Back to Journals » Journal of Pain Research » Volume 18
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Authors Yap EN ![]() , Wei J, Darling C, Linehan E, Behrends M, Ng KP
, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Received 17 May 2025
Accepted for publication 14 August 2025
Published 16 September 2025 Volume 2025:18 Pages 4775—4785
DOI https://doi.org/10.2147/JPR.S538581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Edward N Yap,1,2 Julia Wei,3 Curtis Darling,4 Elizabeth Linehan,5 Matthias Behrends,2 Kevin P Ng6,7
1Department of Anesthesia, The Permanente Medical Group, Kaiser Permanente South San Francisco, South San Francisco, CA, USA; 2Department of Anesthesia and Perioperative Care, University of California San Francisco, San Francisco, CA, USA; 3Division of Research, Kaiser Permanente Northern California, Oakland, CA, USA; 4Department of Anesthesia, The Permanente Medical Group, Kaiser Permanente Santa Clara, Santa Clara, CA, USA; 5Department of General Surgery, Division of Breast Surgical Oncology, the Permanente Medical Group, Kaiser Permanente San Francisco, San Francisco, CA, USA; 6Department of Anesthesia, The Permanente Medical Group, Kaiser Permanente Walnut Creek, Walnut Creek, CA, USA; 7Department of Anesthesiology & Perioperative Medicine, Drexel University College of Medicine, Philadelphia, PA, USA
Correspondence: Edward N Yap, Department of Anesthesia, The Permanente Medical Group, Kaiser Permanente South San Francisco, 1200 El Camino Real, South San Francisco, CA, 94080, USA, Tel +1-415-650-6750, Email [email protected]
Background: Mastectomy patients require effective acute postoperative pain management. Regional anesthesia techniques such as fascial plane blocks are important pain treatment modalities to address pain control. This study compared the effects of the erector spinae plane (ESP) block versus the pectoralis nerve (PECS) block in providing postoperative analgesia for mastectomy patients.
Methods: This retrospective study included 517 breast cancer patients undergoing mastectomy from 2017 to 2020, with 428 receiving a PECS block and 89 an ESP block. The primary outcome examined was total opioid use during hospital stay measured in morphine milligram equivalents (MME). Secondary outcomes included length of hospital stay, post-anesthesia care unit (PACU) pain scores, PACU postoperative nausea and vomiting (PONV), 30-day readmission rates, and development of postmastectomy pain within six months of surgery.
Results: No significant difference in median total opioid use between the ESP (53 MME (IQR: 38– 80 MME)) and PECS (60 MME (IQR: 30– 82.5 MME)) groups. Multivariable analysis confirmed no difference in total opioid consumption. There was no significant difference between the two groups in PACU average and maximum pain scores, PACU PONV, hospital length of stay, 30-day hospital readmission, and development of postmastectomy pain within six months of surgery.
Conclusion: Compared to the PECS block, the ESP block demonstrated no significant difference in acute pain outcomes and recovery in patients undergoing mastectomy for breast cancer, with similar hospital discharge times and long-term outcomes.
Keywords: breast cancer, mastectomy, erector spinae plane block, pectoralis nerve block, postoperative analgesia, regional anesthesia, opioid consumption
Introduction
Breast cancer is one of the leading cancer diagnoses for women in the United States, affecting more than 287,000 patients a year. Surgery is the mainstay treatment in breast cancer, and mastectomy is a common option for surgical therapy.1 Mastectomy causes significant acute postoperative pain, which can lead to prolonged recovery, increased risk of chronic post-mastectomy pain, and development of chronic opioid dependence.2–5 Higher levels of acute postoperative pain has been associated with increased risk of persistent post-surgical pain. Therefore, aggressive treatment of acute postoperative pain is important in the prevention of persistent post-surgical pain, which can affect over a third of mastectomy patients.2,6–8 An anesthetic plan utilizing multimodal analgesia that includes regional anesthesia has been shown to decrease severe acute postoperative pain associated with mastectomy. Additionally, regional anesthesia techniques have shown to reduce the incidence of persistent post-surgical pain after breast cancer surgery, highlighting their importance in the anesthetic management of mastectomies.5,9–13
Fascial plane blocks have increasingly been utilized for mastectomy, replacing other established regional anesthetic techniques such as paravertebral blocks and thoracic epidurals. The pectoralis nerve (PECS) block, a type of fascial plane block, has been shown to have comparable postoperative analgesic effects to paravertebral blocks in breast surgery.14 The erector spinae plane (ESP) block is a recently introduced fascial plane technique that was initially described to treat chronic thoracic neuropathic pain and postoperative pain from video-assisted thoracic surgery.15 It has gained popularity due to its ease of application, safety, and potential for effective pain management in comparison to no block for breast and thoracic surgery.16,17 Furthermore, the ESP block is performed away from the surgical site and associated lymph nodes, potentially making it a better option than the PECS block.
Comparative studies of the ESP block versus the PECS block or paravertebral block in breast surgery have shown mixed results, with some evidence suggesting the ESP block may be inferior to the PECS block but comparable to the paravertebral block.18 Some studies have reported that patients who received ESP blocks have higher postoperative pain scores and postoperative opioid consumption compared to patients receiving a PECS block or a paravertebral block. The PECS block, in particular, may offer superior analgesia due to its more targeted coverage of the pectoral nerves and anterior chest wall.19–22 Conversely, other studies find no significant differences in pain scores or postoperative opioid consumption between these techniques in breast surgery.23,24 Furthermore, there is a lack of studies examining discharge readiness dependent on the type of regional anesthetic technique used. Therefore, we conducted a multicentered retrospective study comparing acute pain outcomes and hospital discharge times between the ESP block and the PECS block in patients undergoing mastectomy for breast cancer. We hypothesized that patients receiving a PECS block would experience significantly improved acute pain outcomes and discharge success compared to those receiving an ESP block.
