Back to Journals » Infection and Drug Resistance » Volume 19
Establishment of a Risk Prediction Model for Metabolic Dysfunction-Associated Steatotic Liver Disease in People Living with HIV in China
Authors Lin Y, Kong D, Cao Y, Xie X, Jin Y ![]()
Received 16 December 2025
Accepted for publication 4 March 2026
Published 9 March 2026 Volume 2026:19 584601
DOI https://doi.org/10.2147/IDR.S584601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chi H. Lee
Yunting Lin,1,* Dongji Kong,2,* Yi Cao,1,* Xiaohong Xie,2 Yong Jin3,*
1Department of Hepatobiliary Surgery, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, People’s Republic of China; 2Department of Ultrasonic, Ningbo Hospital of Integrated Traditional Chinese and Western Medicine, Ningbo, Zhejiang, People’s Republic of China; 3Department of Infectious Diseases, Ningbo Hospital of Integrated Traditional Chinese and Western Medicine, Ningbo, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Jin, Department of Infectious Diseases, Ningbo Hospital of Integrated Traditional Chinese and Western Medicine, No. 998 Qianhe Road, Ningbo, Zhejiang, 315100, People’s Republic of China, Email [email protected]
Purpose: The development of metabolic dysfunction-associated steatotic liver disease (MASLD) in people living with HIV (PLWH) is more complex than in the general population. Despite this, PLWH are often excluded from large-scale MASLD studies. This study aims to develop and validate a nomogram for predicting the risk of MASLD in PLWH.
Patients and Methods: This retrospective cohort study included PLWH who attended the outpatient clinic at Ningbo Hospital of Integrated Traditional Chinese and Western Medicine. A total of 717 participants were randomly assigned at a ratio of 7:3. Least absolute shrinkage and selection operator (LASSO) regression was employed to identify significant predictors of MASLD. A multivariable Cox regression model was then utilized to develop a nomogram for predicting the risk of MASLD. The performance of the nomogram was assessed using the concordance index (C-index), receiver operating characteristic curve, calibration plots, and decision curve analysis (DCA). Competing risk analysis was conducted to further validate the identified predictors.
Results: The LASSO regression analysis identified eight independent predictors, including the antiretroviral therapy regimen, alanine aminotransferase, serum amylase, uric acid, triglycerides, high-density lipoprotein cholesterol, and CD4 and CD8 T lymphocyte counts. The Area Under the Curve (AUC) for 1-, 3-, and 5-year outcomes in the development cohort ranged from 0.793 to 0.830, while the validation cohort exhibited AUC ranging from 0.749 to 0.903. Calibration plots confirmed a robust agreement between the predicted and observed outcomes. The C-index and DCA indicated the superior prediction performance of the nomogram. This relationship remained statistically significant after using the competing risk analysis.
Conclusion: This study developed the first clinical nomogram specifically for PLWH based on the 2023 MASLD definition. The model is based on eight clinically accessible and objective variables, including HIV-specific parameters, and is intended for the early screening of MASLD within this population.
Keywords: metabolic dysfunction-associated steatotic liver disease, nomogram, prediction model, HIV, cohort study
Introduction
The advent of effective antiretroviral therapy (ART) has transformed human immunodeficiency virus (HIV) from a fatal disease into a manageable chronic condition. However, this transformation has been accompanied by an increasing prevalence of non-communicable diseases, including metabolic dysfunction-associated steatotic liver disease (MASLD), which is driven by metabolic risk factors such as obesity, insulin resistance, dyslipidemia, and chronic low-grade inflammation.1 The prevalence of MASLD among people living with HIV (PLWH) is 13.9%, as revealed in cohort study, and it is influenced by metabolic characteristics, age, disease duration, and ART regimen.2,3 In comparison, recent epidemiological data indicate that the prevalence of MASLD in the general Chinese population is approximately 16.9% (95% CI, 14.7%–18.9%).4 Differences in overall prevalence across populations may reflect heterogeneity in the underlying pathogenesis. Moreover, PLWH with MASLD have been reported to exhibit more advanced fibrosis and faster disease progression, underscoring the clinical importance of early identification in this population.5 In 2023, nonalcoholic fatty liver disease (NAFLD) was officially redefined as MASLD.6 Unlike NAFLD, MASLD is characterized by a robust association with metabolic dysfunction, offering a more comprehensive framework for evaluating liver disease in this population. The pathogenesis of MASLD begins with hepatic steatosis, where unmitigated tissue injury and repair cycles drive the progression to fibrosis, cirrhosis, and ultimately hepatocellular carcinoma.7 MASLD has emerged as the most prevalent hepatic disease among PLWH in the United States.8 However, clinical understanding of MASLD in PLWH remains limited, as individuals with HIV are frequently excluded from large-scale MASLD studies. This exclusion impedes efforts to clarify its natural history, identify unique risk factors, and establish optimal management strategies for this vulnerable population. Incretin-based therapies, particularly glucagon-like peptide-1 receptor agonists, have shown substantial therapeutic potential in the treatment of MASLD.9,10 Therefore, early detection and intervention are crucial. Identifying modifiable risk factors may help reverse the disease during its early stages.
The pathogenesis of MASLD in PLWH differs substantially from that in the general population. PLWH with MASLD typically demonstrates more advanced fibrosis.5 Latent HIV reservoirs persist even in individuals undergoing effective ART.11 HIV itself directly contributes to the progression of hepatic steatosis by disrupting adipogenesis and adipokine synthesis.12 Although ART is life-saving, it plays a pivotal role in the distinct mechanisms driving MASLD in PLWH. Certain antiretroviral drugs are associated with adverse metabolic effects, such as dyslipidemia, insulin resistance, and mitochondrial toxicity.13 The pathogenesis of MASLD in PLWH is shaped by a combination of shared and HIV-specific factors, which complicates the identification of MASLD risk factors within this population.
Nomograms have considerable advantages in identifying and predicting the risk of MASLD. While they have been extensively applied in risk prediction for non-HIV-infected individuals,14–16 their application in PLWH remains unexplored. Building on our previous study that established a predictive model for metabolic syndrome in PLWH,17 this study further integrates hepatic steatosis–related parameters with metabolic indicators to develop a more comprehensive and individualized nomogram for predicting the risk of MASLD. This comprehensive data integration enables a more personalized evaluation of MASLD risk in PLWH, accounting for the complex interplay of metabolic and HIV-related factors in this population. Additionally, nomograms convert statistical risk models into visual, user-friendly formats, allowing clinicians to easily estimate an individual’s risk, thereby facilitating early detection and intervention. By expanding our previous research and systematically incorporating hepatic and metabolic parameters, our study offers a novel and comprehensive framework for the prevention, risk stratification, and management of MASLD in PLWH.
Materials and Methods
Data Source and Study Population
This is a retrospective cohort study. PLWH who visited Ningbo Hospital of Integrated Traditional Chinese and Western Medicine at least twice between November 2018 and September 2024 were included in the study. As the designated healthcare facility for PLWH in the region, this hospital serves the majority of PLWH in the area. Inclusion criteria were: (1) a confirmed HIV diagnosis by the Centers for Disease Control; and (2) age over 18 years. Exclusion criteria were: (1) baseline MASLD; (2) other liver diseases, including autoimmune or viral hepatitis, alcohol- or drug-induced liver diseases, cholestatic diseases, and hereditary liver diseases; and (3) missing baseline records. (4) switching ART regimens during follow-up due to virological failure or other reasons. (5) Drinking history, which was defined as alcohol consumption not exceeding 140 grams per week for females and 210 grams per week for males. A total of 717 PLWH participated in the study. The participants were then randomly assigned to a development cohort and a validation cohort in a 7:3 ratio, with 502 participants in the development cohort and 215 in the validation cohort (Figure 1). The study was approved by the Institutional Review Board of Ningbo Hospital of Integrated Traditional Chinese and Western Medicine (Approval No.: 2023–050). The data were anonymized and handled in accordance with confidentiality requirements. The requirement for informed consent was waived due to the retrospective study design. This study was conducted in accordance with the Declaration of Helsinki.
