Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Correlation Between Hemoglobin Levels and Polycystic Ovary Syndrome Metabolic Disorder
Authors Ha LX, Du YD, Qu XX, Wang JJ
Received 11 July 2023
Accepted for publication 14 September 2023
Published 28 September 2023 Volume 2023:16 Pages 3019—3027
DOI https://doi.org/10.2147/DMSO.S430120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Ling-Xia Ha,1 Yu-Dong Du,2,3 Xiao-Xiao Qu,2 Jin-Juan Wang2
1Reproductive Medicine Center, General Hospital of Ningxia Medical University, Key Laboratory of Fertility Preservation and Maintenance of Ministry of Education, Ningxia Medical University, Yinchuan, Ningxia, 750004, People’s Republic of China; 2Ningxia Medical University, General Hospital of Ningxia Medical University, Yinchuan, Ningxia, 750004, People’s Republic of China; 3Department of Reproductive Medicine, Luoyang Maternal and Child Health Hospital, Luoyang, Henan, 471000, People’s Republic of China
Correspondence: Ling-Xia Ha, Reproductive Medicine Center, General Hospital of Ningxia Medical University, No. 804 of Shengli Road, Xingqing District, Yinchuan, 750004, People’s Republic of China, Tel +86 951 6744033 ; +86 13629500990, Fax +86 951 6743891, Email [email protected]
Objective: The purpose of this study was to explore the relationship between hemoglobin levels and metabolic disorders in patients with PCOS.
Methods: A total of 573 patients were selected, based on the hemoglobin level; 342 patients with PCOS were divided into two groups as follows: Group A (normal Hb group, n = 269) and Group B (high Hb group, n = 73); 231 non-PCOS patients were divided into two groups as follows: Group C (normal Hb group, n = 199), and Group D (high Hb group, n = 32). The general information, glucose and lipid metabolism indicators, and uric acid levels of all patients were compiled for data analysis.
Results: (1) Hb, HGB concentration in mean red blood cells and RDW in PCOS patients were higher than those in non-PCOS patients, and MCV was lower than that in non-PCOS patients (P < 0.05); (2) Compared with Group A, patients in Group B had higher BMI, Hb, 2-hPG, FINS, 2-hINS, HOMA-IR, LDL-C, and uric acid levels while the QUICKI was lower; in Group C, the age, FSH, HDL-C, and LDL-C were higher, and AMH, BMI, T, TG, and uric acid level were lower (P< 0.05); compared with Group D, AMH, BMI, FINS, HOMA-IR, TG, uric acid level increased, while age, FSH, and QUICKI decreased in Group B; and Hb and T decreased in Group C (P< 0.05); (3) Pearson’s correlation analysis indicated that Hb in PCOS patients was positively correlated with BMI, FPG, 2-hPG, FINS, 2-hINS, and HOMA-IR, and negatively correlated with the QUICKI (P< 0.05); (4) Multi-factor logistic regression analysis suggested that the high Hb level in PCOS patients was an independent risk factor of IR (P< 0.05).
Conclusion: Hb level in patients with PCOS was associated with BMI and glucose metabolism indicators; a high Hb level may be an independent risk factor for IR.
Keywords: hemoglobin, insulin resistance, metabolic disorder, polycystic ovary syndrome
Introduction
Polycystic ovary syndrome (PCOS) is one of the most common endocrine metabolic disorders affecting women of childbearing age.1 It is characterized by hyperandrogenemia, scanty or amenorrhoeic menstruation, and infertility, as well as metabolic disorders such as obesity, insulin resistance, abnormal glucose tolerance, and lipid spectrum disorder, as well as long-term susceptibility to diabetes, cardiovascular disease, tumors, and so on.2 A large-scale national epidemiological survey in China reported that the prevalence of metabolic syndrome in women with PCOS was significantly higher than that in non-PCOS women of childbearing age.3 As a result, detecting metabolic changes in PCOS patients at an early stage is crucial.
Hemoglobin (Hb) is an important transporter of oxygen in the body, and its level can be influenced by genes and the environment.4 A number of previous studies have demonstrated that a high Hb level is associated with the incidence of metabolic syndrome (MS), hyperuricemia (HUA), and nonalcoholic fatty liver disease (NAFLD), and it can be considered one of the predictors of MS.5–8 Hemoglobin can induce vasoconstriction by limiting nitric oxide in vascular smooth muscle cells, and induced hypertension.9 Several studies have shown associations of HCT, Hgb, RBC, and WBC with insulin resistance.10,11 However, the relationship between Hb levels and metabolic disorders in patients with PCOS has not been reported. Therefore, in this study, we investigated the possible mechanisms of metabolic disorders in patients with PCOS by examining the relationship between Hb levels and metabolic indicators.
Materials and Method
Study Participants and Grouping
A total of 342 patients with PCOS undergoing treatment at the Reproductive Medicine Center of Ningxia Medical University from January 2020 to July 2022 were selected and included in the study groups; and 231 individuals who have regular menstrual cycles with male factor or tubal factor infertility were included in the control group. PCOS was diagnosed based on any two of the following three items based on the 2003 Rotterdam PCOS Diagnostic Criteria (excluding other conditions causing hyperandrogenemia):12–14 1) Sporadic ovulation or anovulation; 2) Hyperandrogenemia suggested by clinical or biochemical tests; 3) Ovarian polycystic change indicated by ultrasonography: ≥ 12 small follicles of 2–9 mm diameter in at least one ovary, and/or ovarian volume > 10 cm3. For all patients, hematologic disorders such as leukemia, anemia, liver or kidney disease, hyperthyroidism or hypothyroidism, autoimmune disease, and acute or chronic infectious disease were excluded from the study.
