Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Establishment and Validation of a Nomogram Based on Inflammation-Immunity-Nutrition Biomarker Scores to Predict Postoperative Early Recurrence in Patients with Hepatocellular Carcinoma: A Multicenter Study
Authors Zhang Y, Tang J, Liu Y, Tao L, Liu Z, Liao K, Yuan Q
Received 23 October 2025
Accepted for publication 23 December 2025
Published 8 January 2026 Volume 2026:13 572863
DOI https://doi.org/10.2147/JHC.S572863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Yuhan Zhang,1,* Jin Tang,2,* Yan Liu,3,* Limei Tao,1 Zhiying Liu,1 Kexi Liao,4 Qiaoying Yuan1
1Department of Nutrition, The First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China; 2Department of Nutrition, Guang’an People’s Hospital, Guang’an, People’s Republic of China; 3Prevention and Health Section, 958th Hospital of the Chinese People ‘s Liberation Army, Chongqing, People’s Republic of China; 4Department of Hepatobiliary Surgery, The First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiaoying Yuan, Department of Nutrition, The First Affiliated Hospital of Army Medical University, Gaotanyan Road 30, Shapingba District, Chongqing, 400038, People’s Republic of China, Email [email protected] Kexi Liao, Department of Hepatobiliary Surgery, The First Affiliated Hospital of Army Medical University, Gaotanyan Road 30, Shapingba District, Chongqing, 400038, People’s Republic of China, Email [email protected]
Purpose: Early postoperative recurrence of hepatocellular carcinoma (HCC) significantly impairs patient quality of life and shortens survival. However, existing models rely on single-center or single-dimensional data, making accurate detection of early postoperative HCC recurrence challenging. Thus, designing/evaluating a reliable, non-invasive, comprehensive tool to predict HCC recurrence risk is crucial for guiding postoperative individualized antitumor treatment and improving prognosis.
Patients and methods: We retrospectively enrolled patients with HCC (n=1424) receiving curative-intent hepatectomy at the First Affiliated Hospital of Army Medical University of China between December 2012 and December 2022. Patients were randomly stratified into training and testing cohorts in a 7:3 ratio. Using least absolute shrinkage and selection operator (LASSO) logistic and multivariate logistic regression, we screened optimal predictors and subsequently developed a nomogram alongside an online calculator. The prediction model was externally validated at two other medical institutions (n = 218). The area under the curve (AUC) of the receiver operating characteristic, calibration, and decision curves were used to evaluate model performance.
Results: The nomogram intuitively showed nine independent risk factors in the prediction model for short-term recurrence in patients with HCC: Edmondson Steiner III–IV, tumor satellite nodules, vascular invasion, largest tumor > 5 cm, alpha-fetoprotein (AFP) level ≥ 400 μg/L, DeRitis ratio ≥ 1.49, gamma-glutamyl transferase (GGT) level ≥ 63.5 U/L, prognostic nutritional index (PNI) < 46.18, and neutrophil-to-lymphocyte ratio (NLR) ≥ 1.91. The AUCs of the training, testing, and validation cohorts were 0.760 (95% CI: 0.731– 0.790), 0.784 (95% CI: 0.741– 0.828), and 0.787 (95% CI: 0.728– 0.846), respectively, indicating good predictive performance. The calibration and decision curves indicated that the model could be translated into tangible clinical benefits.
Conclusion: We constructed and evaluated a nomogram based on inflammation-immunity-nutrition biomarker scores to predict early postoperative recurrence of HCC, offering a free, user-friendly online calculator for quick access to results. This calculator empowers clinicians to convert complex clinical data into actionable insights, enabling the design of risk-stratified postoperative management strategies.
Keywords: HCC, postoperative early recurrence, prediction model, nomogram, inflammation-immunity-nutrition biomarker scores
Introduction
Hepatocellular carcinoma (HCC) is a highly recurrent and metastatic malignancy, posing a significant global health burden. HCC is currently the sixth most common cancer and the third leading cause of cancer-related deaths globally.1,2 HCC treatment is based on surgical resection; however, even after surgery, an alarmingly high risk (70%) of tumor recurrence within five years remains.3–6 This high recurrence remains among the main bottlenecks that limit long-term treatment efficacy in patients with HCC.
Clinically, early and late recurrences generally manifest within a 2-year window following surgical resection.7,8 In contrast to late recurrence, early recurrence can lead to a worse quality of life and lower survival rate, severely challenging the prognostic management of patients with HCC.7,9 Most of the existing prediction models have limited predictive value for postoperative early recurrence owing to small sample size, single-center design, or single-dimensional variables.10–12 Thus, identifying and developing a trustworthy and comprehensive tool for predicting risk of recurrence in HCC for guiding individualized postoperative medical care is warranted.
Recent research has confirmed that nutritional status, immune defense, and inflammatory response are closely related to tumor recurrence. Several existing clinical prediction models aim to combine preoperative inflammation and nutrition or immune-related indicators of patients with HCC, including albumin, platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio (NLR), prognostic nutritional index (PNI), and preoperative alpha-fetoprotein (AFP) values, which are more innovative and practical than traditional models.10,13,14 However, these models often ignore the correlations, interactions, and inseparability between nutrition, immunity, and inflammatory states. Previous studies have used the inflammation-immunity-nutrition score nomogram to predict the prognosis of different tumours15–18 but have rarely forecasted the likelihood of early postoperative recurrence for HCC patients.
This research aimed to formulate a novel inflammation-immunity-nutrition biomarker score, providing a practical tool for predicting early postoperative risk in HCC. Furthermore, the nomogram transforms a complex regression equation into a visual graph, enhancing prediction readability and substantially improving ease of use in clinical practice and the operability of personalized assessment and intervention.
Methods
Patients
In this study, we employed a retrospective case-control design to retrieve HCC data from the First Affiliated Hospital of Army Medical University, the 958th Hospital of the Chinese People’s Liberation Army, and Guang’an People’s Hospital. Overall, 2651 HCC patients meeting the eligibility criteria were subjected to screening. The criteria for inclusion were as follows: (1) between 18 and 75 years of age; (2) previous radical hepatectomy performed by the same surgical team; (3) HCC confirmed by postoperative pathological examination; and (4) histologically confirmed R0 resection. The exclusion criteria included: (1) preoperative liver function classification Child-Pugh C; (2) prior preoperative anticancer treatment; (3) combination with other or secondary malignant tumors; and (4) incomplete clinical records or lack of follow-up post-surgery within a 24-month period. Patient data were collated by three investigators, two of whom were responsible for data extraction, while the other investigator performed accuracy checks.