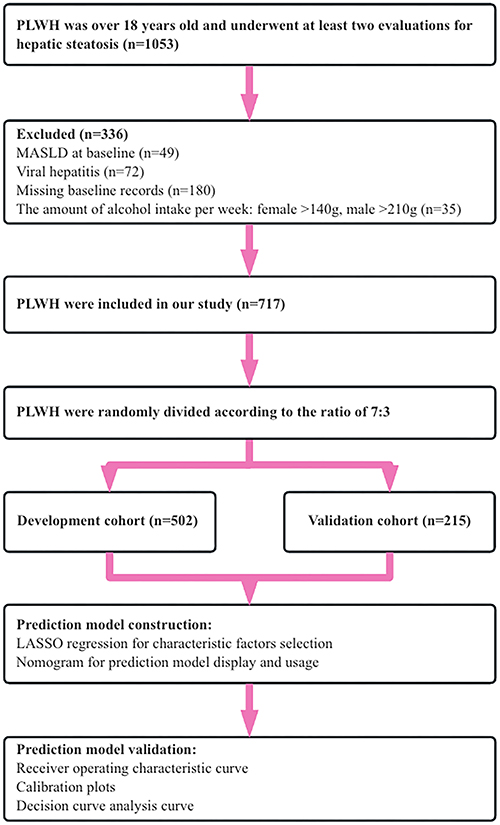 |
Figure 1 Flowchart of the study design. |
Clinical Variables
The potential influencing factors were selected based on their clinical relevance and the support provided by existing literature. These factors are readily accessible from medical records and laboratory test results. The first outpatient visit of PLWH was defined as the baseline follow-up. All patients underwent a comprehensive review of their medical history and a thorough physical examination. The initial factors included basic demographic information (age, sex, transmission category, ART regimen), a history of hypertension and diabetes, and laboratory test results, including fasting blood glucose (FBG), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum amylase, indirect bilirubin (IBIL), direct bilirubin (DBIL), uric acid (UA), creatinine (CREA), blood urea nitrogen (BUN), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), CD4 T lymphocyte count, CD8 T lymphocyte count, and HIV viral load. All subjects fasted for approximately 8 hours prior to laboratory testing.
Outcome
All PLWH were followed up approximately every three months. The primary outcome of this study was the incidence of MASLD. Hepatic steatosis was diagnosed using color Doppler ultrasound, based on markedly increased echogenicity of the liver compared to the kidney, elevated liver parenchymal brightness, or blurring of blood vessels.18 Liver ultrasonography was performed by trained sonographers. MASLD was diagnosed based on the presence of hepatic steatosis and at least one component of metabolic dysfunction, defined by the following criteria: 1) Body mass index (BMI) ≥24 kg/m2, or waist circumference ≥90 cm for males and ≥85 cm for females; 2) hypertension; 3) pre-diabetes or diabetes; 4) fasting serum TG level ≥1.7 mmol/L, or treatment with hypolipidemic drugs; 5) HDL-C ≤1 mmol/L for males and ≤1.3 mmol/L for females. We adopted the most recent version of the diagnostic criteria released by the Chinese Society of Hepatology to ensure its applicability for the Chinese population.19 In addition, all-cause death without prior MASLD was treated as a competing event.
Statistical Analysis
Statistical analyses were performed using R software (v4.4.2) and IBM SPSS Statistics (v29.0), with a significance level set at P < 0.05. Categorical data were expressed as frequencies and percentages, and were compared using the chi-square test or Fisher’s exact test, as appropriate. Continuous variables were expressed as medians with interquartile ranges (IQR) and compared using the Mann–Whitney U-test. Prior to variable selection for model development, Spearman’s rank correlation analysis was conducted to evaluate potential multicollinearity among candidate predictors. The analysis revealed a strong correlation between ALT and AST (r > 0.7); therefore, AST was excluded from the model. All other variables exhibited correlation coefficients < 0.7. Variance inflation factor (VIF) analysis further confirmed the absence of significant multicollinearity, as all VIF values were below 5.
Construction and Validation of Predictive Models
PLWH were randomly assigned to the development and validation cohorts in a 7:3 ratio. The development cohort was used to construct the risk prediction model, while the validation cohort was utilized for internal validation. The process was conducted as follows: (1) Screening of characteristic factors: Variable selection and complexity adjustment were performed using least absolute shrinkage and selection operator (LASSO) regression analysis, conducted with the “glmnet” package. The results of the LASSO regression analysis were employed to identify the characteristic factors with λ ≠ 0. To improve figure clarity and reduce label overlap, we generated the LASSO coefficient path plot using the “ggplot2” package, displaying only the selected key variables and presenting their labels in the legend. (2) Nomogram development: The nomogram was developed using the “rms” package. Each regression coefficient from the multivariate Cox regression analysis was proportionally mapped onto a scale ranging from 0 to 100, with the variable exhibiting the highest absolute β coefficient assigned a value of 100%. The individual scores for each independent variable were summed to calculate the total score, which was then converted into predicted probabilities. (3) Model training, validation, and testing: The “timeROC” package was used to plot Receiver Operating Characteristic (ROC) curves and calculate the Area Under the Curve (AUC) to assess the model’s accuracy and discriminative power for 1-, 3-, and 5-year predictions. The concordance index (C-index) and calibration methods from the “rms” package were applied to address potential overfitting. Additionally, a decision curve analysis (DCA) was performed using the “rmda” package to evaluate the clinical utility of the predictive model.
Competing Risk Sensitivity Analysis
To address the potential impact of competing events, we additionally performed a competing risk analysis using the “cmprsk” package. Given that death may preclude the occurrence of MASLD, all-cause death without prior MASLD was treated as a competing event. The cumulative incidence function (CIF) of MASLD was estimated using the Fine–Gray subdistribution hazards model. Subdistribution hazard ratios (HRs) with 95% confidence intervals (CI) were calculated to evaluate associations between candidate predictors and the cumulative incidence of MASLD in the presence of competing risk. The same set of variables selected for the multivariable Cox regression model was included in the competing risk analysis. Results from the Fine–Gray model were compared with those from the Cox proportional hazards model to assess the robustness of the identified risk factors.
Results
Comparison of Baseline Characteristics
Among the 717 participants, 502 (70%) were assigned to the development cohort, and 215 (30%) to the validation cohort. In the development and validation cohorts, 66 (13.1%) and 28 (13.0%) participants, respectively, were diagnosed with MASLD. The overall median follow-up time was 2.7 (1.4, 4.0) years, corresponding to a total of 1971 person-years of observation. In the development cohort, the median follow-up time was 2.7 (1.5, 4.0) years, with 1388 person-years accumulated, whereas the validation cohort had a median follow-up time of 2.7 (1.2, 3.9) years and contributed 583 person-years. During follow-up, 66 (13.1%) participants in the development cohort and 28 (13.0%) in the validation cohort were diagnosed with MASLD. As anticipated, no significant differences were observed between the two groups, indicating that the baseline characteristics were comparable (Table 1).
