Back to Journals » Journal of Pain Research » Volume 16
Utility of Ultrasound-Guided Erector Spinae Plane Blocks for Postoperative Pain Management Following Thoracolumbar Spinal Fusion Surgery
Authors Zelenty WD ![]() , Li TY, Okano I, Hughes AP, Sama AA, Soffin EM
, Li TY, Okano I, Hughes AP, Sama AA, Soffin EM ![]()
Received 3 May 2023
Accepted for publication 7 August 2023
Published 16 August 2023 Volume 2023:16 Pages 2835—2845
DOI https://doi.org/10.2147/JPR.S419682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
William D Zelenty,1,* Tim Y Li,2,* Ichiro Okano,1,3,* Alexander P Hughes,1 Andrew A Sama,1 Ellen M Soffin4,*
1Department of Orthopaedic Surgery, Spine Service, Hospital for Special Surgery, New York, NY, 10021, USA; 2Weill-Cornell Medical College, New York, NY, 10021, USA; 3Department of Orthopaedic Surgery, Spine Service, Showa University Hospital, Hatanodai, Tokyo, Japan; 4Department of Anesthesiology, Critical Care & Pain Management, Hospital for Special Surgery, New York, NY, 10021, USA
*These authors contributed equally to this work
Correspondence: William D Zelenty, Assistant Attending Spinal Surgeon, Hospital for Special Surgery, Assistant Professor of Orthopaedic Surgery, Weill-Cornell Medical College, 523 East 72nd Street, 3rd Floor, New York, NY, 10021, USA, Email [email protected]
Purpose: The primary objective of this study is to determine if ultrasound-guided erector spinae plane blocks (ESPB) prior to thoracolumbar spinal fusion reduces opioid consumption in the first 24 hours postoperatively. Secondary objectives include ESPB effects on administration of opioids, utilization of intravenous patient-controlled analgesia (IV-PCA), pain scores, length of stay, and opioid related side effects.
Methods: A retrospective cohort analysis was performed on consecutive, adult patients undergoing primary thoracolumbar fusion procedures. Demographic and baseline characteristics including diagnoses of chronic pain, anxiety, depression, and preoperative use of opioids were collected. Surgical data included surgical levels, opioid administration, and duration. Postoperative data included pain scores, opioid consumption, IV-PCA duration, opioid-related side effects, ESPB-related complications, and length of stay (LOS). Statistical analysis was performed using chi-squared and t-test analyses, multivariable analysis, and covariate adjustment with propensity score.
Results: A total of 118 consecutive primary thoracolumbar fusions were identified between October 2019 and December 2021 (70 ESPB, 48 no-block [NB]). There were no significant demographic or surgical differences between groups. Median surgical time (262.50 mins vs 332.50 mins, p = 0.04), median intraoperative opioid consumption (8.11 OME vs 1.73 OME, p = 0.01), and median LOS (152.00 hrs vs 128.50 hrs, p = 0.01) were significantly reduced in the ESPB group. Using multivariable covariate adjustment with propensity score analysis only intraoperative opioid administration was found to be significantly less in the ESPB cohort.
Conclusion: ESPB for thoracolumbar fusion can be performed safely in index cases. There was a reduction of intraoperative opioid administration in the ESPB group, however the care team was not blinded to the intervention. Extensive thoracolumbar spinal fusion surgery may require a different approach to regional anesthesia to be similarly effective as ESPB in isolated lumbar surgeries.
Keywords: erector spinae plane block, regional anesthesia, local anesthesia, pain management, thoracolumbar fusion
A Letter to the Editor has been published for this article.
Introduction
Complex thoracolumbar fusion is associated with significant postoperative pain.1 In turn, pain is a major factor limiting prompt recovery, discharge from the hospital, and contributes to poor long-term outcomes.2,3 The increasing number and frailty of patients undergoing these types of procedures4,5 coupled with the ongoing opioid crisis occurring in the United States, has created an urgent need for improved analgesia and interventions which promote rapid recovery after complex spine surgery.
Current best practices call for multimodal analgesia (MMA) emphasizing non-opioid agents (including acetaminophen, non-steroidal anti-inflammatory drugs [NSAIDs], and NMDA receptor antagonists)6 and judicious use of opioids within enhanced recovery after surgery (ERAS) protocols.6–9 Local anesthetics for spine surgery in the form of field and fascial plane blocks have become a recent focus of clinical and research interest.10 Of all published interventions, the erector spinae plane block (ESPB) has received the most attention. However, results from systematic reviews and large retrospective series have yielded mixed evidence on the benefits of the block for postoperative pain scores, opioid consumption, and length of stay.8,11 Indeed, the recent PROSPECT guidelines on MMA for complex spine surgery recommended against ESPB due to insufficient evidence of benefit and overall low quality of evidence.6 Further, most of the studies to date have focused on lumbar spinal procedures; and the value of the ESPB may be procedure specific. Thus far, the available literature on ESPB for thoracolumbar fusion procedures is limited to case reports12,13 and a single randomized controlled trial that included 10 patients undergoing fusion procedures in the thoracolumbar spine, only 3 of which had fusions of more than 2 levels.14
Accordingly, the purpose of this study was to evaluate the association of ESPB with pain scores and opioid consumption during the first 24 hours after thoracolumbar fusion surgery. Secondary outcomes included associations of ESPB and length of stay (LOS), intravenous opioid patient-controlled analgesia (IV-PCA) use, opioid consumption at other time points, and opioid-related side effects. We hypothesized that there would be a significant reduction in postoperative opioid consumption without adversely effects on pain scores along with reductions in LOS and opioid-related side effects among patients who received ESPB.
Methods
Study Design and Patients
This is a single-center, retrospective cohort study. The study was conducted in accordance with the ethical principles of the Helsinki declaration and approved by the institutional review board of Hospital for Special Surgery (IRB #2020-1877). Written informed consent was waived.
The electronic medical records (EMR) of all patients who underwent posterior multilevel thoracolumbar spinal fusion (with or without decompression) under general anesthesia between October 2019 and December 2021 were reviewed to identify cases with the following criteria: age >18 years; primary posterior procedure; received either pre-incision bilateral ultrasound-guided ESPB or no ESPBs; and elective surgery. Patients with any of the following factors were excluded from analysis: emergent or revision surgery; known or suspected spinal infection; continuous catheter or neuraxial analgesia; unilateral ESPB.
Patients were grouped into 2 cohorts depending on whether they received ESPBs (ESPB cohort) or no-blocks (NB cohort).
