Back to Journals » Journal of Pain Research » Volume 19
Efficacy of Acupuncture for Pain in Parkinson’s Disease: Study Protocol for a Randomized Controlled Trial
Authors Wu Y, Zhang F, Xiao L, Wang Y, Lin S, Wu S, Liu X ![]() , Zhuang L
, Zhuang L ![]()
Received 26 May 2026
Accepted for publication 24 June 2026
Published 29 June 2026 Volume 2026:19 622950
DOI https://doi.org/10.2147/JPR.S622950
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yixuan Wu1, Fan Zhang1, Liangman Xiao1, Yuting Wang2, Shumin Lin1, Shunan Wu1, Xin Liu3, Lixing Zhuang4
1The First Clinical Medical College, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China; 2Department of Rehabilitation, Shenzhen Hospital (Fu Tian) of Guangzhou University of Chinese Medicine, Shenzhen, Guangdong, People’s Republic of China; 3Department of General Practice, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China; 4Lingnan Institute of Acupuncture and Rehabilitation, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Xin Liu, Department of General Practice, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]; Lixing Zhuang, Lingnan Institute of Acupuncture and Rehabilitation, The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Introduction: Pain in Parkinson’s disease (PD) is common and significantly reduces quality of life, yet it is often poorly managed. As current treatments have limitations, acupuncture may offer a non-pharmacological option. This trial aims to evaluate the efficacy and safety of acupuncture versus sham acupuncture for pain in PD.
Material and Methods: This prospective, double-blind, randomized controlled trial will enroll 66 patients with Parkinson’s disease-related pain at the First Affiliated Hospital of Guangzhou University of Chinese Medicine between April 2026 and June 2027. Participants will be allocated via block randomization to either an acupuncture group or a sham acupuncture group. Rigorous blinding of patients, practitioners, outcome assessors, and statisticians will be implemented. Both groups will receive 12 sessions (3 sessions per week for 4 weeks) of their assigned intervention while maintaining stable anti-PD medication. The primary outcome is the change in the King’s Parkinson’s Disease Pain Scale (KPPS) score. Secondary outcomes include the painDETECT Questionnaire (PD-Q), Unified Parkinson’s Disease Rating Scale (UPDRS), 39-item Parkinson’s Disease Questionnaire (PDQ-39), Hamilton Depression Rating Scale (HAMD), somatosensory evoked potentials (SSEPs), and serum levels of Tumor Necrosis Factor-alpha (TNF-α), S100 calcium-binding protein B (S100B), and Glial Fibrillary Acidic Protein (GFAP). All analyses will follow the intention-to-treat principle.
Discussion: Pain in PD is prevalent but undertreated due to limited evidence, invasiveness, or high cost of current therapies. This study aims to determine if acupuncture significantly reduces pain scores compared to sham acupuncture, potentially offering an effective, safe, and cost-effective complementary option. By assessing changes in serum biomarkers, it will also explore whether acupuncture’s effects involve modulating neuroinflammation. With its rigorous design, this trial is expected to provide high-level evidence for integrating acupuncture into PD pain management.
Trial Registration: International Traditional Medicine Clinical Trial Registry (ITMCTR2026000325).
Keywords: Parkinson’s disease, pain, acupuncture, randomized controlled trial, sham acupuncture
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disorder caused by the degeneration of substantia nigra dopaminergic neurons and the abnormal aggregation of alpha-synuclein (α-syn).1 In addition to typical motor symptoms, such as bradykinesia, resting tremor, muscle rigidity, and postural instability, non-motor symptoms represented by pain, depression, and sleep disturbances often appear early in the disease course, sometimes even preceding motor symptoms.2 Among these, pain occurs in up to 68%–95% of patients3 and is frequently complicated by other conditions such as motor disorders, anxiety, and depression,4 which severely affect patients’ quality of life. However, the effective treatment rate for pain in PD in clinical practice is currently less than 38%,5 indicating that clinical recognition and management remain inadequate.
Current primary clinical interventions for pain in PD include pharmacological therapy, rehabilitation and physiotherapy, and surgical intervention. However, existing treatments have limitations, such as insufficient evidence grading, invasiveness, and high costs.6 Therefore, it is necessary to explore more therapeutic options for pain in PD. In recent years, multiple studies have suggested that acupuncture may have an ameliorative effect on pain in PD.7 Its mechanism may involve enhancing or modulating key brain regions related to pain perception or activating endogenous analgesic systems, thereby exerting an analgesic effect.8 Acupuncture offers a new therapeutic option for pain in PD.
Thus, this study intends to conduct a single-center, double-blind, block-randomized, parallel-controlled clinical trial. By comparing the efficacy between the acupuncture group and the sham acupuncture group in treating pain in PD, this study aims to investigate the therapeutic effect of acupuncture on patients with pain in PD and to provide an effective, safe, and more evidence-based treatment option for the management of pain in PD.
Material and Methods
This prospective, double-blind, randomized controlled clinical trial targets patients with pain in PD in China. It will be conducted at the First Affiliated Hospital of Guangzhou University of Chinese Medicine from April 2026 to June 2027. The protocol has been approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine, and will follow the principles of the Declaration of Helsinki. The trial is registered with International Traditional Medicine Clinical Trial Registry (ITMCTR2026000325). The protocol was developed in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT), and the checklist is provided as an attachment. A total of 66 eligible patients with pain in PD will be enrolled. The study flowchart is shown in Figure 1.
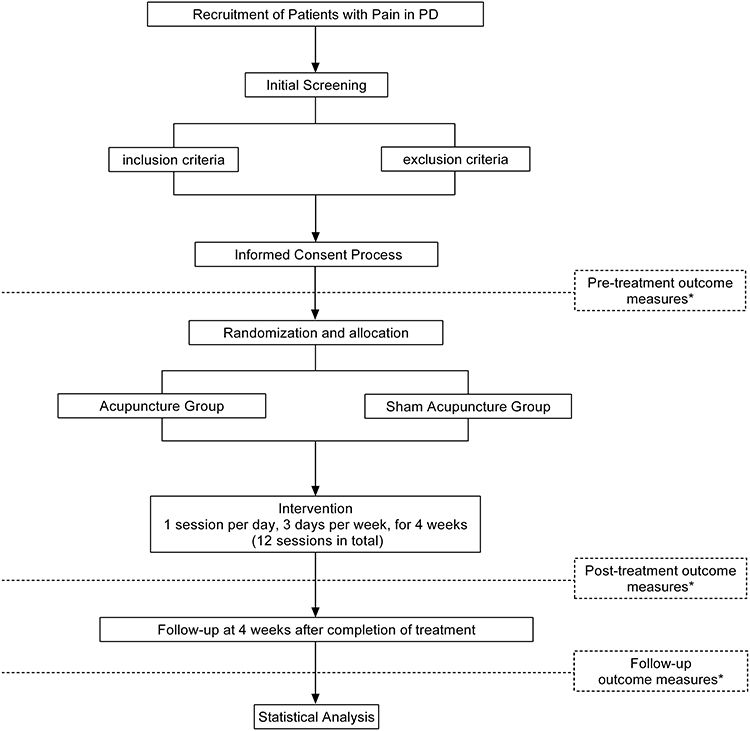 |
Figure 1 Flowchart of the trial. The asterisk indicates the outcome measures assessed at the corresponding time points, including KPPS, PD-Q, UPDRS, PDQ-39, HAMD, SSEPs, TNF-α, S100B, and GFAP. Abbreviations: PD, Parkinson’s disease; KPPS, King’s Parkinson’s Disease Pain Scale; PD-Q, painDETECT Questionnaire; UPDRS, Unified Parkinson’s Disease Rating Scale; PDQ-39, 39-item Parkinson’s Disease Questionnaire; HAMD, Hamilton Depression Rating Scale; SSEPs, somatosensory evoked potentials; TNF-α, tumor necrosis factor-α; S100B, S100 calcium-binding protein B; GFAP, glial fibrillary acidic protein. |
Diagnostic Criteria
The diagnostic criteria for PD refer to the “Chinese Diagnostic Criteria for Parkinson’s Disease (2016 Edition)”.9 The diagnostic criteria for pain refer to the revised definition of pain by the International Association for the Study of Pain (IASP).10 Based on meeting the above diagnostic criteria for PD and pain, and to clarify the correlation between pain symptoms and PD, the criteria for determining pain in PD from the Parkinson’s disease pain classification system questionnaire (PD-PCS)6 were referenced: ① The pain occurs after the onset of PD symptoms or worsens with disease progression; ② The pain intensifies when limb rigidity, tremor, or bradykinesia worsens; ③ The pain is associated with dyskinesia (eg., choreiform movements); ④ The pain is alleviated after taking PD medication. Meeting any one of the above four criteria is sufficient for diagnosis.
