Back to Journals » Journal of Pain Research » Volume 15
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial
Authors Yin S ![]() , Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD
, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD ![]() , Wu N
, Wu N ![]()
Received 26 January 2022
Accepted for publication 29 April 2022
Published 18 May 2022 Volume 2022:15 Pages 1443—1455
DOI https://doi.org/10.2147/JPR.S356044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Shuai Yin,1,* Zhen-Hua Zhang,1,* Yi-Niu Chang,2,* Jin Huang,2 Ming-Li Wu,1 Qi Li,1 Jin-Qi Qiu,1 Xiao-Dong Feng,1,2 Nan Wu2
1Rehabilitation Center, The First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, 450000, People’s Republic of China; 2School of Rehabilitation Medicine, Henan University of Chinese Medicine, Zhengzhou, Henan, 450046, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Dong Feng, Rehabilitation Center, The First Affiliated Hospital of Henan University of Chinese Medicine, No. 19, Renmin Road, Zhengzhou, 450000, People’s Republic of China, Tel +8615303828605, Email [email protected] Nan Wu, School of Rehabilitation Medicine, Henan University of Chinese Medicine, No. 156, Jinshui East Road, Zhengzhou, 450046, People’s Republic of China, Tel +8613540484550, Email [email protected]
Purpose: Abnormal central nervous system function is the key central pathological factor leading to chronic pain in patients with knee osteoarthritis (KOA). Acupuncture can effectively relieve the pain of KOA patients. However, the central nervous mechanism of acupuncture treating KOA is not fully understood. This trial will use functional magnetic resonance imaging (fMRI) analysis techniques to investigate the potential central nervous mechanism of acupuncture treatment of KOA.
Materials and Methods: A total of 108 patients will be randomized (in a 1:1:1 ratio) into three groups, this trial will include 4-week treatment, patients in groups A and B will receive 20 acupuncture and sham acupuncture sessions, respectively, patients in group C will not receive any intervention, and all patients will receive fMRI scans before and after the intervention. The Western Ontario and McMaster Universities Osteoarthritis Index score (WOMAC) will be the primary clinical outcome. Then, we will explore the functional changes of the cognitive control network (CCN) in the brains of KOA patients through whole brain functional connectivity (FC) analysis and seed-based functional connectivity (sFC) analysis. Pearson correlation coefficient will be used to analyze the relationship between the improved value of the clinical correlation scale and the change of fMRI data.
Discussion: This trial will analyze the efficacy of verum acupuncture, sham acupuncture and the waiting-list for KOA and explore the activity of the CCN in three groups of patients by fMRI, so as to reveal the central nervous mechanisms of acupuncture in the treatment of KOA.
Study Registration: This study is approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Traditional Chinese Medicine (No: 2019HL-133-01) and registered in the Chinese Clinical Trial Registry, ChiCTR2000038554.
Keywords: knee osteoarthritis, acupuncture, cognitive control network, randomized controlled trial
Graphical Abstract:

Introduction
Knee osteoarthritis (KOA) is a joint disease characterized by degeneration, destruction, and hyperosteogeny of knee cartilage.1 Currently, the pathogenesis of KOA is not completely clear, but some studies have shown that KOA is more common in the elderly and may be related to factors such as gender, obesity, knee joint injury, and gastrointestinal microbiome.2,3 Its typical manifestations are intermittent pain, weight-bearing pain, which gradually develop into chronic pain.4 Compared with acute pain, chronic pain involves sensory, emotional, cognitive, and other problems,5 which significantly reduces the quality of life of patients and increases the burden of society.6 Approximately 250 million people worldwide have been diagnosed with KOA, accounting for 3.6% of the global population, and their disease burden continues to increase due to the aging population.7 The aim of KOA treatment is to provide symptomatic pain relief, improve knee function, and improve the patient’s quality of life.8 At present, the treatment methods for KOA mainly include self-management including proper diet, weight loss and control poor posture, etc.9 scientific exercise including aerobic exercise and joint range of motion training, etc.10 drug treatment including non-steroidal anti-inflammatory drugs and analgesics, etc.11 and surgical treatment including joint replacement, arthroscopic surgery and so on.12 However, these treatments can not fully satisfy the treatment needs of all KOA patients. Consequently, an increasing number of patients with KOA is likely to choose complementary and alternative treatments.13
As one of the most popular complementary and alternative treatments,14 acupuncture has been used to treat osteoarthritis disorders in China since ancient times, and systematic reviews of Randomised Controlled Trials (RCTs) suggested benefits of acupuncture for KOA.13,15 However, the central nervous mechanism of acupuncture in treating patients with KOA is not clear, which prevents its clinical application and further promotion.
