China and its association with stroke: results from a national stroke screening survey. Int J Cardiol. 2018;271:92–97. doi:10.1016/j.ijcard.2018.05.131
20. Cheng C, Gang Y, Guozhen S, et al. Comparison of a portable electrocardiographic home monitor device and conventional 24 h holter during the follow-up of the patient after atrial fibrillation ablation. Chin J Cardiac Arrhyth. 2017;21(04):331–335.
21. Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. 2017;14(11):627–628. doi:10.1038/nrcardio.2017.153
22. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
23. Chao TF, Joung B, Takahashi Y, et al. Focused update consensus guidelines of the asia pacific heart rhythm society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost Nov. 2021;13:2021.
24. Romiti GF, Pastori D, Rivera-Caravaca JM, et al. Adherence to the ‘atrial fibrillation better care’ pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemost. 2021;122(03):406–414.
25. Yoon M, Yang PS, Jang E, et al. Improved population-based clinical outcomes of patients with atrial fibrillation by compliance with the simple ABC (Atrial Fibrillation Better Care) pathway for integrated care management: a nationwide cohort study. Thromb Haemost. 2019;119(10):1695–1703. doi:10.1055/s-0039-1693516
26. Rosendaal FR, Cannegieter SC, van der Meer FJ, Briët E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost. 1993;69(3):236–239. doi:10.1055/s-0038-1651587
27. Kirchhof P, Auricchio A, Bax J, et al. Outcome parameters for trials in atrial fibrillation: executive summary. Eur Heart J. 2007;28(22):2803–2817. doi:10.1093/eurheartj/ehm358
28. Mancia G, Fagard R, Narkiewicz K, et al. 2013 practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC task force for the management of arterial hypertension. J Hypertens. 2013;31(10):1925–1938. doi:10.1097/HJH.0b013e328364ca4c
29. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: the Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
30. Members ATF, McMurray JJV, Adamopoulos S, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. Eur J Heart Fail. 2012;14(8):803–869. doi:10.1093/eurjhf/hfs105
31. Members ATF, Rydén L, Grant PJ, et al. ESC guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the task force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur Heart J. 2013;34(39):3035–3087. doi:10.1093/eurheartj/eht108
32. Friberg L, Rosenqvist M, Lip GYH. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 patients with atrial fibrillation: the Swedish Atrial Fibrillation cohort study. Eur Heart J. 2012;33(12):1500–1510. doi:10.1093/eurheartj/ehr488
33. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395(10239):1802–1812. doi:10.1016/S0140-6736(20)30122-7
34. National healthcare policy announcement of strategic plan on national healthcare service system; 2021. Available from http://www.gov.cn/zhengce/content/2015-03/30/content_9560.htm.
35. Zhang X, Bai X, Bian L, Wang M. The influence of personality, alexithymia and work engagement on burnout among village doctors in China: a cross-sectional study. BMC Public Health. 2021;21(1):1507. doi:10.1186/s12889-021-11544-8
36. Wang S, Marquez P, Langenbrunner J, Niessen L, Suhrcke M, Song F. Toward a healthy and harmonious life in China: stemming the rising tide of non-communicable diseases. The Word Bank; 2012.
37. Vinereanu D, Lopes RD, Bahit MC, et al. A multifaceted intervention to improve treatment with oral anticoagulants in atrial fibrillation (IMPACT-AF): an international, cluster-randomised trial. Lancet. 2017;390(10104):1737–1746. doi:10.1016/S0140-6736(17)32165-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.