Back to Journals » International Journal of Women's Health » Volume 18
Elevated Visceral Adiposity Index is Associated with Reproductive Endocrine Characteristics, and Adverse Pregnancy Outcomes in Chinese Women with Polycystic Ovary Syndrome
Authors Shi B ![]() , Feng J, Lu F, Guan M, Yu J, Gao Z
, Feng J, Lu F, Guan M, Yu J, Gao Z ![]() , Wang Y, Cong J, Ma H, Han C, Yang W, Wu X, Gao J
, Wang Y, Cong J, Ma H, Han C, Yang W, Wu X, Gao J
Received 21 October 2025
Accepted for publication 4 March 2026
Published 17 June 2026 Volume 2026:18 575900
DOI https://doi.org/10.2147/IJWH.S575900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Baichao Shi,1 Jiaxing Feng,2 Fengjuan Lu,1 Muxin Guan,1 Jiannan Yu,1 Zhuwei Gao,1 Yu Wang,2 Jing Cong,2 Hongli Ma,2 Conghui Han,3 Wen Yang,4 Xiaoke Wu,2,5 Jingshu Gao5
1Graduate School, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 2Department of Gynecology, The First Affiliated Hospital, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 3Urology Department, Xuzhou Central Hospital Southeast University, Xuzhou, Jiangsu, People’s Republic of China; 4Reproductive medicine Center, Xuzhou Medical University Affiliated Lianyungang Hospital, Lianyungang, Jiangsu, People’s Republic of China; 5Department of Gynecology, Zhejiang Provincial Hospital of Chinese Medicine, and Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Xiaoke Wu, Email [email protected] Jingshu Gao, Email [email protected]
Objective: To evaluate the visceral adiposity index (VAI) as a metabolic and reproductive risk marker in Chinese women with polycystic ovary syndrome (PCOS).
Methods: Secondary analysis of 956 women with PCOS from the PCOSAct trial. VAI was calculated from waist circumference, BMI, triglycerides, and HDL-C. Associations with anthropometric, metabolic, endocrine, and pregnancy outcomes were assessed using regression models. Predictive performance for insulin resistance (IR) and non-alcoholic fatty liver disease (NAFLD) was evaluated via ROC analysis.
Results: Elevated VAI was positively associated with age, BMI, blood pressure, dysglycemia, dyslipidemia, FT, hepatic enzymes, and prevalence of IR, MetS, and NAFLD (all P-trend < 0.05). VAI was negatively correlated with QUICKI, HDL, SHBG, gonadotropins and AMH (all P-trend < 0.01). In fully adjusted models, the highest VAI quartile had an increased risk of IR (OR: 4.58, 95% CI: 1.53– 6.02, P-trend = 0.002) compared to the lowest quartile. VAI predicted IR (AUC = 0.74) and NAFLD (AUC = 0.71) with moderate accuracy. Higher VAI quartiles were dose-dependently associated with reduced reproductive success (P-trend < 0.01).
Conclusion: VAI is a practical, non-invasive tool for identifying metabolic dysfunction and predicting adverse pregnancy outcomes in women with PCOS, supporting its use for risk stratification and early intervention.
Keywords: polycystic ovary syndrome, visceral adiposity index, insulin resistance, metabolic syndrome, pregnancy outcomes
Introduction
Polycystic ovary syndrome (PCOS) is a common gynecological endocrine disorder in reproductive-aged women, with an estimated prevalence ranging from 5% to 18% worldwide.1 Diagnostically, it is characterized by clinical/biochemical hyperandrogenemia (HA), chronic oligo-ovulation, and polycystic ovarian morphology.2 Beyond these core features, the syndrome frequently presents with a spectrum of metabolic disturbances, including insulin resistance (IR), obesity, type 2 diabetes mellitus (T2DM), non-alcoholic fatty liver disease (NAFLD), and atherogenic dyslipidemia.3–7 Importantly, PCOS predisposes patients to serious long-term sequelae, such as infertility, cardiovascular disease (CVD), and endometrial carcinoma.8–10 Additionally, PCOS is now recognized as a multisystem condition that adversely affects mental health, manifesting as anxiety, depression, disordered eating patterns, negative body image—all of which contribute to substantially impaired quality of life throughout the lifespan.1,11,12
Overweight/obesity is a major clinical feature of PCOS patients and significantly exacerbates metabolic risks.13 While body mass index (BMI) is usually utilized to assess for obesity, it cannot reflect overall obesity and quantify visceral adiposity. Growing evidence indicates that fat accumulation, particularly visceral adipose tissue, is more closely associated with metabolic syndrome (MetS) such as diabetogenic, atherogenic, prothrombotic and proinflammatory metabolic abnormalities.14 The visceral adiposity index (VAI) overcomes this limitation by anthropometric and laboratory-measured parameters, providing superior prediction of MetS, T2DM, and CVD.15–17 A cross-sectional study has confirmed that VAI serves as a sensitive marker for visceral adipose dysfunction and MetS risk in PCOS patients.18 Another study also found that VAI levels were elevated in overweight/obese PCOS patients and were correlated with IR.19 However, these studies have primarily focused on the association between VAI and metabolic outcomes, and have not thoroughly investigated its relationship with reproductive outcomes, such as ovulation rates and pregnancy complications. Given the clinical implications, this association urgently requires further research.
The present study aimed to comprehensively evaluate the VAI in PCOS patients by examining its associations with clinical characteristics and metabolic profiles; as the first large-scale study, it specifically investigated the dose-response relationship between VAI and a complete spectrum of pregnancy outcomes (from ovulation to live birth); and further assessed its predictive utility for IR and NAFLD in this high-risk population.
Material and Methods
Target Population
This study constituted a secondary analysis derived from the Polycystic Ovary Syndrome Acupuncture and Clomiphene Trial (PCOSAct), which was carried out at 27 clinical sites throughout mainland China from 2011 to 2015. A total of 1000 infertile women diagnosed with PCOS, aged 20–40 years, were randomly and equally allocated to one of four intervention groups: (1) clomiphene combined with active acupuncture, (2) placebo plus active acupuncture, (3) clomiphene with sham acupuncture, or (4) placebo alongside sham acupuncture. All participants received and completed four consecutive menstrual cycles of the assigned intervention. The trial design, intervention protocols, and primary outcome results have been previously detailed in published literature.20,21 The study protocol received ethical approval from the Ethics Committee of the First Affiliated Hospital of Heilongjiang University of Chinese Medicine (Approval No. 2010HZYLL-010) and was registered on chictr.org.cn (ChiCTR-TRC-12002081) and ClinicalTrials.gov (NCT01573858).
