")
Back to Journals » Patient Preference and Adherence » Volume 17
Adherence to Atrial Fibrillation Better Care (ABC) Pathway Management of Chinese Community Elderly Patients with Atrial Fibrillation: A Cross-Sectional Study
Authors Zhang X, Huang J, Weng F, Wen Y, Wang X, Jiang J, Xue Y, Li K
Received 15 April 2023
Accepted for publication 8 July 2023
Published 25 July 2023 Volume 2023:17 Pages 1813—1823
DOI https://doi.org/10.2147/PPA.S417384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xiaomin Zhang,1,* Jun Huang,2,* Fan Weng,3 Yanting Wen,3 Xiaoxia Wang,2 Junrong Jiang,4 Yumei Xue,4 Kun Li1
1School of Nursing, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Geriatrics, Guangdong Provincial Geriatrics Institute, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 3Yuexiu District Center for Disease Control and Prevention, Guangzhou, People’s Republic of China; 4Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Xue, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, No. 106 Zhong Shan Second Road, Guangzhou, 510080, People’s Republic of China, Tel +8613570082363, Email [email protected] Kun Li, School of Nursing, Sun Yat-sen University, No. 74 Zhong Shan Second Road, Guangzhou, 510080, People’s Republic of China, Tel +8613822206519, Email [email protected]
Background: Investigating adherence to the Atrial Fibrillation Better Care (ABC) pathway management and identifying gaps between the real world and established guidelines can lead to better integrated management of AF. Current data on adherence to ABC pathway management among community elderly patients with atrial fibrillation (AF) in Chinese communities is limited.
Aim: To investigate the adherence to ABC pathway management among community elderly patients with AF in China.
Methods: In this cross-sectional study, data were collected from the 2020 National Basic Public Health Service Program database that includes health examination information for all residents > 65 years of age in Yuexiu, Guangzhou, Guangdong Province. Demographic and clinical characteristics data from 197 community AF patients were obtained.
Results: Among the 197 AF patients, 103 (52.3%) were male, 117 (59.4%) were ≥ 75 years of age, 127 (64.5%) had a senior middle school education or above, 84.3% were married, and 195 (99.0%) had medical insurance. The most common comorbidities were hypertension (72.1%, 142/197), dyslipidaemia (28.4%, 56/197), CAD (28.9%, 57/197), and diabetes (24.9%, 49/197). In terms of the ABC management pathway, 21.8% (43/197), 82.7% (163/197), and 31.5% (62/197) of AF patients were classified into the A-adherent group, B-adherent group, and C-adherent group, respectively. The level of adherence to ABC pathway management was very low (9.1%, 18/197) and independently associated with age and multimorbidity.
Conclusion: The level of adherence to ABC pathway management in community elderly patients with AF was unsatisfactory. Further research is warranted to improve the integrated management of AF.
Keywords: atrial fibrillation, community, integrated management, elderly
Introduction
Atrial fibrillation (AF) is a type of supraventricular tachyarrhythmia caused by ineffective atrial contraction that results from uncoordinated atrial electrical activity.1 According to 2020 data from the European Society of Cardiology (ESC), there are approximately 46.3 million AF patients worldwide, and this is projected to increase 2.3 times by 2060.1 AF imposes a heavy burden on society and families,2 with about 30% of AF patients hospitalized at least once each year.1 The prevalence of AF increases with age. Results from the largest epidemiological study of AF in China found that the mean age of AF patients was 69.5±11.9 years.3 Patients >60 years of age account for 81.6% of all cases.4 It is critical that AF is effectively managed in elderly individuals.
AF can increase the risk of total death by 3.5 times and cause many complications, of which the most serious is stroke.1 The risk of stroke is 4–5 times higher in patients with AF than those without and is associated with 20% mortality and 60% disability in this patient population.1 Effective anticoagulation is associated with a 64% reduction in stroke risk and a 26% reduction in mortality.1 The main symptoms of AF include palpitations, dyspnea, fatigue, chest tightness/pain, poor endurance and sleep disturbances, which reduce AF patients’ quality of life.5 There are many cardiovascular risk factors for AF.1 Effective risk factor management can reduce the adverse outcomes of AF.1
The 2020 ESC guidelines suggested that the Atrial Fibrillation Better Care (ABC) pathway should be implemented for the integrated management of AF.1 ABC pathway management includes three components: (A) Avoid stroke or anticoagulation, (B) Better symptom control using rate or rhythm control strategies, and (C) Cardiovascular and other comorbidity management.1 A systematic review of 285,000 AF patients by Romiti et al6 showed that adherence to the Atrial Fibrillation Better Care (ABC) pathway resulted in a 58% reduction in all-cause death risk, 63% reduction in cardiovascular disease risk, and 45% reduction in ischemic stroke risk. Investigating the adherence to ABC pathway management and identifying gaps between the real world and established guidelines can lead to better integrated management. The review by Romiti et al6 showed that only 21% AF patients adhered to ABC pathway management. And there was great heterogeneity among different regions and subjects.