ESPB Technique
Bilateral ultrasound-guided ESPBs were performed with the patient in prone position after induction of GA, prior to surgical incision, as previously described.8 In brief, the tips of the transverse processes at the relevant spinal level were visualized using a C60 curved array ultrasound probe (FUJIFILM Sonosite, Inc., WA, USA). A 20-Ga 4-inch Ultraplex needle (B. Braun Medical Inc., PA, USA) was placed in-plane and advanced in a cranial-to-caudal direction until the tip was under the erector spinae plane. Depending on patient body mass index (BMI), between 20 and 30 mL 0.25–0.375% bupivacaine was injected bilaterally.
Demographic and Preoperative Clinical Data
Demographics and preoperative clinical data were collected from the EMR, including age, sex, height, weight, BMI, race/ethnicity, American Society of Anesthesiologists (ASA) Classification, smoking status, history of psychiatric illness (anxiety, depression), clinical diagnosis of chronic pain, opioid use for more than 3 months, neuroleptic medication use for more than 3 months, and indication for surgery.
Surgical Data
Intraoperative and surgical data were collected from the EMR, including surgeon and anesthesiologist of record, surgical duration, levels fused, number of levels fused, presence of decompression, presence of osteotomy, and use of adjunctive procedures. Surgical indications were binned for statistical analysis into one of 7 categories: lumbar degenerative scoliosis, thoracolumbar degenerative scoliosis, spondylosis/stenosis, adolescent idiopathic scoliosis in adulthood, adolescent idiopathic scoliosis, kyphoscoliosis, and other. Fusion constructs were binned into one of 6 categories for statistical analysis: low thoracic to pelvis fusion (upper instrumented vertebra [UIV]: T9-12), mid-thoracic to pelvis fusion (UIV: T5-8), high thoracic to pelvis fusion (UIV: T1-4), thoracolumbar fusion (UIV: thoracic level, lower instrumented vertebra [LIV]: L1-4), thoracic fusion (LIV within the thoracic spine), and short thoracolumbar fusion (UIV: thoracic level, LIV: L5 or S1).
Outcomes
The primary study outcome was opioid consumption in the first 24 hours after surgery (recorded as oral morphine equivalent, OME, milligrams). Secondary study outcomes were length of stay (LOS), intraoperative and total opioid consumption, IV-PCA dose and duration, numeric rating scale (NRS) pain scores (0–10; divided into post anesthesia care unit (PACU) and nursing floor phases of care), opioid related side effects and adverse events related to ESPB. Opioid-related side effects were defined a priori as postoperative nausea/vomiting (indicated by administration of rescue anti-emetic medications), sedation/respiratory depression (indicated by escalation of care and/or need for supplemental oxygen and/or naloxone), constipation/obstipation, and cognitive/ central nervous system (CNS) changes (dizziness, confusion, and disorientation). Complications of ESPB were defined a priori as any motor, sensory, neurologic, or respiratory complication reasonably attributed to the block.
Statistical Analysis
Continuous variables are summarized as mean (standard deviation) or median [range]. Categorical variables are summarized as counts (%). Demographic and preoperative and postoperative clinical data were compared using chi-squared for categorical and t-testing for continuous variables. In addition to the simple comparisons between no block and ESPB groups and conventional multivariable analyses, we added the analysis of covariate adjustment with propensity score (PS). PS was defined as the probability of undergoing ESPB or not, and PS was calculated using a logistic regression model including all preoperative variables. Linear regression analyses were conducted by setting the outcomes which showed statistical significance in the simple comparisons as response variables, ESPB as the predictor variable, intraoperative factors such as operation time, and the PS as confounding variables. Estimates were calculated using the beta coefficient of linear regression. Statistical analysis was performed utilizing R software (R for 4.1.2). The statistical significance was set at p < 0.05.
Results
Demographic and Preoperative Clinical Data
We identified 118 patients for analysis: 70 received bilateral ESPBs and 48 did not. Patient demographics and preoperative clinical data are detailed in Table 1. There were no statistically significant differences between the cohorts.
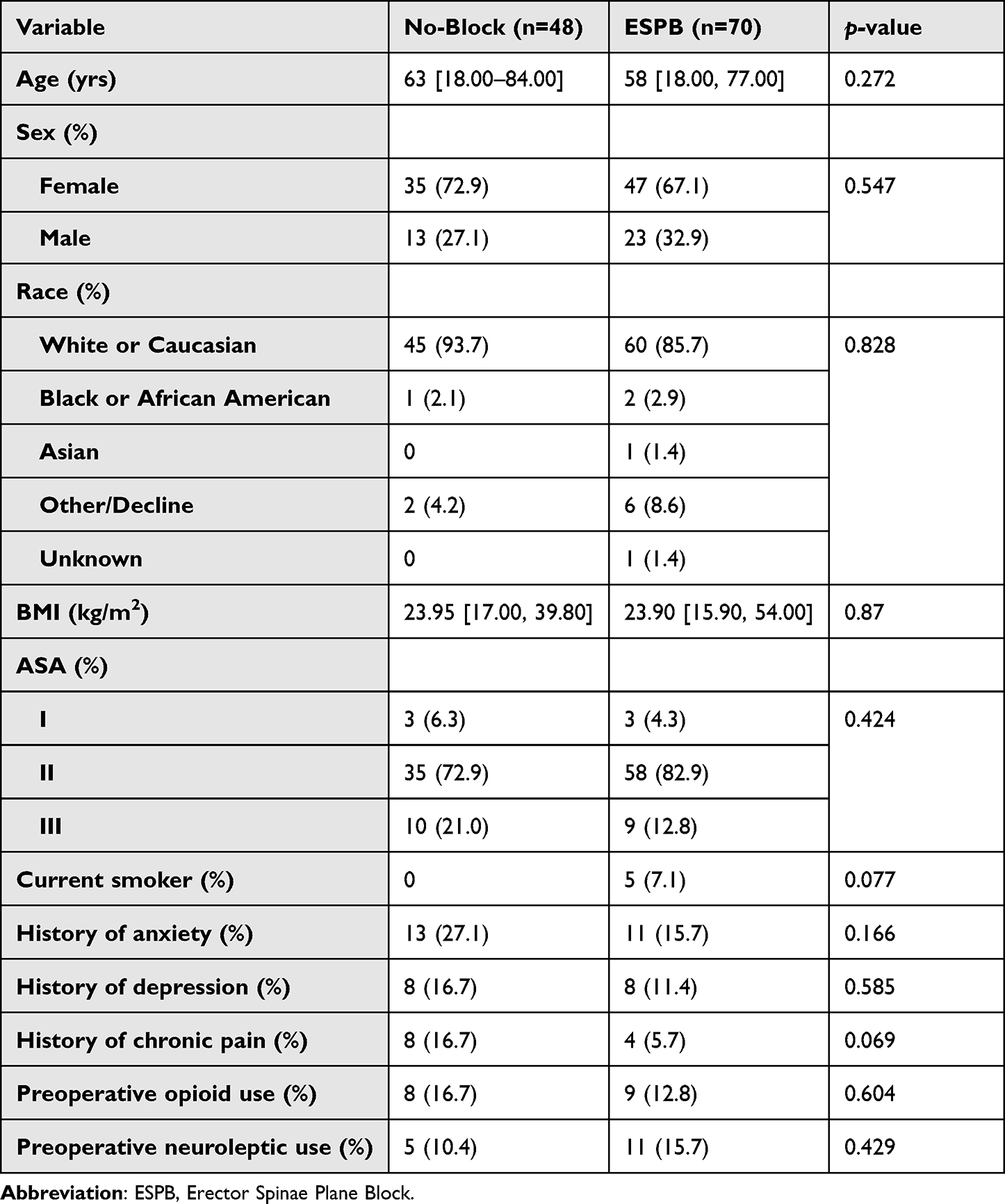 |
Table 1 Demographic and Preoperative Clinical Data |
Surgical Data
Simple analyses of intraoperative clinical data are displayed in Table 2. There were no statistically significant differences between groups in terms of surgical indication, construct type, number of levels fused, use of adjunctive procedures, decompressions, or osteotomies. Median surgical duration in the no-block cohort was over 70 minutes longer than in the ESPB group (332.50 mins vs 262.50 mins, p = 0.046).
