")
Back to Journals » International Journal of Women's Health » Volume 15
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Received 25 January 2023
Accepted for publication 11 July 2023
Published 26 July 2023 Volume 2023:15 Pages 1197—1203
DOI https://doi.org/10.2147/IJWH.S405942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Walaa Mohammed Saeed,1 Fahad Alsehli2
1Department of Medical Laboratory Technology, Faculty of Applied Medical Science, Taibah University, Al Madinah Al Munawarah, Saudi Arabia; 2Pathology, King Salman Medical City, Madinah, Saudi Arabia
Correspondence: Walaa Mohammed Saeed, Department of Medical Laboratory Technology, Faculty of Applied Medical Science, Taibah University, 344, Postal Code 3000, Al Madinah Al Munawarah, Saudi Arabia, Tel +96506320307, Email [email protected]
Objective: The PCOS-thyroid nexus has recently drawn the focus of various investigations due to the prevalence of thyroid problems in PCOS. Additionally, risk factors for cardiovascular disease (CVD) are more prevalent in PCOS women. Therefore, we aim to assess the levels of thyroid hormones in Saudi females with polycystic ovary syndrome (PCOS) and to examine the correlation between cardiometabolic risk factors (CMRFs) and thyroid hormones in PCOS patients.
Methods: A cross-sectional research with 200 PCOS-diagnosed female patients was conducted from April 2018 to April 2020. In addition to other anthropometric and serum biochemical markers, glycemic status, thyroid function test, lipid profiles, homocysteine, and C-reactive protein levels were detected in patients.
Results: In PCOS, hypothyroidism is more common than hyperthyroidism (55 vs 27.5%, p = 0.05). While women with raised TSH (hypothyroidism) had a higher BMI, WC, FBG, and poorer HDL-C (p< 0.05). Significant differences were found in LDL-C, TG, Homocysteine, and CRP levels (all p< 0.001 and< 0.05). PCOS women with hypothyroidism at increased risk of CVD, as indicated by AIP (Atherogenic Index of plasma) (0.57± 0.42) was found. The elevated TSH levels were favorably linked with TG, Homocysteine, CRP, BMI, AIP, and WC (all p< 0.001, 0.05) but negatively connected with HDL-C and FT4.
Conclusion: A strong relationship between PCOS and thyroid dysfunction was detected since PCOS hypothyroid groups had higher TSH levels and CMRFs. This group’s CVD risk was elevated due to CRP, homocysteine, triglycerides, and obesity.
Keywords: thyroid disorder, insulin resistance, obesity, polycystic ovary syndrome, atherogenic index of plasma
Introduction
PCOS (polycystic ovary syndrome), which involves about one in 15% of women worldwide, is a heterogeneous endocrine disorder that is defined by oligo- or anovulation, clinical and/or biochemical signs of hyperandrogenism, and polycystic ovaries.1 The prevalence of PCOS represents 5–10% of women worldwide.1 The latest studies on Madinah females stated that 32.5% have PCOS with an average age of 21 ± 2 years. PCOS is a condition that affects a woman’s reproductive system, but it is also an endocrinopathy that may have serious consequences for her overall health. It has been established that PCOS and thyroid problems may impact fertility and reproductive biology.
What’s more noteworthy is that hypothyroidism may initiate, maintain, or exacerbate this disease.2 Due to the frequency of thyroid disorders in PCOS, the PCOS-thyroid nexus has been the recent interest of several studies.2,3 The bulk of the data indicated that PCOS patients were four times more likely to develop autoimmune thyroiditis and excessively elevated TSH levels.2,3 Many reproductive-aged women with PCOS also suffer from hypothyroidism. Ramanand et al found that 3–4% of women of reproductive age had hypothyroidism.4 It has been shown that the prevalence of hypothyroidism is above average (18% vs 6%).3 Numerous recent studies, however, have shown that women with PCOS have a greater chance of having thyroid disorders. Hyperthyroidism may contribute to some PCOS symptoms, including infertility, hypertension, irregular menstrual cycles, mental illnesses, and a low body mass index.5,6 Similarly, data indicates that 65% of women with hyperthyroidism had menstrual irregularities, compared to only 17% of women with normal thyroid function.7 According to another study, menstrual abnormalities caused by hyperthyroidism are 2.5 times more prevalent than the control group.8
Several studies have also shown that women with PCOS are more likely to have cardiovascular disease (CVD) risk factors such as hypertension, dyslipidemia, diabetes, and obesity, as well as raised C-reactive protein (CRP) or homocysteine levels.9–11 In addition, both clinical and subclinical, hyperthyroidism and hypothyroidism may contribute to the progression of CVD. Even modest changes in thyroid hormone levels elevate CVD mortality by 20% to 80%.12
Thyroid problems often substantially affect the CVD system through numerous mechanisms, such as dyslipidemia or hypertension. Further study of this kind is required to characterize the correlation between thyroid hormone levels and PCOS complications such as CVD, especially in Saudi Arabian females. Therefore, the study aims to assess the levels of thyroid hormones in Saudi females with PCOS and the relationship between thyroid hormones and PCOS comorbidities such as CVD.