The study was conducted in accordance with the principles of the Declaration of Helsinki (as revised in 2013) and approved by the ethical committee of each participating hospital: the First Affiliated Hospital of Army Medical University [Approval No. (B)KY2025011], Guang’an People’s Hospital [Approval No. 2025022], and the 958th Hospital of the Chinese People’s Liberation Army [Approval No. ER2025KY088]. Informed consent was waived by the Ethics Committees due to the use of de-identified, historical medical records in this retrospective study.
Data
Input variables were divided into the following groups: (1) basic demographic features: sex, body mass index (BMI), age, smoking behavior, drinking behavior, and history of hepatitis B virus infection; (2) pathological tumor features: maximum tumor diameter, vascular invasion, tumor satellite nodules, and Edmondson Steiner grade; (3) preoperative hematological indicators: inflammatory-immune markers, such as neutrophil (NEUT), lymphocyte (LYMPH), and white blood cell counts, hepatitis B surface antigen, AFP level and NLR; (4) nutrition-related markers: hemoglobin, albumin (ALB), fasting blood glucose, blood creatinine, and PNI; and (5) hepatic function indicators: alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), and alkaline phosphatase (ALP) levels, platelet count, prothrombin activity (PTA), and DeRitis ratio.
The formulas employed to determine the clinical indicators included: BMI = weight (kg)/height2 (m2); PNI = ALB (g/L) + 5 * Lymph; DeRitis ratio = AST (U/L) / ALT (U/L); and NLR = NEUT / LYMPH.
Follow-up
Patients were monitored monthly for the initial three months following surgery and every 3 months up to the 2-year mark postoperatively. Follow-up was conducted to evaluate whether tumor recurrence occurred within 2 years post-surgery in patients with HCC. Follow-up evaluation included routine liver function tests, serum AFP measurement, liver contrast-enhanced ultrasound, abdominal enhanced computed tomography, and tumor-specific magnetic resonance imaging. Diagnosis of HCC recurrence adhered to the criteria outlined in the 2022 Chinese guidelines for primary liver cancer therapy and diagnosis.19