KOA is a complex chronic pain disease, partly due to both nociceptive and neuropathic mechanisms.16 It is often accompanied by changes in neuroplasticity and central nervous system sensitization.17,18 Functional Magnetic Resonance Imaging (fMRI) technology has to play an important role in the brain of pain management, emotional cognition, memory research and so on. It is one of the advanced functional medical imaging research methods for studying the human brain.19 In recent years, some studies have shown that compared with healthy subjects, the cognitive control network (CCN) of chronic pain patients has changed, such as the volume of gray matter in the orbitofrontal cortex and the anterior cingulate gyrus decreases, the volume of thalamus gray matter increases,20 and the functional connectivity between the forebrain insula and the nucleus accumbens decreases,21 they believe that the dysfunction of the CCN is an important factor that causes chronic pain. Moreover, a neuroimaging study of KOA patients showed that compared with healthy subjects, the blood flow in the bilateral anterior cingulate gyrus, hippocampus, amygdala, and insula of KOA patients has changed, while these encephalic regions belong to the CCN.22 So, we infer that the functional abnormality of the brain’s CCN is the key central pathological factor that causes KOA patients’ chronic pain persisted and difficult to eliminate. In addition, an fMRI study of migraine subjects showed that acupuncture can widely regulate the CCN function of migraine patients by reducing the abnormal functional connection of the medial prefrontal lobe, anterior cingulate, bilateral ventral striatum and the periaqueductal gray matter, and exert a lasting analgesic effect.23 Therefore, we hypothesized that acupuncture can also exert its therapeutic role by regulating the CCN in KOA patients and designed this fMRI study of acupuncture for KOA, using the analysis of the functional connectivity (FC) of the whole brain and the seed-based functional connectivity (sFC) analysis to explore the functional changes in the CCN in the brain of KOA patients.
However, there are many problems in the previous researches on the central nervous mechanisms of KOA. KOA may have a tendency to self-heal over time,24 so that the lack of waiting list group control may not be able to rule out the self-healing tendency, this may influence the exploration of the therapeutic effect of acupuncture. The experimental design of the sham acupuncture group is unreasonable, since the acupoint selection and stimulation amount have not been considered. The analysis technique of functional magnetic resonance imaging is single, and the repeatability of the result is not high. All of these limit further study on the central nervous mechanisms of acupuncture in the treatment of knee osteoarthritis. Therefore, this trial increased the waiting-list group, introduced the deqi rating scale, and adopted the analysis methods of FC and sFC, with the help of multi-mode fMRI, including Blood Oxygen Level Dependent-fMRI (BOLD-fMRI) and Arterial Spin Labeling-fMRI (ASL-fMRI), combined with clinical efficacy evaluation, aiming to explore the central nervous mechanisms of acupuncture treatment of chronic pain in KOA patients by observing the activity of the CCN in the brain and re-verify the clinical efficacy of acupuncture in the treatment of KOA.
Methods
Trial Design
This is a parallel-design, randomized controlled neuroimaging trial that aims to explore the central nervous mechanisms of acupuncture treatment of chronic pain in KOA. This trial has been approved by the ethical committees of the First Affiliated Hospital of Henan University of Traditional Chinese Medicine (No: 2019HL-133-01) and registered in the Chinese Clinical Trial Registry, ChiCTR2000038554. This trial will be conducted in accordance with the Declaration of Helsinki. The protocol will be reported in following Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement (Additional File 1: Completed Standard Protocol Items). After informed consent acquisition (Additional File 2: Informed Consent Form), a total of 108 eligible KOA patients diagnosed with the Chinese Medical Association (CMA) diagnostic criteria25 will be recruited and randomized to the verum acupuncture group (Group A), the sham acupuncture group (Group B), and the waiting-list group (Group C) at 1:1:1. The treatment period will last for 4 weeks. fMRI scan and clinical evaluation data will be collected and assessed at baseline and the end of treatment. The collected data will be analyzed to investigate the relationship between clinical efficacy changes and brain functional activity changes in each group. Adverse events will be recorded in the case report forms (CRF) at any time during the study. Figure 1 shows the study design in the flowchart, and Table 1 illustrates the time schedule of enrollment, interventions, assessments, and visits of participants (Figure 1 and Table 1).