Methods
A cross-sectional study included female patients already diagnosed with PCOS but not yet received treatments. Their age ranged from 20–35 years and was recruited from different hospitals in the Madinah region during the period of April 2018 to April 2020. Generally women between the ages of 20 and 40 were diagnosed with PCOS using the ROTTERDAM criterion were selected for study.13 200 healthy females as controls range age 18–33years without a history of irregularly menstruating or cardiovascular disease (CVD), diabetes or thyroid disorders, without clinically apparent of hyperandrogenism or pregnant, or menopause was included in the study. While, patients with congenital hypothyroidism or hyperthyroidism, CVD, diabetes, thyroidectomy patients, and a history of radiation to the neck and head in cancer patients were excluded from study. Before enrollment in the trial, each participant’s informed written permission was obtained.
Analysis of Blood Samples
Blood tests were conducted at Madinah hospital labs for thyroid-stimulating hormone (TSH), fasting blood glucose (FBG), homocysteine levels, triglyceride (TG), total cholesterol, high-density lipoprotein cholesterol (HDL-C), free tetraiodothyronine (FT4), low-density lipoprotein-cholesterol (LDL-C) and C-reactive protein (CRP). Meanwhile, 2 mL of the leftover blood sample was centrifuged (1000-x g, 5 minutes), then, the hormone levels in serums were evaluated by a completely quantitative ELISA-based chemiluminescent assay (CUSABIO Technology LLC, Houston, USA). All operations were done according to the manufacturer’s instructions provided by the lab in Madinah Hospitals. The normal values of homocysteine vary between 5 and 15 μmol/L and CRP < 10 mg/L.14 The reference ranges for TSH, and FT4 were set as 0.35 to 4.94 IU/mL and 0.70 to 1.48 ng/dL, respectively. Participants with thyroid dysfunction were divided into four groups: Primary hypothyroidism (a) is defined by a serum TSH level > 4.94 IU/mL and a low FT4 level (0.7 ng/dL); primary hyperthyroidism (b) is defined by a serum TSH level 0.35 IU/mL and a high FT4 level (> 1.48 ng/dL); and subclinical hypothyroidism (c) is defined by elevated TSH values with normal FT4 levels.15 In particular, the Atherogenic Index of plasma = log (TG/HDL-C) was also determined. AIP levels less than 0.11 suggest a low risk for CVD, whereas values between 0.11 and 0.21 indicate a moderate risk and values above 0.21 indicate a high risk.16
Anthropometric Measurements
Measurements of height and weight were performed. All measures were averaged after being assessed three times to compute the mean. The weight was calculated using an electronic scale. The height of a vertical wall was measured using a measuring tape. The body mass index was calculated using the subjects’ height and weight. Obesity (> 30.0 kg/m2), overweight (25.0–29.9Kg/m2), and normal weight (18.5–25.0Kg/m2) were determined based on the BMI.14 Three measurements of each participant’s waist were taken using a flexible but non-elastic measuring tape within half a centimetre. While waist circumference was taken at the level of the natural waist (the narrowest part of the torso) or one finger width under the umbilicus. Women who measured 88 centimeters or more around their waist were classified as being obese in their abdominal region, while those who measured less than 88 centimeters were classified as being normal in this area.14
Ethical Consideration
This study was authorized by Taibah University in Al Madinah Al Munawarah’s ethical committee (CLN201704) in the field of applied medical sciences.
Data Analysis
For statistical analysis, GraphPad Prism 7 (GraphPad Software, CA, USA) was utilized. In the quantitative statistics, percentages mean, and standard deviations all showed. Using a one-way analysis of variance (ANOVA), several continuous variables were compared across categories. Using Pearson’s correlation, thyroid hormone levels were associated with glucose, CRP, homocysteine, BMI, atherogenic index of plasma (AIP), and lipid profile. At the 5% significance level (p ≤ 0.05), all changes were determined to be statistically significant.
