Back to Journals » Journal of Pain Research » Volume 16
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Authors Hu H ![]() , Lin X, Fang L, Li Y, Gao H
, Lin X, Fang L, Li Y, Gao H
Received 29 July 2023
Accepted for publication 21 September 2023
Published 4 October 2023 Volume 2023:16 Pages 3367—3378
DOI https://doi.org/10.2147/JPR.S433048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Hantong Hu,1,2,* Xiaoqi Lin,3,* Lianqiang Fang,1 Yang Li,1 Hong Gao1
1Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China; 2Department of Neurobiology and Acupuncture Research, Zhejiang Chinese Medical University, Key Laboratory of Acupuncture and Neurology of Zhejiang Province, Hangzhou City, People’s Republic of China; 3The Third Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Gao, Department of Acupuncture and Moxibustion, the Third Affiliated Hospital of Zhejiang Chinese Medical University, No. 219 Moganshan Road, Hangzhou City, People’s Republic of China, Email [email protected]
Objective: This study aims to evaluate the efficacy and safety of acupuncture for chronic subjective tinnitus and explore the central mechanism underlying acupuncture for chronic subjective tinnitus using functional near-infrared spectroscopy (fNIRS).
Methods: We will randomly assign 60 tinnitus patients to either an acupuncture group or a waiting-list control group. The acupuncture group will undergo 12 treatment sessions over 4 weeks, whereas the waiting-list control group will receive no intervention concurrently. Clinical outcome measures include the Tinnitus Handicap Inventory (THI) score, tinnitus loudness assessed by 11-point NRS, average pure-tone threshold, and Hamilton Anxiety Scale (HAM-A) score. Neuroimaging outcomes assessed by fNIRS included blood oxygen concentration and resting-state functional connectivity (RSFC). All outcome measurements will be assessed at the baseline, after 4-week treatment, and at 3-month follow-ups.
Results: Our investigation will determine if significant differences exist between the two groups regarding THI, NRS, average pure-tone threshold, and HAM-A scores. Moreover, the analysis will reveal whether the acupuncture group demonstrates significant change in blood oxygen concentration and RSFC between specific brain regions compared to the waiting-list control group.
Conclusion: With the novel technique of fNIRS, in addition to efficacy evaluation of acupuncture, this study’s findings are anticipated to partly elucidate the neural mechanisms underlying acupuncture treatment for subjective tinnitus and offer an objective assessment method for its therapeutic impact, thereby contributing to filling the research gap.
Trial Registration: Clinicaltrials registry (identification code NCT05829278).
Keywords: acupuncture, functional near-infrared spectroscopy, randomized controlled trial, subjective tinnitus, neural mechanisms
Introduction
Tinnitus is the auditory perception of noise in the absence of an external source, occurring either bilaterally or unilaterally. Almost everyone experiences tinnitus at least once in their lifetime, and while it usually disappears within seconds or minutes, a significant portion of the population suffers from persistent tinnitus that negatively impacts their lives. The prevalence of tinnitus is increased with age and is expected to rise in the future due to growing noise exposure.1,2 Regarding the prevalence of tinnitus in different age groups, for 40–50 year olds, the prevalence ranged from 11.2% to 25.0% across different epidemiological surveys; for 50–60 year olds, it ranged from 9.5% to 29.8%; for 60–70 year olds, it ranged from 13.3% to 33.5%; and for 70–80 year olds, the prevalence ranged from 15.0% to 31.7%.2
Subjective tinnitus accounts for most distressing tinnitus.3 Subjective tinnitus is defined as the auditory perception of sound in the absence of any external audio source, a phenomenon exclusively perceived by the affected individual. Unlike objective tinnitus, which has a vascular or myoclonus origin, the exact mechanisms of subjective tinnitus remain inconclusive.1 However, previous studies have made some progress in elucidating some possible causes and mechanisms of subjective tinnitus. Regarding the causes, it can be caused by a variety of factors, including exposure to loud noises, age-related hearing loss, earwax blockages, certain medications, and underlying medical conditions like sudden sensorineural hearing loss and Meniere’s disease. Regarding potential disease mechanisms, it is commonly recognized that neural plasticity at different relays along the auditory pathway plays an important role in the mechanisms of subjective tinnitus.4,5 In addition, animal studies have identified increased excitation in the cochlear nucleus, inferior colliculus, and auditory cortex, as well as heightened synchrony of neuronal firing involved in tinnitus generation.6 Furthermore, recent studies reveal a more complex pathology that includes various non-auditory brain areas and networks.7 It is suggested that activation of the auditory cortex in the resting-state is associated with tinnitus loudness, while co-activation of non-auditory cortex is key to other tinnitus-associated manifestations (eg, irritability, distress).8 Unfortunately, the complex neural pathology of tinnitus has posed significant difficulties in its treatment. Currently available remedies such as hearing aids, sound therapy, and cognitive behavioral therapy are beneficial for a portion of patients, but these approaches are often limited by clinical scenarios and the heterogeneity of tinnitus sufferers.1 As a result, an increasing number of tinnitus patients are seeking help from complementary and alternative medicine.9,10
Acupuncture, a complementary therapy with easy application and few side effects, has been adopted for treating tinnitus for a long period, especially in China. A growing number of clinical trials have found that acupuncture can significantly improve tinnitus symptoms, including studies published in recent years.11–13 Moreover, although the evidence level is inadequate for establishing a firm conclusion, several systematic reviews and meta-analyses14–17 generally support acupuncture’s effectiveness and safety for treating tinnitus. However, the neural mechanisms underlying acupuncture’s treatment of subjective tinnitus remain unclear and require further in-depth investigations. Additionally, since subjective tinnitus is a subjective symptom self-reported by patients, to date, there have been no objective assessment tools to quantitatively evaluate the therapeutic effect of specific therapies on tinnitus improvement.