The level of adherence to ABC pathway management in elderly AF patients may be very low. Elderly AF patients are frailer, have more comorbidities, and take more drugs.7 In China, 73.2% of elderly patients with atrial fibrillation have two or more comorbidities.8 Multimorbidity make the integral management of AF in elderly patients more difficult.8 In addition, social support for the elderly is relatively insufficient due to retirement and widowed.9,10 Therefore, more attention should be paid to the adherence to ABC pathway management in elderly AF patients.
To date, only two cohort studies in China have investigated the adherence to ABC pathway management in AF patients.8,11 Wang et al11 conducted the Chinese Atrial Fibrillation registry (CAFR) study which enrolled AF patients >18 years of age, and the adherence in elderly AF patients was unclear. Kotalczyk et al8 conducted the Optimal Thromboprophylaxis in Elderly Chinese Patients With Atrial Fibrillation (ChiOTEAF) study in AF patients aged ≥65 years. However, of the 42 sites in the study, 40 were tertiary-level hospitals and 2 were secondary-level hospitals.12 And 71.7% of the subjects were follow-up patients after hospitalization.12
There are likely more AF patients in the community who are not being managed. A study showed that while 60% of hospitalized AF patients were treated with anticoagulant therapy, only 25% continued treatment after discharge.13 In addition, 50–87% of AF patients are asymptomatic and patients often wait to seek medical attention until they have obvious symptoms.1,14
To our knowledge, there are no related studies on elderly community patients with AF in China. The adherence to ABC pathway management of elderly community patients with AF in China remains unclear. The current study aimed to investigate the adherence to ABC pathway management among elderly community patients with AF in China, so as to better integrate AF management into community settings and improve health outcomes and quality of life for these patients.
Methods
Design and Study Population
This is a cross-sectional study. Health examination data from 2020 was collected from the National Basic Public Health Service Program database for all residents of Yuexiu, Guangzhou, Guangdong Province who were >65 years of age. Cluster sampling was used by the program and all community hospitals in Yuexiu District were included in the study. Community hospitals send notices about health exam programs to residents in their districts who are >65 years of age based on the National Medical registration system. Those who are unable to reach a community hospital can make appointments with a primary care physician for an in-home health exam. From 54,845 residents aged >65 years, a total of 709 AF patients met the inclusion criteria of (1) a 12-lead, digital electrocardiogram (ECG) reporting an AF pattern or (2) a report of AF on previous ECG or medical records. It included 197 patients with a previous diagnosis and 512 with first diagnosis in from a current physical examination. Given that first-diagnosed patients may not have started treatment, the 197 previously-diagnosed patients were considered for the adherence analysis (Figure 1). The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of Guangdong Provincial People’s Hospital, China (Approval number: KY-Z-2020-632-02).
 |
Figure 1 Flow chart of AF patients’ selection. |
Data Collection and Measurement
- Demographic information completed by AF patients, including age, sex, educational level, marital status, and medical insurance;
- Disease information obtained by the physician based on medical history and health records, including history of cardiovascular and other comorbidities, CHA2DS2-VASc score, HAS-BLED score, AF-related symptoms, medications, and surgery records. CHA2DS2-VASc [congestive heart failure, hypertension, aged ≥75 years (doubled), diabetes mellitus, history of stroke (doubled), vascular disease, aged 65–74 years, and sex (female)] score was calculated to estimate the stroke risk for AF patients.1 HAS-BLED [hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly (aged >65 years), drugs/alcohol concomitantly] was calculated to predict the bleeding risk of AF patients on anticoagulants.1 AF-related symptoms included dizziness, fatigue, chest pain, chest tightness, palpitations, and dyspnoea. Multimorbidity was defined as the presence of two or more diseases (in addition to AF) including hypertension, diabetes, dyslipidaemia, HF, CAD, stroke/TIA, and PAD.15 Polypharmacy was defined as the use of ≥5 drugs.16
- Physical exams were completed by the physician. Hypertension was defined as a systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg and/or a previous diagnosis of hypertension with the use of antihypertensive medication.17 Body mass index (BMI) was expressed as weight (kg) / height2 (m).18 Diabetes was defined as fasting blood glucose (FBG) ≥7.0 mmol/L and/or a previous diagnosis of diabetes with use of insulin or hypoglycaemic agents.18 Dyslipidemia was defined as total cholesterol (TC) ≥6.2 mmol/L, triglycerides (TG) ≥2.3 mmol/L, low-density lipoprotein cholesterol (LDL-C) ≥4.1 mmol/L, and high-density lipoprotein cholesterol (HDL-C) <1.0 mmol/L and/or a previous diagnosis of dyslipidemia with use of lipid-lowering drugs.18 AF was diagnosed by Standard 12-lead digital ECG.
Assessment of Adherence to the ABC Pathway
Based on the 2020 ESC guidelines, adherence to the ABC pathway management was defined as follows:1
“A-adherent”—Patients were considered to meet this criterion if they received appropriate anticoagulants based on the CHA2DS2-VASc score. Male patients with CHA2DS2-VASc≥2 and female patients with CHA2DS2-VASc≥3 who received oral anticoagulants (OAC), including warfarin with a time in therapeutic range (TTR >70%) or non-vitamin K antagonist oral anticoagulant (NOAC); male patients with CHA2DS2-VASc=1 and female patients with CHA2DS2-VASc=2 who received or did not receive OAC; and male patients with CHA2DS2-VASc=0 and female patients with CHA2DS2-VASc=0 or 1 who did not receive OAC were considered to meet this criterion.