Results
PCOS Patients and Controls’ Clinical and Biochemical Features
Table 1 summarizes the clinical and biochemical features of PCOS and control women. It was found that PCOS participants had substantially higher BMI, waist circumference (WC), homocysteine, and CRP levels than control subjects (all p < 0.001). The value of AIP differs significantly between PCOS and control participants (0.5±0.16 vs 0.10±0.11, p = 0.002). In addition, TSH, TG, and total cholesterol (TC) levels were higher in PCOS than in controls (all p< 0.05); although FT4 and HDL-c levels were lower (all p < 0.05).
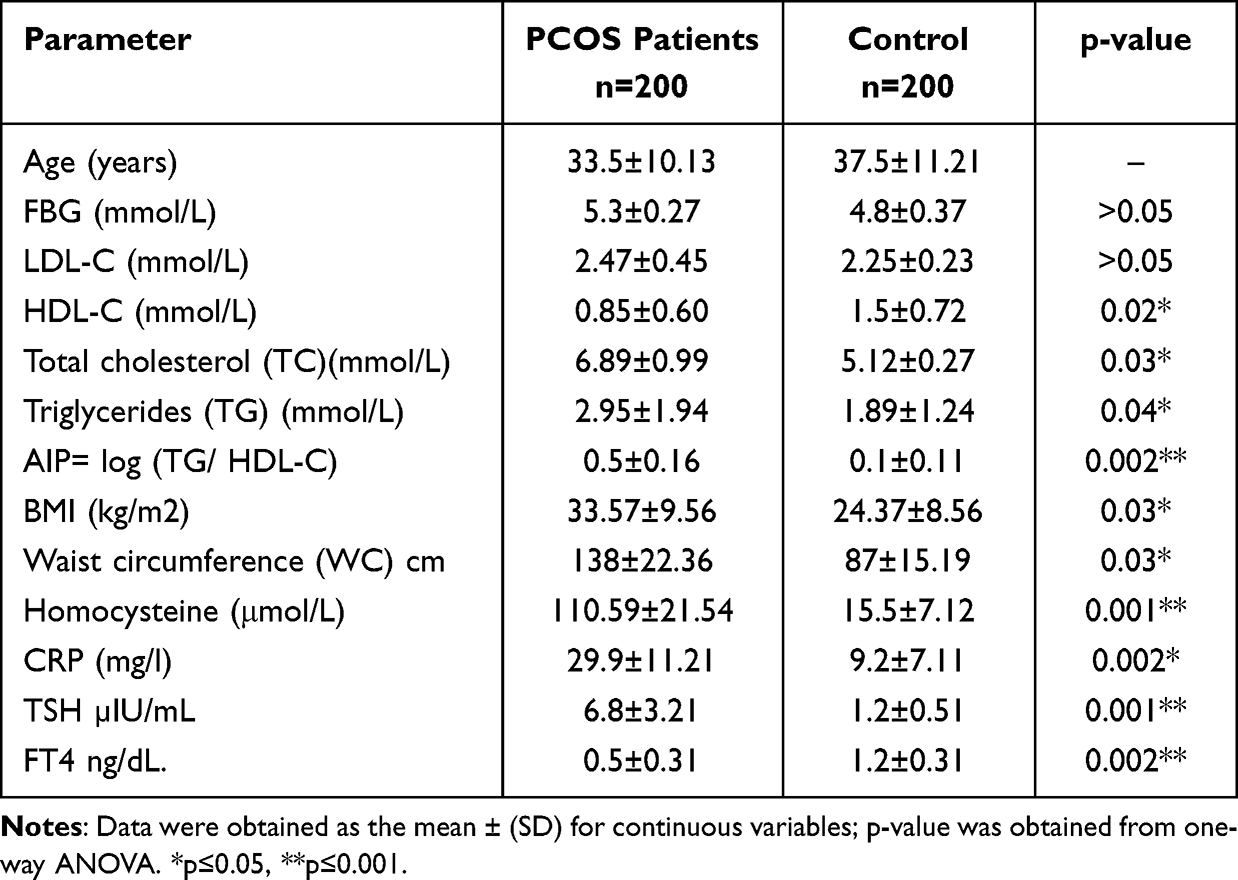 |
Table 1 Clinical and Biochemical Characteristics in PCOS Patients and Controls |
Clinical and Biochemical Characteristics of PCOS Women Categorized by Thyroid Disorders Categories
Further subdivision of PCOS patients is done by types of thyroid disorders; hypothyroidism, subclinical hypothyroidism, hyperthyroidism, and subclinical hyperthyroidism. Besides, higher ubiquity of hypothyroidism was observed in PCOS compared to the ubiquity of hyperthyroidism (55% vs 27.5%, p = 0.05). Whereas a lower ubiquity of subclinical hypothyroidism and subclinical hyperthyroidism (15% vs 2.5%) were observed. As demonstrated in Table 2, women with relatively elevated TSH levels (hypothyroidism) had significantly higher WC, FBG, BMI, and lower HDL-C compared with the hyperthyroidism group (all p < 0.05). Also, substantial differences between the hypothyroidism and hyperthyroidism groups in the levels of LDL-C, TG, Homocysteine, and CRP (all p<0.001 and <0.05, Table 2) were detected. Furthermore, observed PCOS women with hypothyroidism were at high risk of CVD as indicated by AIP value (0.6±0.42) compared with other groups.