Construction and Verification of the Nomogram
Based on the training dataset, significant differences between the recurrence and non-recurrence groups were analyzed using univariate logistic regression. Furthermore, we optimized variable selection, reduced multicollinearity, and controlled model overfitting using least absolute shrinkage and selection operator (LASSO) regression. Predictors identified via LASSO were included in the multivariate logistic regression model and a nomogram established thereafter. Finally, a practical online calculator was created based on the nomogram.
The performance of a prediction model is typically verified via multiple validations of three dimensions: discrimination, accuracy, and clinical validity. Receiver operating characteristic (ROC) curve analysis was performed to assess model discrimination, with an area under the curve (AUC) ≥0.75 indicating good discrimination. A calibration curve was used to assess consistency between the predicted probability and the observed results. Additionally, clinical applicability was examined using decision curve analysis (DCA).
Statistical Analysis
Statistical analyses were performed using SPSS (version 26.0) and the R software (version 4.3.2). Normally distributed quantitative variables are presented as the mean ± standard deviation and were compared using independent t-tests, whereas non-normally distributed quantitative variables are presented as median (Q1, Q3) quartiles and were analyzed using the Mann–Whitney U-test. Categorical variables are described as frequencies and were compared using chi-square tests. All tests were two-tailed, with P < 0.05 considered statistically significant.
Results
Patient Characteristics
Relevant clinical data entered into the database were retrospectively reviewed and screened in strict accordance with the inclusion and exclusion criteria. Finally, 1424 eligible patients from the First Affiliated Hospital of Army Medical University between 2012 and 2022 were included and randomly allocated to the training (n = 996) and testing (n = 428) cohorts in a 7:3 ratio. Additionally, 