“B-adherent”—Patients self-reported no AF-related symptoms.
“C-adherent”—Cardiovascular disease and comorbidities associated with AF were treated with specific medications or met the treatment criteria. (1) For hypertension, blood pressure ≤140/90 mmHg was considered well controlled.17 (2) For HF, angiotensin-converting enzyme inhibitors (ACEI)/angiotensin receptor blockers (ARB) and β-blockers were used.18 (3) For CAD, ACEI/ARB, β-blockers, and lipid-lowering drugs (LLD) were used.18 (4) PAD treated with LLD.18 (5) Stroke/TIA treated with LLD. (6) Dyslipidaemia treated with LLD.18 (7) For diabetes, insulin or oral hypoglycaemic drugs were used.18 (8) BMI<28.0 kg/m2.18 When all of these diseases were well controlled or properly medicated, it was defined as adherence to C pathway management.
“ABC-adherent”—If all three components met the criteria, the patient was identified as adherent to the ABC pathway management.
Statistical Analysis
All data were analyzed using IBM SPSS Statistics version 25.0 (SPSS Inc., Chicago, IL, USA). Basic characteristics and the adherence to ABC pathway management were evaluated by descriptive statistics. A Chi-square test was used to compare differences in adherence to ABC pathway management using different demographic and clinical data. All statistical tests were two-sided. Variables with statistical significance in the chi-square test were included in the multivariate logistic regression model to determine the independent factors associated with the non-adherence to the ABC pathway after adjusting for sex. P <0.05 was considered statistically significant.
Results
Basic Characteristics of the Study Participants
Sociodemographic and clinical information is shown in Table 1. Among the 197 patients with AF, 52.3% were male, 59.4% were ≥75 years of age, 64.5% had a senior middle school education or above. The most common comorbidities were hypertension (72.1%), CAD (28.9%), dyslipidaemia (28.4%) and diabetes (24.9%). Stroke or TIA occurred in 13.7% of AF patients. Based on the CHA2DS2-VASc and HAS-BLED Scores, 88.3% (174/197) participants were strongly recommended to take oral anticoagulants, and 12.2% (17/197) had a high risk of bleeding. For comorbidities and treatment, 84.8% (167/197) AF patients had ≥2 cardiovascular, and 6.1% (12/197) AF patients took ≥5 medications.