The normal range of hemoglobin concentration in adult women in China is 110–150 g/L, and concentration > 150 g/L was defined as elevated hemoglobin concentration.15 Based on hemoglobin levels, the patients were divided into Group A (PCOS normal hemoglobin group, n = 269), Group B (PCOS high hemoglobin group, n = 73), Group C (non-PCOS normal hemoglobin group, n = 199), and Group D (non-PCOS high hemoglobin group, n = 32). The study was approved by the Ethics Committee of Ningxia Medical University General Hospital, and all patients signed the informed consent form.
Medical History and Physical Examination
The medical history of the study participants was collected based on a standardized questionnaire and the participants underwent a physical examination that included measurement of height, body mass, waist circumference, hip circumference, and calculation of body mass index: BMI = body mass (kg)/height2 (m2) while they were fasting. Overweight or obese: BMI ≥ 25 kg/m2.
Determination of Physiological and Chemical Indicators
Fasting venous blood was drawn from the participants in the early morning of the 2nd to 5th day of menstruation, to test follicle stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), testosterone (T), prolactin (PRL), anti-Müllerian hormone (AMH) using the chemiluminescence method. Blood routine was tested using an automatic blood cell analyzer. Fasting insulin (FINS), fasting plasma glucose (FPG), 2-hours plasma glucose (2-hPG), 2-hours insulin (2-hINS), blood lipids, and liver and kidney functions were tested using a fully automatic biochemical analyzer. HOMA-IR = (FPG×FINS)/22.5, QUICKI = 1/(lgFINS+lgFPG).
Statistical Analysis
The data were analyzed using SPSS 24.0 software. We used the Shapiro–Wilk test to determine if the measurement data conformed to the normal distribution or not. Data conforming to a normal distribution were expressed as ( ), t-test was used to compare two groups, and the comparison between multiple groups was conducted using one-way analysis of variance (ANOVA). Data failing to conform to a normal distribution were expressed using the median (interquartile range), and inter-group comparisons were performed using the non-parametric Kruskal–Wallis H-test. We used Pearson correlation analysis for correlation analysis, and multiple-factor analysis was performed using multivariate logistic regression analysis. The receiver operating characteristic (ROC) curve was used to analyze the predictive value of hemoglobin levels for metabolic disorders in patients with PCOS. P < 0.05 indicated that there was a statistically significant difference. GraphPad Prism 8.0 was used for plotting and graphing data.
), t-test was used to compare two groups, and the comparison between multiple groups was conducted using one-way analysis of variance (ANOVA). Data failing to conform to a normal distribution were expressed using the median (interquartile range), and inter-group comparisons were performed using the non-parametric Kruskal–Wallis H-test. We used Pearson correlation analysis for correlation analysis, and multiple-factor analysis was performed using multivariate logistic regression analysis. The receiver operating characteristic (ROC) curve was used to analyze the predictive value of hemoglobin levels for metabolic disorders in patients with PCOS. P < 0.05 indicated that there was a statistically significant difference. GraphPad Prism 8.0 was used for plotting and graphing data.
Results
Comparison of the Red Blood Cell Parameters of Patients in the PCOS and Control Groups
In patients with PCOS, the hemoglobin level, HGB concentration in mean red blood cells, and RDW (CV) were higher when compared to non-PCOS patients, while the red blood cell distribution volume was lower than that in non-PCOS patients (both P < 0.05). There was no significant difference in the other indicators between the two groups (P > 0.05), as shown in Table 1.
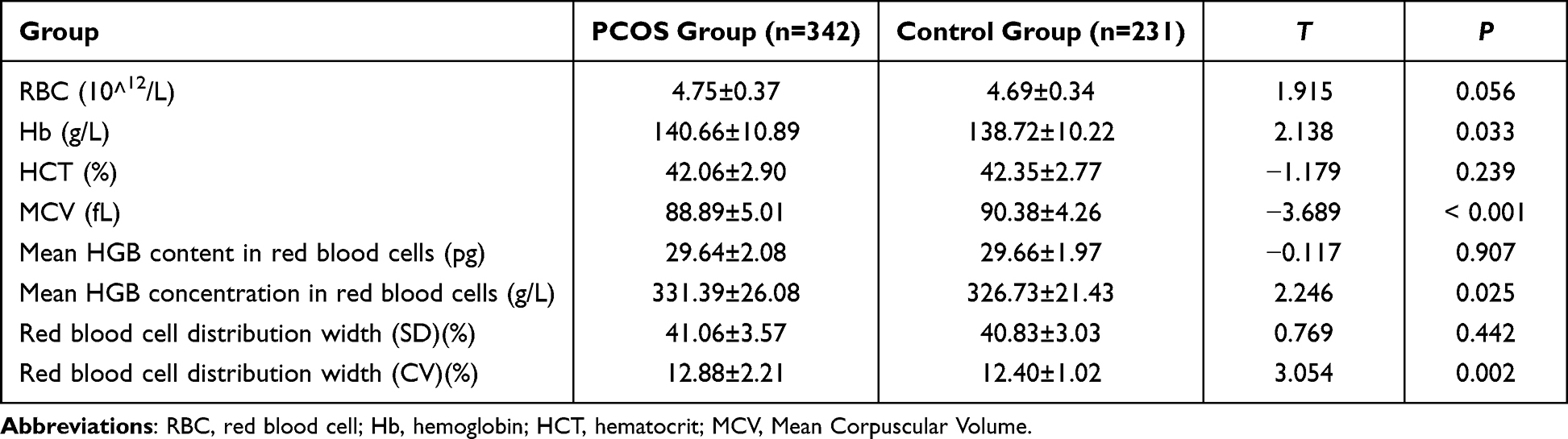 |
Table 1 Comparison of Erythrocyte Parameters Between the PCOS Group and Control Group ( |

Comparison of General Information of Patients in Different Groups
Compared with Group A, BMI and hemoglobin levels were higher in Group B, while in Group C, patient age and FSH levels were higher, but AMH, BMI, and T levels were lower. Compared with Group D, patient age and FSH level were lower, but BMI and AMH level were higher in Group B, while in Group C, hemoglobin level and T levels were lower, showing a statistically significant difference (P < 0.05). There was no significant difference in LH, E2, PRL, and P levels in patients between different groups (P > 0.05), as shown in Table 2.