Anthropometric Measurements
At baseline, we collected age, height, weight, body mass index (BMI), waist circumference (WC), hip circumference (HC), waist‑to‑hip ratio (WHR), systolic and diastolic blood pressure (SBP and DBP), and clinical signs of hyperandrogenism (hirsutism, acne, acanthosis nigricans).
Biochemical Measurements
Fasting blood samples were obtained on day 3 of the menstrual cycle. Measured parameters included fasting blood glucose (FBG) and fasting insulin (FINS). Insulin resistance was assessed using the homeostasis model assessment-insulin resistance (HOMA-IR), calculated as [FBG × FINS] / 22.5,22 and the quantitative insulin sensitivity check index (QUICKI), determined as 1 / [log FINS + log FBG].23 Lipid profiles comprised high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides (TG), total cholesterol (TC), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), the ApoB/ApoA1 ratio, and lipoprotein(a) (Lp[a]). The VAI was calculated using the formula: [WC / (36.58 + 1.89 × BMI)] × [TG / 0.81] × [1.52 / HDL].24
Reproductive and endocrine biomarkers included progesterone (P), total testosterone (TT), free testosterone (FT), sex hormone-binding globulin (SHBG), free androgen index (FAI, calculated as [TT / SHBG] × 100), luteinizing hormone (LH), follicle-stimulating hormone (FSH), the LH/FSH ratio, estradiol (E2), and anti-Müllerian hormone (AMH). Hepatic function parameters consisted of alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TB), direct bilirubin (DB), indirect bilirubin (IDB), and total bile acid (TBA). Renal and cardiac enzyme markers included blood urea nitrogen (BUN), creatinine (Cr), beta 2-microglobulin (B2M), cystatin C (CysC), lactate dehydrogenase (LDH), creatine kinase (CK), creatine kinase MB isoenzymes (CK-MB), and homocysteine (HCY).
IR was defined as HOMA-IR ≥ 2.69.25 MetS was diagnosed according to criteria for Chinese women, requiring at least three of the following: WC ≥ 85 cm; SBP ≥ 130 mmHg and/or DBP ≥ 85 mmHg; TG ≥ 1.7 mmol/L; HDL < 1.04 mmol/L; or FBG ≥ 6.1 mmol/L.26 NAFLD was identified based on prior medical records indicating a diagnosis of fatty liver disease, typically established by abdominal ultrasonography performed during routine health examinations. No additional standardized imaging or biopsy was conducted within the trial.
Pregnancy Outcomes
Ovulation was confirmed by a serum P level exceeding 5 ng/mL. Conception was identified as a serum human chorionic gonadotropin (hCG) concentration greater than 10 IU/L, at which point all study interventions were ceased. Pregnancy was verified via transvaginal ultrasound as the presence of an intrauterine gestation with detectable fetal cardiac activity. Live birth was defined as the delivery of a viable infant after 20 weeks of gestation. Pregnancy losses, calculated among participants who achieved a conception, included miscarriages, fetal deaths, and stillbirths.
Statistical Analysis
Data were analyzed using SPSS Statistics (version 26.0; IBM SPSS, Inc., Chicago, IL, USA). Continuous variables are expressed as means ± standard deviations, and categorical variables as frequencies and percentages. Linear trend tests were employed to compare anthropometric and biochemical parameters, as well as the prevalence of IR, MetS, NAFLD, and pregnancy outcomes across VAI quartiles. Linear regression was used to examine correlations between VAI and biochemical measures. Multivariable logistic regression was performed to estimate odds ratio (OR) and 95% confidence interval (CI) for the associations of VAI (as independent variable) with IR, NAFLD, and pregnancy outcomes (as dependent variables). Receiver operating characteristic (ROC) curves were generated to evaluate the predictive performance of VAI for IR and NAFLD; the area under the curve (AUC), optimal cutoff value, sensitivity, specificity, and Youden index were derived accordingly. A P-value < 0.05 was considered statistically significant.
Results
Of the original 1000 participants, 44 were excluded due to incomplete data required for VAI calculation (missing WC, BMI, TG, or HDL-C values). Thus, 956 participants were included in the final analysis. Based on the distribution within this cohort, they were classified into four VAI quartiles: quartile 1 (Q1) ≤ 1.29, n = 238; quartile 2 (Q2) 1.30–2.10, n = 240; quartile 3 (Q3) 2.11–3.59, n = 238; and quartile 4 (Q4) > 3.59, n = 239.
The Anthropometric, Biochemical Characteristics, Prevalence of IR, MetS, NAFLD and Pregnancy Outcomes Across the Quartiles of VAI
As shown in Table 1 and Table S1, across ascending VAI quartiles, all anthropometric measures significantly increased except hirsutism score. Significant positive trends (all P-trend < 0.001) were observed for markers of dysglycemia (including FBG, FINS and HOMA-IR) and dyslipidemia (including LDL, TG, TC, ApoB and ApoB/ApoA1), alongside declining QUICKI, HDL, and ApoA1. Sex hormone profiles showed increases in FT and FAI and decreases in P, SHBG, LH, FSH, LH/FSH, E2, and AMH (all P-trend < 0.01). Hepatic (ALT, AST) and renal markers (B2M, CysC) increased, whereas bilirubin components (TB, DB) and TBA decreased. Cardiac markers LDH rose, and CK-MB levels exhibited a nonlinear U-shaped relationship (all P-trend < 0.05). The prevalence of IR, MetS, and NAFLD significantly increased (all P-trend < 0.001). Adverse trends in reproductive outcomes included declining ovulation, conception per cycle, pregnancy and live birth rates, and increasing pregnancy loss (all P-trend < 0.01). No significant linear trends were detected for LP, TT, IDB, BUN, Cr, HCY, or CK (all P-trend > 0.05).