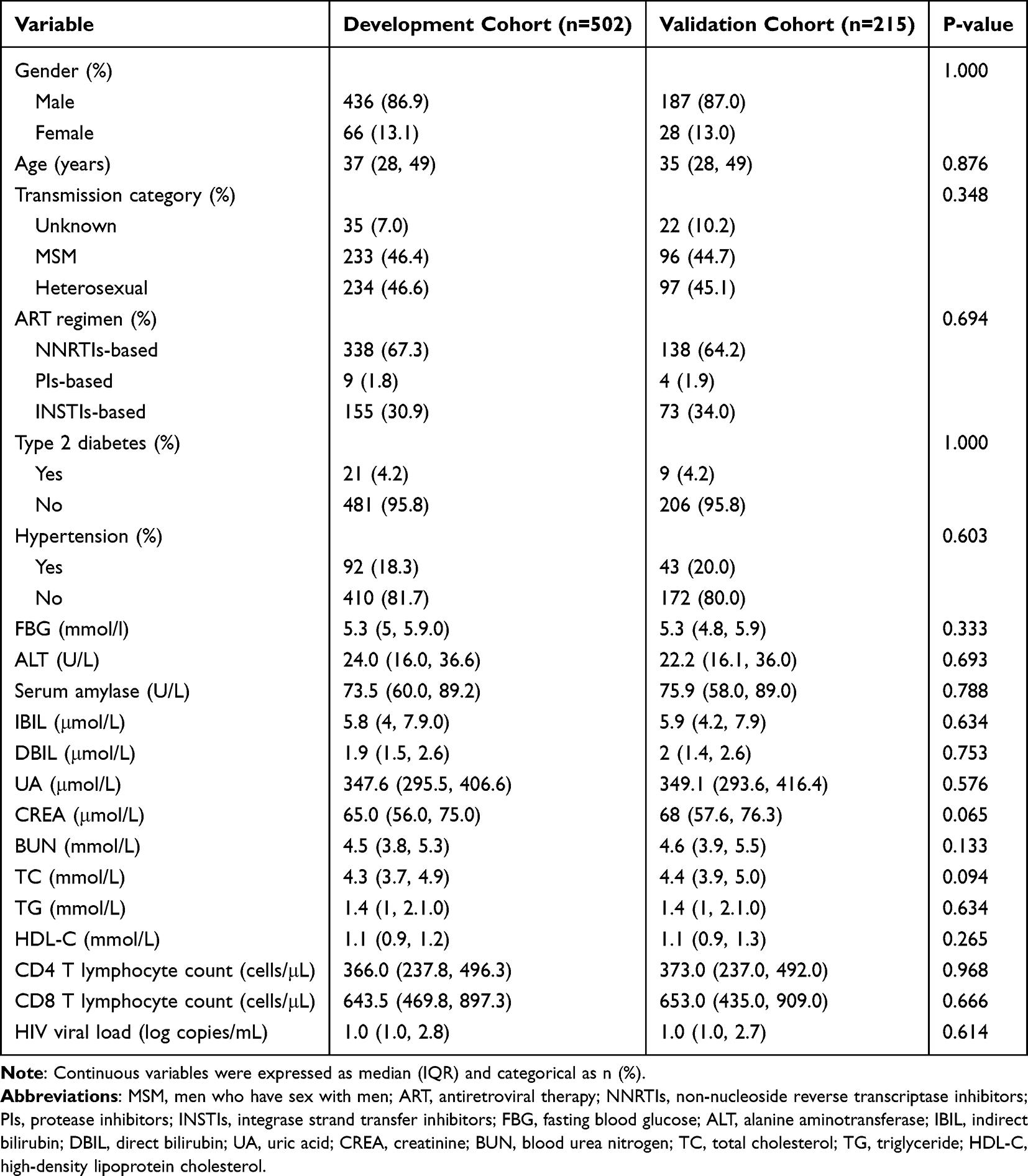 |
Table 1 Baseline Characteristics in Development and Validation Cohorts |
Screening of Characteristic Factors for MASLD Risk
LASSO regression analysis was conducted with the occurrence of MASLD as the dependent variable. Variables were selected using 5-fold cross-validation, and the results are illustrated in Figure 2. The initial set of 20 variables was narrowed down to 8 potential predictors based on the optimal penalty parameter (Lambda.min = 0.024). These predictors included ART regimen, ALT, serum amylase, UA, TG, HDL-C, CD4 and CD8 T lymphocyte counts. These 8 features were identified by nonzero coefficients in the LASSO logistic regression model.
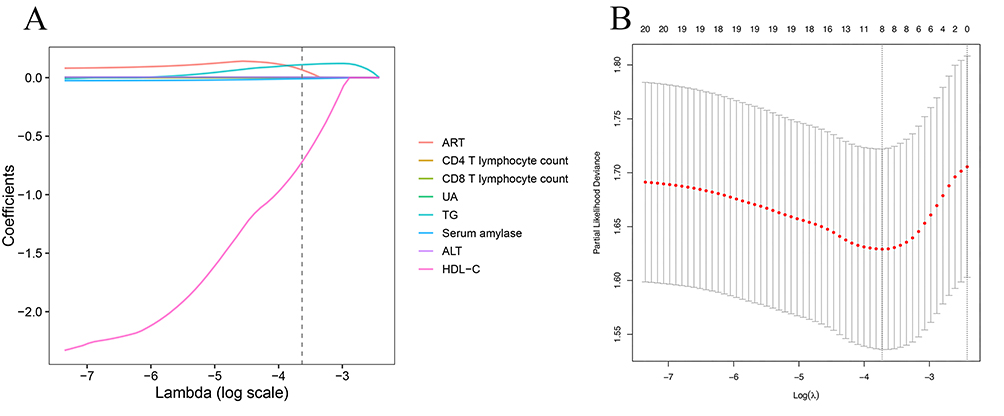 |
Figure 2 The LASSO regression analysis was conducted to identify key predictive factors. Notes: (A) Eight variables with non-zero coefficients were selected according to the optimal lambda value. (B) The 5-fold cross-validation curve is shown, with vertical dotted lines indicating the one standard error criterion (right) and the minimum lambda value (left). |
Construction of the Prediction Model
The aforementioned factors were incorporated into a multivariable Cox regression analysis to develop a nomogram for predicting the risk of MASLD in the development cohort. The resulting nomogram is presented in Figure 3. The risk score for each variable, derived from the score bar at the top, is aggregated to generate a total score. This total score is subsequently used to calculate the 1-, 3-, and 5-year overall MASLD probabilities. A higher total score correlates with a greater risk of developing MASLD in PLWH following ART. To facilitate clinical implementation, we developed an Excel-based risk calculator derived directly from the multivariable Cox proportional hazards model (Table S1).