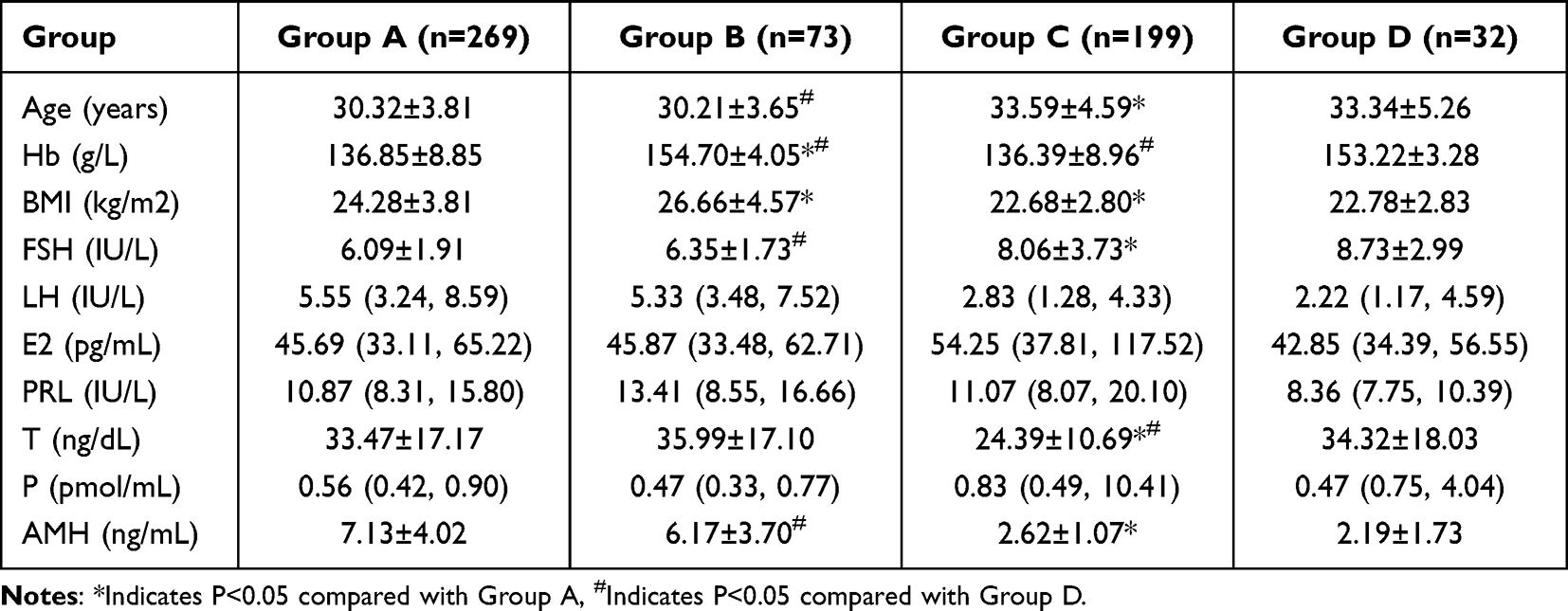 |
Table 2 Comparison of General Information of Patients Between Groups [( |

Comparison of Metabolic Indicators Between Different Groups
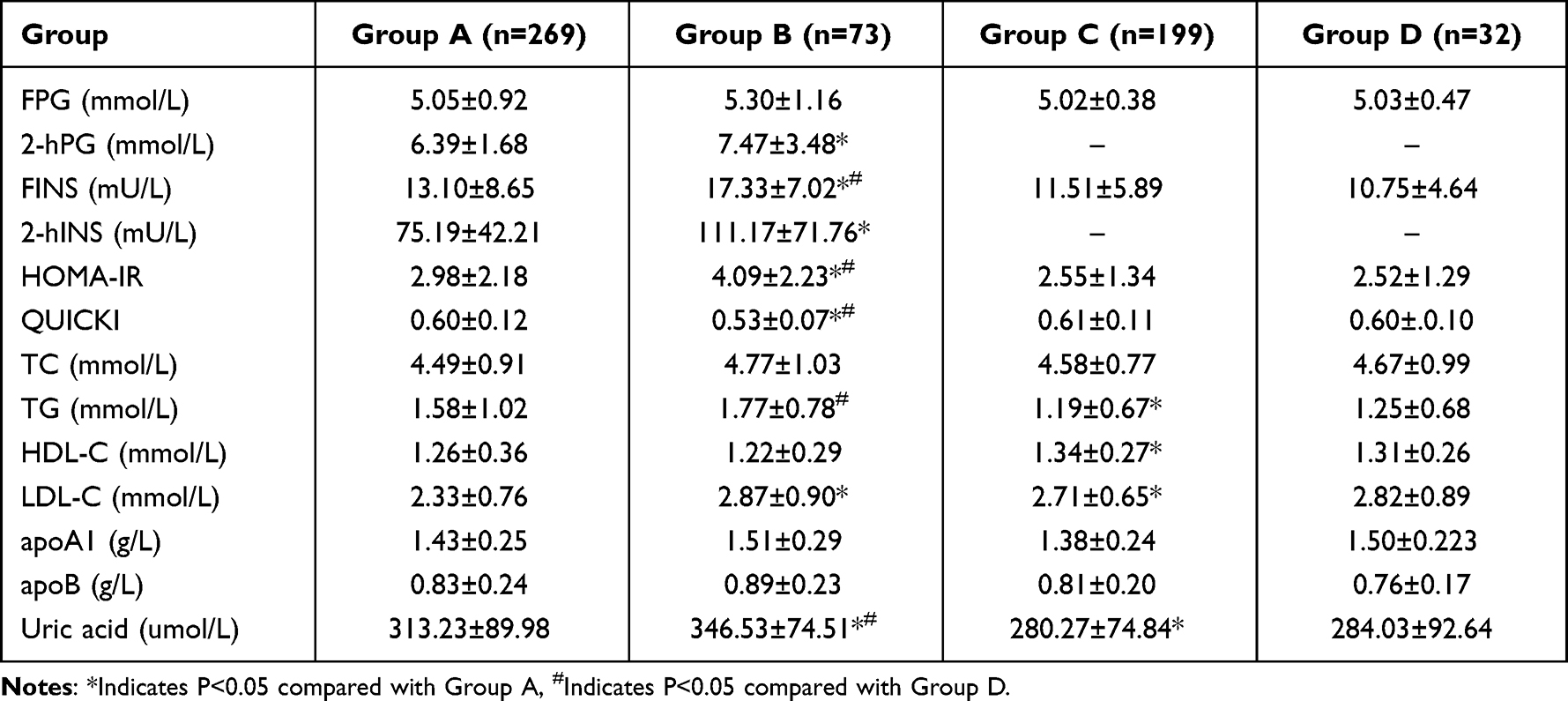
Compared with Group A, 2-hPG, FINS, 2-hINS, HOMA-IR, LDL-C, and uric acid levels were higher but QUICKI levels were lower in Group B, while in Group C, TG and uric acid levels were lower but HDL-C and LDL-C were higher (P < 0.05). Compared with Group D, FINS, HOMA-IR, TG, and uric acid levels were higher in Group B, but QUICKI levels were lower, showing a statistically significant difference (P < 0.05). There was no significant difference in FPG, TC, apoA1, and apoB between the different groups (P > 0.05), as shown in Table 3.
 |

Correlation Between Hemoglobin Levels and Metabolic Indicators in PCOS Patients
In patients with PCOS, the hemoglobin level was positively correlated with BMI, FPG, 2-hPG, FINS, 2-hINS, and HOMA-IR, but was negatively correlated with the QUICKI index, indicating statistical significance (P < 0.05), as shown in Table 4 and Figure 1.