218 eligible patients with HCC from two tertiary hospitals between 2015 and 2022 were enrolled in the external validation cohort (Figure 1). Baseline characteristics were not significantly different between the training and testing groups (Table 1). For most factors, significant differences were observed between the training and validation cohorts, warranting further discussion. In the training cohort, early HCC recurrence risk was 44.6%; moreover, smoking behavior, drinking behavior, NEUT and LYMPH counts, AST, ALT, GGT, ALP, and AFP levels, PTA, PNI, and NLR, along with some pathological features, differed significantly between the recurrence and non-recurrence groups (Table 2).
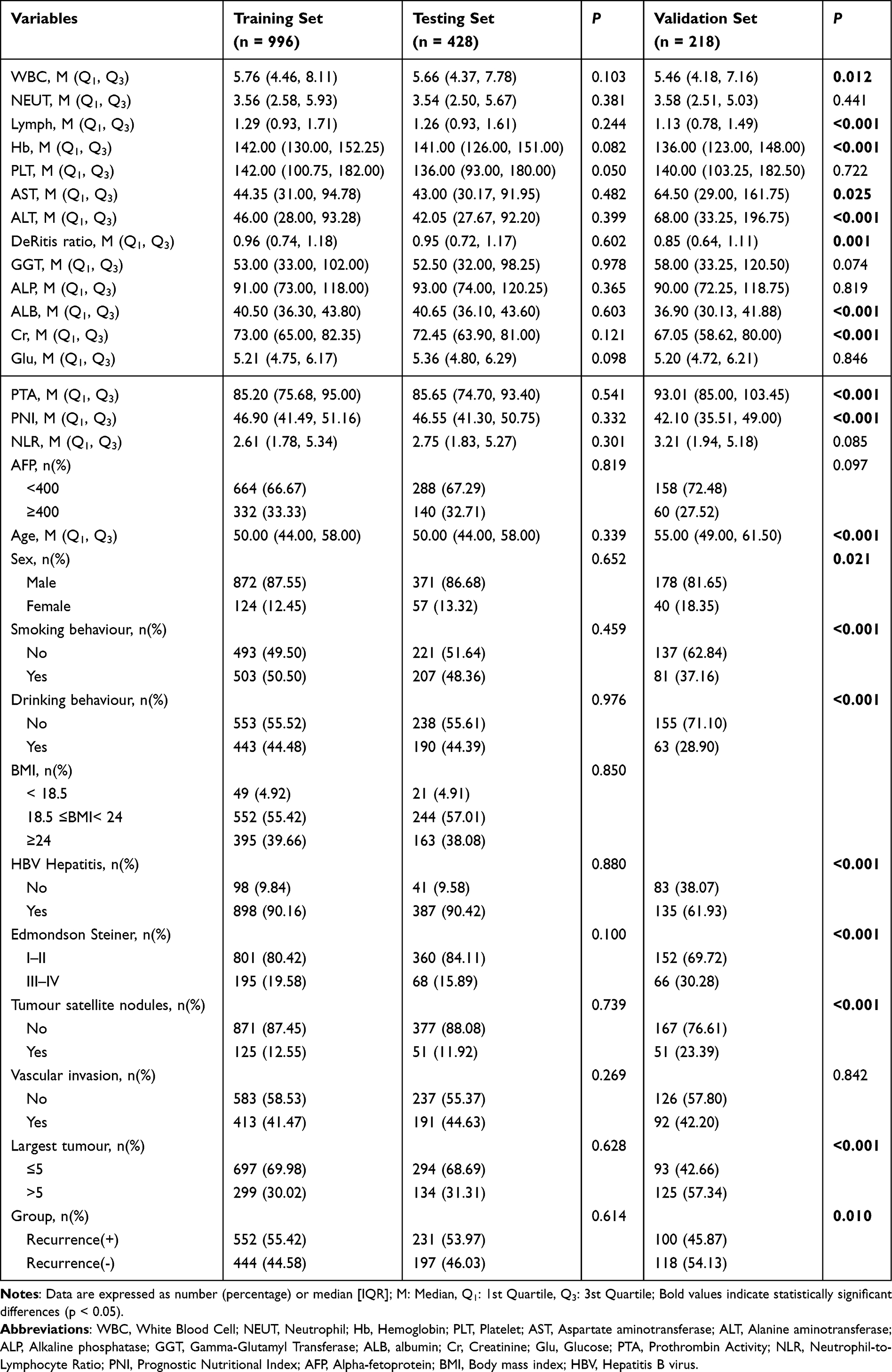 |
Table 1 Characteristics in the Training, Testing, and Validation Cohorts |
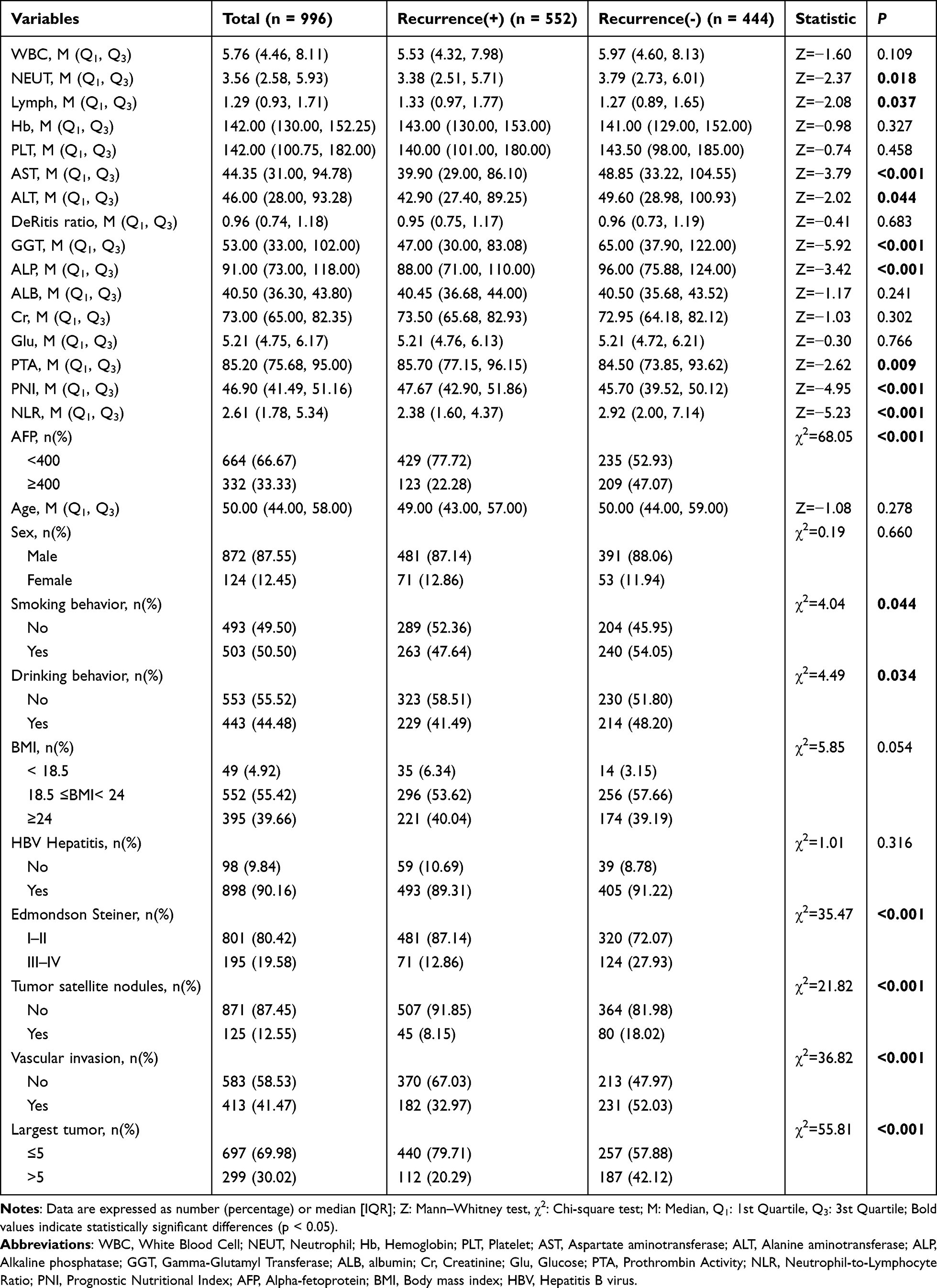 |
Table 2 Characteristics of the Patients Presenting with and Without Early Recurrence in the Training Set |
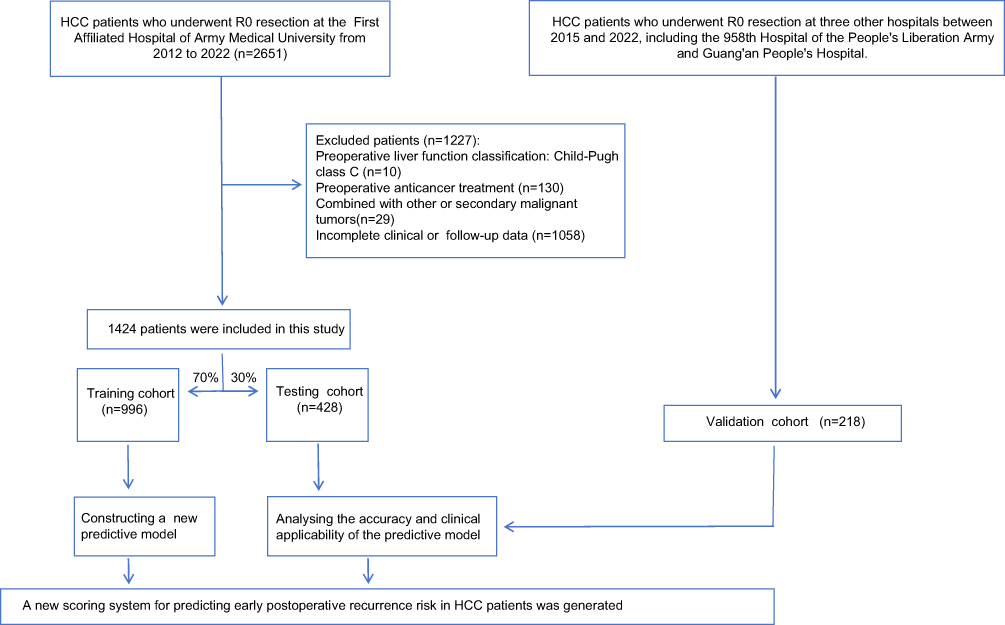 |
Figure 1 Patient selection flowchart. Abbreviations: HCC, hepatocellular carcinoma; R0, complete tumor resection with negative margins. |
LASSO, Univariate, and Multivariate Logistic Regression Analyses
Univariate logistic analysis identified 13 risk factors associated with early HCC recurrence, including smoking behavior, drinking behavior, LYMPH count, and PTA, PNI, NLR, GGT, and AFP levels, DeRitis ratio, Edmondson-Steiner, vascular invasion, tumor satellite nodules, and largest tumor diameter (Table 3). Through LASSO regression, 10 potential predictors were selected from 13 candidates to enhance the robustness of the model and avoid overfitting (Figure 2A and B). Finally, multivariate logistic regression analysis was performed to further screen nine independent risk-associated variables for postoperative early HCC recurrence (Table 4): Edmondson Steiner III–IV (odds ratio [OR] = 2.584, 95% confidence interval [CI]: 1.804–3.700, P <0.001), tumor satellite nodules (OR = 2.133, 95% CI: 1.383–3.291, P < 0.001), vascular invasion (OR = 1.768, 95% CI: 1.328–2.354, P < 0.001), largest tumor ≤5 cm (OR = 0.483; 95% CI: 0.351–0.665; P < 0.001), AFP level ≥ 400 ng/µL (OR = 2.645; 95% CI: 1.953–3.581; P < 0.001), DeRitis ratio (OR = 2.232, 95% CI: 1.482–3.363, P < 0.001), GGT level (OR = 1.002, 95% CI: 1.001–1.004, P = 0.003), PNI (OR = 0.967, 95% CI: 0.946–0.988, P = 0.002), and NLR (OR = 1.026, 95% CI: 1.002–1.051, P = 0.036).