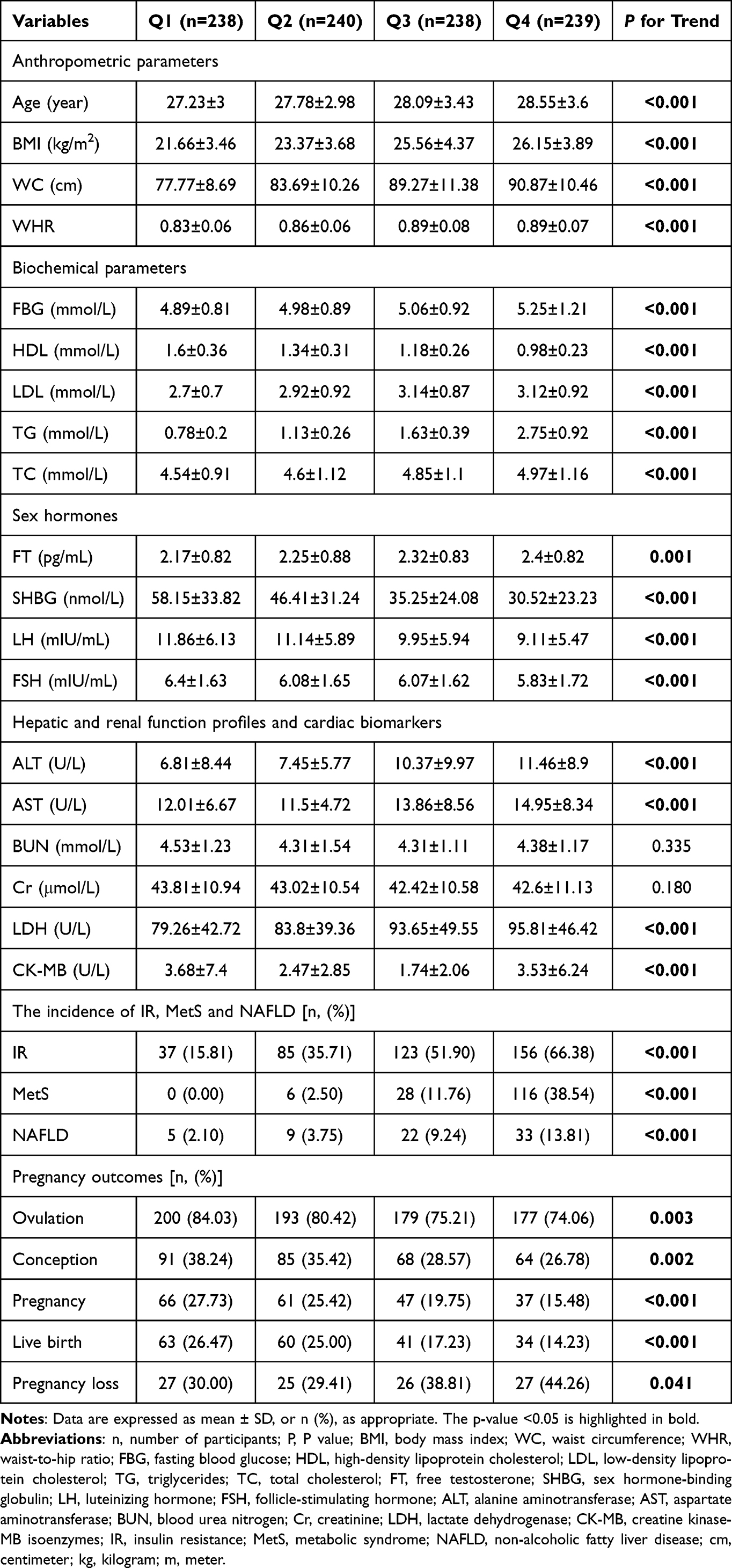 |
Table 1 Clinical and Biochemical Characteristics Across Quartile of VAI |
Linear Regression Analysis Between the VAI and Anthropometric, Biochemical Characteristics
VAI exhibited significant linear correlations with BMI, WC, HC, WHR, SBP, DBP, acanthosis nigricans score, mean menstrual cycle, FBG, FINS, HOMA-IR, QUICKI, HDL, LDL, TG, TC, ApoA1, ApoB, ApoB/ApoA1, FT, SHBG, FAI, LH, FSH, LH/FSH, AMH, ALT, AST, TB, DB, B2M, CysC, and LDH (all P < 0.05). However, after age adjustment, the association with TBA was no longer significant (Table 2 and Table S2).
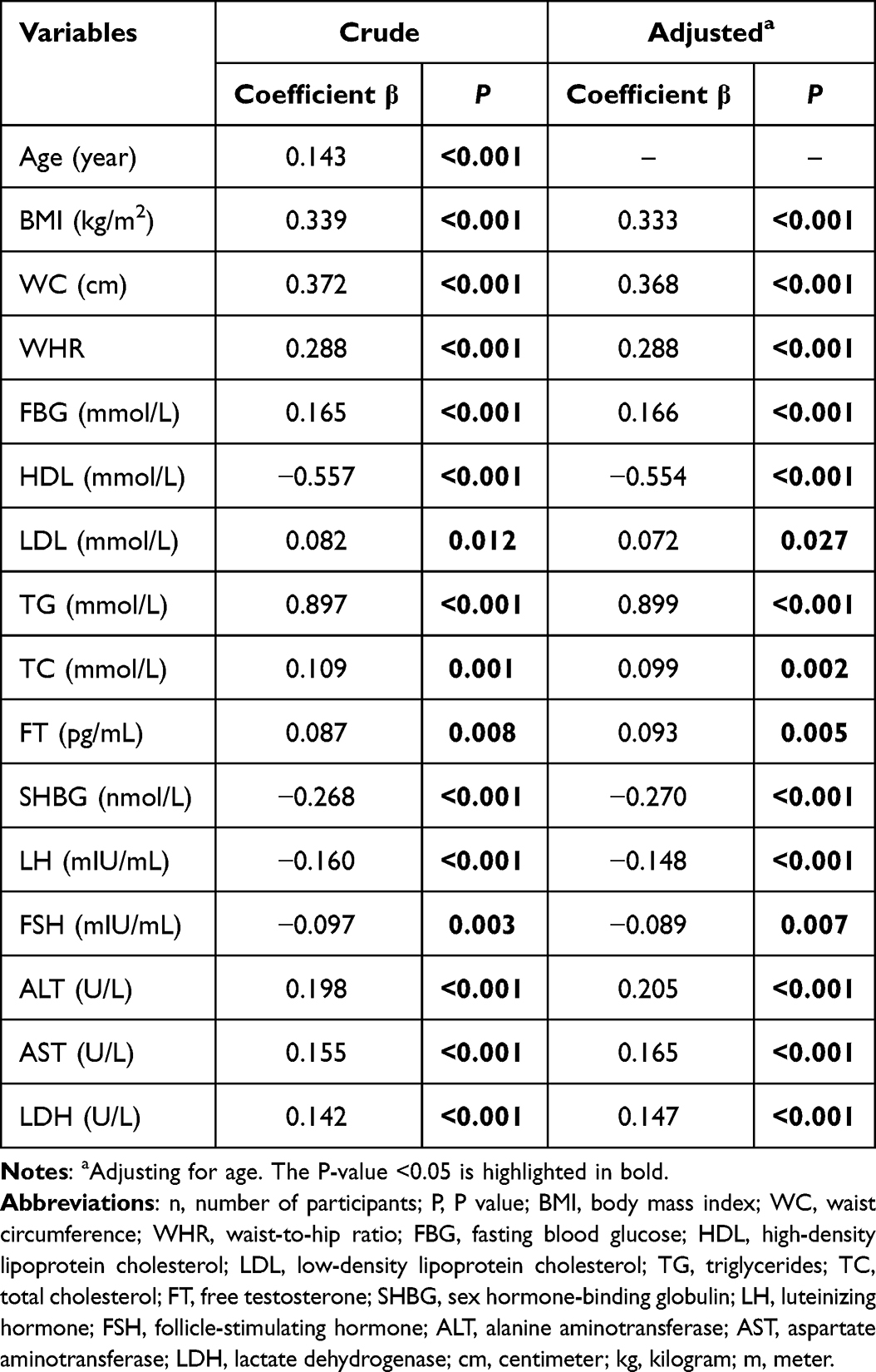 |
Table 2 Linear Associations Between the VAI and Clinical and Biochemical Parameters |
Logistic Regression Analysis Between VAI Quartiles and IR and NAFLD
As shown in Table 3, both univariate and age-adjusted logistic regression revealed associations between increased VAI and elevated risk of both IR and NAFLD. After further adjustment for LDL, TC, ApoB, ApoA1, ApoB/ApoA1, FT, SHBG, FAI, LH, FSH, LH/FSH and AMH, VAI remained significantly associated with increased IR risk (OR: 4.58, 95% CI: 2.35–8.93, P < 0.001 in Q4 vs Q1), with the highest OR for IR. However, the association with NAFLD was no longer significant (OR: 1.56, 95% CI: 0.45–5.43, P > 0.05).