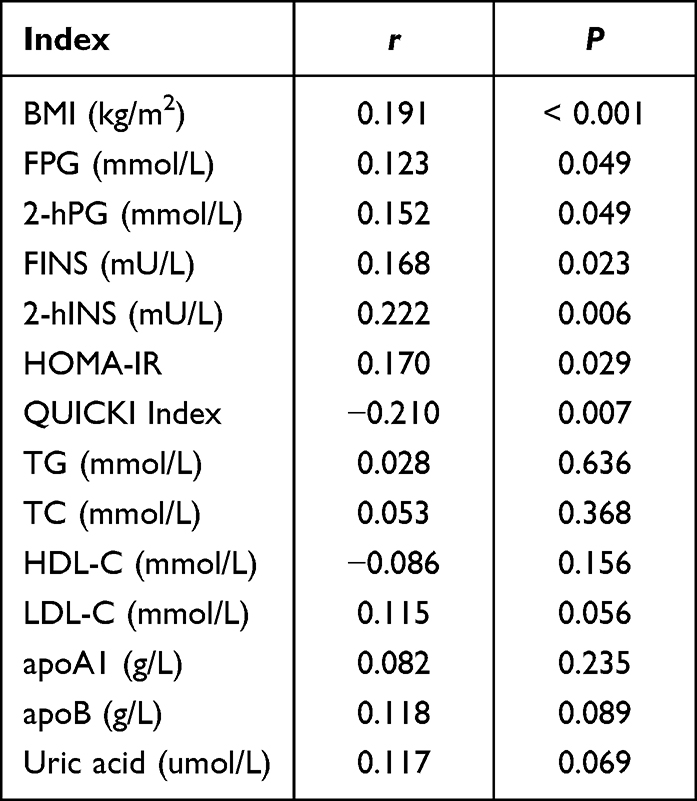 |
Table 4 Correlation Between Hemoglobin and Metabolic Indicators in Patients with PCOS |
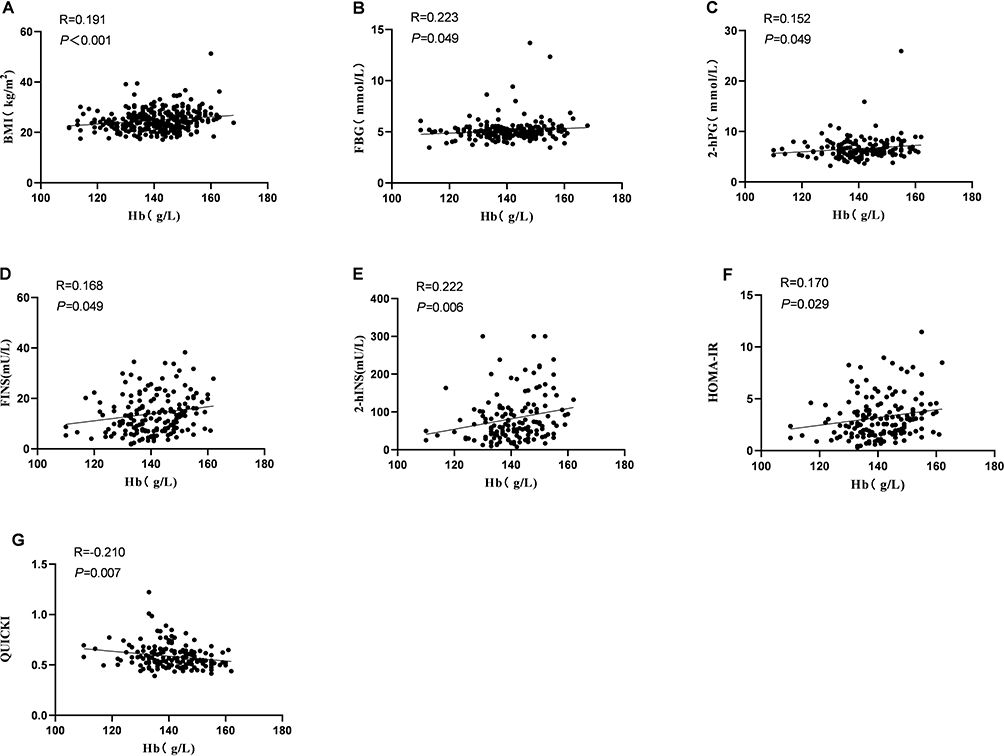 |
Figure 1 Relationship between hemoglobin levels and related metabolic indicators ((A) BMI, (B) FPG, (C) 2-hPG, (D) FINS, (E) 2-hINS, (F) HOMA-IR, (G) QUICKI) in patients with PCOS. |
Relationship Between Hemoglobin Level and Metabolic Components
In our regression model, we took the hemoglobin group as the independent variable, and the metabolic components (obesity, hyperglycemia, insulin resistance, dyslipidemia, and hyperuricemia) were the dependent variables. The model results showed that hemoglobin level was an independent risk factor affecting insulin resistance, and the risk of insulin resistance increased with the rise of hemoglobin levels, as shown in Table 5.