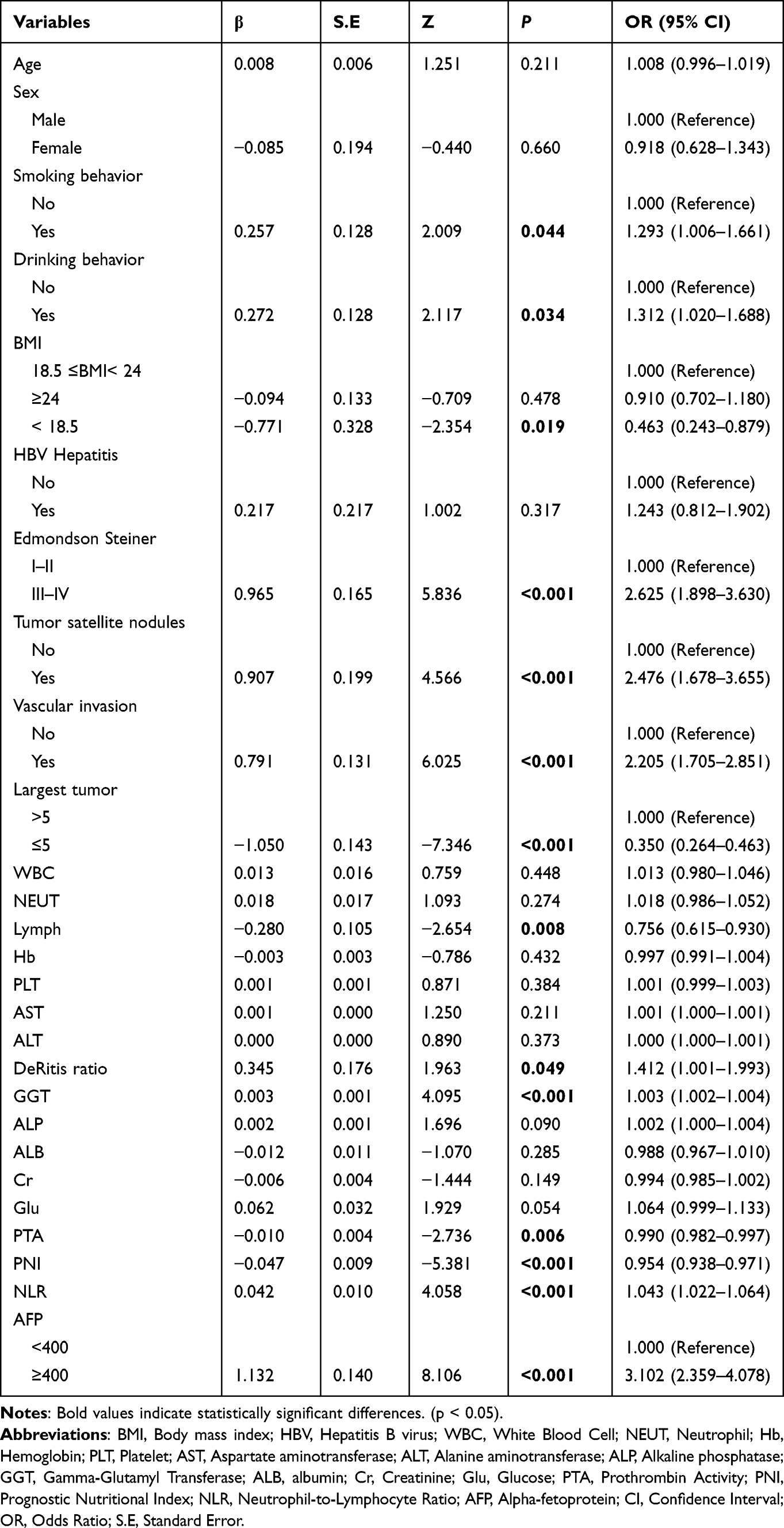 |
Table 3 Univariable Logistic Regression Analyses of Risk Factors for Postoperative Early Recurrence in Patients with HCC |
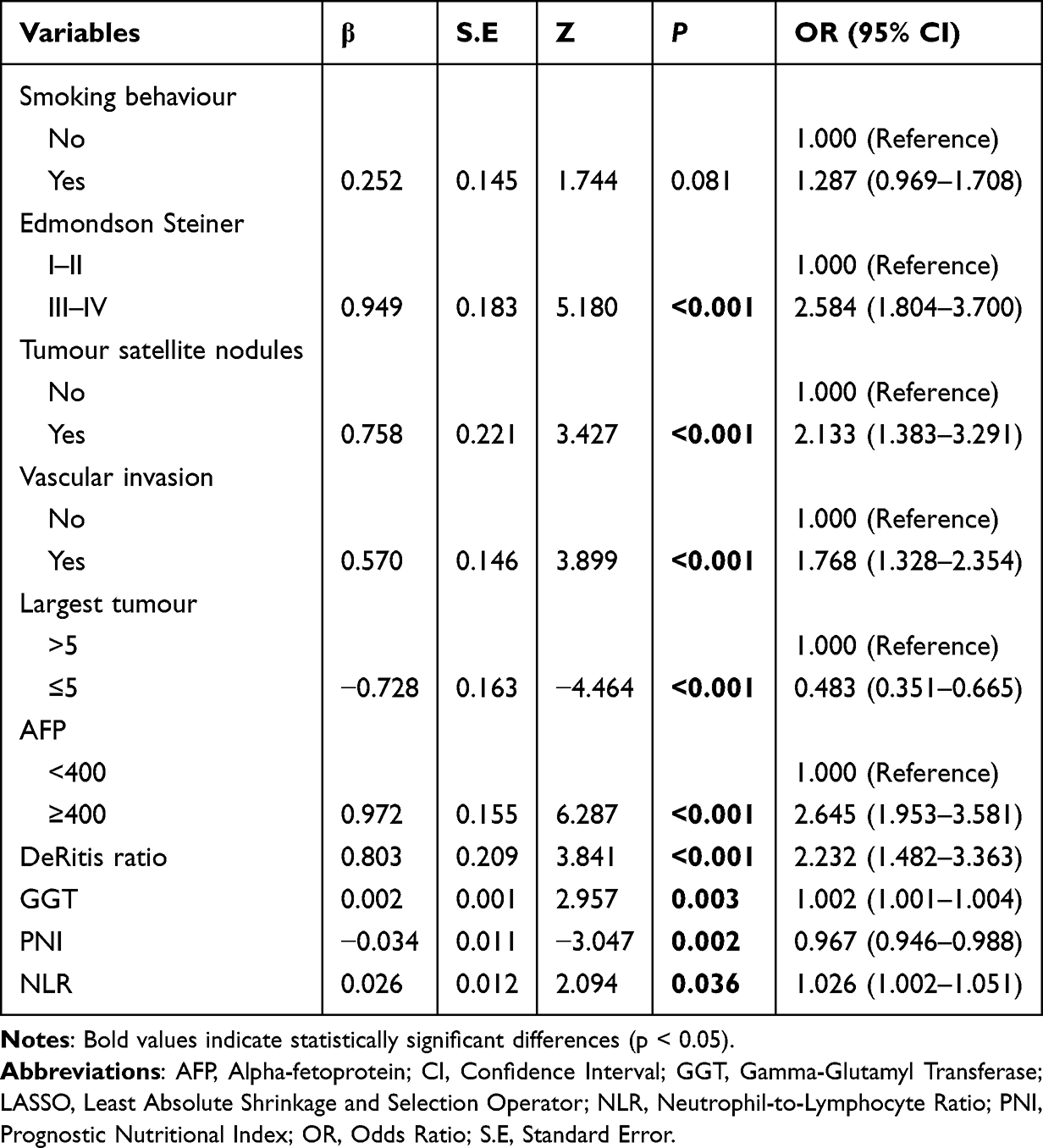 |
Table 4 Multivariate Logistic Regression Analysis of Predictors Selected by the LASSO Regression Procedure in the Training Set |
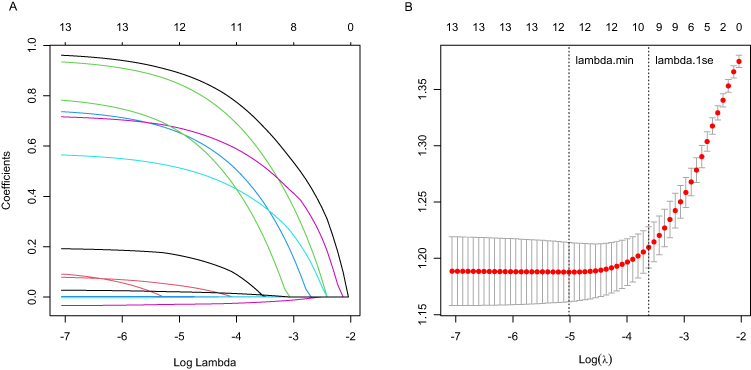 |
Figure 2 LASSO coefficient profiles for postoperative early recurrence in patients with HCC. (A) Each curve presents the change in the coefficient. The ordinate is the coefficient value, the lower abscissa is log(λ), and the upper abscissa is the number of non-zero coefficients in the model. (B) Ten-fold cross-validation was performed to fit and select the model. Abbreviations: LASSO, least absolute shrinkage and selection operator; HCC, hepatocellular carcinoma. |
Nomogram Construction
To simplify the model, we used DeRitis ratio, GGT level, PNI, and NLR to select the best threshold point on the ROC curve and calculated the critical values as follows: 1.49, 63.50 U/L, 46.18, and 1.91, respectively. This method transforms continuous variables into categorical variables and reintroduces them into the constructed model, improving its clinical applicability to a certain extent. Based on the nine risk factors screened, a nomogram was developed to quantify the risk of early postoperative HCC recurrence.
As shown in Figure 3, Edmondson Steiner III–IV, tumor satellite nodules, vascular invasion, largest tumor > 5 cm, AFP level ≥ 400 ng/µL, DeRitis ratio ≥ 1.49, GGT level ≥ 63.5 U/L, PNI < 46.18, and NLR ≥ 1.91 were independent risk factors for short-term HCC recurrence, with scores of 100, 78, 67, 72, 93, 98, 54, 38, and 59, respectively. Indicator scores were summed to obtain a total score, and a corresponding risk scale is presented in the nomogram (Figure 3).