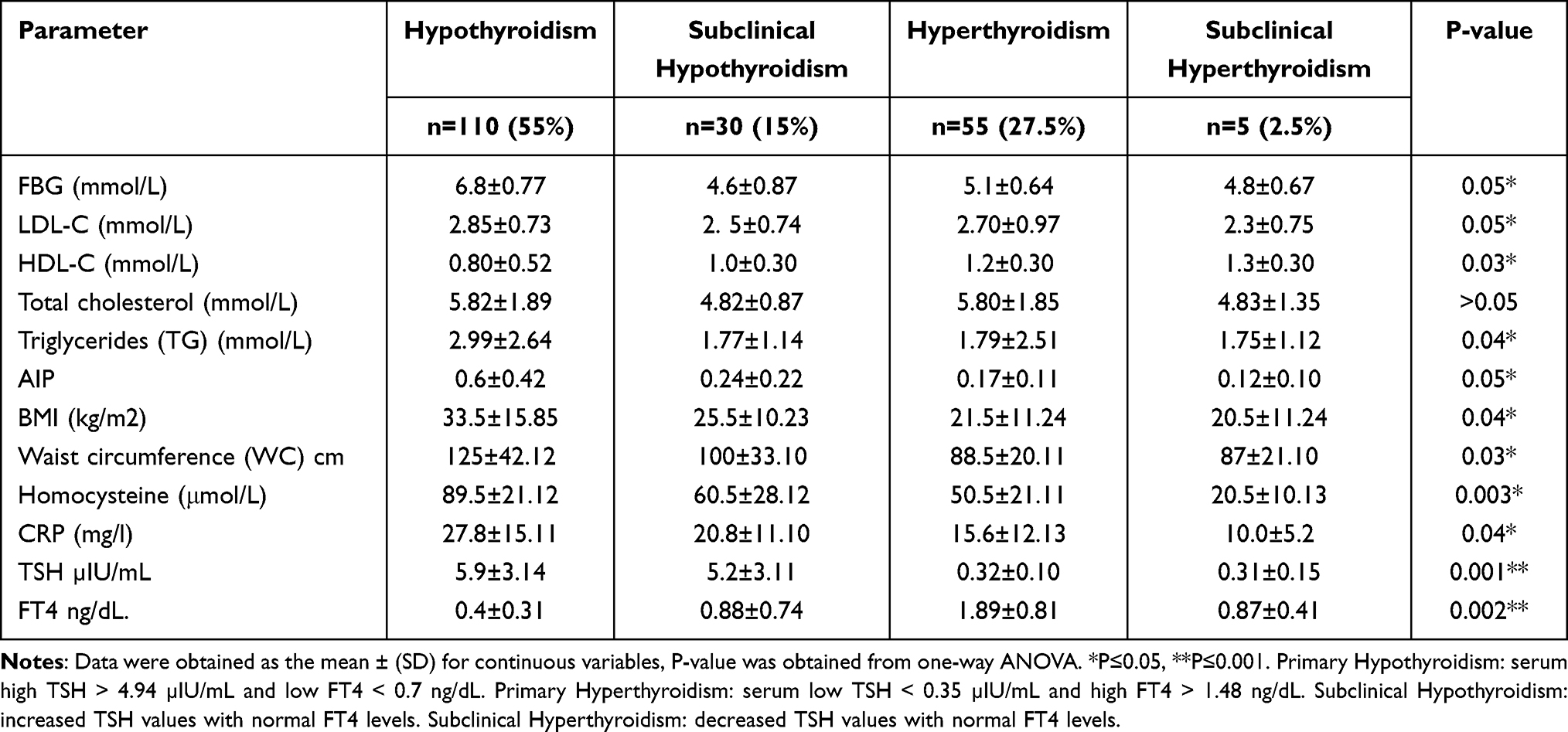 |
Table 2 Characteristics of PCOS Women According to Categories of Thyroid Disorders |
Analysis of PCOS and Hypothyroidism in Females and the Risk of CMRFs
Cardiometabolic risk factors (CMRFs) includes high LDL-C, high triglycerides, low HDL-C, hyperglycemia (high blood glucose levels), obesity, increased waist circumference, and high CRP levels.16 Therefore, the associations of high levels of TSH, CRP, and Homocysteine with CMRFs in women with PCOS and Hypothyroidism were analyzed. The participants with hypothyroidism have a significant positive association between CRP levels and cardiometabolic variables evaluated such as FBG, TG, AIP, and BMI, except FT4 (r = −0.52; p = 0.04). Also, it is positively correlated with high levels of TSH (all p<0.05, Table 3).
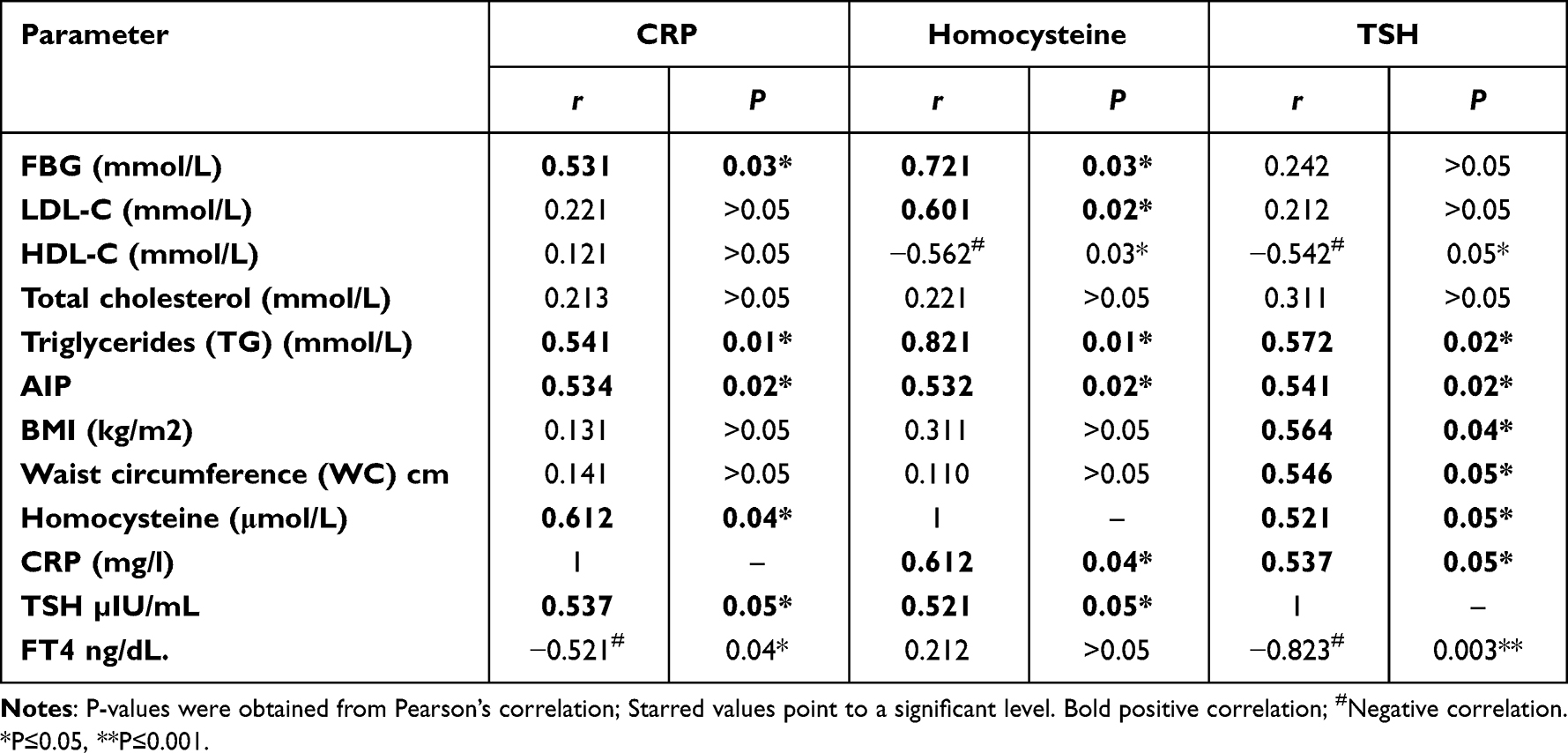 |
Table 3 Pearson’s Correlation Coefficients Between Key Variables in Women with PCOS and Hypothyroidism |
In the same group, FBG (r = 0.72; p = 0.03), LDL-C (r = 0.60; p = 0.02), TG (r = 0.82; p = 0.01), AIP (r = 0.53; p = 0.02), TSH (r = 0.52; p =0.05), and CRP (r = 0.61; p =0.04) correlated positively, while HDL-C (r = −0.56; p = 0.03) were negatively correlated with Homocysteine levels (Table 3). In addition, the high TSH levels positively correlated with CMRFs variables such as TG (r = 0.57; p = 0.02), BMI (r = 0.56 p =0.04), AIP (r = 0.54; p = 0.02), and WC (r = 0.54; p = 0.05) but negatively correlated with HDL-C and FT4 (r = −0.54; p = 0.05, r = −0.82; p = 0.003, respectively).
Discussion