Faced with such research gaps, as a relatively novel neuroimaging technique, functional near-infrared spectroscopy (fNIRS) has the potential to provide valuable insights. fNIRS is a reliable and sensitive tool to monitor hemodynamic and neural activity in specific brain regions based on different absorption rates of near-infrared light at 600–900nm.18 Given its non-invasiveness, non-radioactivity, ease of use, minimal scanning noise, and high temporal resolution, fNIRS is more appropriate for examining the central effects of acupuncture on tinnitus compared to other neuroimaging techniques like functional magnetic resonance imaging (fMRI).19,20 Particularly, the negligible machine noise of fNIRS can minimize interference from external acoustic stimuli on auditory cortical activity, thereby improving result reliability in tinnitus research. In recent years, a growing number of trials using fNIRS have been conducted in tinnitus research.7,21–24 For example, two fNIRS-based trials have shown that tinnitus patients exhibit significantly stronger resting-state functional connectivity (RSFC) between temporal regions and frontal and occipital regions than healthy controls.7,21 These findings indicate that enhanced connectivity in both auditory and non-auditory regions measured by fNIRS contribute to the central neural pathology of tinnitus and highlight the potential of fNIRS as an objective measurement tool for tinnitus.25 More recently, an up-to-date study26 published in April 2023 utilized fNIRS to evaluate the central mechanisms of acupuncture for treating subjective tinnitus, and the results revealed that acupuncture could increase oxygenated hemoglobin (HbO2) concentration in the temporal lobes and influence auditory cortex activation, suggesting the feasibility of fNIRS for investigating the central mechanism of acupuncture for tinnitus. However, this previous study was a pilot trial that had limitations such as a small sample size and a lack of randomized controlled design. Moreover, this fNIRS-based study26 also focused exclusively on HbO2 concentration and lacked measurements of other important fNIRS-related outcomes such as RSFC.
Considering the promising potential of fNIRS in tinnitus research, as well as the limitations of previous study,26 we designed this randomized controlled trial (RCT) to explore the therapeutic effect and central mechanism using fNIRS. The objectives of this trial are to 1) evaluate the efficacy and safety of acupuncture for chronic subjective tinnitus, and 2) explore the central mechanism underlying acupuncture for chronic subjective tinnitus. By utilizing fNIRS, the findings of this study are anticipated to promote further understanding of acupuncture’s efficacy and central mechanisms in treating chronic subjective tinnitus, offering valuable information for both researchers and clinicians in the field.
Methods
Study Design
This study is designed as a randomized, waiting-list controlled, assessor-blinded trial. Qualified participants will be allocated to either the acupuncture group or the waitlist control group at a 1:1 ratio. This protocol’s reporting adheres to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guideline.27 The overall schedule of the trial is presented in Table 1, and a flow diagram of the study is shown in Figure 1.
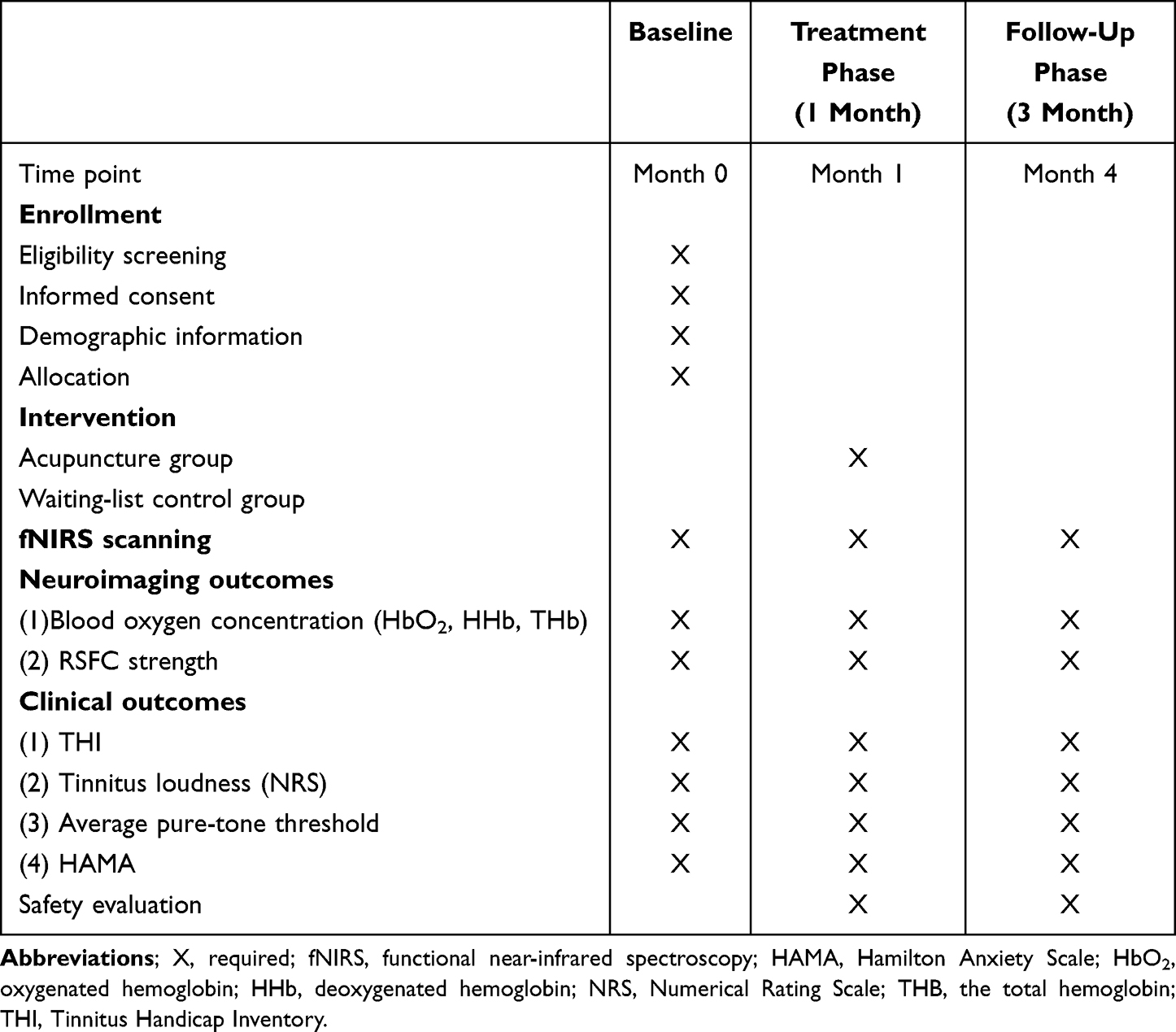 |
Table 1 Schedule of Enrolment, Interventions and Outcome Assessments |
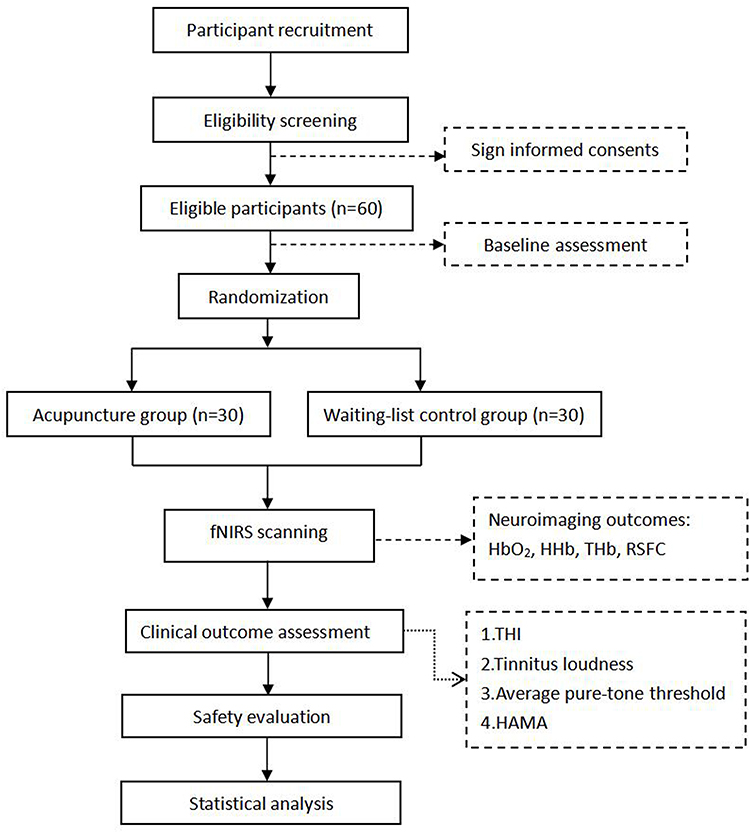 |
Figure 1 Flow chart of the study process. |
Participant Recruitment
Potentially eligible participants with tinnitus will be recruited from the Otolaryngology Department of the Third Affiliated Hospital of Zhejiang Chinese Medical University. Each participant will receive a comprehensive explanation of the protocol before signing their informed consent.
Diagnosis Criteria