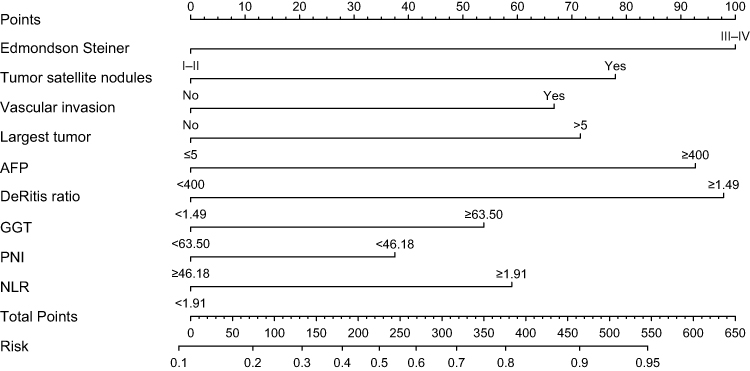 |
Figure 3 Nomogram for predicting early HCC recurrence risk after surgery. The predictive indicators on each level represent a certain score. The total score corresponds to the early recurrence risk and is generated by summing the scores of each predictor. Abbreviations: AFP, alpha-fetoprotein; GGT, gamma-glutamyl transferase; HCC, hepatocellular carcinoma; NLR, neutrophil-to-lymphocyte ratio; PNI, prognostic nutritional index. |
Evaluation and Verification of the Prediction Model
In the training set, the ROC curve exhibited strong discriminative ability (AUC, 0.760; 95% CI: 0.731–0.790; Figure 4A). The discriminative ability in the test (AUC, 0.784; 95% CI: 0.741–0.828) and validation (AUC, 0.787; 95% CI: 0.728–0.846) sets was verified (Figure 4B and C). In the Hosmer–Lemeshow test, χ2 values of 14.78 (P = 0.063), 10.91 (P= 0.207), and 13.97 (P = 0.083) were obtained in the training, test, and validation sets, respectively. Therefore, the model displayed good goodness-of-fit, and the calibration curve analysis showed that the predicted probability of short-term postoperative recurrence in patients with HCC was highly consistent with the actual risk in both internal and external validations (Figure 5). Furthermore, the DCA method was applied to evaluate the transferability of the model to clinical contexts. The model demonstrated significantly higher net benefit in internal/external validation sets than the two extremes, indicating good clinical utility (Figure 6).
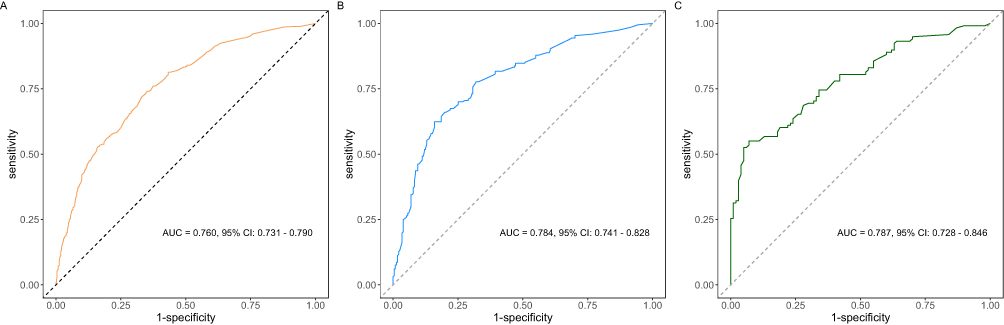 |
Figure 4 ROC curve and AUC of the prediction model. (A) ROC curve in the training cohort. (B) ROC curve in the testing cohort. (C) ROC curve in the validation cohort. Abbreviations: ROC, receiver operating characteristic; AUC, area under the curve; CI, confidence interval. |
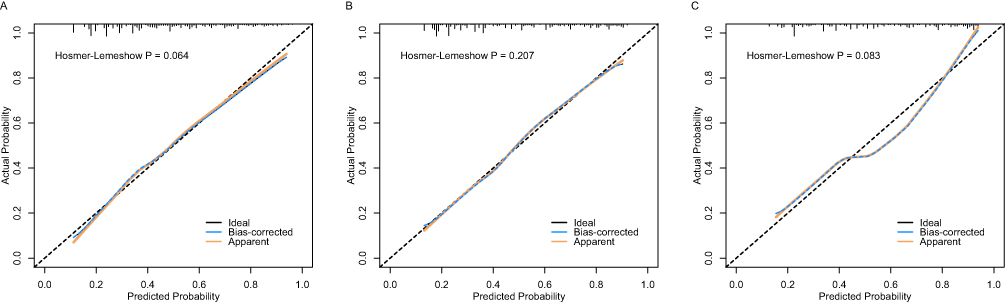 |
Figure 5 Nomogram calibration plots in the training (A), testing (B), and validation (C) cohorts. |
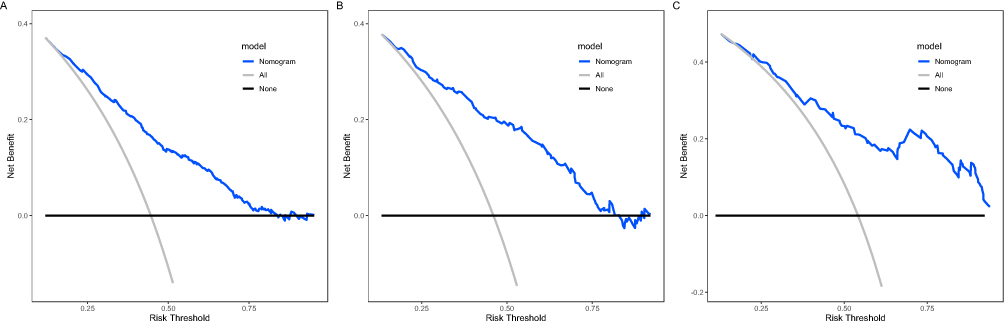 |
Figure 6 Decision clinical analysis curves of the nomogram in the training (A), testing (B), and validation (C) cohorts. |
Web-Based Calculator
Using the above nomogram, we created a web-based calculator to predict short-term recurrence risk in patients with HCC post-hepatectomy (Figure 7). The clinician enters the variable in the left option box, upon which the right-hand section presents the predicted likelihood of early recurrence in patients with HCC. The excellent performance of the web-based calculator in terms of accuracy, convenience, and speed can assist clinical decision makers in personalized medicine implementation. The calculator has been published online and is available at this URL: https://zhangxiaosong520.shinyapps.io/Prediction_model/.
 |
Figure 7 Multicenter validation of a web-based tool for early HCC recurrence risk assessment. Abbreviations: AFP, alpha-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma-glutamyl transferase; HCC, hepatocellular carcinoma; NLR, neutrophil-to-lymphocyte ratio; PNI, prognostic nutritional index. |
Discussion
This study formulated and validated a novel multidimensional model that, for the first time, integrates clinical indicators across four critical dimensions, namely tumor characteristics, nutritional status, immunity, and inflammation, thereby providing a more com; prehensive risk assessment framework compared with those based on traditional single-dimensional indicators (eg, AFP level, microvascular invasion [MVI], and NLR).10–12,14,20 Notably, this model demonstrated enhanced predictive ability compared with conventional metrics. Moreover, based on conventional laboratory test indicators, no special molecular markers (eg, AFP-L3 or PIVKA-II) are required.21,22
Although surgical resection is the main HCC treatment, the postoperative recurrence rate remains high.2,3 Early recurrence of HCC is linked to lower quality of life and reduced survival rates, presenting substantial challenges in effective prognostic management.2,7 Studies have aimed to develop models to predict early HCC recurrence risk. For instance, a multicenter study found that a tumor diameter > 5 cm, AFP level > 400 μg/L, satellite nodules, and MVI served as independent risk markers for postoperative early recurrence (≤ 2 years).23 Additionally, the Chinese Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2024 Edition) define AFP ≥ 400 ng/mL as a core threshold for the diagnosis and prognosis evaluation of HCC.24 Moreover, Liu et al indicated that the GGT level is an aggravating parameter for such a risk.25 The joint application of GGT levels and the DeRitis ratio exhibited strong predictive ability for MVI occurrence in patients with HCC, which aids in the timely identification of poor prognosis.26 However, the predictive value of existing models in estimating outcomes is limited, highlighting the urgent need for novel, accurate, and comprehensive predictive models for personalized diagnostic and therapeutic approaches for patients with HCC.