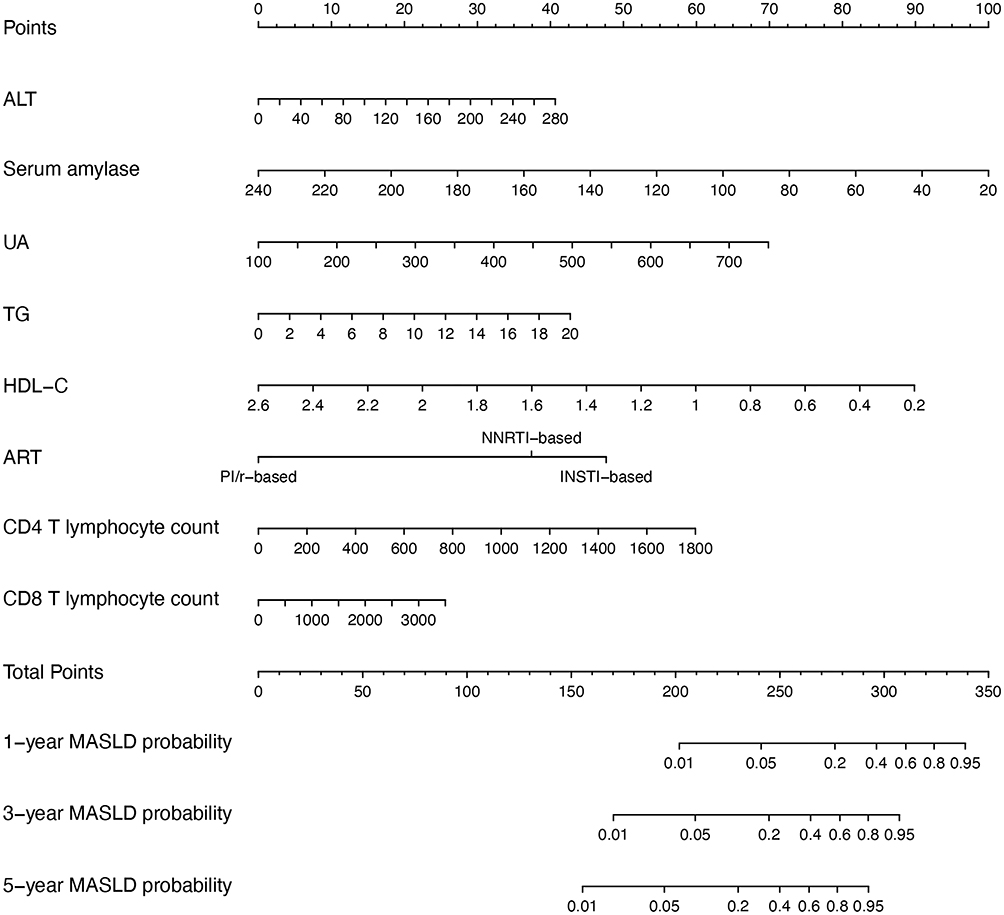 |
Figure 3 Nomogram for predicting the risk of MASLD. Notes: Risk scores are assigned based on the reference scale at the top, with higher scores to the right. Individual scores are summed to generate a total score, which is then located on the total score scale. The total score is translated into estimated 1-, 3-, and 5-year incidence rates. Example of nomogram application: A patient with ALT 19 U/L, serum amylase 105 U/L, UA 466.1 μmol/L, TG 2.96 mmol/L, HDL-C 1.16 mmol/L, receiving an INSTI-based regimen, a CD4 T lymphocyte count of 323 cells/μL, and a CD8 T lymphocyte count of 2085 cells/μL has an estimated 1-, 3-, and 5-year MASLD risk of approximately 3%, 11%, and 19%, respectively. |
Validation of the MASLD Nomogram
The C-index was 0.803 (95% CI: 0.765–0.856) for the development cohort and 0.803 (95% CI: 0.747–0.907) for the validation cohort. The discriminatory ability of the predictive model was assessed using a ROC curve (Figure 4). For the development cohort, the AUC of the nomogram at 1, 3, and 5 years was 0.830 (95% CI: 0.753–0.907), 0.793 (95% CI: 0.730–0.856), and 0. 808 (95% CI: 0.753–0.862), respectively (Figure 4A). For the validation cohort, the AUC at 1, 3, and 5 years was 0.903 (95% CI: 0.817–0.989), 0. 800 (95% CI: 0. 701–0.900), and 0.749 (95% CI: 0. 643–0. 0.853), respectively (Figure 4B). These results indicate that the model possesses strong discriminatory ability and consistent predictive performance across multiple time points. Notably, the close concordance between the C-index and AUC values in the development and validation cohorts suggests that the model demonstrates excellent internal validity and stable predictive performance within this cohort.
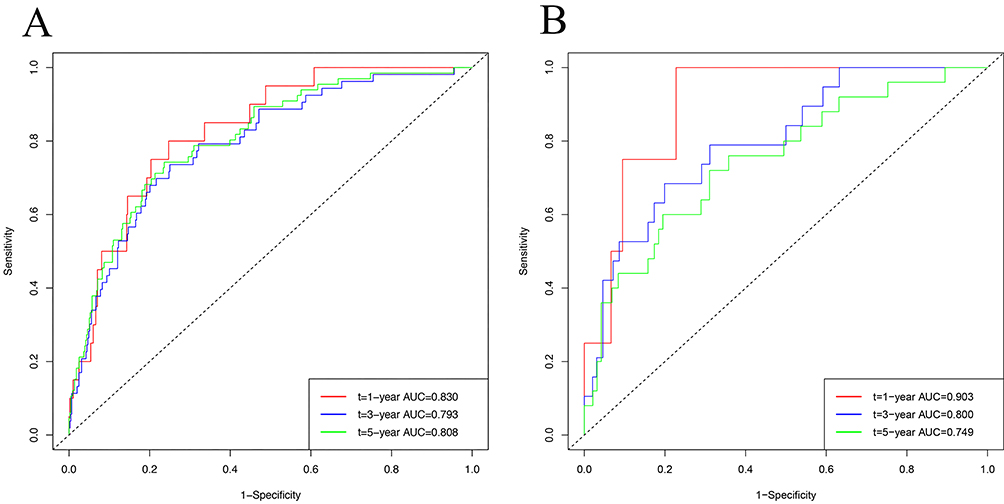 |
Figure 4 ROC curves for the MASLD risk nomogram at 1, 3, and 5 years. Notes: (A) Development cohort; (B) Validation cohort. The y-axis represents the true positive rate, and the x-axis indicates the false positive rate for the predictive model. |
Calibration of the MASLD Nomogram
Calibration plots revealed strong agreement between the predicted and observed MASLD risk for 1-, 3-, and 5-year outcomes in PLWH (Figure 5). The x-axis represents the predictions derived from the nomogram, while the y-axis represents the actual occurrence of MASLD. The 45-degree line serves as the reference for an ideal nomogram, demonstrating that the predicted outcomes closely align with the actual outcomes. Both models exhibited favorable calibration curves for risk estimation.
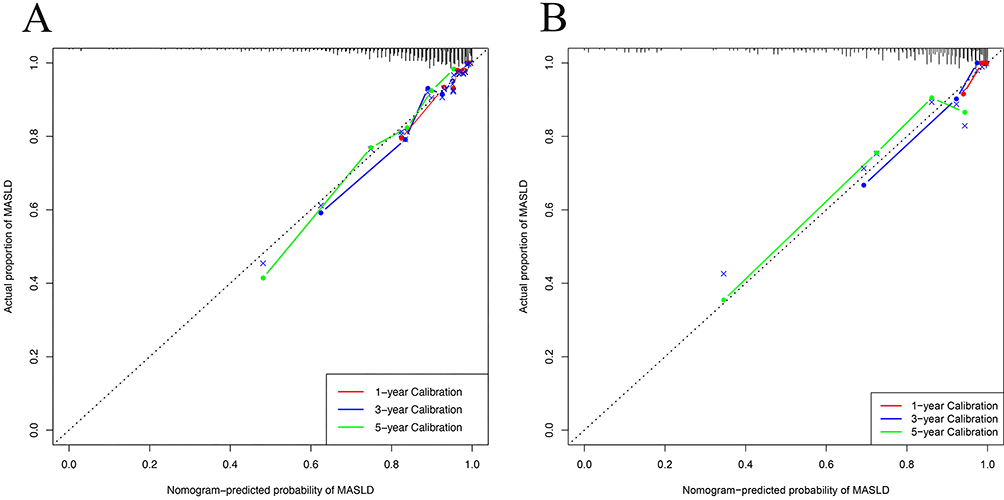 |
Figure 5 Calibration curves of the MASLD risk nomogram. Notes: (A) Development cohort; (B) Validation cohort. The y-axis indicates the observed incidence of MASLD, while the x-axis shows the predicted risk. The diagonal line represents the ideal model, and the solid line illustrates the performance of the validation cohort. |
Clinical Use of the MASLD Nomogram
DCA is an innovative method for evaluating diagnostic tests and prediction models, effectively integrating accurate measurements such as sensitivity and specificity with decision analysis techniques. This method assesses the net benefit of prediction models without altering their intended meaning. The relative threshold probability represents the point at which the anticipated benefits of treatment equal the expected benefits of withholding treatment.20 As shown in Figure 6A, the threshold probabilities in the development cohort ranged from 0% to 75% at the 1-, 3-, and 5-year follow-up periods. Within this range, the nomogram consistently yielded a greater net benefit than the “treat-all” and “treat-none” strategies, highlighting its superior clinical utility for decision-making. Higher threshold probabilities reflected the model’s ability to accurately identify individuals at increased risk of MASLD while reducing unnecessary interventions in low-risk populations. In the validation cohort (Figure 6B), the nomogram similarly demonstrated a favorable net benefit across clinically relevant threshold probabilities (0–36% for 1-year prediction, 0–43% for 3-year prediction, and 0–45% for 5-year prediction). These findings suggest that the model’s clinical utility was maintained in the validation cohort, supporting its robustness and potential generalizability.
