Back to Journals » Local and Regional Anesthesia » Volume 16
Case Report: Erector Spinae Block in Perforated Viscus
Authors Rauf J ![]() , A M Haji MM
, A M Haji MM ![]()
Received 3 November 2022
Accepted for publication 9 February 2023
Published 16 February 2023 Volume 2023:16 Pages 19—23
DOI https://doi.org/10.2147/LRA.S393913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Stefan Wirz
Jassim Rauf,1 Mohammad Mohsin A M Haji2
1Department of Anesthesiology, ICU & Perioperative Medicine, Hazm Mebaireek General Hospital, Hamad Medical Corporation, Doha, Qatar; 2Department of Anesthesiology, ICU & Perioperative Medicine, Hamad General Hospital, Hamad Medical Corporation, Doha, Qatar
Correspondence: Jassim Rauf, Department of Anesthesiology, ICU & Perioperative Medicine, Hamad General Hospital, Hamad Medical Corporation, P.O.Box 3050, Doha, Qatar, Tel +97433622191, Email [email protected]
Background: Erector spinae plane block (ESPB) a new block described for post-operative analgesia. Since 2016 the block has become a common practice in many institutions globally. Evidence has shown that ESPB is superior to truncal and abdominal wall blocks for many thoracic and abdominal surgeries.
Case Presentation: A 29-year-old male, ASA (American Society of Anesthesiologists) IIE patient presented with acute appendicitis. Patient was scheduled to undergo Laparoscopic Appendicectomy under general anesthesia (GA) with ESPB for post op analgesia. In the operating room after induction of GA patient received an ultrasound (US) guided bilateral ESPB at T10 level of the spinal cord with 20 mls of 0.25% levobupivacaine on each side. Intraoperatively the appendix was found to be normal and there was an incidental finding of perforated superior/first part of duodenum (D1). The duodenum was repaired. Patient remained hemodynamically stable intraoperatively. No intraoperative morphine was required. After uneventful extubation, the patient was transferred to post-operative anesthesia care unit (PACU). Patient reported pain score of zero on a 11-point numerical rating scale (NRS) in PACU. No morphine was required in the next 24 hours on the ward either.
Conclusion: ESPB can provide opioid free analgesia for laparoscopic repair of perforated duodenal ulcer both intra and postoperatively.
Keywords: erector spinae plane block, perforated duodenal ulcer, regional anesthesia, truncal block, levobupivacaine, ESPB
Introduction
Intraoperative analgesia practice has been traditionally achieved by administration of opioids. Regional Anesthesia as part of multimodal analgesia not only reduces intra operative but also post-operative opioid requirements. Also, administration of analgesic medications or performing a regional nerve block prior to surgical stimulus can change central and peripheral nervous system processing of noxious stimuli.1,2
Erector spinae plane block (ESPB) was first described in 2016.3 Since this time, it has gained increased interest and use.4 It has been identified as an effective mode of analgesia for abdominal and thoracic surgeries. While there is still some controversy about its mechanism of action, but most of the literature favours its initially proposed mechanism of action that not only it blocks the nerves in the dorsal horn of the spinal cord, but also spreads to the ventral horn and the paravertebral space (in some instances even epidural space) thus providing both somatic and visceral analgesia. With emerging evidence, the ESPB appears to be more effective than other truncal and abdominal blocks.
In this case report we will look at the analgesic efficacy of ESPB in surgical repair of a perforated viscus.
Case Report
We report a case study of a 29-year-old male ASA (American Society of Anesthesiologists) grade II E, a regular smoker, with a possible diagnosis of acute appendicitis and was scheduled to undergo emergency laparoscopic appendicectomy. The patient weighed 59kg with a body mass index (BMI) of 21kg/m2. He had a past medical history of left thumb extensor tendon repair. Preoperatively patient was on paracetamol 1g 6 hourly (the last dose was 3 hours prior to the surgery) and had received 5 mg of morphine 11 hours before surgery. In the operating theatre pre holding area patient reported a pain score of 7/10 on the numerical rating scale (NRS). A written informed consent for general anesthesia (GA) and an ESPB under GA for post operative pain relief was obtained from the patient.
In the operating theatre the patient was connected to standard monitors. Anesthesia was induced by intravenous (IV) lidocaine (1mg/kg), fentanyl (1.5mcg/kg), propofol (2.5mg/kg) and rocuronium (0.9mg/kg) followed by orotracheal intubation.