 |
Table 1 Sociodemographic and Clinical Characteristics of the AF Patients |
Adherence to the ABC Pathway Management and Its Components in Patients with AF
Table 2 shows the ABC pathway management data of AF patients. Regarding the ABC pathway, very few patients (9.1%) met all the criteria. Regarding “A”, avoid stroke or anticoagulation, only 21.8% (43/197) AF patients were in the A-adherent group. Among them, 11.2% (22/197) received OAC, including 4.1% (8/197) who received warfarin and 7.1% (14/197) who received NOAC (Table 1). Regarding “B”, better symptom control, 82.7% (163/197) AF patients were in the B-adherent group. Among them, 32.0% (76/197) received medications for arrhythmia or heart rate control, 23.4% (46/197) received radiofrequency catheter ablation (RFCA). Regarding “C”, cardiovascular and other comorbidity management, 31.5% (62/197) patients were in the C-adherent group. For the C component, the level of adherence to hypertension (65.6%), diabetes (77.6%), and BMI (88.5%) was relatively higher, and the level of adherence to HF (22.2%), CAD (1.8%), stroke/TIA (22.2%), and dyslipidaemia (38.9%) was lower.
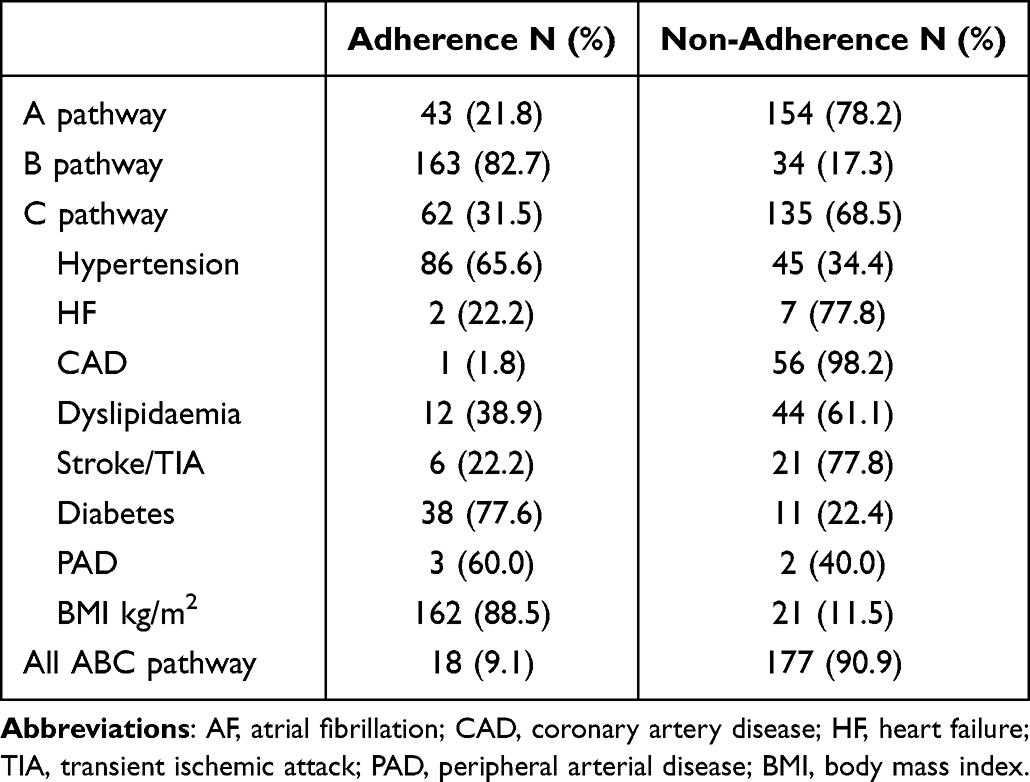 |
Table 2 Adherence to ABC Pathway Management and Its Components Among AF Patients |
Differences in the Adherence to ABC Pathway Management by Demographic and Clinical Characteristics
Table 3 shows that AF patients who adhered to the ABC pathway management were more likely to be 65–74 years of age (P<0.001), without multimorbidity (P<0.001), and CHA2DS2-VASc Score≤1 (male)/≤2 (female) (P<0.001). AF patients in the A-adherent group were more likely to be 65–74 years of age (P<0.001), disease course<1 year (P=0.028), without multimorbidity (P<0.001), and CHA2DS2-VASc score≤1 (male)/≤2 (female) (P<0.001). AF patients in the B-adherent group were more likely to have a disease course ≥1 year (P=0.002). AF patients in the C-adherent group were more likely to be without multimorbidity (P<0.001), and CHA2DS2-VASc score≤1 (male)/≤2 (female) (P<0.001).