 |
Table 3 Adjusted OR (95% CI) for the Associations Between the VAI and the Risk of IR and NAFLD |
Logistic Regression Analysis Between VAI Quartiles and Pregnancy Outcomes
Using the Q4 as reference, Q1-Q3 demonstrated progressively improved pregnancy outcomes in both unadjusted and treatment-adjusted logistic regression models (Table 4). Q1 consistently exhibited the strongest protective associations, showing significantly higher odds of ovulation (OR: 1.84, 95% CI: 1.17–2.90, P-trend = 0.003), conception (OR: 1.69, 1.15–2.50; P-trend = 0.002), clinical pregnancy (OR: 2.10, 1.33–3.29, P < 0.001), and live birth (OR: 2.17, 1.37–3.45, P-trend < 0.001) compared to Q4. These associations remained significant after treatment adjustment. No significant association was observed between VAI quartiles and pregnancy loss (P-trend > 0.05).
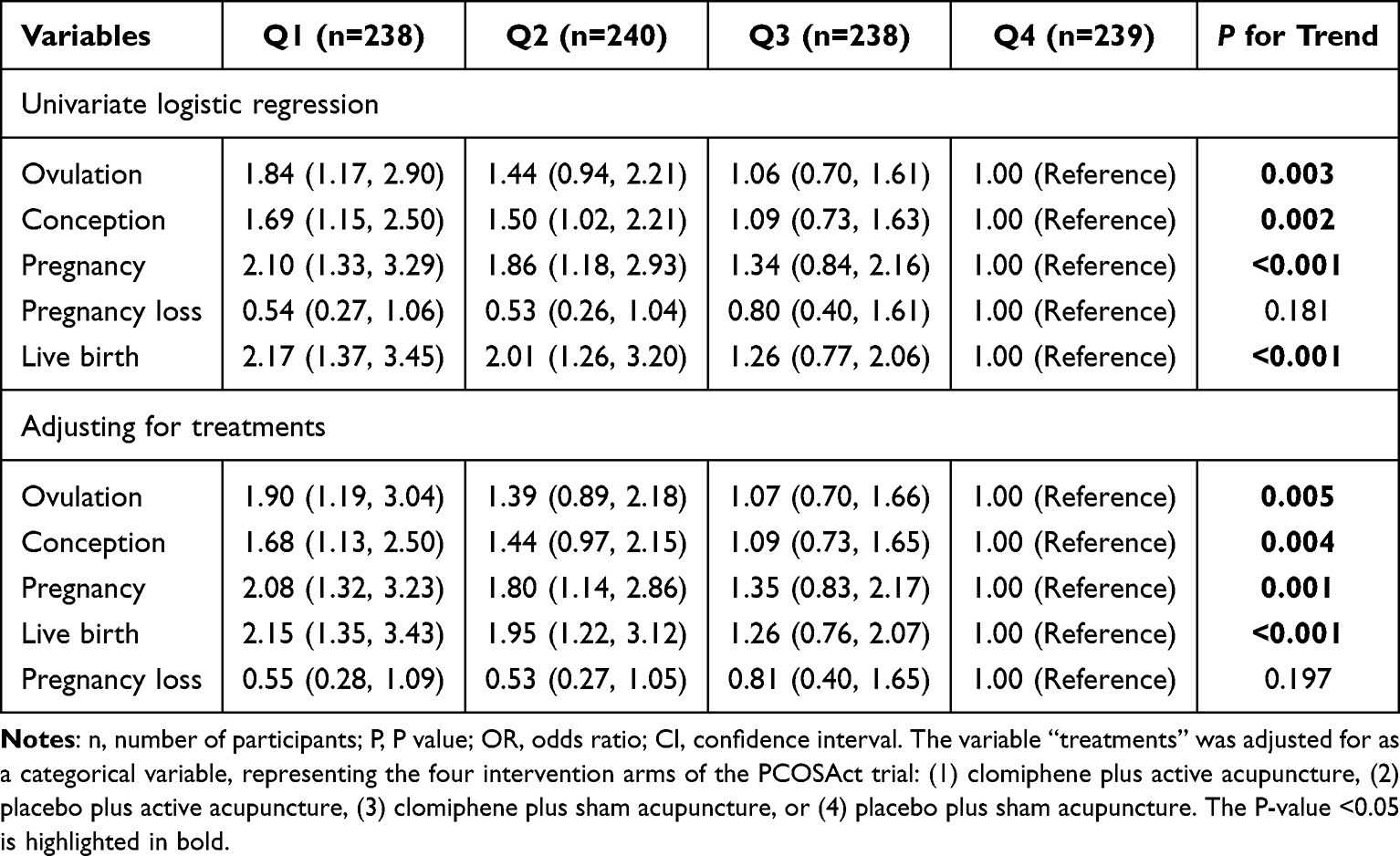 |
Table 4 Logistic Regression Analysis of VAI Quartiles and Pregnancy Outcomes |
Diagnostic Performance of VAI for IR and NAFLD
Figure 1 illustrates the ROC curves assessing VAI’s predictive capacity for IR (Panel a) and NAFLD (Panel b). For IR prediction, VAI (AUC = 0.74, cutoff = 2.07, Youden index = 0.367) demonstrated comparable diagnostic performance to HOMA-IR, with 69.1% sensitivity and 67.6% specificity. For NAFLD prediction, VAI showed moderate predictive accuracy (AUC = 0.71, cutoff = 2.21, Youden index = 0.343) with 79.7% sensitivity and 54.6% specificity.
 |
Figure 1 The results of ROC curve analysis regarding the predictability of VAI in IR (a) and NAFLD (b). |
Discussion
The current study demonstrates that elevated VAI is significantly associated with adverse anthropometric profiles, dysregulated glucolipid metabolism, and altered hepatic-renal function biomarkers in women with PCOS. It emerges as a valuable predictor for IR and NAFLD and may serve as a clinical indicator for pregnancy outcomes following ovulation induction in this population.