Inclusion Criteria
The inclusion criteria are as follows:
- Aged 45–80 years, both males and females are eligible.
- Hoehn–Yahr stage 1–3.
- Have been on anti-PD medication for at least six months, with a stable dose maintained for at least one month prior to enrollment.
- Able to understand and voluntarily sign the informed consent form.
- Meet the diagnostic criteria for pain in PD.
- Visual Analog Scale (VAS) score between 1 and 6, indicating mild-to-moderate pain.
Exclusion Criteria
The exclusion criteria are as follows:
- Patients with severe cognitive impairment and hallucinations who are unable to cooperate with scale assessments.
- Patients with severe comorbidities, including senile psychosis, epilepsy, malignant tumors, endocrine and metabolic diseases, or severe cardiac, pulmonary, hepatic, renal, or other organ-related diseases.
- Participation in other clinical trials involving drugs, acupuncture, or other interventions within one month prior to enrollment in this study.
- Inability to regularly take anti-PD medication due to adverse reactions or other reasons.
- Patients who have previously undergone or plan to undergo deep-brain stimulation therapy or rectal infusion of levodopa during the study period.
- Female patients who are pregnant, breastfeeding, or planning to become pregnant in the near future.
- Patients unable to cooperate with acupuncture treatment.
- Patients requiring analgesic medications such as opioids or nonsteroidal anti-inflammatory drugs.
Sample Size
Based on the objectives of this study, the King’s Parkinson’s Disease Pain Scale (KPPS) was selected as the primary outcome measure. According to preliminary research conducted by our team and relevant studies reporting KPPS outcomes in patients with PD-related pain, the expected mean KPPS score for the acupuncture condition was estimated from a prior acupuncture study (21.59 ± 5.43),11 while the expected mean KPPS score for the comparator condition was estimated from the control condition of a prior study on PD-related pain (28.45 ± 8.89).12 With a statistical power of 0.90 and a two-sided significance level of 0.05, the required sample size per group was calculated as 26 by a statistician using PASS 2025. Accounting for a 20% dropout rate, the final total sample size was determined to be 66, with 33 participants allocated to each group.
Recruitment of Participants
Participants will be recruited at the First Affiliated Hospital of Guangzhou University of Chinese Medicine from April 2026 to June 2027 through recruitment advertisements and WeChat promotion.
Randomization
Allocation will be performed using a block randomization method. Based on the sample size estimation, the 66 patients required for the study will be randomly assigned to either the Acupuncture Group or the Sham Acupuncture Group according to a sequence generated by a statistician using SPSS 26.0. The block size will remain concealed until after the study is completed. The generated random numbers will be placed in opaque, sealed envelopes and kept by an independent randomization coordinator. The coordinator will not be involved in participant recruitment, intervention delivery, or outcome assessment. Each envelope will contain only a group code (“Group A” or “Group B”). The coordinator will translate the group code into a corresponding treatment kit—either containing genuine or sham acupuncture devices—by referring to a confidential “Treatment Kit Allocation Table.” The two types of kits will be visually identical. This allocation table will be kept confidential from the investigators, participants, and outcome assessors until the conclusion of the study.
Blinding
This trial will implement blinding for the acupuncturists, participants, outcome assessors, and statisticians. Prior to the start of treatment, the coordinator will provide the acupuncturist with the prepared treatment kit. The acupuncturist will be unaware of the group code corresponding to the kit. Throughout the treatment session, participants will wear eye masks. Upon completion of the treatment, the coordinator will remove the needles to ensure that both the acupuncturist and the participant remain blinded. The aforementioned coordinator will not be involved in acupuncture administration, outcome assessment, or statistical analysis.
The needle devices used in this study were developed and designed by the Parkinson’s Disease Research Team led by Zhuang Lixing. The needle system for the acupuncture group consists of a base, a guide tube, and a standard acupuncture needle, with the needle housed within the guide tube. The needle system for the sham acupuncture group consists of a base, a guide tube, and a specially designed blunt-tip needle, which is also housed within the guide tube. The base of each device features an adhesive layer on its bottom surface, allowing it to adhere securely to the skin and prevent displacement during treatment. During use, the standard acupuncture needle in the acupuncture group can penetrate the skin through the adhesive layer, while the blunt-tip needle in the sham group, when pressure is applied, generates tactile pressure on the skin via the adhesive layer. This provides participants with a somatosensory sensation similar to needle insertion without actual skin penetration. Simultaneously, the acupuncturist experiences a tactile feedback of initial resistance followed by a sudden give when advancing the blunt-tip needle, closely simulating the subcutaneous penetration process of real acupuncture. Both the acupuncture and sham needle systems are available in two types—vertical and oblique insertion—to accommodate the operational requirements of different acupuncture points. The external appearance of the needle system is shown in Figure 2. The specific steps for using the needle device are as follows: The acupuncturist first performs routine disinfection of the skin at the acupoint. Then, the protective film covering the adhesive layer on the base bottom is removed (as shown in Figure 3), allowing the adhesive to firmly adhere to the skin over the acupoint. Next, while stabilizing the device with one hand, the acupuncturist uses the other hand to press the needle handle until the needle body is fully inserted into the base (as shown in Figure 4). It is important to note that the handles of both the genuine and sham needles are of equal length, while the needle bodies differ slightly in length. Prior to acupuncture, since the needle body is concealed within the guide tube and only the handle of equal length is visible, the two devices appear identical. After insertion, the slightly shorter body of the sham needle creates a visual impression of partial needle penetration into the skin, ensuring that both participants and acupuncturists remain blinded to group allocation throughout the treatment based on visual and tactile cues. The aforementioned needle system has been granted a Chinese National Utility Model Patent (Patent No.: ZL202121352221.7) and is standardized, produced, and supplied by the manufacturer “Laozongyi Co. Ltd.” which holds the requisite medical device production qualifications.