Methods
This article was prepared according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.25
Study Design
After obtaining Institutional Review Board approval at the Kaiser Permanente Northern California Region (Study# 1818117–2), we performed a retrospective cohort study comparing patients who received an ESP block to those who received a PECS block undergoing mastectomy without reconstruction (simple mastectomy, modified radical, or nipple sparing mastectomy without reconstruction) for breast cancer at Kaiser Permanente Northern California hospitals. The requirement for informed consent was waived by the IRB due to the retrospective nature of the study, minimal risk to participants, and use of data collected as part of routine clinical care. All data were handled in accordance with institutional policies for maintaining patient confidentiality and privacy, and access was limited to authorized study personnel. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The primary outcome examined was total opioid usage during the patient’s hospital stay measured in morphine milligram equivalents (MME). A multivariable analysis examining post anesthesia care unit (PACU) opioid usage was also performed to examine individual characteristic effects. Secondary outcomes examined included PACU pain scores, incidence of PACU postoperative nausea and vomiting (PONV), surgical duration, length of PACU stay, length of hospital stay, incidence of 30-day hospital readmission, and new diagnosis of postmastectomy pain within six months after date of surgery.
Setting
Kaiser Permanente Northern California is a multicentered integrated health care medical system with 21 medical centers in Northern California that utilize the same electronic medical record (EMR, EpicTM, Verona, WI, USA). All patients undergoing surgery within the hospital system receive a preoperative evaluation prior to surgery to identify and optimize modifiable risk factors. The healthcare system also utilizes an enhanced recovery pathway for all mastectomies that helps standardize education, pain control, nutrition, and mobility.26 Regional anesthesia is encouraged within the enhanced recovery pathway and each anesthesia department and anesthesiologist determines the type of regional anesthesia technique used based on patient clinical factors, clinician experience, and hospital workflow. A standardized PACU order set was used at each hospital for patients to receive analgesic and opioid medications on an as needed basis dependent on patient pain scores.
Study Population
We identified patients 18 years of age and older with a diagnosis of breast cancer using International Classification of Diseases, 10th Revision (ICD-10) codes (C50, D05) who underwent mastectomy at one of our 21 medical centers between January 1st, 2017 and December 31st, 2020. Our definition of mastectomy included simple mastectomy (to include skin sparing and total mastectomy), nipple sparing mastectomy, and modified radical mastectomy. We included patients who received both unilateral and bilateral mastectomies. Axillary lymph node surgery, either as a sentinel lymph node biopsy or as an axillary lymph node dissection, was also recorded. We excluded patients who joined the health system less than one year prior to surgery date to ensure complete capture of patient preoperative data, concurrent surgery at the time of surgery (e.g. breast reconstruction, gynecologic surgery), emergent surgery, and patients who received two types of nerve block or surgeon local anesthetic infiltration on one surgical side. We counted the PECS block as one type of nerve block in our study.
Exposure Variable
The exposure examined was the type of nerve block received by a patient, either an ESP block or a PECS block, which was performed preoperatively and obtained through perioperative records. The ESP block was defined as a block performed in the upper thoracic level (T1-6) and with the placement of local anesthetic between the plane deep to the erector spinae muscles and superficial to the transverse process. PECS blocks were performed as PECS II blocks, also described as combined pectoserratus plane and interpectoral plane blocks, which includes placement of local anesthetic between the pectoralis major and minor muscles as well as between the pectoralis minor muscle and the serratus anterior muscle.27 The performance of the blocks and technique were chart reviewed and adjudicated by clinician chart review. The type of local anesthetic used varied by hospital site and was not included as an exposure variable. However, most centers used long-acting local anesthetic, such as bupivacaine or ropivacaine with or without epinephrine, while other injectate adjuncts were not typically used in our setting. Patients who received liposomal bupivacaine were excluded.
Outcome Variables
Medications administered throughout the perioperative period were collected through the Medication Administration Record. Opioids administered were reported as MME. Pain scores were reported using the Numeric Rating Scale, a scale from 0 to 10, 0 representing no pain, 1–2 representing mild pain, 3–6 representing moderate pain, and 7–10 representing severe pain. We reported both average pain score and maximum pain score during the PACU stay for each patient. PONV was identified through the nursing flowsheet and was recorded using a postanesthetic scoring system and rated as none/minimal, moderate, or severe. We categorized patients as either having PONV (moderate or severe) or no PONV (none/minimal). Surgery duration was measured as the time from procedure start to procedure end. PACU length of stay was measured as the time the patient arrived in the PACU to the time the patient met discharge criteria from the PACU. Hospital length of stay was defined as the time of admission to time of discharge.28 Readmission was defined as any hospital admission occurring within 30-days following surgery, regardless of the cause. A new diagnosis of postmastectomy pain within 6 months after surgery was captured by ICD-10 code (G89.28) and adjudicated by clinician chart review.