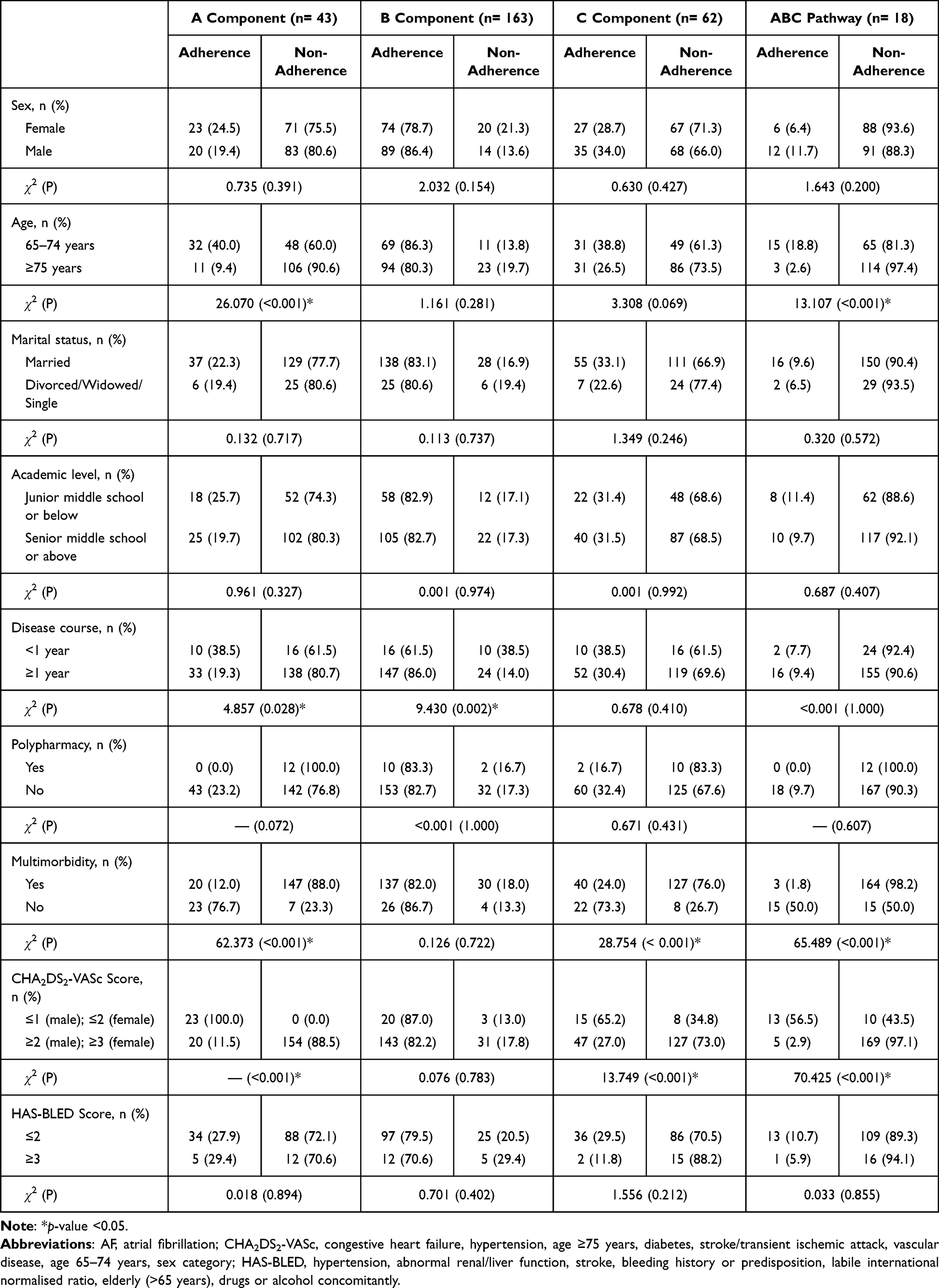 |
Table 3 Adherence to ABC Pathway Management According to the Sociodemographic and Clinical Characteristics of AF Patients |
Factors Independently Associated with the Non-Adherence to the ABC Pathway Management
Multivariate logistic regression analyses showed that sex-adjusted factors independently associated with the non-adherence to the ABC pathway management included aged ≥75 years (compared with aged 65–74 years, OR=4.665, 95% CI: 1.072–20.291, P=0.040), and multimorbidity (OR=45.891, 95% CI: 11.112–189.528, P<0.001). The factor independently associated with non-adherence to the “A” component management was aged ≥75 years (compared with aged 65–74 years, OR=5.776, 95% CI: 2.331–14.310, P<0.001) and multimorbidity (OR=21.179, 95% CI: 7.433–0.348, P<0.001). The factor independently associated with non-adherence to the “B” component management was disease course <1 year (compared with disease course ≥1 year, OR=0.253, 95% CI: 0.102–0.629, P=0.003). The factor independently associated with non-adherence to the “C” component management was multimorbidity (OR=8.780, 95% CI: 3.620–21.297, P<0.001) (Table 4).
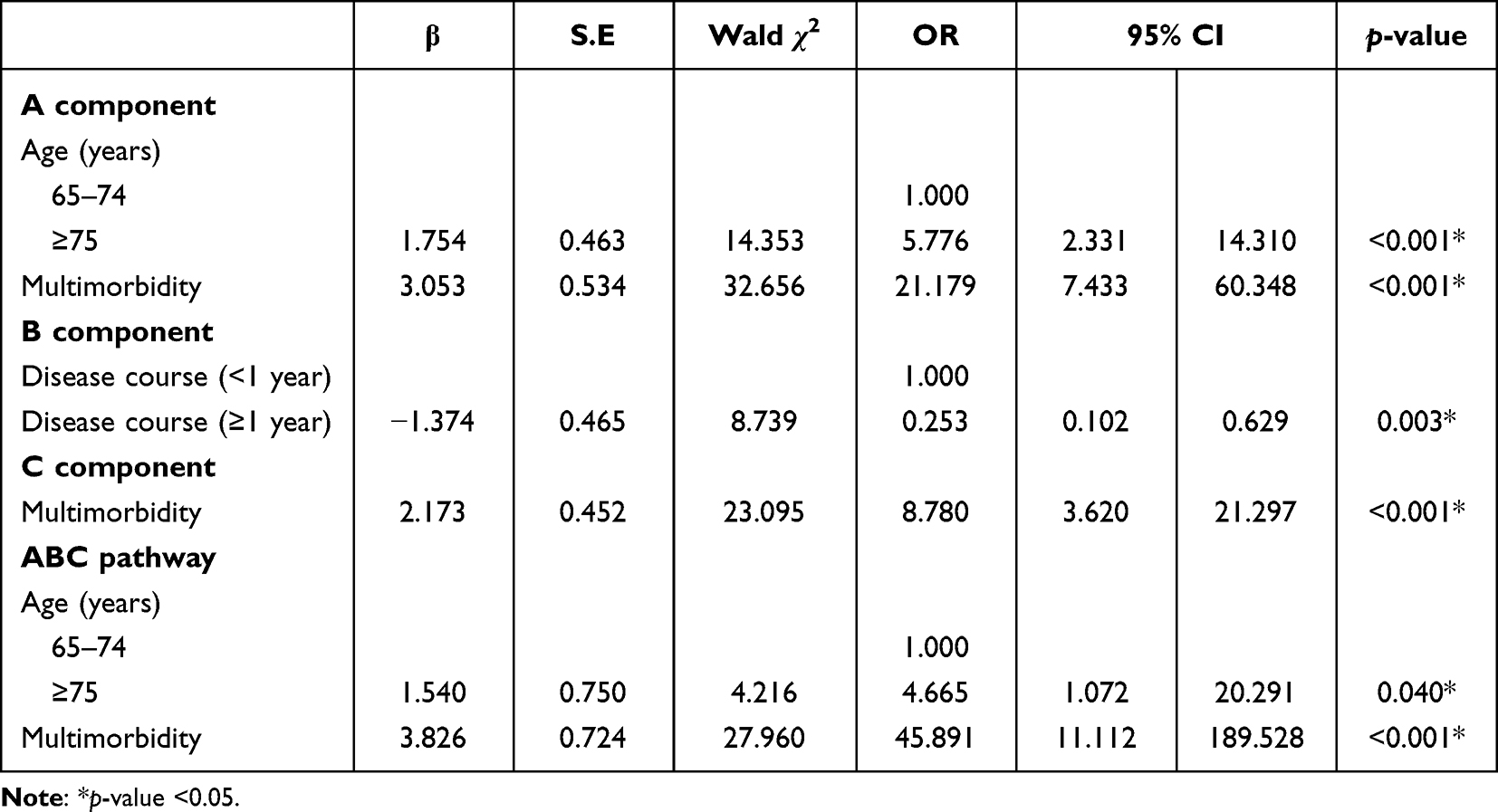 |
Table 4 Sex-Adjusted Factors Independently Associated with Non-Adherence to the ABC Pathway Management Among AF Patients |
Discussion
There were three main findings: (1) The level of adherence to ABC pathway management among the elderly community patients with AF was low (9.1%); (2) There were very few AF patients in the A-adherent group (21.8%), followed by the C-adherent group (31.5%), but relatively more in the B-adherent group (84.8%); (3) Aged ≥75 years and multimorbidity independently associated with non-adherence to the ABC pathway management and non-adherence to the “A” component management. Disease course ≥1 year independently associated with adherence to the “B” component management. Multimorbidity independently associated with non-adherence to the “C” component management.