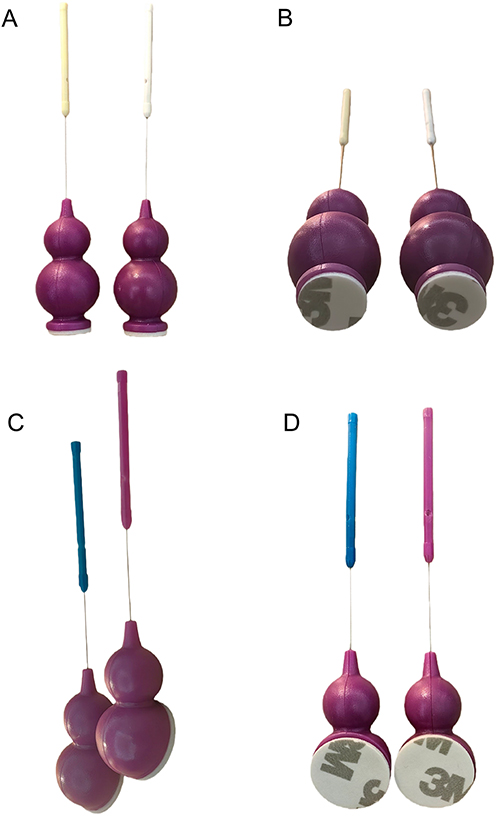 |
Figure 2 External views of the needle device system. (A) Front view of the acupuncture and sham needle devices for perpendicular insertion (90°). (B) Bottom view of the acupuncture and sham needle devices for perpendicular insertion (90°). (C) Lateral view of the acupuncture and sham needle devices for oblique insertion (15°). (D) Top view of the acupuncture and sham needle devices for oblique insertion (15°). The colors of the needle handles were randomly assigned and did not indicate whether a device was a genuine acupuncture needle or a sham needle; therefore, the handle colors could not be used to infer the needle type or treatment allocation. |
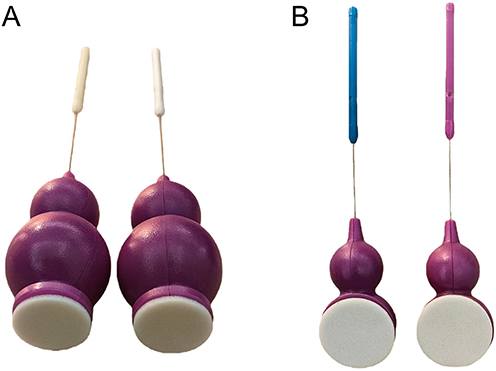 |
Figure 3 Removal of the adhesive protective film from the base bottom. (A) Removal of the adhesive protective film from the bases of the acupuncture and sham needle devices for perpendicular insertion (90°). (B) Removal of the adhesive protective film from the bases of the acupuncture and sham needle devices for oblique insertion (15°). |
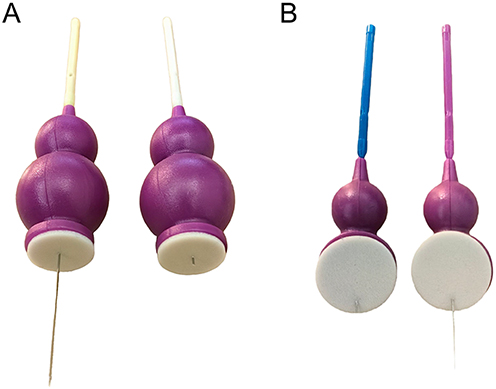 |
Figure 4 Needle body fully inserted into the base. (A) Acupuncture and sham needle devices for perpendicular insertion (90°) after the needle body was fully inserted into the base. From left to right: acupuncture needle device and sham needle device. (B) Acupuncture and sham needle devices for oblique insertion (15°) after the needle body was fully inserted into the base. From left to right: sham needle device and acupuncture needle device. |
Unblinding will be performed at the conclusion of the study, and participants will be informed of their group allocation and the acupuncture method they received. For the purpose of this trial, serious adverse events refer to adverse events that result in death, are life-threatening, require hospitalization or prolongation of existing hospitalization, result in persistent or significant disability or incapacity, or constitute other medically important events requiring intervention to prevent these outcomes; all other adverse events will be regarded as non-serious adverse events. In the event that a participant experiences a serious adverse event during the trial, and the investigator determines that immediate clarification of the intervention is necessary for urgent medical management, the investigator is authorized to conduct emergency unblinding for that participant to facilitate appropriate emergency treatment. For non-serious adverse events, blinding will be maintained whenever the event can be safely managed according to the predefined management procedures without knowledge of group allocation. If knowledge of the actual intervention or needle device type is considered necessary to ensure participant safety during the management of a non-serious acupuncture-related adverse event, such as difficulty in device removal, suspected needle breakage, or a retained needle fragment, participant-specific safety unblinding may be performed. In such cases, unblinding will be restricted to personnel directly involved in clinical management, including the treating acupuncturist when clinically necessary, whereas outcome assessors, statisticians, and other research staff will remain blinded whenever possible. The reason for unblinding, date and time, personnel unblinded, treatment allocation disclosed, management measures, subsequent trial status of the participant, continuation of treatment and assessment, and analysis set classification will be documented in the CRF and reviewed by the Research Safety and Quality Monitoring Committee; unblinded participants will be included in the Full Analysis Set but not in the Per-Protocol Set.
Interventions
All acupuncturists involved in the study have received formal education in traditional Chinese medicine institutions, hold a valid Physician Qualification Certificate, and possess over one year of clinical acupuncture experience. Additionally, prior to the commencement of the study, all treating acupuncturists will undergo systematic training to ensure procedural consistency. Throughout the entire treatment period, each participant will be assigned to the same treating acupuncturist.
Acupuncture Group
Participants in the acupuncture group will receive acupuncture treatment once per session on Mondays, Wednesdays, and Fridays each week, totaling three sessions per week. Each treatment session will last 30 minutes. The intervention will be conducted over a continuous period of 4 weeks, resulting in a total of 12 treatment sessions. Following the completion of treatment, a 4-week follow-up period will be implemented. Throughout the treatment and follow-up phases, the effective dosage of existing anti-PD medication will be maintained. Any necessary adjustments to the medication dosage due to special circumstances will be documented in the Case Report Form (CRF).
The acupoints selected for the acupuncture group include Four Divine Needles (composed of GV21, GV19, and two bilateral points located 1.5 B-cun lateral to GV20), GV24, GV29, bilateral HT7, bilateral SP6, and GV25. The localization of Four Divine Needles is based on the “Application of Jin’s Three-Needle Acupoint Group”13 while the localization of all other acupoints follows the national standard of the People’s Republic of China, “Nomenclature and Location of Meridian Points” (GB/T 12346–2021).14
The acupuncture procedure utilizes a genuine needle system, which includes a base, a guide tube, and standard acupuncture needles (specification for the acupuncture needle used in perpendicular insertion: φ0.35 mm×65 mm, specification for the acupuncture needle inserted at a 15-degree angle: φ0.35 mm×50 mm, manufactured by Laozongyi Co. Ltd)., sterile medical cotton swabs (specification: 12cm, produced by Foshan Shunde Kangzheng Hygiene Materials Co., Ltd)., and Anerdian skin disinfectant (specification: 60mL/bottle, manufactured by Likang Pharmaceutical Technology Jiangsu Co., Ltd).
During the treatment, patients will wear eye masks throughout the procedure. Following routine skin disinfection, the acupuncturist will place the needles on the skin over the selected acupoints. For Four Divine Needles, GV24, and GV29, needles will be inserted at a 15-degree angle. For GV25, bilateral HT7, and bilateral SP6, needles will be inserted at a 90-degree angle. All needles will be inserted through a guide tube and a perforated base placed on the skin. The precise locations of each acupoint are detailed in Table 1 and Figure 5. The needles will be retained for 30 minutes. After 30 minutes, the coordinator will remove the needles to prevent unblinding.
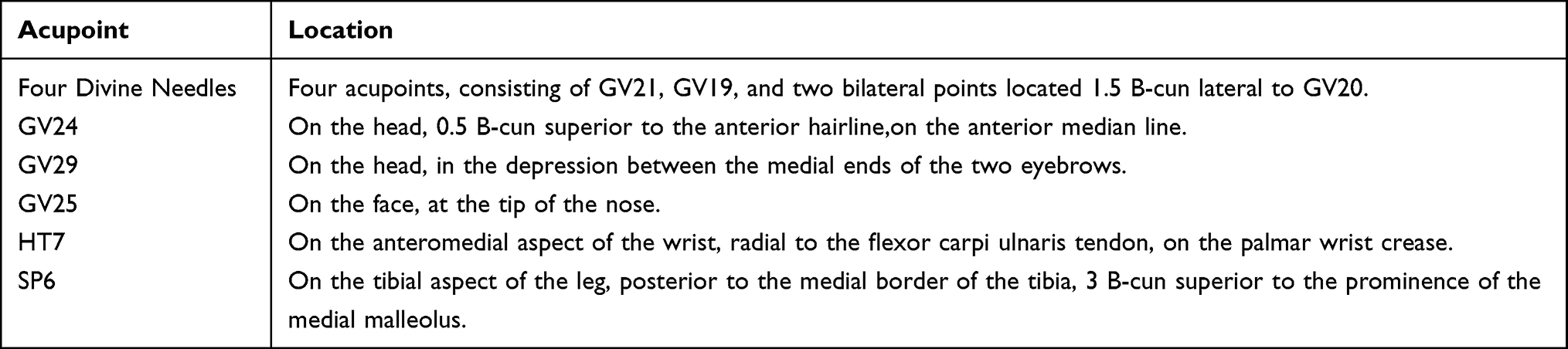 |
Table 1 The Location of Each Acupoint |
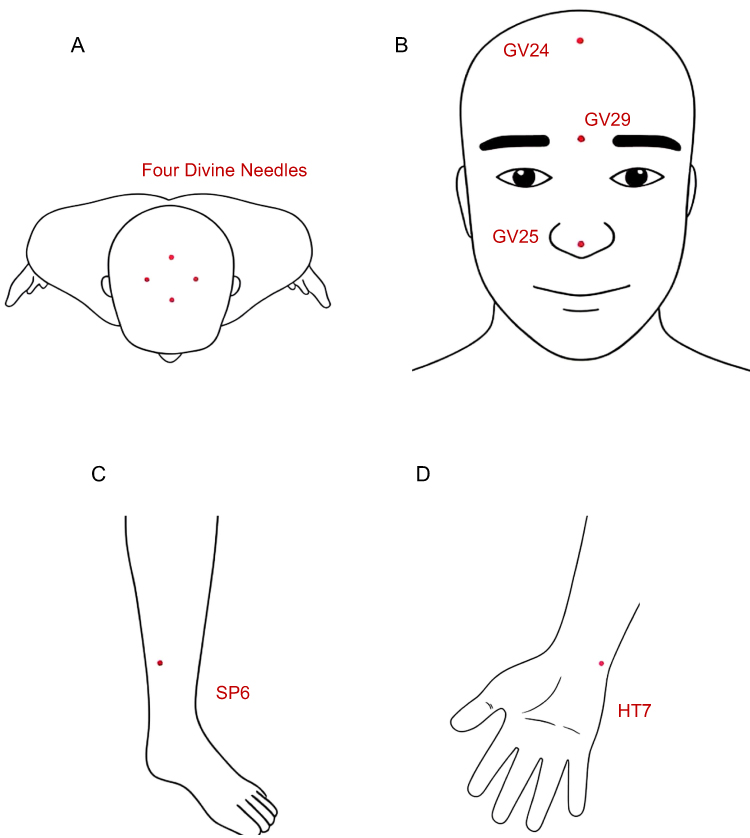 |
Figure 5 Locations of the selected acupoints. (A) Locations of the Four Divine Needles. (B) Locations of GV24, GV29, and GV25. (C) Location of SP6; bilateral SP6 was used in this trial, with one side shown as a representative illustration. (D) Location of HT7; bilateral HT7 was used in this trial, with one side shown as a representative illustration. |
The Sham Acupuncture Group
Participants in the sham acupuncture group will receive sham acupuncture treatment once per session on Mondays, Wednesdays, and Fridays each week, totaling three sessions per week. Each treatment session will last 30 minutes. The intervention will be administered over a continuous period of 4 weeks, resulting in a total of 12 treatment sessions. Following the completion of treatment, a 4-week follow-up period will be implemented. Throughout the treatment and follow-up phases, the effective dosage of existing anti-PD medication will be maintained. Any necessary adjustments to the medication dosage due to special circumstances will be documented in the CRFs.