Statistical Analysis
Demographic and clinical characteristics for the cohort were summarized descriptively using frequencies, proportions, means, and standard deviations. Fisher’s exact tests and Pearson’s chi-square test were used to determine differences between patients receiving the ESP block compared to patients receiving the PECS block for categorical demographic and clinical variables as well as secondary outcomes such as PACU PONV, 30-day hospital readmission, and postmastectomy pain. The Student’s t-test was used to assess difference in age between the ESP and PECS group. Wilcoxon rank sum test was used to assess for differences between ESP and PECS groups in non-normally distributed continuous outcomes such as opioid usage, pain scores, surgical duration, and length of PACU and hospital stay. Multivariable linear regression was performed to assess if the type of block was associated with total opioid usage during hospital stay adjusted for age, race, ethnicity, gender, BMI, ASA score, surgical duration, surgery type, axillary lymph node dissection, chronic pain, and perioperative non-opioid analgesic usage. Adjusted beta coefficients and their 95% confidence intervals were reported. To further reduce residual confounding, we conducted a sensitivity analysis using inverse probability of treatment weighting (IPTW). IPTW was derived using a logistic regression in which the outcome was the type of nerve block received (ESP vs PECS), with ESP defined as the treated group. These weights were then applied to the multivariable regression model. There was no missingness for any of the variables. A p-value of <0.05 was statistically significant. All data management and statistical analyses were performed in SAS 9.4.
Results
Patient and Clinical Characteristics