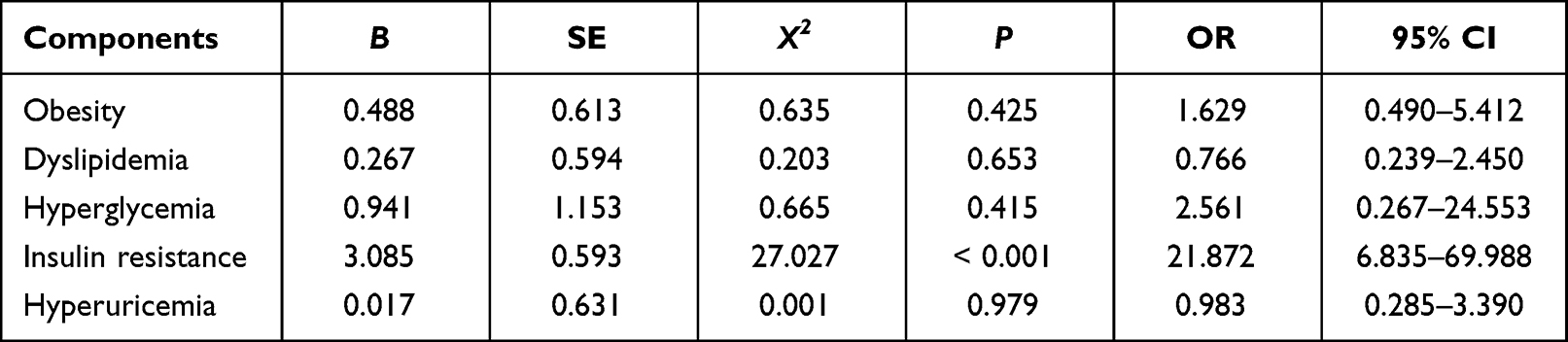 |
Table 5 Correlation Between Metabolic Disorders and High Hemoglobin in Patients with PCOS |
Prediction of IR in PCOS Patients Based on the Hemoglobin Level
ROC curve analysis was performed for predicting IR in patients with PCOS based on the hemoglobin level; based on the results, the area under the curve (AUC) was 0.801, P < 0.001, 95% CI (0.743, 0.850); when the hemoglobin level was 149.5 g/L, the sensitivity of IR in patients with PCOS was 0.718, and the specificity was 0.764, as shown in Figure 2.
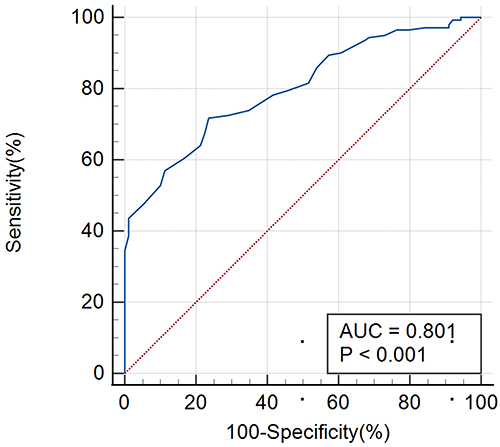 |
Figure 2 Prediction of IR in patients with PCOS based on hemoglobin levels based on the ROC curve. |
Discussion
PCOS is a common reproductive endocrine metabolic disorder that can lead to ovulatory infertility as well as obesity and glucose and lipid metabolism disorders; as a result, it has gradually gained a lot of research attention. In the current study, we found that Hb levels, HGB concentration in mean red blood cells, and the red blood cell distribution width (RDW) in patients with PCOS were higher than those in non-PCOS patients, while the mean corpuscular volume (MCV) was lower than that in non-PCOS patients.
Hyperandrogenemia is an important pathophysiological feature of PCOS. In the current study, the T level in patients in the PCOS group and non-PCOS high hemoglobin group was significantly higher than that in the non-PCOS normal hemoglobin group, suggesting that testosterone may be involved in the elevation of Hb. Testosterone was found to induce erythropoiesis and increase Hb levels by affecting the bioavailability of iron and stimulating the differentiation of erythropoietin (EPO).16,17
Multiple studies have shown that patients with PCOS are more prone to obstructive sleep apnea (OSA) than non-PCOS patients of childbearing age,18,19 and Hb levels were significantly higher in patients with OSA.20 Persistent hypoxemia has been recognized to be involved in the pathological change process of OSA,21 and chronic hypoxia stimulates EPO synthesis, thus promoting an increase in Hb and RBC in the peripheral circulation.22 Therefore, it is necessary to screen for OSA in patients with PCOS presenting elevated hemoglobin levels.