The sham acupuncture group will use exactly the same acupoint locations as the acupuncture group. The sham acupuncture procedure utilizes a sham needle system, which includes a base, a guide tube, and blunt-tip needles (specification for the blunt-tip needle used in perpendicular insertion: φ0.35mm×42mm, specification for the blunt-tip needle inserted at a 15-degree angle: φ0.35mm×36mm, manufactured by Laozongyi Co. Ltd)., sterile medical cotton swabs (specification: 12cm, produced by Foshan Shunde Kangzheng Hygiene Materials Co., Ltd)., and Anerdian skin disinfectant (specification: 60mL/bottle, manufactured by Likang Pharmaceutical Technology Jiangsu Co., Ltd).
During the treatment, patients will wear eye masks throughout the procedure. Following routine skin disinfection, the acupuncturist will place the sham needle device on the skin over the acupoint and apply pressure through the guide tube, allowing the patient to experience a mild needling sensation without skin penetration. The sham needles will remain in place for 30 minutes. After 30 minutes, the coordinator will remove the devices to prevent unblinding. The acupoint selection, needle retention duration, removal procedure, and treatment frequency in the sham acupuncture group are identical to those in the acupuncture group. Upon completion of the study, participants in the sham acupuncture group will be offered the same genuine acupuncture treatment as the acupuncture group as compensation, based on their personal preference.
Outcome Measure
Prior to the commencement of the study, baseline information will be collected from participants, including name, age, sex, disease duration, education level, levodopa equivalent daily dose, and prior acupuncture experience. The primary outcome measure will be the KPPS. Secondary outcome measures will include the painDETECT Questionnaire (PD-Q), the Unified Parkinson’s Disease Rating Scale (UPDRS), the 39-item Parkinson’s Disease Questionnaire (PDQ-39), the Hamilton Depression Rating Scale (HAMD), Somatosensory Evoked Potentials (SSEPs) measurement, serum levels of Tumor Necrosis Factor-alpha (TNF-α), S100 calcium-binding protein B (S100B), and Glial Fibrillary Acidic Protein (GFAP). Serum biomarkers will be assayed using Enzyme-Linked Immunosorbent Assay (ELISA). The blinding status of participants and research personnel was assessed by calculating Bang’s blinding index15 based on data collected from the Acupuncture Perception (Credibility) Scale (APS).16 The specific schedule for these assessments is detailed in Table 2.
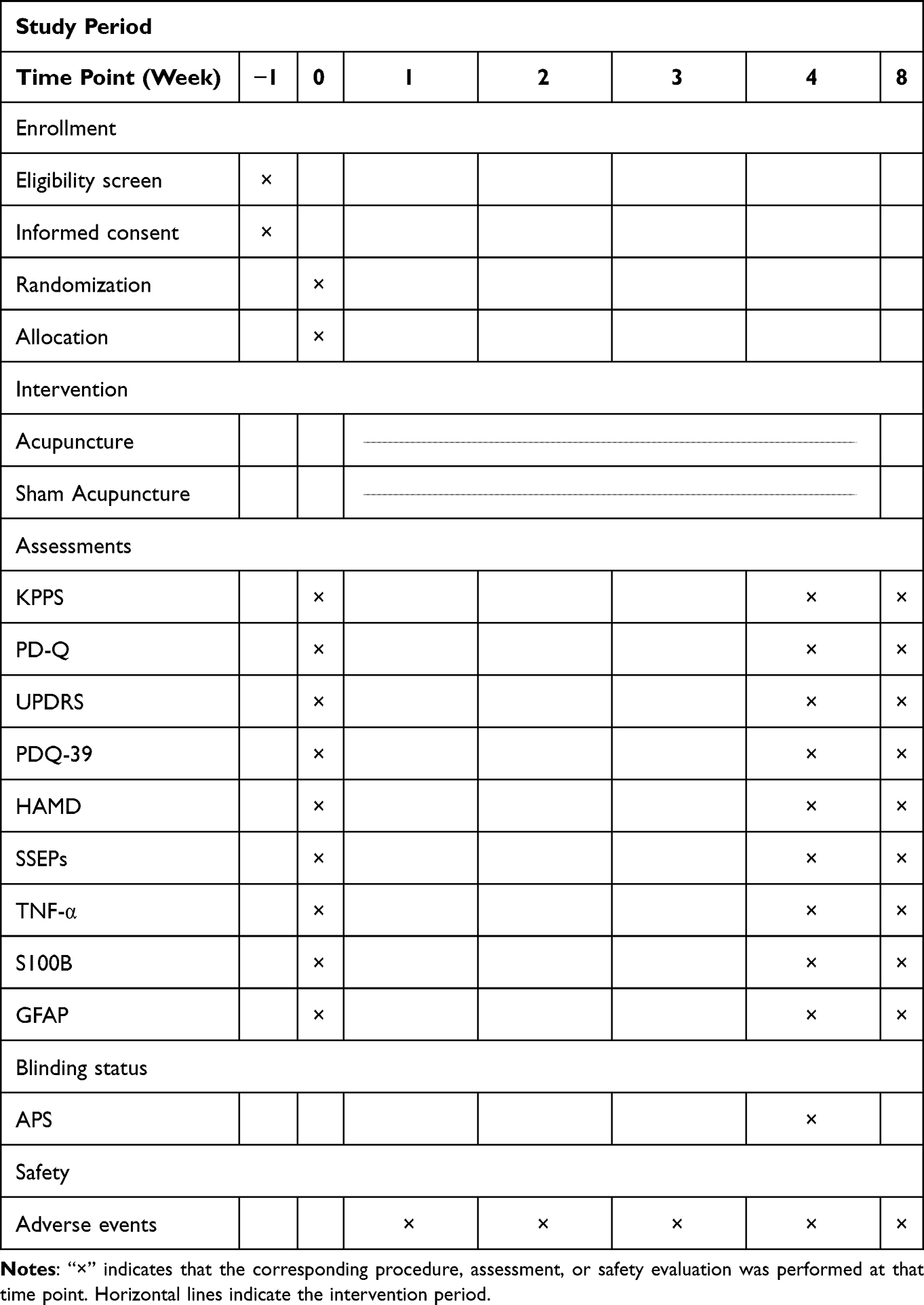 |
Table 2 Schedule of Enrollment, Intervention, Assessment and Safety |
Primary Outcome
King’s Parkinson’s Disease Pain Scale (KPPS)
The KPPS is currently a recommended scale for assessing pain in PD. It comprises seven dimensions across a total of 14 items: musculoskeletal pain (1 item), chronic pain (2 items), fluctuation-related pain (3 items), nocturnal pain (2 items), orofacial pain (3 items), swelling/pain associated with edema (2 items), and radicular pain (1 item). The total possible score is 168. Each item is scored from 0 to 12, derived by multiplying the severity of pain (rated on a scale of 0–3) by its frequency (rated on a scale of 0–4). A higher score indicates greater pain severity.