We identified 7518 patients who underwent total mastectomy from the start of 2017 through the end of 2020. We excluded 6684 of patients who met exclusion criteria such as under 18 years of age, concurrent surgery at the time of mastectomy, emergency surgery, patients with less than 1 year of KPNC membership before surgery date, patients who received two different types of nerve block, and patients who received surgeon-performed local infiltration. Of the 517 patients included in the study, 428 patients received a PECS block and 89 received an ESP block (Figure 1). Baseline demographics and clinical characteristics of the primary analysis cohort are presented in Table 1.
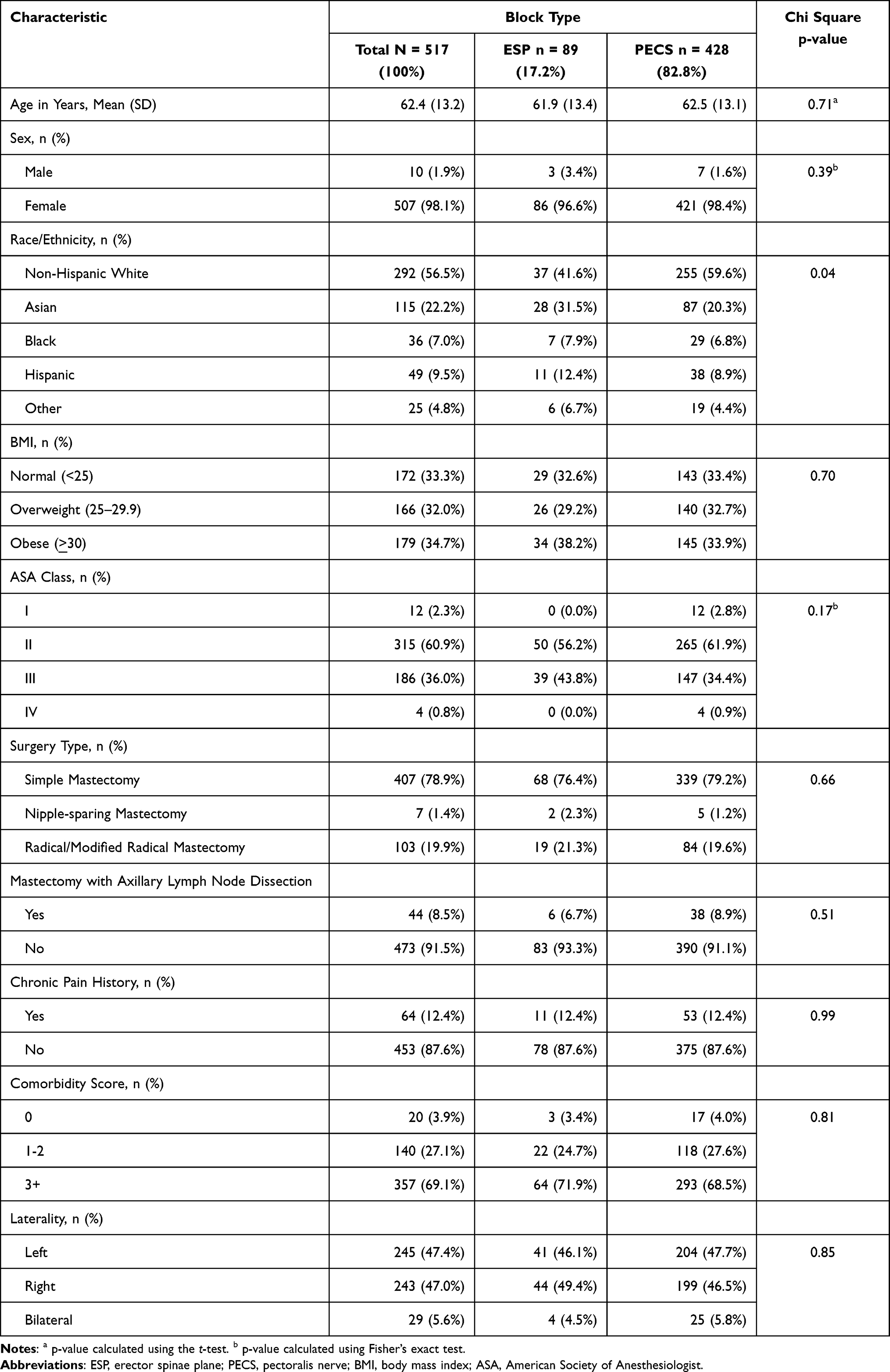 |
Table 1 Baseline Demographic and Clinical Characteristics of Mastectomy Surgery Patients by Block Type (N = 517) |
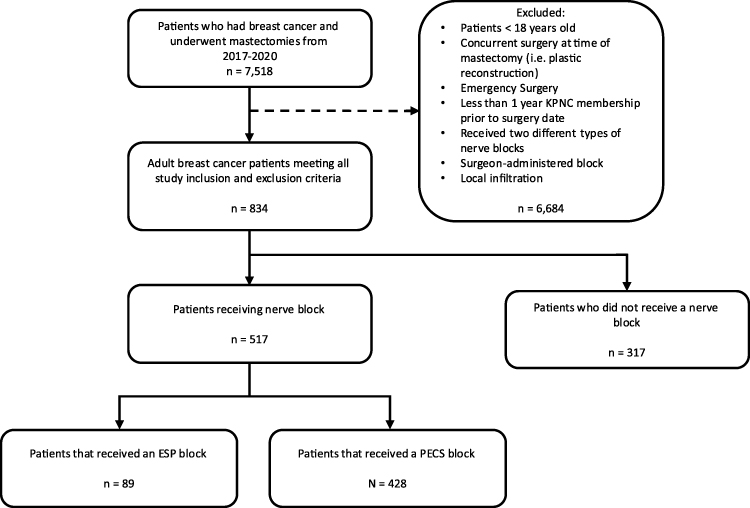 |
Figure 1 Flowchart of Study Cohort. |
Patient characteristics were very similar between the ESP group and the PECS group. There was no significant difference between average age between the ESP and PECS groups (61.9 (SD 13.4) vs and 62.5 (SD 13.1), p = 0.71). Similarly, there were no significant differences in sex, BMI, ASA classification, surgery type, chronic pain history, comorbidity score, or laterality between the ESP and PECS groups. Race/ethnicity was associated with type of block received (p = 0.04). A higher percentage of patients receiving a PECS block were non-Hispanic White compared to those receiving an ESP block (59.6% vs 41.6%). Conversely, a higher percentage of patients that received an ESP block were Asian, Black, and Hispanic compared to patients that received a PECS block (31.5% vs 20.3%, 7.9% vs 6.8%, 12.4% vs 8.9%, respectively).
Primary Outcome – Total Opioid Administration