With references to international guidelines,28,29 the diagnostic criteria for subjective tinnitus are defined as follows. Moreover, tinnitus is termed “chronic” when the duration ≥6 months based on the multidisciplinary European Guideline for tinnitus.29
- Subjective tinnitus is only perceptible to the patient and cannot be examined through auscultation by physicians, unlike objective tinnitus.
- The patient perceives ear noise in the absence of an external source, which may be constant or intermittent and have various sound qualities such as ringing, buzzing, clicking, or roaring.
- The ears show no abnormalities upon otoscopic examination, including the ear canal and eardrum.
- The tinnitus impacts the patient’s quality of life in some way, and the level of annoyance varies among individuals.
Inclusion Criteria
- Participants have a definitive diagnosis of subjective tinnitus with a duration of ≥6 months.29,30
- Tinnitus is occurring bilaterally.
- Males and females, aged 18 to 60 years.
- Participants can cooperate with experimental procedures and sign written informed consent.
- Not participating in other clinical trials concurrently.
Exclusion Criteria
- Participants diagnosed with objective tinnitus.
- Participants with comorbid nervous system or neuropsychiatric disorders that potentially intervene the results of fNIRS, such as auditory neuroma, craniocerebral trauma, and cerebrovascular lesions.
- Participants with severe cardiovascular and cerebrovascular diseases, malignant liver and kidney diseases, or other critical diseases.
- Participants with any contraindications to acupuncture (eg, bleeding tendencies).
- Pregnant or lactating women.
- Participants who have undergone tinnitus treatment using pharmaceuticals or other therapies within the past four weeks.
Randomization and Allocation Concealment
Using a random block scheme stratified by sex and age with Statistical Product and Service Solutions Version 25.0 (SPSS Inc., Chicago, IL, USA) software, eligible participants will be assigned to either the acupuncture group or waiting-list control group at a 1:1 ratio. An independent administrator, who is uninvolved in other procedures of the study, will execute this process, and the random allocation list’s information will be kept strictly confidential. Subsequently, randomization results will be stored in opaque, sealed, sequentially numbered envelopes to maintain allocation concealment.
Blinding
Due to the specific nature of acupuncture operation and waiting-list control, the acupuncture practitioners and the patients will not be blinded in this study. Nonetheless, by employing specially designated person, outcome assessors will be blinded to the assignment of groups.
Intervention Procedures
Subjects in the acupuncture group will undergo 4-week acupuncture treatment, while subjects in the waiting-list control group will receive no treatment during the 4 weeks. The reporting of acupuncture intervention adheres to the revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA)31 as follows.
Acupuncture Group
Qualifications of Practitioners
Acupuncture practitioners in this study are licensed acupuncture doctors who have over 10 years of clinical experience in acupuncture. To ensure strict adherence to the standardized acupuncture protocol, all practitioners will receive specialized training on acupuncture procedures before the study.
Acupoint Selection
Drawing from traditional Chinese medicine (TCM) literature and clinical experience, acupoint prescriptions will be formulated in accordance with local and distal acupoint selection principles: Yifeng (TE17), Tinggong (SI19), Tinghui (GB2), Waiguan (TE5), Zhongzhu (TE3), Zusanli (ST36), and Taixi (KI3). As all enrolled participants experience bilateral tinnitus, the acupoints mentioned above will be needled on both sides. The locations of the above acupoints are summarized in Table 2.