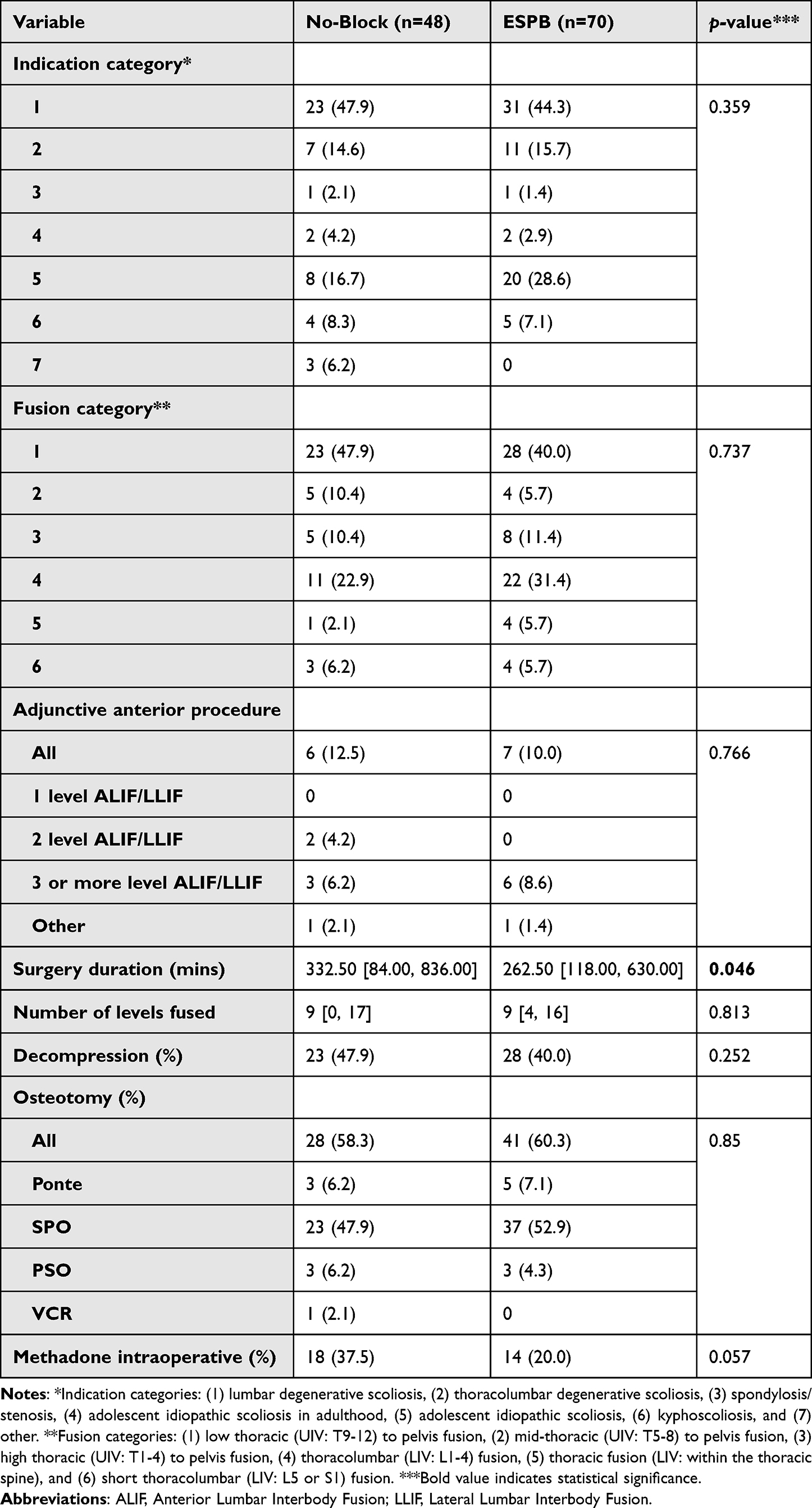 |
Table 2 Surgical Data |
Simple Comparison of Study Outcomes
Simple comparisons of study outcomes are displayed in Table 3. Median LOS was significantly shorter in the ESPB cohort (128.50 hrs vs 152.00 hrs, p = 0.011) and median intraoperative opioid administration was significantly lower in the ESPB cohort (1.73 mg vs 8.11 mg, p = 0.011). IV-PCA duration, LOS in PACU and nursing floors, pain scores, postoperative opioid consumption, and opioid-related side effects were similar between cohorts. There were no complications detected due to ESPB.