The VAI was initially developed as a sex-specific biomarker based on WC, BMI, TG, and HDL-C levels in a cohort of 315 non-obese, healthy individuals.24 This novel index demonstrated significant associations with MetS components and predicted increased CVD risk in its original validation study.24 WC reflects visceral fat accumulation, whereas BMI indicates general obesity; both are established predictors of IR.27,28 Excessive adipocyte accumulation and adipose tissue expansion promote the release of free fatty acids and inflammatory cytokines,29,30 which impair insulin signaling pathways and create a vicious cycle of lipotoxicity and glucotoxicity, thereby exacerbating IR. Moreover, when TG deposition in skeletal muscle exceeds 5% of tissue weight, it significantly worsens IR.31 Similarly, hepatic TG content exceeding 5% of liver weight defines NAFLD, with hypertriglyceridemia representing a direct biochemical manifestation of impaired hepatic lipid metabolism.32 These findings collectively support VAI as a clinically valuable biomarker for assessing glucolipid metabolic disturbances in the pathophysiology of PCOS.
In assessing IR prediction, our study demonstrates the significant discriminative value of VAI. IR manifests as impaired responsiveness to insulin stimulation in target tissues.33 The hyperinsulinemic-euglycemic clamp (HIEC), the gold standard for quantifying insulin sensitivity, documented a 27% decrease in insulin sensitivity in women with PCOS compared to healthy controls, independent of BMI.34 Notably, a HIEC-based study evaluating IR prevalence in PCOS women revealed an overall rate of 74.9%, with prevalence varying across BMI strata: 59.3% in normal-weight, 77.5% in overweight, and 93.9% in obese individuals.35 While our HOMA-IR assessed IR prevalence (41.99%) was lower than clamp-based estimates, the Q4 showed markedly elevated prevalence (66.38%). Furthermore, we observed significant correlations between VAI and MetS components (WC, SBP, DBP, FBG, HDL and TG), IR-related indices (FINS, HOMA-IR and QUICKI), and lipid profiles (LDL, TC, ApoB, ApoA1 and ApoB/ApoA1), all of which persisted after age adjustment. Consistent with much evidence, our logistic regression revealed an increased IR risk (OR: 4.58, 95% CI: 2.35–8.93) in the Q4 versus Q1, which was comparable to Jiang et al’s findings in a US cohort (OR: 1.28, 95% CI: 1.2–1.37),36 Oh et al’s Korean PCOS data (β = −0.93),37 and Bozorgmanesh’s report on diabetes risk (HR = 4.5, 95% CI: 3.0–6.9).38 Furthermore, the optimal VAI cutoff of 2.07 provided sensitivity (69.1%) and specificity (67.6%) with an AUC of 0.74, collectively establishing VAI as a clinically useful IR predictor in PCOS.
Hepatic TG deposition in lipid droplets is a key driver of hepatic steatosis, and elevated serum TG levels correlate directly with NAFLD severity—including inflammatory activity and fibrosis progression. In particular, NAFLD patients with TG ≥1.7 mmol/L face heightened risks of progression to non-alcoholic steatohepatitis (NASH) and extrahepatic organ injury.39 Multiple clinical studies support the value of VAI in NAFLD risk stratification. For instance, Xu et al40 reported an increased NAFLD risk (HR = 2.13, 95% CI: 1.86–2.45) in the highest versus lowest VAI quartile, while Ismaiel et al41 recorded that VAI’s predictive capacity for both NAFLD (AUC = 0.767) and NASH (AUC = 0.732). Similarly, unadjusted models from another study showed VAI predicted NAFLD with an AUC of 0.767 and a Youden index of 0.417 (P < 0.05), and its performance further improved after covariate adjustment (AUC = 0.83, Youden index = 0.518).42 Our study also demonstrated comparable predictive accuracy for NAFLD (AUC = 0.71, cutoff = 2.21, sensitivity = 79.7%, specificity = 54.6%), supporting VAI’s utility as an initial screening tool for high-risk PCOS populations. Beyond NAFLD, VAI shows broader clinical relevance. Chen et al42 expounded significant positive associations between increasing WC, VAI, lipid accumulation product, Chinese visceral adiposity index and NAFLD prevalence – partially consistent with our observations. Moreover, Wang et al17 further established VAI as a dose-dependent predictor of CVD/cardiovascular death. Crucially, in our study, VAI maintained significant multivariable-adjusted associations with hepatic enzymes (ALT, AST), bilirubin fractions (TB, DB), and renal/cardiac biomarkers (B2M, CysC, and LDH). This multi-organ relevance is further corroborated by existing literature. Petta et al43 and Van der Poorten et al44 confirmed significant associations between elevated VAI and both hepatic inflammatory activity and fibrosis severity, whereas Thi et al45 and Lin et al46 elucidated that obesity enhanced intrarenal renin-angiotensin-aldosterone system activation, correlating significantly with renal impairment risk. Additionally, experimental models further indicated that visceral adipose tissue induced myocardial LDH elevation via oxidative-inflammatory pathways—a phenomenon attenuated by antioxidant intervention.47 Collectively, VAI serves as a non-invasive, clinically informative biomarker that reflects visceral adiposity and its systemic metabolic repercussions.