Furthermore, other studies23,24 found that the RDW level was higher in patients with PCOS, which was consistent with the results of our study. Qiang et al23 showed that the high RDW level in PCOS patients was positively correlated with hs-CRP, HOMA-IR, and BMI. PCOS is a chronic inflammatory disease25 that can cause oxidative stress by stimulating immature red blood cells to release RDW and increasing the mean HGB concentration.26 As a result, the increase in RDW and mean HGB concentration can be associated with chronic low-grade inflammation in patients with PCOS.
MS was found to be 2.5 times more common in patients with PCOS than in normal women.27 Previous studies showed that PCOS patients had varying degrees of metabolic disorders.28,29 In the current study, BMI and uric acid levels in the PCOS high Hb level group were higher than those in other groups, suggesting that BMI could affect Hb levels in patients with PCOS. Our correlation analysis revealed a significant positive correlation between Hb levels and BMI in patients with PCOS, which was consistent with the result of Shimizu et al.30 Obesity was seen in 30–70% of PCOS patients,31 and the decreased oxygenation of adipose tissue resulted in overexpression of erythropoietin transcription-stimulating factors such as hypoxia-inducible factor (HIF-1),32 thus stimulating the increase of hemoglobin synthesis. Very high rates of OSA have been reported in women with obese PCOS,33,34 and obesity and OSA cooperate with each other to further promote elevated hemoglobin levels.
In addition, CD40L is a member of the tumor necrosis factor (TNF) family that has been linked to glucose and lipid metabolism disorders and the development of cardiovascular disease.35 CD40L levels were significantly higher in patients with high Hb levels and patients with obesity36,37 while other studies found CD40L to be positively correlated with BMI and Hb levels37,38 and Hb to be an independent risk factor for elevated CD40L.36 Therefore, we hypothesized that CD40L could have a potential link between hemoglobin and obesity.
Insulin resistance (IR) has been identified as the critical link in the development and progression of PCOS.39 We found that 2-hPG, FINS, 2-hINS, and HOMA-IR were higher, but the QUICKI index was lower in the high Hb level group, and they were significantly correlated with the Hb level. Additional logistic regression revealed that the Hb level was an independent risk factor for the development of insulin resistance in patients with PCOS, which was consistent with the results of previous studies.40,41 Endothelial dysfunction has been found to be an important risk factor for insulin resistance; hemoglobin, as the carrier and buffer of nitric oxide (NO), can regulate vascular endothelial function via the L-arginine-NO pathway, and a high Hb level can lead to endothelial dysfunction, thus causing insulin resistance.42–44 Hemoglobin has been found to be closely related to HCT; elevated hemoglobin increases blood viscosity, reduces blood flow, and affects the supply of oxygen, glucose, and insulin in the tissues, thus promoting insulin resistance.45 Furthermore, high Hb levels can cause oxidative stress in pancreatic β-cells, impair their functioning, and lower insulin sensitivity, thus leading to abnormal glucose metabolism.46
Another study showed that insulin could also promote the proliferation of bone marrow and hematopoietic stem cells, and bind to receptors on red blood cells,47 thus stimulating the proliferation of red blood cells and increasing the Hb level. Hyperinsulinemia might exert its effects in erythropoiesis through several different mechanisms. Insulin and its analogues, such as the IGF-1, have a synergistic effect with erythropoietin on stimulating the proliferation of erythroid colonies.48,49 Also, hyperinsulinemia has been associated with increased levels of the hypoxia-inducible factor-1 alpha (HIF-1α), which promotes the synthesis of proteins, including the vascular endothelial growth factor and erythropoietin that stimulate erythropoiesis.50,51 As a result, hemoglobin and insulin resistance may be regulated in a two-way manner, with each influencing the other.
Conclusion
In conclusion, we found that hemoglobin levels in patients with PCOS were higher than in non-PCOS patients. High hemoglobin levels were an independent risk factor of IR in PCOS patients. Blood routine testing is a simple and low-cost testing method, and its use as an indicator for screening metabolic disorders in patients with PCOS should be further studied.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the General Hospital of Ningxia Medical University (No.KYLL-2021-1073). Written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
This study was supported by the National Key Research and Development Program of China (Grant No.2021YFC2700402), Ningxia Hui Autonomous Region Science and Technology Special Project to Benefit the People (Grant No.2022CMG03018).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hoeger KM, Dokras A, Piltonen T. Update on PCOS: consequences, challenges, and guiding treatment. J Clin Endocrinol Metab. 2021;106(3):e1071–e1083. doi:10.1210/clinem/dgaa839
2. Escobar-Morreale Héctor F. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nat Rev Endocrinol. 2018;14(5):270–284. doi:10.1038/nrendo.2018.24
3. Li R, Yu G, Yang D, et al. Prevalence and predictors of metabolic abnormalities in Chinese women with PCOS: a cross-sectional study. BMC Endocr Disord. 2014;14(1):1–8. doi:10.1186/1472-6823-14-76