After intubation, patient was positioned in the left lateral position. Under full aseptic conditions, using a landmark technique, a line was drawn adjoining the lower edge of the two scapulae in order to mark the spinous process (SP) of the seventh thoracic vertebral body. After placing a 6–13-mHz linear ultrasound (US) probe (Sonosite M-Turbo ultrasound device, Fujifilm, Sonosite, WA, USA), on the T7 SP, the probe was moved laterally till the transverse process (TP) was identified. Thereafter the US probe was moved in the caudad direction till we identified the T10 TP. The TP of the T 10 was then marked with a marker on both sides. Using a parasagittal approach with the US the erector spinae muscle (ESM) was identified. An 80 mm 22 G sonoplex STIM needle, in plane with US probe was inserted from cephalad to caudad direction till the tip of the needle was in contact with the TP just in front of the ESM. At this point the needle was withdrawn 1 mm and 1 mL of local anesthetic (LA) was injected in order to visualize the spread and rise of the ESM. Once confirmed 20mL of 0.25% Levobupivacaine was injected on the right side and then on the left side, with aspiration done every 5 mL to confirm any inadvertent injections. The total duration of the procedure was 11 minutes.
At surgical incision, no change in the patient’s hemodynamic markers was observed. Anesthesia was maintained with sevoflurane at a minimum alveolar concentration of 0.7–1.4 Vol%. Patient’s hemodynamic parameters at different intraoperative time points are shown in Figure 1. Laparoscopically, the surgeons found a normal appendix, but there was some pus seen. On further look around, a a perforation in the superior/First part of the duodenum (D1) was identified and repaired by the surgeons. Intraoperatively, the patient received IV paracetamol 1g, ketorolac 30mg, dexamethasone 8mg, and ondansetron 4 mg.
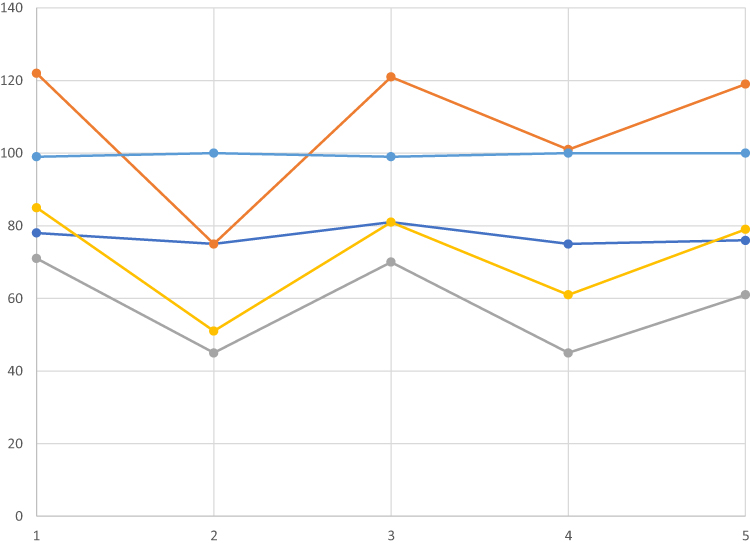 |
Figure 1 The colored lines/dots on the y axis are: Dark Blue Line: Heart Rate, Red Line: Systolic Blood Pressure, Grey Line: Diastolic Blood Pressure, Yellow Line: Mean Arterial Blood Pressure, Light Blue Line: SpO2 (oxygen saturation). The 5 points on the x axis indicate 5 different perioperative time points at which the above patient’s variables are mentioned. 1: 5 min Pre Induction of GA, 2: 5 min Post Induction of GA, 3: 5 min Pre Block performance, 4: 5 min Post Block performance, 5: 5 min Post Incision. |
Total surgical time was 60 minutes and total anesthesia time was 89 minutes. The surgery was completed uneventfully. After which the patient was extubated safely and was transferred to Post-Operative Anesthesia Care Unit (PACU).
The patient was followed up in PACU where he reported a pain score of zero on the NRS. The hemodynamic parameters during patients’ stay in PACU are presented in Figure 2. After a two hour stay in PACU the patient was transferred to the ward.
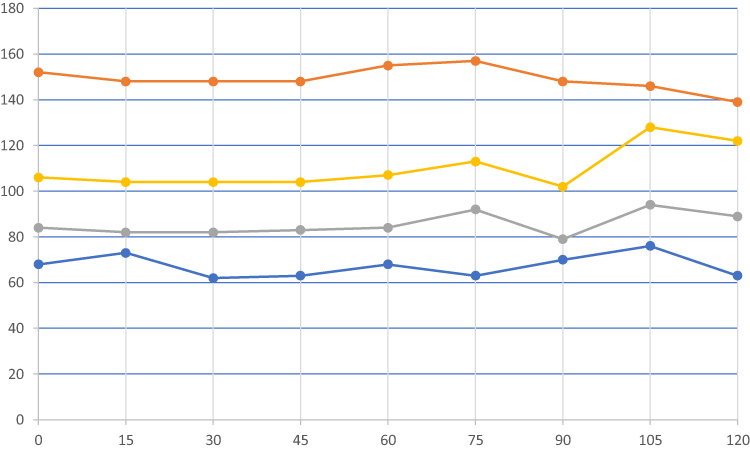 |
Figure 2 Patient Hemodynamic parameters in Post Anesthesia Care Unit. Colored Lines/dots on the Y axis represent: Blue Line: Heart rate, Red Line: Systolic Blood Pressure, Grey Line: Diastolic Blood Pressure, Yellow Line: Mean Arterial Blood Pressure. The x axis: Time, readings were taken at 15 min interval. |
On the ward the patient received regular IV paracetamol 1g 6 hourly post operatively in the next 24 hrs. Patient reported NRS pain score of zero at 7, 10, 14, 18, 22 and 26 hours in the postoperative period on the ward. Thereafter the patient re-developed abdominal pain 24 hours post operatively for which he required morphine. The patient’s stay was complicated by further abdominal fluid collections and pleural effusions, which were appropriately managed, and the patient was ultimately discharged after 23 days.