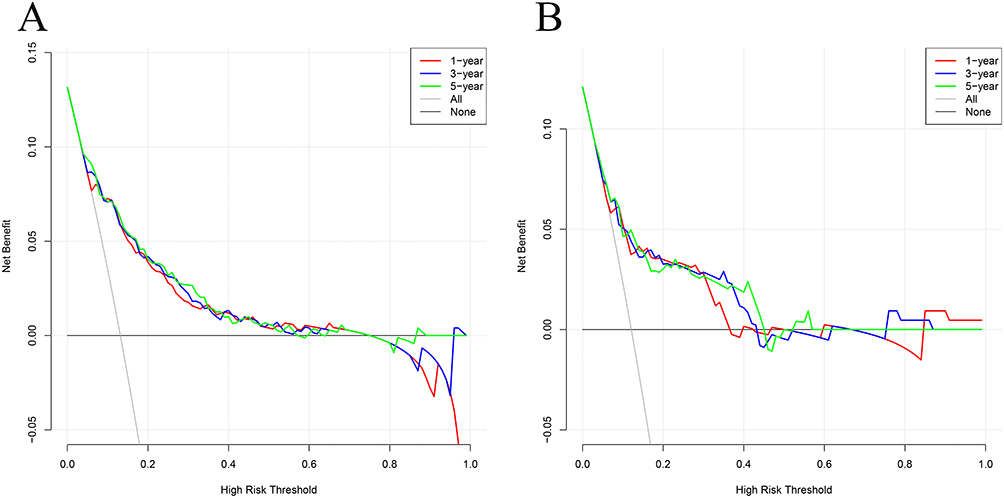 |
Figure 6 DCA for the MASLD risk nomogram. Notes: The x-axis shows the threshold probability, and the y-axis indicates the net benefit. The DCA demonstrates the clinical utility of the nomogram across a range of threshold probabilities in the development cohort (A) and validation cohort (B). |
Competing Risk Sensitivity Analysis
During follow-up, 7 participants (0.97%) died before developing MASLD and were treated as competing events. The CIF of MASLD was further evaluated using a Fine–Gray competing risk model (Figure 7). All deaths occurred in individuals without MASLD, resulting in a low cumulative incidence of death throughout follow-up. Consequently, the competing risk of death had minimal impact on the estimated risk of MASLD.
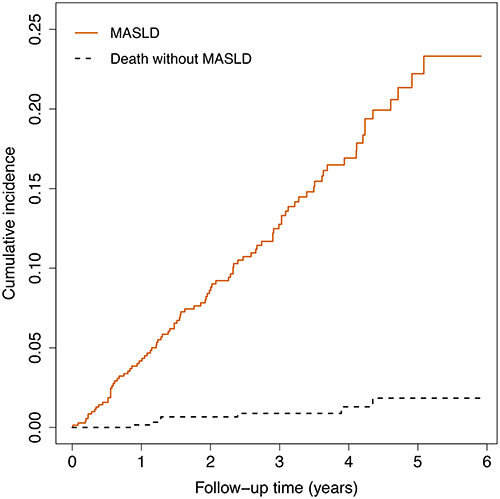 |
Figure 7 The CIF for the MASLD. Notes: The solid line denotes MASLD, and the dashed black line denotes death without MASLD. |
In the competing risk analysis, associations between the selected predictors and MASLD risk remained largely consistent with those observed in the primary multivariable Cox regression model (Figure 8). ALT, serum amylase, UA, HDL-C, ART regimen, and CD4 T lymphocyte count remained statistically significant, whereas TG and CD8 T lymphocyte count did not. Overall, these findings indicate that accounting for death as a competing event did not materially alter the main results, supporting the robustness of the identified risk factors.
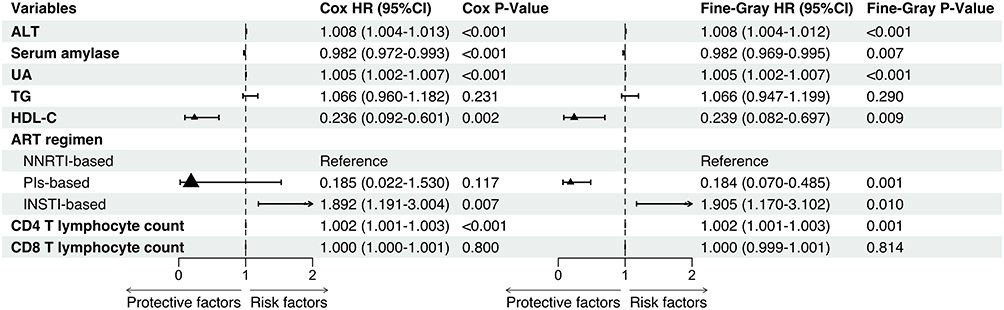 |
Figure 8 Forest plots from multivariable competing risk and Cox regression analyses of MASLD risk. |
Discussion
This study is a retrospective cohort investigation. The incidence of MASLD in PLWH is mediated by multifactorial etiologies. Predictive models for non-HIV populations generally rely on traditional metabolic indicators, such as blood lipids, blood pressure, and glucose levels; however, these parameters may not fully reflect the factors contributing to MASLD in PLWH. In addition to the conventional variables previously studied, we incorporated the transmission category, ART regimen, HIV viral load, CD4 T and CD8 T lymphocyte counts into LASSO regression analysis, ultimately developing a MASLD prediction model specifically tailored for PLWH. The final model included the ART regimen, ALT, serum amylase, UA, TG, HDL-C, and CD4 and CD8 T lymphocyte counts. In addition, this relationship remained statistically significant after using the competing risk analysis. By incorporating HIV-specific parameters, our predictive model provides a more personalized and accurate risk assessment, thereby enhancing the early identification of high-risk individuals.