This analysis of PCOS patients with hypothyroidism is the first to examine the correlation between TSH and CMRFs. In our cohort, the higher ubiquity of hypothyroidism was detected in PCOS compared to the prevalence of hyperthyroidism (55% vs 27.5%). While a lower prevalence of subclinical hypothyroidism and subclinical hyperthyroidism (15% vs 2.5%) were revealed. This is in agreement with earlier studies. For example, Nanda et al study report that out of 196 cases of PCOS, 1.02% had hyperthyroidism, and 13.26% had hypothyroidism.17 Also, Ozdemir et al identified that there were 107 women with PCOS, 15.9% of patients had hypothyroidism and 1.8% had hyperthyroidism.18
In this study, researchers discovered evidence that PCOS patients with moderately elevated TSH levels and had a higher risk of CVD development. It was discovered that the PCOS women with hypothyroidism had high levels of TSH, CRP, and Homocysteine, which were considered previously as important independent predictors of high CVD risk. In addition, the study revealed significant strong associations between them and traditional CMRFs such as fasting blood glucose levels, BMI (obesity indicators), triglycerides, and waist circumstances (central obesity indicator).
The first evidence that supported the study’s hypotheses is that serum TSH level was substantially higher in the PCOS population with an increase in the BMI, WC, and triglycerides levels associated with a high value of AIP, which is an essential indicator for CVD. Some studies in adults who have hypothyroidism (high levels of TSH) showed that there was an association with adverse cardiovascular outcomes, for example, carotid intima thickness,19,20 coronary heart disease,21 heart failure22 and stroke.23