Elevated VAI was robustly correlated with adverse pregnancy outcomes in this study, a relationship likely mediated through aggravated metabolic dysfunction encompassing IR, obesity, and HA. Among Chinese women with PCOS, we observed a dose-dependent deterioration in reproductive metrics across increasing VAI quartiles, reflected in progressively reduced rates of ovulation, conception, clinical pregnancy, and live birth. Elevated VAI demonstrated significant correlations with increased TT and decreased SHBG,48 establishing a “HA-IR axis”. This axis likely originates from visceral adipose tissue potentiating ovarian theca cell androgen synthesis through hyperinsulinemia. Subsequent peripheral aromatization of androgens to estrogens within adipose tissue disrupts hypothalamic-pituitary-ovarian axis regulation, driving gonadotropin secretion imbalances.49 Complementing these mechanisms, Zeng et al50 identified an independent inverse correlation between AMH and visceral adiposity – potentially mediated through hyperinsulinemia downregulating AMH gene expression (reducing preantral follicle recruitment) or via oxidative stress/inflammatory damage to ovarian granulosa cells. Successful embryo implantation requires optimal endometrial receptivity, which is compromised through dual visceral adipose-mediated pathways: pro-inflammatory adipokines deplete uterine natural killer cell populations, disrupting immunotolerance; and hyperinsulinemia downregulates endometrial glucose transporter 4 expression.51 This combined impairment of immunomodulatory capacity and glucose hypometabolism induces endometrial dysfunction, ultimately diminishing implantation potential. Post-conception, visceral adiposity-driven hyperglycemia and dyslipidemia compromise placental vascular development, promoting adverse pregnancy outcomes.52 The hyperandrogenic milieu associated with obesity and IR heightens uterine artery vascular tone, impairing uteroplacental perfusion.53 Concurrently, elevated placental inflammatory markers induce aberrant trophoblast function.54 Collectively, these mechanisms reduce ongoing pregnancy and live birth rates.
An interesting discrepancy was noted in the analysis of pregnancy loss. While a significant increasing trend across VAI quartiles was observed in Table 1, this association was attenuated and lost statistical significance in Table 4. This discrepancy likely stems from the adjustment for potential confounders in the multivariate model, which provides a more robust estimate of VAI’s independent effect. Furthermore, although the overall sample size was substantial, the limited number of pregnancy loss events (n = 105) may reduce the statistical power to detect a significant independent association in adjusted analyses. Therefore, the findings from the adjusted models, which indicate no statistically independent association between VAI and pregnancy loss, should be considered the more reliable interpretation.
The primary strength of this study is the systematic validation of VAI as a practical, non-invasive marker for metabolic and reproductive risk stratification in a large, well-characterized PCOS cohort. By integrating four routine clinical parameters, VAI offers a feasible tool for estimating visceral adiposity and its related dysfunctions. We confirm its predictive value for IR and NAFLD and extend its relevance to hepatic and renal biomarkers. Most notably, we report, for the first time, a clear dose-dependent relationship between VAI and a spectrum of pregnancy outcomes following ovulation induction.
Several limitations must be acknowledged. First, the cross-sectional design of this secondary analysis precludes the assessment of causal relationships or the dynamic changes in VAI over time and during pregnancy. Second, the lack of a non-PCOS control group limits the generalizability of the findings to other populations and the ability to make direct comparative risk assessments. Third, the diagnosis of NAFLD relied on non-standardized criteria (abdominal ultrasonography), which may affect diagnostic accuracy and comparability with studies using more precise techniques like controlled attenuation parameter or liver biopsy. Fourth, the number of certain pregnancy outcome events, particularly pregnancy loss, was relatively limited, which may constrain the statistical power of related multivariate analyses. Finally, VAI was calculated from a single baseline measurement; serial assessments could provide deeper insights into its temporal relationship with metabolic and reproductive changes.
This study supports the integration of the VAI into the routine metabolic assessment of women with PCOS. For individuals with elevated VAI, more proactive metabolic screening—including evaluation for IR and NAFLD—and lifestyle interventions are recommended. In the context of reproductive medicine, VAI may serve as an auxiliary tool for assessing baseline metabolic risk prior to ovulation induction, facilitating personalized counseling and treatment modification. Future research should prioritize longitudinal studies to clarify the temporal relationship and potential causal role of VAI in the progression of metabolic dysfunction and reproductive outcomes in PCOS. Interventional studies are necessary to determine whether strategies aimed at reducing VAI—such as lifestyle modification, insulin-sensitizing agents, or metabolic surgery—can effectively improve metabolic health and pregnancy success rates. Furthermore, validating standardized VAI cut-off points for specific clinical endpoints (eg, ovulation or live birth) across diverse PCOS populations would significantly enhance its clinical utility. Integrating VAI with other novel biomarkers or imaging techniques also holds promise for optimizing comprehensive risk-prediction models.
Conclusion
In conclusion, VAI serves as a valuable, accessible clinical tool for identifying Chinese women with PCOS who are at heightened risk for metabolic dysregulation, including IR and NAFLD, and for poorer reproductive outcomes. Its implementation in clinical settings could enhance early risk stratification, guide personalized monitoring, and inform targeted intervention strategies, ultimately improving the comprehensive management of this complex condition.
Data Sharing Statement
Data available upon request to corresponding author.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. The study was approved by the First Affiliated Hospital, Heilongjiang University of Chinese Medicine. The participants provided their written informed consent to participate in this study.
Funding
This work is supported by (1) The National key R&D Program of China (2019YFC1709500); (2) The National Collaboration Project of Critical Illness by Integrating Chinese Medicine and Western Medicine; (3) Project of Heilongjiang Province Innovation Team “TouYan” (LH2019H046); (4) Heilongjiang Provincial Clinical Research Centre for Ovary Diseases (LC2020R009); (5) Traditional Chinese Medicine Research Project of Heilongjiang Administration of Traditional Chinese Medicine (ZHY2022-124); (6) The project of Evidence-based capacity in Traditional Chinese Medicine (TCM Sci-Tech Internal Letter [2023] No. 24).
Disclosure
The authors declared no conflicts of interest in this work.