Several traditional predictors, such as ALT, UA, TG, and HDL-C, have been extensively discussed in relation to hepatic steatosis. Elevated ALT,15,21,22 a marker of hepatocellular injury, is commonly observed in MASLD and reflects liver damage caused by fat accumulation and inflammation, often serving as an early indicator of progression to non-alcoholic steatohepatitis.23 UA has emerged as a potential contributor to MASLD, given its role in oxidative stress, inflammation, and apoptosis pathways,24 which exacerbate hepatic metabolic dysfunction.15,16,22 Dyslipidemia, characterized by elevated levels of TG, or reduced levels of HDL-C, is a hallmark feature of MASLD.14–16,21,22 Dyslipidemia reflects abnormal cholesterol transport, leading to lipid accumulation within liver cells. Collectively, these predictors provide critical insights into the metabolic and hepatic abnormalities underlying MASLD, underscoring their significance in risk stratification and early diagnosis, as highlighted in prior studies. In contrast, serum amylase has received less attention as a predictor in the context of MASLD, though emerging evidence underscores its potential significance. Previous research has shown that low serum amylase levels are associated with conditions such as metabolic syndrome,25 obesity,26 and diabetes mellitus,27 which are all key risk factors for MASLD. Notably, in non-HIV-infected individuals, serum amylase levels in NAFLD patients were significantly lower than those in healthy controls.28 The underlying mechanisms of this association may involve interactions between the endocrine and exocrine functions of the pancreas, wherein diminished insulinotropic effects and increased glucagon activity suppress pancreatic enzyme secretion.29,30
In this study, baseline CD4 and CD8 T lymphocyte counts—two HIV-specific immunological parameters—were identified as independent predictors of MASLD in PLWH. This finding is consistent with previous studies reporting that elevated CD4 and CD8 T lymphocyte counts are associated with hepatic steatosis and metabolic abnormalities in this population.2,31,32 CD4 and CD8 T cells play critical immunomodulatory roles by regulating the differentiation of Th1, Th2, and Th17 cells and secreting a variety of cytokines.33–35 Elevated baseline levels of these lymphocyte subsets may reflect persistent immune activation caused by chronic HIV infection, which could promote hepatic lipid accumulation through cytokine-mediated inflammation and dysregulated lipid metabolism.36 These findings suggest that baseline CD4 and CD8 T lymphocyte counts may serve as immunometabolic biomarkers reflecting the complex interplay between immune dysregulation and hepatic steatosis in PLWH. In our study, the INSTIs based regimen was also identified as an important predictor of MASLD. INSTIs have become a cornerstone of ART. INSTIs, such as dolutegravir and bictegravir, are associated with significant weight gain in PLWH.37,38 This weight gain is particularly concerning as it often manifests as visceral fat, a metabolically active tissue strongly associated with the development of MASLD.39 The impact of INSTIs on MASLD remains somewhat controversial. Two studies suggest that INSTIs increase the risk of MASLD,40,41 while three studies do not support these findings.42–44 The discrepancies among these studies may be attributed to several factors. Firstly, the region and ethnicity were different. Shengir et al43 conducted their study in North America, whereas the other studies were performed in various European countries. Secondly, the types of INSTIs are different. Shengir et al43 included only raltegravir, excluding other drugs such as dolutegravir, which limits the generalizability of their findings to all INSTI regimens. Thirdly, liver steatosis was defined differently. Navarro et al42 and Fernandes et al44 used the Hepatic Steatosis Index (HSI) to assess steatosis. Although HSI is a non-invasive tool based on serum markers and clinical parameters, it relies on indirect factors and cannot directly measure liver fat accumulation.45 The mechanisms by which INSTIs contribute to MASLD are multifactorial, involving mitochondrial dysfunction, oxidative stress, adipokine imbalance, and weight gain, all of which collectively disrupt hepatic and systemic metabolic homeostasis.46 Given the central role of ART in HIV management, careful selection of ART regimens is crucial, especially for individuals with underlying MASLD risk factors.
In the context of the growing burden of steatosis among PLWH, several studies have examined risk factors and diagnostic approaches for fatty liver disease in this population. Bischoff et al41 conducted a prospective study and identified BMI, tenofovir alafenamide, INSTIs, and type 2 diabetes mellitus as independent predictors of NAFLD in PLWH, with hepatic steatosis assessed using the controlled attenuation parameter (CAP). Although this work provided important prospective evidence linking ART exposure and metabolic factors to steatosis development, it was limited by a relatively small sample size and did not establish a multivariable longitudinal prediction model for individualized risk estimation. In addition, Xu et al47 evaluated ten general population–based diagnostic models, including the fatty liver index (FLI) and HSI, for predicting metabolic dysfunction–associated fatty liver disease (MAFLD) in PLWH. While these indices demonstrated moderate diagnostic accuracy overall, their performance was suboptimal in overweight PLWH, underscoring the limitations of applying general-population tools to this distinct clinical subgroup. Conversely, Hu et al48 investigated inflammatory and metabolic parameters in PLWH and reported that the lymphocyte-to–high-density lipoprotein ratio, which reflects both immune and metabolic characteristics, had superior predictive value compared with conventional indices. However, these studies primarily focused on individual predictors or diagnostic performance, rather than developing an integrated, individualized prediction tool tailored to PLWH. In comparison with previous investigations, our study has several distinctive strengths. First, to our knowledge, this is the first study to develop a nomogram for predicting MASLD risk specifically in PLWH. Nomograms provide a simple, visual tool for individualized risk estimation. Building on this, our model captures key immunometabolic mechanisms underlying MASLD in PLWH and enables clinicians to estimate individualized risk using readily available parameters by incorporating HIV-specific variables. Second, we used the updated MASLD definition rather than traditional NAFLD or MAFLD criteria, aligning our predictive framework with contemporary consensus that emphasizes the central role of metabolic dysfunction in steatotic liver disease. This alignment enhances the clinical relevance of our findings under current diagnostic standards. Third, hepatic steatosis was assessed by ultrasound, which is generally more reliable than indirect biochemical indices such as HSI. Although liver biopsy remains the diagnostic gold standard, its invasiveness and limited feasibility preclude routine use in large-scale cohort studies. Other noninvasive imaging modalities, including CAP49 and magnetic resonance imaging–proton density fat fraction (MRI-PDFF),50 have shown promise for MASLD assessment; however, limited availability and higher cost may constrain their routine use. Furthermore, although surrogate biochemical indices such as FLI, FIB-4, and BARD are widely used in epidemiological studies,51,52 their sensitivity and specificity may be lower than those of imaging-based approaches. Finally, the retrospective cohort design enabled longitudinal assessment of incident MASLD and temporal evaluation of baseline predictors in relation to subsequent outcomes, strengthening causal inference compared with cross-sectional analyses. Although the overall sample size was relatively large, the number of MASLD events was modest, resulting in a low events-per-parameter ratio of approximately 8 in the development cohort. This value is below commonly recommended thresholds for prediction modeling and may compromise coefficient stability and increase the risk of overfitting. To mitigate this concern, we used LASSO regression for variable selection and coefficient shrinkage and performed internal validation in an independent validation cohort. Nevertheless, the limited number of events may still compromise model stability despite these measures. Notably, the 1-year AUC was higher in the validation cohort (0.903) than in the development cohort (0.830). This apparent difference is likely attributable to the small number of outcome events in the validation cohort (n = 28), which can yield unstable estimates with wide confidence intervals. Taken together, these findings suggest that the observed predictive performance—particularly the short-term AUC in the validation cohort—should be interpreted cautiously.
Our study has several limitations. First, this single-center study conducted in China may limit generalizability to other geographic regions and ethnic populations; therefore, external validation in independent multicenter cohorts is warranted. Second, hepatic steatosis was diagnosed by ultrasound rather than liver biopsy or quantitative imaging modalities such as CAP or MRI-PDFF, which may limit diagnostic precision, particularly for mild steatosis. Third, although multiple metabolic and immunological variables were incorporated, residual confounding cannot be excluded. Unmeasured lifestyle factors, genetic susceptibility, and treatment modifications—including antiretroviral regimen switching during follow-up, which was excluded to isolate stable ART effects—may influence MASLD risk and were not fully captured. External validation in larger, independent, and multicenter cohorts is warranted to further confirm the robustness and generalizability of the proposed model, and more comprehensive assessments across diverse populations may help refine and extend its clinical applicability.
Conclusion
This study developed an effective clinical nomogram specifically for PLWH. The model is based on eight clinically accessible and objective variables, including HIV-specific parameters, and can be used for early screening of MASLD in PLWH. By leveraging routinely available baseline clinical and laboratory parameters, the nomogram enables early risk stratification at the baseline assessment. These efforts will facilitate the early detection and effective management of fatty liver disease, ultimately improving overall health outcomes for PLWH.