Evidence suggests that CRP may greatly indicate CVD and chronic vessel inflammation.24,25 This is because a growing CRP level may serve as a signal of circulating inflammatory markers before acute events occur. There is a correlation between elevated levels of CRP and the development of CVD.26 Previous studies were used to determine how PCOS and hypothyroidism affected CRP levels in Saudi women. CRP, thyroid stimulating hormone, and triglyceride levels were considerably higher in patients with PCOS who had a high cardiovascular risk, as defined by AIP (0.21); although HDL-C were lower. Patients with elevated CRP levels also tended to be overweight, as measured by their BMI and WC, suggesting that CRP may indirectly impair cardiovascular health by influencing cardiometabolic factors. CRP levels were inversely related to WC, BMI, and AIP. CRP is correlated with measures of obesity such as BMI, adiposity, and, WC, according to previous cross-sectional studies.27,28
In addition, recent studies have shown that elevated homocysteine levels are associated with an increased risk of CVD.29 Researchers believe that homocysteine causes endothelial dysfunction, which in turn causes vascular damage and CVD.30 Several other studies have shown a correlation between homocysteine and CVD, although most of these studies failed to consider the impact of other traditional CVD risk factors. Even after accounting for established CVD risk variables such as fasting blood glucose, triglyceride levels, HDL-C, BMI, and adiposity index, a high homocysteine level may be an independent predictor of increased CVD risk in PCOS women with hypothyroidism. Homocysteine’s effect on cardiometabolic variables may have a knock-on effect on cardiovascular health. From the results of our research, we conclude that PCOS patients with hypothyroidism and an elevated AIP value are more likely to have high levels of homocysteine, which is associated with elevated glucose, low-density lipoprotein (LDL), and triglyceride levels.