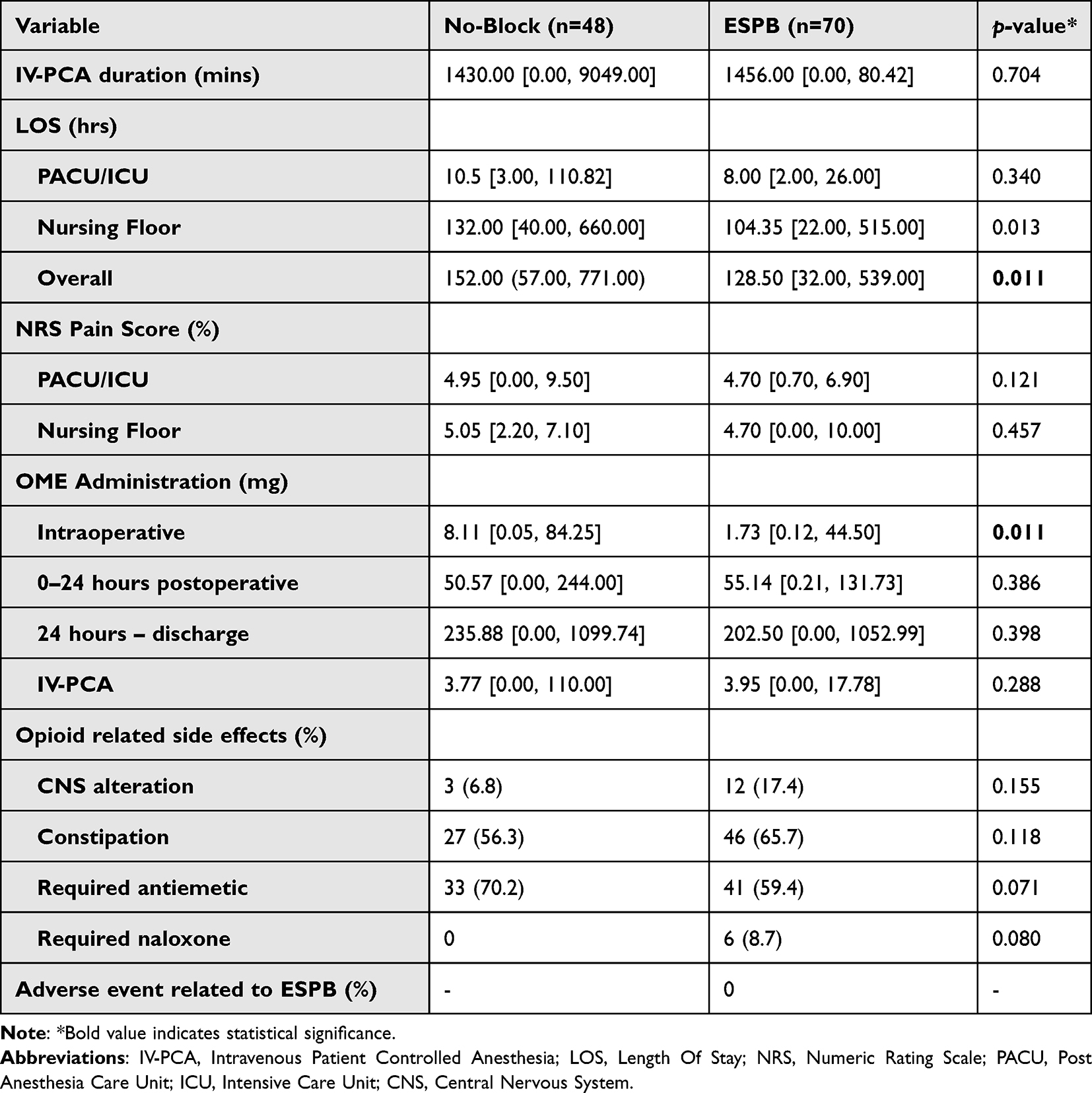 |
Table 3 Simple Comparison of Study Outcomes |
Multivariable Analysis
Multivariable analyses and covariate adjustment with propensity score analyses are displayed in Table 4 and 5, respectively. On multivariable analyses, surgical duration was significantly associated with LOS (0.29 [0.16–0.41]), but ESPB was not (−21.67 [−58.24–14.89]). Intraoperative opioid administration was significantly associated with ESPB (−7.96 [0.26–18.3]) and preoperative opioid use (9.14 [0.26–18.3]).
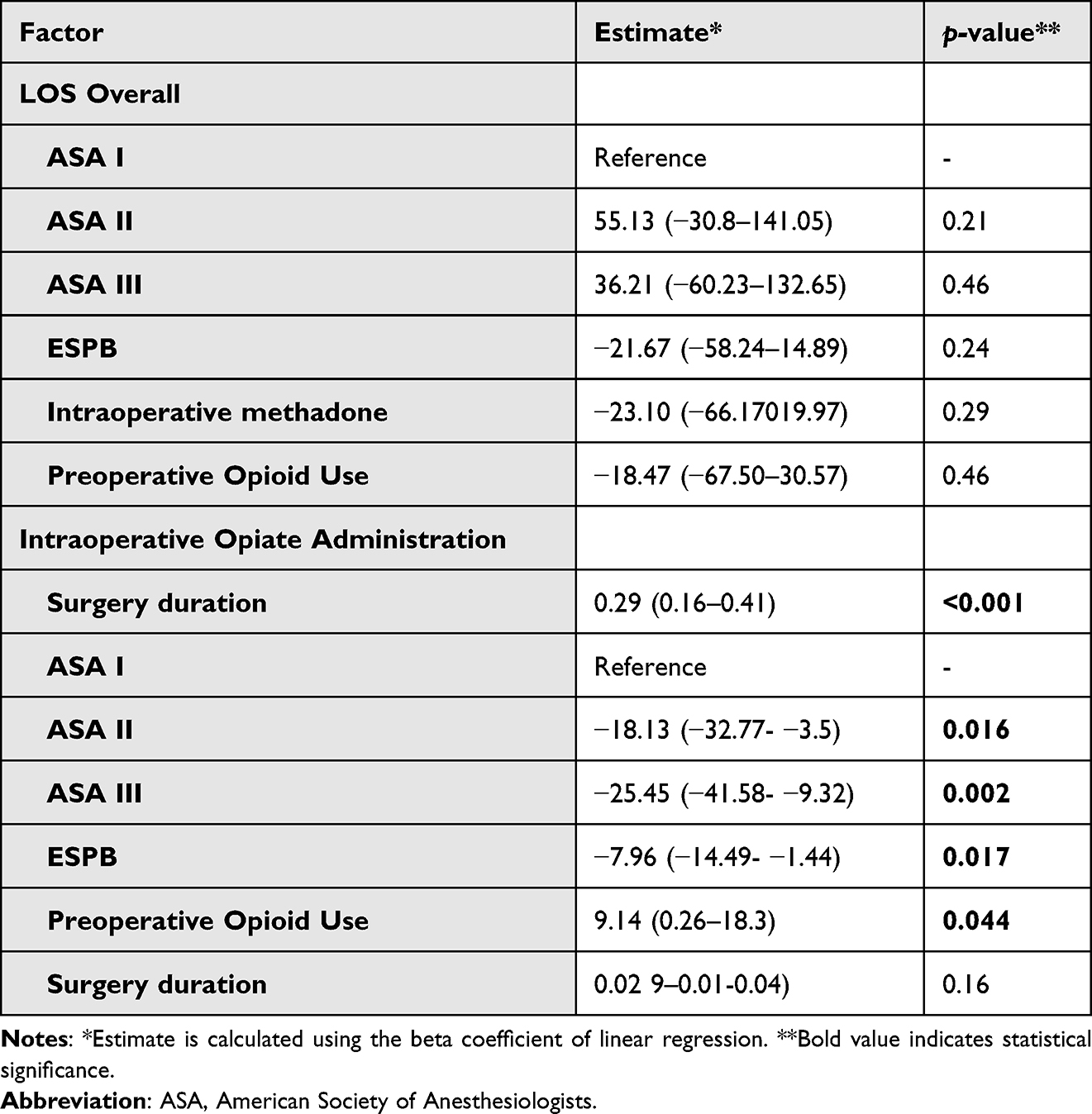 |
Table 4 Multivariable Analysis |
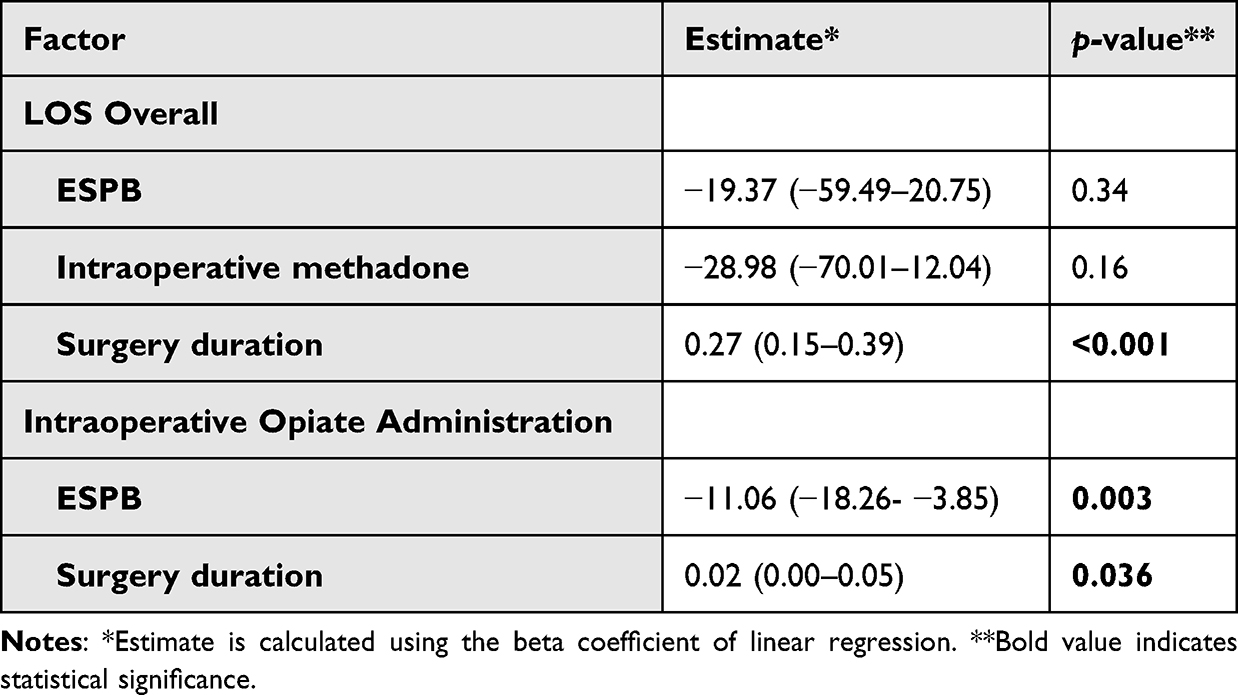 |
Table 5 Covariate Adjustment with Propensity Score Analysis |
After covariate adjustment with PS, the only variable which remained significantly associated with LOS was surgical duration (0.27 [0.15–0.39]). Both ESPB (−7.96 [−14.49- −1.44]) and surgical duration (0.02 [0.00–0.05]) were significantly associated with intraoperative opioid administration.
Discussion
In this retrospective cohort study, we found a positive association between bilateral ESPB and a reduction of intraoperative opioid administration among 118 patients who underwent multilevel thoracolumbar fusion. There were no differences in postoperative opioid consumption at any time, utilization of IV-PCA, NRS pain scores, or opioid-related side effects between the groups. While LOS and surgical duration were shorter among patients who received ESPB on simple comparisons, this effect was lost on multivariable analyses.
Emerging literature supports ESPB to improve pain and opioid-related outcomes after lumbar spinal procedures.10 Results from systematic reviews/meta-analyses, prospective randomized clinical trials, and large retrospective series show no or small effects of the blocks on outcomes of interest.8,11,15,16 Where demonstrated, ESPB appears to modestly lower early postoperative pain scores (at rest and with movement) and opioid consumption, and limit opioid-related side effects. The block has predominately been studied in lumbar surgery, with thoracic and thoracolumbar procedures being relatively underexplored. Given the possibility of differential benefits of ESPB for these latter procedures (with larger anticipated pain burden), we sought to establish associations of ESPB on clinically relevant outcomes after complex thoracolumbar spinal fusion procedures.