4. Gell DA. Structure and function of haemoglobins. Blood Cells Mol Dis. 2018;70:13–42.
5. Hashimoto Y, Tanaka M, Kimura T, et al. Hemoglobin concentration and incident metabolic syndrome: a population-based large-scale cohort study. Endocrine. 2015;50(2):390–396. doi:10.1007/s12020-015-0587-9
6. Ahmadzadeh J, Mansorian B, Attari MMA, et al. The association between hematological parameters and metabolic syndrome in Iranian men: a single center large-scale study. Diabetes Metab Syndr. 2018;12(1):17–21. doi:10.1016/j.dsx.2017.07.044
7. He S, Gu H, Yang J, et al. Hemoglobin concentration is associated with the incidence of metabolic syndrome. BMC Endocr Disord. 2021;21(1):1–11. doi:10.1186/s12902-021-00719-4
8. Tanaka M, Okada H, Hashimoto Y, et al. Combined effect of hemoglobin and mean corpuscular volume levels on incident metabolic syndrome: a population-based cohort study. Clin Nutr ESPEN. 2020;40:314–319. doi:10.1016/j.clnesp.2020.08.010
9. Cabrales P, Han G, Nacharaju P, Friedman AJ, Friedman JM. Reversal of hemoglobin-induced vasoconstriction with sustained release of nitric oxide. Am J Physiol Heart Circ Physiol. 2011;300(1):H49–H56. doi:10.1152/ajpheart.00665.2010
10. Facchini FS, Carantoni M, Jeppesen J, Reaven GM. Hematocrit and hemoglobin are independently related to insulin resistance and compensatory hyperinsulinemia in healthy, non-obese men and women. Metabolism. 1998;47(7):831–835. doi:10.1016/S0026-0495(98)90121-4
11. Hanley AJ, Retnakaran R, Qi Y, et al. Association of hematological parameters with insulin resistance and beta-cell dysfunction in nondiabetic subjects. J Clin Endocrinol Metab. 2009;94(10):3824–3832. doi:10.1210/jc.2009-0719
12. ESHRE T R, ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril. 2004;81(1):19–25. doi:10.1016/j.fertnstert.2003.10.004
13. Metabolic Syndrome Research Cooperative Group of Chinese Diabetes Society. Recommendations of Chinese Diabetes Society on metabolic syndrome. Chin J Diabetes. 2004;3:5–10.
14. Sun L, Wang GX, Guo YY. Research progress of hyperuricemia. Chin J Gerontol. 2017;37(4):1034–1038.
15. Wan XH, Lu X. Diagnostics.
16. Qiao B, Sugianto P, Fung E, et al. Hepcidin-induced endocytosis of ferroportin is dependent on ferroportin ubiquitination. Cell Metab. 2012;15(6):918–924. doi:10.1016/j.cmet.2012.03.018
17. Luque-Ramírez M, Alvarez-Blasco F, Alpanes M, et al. Role of decreased circulating hepcidin concentrations in the iron excess of women with the polycystic ovary syndrome. J Clin Endocrinol Metab. 2011;96(3):846–852. doi:10.1210/jc.2010-2211
18. Kahal H, Kyrou I, Uthman OA, et al. The prevalence of obstructive sleep apnoea in women with polycystic ovary syndrome: a systematic review and meta-analysis. Sleep Breath. 2020;24(1):339–350. doi:10.1007/s11325-019-01835-1
19. Song Y, He X, Hu K. Clinical features and risk factors of polycystic ovary syndrome complicated with obstructive sleep apnea. J Clin Pulm Med. 2022;27(06):822–828.
20. Feliciano A, Vaz F, Valentim-Coelho C, et al. Evening and morning alterations in Obstructive Sleep Apnea red blood cell proteome. Data Brief. 2017;11:103–110. doi:10.1016/j.dib.2017.01.005
21. Bi YW, Li NF, Yao XG, et al. Changes of hemoglobin in patients with obstructive sleep apnea-hypopnea syndrome. Chin J Hypertens. 2021;29(02):176–179.
22. Zhang X-B, Zeng Y-M, Zeng H-Q, Zhang H-P, Wang H-L. Erythropoietin levels in patients with sleep apnea: a meta-analysis. Eur Archiv Oto Rhino Laryngol. 2017;274(6):2505–2512. doi:10.1007/s00405-017-4483-1
23. Qiang S, Long K, Ke LH, Liang K, Zhang HY. Relationship between red blood cell distribution width and polycystic ovary syndrome. J Clin Transfus Lab Med. 2021;23(06):779–782.
24. Yilmaz Ö, Mehmet C, Kelekci S, et al. Association between red blood cell distribution width and polycystic ovary syndrome. Endocr Res. 2015;40(4):181–187. doi:10.3109/07435800.2014.987398
25. Kelly CCJ, Lyall H, Petrie JR, et al. Low grade chronic inflammation in women with polycystic ovarian syndrome. J Clin Endocrinol Metab. 2001;86(6):2453–2455. doi:10.1210/jcem.86.6.7580
26. Yang DY, Quan WQ, Sun ZJ, et al. Research progress in RDW for the diagnosis and treatment of malignant tumors. Lab Med. 2018;33(09):844–849.
27. Behboudi‐Gandevani S, Amiri M, Bidhendi Yarandi R, et al. The risk of metabolic syndrome in polycystic ovary syndrome: a systematic review and meta‐analysis. Clin Endocrinol. 2018;88(2):169–184. doi:10.1111/cen.13477
28. Li Y, Chen C, Ma Y, et al. Multi-system reproductive metabolic disorder: significance for the pathogenesis and therapy of polycystic ovary syndrome (PCOS). Life Sci. 2019;228:167–175. doi:10.1016/j.lfs.2019.04.046
29. Ha LX, Yin T, Wu YY, Li WX, Du YD. Correlation between insulin resistance and expressions of local inflammatory factors and glucose transporter protein type-4 in the endometrium of patients with polycystic ovary syndrome. J Shandong Univ. 2021;59(11):41–47.