Based on the findings, it was evaluated that women with PCOS are at high risk of hypothyroidism as indicated by high levels of TSH, which was positively correlated with increasing the risk of CVD through its influencing on raising the levels of CRP, Homocysteine, triglycerides, and BMI. The research is the first to evaluate in-depth the connection between TSH levels and CMRFs in PCOS patients. Therefore, the link between thyroid profile and CMRFs in PCOS patients may be better detected. A limited sample size, however, is one of the study’s drawbacks. Prospectively, this research may be conducted with a bigger sample size.
Conclusion
There was an association between the PCOS and thyroid dysfunction as the TSH levels of the PCOS hypothyroid groups were significantly higher than the control groups, and the CMRFs were significantly high in the PCOS hypothyroid groups. This group was at high risk of CVD due to high levels of CRP, Homocysteine, triglycerides, and obesity. Therefore, physicians need to monitor the thyroid profile, CRP, and homocysteine levels of PCOS patients and treat the thyroid dysfunction that may assist in managing menstrual irregularities and infertility and reduce the risk of CVD.
Data Sharing Statement
The dataset produced for this study is accessible on request to the corresponding author.
Ethics Approval Statement
Ethical authorization to carry out the study was obtained from the Ethical Committee at the College of Applied Medical Sciences (CLN201704), Taibah University, and Madinah.
Consent
Written informed consent was obtained according to the Helsinki guidelines.
Acknowledgments
The Authors gratefully acknowledge the assistance of Miss Johayna Aboalkayer (Taibah University, Medical Applied Science Collage’s technician), the lab technician who supported and helped us in the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
There is no conflict of interest.
References
1. Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565–4592. doi:10.1210/jc.2013-2350
2. Zwain ZM, Aziz MK. Polycystic ovarian syndrome and thyroid disorders. Int J Technol Res. 2016;4:73–77.
3. Sinha U, Sinharay K, Saha S, et al. Thyroid disorders in polycystic ovarian syndrome subjects: a tertiary hospital based cross-sectional study from Eastern India. Indian J Endocrinol Metab. 2013;17(2):304. doi:10.4103/2230-8210.109714
4. Ramanand S, Raparti GT, Halasawadekar NR, et al. Hypothyroidism in polycystic ovarian syndrome: a comparative study of clinical characteristics, metabolic and hormonal parameters in euthyroid and hypothyroid polycystic ovarian syndrome women. Int J Reprod Contracept Obstet Gynecol. 2016;5(9):3181–3185.
5. Gilbert EW, Tay CT, Hiam DS, et al. Comorbidities and complications of polycystic ovary syndrome: an overview of systematic reviews. Clin Endocrinol (Oxf). 2018;89(6):683–699. doi:10.1111/cen.13828
6. Singla R, Gupta Y, Khemani M, et al. Thyroid disorders and polycystic ovary syndrome: an emerging relationship. Indian J Endocrinol Metab. 2015;19(1):25. doi:10.4103/2230-8210.146860
7. Ajmani NS, Sarbhai V, Yadav N, et al. Role of thyroid dysfunction in patients with menstrual disorders in tertiary care center of walled city of Delhi. J Obstetr Gynecol India. 2016;66(2):115–119. doi:10.1007/s13224-014-0650-0
8. Pahwa S, Shailja G, Jasmine K. Thyroid dysfunction in dysfunctional uterine bleeding. J Adv Res Bio Sci. 2013;5(1):78–83.
9. Conway G, Dewailly D, Diamanti-Kandarakis E, et al. The polycystic ovary syndrome: a position statement from the European Society of Endocrinology. Eur J Endocrinol. 2014;171(4):P1–P29. doi:10.1530/EJE-14-0253
10. Fauser BC, Tarlatzis BC, Rebar RW, et al. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): the Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil Steril. 2012;97(1):28–38. e25. doi:10.1016/j.fertnstert.2011.09.024
11. Toulis KA, Goulis DG, Mintziori G, et al. Meta-analysis of cardiovascular disease risk markers in women with polycystic ovary syndrome. Human Reprod. 2011;17(6):741–760.