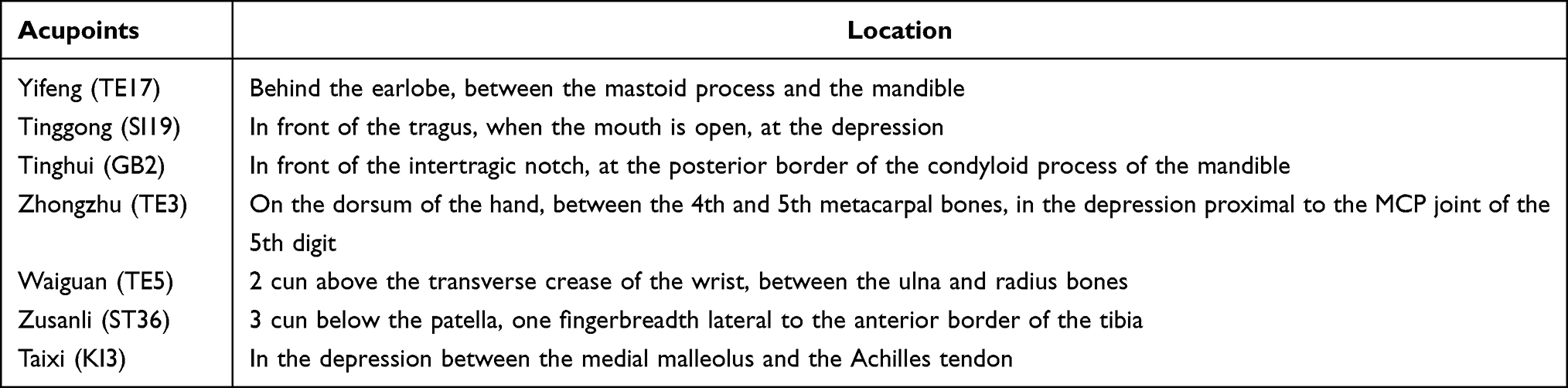 |
Table 2 Locations of the Selected Acupoints for Treating Subjective Tinnitus |
Acupuncture Procedures
Acupuncture procedure will be conducted using sterile and disposable acupuncture needles with 40 mm in length and 0.25 mm in diameter (Hwato Brand, Suzhou Medical Instrument, China). Participants will lie in a supine position, and following local skin sterilization, needles will be inserted into the acupoints. Local acupoints around the ear (ie, SI19, GB2, TE17) will be inserted vertically, and then the needles will be slowly rotated within a small range to an insertion depth of 20–25 mm, ensuring the transmission of deqi sensations (eg, distention, soreness, and numbness) to the ear canal. For distal acupoints (ie, TE5, TE3, ST36, KI3 (Taixi)), they will be inserted vertically, with lifting and thrusting or rotating manipulation to elicit deqi sensations. Subsequently, all needles will be retained in the acupoints for 30min.
Acupuncture Frequency and Treatment Course
Participants in the acupuncture group will undergo a treatment course comprising 12 treatment sessions, with acupuncture administered three times a week for four weeks.
Waiting-List Control Group
No intervention will be provided to the waiting-list control group during the 4-week observation period. Participants in this group will complete outcome measurements at corresponding time points.
Considering participant adherence and ethical implications, subjects in the waiting-list control group will be informed that they will be offered 12 acupuncture sessions free of charge at the end of the trial. The acupuncture treatment protocol will be identical to that administered to the acupuncture group.
Concomitant Care and Intervention
Throughout the study period, participants will be advised to refrain from receiving other tinnitus interventions that could influence the study results, including but not limited to behavioral therapy and medication. If a participant engages in other co-interventions for tinnitus, investigators should document relevant information for subsequent analysis. Nonetheless, for participants with comorbid conditions such as hypertension, diabetes, and other chronic diseases, they can continue their routine medications and therapies. Research staff will record the names of these comorbid conditions, medications, and therapies in the case report form.
fNIRS Scanning and Data Processing Rocedure
fNIRS Scanning
The device used in our experiment is the ETG-4000 (Hitachi Corporation, Japan), which is capable of detecting alterations in oxyhemoglobin (HbO), deoxyhemoglobin (HbR), and total hemoglobin (HbT) by employing two infrared light wavelengths (695 and 830 nm). Utilizing a source-detector distance of 3 cm, hemoglobin changes can be measured at a depth of 2–3 cm, corresponding to the cerebral cortex. A 52-multichannel fNIRS system will be employed for measurements. The system comprises 33 probes (17 emitters and 16 detectors) secured on the scalp in a 3×11 arrangement, conforming to the international 10–20 system32 (Figure 2). The establishment of measurement channels between each emitter-detector pair produces 52 channels in total. The prefrontal cortex and the superior temporal cortex will be covered by the fNIRS probe set (Figure 3). Once probes are stabilized, the signal strength of each channel will be checked. Channel signals can be affected by probe cleanliness and obstructions such as hair between the probe and scalp. Therefore, if a channel’s signal strength is found to be weak, measures such as cleaning the scalp, adjusting the probe, and moving hair aside will be taken promptly. Each subject will complete a 5-minute resting-state scan, during which they will be asked to remain quiet, avoid head movements, and close their eyes without falling asleep.