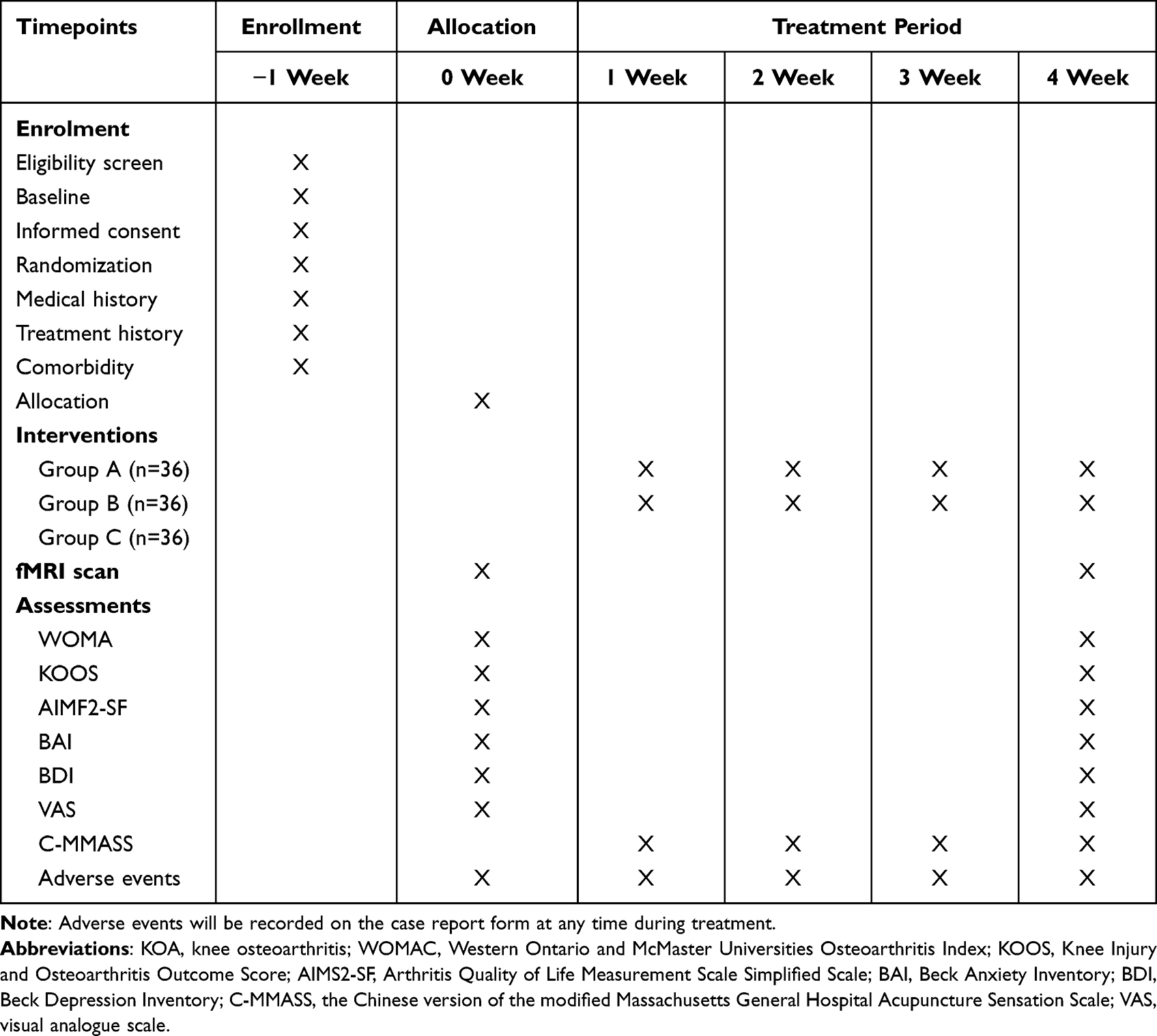 |
Table 1 Study Design Schedule |
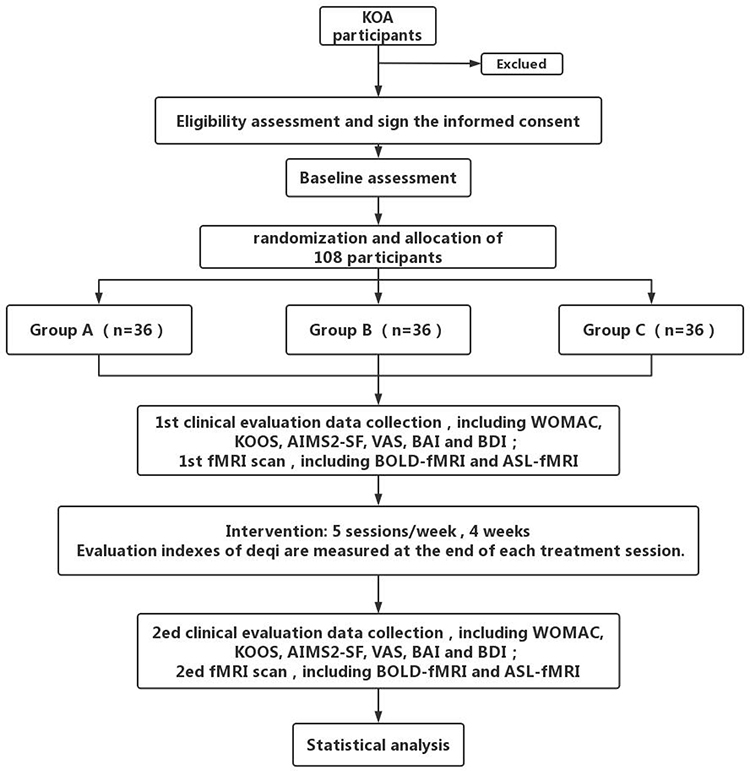 |
Figure 1 Flowchart of the study procedure. |
Recruitment
Patients with knee osteoarthritis who meet the CMA diagnostic criteria will be recruited from the outpatient and inpatient departments of the First Affiliated Hospital of Henan University of Traditional Chinese Medicine. We will use the Internet and posters to briefly introduce the trial and provide eligible participants with treatment details and contact information.