Patients who received the ESP block had a median of 53 MME (IQR: 38–80 MME) for total in hospital opioid usage compared to 60 MME (IQR: 30–82.5 MME) for patients who received a PECS block (Table 2). There was no significant difference between the ESP block vs PECS block patients in bivariate (p = 0.63) or multivariable analysis for total opioid usage during hospital stay (p = 0.26, Table 3). In a sensitivity analysis using IPTW, the association remained non-significant (p = 0.87, Supplementary Table 1). Multivariable analysis using linear regression demonstrated longer surgical duration, obesity, corticosteroid use, and history of chronic pain were associated with higher in hospital opioid use while Asian and Black race/ethnicity and age were associated with lower in hospital opioid use (Table 3).
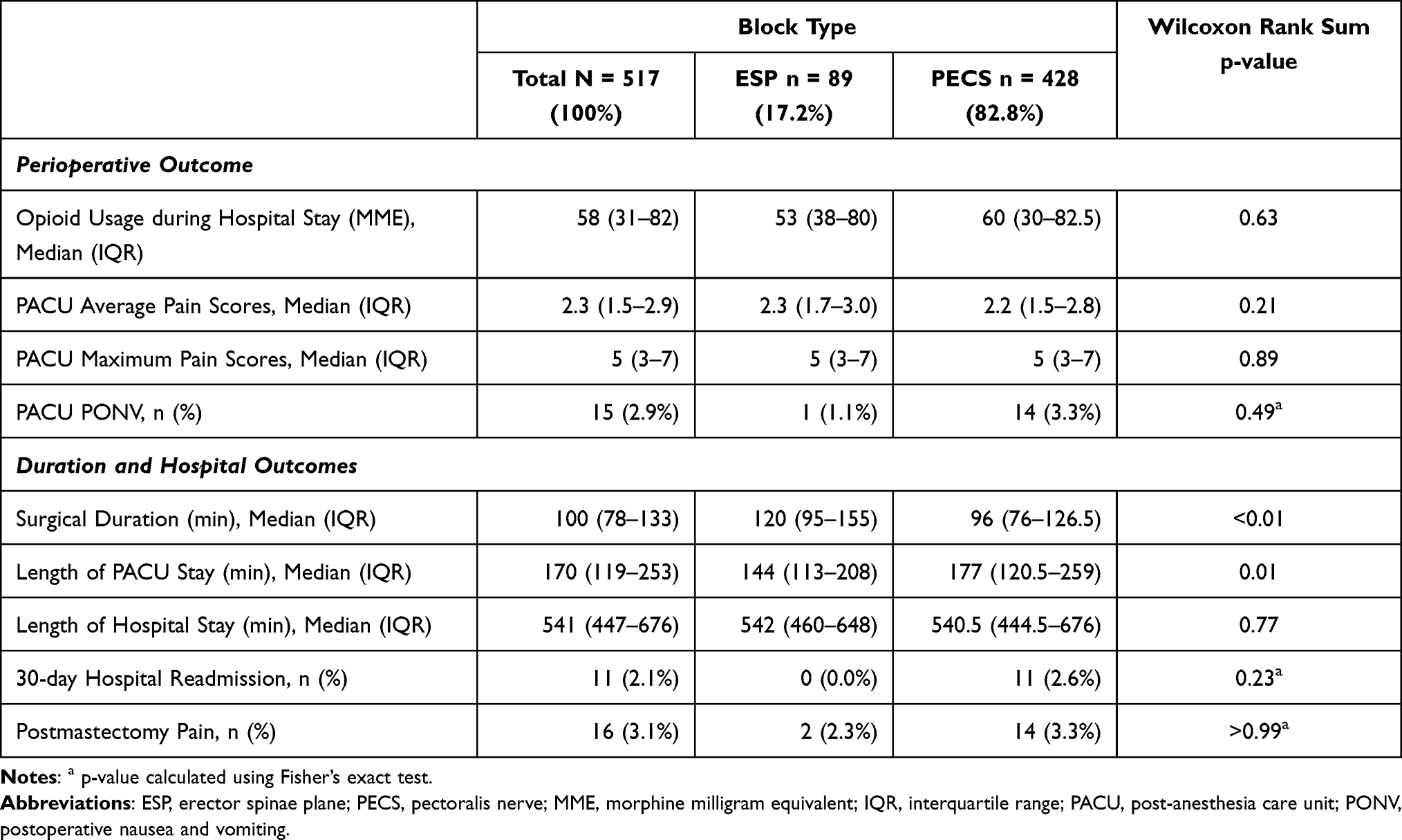 |
Table 2 Perioperative and Hospital Outcomes of Mastectomy Surgery Patients with ESP vs PECS Block (N = 517) |
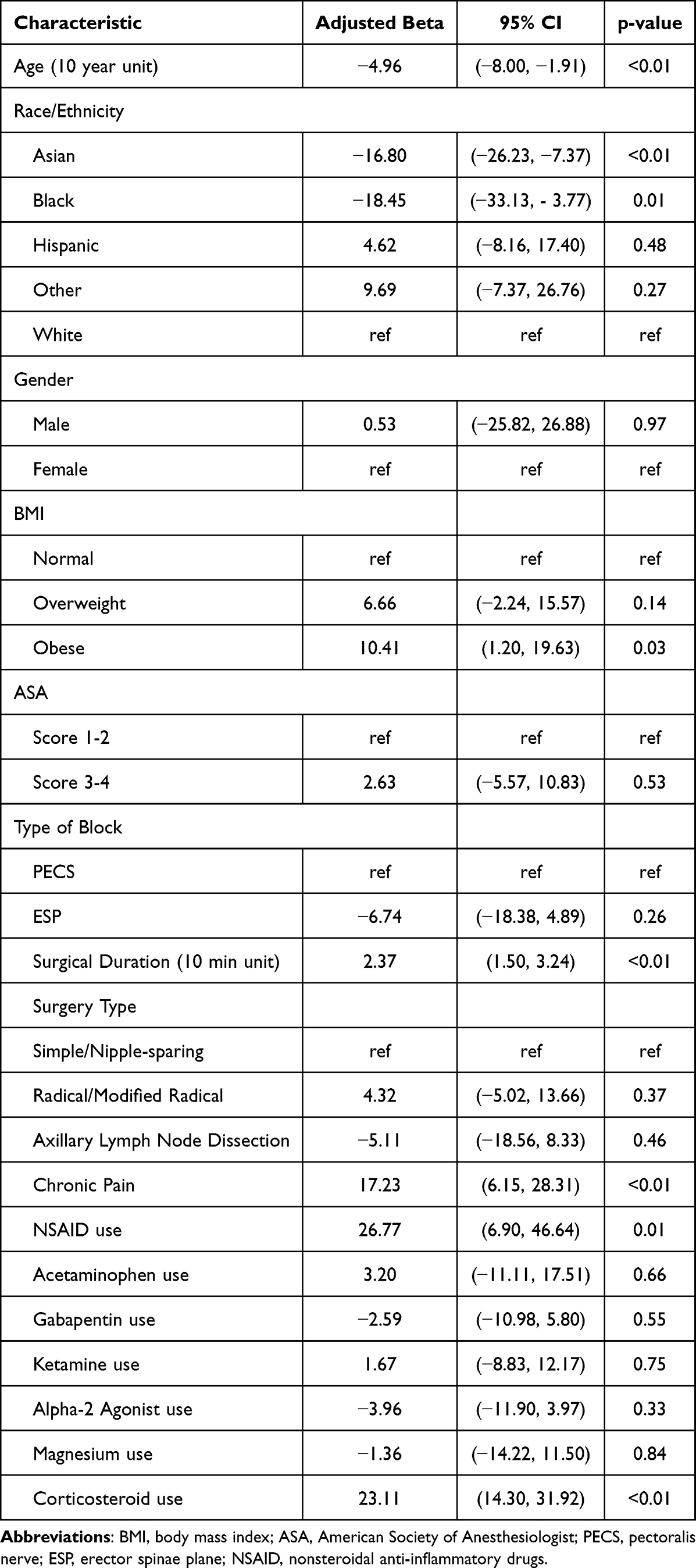 |
Table 3 Adjusted Betas of Opioid Usage During Hospital Stay (N = 517) |
Secondary Outcomes
The ESP block group was noted to have a significant longer surgical duration compared to the PECS block group [Median (IQR) 120 (95–155) min vs 96 (76–126.5) min, p < 0.01]. The ESP block group had lower PACU length of stay [Median (IQR) 144 (113–208) min vs 177 (120.5–259) min, p = 0.01]. There was no significant difference between the two groups in PACU average and maximum pain scores, PACU PONV, hospital length of stay, 30-day all cause hospital readmission, and development of postmastectomy pain within six months of surgery (Table 2). We found that patients in the ESP block group more frequently received gabapentinoids, ketamine, magnesium sulfate, and corticosteroids (Table 4).