Secondary Outcomes
PainDETECT Questionnaire (PD-Q)
The PD-Q is a tool used to assess the neuropathic components of pain (eg., burning, electric shock-like sensations, pain evoked by light touch) and symptoms of paresthesia (eg., numbness, tingling). The total score, calculated by summing the weighted scores of all items, has a maximum of 38 points. A higher total score indicates a greater likelihood of neuropathic pain origin. A PD-Q score below 12 suggests that neuropathic pain is unlikely, a score between 13 and 18 indicates an uncertain result (suggestive of possible mixed pain), and a score of 19 or above highly suggests neuropathic pain. This scale can compensate for the KPPS’s limited capacity to identify neuropathic pain.
Unified Parkinson’s Disease Rating Scale (UPDRS)
The UPDRS is a commonly used scale for evaluating patients with PD. It provides an objective assessment of various aspects, including motor symptoms, activities of daily living, disease progression, post-treatment status, treatment side effects, and complications. Specifically, UPDRS Part I assesses the participant’s mentation, behavior, and mood. UPDRS Part II assesses activities of daily living, and UPDRS Part III assesses motor signs. Higher scores indicate more severe symptoms.
39-Item Parkinson’s Disease Questionnaire (PDQ-39)
This questionnaire consists of eight dimensions: mobility (10 items), activities of daily living (6 items), emotional well-being (6 items), stigma (4 items), social support (3 items), cognition (4 items), communication (3 items), and bodily discomfort (3 items). It comprises a total of 39 items, each scored from 0 to 4. The PDQ-39 reflects the patient’s quality of life over the past month. Higher scores indicate a lower quality of life.
Hamilton Depression Rating Scale (HAMD)
The HAMD is used to assess the severity of depressive symptoms. The total score is the sum of all item scores, comprising 17 observer-rated items organized into five factor structures. A higher score indicates more severe depressive symptoms in the patient. Specifically, an HAMD score below 7 points is considered normal, a score between 7 and 17 points indicates mild depression, a score between 17 and 24 points indicates moderate depression, and a score above 24 points indicates severe depression.
Somatosensory Evoked Potentials (SSEPs)
Typically, electrical stimulation or thermal electrode stimulation is applied to the sural nerve to evoke the spinal-level nociceptive withdrawal reflex and the centrally mediated nociceptive flexion reflex. Pain threshold and pain sensitivity are quantified by recording both the spinal nociceptive reflex and the electromyographic reflex of the gastrocnemius muscle.
Blood Serum Index
The therapeutic effect of acupuncture on pain in PD may be associated with the amelioration of neuroinflammation and repair of the blood-brain barrier (BBB). TNF-α is a key pro-inflammatory cytokine that can activate astrocytes and promote their expression of GFAP, thereby forming a self-amplifying inflammatory cycle that exacerbates neural damage.17 S100B is predominantly found in the central nervous system, and elevated levels in peripheral blood can serve as a marker of impaired BBB integrity.18 During the pathological process of PD, increased BBB permeability may facilitate the entry of peripheral inflammatory signals into the central nervous system,19 further activating microglia and astrocytes and aggravating neuroinflammation and neurodegeneration.20 Monitoring the changes in the aforementioned indicators at baseline, at the end of treatment, and at the 4-week follow-up will help elucidate whether acupuncture exerts neuroprotective effects by modulating neuroinflammation and repairing the BBB.
Serum concentrations of TNF-α, S100B, and GFAP will be measured at baseline, at the end of treatment, and at the 4-week follow-up using ELISA according to the kit instructions. All ELISA kits will be provided by Jiangsu Enzyme Free Industrial Co., Ltd.
Blinding Assessment
After treatment, group allocation guesses will be collected from participants and investigators using the APS. These data will be used to calculate Bang’s blinding index, which objectively quantifies the success of blinding. The index ranges in absolute value from 0 to 1, where a higher absolute value denotes a greater deviation from random guessing and thus poorer blinding integrity. Prior acupuncture experience will be recorded and considered when interpreting the results of the blinding assessment.
Safety Evaluation
All adverse events occurring during the study implementation—such as needle fainting, needle breakage, hematoma, and infection—along with their management measures, shall be documented. In the event of any serious adverse event, treatment will be terminated immediately and emergency measures will be implemented, with simultaneous reporting to the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine. All adverse events will be categorized and reported in accordance with the CONSORT Harms reporting guidelines.21
Follow-Up
After the completion of treatment, subjects will undergo a 4-week follow-up period, during which primary and secondary outcome measures will be assessed to evaluate the long-term efficacy of acupuncture.
Data Management and Quality Control
To ensure trial quality and data reliability, all research personnel will receive standardized training before the study initiation. The training content will cover acupoint localization, sham needle operation, scale assessment, collection and testing of serum samples, participant communication, and follow-up procedures.
Assessors must be proficient in completing the CRFs and conduct objective evaluations of the participants. Both the assessors and participants are required to co-sign the CRFs to confirm the data. All study documents will be securely stored, and electronic data will be managed under strict access control, permitting only authorized personnel to view or modify the data. Regular data quality control will be conducted throughout the trial to verify the completeness and accuracy of the data.
Study Safety and Quality Monitoring
The Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine will be responsible for the safety and quality monitoring of this study. It may propose modifications to the study design based on the principle of protecting participants, with the final decision to be made by the principal investigator. All participants must provide written informed consent before enrollment.
The following adverse events may occur during this study, primarily including acupuncture-related incidents such as needle fainting, bent needles, stuck needles, broken needles, and hematomas, as well as exacerbation of symptoms or acute events in patients with underlying conditions such as hypertension or coronary heart disease during acupuncture. Standardized management protocols have been established for these situations: In the event of needle fainting, needles will be removed immediately, and the patient will be placed in a supine position, with warm sugared water administered orally as needed. For bent or stuck needles, needles will be gently removed by adjusting the patient’s posture, applying local massage along the meridian, or applying counter-rotation based on the degree of bending or direction of muscle fiber entanglement. In case of a broken needle, the patient will be instructed to remain still, and the fragment will be removed with forceps or, if necessary, through surgical intervention depending on its location. Local hematomas will be managed with cold compression initially to stop bleeding, followed by warm compression to promote absorption. If patients with underlying conditions experience symptoms such as a sharp increase in blood pressure or chest pain, acupuncture will be terminated immediately, vital signs will be assessed, appropriate emergency medications will be administered, and preparations will be made for cardiopulmonary resuscitation or emergency referral. When unexpected serious adverse events occur, the attending physician must report to the project leader within 24 hours, who will then notify the Research Safety and Quality Monitoring Committee for documentation. To ensure participant safety, participant-specific safety unblinding will be initiated according to predefined procedures when necessary, including emergency unblinding for serious adverse events and limited unblinding for non-serious events when clinically required. All adverse events and management procedures must be fully documented and archived.
The Research Safety and Quality Monitoring Committee will review this study every three months. The review will include documents such as the study protocol, ethical approval, informed consent forms, and case report forms, with a focus on verifying the compliance of participant baseline information, the appropriateness of blinded group code assignments, the standardization of adverse event records, and the completeness of outcome data.
Statistical Analysis
This study will adopt the Intention-To-Treat (ITT) principle, with the Full Analysis Set (FAS) serving as the primary analysis set for statistical analysis of patients who were centrally randomized and received at least one treatment session. Concurrently, a Per-Protocol Set analysis will be conducted as a sensitivity analysis to evaluate the robustness of the results. For missing data in the primary outcome, the prespecified primary analysis model and the sensitivity analysis based on multiple imputation are described below.