Participants
Informed Consent
We will provide the potential participants with a detailed description of the benefits of the trial and the risks that may exist. If they decide to take part in, they will be asked to sign the informed consent. Then, they will be included in this trial after randomization. If a participant withdraws from the trial, the reasons for withdrawal will be recorded.
Inclusion Criteria
Participants who meet all of the following requirements will be considered for inclusion: 1) Male or female, aged 45–75 years; 2) Following the diagnostic criteria of knee osteoarthritis, and Right-handed; 3) Good compliance and willingness to cooperate with the research; 4) Radiologic confirmation of knee osteoarthritis (Kellgren–Lawrence grade I-III); 5) The informed consent form was signed by the patient or by their immediate family members.
Exclusion Criteria
Subjects will be excluded if they meet any of the following criteria: 1) Patients with other knee joint diseases, such as tuberculosis, tumor, rheumatism and rheumatoid arthritis; 2) Patients with sprain, contusion or other trauma, foot deformity, pain and other diseases affecting normal walking; 3) Patients with severe cardiovascular disease, damage of liver and kidney function, immune deficiency, diabetes mellitus, and blood disease; 4) Patients with severe drug and alcohol dependence, mania or schizophrenia; 5) Patients with obvious headache, migraine, dysmenorrhea and other chronic pain diseases, history of head trauma; 6) Patients are insensitive to pain due to advanced diabetes, neuropathy or use of strong painkillers; 7) Have knee pain caused by radiculopathy/herniation of an intervertebral disc; 8) Have a history of prolotherapy, hyaluronic acid injections or corticosteroid injections within 3 months; 9) Have received acupuncture, electro-acupuncture, Tui-na therapy, massage, or physiotherapy 8 weeks prior to enrollment of this trial; 10) Have MRI contraindications such as claustrophobia, cardiac pacemaker, defibrillator, heart stenting, or intrauterine device.
Sample Size Estimation
According to previous studies, the WOMAC functional score of KOA patients decreased by 12.1 points after acupuncture, 9.4 points after sham acupuncture, and 5.6 points after education, and the WOMAC pain score of KOA patients decreased by 3.6 points after acupuncture, 2.6 points after sham acupuncture and 1.5 points after education.26 In this study, we anticipated that the total WOMAC score would be reduced by 17 points after verum acupuncture, 13 points after sham acupuncture, and 8 points after the waiting list. With α = 0.05, 1 − β = 0.9, and a standard deviation of 10, we need at least 99 participants in total. Considering a dropout rate of 10%, a total of 108 participants will be included in this trial. All 108 participants will receive fMRI scans and corresponding treatments, and this sample size is much larger than the 12 cases per group required by the technical requirements of quality control and network analysis of acupuncture brain functional imaging,27 which can make the test results more reliable.
Randomization
In this trial, eligible patients who consent to participate will be randomly assigned to one of three groups via a central randomization system for clinical research in a ratio of 1:1:1 by an independent researcher, who will not involve in the implementation or statistical analysis of the trial. Random number lists will be created by PROCPLAN of SAS 9.2 (SAS Institute Inc., Cary, NC, USA). The randomization allocation will use sequentially numbered, opaque and sealed envelopes. The participants’ screening sequence numbers will be printed outside the envelope, whereas the group names will be printed inside. After a participant has met all selection criteria, signed the informed consent form and completed the baseline assessments, the researcher will inform the statistician in the center. The statistician will open the envelope according to the participant’s screening sequence number and then assign the participant to one of the three groups.
Blinding
The acupuncturist and patients will not be blinded because of the nature of the intervention. However, it is feasible to conceal the researchers, statisticians, and outcome assessors. The outcome assessor and data analyst will be blinded to group assignments. Unblinding will not be done until the completion of data analysis, and after the data analysis, we will have a blinded interpretation of the study results to minimize misleading data interpretation.
Researchers
The treatment will be performed by the same licensed acupuncturist with more than six years of experience. Besides, two supervisory data collectors and analysts who do not know the random assignment protocol will monitor the whole experiment. People who are responsible for recruitment, researchers, outcome assessors, and the statistician in the trial will be trained strictly before the trial.