Consistent with the findings of previous research regarding the incidence of early recurrence among patients with HCC, 46% of the 1642 cases included in this study experienced early recurrence after surgery.4–6 Our nomogram model was based on the following nine variables: Edmondson Steiner III–IV, tumor satellite nodules, vascular invasion, largest tumor, AFP level, DeRitis ratio, GGT level, PNI, and NLR. Among these, the first seven variables have been widely included in previous risk models of postoperative early HCC recurrence. However, the predictive capability of NLR and PNI, when integrated with the above variables, remains unknown. An elevated NLR reflects either increased neutrophil infiltration or decreased lymphocytes in the tumor microenvironment, which may promote tumor immune escape and accelerate recurrence.27,28 Wong et al reported that NLR is a valuable biomarker for predicting postoperative early recurrence in patients with HCC, with NLR ≥ 3 being associated with shortened overall survival;14 our findings corroborate these results. Furthermore, the PNI calculated from serum albumin and circulating blood lymphocyte counts has frequently been used to assess the nutritional-immune profile of patients with diverse tumors. Zhao et al confirmed that PNI, a nutritional indicator, exhibits an independent association with the overall survival of patients with nasopharyngeal carcinoma.29 In several studies, PNI has been recognized as a practical prognostic indicator for HCC.10,30 Specifically, Chan et al confirmed that PNI serves as an independent predictor of early-stage HCC recurrence.10 Therefore, of the nine independent risk factors for early postoperative HCC recurrence that were screened in this investigation, NLR and PNI served as critical factors in the inflammatory-immune-nutrition biomarker score.
The predictive performance of the model in forecasting postoperative HCC early recurrence in the training, testing, and verification sets was 0.760, 0.784, and 0.787, respectively, suggesting the effectiveness of the model’s predictive performance. The model’s clinical applicability and application value underwent further evaluation using calibration and DCA curve analysis. Additionally, our nomogram was based on datasets from three clinical institutions, which were internally and externally validated using the test and validation sets, respectively. Compared with that of a previous single-center model, the predictive efficacy of the current multicenter model was high and the reliability was strong.11,25 Despite baseline disparities between the training and validation sets, the excellent real-world applicability of the model in external validation indirectly highlights its replicability and generalizability. The model results were visualized in a nomogram, and clinicians can objectively evaluate various HCC-related clinical indicators in patients.
This study has several strengths. First, all data are from real‑world settings, and the large sample size together with internal and external validation ensures high credibility and authenticity. Second, we developed a multidimensional model based on nutrition–immunity–inflammation status, which complements existing models for predicting HCC recurrence. Finally, the web‑based calculator enables clinicians to turn complex clinical data into actionable decisions, allowing risk‑stratified postoperative strategies—avoiding unnecessary tests in low‑risk patients and focusing resources on high‑risk groups—while empowering patients and achieving both precision medicine and humanistic care.
Nevertheless, the study also had certain limitations. First, retrospective data inevitably introduce selection or information bias, leading to insufficient representation of high-risk recurrence groups. Second, although reliability was enhanced through multicenter internal validation, the model has not yet been validated in major HCC-endemic regions outside East Asia (eg, Africa, Southeast Asia), and its generalizability requires further exploration. In future work, we plan to conduct prospective validation in patients with different risk strata of HCC and establish international multicenter collaborations.
Recurrence risk can be rapidly and conveniently estimated using the online calculator derived from the nomogram, which aids in preliminary risk stratification in clinical practice and assists surgeons in implementing accurate monitoring and early intervention.
Conclusions
We established and verified an integrated nomogram formulated on inflammation, immunity, and nutrition biomarker scores, which may assist clinicians in predicting early recurrence after HCC resection and in providing appropriate actions to ameliorate survival outcomes. Moreover, this study provides a free and available online calculator for clinicians to quickly obtain results and customize individualized antitumor strategies.
Acknowledgments
We thank all the patients and the medical staff.
Funding
This work was supported by the National Natural Science Foundation of China (NSFC) (No. 82504206).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–14. doi:10.3322/caac.21834
2. Ganesan P, Kulik LM. Hepatocellular carcinoma: new developments. Clin Liver Dis. 2023;27(1):85–102. doi:10.1016/j.cld.2022.08.004
3. Tang SC, Diao YK, Lin KY, et al. Association of Pringle maneuver with postoperative recurrence and survival following hepatectomy for hepatocellular carcinoma: a multicenter propensity score and competing-risks regression analysis. Hepatobiliary Surg Nutr. 2024;13(3):412–424. doi:10.21037/hbsn-23-7
4. Shang C, Zhong J, Luo X, Wei J, Chen Y. Postoperative adjuvant therapy with donafenib in hepatocellular carcinoma with high-risk recurrence factors: a real-world, prospective, observational study. J Clin Oncol. 2025;43:e16316–e16316. doi:10.1200/JCO.2025.43.16_suppl.e16316
5. Yan WT, Li C, Yao LQ, et al. Predictors and long-term prognosis of early and late recurrence for patients undergoing hepatic resection of hepatocellular carcinoma: a large-scale multicenter study. Hepatobiliary Surg Nutr. 2023;12(2):155–168. doi:10.21037/hbsn-21-288
6. Zhang ZJ, Wei BJ, Liu ZK, Xuan ZF, Zhou L, Zheng SS. Nomogram for prediction of hepatocellular carcinoma recurrence after liver resection. Hepatobiliary Pancreat Dis Int. 2025;24(3):269–276. doi:10.1016/j.hbpd.2024.09.006
7. Xu XF, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from China. JAMA Surg. 2019;154(3):
8. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019.