Discussion
Duodenum derives its parasympathetic supply from Vagus nerve and its sympathetic nerve supply from the celiac plexus. The celiac plexus is made up by nerve fibers predominantly travelling in the greater splanchnic nerve, with some contribution from the lesser splanchnic nerve. The greater splanchnic nerve, derived from T5-T9 spinal cord segments, transmits the nociceptive information from duodenum.
ESPB at T5 or T7 level have been reported to provide enough analgesic cover for thoracotomies and abdominal surgeries.3–6 In addition, an injection at T9 level has been proven to provide excellent analgesia for open abdominal hysterectomies.7 We have been doing ESPB at our institute for laparoscopic appendicectomies at T10 level with good results. Schwartzmann et al, presented a case report in which they conducted magnetic resonance imaging (MRI) of a patient who received an ESPB at T 10 level. They reported loss of sensation to cold from T6 to T12 level, whereas the MRI study showed spread of the LA not only from T5 to T12 levels, but also to the paravertebral space and epidural space. They postulated in their study that an ESPB at T10 could be beneficial for many abdominal surgeries based on their findings.8 Our rational to choose this level is that the appendix derives its nerve supply from T10 level, hence giving a bilateral ESPB at this level covers not only the somatic pain from the abdominal port wounds, but also the visceral pain. In our case report, we found that the ESPB performed at T10 level provided a totally morphine sparing effect and supports Schwartzmann et al’s case report findings that an ESPB at T10 level is enough to cover spinal cord segments up to T5 and hence the duodenum. In the postoperative period our patient did not require any morphine for 24 hours. After 24 hours the patient developed abdominal pain and required morphine. The pain was due to a new onset of intraabdominal fluid collection as confirmed on the computed tomography (CT) of the abdomen.
We could not objectively follow the block duration, but the patient’s clinical status was convincing enough to say that the block provided adequate analgesia.
Conflicting data regarding the spread of the LA and the mechanism of action of ESPB keeps appearing in the journals. Mostly, the conflict is found in the cadaveric studies done on the spread of LA. The initial proposed mechanism of action of the ESPB was that the LA once injected superficially to the ESM, diffuses to the paravertebral space, which provides the visceral analgesia.3,9 Ahikari et al studied the spread of LA in 2 different blocks, the ESPB and the retrolaminar block at T5 level. In both the blocks the study showed spread of the dye to ventral rami of the spinal cord, the paravertebral space and the epidural space.10 Hesham et al studied the spread of the ESPB at C6 and C7 spinal cord levels. In their study there was clear staining of the brachial plexus and the ventral rami which they concluded that ESPB block at this level could be beneficial for shoulder surgeries.11 Similar studies demonstrating the spread to the ventral rami have been published by Ece at al and Vidal et al.7,12 However studies conducted by Adriana et al and Ivanusic et al showed different results. In the two cadaveric studies, ESPB was performed at T7 level of the former and T5 of the later study, no spread of the dye was detected to the ventral rami of the spinal cord.13,14 The authors did however state that a difference in live human and a cadaver, dye and LA characteristics and volume and different ligamentous anatomy at different levels of the spinal cord might have some role in the different results of different studies.15 Hence the overall clinical evidence keeps favoring the fact that there is spread of LA to the ventral horn of the spinal cord and paravertebral space that provides the visceral analgesia.
Conclusion
We conclude from our case report that an ESPB performed at T10 spinal cord level provides totally opioid free anesthesia with no opioid requirements in the postoperative period for perforated duodenal ulcer surgery.
Ethics Approval
This case report went through screening first by the Corporate Research Committee of the Dept. of Anesthesia.ICU and Perioperative Medicine, Hamad Medical Corporation (HMC). There by the case report was submitted to the Medical Research Centre of HMC through and was approved with ID MRC-04-21-871.