Adherence to the ABC pathway management was extremely low among elderly community patients with AF, with only 9.1% of patients meeting the criteria, which was much lower than in other studies.6 The ChiOTEAF study by Kotalczyk et al8 in China found that 43.3% and 51.7% of elderly patients with AF in polypharmacy or multimorbidity group adhered to ABC pathway management. It can be seen that the adherence to ABC pathway management in community patients with AF was much worse than in inpatients with AF.8
On the one hand, it may be because community AF patients receive less health education and have less knowledge of disease management than inpatients.19 In this study, 84.8% of participants had two or more comorbidities, and 15.7% were divorced, widowed, or single. Frailty, comorbidity, and insufficient social support make self-management of elderly AF patients more difficult.7,9,10 On the other hand, it may be because primary physicians have insufficient knowledge of AF management.20 In addition, as of the time of data collection in this study, AF was not included in the resident basic health service assessment program and NOAC was not included in the health insurance reimbursement program. The combination of these factors hinders the management of AF in the community.
Regarding “A”, avoid stroke or anticoagulation, this study found that the only 21.8% participants were in the A-adherent group. Proietti et al’s and Pastori et al’s21,22 study of AF patients >65 years of age in Europe and North America showed that 61.8% and 46.3% patients were in the A-adherent group, respectively. There was still a gap in anticoagulant management of elderly AF patients between China and Europe and North American countries. In this study, 88.3% (167/197) participants were strongly recommended OACs according to the guidelines.1 However, only 11.2% of the patients were taking OACs. According to a study by Wei et al,23 only 3.8% of AF patients refused anticoagulant therapy after they were fully informed about the risk of stroke. This is likely because most (82.7%) AF patients in the current study were asymptomatic and did not seek medical attention.
In this study, few community AF patients used NOAC. The 2020 ESC guidelines indicate that NOAC has comparable safety and efficacy to warfarin, is easy to use, and has strong patient adherence.1 Although the use of NOAC has reached 75.8% in Europe,24 only 7.1% (14/197) of AF patients in this study received this treatment. It may be that by the time of this study, NOAC had not yet been included in the national medical insurance. And the average cost of NOAC was about $160 to $191 per month at the time of this study,25 which is nearly half of an individual’s average monthly disposable income. To solve this issue, NOAC were included in China’s National Medical Insurance Program in 2022, with prices similar to warfarin. In the future, it will be more convenient for community AF patients to use anticoagulant drugs.
Regarding “B”, better symptom control, it was satisfactory in this study. Most AF patients had no AF-related symptoms (82.7%). The findings were consistent with Yang et al’s26 study in 262,987 Asian AF patients (82.6%). About symptom management strategies, rate/rhythm control medications were used in 38.6% AF patients, and only 23.4% patients received RFCA. This is likely because the majority (50%–87%) of AF patients are asymptomatic and because a single radiofrequency ablation has a high recurrence rate of AF.27 Thus, radiofrequency ablation was not a priority for most AF patients in this study.
Regarding “C”, cardiovascular and other comorbidity management, only 31.5% AF patients were in the C-adherent group, which was quite different from the results of Proietti et al28 in their global multi-centre study of AF patients aged >65 years. This may be mainly because their study considered fewer comorbidities, and they did not include diabetes, dyslipidaemia, or BMI in the evaluation criteria of C-adherent.28 A study investigating clinically complex patients with AF demonstrated that AF patients with multimorbidity have worse management adherence.29
Hypertension and diabetes are better managed in community patients with AF compared with other comorbidities. It may be because hypertension and diabetes were the most common chronic diseases and were included in the evaluation of chronic disease management efforts by primary care physicians. Dyslipidaemia often neglected by AF patients. Only 38.9% of AF patients in this study met the management criteria. A survey in northern China also found that few (14.7%) of people knew they had dyslipidaemia, and very few of them received treatment.30 Higher TG and HDL-C levels were associated with ischemic stroke in AF patients.31 Closer attention should be paid to dyslipidaemia during the management of chronic diseases in primary hospitals. Management of HF and CAD was extremely poor, with only 22.2% and 1.8% of AF patients meeting the management criteria, respectively. Kotalczyk et al8 study of elderly Chinese patients with AF also found that HF and CAD were the main factors for non-adherence to comorbidity management. In this study, 22.2% of AF patients met the criteria for stroke/TIA management. It can be seen that AF patients have poor cognition of stroke prevention, which is also the main reason why few participants were in the A-adherent group in this study.