9. Wang MD, Li C, Liang L, et al. Early and late recurrence of hepatitis B virus-associated hepatocellular carcinoma. Oncologist. 2020;25(10):e1541–e1551. doi:10.1634/theoncologist.2019-0944
10. Chan AWH, Chan SL, Wong GLH, et al. Prognostic nutritional index (PNI) predicts tumor recurrence of very early/early stage hepatocellular carcinoma after surgical resection. Ann Surg Oncol. 2015;22(13):4138–4148. doi:10.1245/s10434-015-4516-1
11. Wang X, Chai X, Zhang J, Tang R, Chen Q. Nomograms established for predicting microvascular invasion and early recurrence in patients with small hepatocellular carcinoma. BMC Cancer. 2024;24(1):929. doi:10.1186/s12885-024-12655-2
12. Abdelhamed W, El-Kassas M. Hepatocellular carcinoma recurrence: predictors and management. Liver Res. 2023;7(4):321–332. doi:10.1016/j.livres.2023.11.004
13. Suner A, Carr BI, Akkiz H, et al. Inflammatory markers C-reactive protein and PLR in relation to HCC characteristics. J Transl Sci. 2019;5(3):
14. Wong L, Bozhilov K, Hernandez B, et al. Underlying liver disease and advanced stage liver cancer are associated with elevated neutrophil-lymphocyte ratio. Clin Mol Hepatol. 2019;25(3):305–316. doi:10.3350/cmh.2019.0004
15. Zarlashat Y, Tayyeba A, Hussain S. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios in hepatocellular carcinoma: from inflammation to clinical applications. Cancer Plus. 2024;6(4):5758. doi:10.36922/cp.5758
16. Lorente L. Circulating biomarkers predictive of mortality in patients undergoing liver transplantation for hepatocellular carcinoma. GIT. 2023;1. doi:10.54844/git.2023.369.
17. Xie H, Ruan G, Wei L, et al. A novel inflammation-nutrition biomarker score for predicting prognosis of patients with cancer: results from a multicenter study. BMC Cancer. 2022;22(1):1311. doi:10.1186/s12885-022-10399-5
18. Zhang L, Chen S, Wang W, Liang Y, Wang Y. Inflammatory and nutritional scoring system for predicting prognosis in patients with newly diagnosed multiple myeloma. J Inflamm Res. 2023;16:7–17. doi:10.2147/JIR.S390279
19. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of primary liver cancer (2022 Edition). Liver Cancer. 2023;12(5):405–444. doi:10.1159/000530495
20. Zhang J, Wang Z, Wu Q, Liu J, Zeng J, Zeng J. Nomogram for predicting early recurrence of hepatocellular carcinoma with narrow resection margin. Sci Rep. 2024;14(1):28103. doi:10.1038/s41598-024-79760-x
21. Norman JS, Li PJ, Kotwani P, Shui AM, Yao F, Mehta N. AFP-L3 and DCP strongly predict early hepatocellular carcinoma recurrence after liver transplantation. J Hepatol. 2023;79(6):1469–1477. doi:10.1016/j.jhep.2023.08.020
22. Feng H, Li B, Li Z, Wei Q, Ren L. PIVKA-II serves as a potential biomarker that complements AFP for the diagnosis of hepatocellular carcinoma. BMC Cancer. 2021;21(1):401. doi:10.1186/s12885-021-08138-3
23. Yao LQ, Chen ZL, Feng ZH, et al. Clinical features of recurrence after hepatic resection for early-stage hepatocellular carcinoma and long-term survival outcomes of patients with recurrence: a multi-institutional analysis. Ann Surg Oncol. 2022;29:4291–4303. doi:10.1245/s10434-022-11454-y
24. National Health Commission of the People’s Republic of China Department of Medical Administration. Guidelines for the diagnosis and treatment of primary liver cancer (2024 edition) [J/OL]. Chin Arch Gen Surg. 2024;18(06):385–410.
25. Liu R, Wu S, Yu HY, et al. Prediction model for hepatocellular carcinoma recurrence after hepatectomy: machine learning-based development and interpretation study. Heliyon. 2023;9(11):e22458. doi:10.1016/j.heliyon.2023.e22458
26. Gao RQ, Li K, Sun JH, et al. Establishment and validation of a preoperative nomogram model for predicting the risk of hepatocellular carcinoma with microvascular invasion. Zhonghua Wai Ke Za Zhi. 2023;61(1):41–47. doi:10.3760/cma.j.cn112139-20220713-00311
27. Kuang DM, Zhao Q, Wu Y, et al. Peritumoral neutrophils link inflammatory response to disease progression by fostering angiogenesis in hepatocellular carcinoma. J Hepatol. 2011;54(5):948–955. doi:10.1016/j.jhep.2010.08.041
28. Zhou SL, Zhou ZJ, Hu ZQ, et al. Tumor-associated neutrophils recruit macrophages and T-regulatory cells to promote progression of hepatocellular carcinoma and resistance to sorafenib. Gastroenterology. 2016;150(7):1646–1658.e17. doi:10.1053/j.gastro.2016.02.040
29. Zhao R, Liang Z, Chen K, Zhu X. Nomogram based on inflammatory biomarkers and nutritional indicators for predicting overall survival in locoregionally advanced nasopharyngeal carcinoma. J Inflamm Res. 2022;15:2971–2981. doi:10.2147/JIR.S366299
30. Wang D, Hu X, Xiao L, et al. Prognostic nutritional index and systemic immune-inflammation index predict the prognosis of patients with HCC. J Gastrointest Surg. 2021;25(2):421–427. doi:10.1007/s11605-019-04492-7
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predicting the Risk of Unplanned Readmission at 30 Days After PCI: Development and Validation of a New Predictive Nomogram
Xu W, Tu H, Xiong X, Peng Y, Cheng T
Clinical Interventions in Aging 2022, 17:1013-1023
Published Date: 5 July 2022
Development and Validation of a Nomogram for Predicting 28-Day Mortality on Admission in Elderly Patients with Severe Community-Acquired Pneumonia
Song Y, Wang X, Lang K, Wei T, Luo J, Song Y, Yang D
Journal of Inflammation Research 2022, 15:4149-4158
Published Date: 21 July 2022
Development and Validation of a Prediction Model for Chronic Post-Surgical Pain After Thoracic Surgery in Elderly Patients: A Retrospective Cohort Study
Wu XD, Zeng FF, Yu XX, Yang PP, Wu JP, Xv P, Wang HT, Pei YM
Journal of Pain Research 2022, 15:3079-3091
Published Date: 29 September 2022
An Easy-to-Use Nomogram Based on SII and SIRI to Predict in-Hospital Mortality Risk in Elderly Patients with Acute Myocardial Infarction
Chen Y, Xie K, Han Y, Xu Q, Zhao X
Journal of Inflammation Research 2023, 16:4061-4071
Published Date: 13 September 2023
Risk Factors for Granulomatous Mastitis and Establishment and Validation of a Clinical Prediction Model (Nomogram)
Zeng Y, Zhang D, Fu N, Zhao W, Huang Q, Cui J, Chen Y, Liu Z, Zhang X, Zhang S, Mansoor KM
Risk Management and Healthcare Policy 2023, 16:2209-2222
Published Date: 20 October 2023