Data entry and management will be performed by independent researchers not involved in treatment delivery or outcome assessment. Double data entry will be employed to ensure accuracy. Statistical analysis will be conducted using SPSS 26.0. For continuous variables, normality will be assessed using the Shapiro–Wilk test. Data conforming to a normal distribution will be described as mean ± standard deviation and compared between groups using the independent samples t-test (if variances are homogeneous) or Welch’s corrected t-test (if variances are heterogeneous). Non-normally distributed continuous variables will be summarized as median and interquartile range and compared with the Mann–Whitney U-test. Categorical variables will be expressed as counts and percentages and compared between groups using the chi-square test; when more than 20% of expected cell counts are less than 5, Fisher’s exact test will be applied. All baseline comparisons are intended only to describe the balance between groups after randomization and not for inferential purposes.
For continuous variables with repeated measurements, the primary analysis will employ a linear mixed model, with “group”, “time”, and “group × time” included as fixed effects, and a random intercept for each participant to account for within-subject correlations across repeated measurements. The primary endpoint will be the between-group difference in the change in the primary outcome from baseline to the end of treatment, while the follow-up assessment will be used to evaluate the durability of the treatment effect. The statistical significance of the “group × time” interaction effect will also be examined. If the “group × time” interaction is statistically significant, post-hoc simple-effects analyses will be conducted, including between-group comparisons at each time point and within-group comparisons of different time points with baseline. The P-values will be adjusted using the Bonferroni method.
Missing post-baseline data for the primary outcome will not be directly replaced in the primary analysis. The linear mixed model will use all available observed repeated measurements and estimate treatment effects under the missing-at-random assumption using maximum likelihood. The amount, timing, and reasons for missing primary outcome data will be summarized by group.
If post-baseline data for the primary outcome are missing, multiple imputation will be performed as a sensitivity analysis rather than as the primary analysis. The imputation model will include treatment group, time point, baseline value of the primary outcome, observed outcome values, and other clinically relevant variables or variables associated with missingness. At least 20 imputed datasets will be generated, and the number of imputations will be increased when appropriate according to the proportion of missing data. The same primary analysis model will then be fitted to each imputed dataset, and the estimates will be pooled using Rubin’s rules. The results will be compared with those from the primary analysis to assess the robustness of the findings.
This study will uniformly apply two-tailed tests, with the significance level set at α = 0.05. Statistical analysis results will report exact P-values, and effect sizes along with their 95% confidence intervals will be provided for the primary outcome.
Discussion
PD is a common neurodegenerative disorder whose pathological mechanisms are closely associated with the degeneration of substantia nigra dopaminergic neurons and abnormal aggregation of α-syn.1 The risk of developing PD increases with age, and as the global population ages, the disease burden of PD is expected to rise significantly.22 The clinical manifestations of PD can be categorized into motor and non-motor symptoms. As PD progresses, the occurrence of non-motor symptoms becomes almost inevitable, and these symptoms may emerge early in the disease course, sometimes even preceding motor symptoms.2,23 Pain is one of the common non-motor symptoms of PD, affecting 68% to 95% of PD patients.3 Moreover, PD patients with pain are more likely to experience other complications such as motor fluctuations, anxiety, and depression compared to those without pain.4 However, despite the high prevalence and significant impact of pain in PD, less than 38% of PD patients with pain receive effective analgesic treatment.5
Current clinical approaches for managing pain in PD primarily include pharmacotherapy, rehabilitation and physical therapy, and surgical interventions. The primary and foundational treatment is the optimization of dopaminergic therapy. For most pain in PD, the initial approach involves stabilizing plasma drug concentrations by adjusting levodopa dosage,24 adding dopamine agonists (such as rotigotine patch25 or pramipexole26), or adjunctive medications like catechol-O-methyltransferase (COMT) inhibitors and monoamine oxidase-B (MAO-B) inhibitors.27 However, long-term use may lead to complications such as dyskinesias.28 When dopaminergic agents prove insufficient or the nature of the pain is not dopaminergic, non-dopaminergic medications may be added. For example, potent analgesics like oxycodone/naloxone extended-release formulations are considered potentially useful for pain in PD.29 However, these agents are commonly associated with adverse effects such as drowsiness and sedation, dizziness and headache, and hallucinations.30 Additionally, anticonvulsants (eg., gabapentin, pregabalin) or antidepressants (eg., duloxetine) are also referenced in clinical practice,31 although evidence supporting their efficacy specifically for pain in PD remains limited. For patients with medication-refractory mid-to-late-stage PD, surgical intervention is a significant option. For instance, deep brain stimulation (DBS) may alleviate movement-related pain by improving motor function, or directly modulate abnormal central pain-processing networks to achieve analgesic effects.32 However, invasive procedures carry risks such as infection and hemorrhage, and are associated with high costs. Furthermore, non-pharmacological therapies, such as Tai Chi, Qigong, and yoga, not only improve motor symptoms but may also alleviate pain by enhancing proprioception and neuroplasticity. Nonetheless, the scientific evidence supporting their efficacy is relatively weak,33 and their effectiveness depends on patient compliance and specific conditions. Thus, current treatments for pain in PD exhibit multiple limitations across various dimensions.
Acupuncture, as a commonly used complementary and alternative therapy, has been shown to effectively reduce pain levels in patients, accompanied by improvements in motor symptoms and quality of life.34 Patients receiving 4-week acupuncture treatment demonstrated a significant reduction in both KPPS and VAS scores compared to baseline and the control group.35 Regarding its analgesic mechanisms, acupuncture is believed to enhance or modulate functional connectivity between key brain regions involved in pain perception, such as the primary somatosensory cortex (S1), prefrontal cortex, and insula. These regions are associated with the cognitive evaluation of pain, emotional processing of pain, and inhibition of excessive sensitization to pain signals in the brain.8 At the level of neuromodulation and anti-inflammatory pathways, acupuncture may activate the vagus nerve-mediated cholinergic anti-inflammatory pathway or selectively drive the vagal-adrenal axis, achieving targeted analgesia while suppressing neuroinflammation.36 In summary, acupuncture exerts its analgesic effects through multiple dimensions. However, due to the varying quality of reported efficacy in studies on acupuncture for pain in PD, the level of evidence supporting its routine recommendation remains to be further strengthened.
This study intends to conduct a single-center, double-blind, block-randomized, parallel-controlled clinical trial to investigate the therapeutic effect of acupuncture on patients with pain in PD by comparing the efficacy between the acupuncture group and the sham acupuncture group. Concurrently, serum levels of TNF-α, S100B, and GFAP will be assessed using ELISA to explore whether acupuncture exerts its clinical effect by ameliorating neuroinflammation and repairing the damaged BBB. Compared to previous studies, this research employs acupuncture as the intervention, which offers not only favorable efficacy but also cost-effectiveness and a high safety profile. As a complementary and alternative therapy, it can potentially reduce the long-term complications and adverse effects associated with pharmacological treatments. Furthermore, by utilizing sham acupuncture as a control measure and implementing blinding for both investigators and participants, this study addresses the current lack of high-level clinical evidence in the field of pain in PD. Finally, the inclusion of laboratory assessments—specifically testing serum TNF-α, S100B, and GFAP levels—aims to further elucidate the mechanisms underlying acupuncture treatment for pain in PD, thereby providing an objective basis for its clinical promotion.
Regarding the selection of acupoints, the core points chosen are the Four Divine Needles on the head, along with GV24 and GV29, aiming to regulate the central nervous system, improve cerebral blood circulation, and enhance the brain’s inhibition of pain.37 Complementary points include HT7 and SP6 on the extremities to stimulate brain regions associated with cognition and emotion.38 Additionally, GV25 is added to provide strong physical stimulation, activating the brainstem reticular formation.39 This protocol combines head and limb points to intervene across sensory, cognitive, and affective dimensions, embodying the therapeutic principle of addressing both the body and mind.