About factors independently associated with adherence to the ABC pathway. This is likely because, elderly AF patients have more comorbidities, which makes the management of “C” component more difficult and thus, their adherence to ABC pathway management is worse. Similarly, the more comorbidities they have, the higher the CHA2DS2-VASc score, and more patients must then receive OAC. This also resulted in few AF patients in the A-adherent group in this study. As the disease course progresses, patients may become more aware of AF and initiate symptom management strategies. Therefore, patients with disease duration ≥1 year had relatively better symptom management. Gumprecht et al32 also found consistent results in their investigation of AF patients in the Middle East. In the future, elderly community patients with AF should be the targeted population for integrated management of AF, with a focus on anticoagulation therapy and comorbidities management.
Limitations
First, all participants were community residents in this study. Thus, this study can only represent AF patients in Chinese communities, not all AF patients. Second, only 197 previously diagnosed AF patients were included in the cross-sectional survey. In the future, prospective studies with larger samples are needed to further explore the influencing factors for adherence to ABC pathway management among elderly community patients with AF. Finally, The data of the study were from the National Basic Public Health Service Program database. These patients who participated in physical examination and cooperated with data collection may be relatively active in AF management. In fact, the level of adherence to ABC pathway management in community elderly patients with AF may be lower than in the study.
Conclusions
This study investigated the adherence to ABC pathway management among elderly community patients with AF in China. Many gaps were found between the ABC pathway management of AF and the 2020 ESC guidelines. Additional studies should explore effective methods to improve ABC pathway management among elderly community patients with AF.
Data Sharing Statement
The data underlying this article will be shared on reasonable request to the corresponding author.
Acknowledgments
Thanks to the support of all the primary physician and patients in this study.
Funding
This work was supported by the Medical Scientific Research Foundation of Guangdong Province of China [grant number: A2021129, C2021003].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–498. doi:10.1093/eurheartj/ehaa612
2. Wang Z, Chen Z, Wang X, et al. The disease burden of atrial fibrillation in China from a national cross-sectional survey. Am J Cardiol. 2018;122(5):793–798. doi:10.1016/j.amjcard.2018.05.015
3. Cheng X, Zhou X, Song S, et al. Ethnicity and anticoagulation management of hospitalized patients with atrial fibrillation in northwest China. Sci Rep. 2017;7:45884. doi:10.1038/srep45884
4. Guo Y, Tian Y, Wang H, Si Q, Wang Y, Lip GYH. Prevalence, incidence, and lifetime risk of atrial fibrillation in China: new insights into the global burden of atrial fibrillation. Chest. 2015;147(1):109–119. doi:10.1378/chest.14-0321
5. Alobaida M, Alrumayh A. Rate control strategies for atrial fibrillation. Ann Med. 2021;53(1):682–692. doi:10.1080/07853890.2021.1930137
6. Romiti GF, Pastori D, Rivera-Caravaca JM, et al. Adherence to the ‘atrial fibrillation better care’ pathway in patients with atrial fibrillation: impact on clinical outcomes-A systematic review and meta-analysis of 285,000 Patients. Thromb Haemost. 2022;1222(3):406–414. doi:10.1055/a-1515-9630
7. Salis F, Palimodde A, Demelasb G, Scionis MI, Mandas A. Frailty and comorbidity burden in Atrial Fibrillation. Front Public Health. 2023;11:1134453. doi:10.3389/fpubh.2023.1134453
8. Kotalczyk A, Guo Y, Stefil M, Wang Y, Lip GYH; ChiOTEAF Registry Investigators. Effects of the atrial fibrillation better care pathway on outcomes among clinically complex Chinese patients with atrial fibrillation with multimorbidity and polypharmacy: a report from the ChiOTEAF Registry. J Am Heart Assoc. 2022;11(7):e24319. doi:10.1161/JAHA.121.024319
9. Ye RF, Zhang ML, Deng WP, Ogrin R. Correlative analysis between received support, anticipated support and quality of life in retired elderly patients. Chin J Behav Med Sci. 2008;17:217–219.