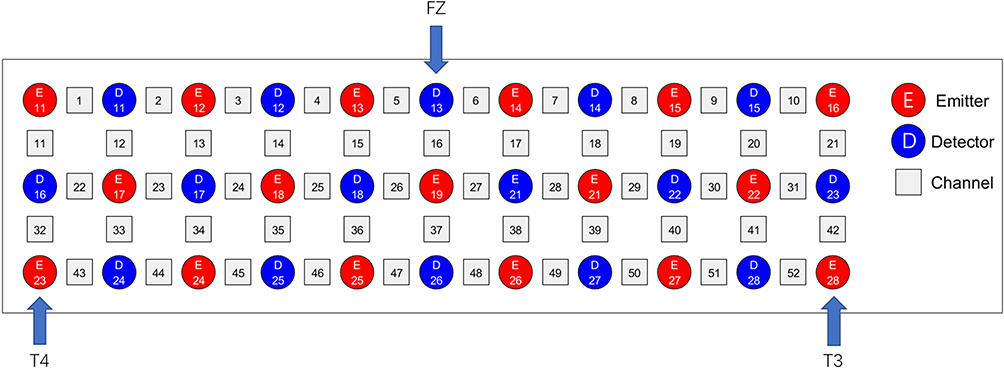 |
Figure 2 The channel map of functional near-infrared spectroscopy based on the international 10–20 system, with 17 light emitters (red squares), 16 detectors (blue squares) and 52 channels (numbers). |
 |
Figure 3 Brain schematic showing the configuration of channels with identified detectors (red circles) and emitters (blue circles) over the prefrontal cortex and the superior temporal cortex. The red shaded area represents the primary auditory cortex (A1), the green areas represent the ventromedial prefrontal cortex (vmPFC) and the dorsolateral prefrontal cortex (dlPFC). |
fNIRS Data Processing
Data from the ETG-4000 will be imported as a CSV file into the NIRS-KIT software, which is a MATLAB-based software providing an open-source tool for researchers to analyze fNIRS data in one suite.33 The fNIRS data will be pre-processed with detrending, motion correlation, and filtering to exclude interference from external factors. After pre-processing, these statistics will be eligible for the calculation of interregional RSFC strength.
Outcome Measures
Demographic and Clinical Outcomes
Demographic Information
At baseline, demographic information, such as name, age, educational level, weight, height, history of tinnitus, along with other concurrent diseases, will be collected. Vital signs, including the blood pressure, pulse, respiration rate, and temperature, will also be assessed.
Clinical Outcomes
Clinical outcome measures include Tinnitus Handicap Inventory (THI) score, Tinnitus Loudness, average pure-tone threshold, and Hamilton Anxiety Scale (HAM-A) score, which will be assessed at the baseline, after 4-week treatment, and at 3-month follow-ups.
THI Score
THI is a self-report inventory that is brief, easy to administer, and interpret, and has a broad scope.34 It contains 25 items, each valued at 0–4 points. A larger THI score indicates a more severe degree of tinnitus.
Tinnitus Loudness
Tinnitus loudness will be measured by using an 11-point Numerical Rating Scale (NRS),35 with 0 indicating no tinnitus, and 10 indicating maximum intolerable tinnitus.
Average Pure-Tone Threshold
Average pure-tone threshold will be assessed by pure-tone audiometry. Both air conduction thresholds and bone conduction thresholds at 250Hz, 500Hz, 1kHz, 2kHz, 4kHz, and 8kHz will be measured for each subject to determine average pure-tone threshold, which can reflect the hearing level of tinnitus patients.36
HAMA Score
The HAMA scale consists of 14 items, each rated on a 5-point scale from 0 to 4. It is a reliable indicator of the severity of anxiety symptoms and is classified as no anxiety (0–6 points), probable anxiety (7–13 points), definite anxiety (14–20 points), significant anxiety (21–28 points), or severe anxiety (above 29 points).37
fNIRS Imaging Outcomes
fNIRS will be scanned at the baseline, after 4-week treatment, and at 3-month follow-up.
Blood Oxygen Concentration
Blood oxygen concentration included the oxygenated hemoglobin (HbO2) concentration, deoxygenated hemoglobin (HHb) concentration, and the total hemoglobin (THb) concentration in each measurement channel.
Interregional RSFC Strength
Interregional RSFC strength can be used to quantify the relationship between channels or regions of interest (ROI) in the fNIRS time series, which is calculated by the Pearson correlation coefficient of the mean time-series between any pair of ROIs.32 With references to prior comparable studies,38 ROIs in this study include the dorsolateral prefrontal cortex (dlPFC), ventromedial prefrontal cortex (vmPFC), and primary auditory cortex. Interregional RSFC between ROIs and between ROI and channel will be calculated using NIRS-KIT software.
Statistical Analysis
SPSS Statistics version 26 (IBM corporation, Armonk, NY, 2019) will be utilized for statistical analysis, with a two-sided significance level set at 0.05. Baseline measurements and demographic information for each group will be listed. If numerical data conform to normality of distribution, they will be expressed as mean ± standard deviation; otherwise, they will be expressed as median and interquartile range. Categorical data (age, sex, etc.) and ranking data are expressed as frequencies and percentages. For between-group comparisons, the 2-independent sample t-test or Mann–Whitney U-test will be used for continuous variables according to their distribution. The χ2 test or Fisher’s exact test will be used for categorical variables. Within-group variations in outcome measures pre- and post-intervention will be assessed via paired t-tests or Wilcoxon signed-rank tests. To assess the association between specific changes in RSFC strength and the improvement of other clinical outcome data, the Pearson correlation analysis or Spearman rank correlation analysis will be conducted based on data type.
Sample Size Estimation
The sample size calculation will be based on the outcome measure of THI score and performed using PASS V.16.0 software (NCSS, Kaysville, Utah, USA). In a 1:1 ratio, eligible participants will be separated into either the acupuncture group or waiting-list control group. Based on our preliminary trial, we assume that the between-group difference of THI score is 27.6, with a combined standard deviation of 34.2. With the use of a two-sided test, α value of 0.05, and a statistical power of 80%, it is estimated that 25 participants will be required per group. Considering a 20% attrition rate, the sample size for each group will comprise 30 participants, yielding a total of 60 subjects for the trial.