Surprisingly minor benefits have been described when adding ESPB to ERAS pathways for lumbar spine surgery which include comprehensive MMA, raising the question whether the lumbar spine is the appropriate anatomic target for ESPB.8,16 Forero et al initially described the ESPB technique for use in thoracic neuropathic pain. Their test cases were rib fracture nonunion and metastatic disease to the ribs.17 Subsequent anatomic studies demonstrated that ESPB performed in the lower thoracic spine had excellent diffusion through the thoracic and lumbar spine compared with other fascial plane blocks (eg, quadratus lumborum block).18,19 Prakash et al suggested that the origin of the spinalis thoracis muscle at about T11 to L2 may block inferior spread of injectate.20 While this may be a limitation when utilized in isolated lumbar surgeries, spread cranially to thoracic levels may be a benefit in thoracolumbar procedures.
We found significantly lower intraoperative opioid administration among patients who received ESPB versus no block. This is consistent with at least one recent systematic review with meta-analysis,21 but also with other reported literature, including a randomized controlled trial that included simulated injections.22 Reductions in anesthetic and analgesic requirements are biologically plausible if ESPB attenuates the patient response to surgical stimulation, thereby lowering anesthetic and analgesic requirements. Although we hypothesize that this explains our findings, due to the retrospective nature of the current study the anesthesia teams were not blinded to treatment group. It is possible that block performance introduced a bias towards administering less opioid analgesia. However, we propose that this was not the case, given that NRS pain scores and opioid consumption were not different between the groups in the PACU or at early recovery times.
Indeed, we found no differences in postoperative opioid consumption at each time interval or when analyzed by route (oral or IV-PCA). Available literature on this topic is mixed, with most (but not all) studies in lumbar spine surgery cohorts concluding significant reductions in postoperative opioid consumption at multiple time points.10 Goel et al performed a randomized, case–control study comparing ESPB with MMA to MMA only after single-level lumbar fusions. They found that opioid consumption during the first 24 hours was significantly lower in the block group, but total opioid consumption was very low in both groups (105.0 ± 15.15 vs 158.00 ± 23.38mcg, p < 0.001).23 Zhu et al performed a randomized controlled trial comparing ESPB versus simulated injection for patients undergoing lumbar fusion surgery. Patients required fewer rescue doses of sufentanil in PACU (2 vs 10, p < 0.001) and the authors found a significant reduction in oral oxycodone administered during each 6-hour interval for the first 24 hours. Between 24 and 48 hours there was no difference, however the total amount consumed over 48 hours was significantly less in the block group (36.40 vs 23.10mg, p < 0.001).22 Zhang et al performed a randomized controlled trial comparing ESPB to no-block on patients undergoing open lumbar laminectomy surgery. All patients received a morphine IV-PCA which included a basal rate of 0.25mg/hr. Total morphine consumed at 24 and 48 hours postoperatively was significantly less in the block group.24 Several recent systematic reviews and meta-analyses which included studies from Chinese language literature support these findings of significant reduction of opioid consumption in the first 24 hours and need for rescue analgesics in lumbar surgeries.21,25–27 The thoracolumbar fusions presented here had an average of 9 levels fused in each group which is represents a substantially different cohort than available literature, the bulk of which reports on single level lumbar fusions.22,23 All of our patients were treated using an MMA regimen which includes IV-PCA.
We did not find significant differences in LOS between the 2 groups. Recovery after extensive thoracolumbar fusion is anticipated to be longer compared to other spinal surgeries, particularly when compared with the single level lumbar fusions and lumbar decompression surgeries typically studied for ESPB. A recent retrospective analysis of mixed lumbar procedures including 1 and 2 level fusions and multilevel decompressions reported a statistically significant reduction in overall LOS of 5 hours between ESPB and no-block cohorts. The unadjusted median LOS was 80.6 hours versus 74.9 hours for ESPB and no-block cohorts, respectively.8 Owen et al retrospectively reviewed 1 and 2 level lumbar fusions that received ESPB versus no block and found that ESPB reduced overall LOS by 19.2 hours (2.4 vs 3.2 days, p < 0.05).28 Similarly, van den Broek et al reviewed 20 single-level PLIF with ESPB versus 20 controls and found a significant reduction in LOS of approximately 12 hours (3.23 vs 2.74 days, p = 0.012).29 By comparison, Zhang et al in their investigation of ESPB effects on lumbar decompression showed a tendency towards shorter LOS, however it was not statistically significant (6.0 vs 6.5 days, p = 0.054).24 It is perhaps unsurprising that in our investigation single-shot ESPBs had no effect on overall LOS considering reported modest effects in less invasive procedures.
Surprisingly, we found no effect on postoperative NRS pain scores, particularly in immediate PACU or subsequent phases of care following the operating room. Lack of ESPB effects on NRS scores has been described in lumbar spine cohorts. For example, a recent prospective randomized trial compared morphine consumption and pain after surgery for lumbar disc herniation. Patients randomized to ESPB consumed less morphine, but there were no differences in pain scores between ESPB and control.30 Our group reported a similar phenomenon wherein we observed a significant reduction in opioid consumption in the first 24 hours after lumbar fusion, but no effect on NRS pain scores over the same interval.8 Finally, a recent prospective clinical trial randomized 50 patients undergoing lumbar surgery to ESPB or no block plus MMA. The authors found no differences in opioid consumption or NRS scores at any time in the postoperative period.16 Where reported, the benefits of ESPBs on pain scores appear to be limited to the first 6 hours after lumbar surgery.11,15,26,31 Interestingly, our median duration of surgery was greater than 4 hours, so the early assessments of pain in the PACU may have coincided with block resolution in the ESPB group. This raises the possibility that continuous erector spinae catheters may be necessary for prolonged analgesia after extensive spinal fusion surgeries.32 An alternative explanation for these results is that the otherwise comprehensive MMA provided was sufficient to create a ceiling effect on NRS scores which nullifies the additive benefit of ESPBs.