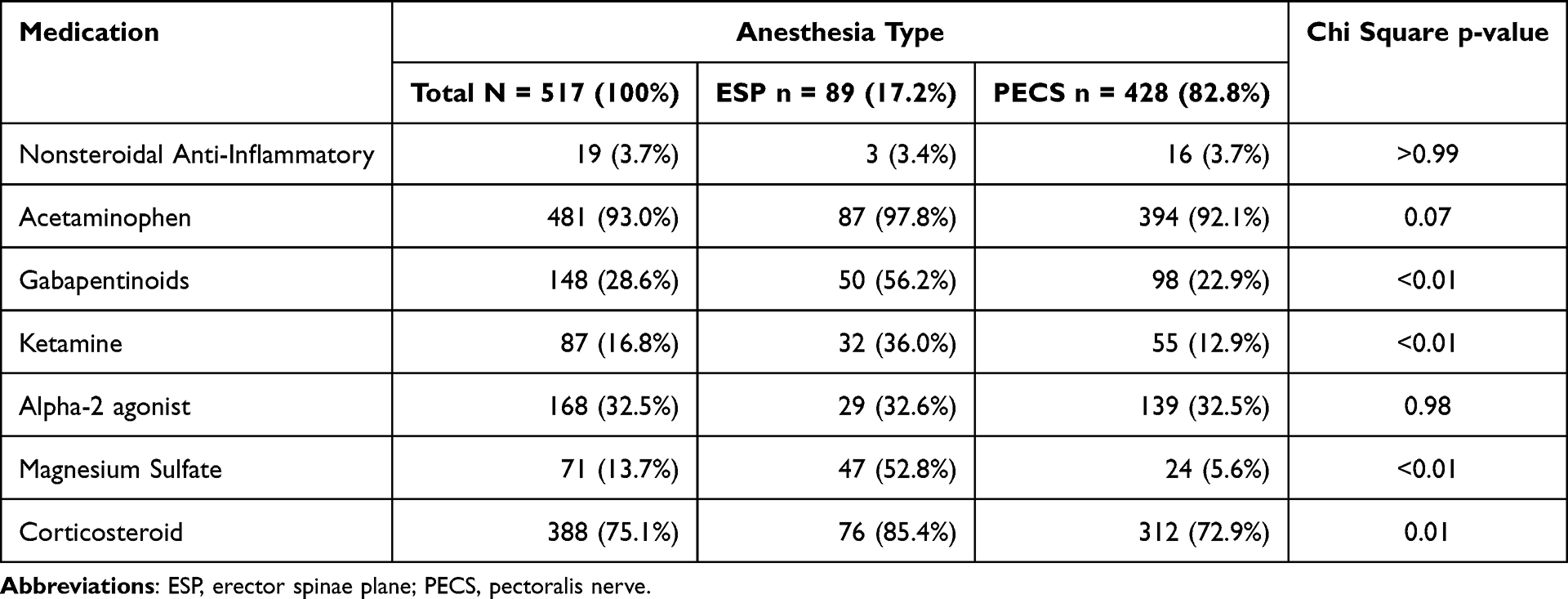 |
Table 4 Nonopioid Adjuncts Usage Throughout Hospital Stay (n = 517) |
Discussion
This study aimed to address the limited understanding of the differences in opioid utilization and hospital length of stay between the ESP block and the PECS block in patients undergoing mastectomy for breast cancer. We investigated 517 patients who underwent mastectomy for breast cancer surgery from 2017 to 2020 across a multicenter hospital system. Contrary to our hypothesis, we found no significant differences in total amount of opioid usage during hospital stay between patients that received an ESP block compared to patients that received a PECS block. Multivariable analysis (with and without IPTW) adjusting for demographic, clinical, and surgical characteristics, demonstrated no significant differences in total hospital opioid consumption. Despite longer surgical duration in the ESP block group, patients in this group had shorter PACU length of stay, though no difference was observed in overall hospital length of stay. Additionally, there were no significant differences in PACU average and maximum pain scores, PACU PONV, hospital readmission rates within 30-days after surgery, or the development of post mastectomy pain within six months of surgery. Notably, the ESP block group had a higher administration rate of non-opioid analgesic adjuncts, which may have contributed to these findings.
Our study was also motivated by the increased utilization of the ESP block in patients undergoing mastectomy in our healthcare system despite lacking evidence for its superiority in the current literature (Supplementary Table 2).29 A recent meta-analysis examining patients undergoing breast surgery, most of the surgeries being modified radical mastectomy, reviewed the efficacy of the ESP block compared to the PECS block. Notably, our patient population differs from this meta-analysis, as modified radical mastectomy is fairly rare in our health system. Compared to the PECS block, the ESP block group required significantly higher amounts of opioids in the first 24-hours after surgery and had higher postoperative pain scores at the 0–2 hour, 6 hour, and 12 hour time points after surgery.18 In contrast, our study found no significant differences in total opioid utilization between the ESP block and the PECS block. There were also no significant differences in the PACU average and maximum pain scores between the two groups. Prior studies describe multiple reasons thought to provide postoperative analgesic advantage of the PECS block compared to the ESP block. These include motor blockade of the pectoral muscles that may relieve postoperative muscle spasm, intercostobrachial nerve blockade that may aid with axillary pain, and improved dermatome spread with the PECS block compared to the ESP block.21,30 However, the likely explanation in the differences seen in our study results compared to the meta-analysis is that our patient population included a minority of patients undergoing modified radical mastectomy. Our patient population also had a perioperative multimodal analgesic approach that allowed the use of different non-opioid analgesics at the clinician’s discretion, whereas the three randomized controlled trials examined in the meta-analysis had structured protocols for perioperative non-opioid analgesic administration. Thus, if the PECS block did confer postoperative analgesic benefits greater than the ESP block, the benefits were too marginal to see any statistical differences in our study.