12. Jabbar A, Pingitore A, Pearce SHS, et al. Thyroid hormones and cardiovascular disease. Nat Rev Cardiol. 2017;14(1):39–55. doi:10.1038/nrcardio.2016.174
13. Eshre TR; A.-S.P.C.W. Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19–25.
14. WHO. Obesity; 2021. Available from: https://www.who.int/health-topics/obesity.
15. Floriani C, Feller M, Aubert CE, et al. Thyroid dysfunction and anemia: a prospective cohort study and a systematic review. Thyroid. 2018;28(5):575–582. doi:10.1089/thy.2017.0480
16. Khazaal MS. Atherogenic index of plasma as a parameter in predicting cardiovascular risk in males compared to the conventional dyslipidemic indices. Karbala J Med. 2013;6:1506–1531.
17. Nanda SS, Dash S, Behera A, et al. Thyroid profile in polycystic ovarian syndrome. J Evol Med Dent Sci. 2014;3(37):9594–9601. doi:10.14260/jemds/2014/3242
18. Kachuei M, Jafari F, Kachuei A, Keshteli AH. Prevalence of autoimmune thyroiditis in patients with polycystic ovary syndrome. Arch Gynecol Obstet. 2012;285(3):853–856. doi:10.1007/s00404-011-2040-5
19. Aziz M, Kandimalla Y, Machavarapu A, et al. Effect of thyroxin treatment on carotid intima–media thickness (CIMT) reduction in patients with subclinical hypothyroidism (SCH): a meta-analysis of clinical trials. J Atheroscler Thromb. 2017;20:39917.
20. Gao N, Zhang W, Zhang Y-Z, et al. Carotid intima-media thickness in patients with subclinical hypothyroidism: a meta-analysis. Atherosclerosis. 2013;227(1):18–25. doi:10.1016/j.atherosclerosis.2012.10.070
21. Collet T-H, Bauer DC, Cappola AR, et al. Thyroid antibody status, subclinical hypothyroidism, and the risk of coronary heart disease: an individual participant data analysis. J Clin Endocrinol Metab. 2014;99(9):3353–3362. doi:10.1210/jc.2014-1250
22. Gencer B, Collet T-H, Virgini V, et al. Thyroid Studies Collaboration: subclinical thyroid dysfunction and the risk of heart failure events: an individual participant data analysis from 6 prospective cohorts. Circulation. 2012;126(9):1040–1049. doi:10.1161/CIRCULATIONAHA.112.096024
23. Chaker L, Baumgartner C, den Elzen WPJ, et al. Subclinical hypothyroidism and the risk of stroke events and fatal stroke: an individual participant data analysis. J Clin Endocrinol Metab. 2015;100(6):2181–2191. doi:10.1210/jc.2015-1438
24. Angelica Sinicato NP, Aparecida da Silva Cardoso P, Appenzeller S. Risk factors in cardiovascular disease in systemic lupus erythematosus. Curr Cardiol Rev. 2013;9(1):15–19. doi:10.2174/157340313805076304
25. Nilsson J. CRP—marker or maker of cardiovascular disease? Am Heart Assoc. 2005;51:1527–1528.
26. Collaboration ERF. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet. 2010;375(9709):132–140.
27. Fröhlich M, Imhof A, Berg G, et al. Association between C-reactive protein and features of the metabolic syndrome: a population-based study. Diabetes Care. 2000;23(12):1835–1839. doi:10.2337/diacare.23.12.1835
28. Lin -C-C, Kardia SL, Li C-I, et al. The relationship of high sensitivity C-reactive protein to percent body fat mass, body mass index, waist-to-Hip ratio, and waist circumference in a Taiwanese population. BMC Public Health. 2010;10(1):1–8. doi:10.1186/1471-2458-10-579
29. Chrysant SG, Chrysant GS. The current status of homocysteine as a risk factor for cardiovascular disease: a mini review. Expert Rev Cardiovasc Ther. 2018;16(8):559–565. doi:10.1080/14779072.2018.1497974
30. Balint B, Jepchumba VK, Guéant J-L, et al. Mechanisms of homocysteine-induced damage to the endothelial, medial and adventitial layers of the arterial wall. Biochimie. 2020;173:100–106. doi:10.1016/j.biochi.2020.02.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.