Safety Assessment
In this study, all patients will not be allowed to take drugs that may change the symptoms of KOA. If severe knee pain occurs, ibuprofen (300 mg per capsule) will be allowed as a first-aid drug, the type and dosage of medication used should be recorded in the case report form (CRF). Any adverse events (AE) during treatment, including pain, hematoma, local infection, folding needle, syncope, nausea, headache, dizziness, insomnia, or vomiting during or after treatment, will be recorded on the AE report form. Any serious adverse events (SAE) will be reported to the lead investigator at once and the Medical Ethics Committee within 24 hours. If a first aid incident is reported, a preliminary investigation and follow-up monitoring will be conducted.
Interventions
The treatment will be performed by the same licensed acupuncturist with more than six years of experience. Besides, two supervisory data collectors and analysts who do not know the random assignment protocol will monitor the whole experiment. People who handle recruiting participants, researchers, outcome assessors, and the statistician in the trial will be trained strictly before the trial.
Group A
Acupoint Choice Scheme
The selected acupoints for the verum acupuncture treatment include Dubi (ST35), Neixiyan (EX-LE4), Heding (EX-LE2), Yanglingquan (GB34), Yinlingquan (SP9). At the same time, depending on the patient’s condition, a ashi acupoint (the point where the patient feels most pain) can be added (Figure 2).
 |
Figure 2 Acupoints location. |
Acupuncture Operation
The patients in the verum acupuncture group maintain a comfortable position, then disinfect their skin with 75% alcohol, and the acupuncturist inserts perpendicularly into the points for 21–26 mm with a sterile needle (Huatuo, Suzhou, China, 0.25 mm, in diameter and 40 mm in length). Then, the needle is twisted between 90° and 180°, and the range of lifting and insertion was between 0.1 and 0.3 centimeters, and the frequency was between 60 times and 90 times per minute. After the deqi response (including soreness, numbness, distention, and heaviness) is obtained, the needle will be kept in the skin for 30 minutes and manipulated every 10 minutes for maintaining the deqi sensation. Every patient will receive acupuncture treatment once a day, 5 days as a course of treatment, 4 consecutive courses of treatment, each course of rest for 2 days.
Group B
Acupoint Choice Scheme
The selected acupoints (NP1-NP6) are all located 1cm away from the outer side of the midline of the lower extremity of the six acupuncture points selected in the Group A “Dubi (ST35), Neixiyan (EX-LE5), Heding (EX-LE2), Yanglingquan (GB34), Yinlingquan (SP9), and a ashi acupoint” (Figure 2).
Acupuncture Operation
To minimize the effect of sham acupuncture, and avoid the deqi response, it is required that the needle should not be inserted longer after piercing the skin, the needle is kept upright and directly retained for 30 minutes without manual operation.
Group C
Wait for observation for 4 weeks without any intervention. At the end of the trial, patients can obtain free acupuncture treatments for 20 times.
Outcome
Primary Outcome
We will use the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) as the primary outcome measurement.28 It consists of 24 items assessing the patients with KOA pain (5 items), stiffness (2 items), and physical function (17 items). The pain, stiffness, and body function sub-scales range from 0–50, 0–20, and 0–170, respectively, and the total score ranges from 0–240. The higher the score, the more severe the symptoms or physical disability.
Secondary Outcomes
1. Knee Injury and Osteoarthritis Outcome Score (KOOS)29 is a self-administered self-explanatory questionnaire. It contains five scales with 42 items, including measure pain (9 items), other symptoms (7 items), activities of daily living (17 items), exercise and entertainment function (5 items), and knee-related quality of life (4 items).
2. Arthritis Quality of Life Measurement Scale Simplified Scale (AIMS2-SF)30 is a reliable and effective self-reporting questionnaire for assessing the health status of patients with arthritis. There are 5 dimensions and 26 items: physical (12 items), symptoms of pain (3 items), affect (5 items), social interaction (4 items), and role components (2 items). All entries are scored on a scale of 1 to 5.
3. Emotional monitoring: Pain symptoms often affect the mood changes of patients, resulting in anxiety and depression. To study the relationship between the changes of emotion and brain activity in patients with KOA before and after treatment, the Baker anxiety scale (BAI)31 and Baker Depression scale (BDI)32 will be used at baseline and the end of treatment.
4. The pain visual analogue scale (VAS):33 this is a 10-point scale ranging from “none” (0) to “unbearable” (10) to assess the degree of knee pain in patients with KOA: “none” (0 points), “mild” (about 2 points), “moderate” (about 5 points), “severe” (nearly 8 points) and “unbearable” (close to 10 points).