The comparative analysis of the ESP and PECS blocks in our study has important implications for pain management strategies for mastectomy patients. Our research also underscores the importance of large-sample retrospective studies in providing useful information when prospective studies yield inconsistent results. Our findings challenge the assumption of clear superiority of one block technique over the other, instead revealing the complexity of perioperative pain management. The similarity in opioid utilization, pain scores, length of stay, and clinical outcomes suggest that physicians have more flexibility in regional anesthetic technique selection. This flexibility, along with a patient-centered approach, emphasizes the value of shared decision making. It also supports a multimodal analgesia strategy that goes beyond a specific block, allowing physicians to tailor a comprehensive pain management protocol based on variability in surgical techniques, patient characteristics, and institutional practices.31 This is particularly crucial for patients with higher pain and opioid needs, such as those who are younger, where surgical duration will be longer, and those with a history of chronic pain, as demonstrated in our study. Furthermore, these findings reinforce that regional anesthesia is an important component in a comprehensive multimodal analgesic approach, which may have a greater impact on optimizing postoperative pain outcomes than block choice alone.
There are several limitations to our study to be noted. Most patients in our study were discharged within 24 hours after surgery and postoperative pain scores and opioid consumption was not collected routinely following discharge from the hospital, therefore comparison between the two different blocks is limited to this timeframe. The retrospective research design faces limitations from various biases or data recording errors that might introduce confounding factors into the study results. Factors such as surgeon preference of length of observation postoperatively, and the type and volume of local anesthetic and adjuncts were not examined, which may have affected the findings of our study. An important limitation of this study is the lack of consistent documentation confirming block success, which may have introduced variability in analgesic outcomes. Lastly, surgeon and anesthesiologist experience were not adjusted for in this study.
Conclusion
Our study investigating patients undergoing mastectomy for breast cancer demonstrated no differences in postoperative analgesia usage between the ESP block and the PECS block. Both block techniques appear to facilitate timely same-day discharge, offering surgeons and anesthesiologists flexibility in regional anesthetic approach for mastectomy patients.
Abbreviations
ESP, Erector Spinae Plane; PECS, Pectoralis Nerve; MME, Morphine Milligram Equivalents; PACU, Post-Anesthesia Care Unit; PONV, Postoperative Nausea and Vomiting; EMR, Electronic Medical Record; ICD-10, International Classification of Diseases, 10th Revision; IPTW, inverse probability of treatment weighting.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical reasons. However, they are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Kaiser Permanente Northern California Institutional Review Board (00001045) and the requirement for written informed consent was waived.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Kaiser Permanente Northern California Community Health Grant.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Cancer Society I. American cancer society. Breast cancer facts & figures 2022-2024. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/2022-2024-breast-cancer-fact-figures-acs.pdf.
2. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
3. Kairaluoma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg. 2006;103(3):703–708. doi:10.1213/01.ane.0000230603.92574.4e
4. Tait RC, Zoberi K, Ferguson M, et al. Persistent post-mastectomy pain: risk factors and current approaches to treatment. J Pain. 2018;19(12):1367–1383. doi:10.1016/j.jpain.2018.06.002
5. Weinstein EJ, Levene JL, Cohen MS, et al. Local anaesthetics and regional anaesthesia versus conventional analgesia for preventing persistent postoperative pain in adults and children. Cochrane Database Syst Rev. 2018;6(6):CD007105. doi:10.1002/14651858.CD007105.pub4
6. Wang L, Cohen JC, Devasenapathy N, et al. Prevalence and intensity of persistent post-surgical pain following breast cancer surgery: a systematic review and meta-analysis of observational studies. Br J Anaesth. 2020;125(3):346–357. doi:10.1016/j.bja.2020.04.088
7. Richebe P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129(3):590–607. doi:10.1097/ALN.0000000000002238
8. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–2298. doi:10.2147/JPR.S144066
9. Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105(6):842–852. doi:10.1093/bja/aeq265
10. Lovett-Carter D, Kendall MC, McCormick ZL, Suh EI, Cohen AD, De Oliveira GS. Pectoral nerve blocks and postoperative pain outcomes after mastectomy: a meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2019;44(10):923–928. doi:10.1136/rapm-2019-100658
11. Kairaluoma PM, Bachmann MS, Korpinen AK, Rosenberg PH, Pere PJ. Single-injection paravertebral block before general anesthesia enhances analgesia after breast cancer surgery with and without associated lymph node biopsy. Anesth Analg. 2004;99(6):1837–1843. doi:10.1213/01.ANE.0000136775.15566.87