References
1. Joham AE, Norman RJ, Stener-Victorin E, et al. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022;10(9):668–12. doi:10.1016/S2213-8587(22)00163-2
2. Hoeger KM, Dokras A, Piltonen T. Update on PCOS: consequences, challenges, and guiding treatment. J Clin Endocrinol Metab. 2021;106(3):e1071–e1083. doi:10.1210/clinem/dgaa839
3. Rahmatnezhad L, Moghaddam-Banaem L, Behroozi-Lak T, Shiva A, Rasouli J. Association of insulin resistance with polycystic ovary syndrome phenotypes and patients’ characteristics: a cross-sectional study in Iran. Reprod Biol Endocrinol. 2023;21(1):113. doi:10.1186/s12958-023-01160-z
4. Amiri M, Hatoum S, Hopkins D, et al. The association between obesity and polycystic ovary syndrome: an epidemiologic study of observational data. J Clin Endocrinol Metab. 2024;109(10):2640–2657. doi:10.1210/clinem/dgae488
5. Choudhury AA, Rajeswari VD. Polycystic ovary syndrome (PCOS) increases the risk of subsequent gestational diabetes mellitus (GDM): a novel therapeutic perspective. Life Sci. 2022;310:121069. doi:10.1016/j.lfs.2022.121069
6. Wu J, Yao XY, Shi RX, Liu SF, Wang XY. A potential link between polycystic ovary syndrome and non-alcoholic fatty liver disease: an update meta-analysis. Reprod Health. 2018;15(1):77. doi:10.1186/s12978-018-0519-2
7. Zhang J, Fan P, Liu H, Bai H, Wang Y, Zhang F. Apolipoprotein A-I and B levels, dyslipidemia and metabolic syndrome in south-west Chinese women with PCOS. Hum Reprod. 2012;27(8):2484–2493. doi:10.1093/humrep/des191
8. Liu X, Zhang J, Wang S. Global, regional, and national burden of infertility attributable to PCOS, 1990-2019. Hum Reprod. 2024;39(1):108–118. doi:10.1093/humrep/dead241
9. Guan C, Zahid S, Minhas AS, et al. Polycystic ovary syndrome: a “risk-enhancing” factor for cardiovascular disease. Fertil Steril. 2022;117(5):924–935. doi:10.1016/j.fertnstert.2022.03.009
10. Haoula Z, Salman M, Atiomo W. Evaluating the association between endometrial cancer and polycystic ovary syndrome. Hum Reprod. 2012;27(5):1327–1331. doi:10.1093/humrep/des042
11. Stener-Victorin E, Teede H, Norman RJ, et al. Polycystic ovary syndrome. Nat Rev Dis Primers. 2024;10(1):27. doi:10.1038/s41572-024-00511-3
12. Jannink T, Bordewijk EM, Aalberts J, et al. Anxiety, depression, and body image among infertile women with and without polycystic ovary syndrome. Hum Reprod. 2024;39(4):784–791. doi:10.1093/humrep/deae016
13. Mongraw-Chaffin M, Foster MC, Anderson CAM, et al. Metabolically healthy obesity, transition to metabolic syndrome, and cardiovascular risk. J Am Coll Cardiol. 2018;71(17):1857–1865. doi:10.1016/j.jacc.2018.02.055
14. Després JP. Is visceral obesity the cause of the metabolic syndrome? Ann Med. 2006;38(1):52–63. doi:10.1080/07853890500383895
15. Lazzer S, D’Alleva M, Isola M, et al. Cardiometabolic index (CMI) and visceral adiposity index (VAI) highlight a higher risk of metabolic syndrome in women with severe obesity. J Clin Med. 2023;12(9):3055. doi:10.3390/jcm12093055
16. Zhou H, Li T, Li J, Zhuang X, Yang J. The association between visceral adiposity index and risk of type 2 diabetes mellitus. Sci Rep. 2024;14(1):16634. doi:10.1038/s41598-024-67430-x
17. Wang R, Liu J, Fang G, Shi J, Zhang C, Huang Y. Association between visceral adiposity index and cardiovascular disease: a systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. 2025;35(12):104216. doi:10.1016/j.numecd.2025.104216
18. Rocha ALL, Baêta T, Nazareth IR, et al. The role of the visceral adiposity index in the assessment of metabolic syndrome of polycystic ovary syndrome patients: a new anthropometric index. Arch Gynecol Obstet. 2024;309(4):1643–1649. doi:10.1007/s00404-023-07328-7
19. Durmus U, Duran C, Ecirli S. Visceral adiposity index levels in overweight and/or obese, and non-obese patients with polycystic ovary syndrome and its relationship with metabolic and inflammatory parameters. J Endocrinol Invest. 2017;40(5):487–497. doi:10.1007/s40618-016-0582-x
20. Kuang H, Li Y, Wu X, et al. Acupuncture and clomiphene citrate for live birth in polycystic ovary syndrome: study design of a randomized controlled trial. Evidence-Based Complementary Alternative Med. 2013;2013(1):527303. doi:10.1155/2013/527303
21. Wu X-K, Stener-Victorin E, Kuang H-Y, et al. Effect of acupuncture and clomiphene in Chinese women with polycystic ovary syndrome: a randomized clinical trial. JAMA. 2017;317(24):2502–2514. doi:10.1001/jama.2017.7217
22. Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. 2004;27(6):1487–1495. doi:10.2337/diacare.27.6.1487
23. Gutch M, Kumar S, Razi SM, Gupta KK, Gupta A. Assessment of insulin sensitivity/resistance. Indian J Endocrinol Metab. 2015;19(1):160–164. doi:10.4103/2230-8210.146874
24. Amato MC, Giordano C, Galia M, et al. Visceral adiposity index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33(4):920–922. doi:10.2337/dc09-1825
25. Jayanthi R, Srinivasan AR, Hanifah M, Maran AL. Associations among Insulin resistance, triacylglycerol/high density lipoprotein (TAG/HDL ratio) and thyroid hormone levels—a study on type 2 diabetes mellitus in obese and overweight subjects. Diabetes Metab Syndr. 2017;11:S121–S126. doi:10.1016/j.dsx.2016.12.020
26. Society CD. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition) (Part 1). Chin J Pract Internal Med. 2021;41(08):668–695. doi:10.19538/j.nk2021080106
27. Ramírez-Manent JI, Jover AM, Martinez CS, Tomás-Gil P, Martí-Lliteras P, López-González ÁA. Waist circumference is an essential factor in predicting insulin resistance and early detection of metabolic syndrome in adults. Nutrients. 2023;15(2):257. doi:10.3390/nu15020257
28. Sinaiko AR, Steinberger J, Moran A, et al. Relation of body mass index and insulin resistance to cardiovascular risk factors, inflammatory factors, and oxidative stress during adolescence. Circulation. 2005;111(15):1985–1991. doi:10.1161/01.CIR.0000161837.23846.57
29. Garg SS, Kushwaha K, Dubey R, Gupta J. Association between obesity, inflammation and insulin resistance: insights into signaling pathways and therapeutic interventions. Diabetes Res Clin Pract. 2023;200:110691. doi:10.1016/j.diabres.2023.110691
30. Gołacki J, Matuszek M, Matyjaszek-Matuszek B. Link between insulin resistance and obesity—from diagnosis to treatment. Diagnostics. 2022;12(7):1681. doi:10.3390/diagnostics12071681