Safety Assessment
Safety assessment will focus on the number of adverse events. Participants will be instructed to report any adverse events. Acupuncture-associated adverse events mainly include pain, bleeding, bruising, burns, blisters, infection and dizziness. For safety evaluations, all adverse events, irrespective of their relevance to acupuncture treatment, will be documented and assessed by investigators in detail on an adverse event form at every visit, including the time of occurrence, symptom duration, severity (mild, moderate, or severe39), management measures, resolution time, and causality classification (certain, probable or likely, possible, unlikely, unclassified, or unclassifiable).40
Ethical Approval and Study Registration
The Third Affiliated Hospital of Zhejiang Chinese Medical University’s Ethics Committee has granted ethical approval (No. ZSLL-KY-2022-042-01) for conducting this trial. Prior to enrollment, researchers will thoroughly explain the study’s objectives, research items, benefits, and potential risks to participants. Participants will retain full rights to decide on trial participation, and informed consent forms must be signed before study inclusion. Strict privacy protection will be maintained throughout the study, with all personal and disease information kept confidential. The study protocol has been registered in the Clinicaltrials registry under the identification code NCT05829278.
Data Collection and Management
After obtaining signed consent forms, data for all subjects will be collected. Participant privacy will be strictly protected throughout the trial. Investigators are responsible for maintaining subject anonymity. Participants will be assigned code numbers as identifiers, and their confidentiality will be safeguarded by the study identification number. Participants will be anonymized and their information and data will be recorded on case report forms. All paper-based data will be verified and entered into an electronic database which is password-protected. Two data entry personnel will enter all data into an electronic database using double data entry to ensure data accuracy. Data confidentiality will be ensured, with access limited to authorized research personnel. Participant study information will not be disclosed outside the study without written permission from the participant.
Study Monitoring and Quality Control
To ensure the study’s quality, preliminary training will be conducted before subject recruitment to guarantee that all investigators and related staff adhere to the study protocol. Concurrently, all outcome assessors will undergo standardized training to uniformly conduct outcome assessments and complete case report forms. Investigators will ensure that all collected data are accurate, complete, and verifiable from source documents. Quarterly monitoring meetings will be organized by the investigators to discuss and resolve issues arising during the trial.
Discussion
To date, the neural mechanisms of acupuncture for treating subjective tinnitus remain inconclusive. Nonetheless, with the aid of advanced neuroimaging techniques such as fMRI and fNIRS, an increasing number of neuroimaging studies have been conducted in recent years to explore the central mechanism underlying the efficacy of acupuncture in treating subjective tinnitus. For example, one fMRI-based study demonstrated that acupuncture treatment in chronic tinnitus patients leads to a significant decrease in dynamic functional connectivity between specific brain regions, positively correlating with tinnitus improvement.41 Another study utilizing fMRI revealed that acupuncture stimulation can effectively relieve the severity of tinnitus by decreasing functional connectivity of amygdala in subjective tinnitus patients. Most recently, a trial based on fNIRS,26 similar to our study, revealed that acupuncture could increase HbO2 concentration in the temporal lobes of tinnitus patients and influence activation of the auditory cortex (Yu et al, 2023). Consequently, the modulation of specific cerebral cortices is likely the target of acupuncture’s action and neural mechanisms for tinnitus treatment, which can be assessed by neuroimaging techniques. With its noise-free and robust anti-interference capabilities, fNIRS is superior to other neuroimaging techniques in investigating tinnitus’ central mechanisms, so we select fNIRS for verifying the research hypothesis in this study. Specifically, we hypothesize that acupuncture treatment will result in significant subjective tinnitus symptom improvements and corresponding observable neural activity changes, as measured by fNIRS. We also hypothesize that fNIRS will unveil alterations in RSFC within particular brain regions, offering insights into the central mechanisms underpinning acupuncture’s tinnitus treatment. Regarding the selection of brain regions in our study, since prior studies have identified that, in addition to the primary auditory cortex, non-auditory brain regions such as the frontal cortex contribute to the development of tinnitus,7,38 hence, our study’s regions of interest (ROIs) for fNIRS measurement consist of the dorsolateral prefrontal cortex (dlPFC), ventromedial prefrontal cortex (vmPFC), and primary auditory cortex.
It is worth noting that our study’s strength lies in its novelty. To our knowledge, only one similar study exists by utilizing fNIRS to examine the neural mechanisms of acupuncture for treating tinnitus,26 which was recently published in April 2023. However, as a pilot trial, the previous study26 only included 18 tinnitus patients and lacked a randomized controlled design. Furthermore, it exclusively focused on HbO2 concentration as the fNIRS-related outcome.26 To overcome these previous limitations, our study is designed as a randomized, assessor-blinded, waiting-list controlled trial. And we plan to analyze more fNIRS-related outcomes, including HbO2, HHb, THb, and RSFC. To note, the RSFC is an important neuroimaging outcome that can measure the temporal correlations between different regions of the brain while a subject is at rest or not performing any specific task. The RSFC is based on the concept that functionally related brain regions exhibit a synchronized low-frequency spontaneous fluctuation of blood oxygen level-dependent (BOLD) signals.42 The use of RSFC has gained popularity in cognitive neuroscience for exploring functional brain networks, investigating changes in functional connectivity associated with neuropsychiatric disorders, and exploring the relationship between brain connectivity and behavior.43 Numerous studies have demonstrated the reliability and sensitivity of RSFC as a functional connectivity measure in the brain.42,44 Thus, RSFC will be one of the key neuroimaging outcome measurements in our study. Owing to the novel technique of fNRIS in tinnitus and acupuncture research, the findings of our study are anticipated to partially elucidate the neural mechanisms underlying acupuncture treatment for tinnitus and offer an objective evaluation method for assessing acupuncture’s therapeutic impact on tinnitus.
Nevertheless, this study has limitations. First, the relatively small sample size in our study may affect result reliability. Second, no restrictions are placed on participants’ hearing levels or tinnitus severity. Future research should consider recruiting participants with similar hearing levels and tinnitus degrees. Third, owing to technical restrictions, fNIRS only measures hemodynamic and neural activity in the superficial regions of the outer cortex, and it is unable to capture activity in the brain’s deeper layers.
Conclusions
The results of this study are expected to enhance our understanding of the efficacy and central mechanisms of acupuncture in treating chronic subjective tinnitus, providing useful insights for both researchers and clinicians in this field.