30. Shimizu Y, Nakazato M, Sekita T, et al. Association between the hemoglobin levels and hypertension in relation to the BMI status in a rural Japanese population: the Nagasaki Islands Study. Inter Med. 2014;53(5):435–440. doi:10.2169/internalmedicine.53.1353
31. Legro Richard S, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565–4592. doi:10.1210/jc.2013-2350
32. Lee YS, Kim J, Osborne O, et al. Increased adipocyte O2 consumption triggers HIF-1α, causing inflammation and insulin resistance in obesity. Cell. 2014;157(6):1339–1352. doi:10.1016/j.cell.2014.05.012
33. Fogel RB, Malhotra A, Pillar G, Pittman SD, Dunaif A, White DP. Increased prevalence of obstructive sleep apnea syndrome in obese women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2001;86(3):1175–1180. doi:10.1210/jcem.86.3.7316
34. Gopal M, Duntley S, Uhles M, Attarian H. The role of obesity in the increased prevalence of obstructive sleep apnea syndrome in patients with polycystic ovarian syndrome. Sleep Med. 2002;3(5):401–404. doi:10.1016/S1389-9457(02)00033-3
35. Li J, Zou CC. Research progress on the relationship between CD40-CD40L system and metabolic syndrome. Int J Pediatr. 2017;44(11):791–794.
36. Kawamoto R, Tabara Y, Kohara K, et al. Hemoglobin is associated with serum high molecular weight adiponectin in Japanese community-dwelling persons. J Atheroscler Thromb. 2011;18(3):182–189. doi:10.5551/jat.6379
37. Li J, Xu J, Zou CC, et al. Association between CD40-CD40L system and obesity in children. Chin J Contemp Pediatr. 2020;22(3):251–256. doi:10.7499/j.issn.1008-8830.2020.03.013
38. Kutlu M, Sonmez A, Genc H, et al. Relationship between hemoglobin and CD40 ligand in prediabetes. Clin Invest Med. 2009;32(6):E244–E250. doi:10.25011/cim.v32i6.10659
39. Qiao J, Qi XY, Xu YL, et al. Pay attention to important reproductive endocrinologic diseases affecting female health-polycystic ovary syndrome. Chin J Pract Gynecol Obstetr. 2020;36(1):1–9.
40. Kawamoto R, Tabara Y, Kohara K, et al. Hematological parameters are associated with metabolic syndrome in Japanese community-dwelling persons. Endocrine. 2013;43(2):334–341. doi:10.1007/s12020-012-9662-7
41. He SY, Lu S, Gu HX, et al. Association of hemoglobin level with type 2 diabetes in middle-aged and elderly population in Shanghai Chongming District. Chin J Diabetes. 2020;12(05):297–304.
42. Sonmez A, Yilmaz MI, Saglam M, et al. The relationship between hemoglobin levels and endothelial functions in diabetes mellitus. Clin J Am Soc Nephrol. 2010;5(1):45–50. doi:10.2215/CJN.05080709
43. Zhang W, Chen Q, Yuan Z, et al. A routine biomarker-based risk prediction model for metabolic syndrome in urban Han Chinese population. BMC Public Health. 2015;15(1):1–9. doi:10.1186/s12889-015-1424-z
44. Assumpção CRL, Brunini TMC, Pereira NR. Insulin resistance in obesity and metabolic syndrome: is there a connection with platelet l-arginine transport? Blood Cells Mol Dis. 2010;45(4):338–342. doi:10.1016/j.bcmd.2010.10.003
45. Moan A, Nordby G, Os I, et al. Relationship between hemorrheologic factors and insulin sensitivity in healthy young men. Metabolism. 1994;43(4):423–427. doi:10.1016/0026-0495(94)90070-1
46. Zhang YL, Li XL. Value of serum ferritin, hemoglobin, and glycosylated hemoglobin during the first and the second trimester of pregnancy for predicting their risk of gestational diabetes mellitus. Chin J Fam Plan. 2021;29(7):1502–1506.
47. Shan ZM, Xia XH, Qian XH, et al. The research on the correlation between male metabolic syndrome and erythrocyte parameters. Zhejiang Med Educ. 2016;15(2):58–60.
48. Miyagawa S, Kobayashi M, Konishi N, Sato T, Ueda K. Insulin and insulin‐like growth factor I support the proliferation of erythroid progenitor cells in bone marrow through the sharing of receptors. Br J Haematol. 2000;109(3):
49. Aoki I, Taniyama M, Toyama K, Homori M, Ishikawa K. Stimulatory effect of human insulin on erythroid progenitors (CFU‐E and BFU‐E) in human CD34+ separated bone marrow cells and the relationship between insulin and erythropoietin. Stem Cells. 1994;12(3):
50. Wang GL, Semenza GL. Molecular basis of hypoxia‐induced erythropoietin expression. Curr Opin Hematol. 1996;3(2):
51. Semenza GL. Regulation of mammalian O2 homeostasis by hypoxia‐inducible factor 1. Annu Rev Cell Dev Biol. 1999;15(1):
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tumor Necrosis Factor Alpha Level in the Uterine Fluid of Patients with Polycystic Ovary Syndrome and Its Correlation with Clinical Parameters
Ha LX, Li WX, Du YD, Yuan YY, Qu XX
Journal of Inflammation Research 2022, 15:6015-6020
Published Date: 29 October 2022
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Effect of Consultation Number on the Assessment and Treatment of Polycystic Ovary Syndrome
Wang Y, Chen J, Dong H, Ma RL, Zou Y, Wang W, Zheng Q, Feng Y, Tan Z, Zeng X, Zhao Y, Deng Y, Wang Y, Gu B, Sun A
International Journal of Women's Health 2024, 16:527-541
Published Date: 25 March 2024
Association Between rs2278426 Polymorphism of the ANGPTL8 Gene and Polycystic Ovary Syndrome
Wu H, Wang H, Sun L, Liu M, Wang H, Sun X, Zhang W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1749-1760
Published Date: 16 April 2024
Glycolytic Dysfunction in Granulosa Cells and Its Contribution to Metabolic Dysfunction in Polycystic Ovary Syndrome
Cao Z, Zhou Q, An J, Guo X, Jia X, Qiu Y
Drug Design, Development and Therapy 2025, 19:5255-5270
Published Date: 18 June 2025