In recent years, the number of clinical studies on acupuncture has increased significantly. However, the improvement of research quality demands the adoption of more rigorous control designs to effectively distinguish the specific therapeutic effects of acupuncture from placebo effects. To optimize the implementation of blinding, this study employs a novel self-developed sham acupuncture device.40 This device utilizes a specially designed blunt-tip needle and a sealed adhesive base to create a genuine needle sensation for the participant without puncturing the skin, while simultaneously simulating the authentic tactile feedback of “resistance followed by a sudden give” for the practitioner. The genuine and sham devices are identical in appearance and handle length, with only subtle differences in the needle body. Both devices support angle adjustment, achieving effective blinding for both participants and investigators. This device has been applied and validated in multiple prior clinical trials conducted by our research team, leading to the generation of significant research findings.41–45
Simultaneously, activated astrocytes (GFAP-positive) can themselves produce more TNF-α,46,47 creating a self-amplifying positive feedback loop that exacerbates neuroinflammation and neuronal damage. The BBB is a critical structure for normal cerebrovascular formation, providing a unique extracellular neuronal environment for its proper function. When the BBB is compromised, the concentration of S100B protein in peripheral blood increases. S100B, primarily located in the central nervous system, serves as a serological marker reflecting BBB integrity. Its level is extremely low in the peripheral blood of healthy adults and becomes elevated only when BBB permeability is increased.18 Under the pathological conditions of PD, peripheral inflammatory signals may enter the central nervous system through a more permeable BBB, thereby aggravating neuroinflammation.19 This process involves enhanced reactivity of microglia and astrocytes, which subsequently secrete excessive amounts of pro-inflammatory factors and chemokines, ultimately contributing to neurodegeneration.20 By monitoring changes in these three markers, this study may help elucidate whether acupuncture exerts its clinical effects by mitigating neuroinflammation and repairing the damaged BBB.
Taken together, this study has several innovative features. Most previous studies, including protocols from our group, have focused on other non-motor symptoms of PD, such as cognitive impairment and anxiety, while high-quality acupuncture trials specifically addressing pain in PD remain scarce. To fill this gap, the present study introduces several methodological features. The KPPS is used as the primary outcome, with the PD-Q included to further assess neuropathic pain components. SSEPs are incorporated as an objective neurophysiological measure of somatosensory processing and pain sensitivity, complementing patient-reported outcomes. In addition, serum TNF-α, S100B, and GFAP are measured to explore mechanisms related to neuroinflammation, glial activation, and BBB dysfunction, which have been insufficiently examined in previous acupuncture studies on pain in PD. The UPDRS, HAMD, and PDQ-39 are also included to evaluate disease severity, emotional status, and quality of life. Collectively, these design features allow a more comprehensive assessment of acupuncture for pain in PD and extend our research program on PD-related non-motor symptoms from cognition and anxiety to pain.
Although this study was designed to address the limitations of previous research, several constraints remain. Firstly, all participants were recruited from a single center and were limited to Chinese patients. Consequently, the generalizability of the findings requires further validation through future multicenter and cross-cultural studies. Secondly, although sham acupuncture was employed as a control to enhance the rigor of blinding, the subtle somatosensory stimulation involved in the sham procedure may still elicit physiological effects.
In summary, this study will further broaden the clinical approach to managing pain in PD and provide reliable evidence-based medical data. The aim is to better alleviate symptoms in patients with pain in PD, delay disease progression, and enhance their quality of life.
Abbreviations
PD, Parkinson’s disease; α-syn, alpha-synuclein; VAS, Visual Analog Scale; KPPS, King’s Parkinson’s Disease Pain Scale; CRF, Case Report Form; PD-Q, painDETECT Questionnaire; UPDRS, Unified Parkinson’s Disease Rating Scale; PDQ-39, 39-item Parkinson’s Disease Questionnaire; HAMD, Hamilton Depression Rating Scale; SSEPs, Somatosensory Evoked Potentials; TNF-α, Tumor Necrosis Factor-alpha; S100B, S100 calcium-binding protein B; GFAP, Glial Fibrillary Acidic Protein; BBB, blood-brain barrier; ELISA, Enzyme-Linked Immunosorbent Assay; APS, Acupuncture Perception (Credibility) Scale; CONSORT, Consolidated Standards of Reporting Trials; ITT, Intention-To-Treat; FAS, Full Analysis Set; S1, primary somatosensory cortex; COMT, catechol-O-methyltransferase; MAO-B, monoamine oxidase-B; DBS, deep brain stimulation; IASP, International Association for the Study of Pain; PD-PCS, Parkinson’s Disease Pain Classification System; SPIRIT, Standard Protocol Items: Recommendations for Interventional Trials.
Data Sharing Statement
No datasets were generated or analysed during the current study.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First Affiliated Hospital of Guangzhou University of Chinese Medicine on December 19, 2025 (Ethics Reference No.: JY2025-166) and registered on February 9, 2026, in the International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/mgt/search) (Registration No.: ITMCTR2026000325). Written informed consent will be obtained from all participants prior to their enrollment in the study. In the event of substantial modifications to the protocol, an amended version will be submitted to the ethics committee for approval, and further research may only proceed upon such approval. For minor administrative revisions and/or clarifications that do not affect the conduct of the study, these changes will be documented in a memorandum after acknowledgment by the ethics committee. All substantive protocol amendments will be transparently disclosed in the trial reports.
Consent for Publication
Participants signed informed consent regarding publishing their photographs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by China Postdoctoral Science Foundation [grant numbers 447645] and the National Natural Science Foundation of China [grant numbers 82474622].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tanner CM, Ostrem JL. Parkinson’s Disease. New Engl J Med. 2024;391(5):442–17. doi:10.1056/NEJMra2401857
2. Siderowf A, Concha-Marambio L, Lafontant D, et al. Assessment of heterogeneity among participants in the Parkinson’s Progression Markers Initiative cohort using α-synuclein seed amplification: a cross-sectional study. Lancet Neurol. 2023;22(5):407–417. doi:10.1016/S1474-4422(23)00109-6
3. Buhmann C, Kassubek J, Jost WH. Management of Pain in Parkinson’s Disease. J Parkinsons Dis. 2020;10(s1):S37–S48. doi:10.3233/JPD-202069
4. Cattaneo C, Jost WH. Pain in Parkinson’s Disease: pathophysiology, Classification and Treatment. J Integr Neurosci. 2023;22(5):132. doi:10.31083/j.jin2205132
5. Janz C, Timpka J, Rosqvist K, Paul G, Storch A, Odin P. Non-Motor Symptom Management: insights into Adherence to Treatment Guidelines in Parkinson’s Disease Patients. J Parkinsons Dis. 2024;14(2):297–312. doi:10.3233/JPD-230263
6. Mylius VM, Ller JC, Bohlhalter S, Ciampi De Andrade D, Perez Lloret S. Diagnosis and Management of Pain in Parkinson’s Disease: a New Approach. Drugs Aging. 2021;38(7):559–577. doi:10.1007/s40266-021-00867-1
7. Qureshi AR, Jamal MK, Rahman E, et al. Non-pharmacological therapies for pain management in Parkinson’s disease: a systematic review. Acta Neurol Scand. 2021;144(2):115–131. doi:10.1111/ane.13435
8. Yu S, Lin S, Tsai C, et al. Acupuncture Effect and Mechanism for Treating Pain in Patients With Parkinson’s Disease. Front Neurol. 2019;10:1114. doi:10.3389/fneur.2019.01114
9. Chinese Society Of Parkinson’S Disease And Movement Disorders CMAO. Professional Committee Of Parkinson’S Disease And Movement Disorders CNAC. Diagnostic criteria of Parkinson’s disease in China (2016 edition). Chin J Neurol. 2016;49(04):268–271.
10. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
11. Keikomukaeda. Regulating Spirit Acupuncture Technique on the Treatment of Pain in Parkinson’s Disease: A Randomized Controlled clinical Trial. Guangzhou University of Chinese Medicine; 2022.
12. Yang Z, Zhixiu L, Xiaoyun Z. Therapeutic effect of low-frequency repetitive transcranial magnetic stimulation on Parkinson’s disease associated with pain. Chin J Contemp Neurol Neurosurg. 2019;19(06):429–436.
13. Lixing Z. Atlas of Jin’s Three-Needle Acupoint Groups. Beijing: China Medical Science Press; 2021.
14. State Administration for Market Regulation, Standardization Administration of China. Nomenclature and Location of Meridian Points|gb/T 12346-2021. Vol. 2026; 2021.
15. Jiang W, Chen W, Coeytaux R, et al. Acupuncture credibility scale scores associated with TCM acupuncture versus a sham acupuncture procedure:implication for clinical trial design. J Integr Med. 2014;03(v.12):184–185.
16. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Controlled Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
17. Cardinale A, Calabrese V, Iure AD, Picconi B. Alpha-Synuclein as a Prominent Actor in the Inflammatory Synaptopathy of Parkinson’s Disease. MDPI AG. 2021;12:6517.