Ethics Approval and Consent to Participate
This clinical trial will adhere to the Declaration of Helsinki guidelines during its implementation and ethics approval (grant number: ZSLL-KY-2022-042-01) has been obtained from the Institutional Ethical Review Board of the Third Affiliated Hospital of Zhejiang Chinese Medical University. Prior to participation, all subjects in the study are required to provide informed consent.
Acknowledgments
Hantong Hu and Xiaoqi Lin are co-first authors for this study. The authors appreciate the support from all participants who have been or will be included in this study.
Funding
This study is funded by the Zhejiang Province Public Welfare Technology Application Research (LTGY23H270003); Zhejiang Provincial Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (GZS2021027); Zhejiang Natural Science Foundation Exploration Project Q (LQ20H270012); and Zhejiang Traditional Chinese Medicine Technology Plan (2020ZB124, 2021ZX010).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013;382(9904):1600–1607. doi:10.1016/S0140-6736(13)60142-7
2. McCormack A, Edmondson-Jones M, Somerset S, et al. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. 2016;337:70–79. doi:10.1016/j.heares.2016.05.009
3. Kang D-W, Kim -S-S, Park D-C, Kim S-H, Yeo S-G. Objective and measurable biomarkers in chronic subjective tinnitus. Int J Mol Sci. 2021;22(12):6619. doi:10.3390/ijms22126619
4. Wang K, Tang D, Ma J, Sun S. Auditory neural plasticity in tinnitus mechanisms and management. Neural Plasticity. 2020;2020:7438461.
5. Shore SE, Roberts LE, Langguth B. Maladaptive plasticity in tinnitus--triggers, mechanisms and treatment. Nat Rev Neurol. 2016;12(3):150–160. doi:10.1038/nrneurol.2016.12
6. Noreña AJ, Eggermont JJ. Changes in spontaneous neural activity immediately after an acoustic trauma: implications for neural correlates of tinnitus. Hear Res. 2003;183(1–2):137–153. doi:10.1016/S0378-5955(03)00225-9
7. San Juan J, Hu X-S, Issa M, et al. Tinnitus alters resting state functional connectivity (RSFC) in human auditory and non-auditory brain regions as measured by functional near-infrared spectroscopy (fNIRS). PLoS One. 2017;12(6):e0179150. doi:10.1371/journal.pone.0179150
8. De Ridder D, Elgoyhen AB, Romo R, Langguth B. Phantom percepts: tinnitus and pain as persisting aversive memory networks. Proc Natl Acad Sci USA. 2011;108(20):8075–8080. doi:10.1073/pnas.1018466108
9. Luetzenberg FS, Babu S, Seidman MD. Alternative treatments of tinnitus. Otolaryngol Clin North Am. 2020;53(4):637–650. doi:10.1016/j.otc.2020.03.011
10. Ismail AMA, Ali SM, Ghuiba K, et al. Autonomic functions, tinnitus annoyance and loudness, and quality of life: randomized-controlled responses to bee-humming (vibrational) respiratory training in tinnitus elderly. Complement Ther Clin Pract. 2022;48:101611. doi:10.1016/j.ctcp.2022.101611
11. Kuzucu I, Karaca O. Acupuncture treatment in patients with chronic subjective tinnitus: a prospective, randomized study. Med Acupunct. 2020;32(1):24–28. doi:10.1089/acu.2019.1367
12. Ismail AMA, Aly ME, Elfahl AA. Effect of acupuncture on tinnitus severity index in the elderly with non-pulsating tinnitus. Physioth Quart. 2022;30:57–60. doi:10.5114/pq.2021.108662
13. Ali Ismail AM. Lipid profile response to acupuncture in obese patients with subjective tinnitus: a randomized controlled trial. J Acupunct Meridian Stud. 2023;16:11–19. doi:10.51507/j.jams.2023.16.1.11
14. Liu F, Han X, Li Y, Yu S. Acupuncture in the treatment of tinnitus: a systematic review and meta-analysis. European archives of oto-rhino-laryngology: official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS): affiliated with the German society for oto-rhino-laryngology. Head Neck Surg. 2016;273(2):285–294.
15. He M, Li X, Liu Y, et al. Electroacupuncture for tinnitus: a systematic review. PLoS One. 2016;11:3.
16. Kim JI, Choi JY, Lee DH, Choi TY, Lee MS, Ernst E. Ernst E: acupuncture for the treatment of tinnitus: a systematic review of randomized clinical trials. BMC Complement Altern Med. 2012;12:97. doi:10.1186/1472-6882-12-97
17. Wu Q, Wang J, Han D, Hu H, Gao H. Efficacy and safety of acupuncture and moxibustion for primary tinnitus: a systematic review and meta-analysis. Am J Otolaryngol. 2023;44(3):103821. doi:10.1016/j.amjoto.2023.103821
18. Ferrari M, Quaresima V. A brief review on the history of human functional near-infrared spectroscopy (fNIRS) development and fields of application. NeuroImage. 2012;63(2):921–935. doi:10.1016/j.neuroimage.2012.03.049
19. Pinti P, Tachtsidis I, Hamilton A, et al. The present and future use of functional near-infrared spectroscopy (fNIRS) for cognitive neuroscience. Ann N Y Acad Sci. 2020;1464(1):5–29. doi:10.1111/nyas.13948
20. Huang B, Wang X, Sun Q, Xiong G. Advances in the Application of Functional Near-Infrared Spectroscopy (fNIRS) in Tinnitus. Chin J Otol. 2022;20:824–828.
21. Shoushtarian M, Alizadehsani R, Khosravi A, et al. Objective measurement of tinnitus using functional near-infrared spectroscopy and machine learning. PLoS One. 2020;15(11):e0241695. doi:10.1371/journal.pone.0241695
22. Issa M, Bisconti S, Kovelman I, Kileny P, Basura GJ. Human auditory and adjacent nonauditory cerebral cortices are hypermetabolic in tinnitus as measured by functional near-infrared spectroscopy (fNIRS). Neural Plast. 2016;2016:1–13. doi:10.1155/2016/7453149
23. San Juan JD, Zhai T, Ash-Rafzadeh A, et al. Tinnitus and auditory cortex: using adapted functional near-infrared spectroscopy to measure resting-state functional connectivity. NeuroReport. 2021;32(1):66–75. doi:10.1097/WNR.0000000000001561
24. Schecklmann M, Giani A, Tupak S, Langguth B, Raab V. Functional near-infrared spectroscopy to probe state- and trait-like conditions in chronic tinnitus: a proof-of-principle study. Neural Plasticity. 2014;2014:894203.