5. Furthermore, after each acupuncture treatment, participants in the two acupuncture groups will be required to fill in the needle sensation evaluation form, which is based on the Chinese version of the modified Massachusetts General Hospital Acupuncture Sensation Scale (C-MMASS).34 The scale will be used to evaluate the 11 acupuncture sensations: soreness, aching, deep pressure, heaviness, fullness, tingling, numbness, dull pain, warmth, cold, and throbbing.
MRI Data Acquisition
Each scan included three sequences: 3DT1 structure image, resting-state BOLD-fMRI and ASL-fMRI. During the data acquisition, participants will be instructed to keep awake, relaxed with their eyes closed, and remain motionless as much as possible. All fMRI data will be obtained in the MRI room of The First Affiliated Hospital of Henan University of Traditional Chinese Medicine. High resolution structural and functional images will be scanned with Ingenia 3.0 Tesla MRI scanner (Philips Medical System, Best, The Netherlands) and head orthogonal coil. The specific parameters are as follows:
1.3DT1 Structural: Repeat Time (TR): 7.7ms, Echo Time (ET): 3.86ms, Field Of View (FOV): 256mm ×256mm, data matrix: 256 × 256, slice thickness: 1mm.
2. The resting-state BOLD-fMRI will be scanned by the whole-brain EPI sequence. The parameters were as follows: TR/TE: 2000/30 ms, FOV: 240mm x 240mm, scan matrix: 64 x 64, flip angle: 90°, slice thickness/slice spacing = 5/0mm, slice number: 32 slices.
3. Arterial spin labeling imaging (ASL): Two delayed pseudo-continuous arterial spin labeling (pCASL) scans would be used. Two marker delay time: 1.5s, 2.5s, FOV: 220 x 220mm, matrix: 64 x 64, layer number: 16, layer thickness: 8mm, echo time (TE): 12 ms, each delay 8 pairs of marker control images, a total of 16 pairs.
Data Collecting and Monitoring
The trial data of all participants will be managed in both paper and electronic forms of CRF. The evidence-based Medicine Center of the university will handle monitoring the study as well as the data every 3 months. During the trial period, only data evaluators can access CRF and enter data.
Data Analysis
All the data of this trial will be uniformly filled in the research report form, and the test results based on computer software will be exported by the program and pasted on the research report form, and other tests will be completed directly in the research report form. After the completed research report form will be reviewed by the project manager, the data entry staff will be organized to input the data and manage the original form uniformly.
Clinical Data Analysis
Clinical data statistical analyses will be performed with SPSS 22.0 statistics software (IBM Corporation, Armonk, NY, USA). The data analysis process will be completed by statisticians who are independent of the research team and blinded to the test settings. Quantile–Quantile Plots will be used to test the normality of the data, changes in the scores from baseline within treatment groups will be assessed by the paired sample t-test or Wilcoxon test (if normality is violated), including the WOMAC, KOOS, AIMS2-SF, BAI, BDI and VAS. One-way analysis of variance (ANOVA) or Kruskal–Wallis one-way ANOVA (if normality is violated) will be used for comparison among the three groups, including age, height, weight, scores of WOMAC, KOOS, AIMS2-SF, BAI, BDI and VAS. In addition, the available data of the three groups will be tested by bilateral tests and the confidence intervals are all 95% bilateral, p < 0.05 (α = 0.05) is considered to indicate statistical significance.
MRI Data Analysis
Based on the SPM8 software platform (SPM8, Wellcome Department of Imaging Neuroscience, London, UK; http://www.fil.ion.ucl.ac.uk/spm/), the MRI data will be preprocessed. After data preprocessing, we will use the analysis of the FC of the whole brain and the sFC analysis to explore the functional changes of the CCN in the brain of KOA patients. Then, based on the results of the FC and sFC analysis of the Bol–d-fMRI data, we will select the relevant region of interest (ROI) and use the ASL-fMRI data to calculate the cerebral blood flow around the ROI, and extract the same brain area on the opposite side of the ROI to calculate various average perfusion parameters. We will also compare the results of ASL-fMRI with the functional network changes of BOLD-fMRI to complete the interactive verification of multi-modal images. The paired t-test will be used to evaluate brain responses in each group through intra-group analysis (post-treatment minus preconditioning). The between-group analysis will be used to compare the differences in the activity of the CCN in the brain. During data analysis, we will include age, gender and other factors into the data analysis as covariates. Pearson correlation coefficient will be used to analyze the relationship between the improved value of the clinical correlation scale and the change of fMRI image data.
Patient and Public Involvement
Patients and the public will not be involved in the development of this clinical trial protocol.