18. Murcko R, Marchi N, Bailey D, Janigro D. Diagnostic biomarker kinetics: how brain-derived biomarkers distribute through the human body, and how this affects their diagnostic significance: the case of S100B. Fluids Barriers CNS. 2022;19(1):32. doi:10.1186/s12987-022-00329-9
19. Iovino L, Tremblay ME, Civiero L. Glutamate-Induced Excitotoxicity in Parkinson’s disease: the Role of Glial Cells. J Pharmacol Sci. 2020;144(3):151–164. doi:10.1016/j.jphs.2020.07.011
20. Parente A, Borzacchiello L, Giaccio M, et al. Progressive activation of the astrocyte A1 phenotype underlies microglia-astroglia crosstalk and contributes to neuroinflammation in neuronopathic MPS. Mol Genet Metab. 2025;146(1–2):109224. doi:10.1016/j.ymgme.2025.109224
21. Hopewell S, Chan A, Collins GS, et al. CONSORT 2025 statement: updated guideline for reporting randomised trials. BMJ. 2025;389:e81123.
22. Su D, Cui Y, He C, et al. Projections for prevalence of Parkinson’s disease and its driving factors in 195 countries and territories to 2050: modelling study of Global Burden of Disease Study 2021. BMJ. 2025;388:e80952. doi:10.1136/bmj-2024-080952
23. Simuni T, Chahine LM, Poston K, et al. A biological definition of neuronal α-synuclein disease: towards an integrated staging system for research. Lancet Neurol. 2024;23(2):178–190. doi:10.1016/S1474-4422(23)00405-2
24. Koeglsperger T, Berberovic E, Dresel C, et al. Real-world experience with continuous subcutaneous foslevodopa/foscarbidopa infusion: insights and recommendations. J Neural Transm. 2026;133(2):347–359. doi:10.1007/s00702-025-02911-5
25. Lau YH, Leta V, Rukavina K, et al. Tolerability of overnight rotigotine transdermal patch combined with intrajejunal levodopa infusion at 1 year: a 24-h treatment option in Parkinson’s disease. J Neural Transm. 2022;129(7):889–894. doi:10.1007/s00702-022-02506-4
26. Li T, Zou S, Zhang Z, Liu M, Liang Z. Efficacy of pramipexole on quality of life in patients with Parkinson’s disease: a systematic review and meta-analysis. BMC Neurol. 2022;22(1):320. doi:10.1186/s12883-022-02830-y
27. Andrenelli E, Baldini N, Barbini FA, et al. Add-on therapies to levodopa improve pain modulation in Parkinson’s disease with motor fluctuations: a prospective cohort study. Parkinsonism Relat Disord. 2025;140:108019. doi:10.1016/j.parkreldis.2025.108019
28. Kwon DK, Kwatra M, Wang J, Ko HS. Levodopa-Induced Dyskinesia in Parkinson’s Disease: pathogenesis and Emerging Treatment Strategies. Cells. 2022;11(23):3736. doi:10.3390/cells11233736
29. Guerriero F, Roberto A, Greco MT, Sgarlata C, Rollone M, Corli O. Long-term efficacy and safety of oxycodone-naloxone prolonged release in geriatric patients with moderate-to-severe chronic noncancer pain: a 52-week open-label extension phase study. Drug Des Devel Ther. 2016;10:1515–1523. doi:10.2147/DDDT.S106025
30. Thakur D, Dickerson S, Kumar Bhutani M, Junor R. Impact of prolonged-release oxycodone/naloxone on outcomes affecting patients’ daily functioning in comparison with extended-release tapentadol: a systematic review. Clin Ther. 2015;37(1):212–224. doi:10.1016/j.clinthera.2014.12.001
31. Gilron I, Baron R, Jensen T. Neuropathic pain: principles of diagnosis and treatment. Mayo Clin Proc. 2015;90(4):532–545. doi:10.1016/j.mayocp.2015.01.018
32. Mostofi A, Morgante F, Edwards MJ, Brown P, Pereira EAC. Pain in Parkinson’s disease and the role of the subthalamic nucleus. Brain. 2021;144(5):1342–1350. doi:10.1093/brain/awab001
33. Deuel LM, Seeberger LC. Complementary Therapies in Parkinson Disease: a Review of Acupuncture, Tai Chi, Qi Gong, Yoga, and Cannabis. Neurotherapeutics. 2020;17(4):1434–1455. doi:10.1007/s13311-020-00900-y
34. Yu P, Wang G, Tan S, et al. Efficacy of various acupuncture modalities on alleviating symptoms in Parkinson’s disease: a systematic review and meta-analysis of randomized controlled trials. Neurol Sci. 2025;46(10):4819–4835. doi:10.1007/s10072-025-08333-1
35. Shaosong W, Jingqing S, Qingyin F, et al. Effectivenss of electroacupuncture for skeletal muscle pain in Parkinson’s disease: a Clinical randomized controlled trial. J Tradit Chin Med. 2024;44(2):388–395. doi:10.19852/j.cnki.jtcm.20240203.004
36. Park J, Oh J, Park H. Potential role of acupuncture in the treatment of Parkinson’s disease: a narrative review. Integr Med Res. 2023;12(2):100954. doi:10.1016/j.imr.2023.100954
37. Birch S, Robinson N. Acupuncture as a post-stroke treatment option: a narrative review of clinical guideline recommendations. Phytomedicine. 2022;104:154297. doi:10.1016/j.phymed.2022.154297
38. Lu G, Chen F, Guo C, Wu J. Acupuncture for senile insomnia: a systematic review of acupuncture point. Arch Gerontol Geriatr. 2024;127:105586. doi:10.1016/j.archger.2024.105586
39. Han J, Yang Y, Wang Y, et al. Effectiveness and safety of Governor vessel acupuncture therapy for post-stroke cognitive impairment: a meta-analysis of randomized controlled trials. Ageing Res Rev. 2024;99:102355. doi:10.1016/j.arr.2024.102355
40. Wang Y, Liu X, Xu Z, Zhuang L. An auxiliary device for double-blind placebo acupuncture research. Chin Acupunct Moxibus. 2022;42(3):351–354.
41. Li Y, Leong I, Fan J, et al. Efficacy of acupuncture for the treatment of Parkinson’s disease-related constipation (PDC): a randomized controlled trial. Front Neurosci. 2023;17:1126080. doi:10.3389/fnins.2023.1126080
42. Liu X, Li M, Xie X, et al. Efficacy of manual acupuncture vs. placebo acupuncture for generalized anxiety disorder (GAD) in perimenopausal women: a randomized, single-blinded controlled trial. Front Psychiatry. 2023;14:1240489. doi:10.3389/fpsyt.2023.1240489
43. Fan J, Xu Z, Chen Y, et al. Efficacy of Acupuncture for Parkinson’s Disease Anxiety: two-Stage Protocol for a Randomized Controlled Clinical Trial. eCAM. 2022;2022:5180193. doi:10.1155/2022/5180193
44. Li M, Wang Y, Li K, Xu X, Zhuang L. The efficacy and safety of Jin’s three-needle therapy vs. placebo acupuncture on anxiety symptoms in patients with post-stroke anxiety: a study protocol for a randomized controlled trial. Front Psychiatry. 2022;13:941566. doi:10.3389/fpsyt.2022.941566
45. Wu S, Leong II, Fan J, et al. Efficacy of acupuncture for Parkinson’s disease with mild cognitive impairment: study protocol for a randomized controlled trial. Front Neurol. 2025;16:1674098. doi:10.3389/fneur.2025.1674098
46. Wang T, Sun Y, Dettmer U. Astrocytes in Parkinson’s Disease: from Role to Possible Intervention. Cells. 2023;12(19):2336. doi:10.3390/cells12192336
47. Yuan W, Huang W, Jiang Y, et al. The function of astrocytes and their role in neurological diseases. Eur J Neurosci. 2023;58(9):3932–3961. doi:10.1111/ejn.16160
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Wang H, Zhang J, Ma D, Zhao Z
International Journal of General Medicine 2023, 16:4039-4050
Published Date: 6 September 2023
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
The Effect of Gua Sha Therapy on Pain in Parkinson’s Disease: a Randomized Controlled Trial
Xu YC, Wang QQ, Chen MY, Gao YJ, Wang JY, Ge HT, Weng H, Chen JP, Xu GH
International Journal of General Medicine 2024, 17:2791-2800
Published Date: 14 June 2024
Effect of Acupuncture for Diminished Ovarian Reserve: A Randomized Sham-Controlled Trial
Wang X, Du P, Yang L, Li J, Hang T, Qi L, Su C, Liu X, Li W, Zhu Y, Lu G, Xu H, Fang Y
International Journal of Women's Health 2026, 18:580821
Published Date: 8 April 2026