12. Blanco R. The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia. 2011;66(9):847–848. doi:10.1111/j.1365-2044.2011.06838.x
13. Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59(9):470–475. doi:10.1016/j.redar.2012.07.003
14. Jin Z, Durrands T, Li R, Gan TJ, Lin J. Pectoral block versus paravertebral block: a systematic review, meta-analysis and trial sequential analysis. Reg Anesth Pain Med. 2020;45(9):727–732. doi:10.1136/rapm-2020-101512
15. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
16. Huang W, Wang W, Xie W, Chen Z, Liu Y. Erector spinae plane block for postoperative analgesia in breast and thoracic surgery: a systematic review and meta-analysis. J Clin Anesth. 2020;66:109900. doi:10.1016/j.jclinane.2020.109900
17. Pawa A, King C, Thang C, White L. Erector spinae plane block: the ultimate ‘plan A’ block? Br J Anaesth. 2023;130(5):497–502. doi:10.1016/j.bja.2023.01.012
18. Leong RW, Tan ESJ, Wong SN, Tan KH, Liu CW. Efficacy of erector spinae plane block for analgesia in breast surgery: a systematic review and meta-analysis. Anaesthesia. 2021;76(3):404–413. doi:10.1111/anae.15164
19. Sinha C, Kumar A, Kumar A, Prasad C, Singh PK, Priya D. Pectoral nerve versus erector spinae block for breast surgeries: a randomised controlled trial. Indian J Anaesth. 2019;63(8):617–622. doi:10.4103/ija.IJA_163_19
20. Swisher MW, Wallace AM, Sztain JF, et al. Erector spinae plane versus paravertebral nerve blocks for postoperative analgesia after breast surgery: a randomized clinical trial. Reg Anesth Pain Med. 2020;45(4):260–266. doi:10.1136/rapm-2019-101013
21. Altiparmak B, Korkmaz Toker M, Uysal AI, Turan M, Gumus Demirbilek S. Comparison of the effects of modified pectoral nerve block and erector spinae plane block on postoperative opioid consumption and pain scores of patients after radical mastectomy surgery: a prospective, randomized, controlled trial. J Clin Anesth. 2019;54:61–65. doi:10.1016/j.jclinane.2018.10.040
22. Gad M, Abdelwahab K, Abdallah A, Abdelkhalek M, Abdelaziz M. Ultrasound-guided erector spinae plane block compared to modified pectoral plane block for modified radical mastectomy operations. Anesth Essays Res. 2019;13(2):334–339. doi:10.4103/aer.AER_77_19
23. Gurkan Y, Aksu C, Kus A, Yorukoglu UH. Erector spinae plane block and thoracic paravertebral block for breast surgery compared to IV-morphine: a randomized controlled trial. J Clin Anesth. 2020;59:84–88. doi:10.1016/j.jclinane.2019.06.036
24. El Ghamry MR, Amer AF. Role of erector spinae plane block versus paravertebral block in pain control after modified radical mastectomy. A prospective randomised trial. Indian J Anaesth. 2019;63(12):1008–1014. doi:10.4103/ija.IJA_310_19
25. von Elm E, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
26. Vuong B, Graff-Baker AN, Yanagisawa M, et al. Implementation of a post-mastectomy home recovery program in a large. Integrated Health Care Delivery System. Ann Surg Oncol. 2019;26(10):3178–3184. doi:10.1245/s10434-019-07551-0
27. El-Boghdadly K, Wolmarans M, Stengel AD, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg Anesth Pain Med. 2021;46(7):571–580. doi:10.1136/rapm-2020-102451
28. Yap E, Wei J, Webb C, Ng K, Behrends M. Neuraxial and general anesthesia for outpatient total joint arthroplasty result in similarly low rates of major perioperative complications: a multicentered cohort study. Reg Anesth Pain Med. 2022;47(5):294–300. doi:10.1136/rapm-2021-103189
29. Hussain N, Brull R, Noble J, et al. Statistically significant but clinically unimportant: a systematic review and meta-analysis of the analgesic benefits of erector spinae plane block following breast cancer surgery. Reg Anesth Pain Med. 2021;46(1):3–12. doi:10.1136/rapm-2020-101917
30. Bakeer A, Abdallah NM. Erector spinae plane block versus PECS block type II for breast surgery: a randomized controlled trial. Anesth Pain Med. 2022;12(2):e122917. doi:10.5812/aapm-122917
31. Chiu C, Aleshi P, Esserman LJ, et al. Improved analgesia and reduced post-operative nausea and vomiting after implementation of an enhanced recovery after surgery (ERAS) pathway for total mastectomy. BMC Anesthesiol. 2018;18(1):41. doi:10.1186/s12871-018-0505-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Predictive Effect of the 8th AJCC Pathological Prognostic Staging on the Benefit of Postmastectomy Radiotherapy in N2/N3 Breast Cancer
Yang SP, Zhou P, Lian CL, He ZY, Wu SG
Breast Cancer: Targets and Therapy 2022, 14:133-144
Published Date: 13 May 2022
Case Report: Erector Spinae Block in Perforated Viscus
Rauf J, A M Haji MM
Local and Regional Anesthesia 2023, 16:19-23
Published Date: 16 February 2023
Efficacy and Safety of Erector Spinae Plane Block for Perioperative Pain Management in Lumbar Spinal Surgery: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Fu MY, Hao J, Ye LH, Jiang W, Lv YW, Shen JL, Fu T
Journal of Pain Research 2023, 16:1453-1475
Published Date: 3 May 2023
Utility of Ultrasound-Guided Erector Spinae Plane Blocks for Postoperative Pain Management Following Thoracolumbar Spinal Fusion Surgery
Zelenty WD, Li TY, Okano I, Hughes AP, Sama AA, Soffin EM
Journal of Pain Research 2023, 16:2835-2845
Published Date: 16 August 2023
Comparison of Costotransverse Foramen Block with Thoracic Paravertebral Block and Erector Spinae Plane Block for Patients Undergoing Video-Assisted Thoracoscopic Surgery: A Randomized Controlled Non-Inferiority Trial
Li J, Shao P, Wen H, Ma D, Yang L, He J, Jiang J
Journal of Pain Research 2025, 18:2427-2438
Published Date: 13 May 2025