Discussion
KOA is a major health concern worldwide. For the most early and middle stage patients, safe and effective early intervention is considered to prevent and delay the occurrence of KOA.35 As a representative of traditional Chinese medicine, acupuncture has a remarkable curative effect on KOA.36,37 However, the mechanism of acupuncture is not clear. As we all know, the effect of acupuncture is a complex biological process. Some mechanism experiments have shown that acupuncture could treat knee osteoarthritis by reducing the content of inflammatory factors,38 and increasing the concentration of β-endorphin.39 At the same time, acupuncture can down-regulate the expression of matrix metalloproteinase-3 and matrix metalloproteinase-1 in cartilage tissue, showing that acupuncture has a certain protective effect on cartilage from KOA.40 However, these factors do not play indispensable roles in the role of acupuncture. In recent years, researchers have turned their attention to the study of the neural mechanism. The results show that acupuncture can achieve an analgesic effect by regulating the relevant pain signals in the central system.41 The modulation of pain signals can be weakened or disappeared with the damage of related brain areas such as the thalamus, caudate nucleus, periaqueductal gray, and so on. Thus, it can be seen that the information regulation of the central system is an indispensable step for acupuncture to take effect. However, researchers gradually realized some problems related to the study of the central nervous mechanisms of acupuncture. The data obtained from animal experiments can not eliminate the influence of species-related differences with the results of the study. Moreover, the results of in-vitro experiments cannot fully reflect systemic interactions. Therefore, elucidating the central nervous mechanisms by obtaining objective and clear visual evidence in vivo has become an urgent task in the study of acupuncture and moxibustion in the treatment of chronic pain in KOA. So, this trial will design a central research scheme of acupuncture treatment of KOA, which consists of verum acupuncture, sham acupuncture, and the waiting-list as a random control group. The advantages of the trial design are shown in the following aspects.
Using BOLD-fMRI and ASL-fMRI Interactive Verification to Make the Results More Reliable
Since the 1990s, a large number of researches on acupuncture brain functional imaging have been carried out. Compared with previous research techniques, fMRI has been widely used to study the central nervous mechanisms of acupuncture effect42 because of its high temporal and spatial resolution, non-radiation, fast imaging speed, and rich data post-processing methods.43 Using this neuroimaging technique, researchers have been able to non-invasively examine the effects of acupuncture on the central nervous system.44 It can directly reflect the effect of acupuncture on the structure and function of the human brain and overcome the influence of species difference and in vitro operation on the research results of acupuncture central nervous mechanisms. Studies showed that acupuncture could regulate the pain-related nerve centers and achieve analgesic effects.45 For example, acupuncture could influence the Regional Homogeneity values of multiple regions in the default mode network for patients with migraines, including posterior cingulate.46 Therefore, fMRI has been selected as a tool with which to reveal the central nervous mechanisms of the acupuncture effect of the KOA in the present study.
Among the many functional neuroimaging techniques, BOLD-fMRI has become the choice of many researchers because of its special advantages. Compared with other brain functional imaging techniques,47 BOLD-fMRI technology can provide omnidirectional brain functional activity information from cortical to subcortical structures and has the characteristics of high temporal and spatial resolution, safety, no radiation hazard, and rich and diverse data analysis. It has been widely used in neuroscience, psychology, psychiatry, and acupuncture of traditional Chinese medicine.48 An rs-fMRI study of acupuncture treatment of KOA found that a positive association in the functional connectivity changes between the right frontoparietal network (rFPN) and the left parietal operculum (post–pre) and the corresponding changes in clinical KOOS pain score in patients with KOA.49 The ASL technique of multi-delay and multi-parameter arterial spin labeling imaging focuses on local cerebral blood perfusion,50 which makes up for the lack of clarity in the physiological mechanism of BOLD-fMRI. Compared with the traditional ASL technology, pCASL has the advantages of higher resolution and less noise. Based on the FC and sFC analysis of BOLD-fMRI data to explore the effect of acupuncture on the CCN, the multimodal verification of the experimental results with ASL-fMRI will effectively improve the reliability and repeatability of the results.
Choose Verum Acupuncture, Sham Acupuncture and Waiting-List to Compare with Each Other, the Control Groups are Reasonable
According to the acupuncture theory of traditional Chinese medicine, the choice of acupoints should follow the following three principles: local selection, meridian selection, identification, and selection of points. In the idea of acupuncture treatment of knee osteoarthritis, local acupoints have been used since ancient times. Some researchers51 used data mining to analyze the relevant literature of modern acupuncture treatment for KOA and found that Dubi, Neixiyan, and Yanglingquan were the top three acupoints with high frequency. Therefore, combined with the literature and expert consensus, this study will select Dubi (ST35), Neixiyan (EX-LE5), Heding (EX-LE2), Yanglingquan (GB34), Yinlingquan (SP9) as the acupuncture points. At the same time, we will also choose a ashi acupoint, which is the pain spots or the tender points that are good for alleviating local pain.