31. Kelley DE. Skeletal muscle triglycerides: an aspect of regional adiposity and insulin resistance. Ann NY Acad Sci. 2002;967(1):135–145. doi:10.1111/j.1749-6632.2002.tb04271.x
32. Beaudry KM, Devries MC. Sex-based differences in hepatic and skeletal muscle triglyceride storage and metabolism. Appl Physiol Nutr Metab. 2019;44(8):805–813. doi:10.1139/apnm-2018-0635
33. Li M, Chi X, Wang Y, Setrerrahmane S, Xie W, Xu H. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduction Target Ther. 2022;7(1):216. doi:10.1038/s41392-022-01073-0
34. Cassar S, Misso ML, Hopkins WG, Shaw CS, Teede HJ, Stepto NK. Insulin resistance in polycystic ovary syndrome: a systematic review and meta-analysis of euglycaemic–hyperinsulinaemic clamp studies. Hum Reprod. 2016;31(11):2619–2631. doi:10.1093/humrep/dew243
35. Tosi F, Bonora E, Moghetti P. Insulin resistance in a large cohort of women with polycystic ovary syndrome: a comparison between euglycaemic-hyperinsulinaemic clamp and surrogate indexes. Hum Reprod. 2017;32(12):2515–2521. doi:10.1093/humrep/dex308
36. Jiang K, Luan H, Pu X, Wang M, Yin J, Gong R. Association between visceral adiposity index and insulin resistance: a cross-sectional study based on US adults. Front Endocrinol. 2022;13:921067. doi:10.3389/fendo.2022.921067
37. Oh JY, Sung YA, Lee HJ. The visceral adiposity index as a predictor of insulin resistance in young women with polycystic ovary syndrome. Obesity. 2013;21(8):1690–1694. doi:10.1002/oby.20096
38. Bozorgmanesh M, Hadaegh F, Azizi F. Predictive performance of the visceral adiposity index for a visceral adiposity-related risk: type 2 diabetes. Lipids Health Dis. 2011;10(1):1–9. doi:10.1186/1476-511X-10-88
39. Koller T, Kollerova J, Hlavaty T, Huorka M, Payer J. Cholelithiasis and markers of nonalcoholic fatty liver disease in patients with metabolic risk factors. Scand J Gastroenterol. 2012;47(2):197–203. doi:10.3109/00365521.2011.643481
40. Xu C, Ma Z, Wang Y, et al. Visceral adiposity index as a predictor of NAFLD: a prospective study with 4-year follow-up. Liver Int. 2018;38(12):2294–2300. doi:10.1111/liv.13941
41. Ismaiel A, Jaaouani A, Leucuta D-C, Popa S-L, Dumitrascu DL. The visceral adiposity index in non-alcoholic fatty liver disease and liver fibrosis—systematic review and meta-analysis. Biomedicines. 2021;9(12):1890. doi:10.3390/biomedicines9121890
42. Chen X, Shi F, Xiao J, et al. Associations between abdominal obesity indices and nonalcoholic fatty liver disease: chinese visceral adiposity index. Front Endocrinol. 2022;13:831960. doi:10.3389/fendo.2022.831960
43. Petta S, Amato M, Cabibi D, et al. Visceral adiposity index is associated with histological findings and high viral load in patients with chronic hepatitis C due to genotype 1. Hepatology. 2010;52(5):1543–1552. doi:10.1002/hep.23859
44. van der Poorten D, Milner KL, Hui J, et al. Visceral fat: a key mediator of steatohepatitis in metabolic liver disease. Hepatology. 2008;48(2):449–457. doi:10.1002/hep.22350
45. Thethi T, Kamiyama M, Kobori H. The link between the renin-angiotensin-aldosterone system and renal injury in obesity and the metabolic syndrome. Curr Hypertens Rep. 2012;14(2):160–169. doi:10.1007/s11906-012-0245-z
46. Lin M, Wu S, Deng X, Chen Y, Tan X. Visceral fat and its dynamic change are associated with renal damage: evidence from two cohorts. Ann Clin Exp Hypertens. 2023;45(1):2271187. doi:10.1080/10641963.2023.2271187
47. Ismail BS, Mahmoud B, Abdel-Reheim ES, et al. Cinnamaldehyde mitigates atherosclerosis induced by high-fat diet via modulation of hyperlipidemia, oxidative stress, and inflammation. Oxid Med Cell Longev. 2022;2022(1):4464180. doi:10.1155/2022/4464180
48. Xiangli L, Pengyi C, Wen T. Effects of visceral adiposity index of patients with polycystic ovary syndrome on their sex hormone levels and insulin resistance. Chin J Family Planning. 2022;30(02):365–369.
49. Lonardo MS, Cacciapuoti N, Guida B, et al. Hypothalamic-ovarian axis and adiposity relationship in polycystic ovary syndrome: physiopathology and therapeutic options for the management of metabolic and inflammatory aspects. Curr Obes Rep. 2024;13(1):51–70. doi:10.1007/s13679-023-00531-2
50. Zeng X, Huang Y, Zhang M, et al. Anti-Müllerian hormone was independently associated with central obesity but not with general obesity in women with PCOS. Endocr Connections. 2022;11(1). doi:10.1530/EC-21-0243
51. Bai X, Zheng L, Li D, Xu Y. Research progress of endometrial receptivity in patients with polycystic ovary syndrome: a systematic review. Reprod Biol Endocrinol. 2021;19(1):122. doi:10.1186/s12958-021-00802-4
52. Heslehurst N, Ngongalah L, Bigirumurame T, et al. Association between maternal adiposity measures and adverse maternal outcomes of pregnancy: systematic review and meta-analysis. Obesity Rev. 2022;23(7):e13449. doi:10.1111/obr.13449
53. Mishra JS, Kumar S. Activation of angiotensin type 2 receptor attenuates testosterone-induced hypertension and uterine vascular resistance in pregnant rats†. Biol Reprod. 2021;105(1):192–203. doi:10.1093/biolre/ioab051
54. Alfian I, Chakraborty A, Yong HEJ, et al. The placental NLRP3 inflammasome and its downstream targets, caspase-1 and interleukin-6, are increased in human fetal growth restriction: implications for aberrant inflammation-induced trophoblast dysfunction. Cells. 2022;11(9):1413. doi:10.3390/cells11091413
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tumor Necrosis Factor Alpha Level in the Uterine Fluid of Patients with Polycystic Ovary Syndrome and Its Correlation with Clinical Parameters
Ha LX, Li WX, Du YD, Yuan YY, Qu XX
Journal of Inflammation Research 2022, 15:6015-6020
Published Date: 29 October 2022
Omentin as an Independent Predictor of Metabolic Syndrome and Obesity Among Adolescents in Northeast China
Sun X, Li T, Tian Y, Ren S, Li L, Li P
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3913-3922
Published Date: 15 December 2022
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Correlation Between Hemoglobin Levels and Polycystic Ovary Syndrome Metabolic Disorder
Ha LX, Du YD, Qu XX, Wang JJ
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3019-3027
Published Date: 28 September 2023
Glycolytic Dysfunction in Granulosa Cells and Its Contribution to Metabolic Dysfunction in Polycystic Ovary Syndrome
Cao Z, Zhou Q, An J, Guo X, Jia X, Qiu Y
Drug Design, Development and Therapy 2025, 19:5255-5270
Published Date: 18 June 2025