25. Basura GJ, Hu XS, Juan JS, Tessier AM, Kovelman I. Human central auditory plasticity: a review of functional near-infrared spectroscopy (fNIRS) to measure cochlear implant performance and tinnitus perception. Laryngoscope Investig Otolaryngol. 2018;3(6):463–472. doi:10.1002/lio2.185
26. Yu X, Gong B, Yang H, et al. Effect of acupuncture treatment on cortical activation in patients with tinnitus: a functional near-infrared spectroscopy study. In:
27. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
28. Tunkel DE, Bauer CA, Sun GH, et al. Clinical practice guideline: tinnitus executive summary. Otolaryngol Head Neck Surg. 2014;151(4):533–541. doi:10.1177/0194599814547475
29. Cima RFF, Mazurek B, Haider H, et al. A multidisciplinary European guideline for tinnitus: diagnostics, assessment, and treatment. HNO. 2019;67(S1):10–42. doi:10.1007/s00106-019-0633-7
30. Jensen M, Hüttenrauch E, Schmidt J, Andersson G, Chavanon ML, Weise C. Neurofeedback for tinnitus: study protocol for a randomised controlled trial assessing the specificity of an alpha/delta neurofeedback training protocol in alleviating both sound perception and psychological distress in a cohort of chronic tinnitus sufferers. Trials. 2020;21(1):382. doi:10.1186/s13063-020-04309-y
31. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. J Evid Based Med. 2010;3(3):140–155. doi:10.1111/j.1756-5391.2010.01086.x
32. Song H, Chen L, Gao R, et al. Automatic schizophrenic discrimination on fNIRS by using complex brain network analysis and SVM. BMC Med Inform Decis Mak. 2017;17(Suppl 3):166. doi:10.1186/s12911-017-0559-5
33. NIRS-KIT: a MATLAB toolbox for both resting-state and task fNIRS data analysis. Available from: https://pubmed.ncbi.nlm.nih.gov/33506071/.
34. Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol. 1998;9(2):153–160.
35. Manning C, Grush L, Thielman E, Roberts L, Henry JA. Comparison of tinnitus loudness measures: matching, rating, and scaling. Am J Audiol. 2019;28(1):137–143. doi:10.1044/2018_AJA-17-0115
36. Shidara J, Kodera K. 純音聴力検査(空気伝導と骨伝導の閾値テスト)[Pure-tone audiometry (air and bone conductive threshold test)]. Nihon Rinsho. 1997;55(1):466–468. Japanese.
37. Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
38. Elgoyhen AB, Langguth B, De Ridder D, Vanneste S. Tinnitus: perspectives from human neuroimaging. Nat Rev Neurosci. 2015;16(10):632–642. doi:10.1038/nrn4003
39. Chung KF, Yeung WF, Yu YM, Kwok CW, Zhang SP, Zhang ZJ. Adverse events related to acupuncture: development and testing of a rating scale. Clin J Pain. 2015;31(10):922–928. doi:10.1097/AJP.0000000000000189
40. Peuker E, Filler T. Guidelines for case reports of adverse events related to acupuncture. Acupunct Med. 2004;22(1):29–33. doi:10.1136/aim.22.1.29
41. Wei Y, Zhang W, Li Y, et al. Acupuncture Treatment Decreased Temporal Variability of Dynamic Functional Connectivity in Chronic Tinnitus. Front Neurosci. 2021;15:737993. doi:10.3389/fnins.2021.737993
42. Fox MD, Raichle ME. Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat Rev Neurosci. 2007;8(9):700–711. doi:10.1038/nrn2201
43. Greicius M. Resting-state functional connectivity in neuropsychiatric disorders. Curr Opin Neurol. 2008;21(4):424–430. doi:10.1097/WCO.0b013e328306f2c5
44. Damoiseaux JS, Greicius MD. Greater than the sum of its parts: a review of studies combining structural connectivity and resting-state functional connectivity. Brain Struct Funct. 2009;213(6):525–533. doi:10.1007/s00429-009-0208-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Clinical Efficacy and Safety of a Modified Moxibustion Therapy for Low Back Pain in Lumbar Disc Herniation: A Two-Center, Randomized, Controlled, Non-Inferiority Trial
Xue K, Wang X, Xiao C, Zhang N, Liu M, Fu J, Cui J
Journal of Pain Research 2024, 17:1853-1865
Published Date: 23 May 2024
A Pilot Study for Effectiveness and Safety of Adjunctive Pharmacopuncture to Acupuncture Treatment for Rotator Cuff Diseases: A Pragmatic Randomized Controlled Trial
Cha HJ, Han CH, Jeon JH, Jeong JK, Jung IC, Yang C, Kang BK, Kim MJ, Choi YE, Kim YI
Journal of Pain Research 2024, 17:2203-2221
Published Date: 24 June 2024
Electro-Acupuncture for Diminished Ovarian Reserve: Protocol for a Randomized, Placebo-Controlled Trial
Tang H, Wang JX, Zheng SZ, Jia YF, Yu X, Zhao NN, Yang YH, Lin LP, Li SY, Zhao H
Journal of Multidisciplinary Healthcare 2025, 18:4341-4352
Published Date: 30 July 2025
Acupuncture for Rapid Pain Relief and Restoration of Motor Function in Acute Lateral Ankle Sprains: A Randomized Controlled Trial Protocol Based on Infrared Thermography
Wen W, Jin Y, Deng Y, Zhao S, Tang X, Li W, Song L, Lv Z, Guo T, Liang F
Journal of Pain Research 2025, 18:4387-4399
Published Date: 27 August 2025