Data Sharing Statement
The data are not publicly available to protect the privacy of PLWH; however, they are available on reasonable request to the corresponding author.
Ethics Statement
The study was approved by the Institutional Review Board of Ningbo Hospital of Integrated Traditional Chinese and Western Medicine (Approval No.: 2023-050). The data were anonymized and handled in accordance with confidentiality requirements. The requirement for informed consent was waived due to the retrospective study design. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank all participants and clinical staff at Ningbo Hospital of Integrated Traditional Chinese and Western Medicine for their invaluable contributions to this study. We also appreciate the support of the HIV Service Database management team for assistance with data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Medical Health Science and Technology Project of Zhejiang Province (grant no. 2024KY1608).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Thet D, Siritientong T. Antiretroviral therapy-associated metabolic complications: review of the recent studies. HIV AIDS. 2020;12:507–15. doi:10.2147/hiv.S275314
2. Maurice JB, Patel A, Scott AJ, Patel K, Thursz M, Lemoine M. Prevalence and risk factors of nonalcoholic fatty liver disease in HIV-monoinfection. Aids. 2017;31(11):1621–1632. doi:10.1097/qad.0000000000001504
3. Cervo A, Milic J, Mazzola G, et al. Prevalence, predictors, and severity of lean nonalcoholic fatty liver disease in patients living with human immunodeficiency virus. Clin Infect Dis. 2020;71(10):e694–e701. doi:10.1093/cid/ciaa430
4. Feng G, Targher G, Byrne CD, et al. Global burden of metabolic dysfunction-associated steatotic liver disease, 2010 to 2021. JHEP Rep. 2025;7(3):101271. doi:10.1016/j.jhepr.2024.101271
5. Allende DS, Cummings O, Sternberg AL, et al. MASLD in people with HIV exhibits higher fibrosis stage despite lower disease activity than in matched controls. Aliment Pharmacol Ther. 2024;60(10):1351–1360. doi:10.1111/apt.18236
6. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542–1556. doi:10.1016/j.jhep.2023.06.003
7. Anstee QM, Reeves HL, Kotsiliti E, Govaere O, Heikenwalder M. From NASH to HCC: current concepts and future challenges. Nat Rev Gastroenterol Hepatol. 2019;16(7):411–428. doi:10.1038/s41575-019-0145-7
8. Gawrieh S, Vilar-Gomez E, Woreta TA, et al. Prevalence of steatotic liver disease, MASLD, MetALD and significant fibrosis in people with HIV in the United States. Aliment Pharmacol Ther. 2024;59(5):666–679. doi:10.1111/apt.17849
9. Bussetty A, Shah N, Chandler TM, Ghattu M, Kesavarapu K. Current and future implications of weight loss drugs on liver disease. Clin Liver Dis. 2025;29(4):743–753. doi:10.1016/j.cld.2025.06.005
10. Liu L, Xia Y, Wang B, Zhang Y. Efficacy of incretin-based therapies in patients with metabolic dysfunction-associated steatotic liver disease: an updated systematic review and meta-analysis of randomized controlled trials. J Gastroenterol Hepatol. 2025;40(11):2659–2673. doi:10.1111/jgh.70084
11. Pedro KD, Henderson AJ, Agosto LM. Mechanisms of HIV-1 cell-to-cell transmission and the establishment of the latent reservoir. Virus Res. 2019;265:115–121. doi:10.1016/j.virusres.2019.03.014
12. Njelekela M, Mpembeni R, Muhihi A, Ulenga N, Aris E, Kakoko D. Lipodystrophy among HIV-infected patients attending care and treatment clinics in dar es salaam. AIDS Res Treat. 2017;2017:3896539. doi:10.1155/2017/3896539
13. Biały M, Czarnecki M, Inglot M. Impact of combination antiretroviral treatment on liver metabolic health in HIV-infected persons. Viruses. 2023;15(12):2432. doi:10.3390/v15122432
14. Lv T, Tian J, Sun Y, et al. Institutional nomogram for estimating risk of metabolic associated fatty liver disease (MAFLD). Diabetes Metab Syndr Obes. 2024;17:3735–3752. doi:10.2147/dmso.S469677
15. Yuan Y, Xu M, Zhang X, et al. Development and validation of a nomogram model for predicting the risk of MAFLD in the young population. Sci Rep. 2024;14(1):9376. doi:10.1038/s41598-024-60100-y
16. Yang M, Chen X, Shen Q, et al. Development and validation of a predictive nomogram for the risk of MAFLD in postmenopausal women. Front Endocrinol. 2024;15:1334924. doi:10.3389/fendo.2024.1334924
17. Jin Y, Zhu J, Chen Q, et al. Development and validation of a nomogram for predicting the outcome of metabolic syndrome among people living with HIV after antiretroviral therapy in China. Front Cell Infect Microbiol. 2025;15:1514823. doi:10.3389/fcimb.2025.1514823
18. Dietrich CF, Shi L, Löwe A, et al. Conventional ultrasound for diagnosis of hepatic steatosis is better than believed [Konventioneller Ultraschall in der Fettleber-Diagnostik ist besser als sein Ruf]. Z Gastroenterol. 2022;60(8):1235–1248. doi:10.1055/a-1491-1771
19. Chinese Society of hepatology CMA. Guidelines for the prevention and treatment of metabolic dysfunction-associated (non-alcoholic) fatty liver disease (Version 2024). Zhonghua Gan Zang Bing Za Zhi. 2024;32(5):418–434. doi:10.3760/cma.j.cn501113-20240327-00163
20. Vickers AJ, Cronin AM, Elkin EB, Gonen M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. 2008;8(1):53. doi:10.1186/1472-6947-8-53
21. Zou H, Zhao F, Lv X, Ma X, Xie Y. Development and validation of a new nomogram to screen for MAFLD. Lipids Health Dis. 2022;21(1):133. doi:10.1186/s12944-022-01748-1
22. Zhou B, Gong N, Huang X, Zhu J, Qin C, He Q. Development and validation of a nomogram for predicting metabolic-associated fatty liver disease in the Chinese physical examination population. Lipids Health Dis. 2023;22(1):85. doi:10.1186/s12944-023-01850-y
23. Wang D, Zhou BY, Xiang L, Chen XY, Feng JX. Alanine aminotransferase as a risk marker for new-onset metabolic dysfunction-associated fatty liver disease. World J Gastroenterol. 2024;30(25):3132–3139. doi:10.3748/wjg.v30.i25.3132
24. Copur S, Demiray A, Kanbay M. Uric acid in metabolic syndrome: does uric acid have a definitive role? Eur J Intern Med. 2022;103:4–12. doi:10.1016/j.ejim.2022.04.022
25. Zhan F, Chen J, Yan H, et al. Association of serum amylase activity and the copy number variation of AMY1/2A/2B with metabolic syndrome in Chinese adults. Diabetes Metab Syndr Obes. 2021;14:4705–4714. doi:10.2147/dmso.S339604
26. Kondo T, Hayakawa T, Shibata T, Sato Y, Toda Y. Serum levels of pancreatic enzymes in lean and obese subjects. Int J Pancreatol. 1988;3(4):241–248. doi:10.1007/bf02788453
27. Muneyuki T, Nakajima K, Aoki A, et al. Latent associations of low serum amylase with decreased plasma insulin levels and insulin resistance in asymptomatic middle-aged adults. Cardiovasc Diabetol. 2012;11(1):80. doi:10.1186/1475-2840-11-80