Patient Consent
A written informed consent was obtained from the patient to publish this case report.
Acknowledgment
The authors would like to thank and acknowledge Qatar National Library for providing funds for the publication of this case report.
Funding
No funding was required for this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kelly DJ, Ahmad M, Brull SJ. Preemptive analgesia I: physiological pathways and pharmacological modalities. Can J Anaesth. 2001;48(10):1000. doi:10.1007/BF03016591
2. Woolf CJ, Chong MS. Preemptive analgesia--treating postoperative pain by preventing the establishment of central sensitization. Anesth Analg. 1993;77(2):362. doi:10.1213/00000539-199377020-00026
3. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;4:51.
4. Tsui BCH, Fonseca A, Munshey F, McFadyen G, Caruso TJ. The erector spinae plane (ESP) block: a pooled review of 242 cases. J Clin Anesth. 2018;53:29–34. doi:10.1016/j.jclinane.2018.09.036
5. Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre-operative bi- lateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;7(4):452–460.
6. Altinpulluk EY, Ozdilek A, Colakoglu N, et al. Fatis Altindas Bilateral postoperative ultrasound-guided erector spinae plane block in open abdominal hysterectomy: a case series and cadaveric investigation. J Anaesth Intensive Care. 2019;26(1):83–88.
7. Schwartzmann A, Peng P, Maciel MA, Forero M. Mechanism of the erector spinae plane block: insights from a magnetic resonance imaging study. Can J Anaesth. 2018;65:1165–1166. doi:10.1007/s12630-018-1187-y
8. Forero M, Rajarathinam M, Adhikary SD, Chin KJ. Erector spinae plane block for the management of chronic shoulder pain: a case report. Can J Anesth. 2018;65:288–293. doi:10.1007/s12630-017-1010-1
9. Adhikary SD, Bernard S, Lopez H, Chin KJ. Erector Spinae plane block versus retrolaminar block: a magnetic resonance imaging and anatomical study. Reg Anesth Pain Med. 2018;43:756–761. doi:10.1097/AAP.0000000000000798
10. Elsharkawy H, Ince I, Hamadnalla H, Drake RL, Tsui BCH. Cervical erector spinae plane block: a cadaver study. Reg Anesth Pain Med. 2020;45(7):552–556. doi:10.1136/rapm-2019-101154
11. Vidal E, Giménez H, Forero M, Fajardo M. Erector spinae plane block: a cadaver study to determine its mechanism of action. Rev Esp Anestesiol Reanim. 2018;65(9):514–519. doi:10.1016/j.redar.2018.07.004
12. Aponte A, Sala-Blanch X, Prats-Galino A, Masdeu J, Moreno LA, Sermeus LA. Anatomical evaluation of the extent of spread in the erector spinae plane block: a cadaveric study. Observational study. Can J Anaesth. 2019;66(8):886–893. doi:10.1007/s12630-019-01399-4
13. Ivanusic J, Konishi Y, Barrington MJ. A cadaveric study investigating the mechanism of action of erector spinae blockade. Reg Anesth Pain Med. 2018;43(6):567–571. doi:10.1097/AAP.0000000000000789
14. Yang HM, Choi YJ, Kwon HJ, Cho OJ, Kim SH, Kim SH. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: a cadaveric study. Anaesthesia. 2018;73:1244–1250. doi:10.1111/anae.14408
15. Damjanovska M, Pintaric TS, Cvetko E, Vlassakov K. The ultrasound-guided retrolaminar block: volume-dependent injectate distribution. J Pain Res. 2018;11:293–299. doi:10.2147/JPR.S153660
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Utility of Ultrasound-Guided Erector Spinae Plane Blocks for Postoperative Pain Management Following Thoracolumbar Spinal Fusion Surgery
Zelenty WD, Li TY, Okano I, Hughes AP, Sama AA, Soffin EM
Journal of Pain Research 2023, 16:2835-2845
Published Date: 16 August 2023
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Yap EN, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Journal of Pain Research 2025, 18:4775-4785
Published Date: 16 September 2025
Pain Management Approaches for Robotic-Assisted Thoracic Surgery: A Retrospective Analysis
Semyonov MA, Shmueli M, Smirnov A, Dubilet M, Refaely Y, Ruderman LN, Maron P, Binyamin Y, Brotfain E, Zlotnik A, Frank D
Journal of Pain Research 2025, 18:6085-6093
Published Date: 14 November 2025
The Emerging Role of Liposomal Bupivacaine in Erector Spinae Plane Blocks for Post-Operative Pain Management in Spine Surgeries: A Narrative Review
Delaney JB, Landry LP, Coggins NC, Ahmadzadeh S, Patil SS, Dorius B, Shekoohi S, Kaye AD
Clinical Pharmacology: Advances and Applications 2025, 17:339-346
Published Date: 22 December 2025