Finally, we did not identify any differences in opioid-related side effects between the groups or in prespecified complications of ESPB. These results are perhaps unsurprising given that we did not find any differences in opioid consumption over time. Likewise, existing literature supports an incidence of complications related to ESPB for lumbar surgery approximating zero.33
Limitations
This study has several limitations. This is a retrospective cohort study and is therefore subject to confounding and selection bias. Although we have attempted to control for bias by excluding revision surgeries, limiting surgical indications, and utilizing covariate adjustment with propensity score analyses there are several key weaknesses inherent in any retrospective study design. The lack of prospective randomization and blinding allows for significant selection bias. There are several sources, including the patient, surgeon, and anesthesia team who may influence the choice to perform ESPBs. Patients and practitioners were not blinded to their treatment. The intraoperative dosage of opioid medication and selection of opioid (such as methadone or hydromorphone) may have been influenced by the anesthesia team’s awareness of the ESPB. Our cohort is heterogeneous, including both adult spinal deformity and pediatric spinal deformities in adulthood (eg patients with adult idiopathic scoliosis over 18 years of age). It is possible that these represent distinct clinical entities in terms of pain burden and management. In addition to some heterogeneity, our cohorts are relatively small which may limit our statistical power. In our institution, ultrasound-guided ESPB is routinely performed and documented, but several details are lacking in the procedure notes which could reasonably affect the interpretation of block effectiveness. Specifically, the spinal level and needle position relative to the transverse processes are not always recorded, and when recorded are subject to the judgement of the performing anesthesiologist. Likewise, the qualitative and quantitative spread of local anesthetic is neither assessed nor confirmed. Multiple anesthesiologists performed the blocks reported in this study and, while all were fellowship trained or grandfathered in regional anesthesia, individual practice and consistency of block performance may have been variable. This study only evaluated short-term outcomes after ESPB, essentially 24 hours after surgery and during their hospital stay. Long-term outcomes after blocks have not been evaluated in this patient cohort. We restricted our findings to those available in the inpatient medical record, which is high fidelity. Long term outcomes may be an interesting avenue of future research.
Conclusions
Here, we report that ESPB can be added as an adjunct to an MMA regimen for thoracolumbar fusion, however there is limited evidence to support regular use. We found the main association of ESPB was with a reduction in intraoperative opioid utilization. We did not identify concomitant reductions in postoperative opioid needs, pain scores, opioid-related side effects, or LOS. ESPB has emerged as a potential adjunct as part of analgesic regimens for spine surgery and a growing body of evidence supports ESPB for minor benefits on important outcomes after 1 and 2 level fusions, decompressions, and discectomy, including pain scores, opioid consumption and- related side effects, and LOS. Block performance appears to be associated with few complications and can be rapidly administered under ultrasound or fluoroscopic guidance. Given the ongoing need for better pain management strategies after complex thoracolumbar procedures, offering ESPB may be reasonable, despite these minor clinical effects. More rigorous study is necessary to make a definitive recommendation on the routine use of ESPB in thoracolumbar fusion surgeries.
Ethical Approval
The study was conducted in accordance with the ethical principles of the Helsinki declaration and approved by the institutional review board of Hospital for Special Surgery (IRB# 2020-1877).
Informed Consent
This was a retrospective study of procedures performed as standard of care, thus informed consent was not required.
Funding
No funding was received to assist with preparation of this manuscript.
Disclosure
Dr Alexander P Hughes reports research support from Kuros Biosciences AG and Expanding Innovations, Inc.; fellowship support from NuVasive, Inc. and Kuros Biosciences BV, outside the submitted work. The authors have no other relevant financial or non-financial conflicts of interest to report for this work.
References
1. Lamperti M, Tufegdzic B, Avitsian R. Management of complex spine surgery. Curr Opin Anesthesiol. 2017;30(5):551–556. doi:10.1097/ACO.0000000000000494
2. Borgeat A, Blumenthal S. Postoperative pain management following scoliosis surgery. Curr Opin Anaesthesiol. 2008;21:313–316. doi:10.1097/ACO.0b013e3282f82baa
3. Devin C, McGirt M. Best evidence in multimodal pain management in spine surgery and means of assessing postoperative pain and functional outcomes. J Clin Neurosc. 2015;22(6):930–938. doi:10.1016/j.jocn.2015.01.003
4. Kebaish KM, Neubauer PR, Voros GD, Khoshnevisan MA, Skolasky RL. Scoliosis in adults aged forty years and older: prevalence and relationship to age, race, and gender. Spine. 2011;36(9):731–736. doi:10.1097/BRS.0b013e3181e9f120
5. Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and nutritional parameters in an elderly volunteer population. Spine. 2005;30(9):1082–1085. doi:10.1097/01.brs.0000160842.43482.cd
6. Waelkens P, Alsabbagh E, Sauter A, Joshi GP, Beloeil H. PROSPECT Working group of the European Society of Regional Anaesthesia and Pain therapy (ESRA). Pain management after complex spine surgery: a systematic review and procedure-specific postoperative pain management recommendations. Eur J Anaesthesiol. 2021;38(9):985–994. doi:10.1097/EJA.0000000000001448
7. Yoo JS, Ahn J, Buvanendran A, Singh K. Multimodal analgesia in pain management after spine surgery. J Spine Surg. 2019;5(S2):S154–S159. doi:10.21037/jss.2019.05.04
8. Soffin EM, Okano I, Oezel L, et al. Impact of ultrasound-guided erector spinae plane block on outcomes after lumbar spinal fusion: a retrospective propensity score matched study of 242 patients. Reg Anesth Pain Med. 2022;47(2):79–86. doi:10.1136/rapm-2021-103199
9. Tong Y, Fernandez L, Bendo JA, Spivak SM. Enhanced recovery after surgery trends in adult spine surgery: a systematic review. Internat J Spine Surg. 2020;14(4):623–640. doi:10.14444/7083
10. McCracken S, Lauzadis J, Soffin EM. Ultrasound-guided fascial plane blocks for spine surgery. Curr Opin Anaesthesiol. 2022;35(5):626–633. doi:10.1097/ACO.0000000000001182
11. Oh SK, Lim BG, Won YJ, Lee DK, Kim SS. Analgesic efficacy of erector spinae plane block in lumbar spine surgery: a systematic review and meta-analysis. J Clin Anesth. 2022;78:110647. doi:10.1016/j.jclinane.2022.110647
12. Chin KJ, Lewis S. Opioid-free analgesia for posterior spinal fusion surgery using erector spinae plane (ESP) blocks in a multimodal anesthetic regimen. Spine. 2018;44(6):E379–E383. doi:10.1097/BRS.0000000000002855
13. Chin KJ, Dinsmore MJ, Lewis S, Chan V. Opioid-sparing multimodal analgesia with bilateral bi-level erector spinae plane blocks in scoliosis surgery: a case report of two patients. Eur Spine J. 2020;29(S2):S138–S144. doi:10.1007/s00586-019-06133-8
14. Finnerty D, Eochagain AN, Ahmed M, Poynton A, Butler JS, Buggy DJ. A randomized trial of bilateral erector spinae plane block vs. no block for thoracolumbar decompressive spinal surgery. Anesthesia. 2021;76:1499–1503. doi:10.1111/anae.15488
15. Qiu Y, Zhang TJ, Hua Z. Erector spinae plane block for lumbar spinal surgery: a systematic review. J Pain Res. 2020;13:1611–1619. doi:10.2147/JPR.S256205
16. Avis G, Gricourt Y, Vialatte PB, et al. Analgesic efficacy of erector spinae plane blocks for lumbar spine surgery: a randomized double-blind controlled clinical trial. Reg Anesth Pain Med. 2022;21:rapm-2022–103737. doi:10.1136/rapm-2022-103737
17. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block, a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
18. Elsharkawy H, Bajracharya GR, El-Boghdadly Drake RL, Mariano ER. Comparing two posterior quadratus lumborum block approaches with low thoracic erector spinae plane block: an anatomic study. Reg Anesth Pain Med. 2018;44:549–555. doi:10.1136/rapm-2018-100147
19. Yang HM, Choi YJ, Kwon HJ, et al. Comparison of injectate spread and nerve involvement between retrolaminar and erector spinae plane blocks in the thoracic region: a cadaveric study. Anesthesia. 2018;73:1244–1250. doi:10.1111/anae.14408
20. Prakash PS. Correspondence: erector spine plane block at the T12 level may not provide good postoperative pain following lumbosacral surgery. J Neurosurg Anesthesiol. 2021;33(1):93–94. doi:10.1097/ANA.0000000000000660
21. Liang X, Zhou W, Fan Y. Erector spinae plane block for spinal surgery: a systematic review and meta-analysis. Korean J Pain. 2021;34(4):487–500. doi:10.3344/kjp.2021.34.4.487
22. Zhu L, Wang M, Wang X, Wang Y, Chen L, Li J. Changes of opioid consumption after lumbar fusion using ultrasound-guided lumbar erector spinae plane block: a randomized controlled trial. Pain Phys. 2021;24:E161–E168.