28. Yao J, Zhao Y, Zhang J, Hong Y, Lu H, Wu J. Serum amylase levels are decreased in Chinese non-alcoholic fatty liver disease patients. Lipids Health Dis. 2014;13(1):185. doi:10.1186/1476-511x-13-185
29. Zhuang L, Su JB, Zhang XL, et al. Serum amylase levels in relation to Islet β cell function in patients with early type 2 diabetes. PLoS One. 2016;11(9):e0162204. doi:10.1371/journal.pone.0162204
30. Yadav R, Bhartiya JP, Verma SK, Nandkeoliar MK. The evaluation of serum amylase in the patients of type 2 diabetes mellitus, with a possible correlation with the pancreatic functions. J Clin Diagn Res. 2013;7(7):1291–1294. doi:10.7860/jcdr/2013/6016.3120
31. Ram R, Subramanian A, R K. Metabolic dysfunction-associated steatotic liver disease (MASLD) in people living with HIV attending centre of excellence in HIV care at a tertiary level teaching hospital in North India-A pilot study. J Int Assoc Provid AIDS Care. 2025;24:23259582241311912. doi:10.1177/23259582241311912
32. van Eekeren LE, Vadaq N, Vos W, et al. Liver steatosis is prevalent in lean people with HIV and associated with exposure to antiretroviral treatment-A cross-sectional study. Open Forum Infect Dis. 2024;11(6):ofae266. doi:10.1093/ofid/ofae266
33. Montacchiesi G, Pace L. Epigenetics and CD8(+) T cell memory. Immunol Rev. 2022;305(1):77–89. doi:10.1111/imr.13057
34. Her Z, Tan JHL, Lim YS, et al. CD4(+) T cells mediate the development of liver fibrosis in high fat diet-induced NAFLD in humanized mice. Front Immunol. 2020;11:580968. doi:10.3389/fimmu.2020.580968
35. Murphy KM, Stockinger B. Effector T cell plasticity: flexibility in the face of changing circumstances. Nat Immunol. 2010;11(8):674–680. doi:10.1038/ni.1899
36. Yan M, Man S, Ma L, Guo L, Huang L, Gao W. Immunological mechanisms in steatotic liver diseases: an overview and clinical perspectives. Clin Mol Hepatol. 2024;30(4):620–648. doi:10.3350/cmh.2024.0315
37. Eckard AR, McComsey GA. Weight gain and integrase inhibitors. Curr Opin Infect Dis. 2020;33(1):10–19. doi:10.1097/qco.0000000000000616
38. Jemal M. A review of dolutegravir-associated weight gain and secondary metabolic comorbidities. SAGE Open Med. 2024;12:20503121241260613. doi:10.1177/20503121241260613
39. Ko YH, Wong TC, Hsu YY, Kuo KL, Yang SH. The correlation between body fat, visceral fat, and nonalcoholic fatty liver disease. Metab Syndr Relat Disord. 2017;15(6):304–311. doi:10.1089/met.2017.0001
40. Kirkegaard-Klitbo DM, Thomsen MT, Gelpi M, et al. Hepatic steatosis associated with exposure to elvitegravir and raltegravir. Clinl Infect Dis. 2021;73(3):e811–e814. doi:10.1093/cid/ciab057
41. Bischoff J, Gu W, Schwarze-Zander C, et al. Stratifying the risk of NAFLD in patients with HIV under combination antiretroviral therapy (cART). EClinicalMedicine. 2021;40:101116. doi:10.1016/j.eclinm.2021.101116
42. Navarro J, Curran A, Raventós B, et al. Prevalence of non-alcoholic fatty liver disease in a multicentre cohort of people living with HIV in Spain. Eur J Intern Med. 2023;110:54–61. doi:10.1016/j.ejim.2023.01.028
43. Shengir M, Lebouche B, Elgretli W, et al. Switch to a raltegravir-based antiretroviral regimen in people with HIV and non-alcoholic fatty liver disease: a randomized controlled trial. HIV Med. 2024;25(1):135–142. doi:10.1111/hiv.13531
44. Fernandes SR, Leite AR, Lino R, et al. The impact of integrase inhibitors on steatosis and fibrosis biomarkers in persons with HIV naïve to antiretroviral therapy. BMC Infect Dis. 2023;23(1):553. doi:10.1186/s12879-023-08530-3
45. Thomson ES, Oommen AT, Thomson ES, Pillai G. Comparison of non-invasive liver fat scoring systems as markers of metabolic dysfunction-associated liver disease. Cureus. 2024;16(10):e72222. doi:10.7759/cureus.72222
46. Iacob SA, Iacob DG. Non-alcoholic fatty liver disease in HIV/HBV patients - a metabolic imbalance aggravated by antiretroviral therapy and perpetuated by the hepatokine/adipokine axis breakdown. Front Endocrinol. 2022;13:814209. doi:10.3389/fendo.2022.814209
47. Xu W, Liu D, Zhang R, Chen J, Shen Y. Evaluation of ten diagnostic models for metabolic dysfunction-associated fatty liver disease in lean people living with HIV. BMC Infect Dis. 2025;25(1):1147. doi:10.1186/s12879-025-11540-y
48. Hu J, Fang Y, Ma S, Jin Y. Novel inflammatory metabolic parameters as predictors of metabolic dysfunction-associated fatty liver disease in people living with HIV receiving antiretroviral therapy: a retrospective cohort study. Front Public Health. 2026;14:1716876. doi:10.3389/fpubh.2026.1716876
49. Fujii H, Uchida-Kobayashi S, Kanamori A, et al. Defining optimal fatty liver index thresholds for MASLD and MetALD using controlled attenuation parameter as reference. J Gastroenterol. 2025;60(10):1296–1309. doi:10.1007/s00535-025-02287-z
50. Malandris K, Korakas E, Sarakapina A, et al. Accuracy of controlled attenuation parameter for liver steatosis in high-risk patients for MASLD using MRI-proton density fat fraction as reference standard. Dig Dis Sci. 2025;70(2):814–824. doi:10.1007/s10620-024-08799-7
51. Patil A, Mungase SB, Nadella M, Adela R. Diagnostic performance of non-invasive markers for distinguishing MASLD/MASH: insights from meta-analysis and real-world data. Clin Chim Acta. 2026;582:120787. doi:10.1016/j.cca.2025.120787
52. Lin F, Obeid A, Sharma M, Kaur P, Chaput K, Liaquat H. Diagnostic performance of fibrosis-4 index, nonalcoholic fatty liver disease fibrosis score, AST-to-platelet ratio index, and BARD score among young and older adults for the diagnosis of advanced MASLD fibrosis: a retrospective cohort study. JGH Open. 2025;9(9):e70281. doi:10.1002/jgh3.70281
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting the Risk of Unplanned Readmission at 30 Days After PCI: Development and Validation of a New Predictive Nomogram
Xu W, Tu H, Xiong X, Peng Y, Cheng T
Clinical Interventions in Aging 2022, 17:1013-1023
Published Date: 5 July 2022
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Development and Validation of a Prediction Model for Chronic Post-Surgical Pain After Thoracic Surgery in Elderly Patients: A Retrospective Cohort Study
Wu XD, Zeng FF, Yu XX, Yang PP, Wu JP, Xv P, Wang HT, Pei YM
Journal of Pain Research 2022, 15:3079-3091
Published Date: 29 September 2022
An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction
Chen Y, Xie K, Han Y, Xu Q, Zhao X
Journal of Inflammation Research 2023, 16:4061-4071
Published Date: 13 September 2023
Risk Factors for Granulomatous Mastitis and Establishment and Validation of a Clinical Prediction Model (Nomogram)
Zeng Y, Zhang D, Fu N, Zhao W, Huang Q, Cui J, Chen Y, Liu Z, Zhang X, Zhang S, Mansoor KM
Risk Management and Healthcare Policy 2023, 16:2209-2222
Published Date: 20 October 2023