10. Green MM, Lowthian JA, Allgood H, et al. Volunteer peer support frameworks supporting older women living alone. Health Soc Care Community. 2022;30(6):e4252–e4263. doi:10.1111/hsc.13818
11. Wang YF, Jiang C, He L, et al. Integrated care of atrial fibrillation using the ABC (Atrial fibrillation Better Care) pathway improves clinical outcomes in Chinese population: an analysis from the Chinese Atrial Fibrillation Registry. Front Cardiovasc Med. 2021;8:762245. doi:10.3389/fcvm.2021.762245
12. Guo Y, Lane DA, Wang L, et al. Mobile health technology to improve care for patients with atrial fibrillation. J Am Coll Cardiol. 2020;75(13):1523–1534. doi:10.1016/j.jacc.2020.01.052
13. Shen AY, Yao JF, Brar SS, Jorgensen MB, Wang X. Racial/Ethnic differences in ischemic stroke rates and the efficacy of warfarin among patients with atrial fibrillation. Stroke. 2008;39(10):2736–2743. doi:10.1161/STROKEAHA.107.508580
14. Freedman B, Camm J, Calkins H, et al. Screening for atrial fibrillation a report of the AF-SCREEN international collaboration. Circulation. 2017;135(19):1851–1867. doi:10.1161/CIRCULATIONAHA.116.026693
15. Diederichs C, Berger K, Bartels DB. The measurement of multiple chronic diseases--a systematic review on existing multimorbidity indices. J Gerontol a Biol Sci Med Sci. 2011;66(3):301–311. doi:10.1093/gerona/glq208
16. Viktil KK, Blix HS, Moger TA, Reikvam A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2007;63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
17. Guo QH, Zhang YQ, Wang JG. Asian management of hypertension: current status, home blood pressure, and specific concerns in China. J Clin Hypertens. 2020;22(3):475–478. doi:10.1111/jch.13687
18. Beijing Association for Hypertension Prevention and Control, Beijing Association for Diabetes Prevention and Control, Beijing Association for Chronic Disease Prevention and Health Education, Hypertension Alliance (China), National Clinical Research Center for Geriatric Diseases, China Alliance for the Prevention and Treatment of Cardiovascular Disease in the Elderly. Practice guidelines (2020) for integrated management of cardiovascular diseases in primary hospitals. Chin J Front Med. 2020;12:1–73.
19. Du X, Guo L, Xia S, et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart. 2021;107(7):535–541. doi:10.1136/heartjnl-2020-317915
20. Ye S, Wang T, Liu A, Yu Y, Pan Z, Gu J. A study of knowledge, attitudes, and practices of primary care physicians toward anticoagulant therapy in patients with non-valvular atrial fibrillation in Shanghai, China. BMC Fam Pract. 2020;21(1):165. doi:10.1186/s12875-020-01236-4
21. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Improved outcomes by integrated care of anticoagulated patients with atrial fibrillation using the Simple ABC (Atrial Fibrillation Better Care) pathway. Am J Med. 2018;131(11):1359–1366.e6. doi:10.1016/j.amjmed.2018.06.012
22. Pastori D, Menichelli D, Violi F, Pignatelli P, Lip GYH; ATHERO-AF study group. The Atrial fibrillation Better Care (ABC) pathway and cardiac complications in atrial fibrillation: a potential sex-based difference. The ATHERO-AF study. Eur J Intern Med. 2021;85:80–85. doi:10.1016/j.ejim.2020.12.011
23. Wei Y, Xu J, Wu H, et al. Survey of antithrombotic treatment in rural patients (>60 years) with atrial fibrillation in East China. Sci Rep. 2018;8(1):6830. doi:10.1038/s41598-018-24878-y
24. Kozieł M, Teutsch C, Bayer V, et al. Changes in anticoagulant prescription patterns over time for patients with atrial fibrillation around the world. J Arrhythm. 2021;37(4):990–1006. doi:10.1002/joa3.12588
25. Wei H, Cui C, Cui X, Liu Y, Li D. Cost-effectiveness analysis of dabigatran, rivaroxaban and warfarin in the prevention of stroke in patients with atrial fibrillation in China. BMC Health Serv Res. 2021;21(1):96. doi:10.1186/s12913-021-06084-1
26. Yang PS, Sung JH, Jang E, et al. Application of the simple atrial fibrillation better care pathway for integrated care management in frail patients with atrial fibrillation: a nationwide cohort study. J Arrhythm. 2020;36(4):668–677. doi:10.1002/joa3.12364
27. Latchamsetty R, Morady F. Atrial fibrillation ablation. Annu Rev Med. 2018;69:53–63. doi:10.1146/annurev-med-041316-090015
28. Proietti M, Vitolo M, Lip G. Integrated care and outcomes in patients with atrial fibrillation and comorbidities. Eur J Clin Invest. 2021;51(6):e13498. doi:10.1111/eci.13498
29. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Comprehensive management with the ABC (Atrial Fibrillation Better Care) pathway in clinically complex patients with atrial fibrillation: a post hoc ancillary analysis from the AFFIRM trial. J Am Heart Assoc. 2020;9(10):e014932. doi:10.1161/JAHA.119.014932
30. Xing L, Jing L, Tian Y, et al. Epidemiology of dyslipidemia and associated cardiovascular risk factors in northeast China: a cross-sectional study. Nutr Metab Cardiovasc Dis. 2020;30(12):2262–2270. doi:10.1016/j.numecd.2020.07.032
31. Li F, Du X, He L, et al. Relationship between serum lipid levels and ischemic stroke in patients with atrial fibrillation: a nested case-control study based on the China Atrial Fibrillation Registry. BMC Cardiovasc Disord. 2021;21(1):424. doi:10.1186/s12872-021-02237-6
32. Gumprecht J, Domek M, Proietti M, et al. Compliance of atrial fibrillation treatment with the Atrial Fibrillation Better Care (ABC) pathway improves the clinical outcomes in the middle east population: a report from the gulf Survey of Atrial Fibrillation Events (SAFE) Registry. J Clin Med. 2020;9(5):1286. doi:10.3390/jcm9051286
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.