23. Goel VK, Chandramohan M, Murugan C, et al. Clinical efficacy of ultrasound guided bilateral erector spinae block for single-level lumbar fusion surgery: a prospective, randomized, case-control study. The Spine J. 2021;21:1873–1880. doi:10.1016/j.spinee.2021.06.015
24. Zhang T, Zhang J, Qu Z, Zhang H, Qiu Y, Hua Z. Bilateral erector spinae plane blocks for open posterior lumbar surgery. J Pain Res. 2020;13:709–717. doi:10.2147/JPR.S248171
25. Liu M, Zhou X, Yao Y, Shen X, Wang R, Shen Q. Postoperative analgesic efficacy of erector spinae plane block in patients undergoing lumbar spinal surgery: a systematic review and meta-analysis. Pain Ther. 2021;10(1):333–347. doi:10.1007/s40122-021-00256-x
26. Ma J, Bi Y, Zhang Y, et al. Erector spinae plane block for postoperative analgesia in spine surgery: a systematic review and meta-analysis. Eur Spine J. 2021;30(11):3138–3149. doi:10.1007/s00586-021-06853-w
27. Viderman D, Aubakirova Umbetzhanov Y, Kulkaeva G, Shalekenov SB, Abdilidin YG. Ultrasound-guided erector spinae plane block in thoracolumbar spinal surgery: a systematic review and meta-analysis. Front Med. 2022;9:1–9.
28. Owen RJ, Quinlan N, Poduska A, et al. Preoperative fluoroscopically guided regional erector spinae plane blocks reduce opioid use, increase mobilization, and reduce length of stay following lumbar spine fusion. Global Spine J. 2021; 13:1–7.
29. van den Broek RJC, van de Geer R, Schepel NC, Liu W, Bouwman RA, Versyck B. Evaluation of adding erector spinae plane block to stand anesthetic care in patients undergoing posterior lumbar interbody fusion surgery. Sci Reports. 2021;11:1–6.
30. Yörükoğlu HU, Içli D, Aksu C, Cesur S, Kuş A, Gürkan Y. Erector spinae block for postoperative pain management in lumbar disc hernia repair. J Anesth. 2021;35(3):420–425. doi:10.1007/s00540-021-02920-0
31. Rizkalla JM, Holderread B, Awad M, Botros A, Syed IY. The erector spinae plane block for analgesia after lumbar spine surgery: a systematic review. J Orthop. 2021;24:145–150. doi:10.1016/j.jor.2021.02.006
32. Oezel L, Hughes AP, Arzani A, et al. Surgeon-placed erector spinae plane catheters for multilevel lumbar spine fusion: technique and outcomes compared with single-shot blocks. Int J Spine Surg. 2022;16(4):697–705. doi:10.14444/8300
33. Oezel L, Hughes AP, Onyekwere I, et al. Procedure-specific complications associated with ultrasound-guided erector spinae plane block for lumbar spine surgery: a retrospective analysis of 342 consecutive cases. J Pain Res. 2022;15:655–661. doi:10.2147/JPR.S354111
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Report: Erector Spinae Block in Perforated Viscus
Rauf J, A M Haji MM
Local and Regional Anesthesia 2023, 16:19-23
Published Date: 16 February 2023
Prolonged Duration of Peripheral Nerve Blockade in a Pediatric Patient with Charcot Marie Tooth Disease: A Case Report
Barnett NR, Bunnell AM, Dow MA
Local and Regional Anesthesia 2024, 17:49-53
Published Date: 20 April 2024
Erector Spinae Plane versus Pectoralis Nerve Block for Mastectomy in Cancer Patients: A Retrospective, Multicenter Cohort Study
Yap EN, Wei J, Darling C, Linehan E, Behrends M, Ng KP
Journal of Pain Research 2025, 18:4775-4785
Published Date: 16 September 2025
Median Effective Volume of 0.25% Ropivacaine for Bilateral Transversus Thoracis Muscle Plane Block in Patients Undergoing Open Cardiac Surgery
Sun J, Liu C, Gong X, Chen R, Deng S, Zha Y, Ji S, Jin Z, Chen H
Journal of Pain Research 2025, 18:5321-5329
Published Date: 11 October 2025
The Emerging Role of Liposomal Bupivacaine in Erector Spinae Plane Blocks for Post-Operative Pain Management in Spine Surgeries: A Narrative Review
Delaney JB, Landry LP, Coggins NC, Ahmadzadeh S, Patil SS, Dorius B, Shekoohi S, Kaye AD
Clinical Pharmacology: Advances and Applications 2025, 17:339-346
Published Date: 22 December 2025