A suitable control group is particularly important for well-designed clinical trials and is an important source of high-quality evidence-based medicine for acupuncture. However, it is difficult to design an inert placebo control for acupuncture because it is a physical intervention. At present, acupuncture treatment of KOA clinical trials, most of them used acupuncture at non-effective acupoints or non-effective acupuncture at effective acupoints as a placebo control. However, it was found that this approach may induce a wide range of peripheral, segmental and central physiological responses to an unpredictable degree.52–54 In order to effectively avoid these physiological reactions, we can only use the method of non-effective acupoints with non-effective puncture at the local of the knee as sham acupuncture. The non-acupoints in the sham acupuncture group are also selected around the knee joint, located at 1 cun away from the outer side of the real acupuncture points and not on any regular meridians. While the needle depth is 1~2mm and do no other operations after the insertion of needles to avoid the deqi sensation as much as possible, which could minimize the possible effect of sham acupuncture, overcome the bias caused by psychological factors in patients receiving sham acupuncture as far as possible and maximally help to exclude the bias of the spinal segmental effect of the acupoints. In addition, we also used waiting-list group as a blank-control group.
In conclusion, we set up control groups reasonably, through the mutual comparison between verum acupuncture, sham acupuncture and the waiting-list for knee osteoarthritis, which can better help us to explore the influence of acupuncture on the CCN, and reveal the central nervous mechanisms of acupuncture treatment of KOA.
Strict Quality Control to Improve the Reliability of the Research Results
Determining strict control methods is the key to ensure the methodological quality of RCT. To improve the result reliability of this study, we designed the quality control program from the following aspects: 1. Strictly screen the subjects with similar demographic indicators (age between 45 and 75 years and being right-handed) and the same disease state to avoid excessive difference in brain function at baseline; 2. sample size to obtain stable statistical power; we include 36 patients in each group, this sample size is much larger than the 12 cases per group required by the technical requirements of quality control and network analysis of acupuncture brain functional imaging,27 which can make the test results more reliable. 3. fMRI scan: collect BOLD-fMRI + ASL-fMRI data strictly according to the operating procedures of fMRI and the design of this experiment, only one technician will perform all scans in the same MRI machine according to the related operation standard and the design of the study in the fixed condition. Furthermore, the unified guidebook will be used to standardize the opinions and behaviors of the researchers. Moreover, during the 24h before scanning, participants will be asked to maintain their regular lifestyle and avoid overexertion and staying up late. The use of alcohol, tobacco, tea, and coffee is prohibited. Before being scanned, the emotional state of each participant will be evaluated via the emotional state assessment scales. During the scan, participants will be asked to close their eyes and use a blindfold and to plug their ears with earplugs, stay awake and not speak; 4. The acupuncturist is a doctor with more than six years of work experience and a medical practitioner certificate. Relevant personnel and data evaluators responsible for recruiting patients must undergo a rigorous training before the study to ensure that all experimental procedures have uniform standards and avoid observational bias.
In summary, for the first time in this trial, we combine BOLD-fMRI with ASL-fMRI and use the FC of the whole brain and the sFC analysis to observe the functional changes of the CCN in the brain of KOA patients. Then, the Pearson correlation coefficient will be used to analyze the relationship between the improved value of the clinical correlation scale and the function changes of CCN, to explore the central nervous mechanisms of acupuncture in the treatment of KOA.
Abbreviations
KOA, knee osteoarthritis; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; KOOS, knee Injury and Osteoarthritis Outcome Score; AIMS2-SF, Arthritis Quality of Life Measurement Scale Simplified Scale; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; VAS, visual analogue scale; C-MMASS, the Chinese version of modified Massachusetts General Hospital Acupuncture Sensation Scale; 3DT1, three-dimensional MRI sequence with a voxel size of 1 mm; ACC, anterior cingulate cortex; CMA, Chinese Medical Association; BOLD, blood-oxygen-level-independent; ASL, arterial spin labeling; CRF, Case report form; CCN, cognitive control network; sFC, seed-based functional connectivity; fMRI, functional magnetic resonance imaging; MRI, magnetic resonance imaging; rs-fMRI, resting-state functional magnetic resonance imaging.
Trial Status
The trial was registered at China Clinical Trials Registry on September 24, 2020. (No. ChiCTR2000038554). The dates of the intended trial period were from 1 October 2020 to 31 December 2022. This study is approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Traditional Chinese Medicine (Ethics Reference No: 2019HL-133-01). The first participant was recruited on 1 March 2021, and the intended completion date will be 31 December 2022.
Acknowledgments
We are very grateful to Dr. Ruiqing Li from the first affiliated Hospital of Henan University of traditional Chinese Medicine and Dr. Ruirui Sun, teacher of acupuncture and massage at Chengdu University of traditional Chinese Medicine, who helped us design the thesis and the editor of English language and grammar.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the Science and Technology Department of Henan Province (182102310311, 192102310162), Special Project of Scientific Research on Traditional Chinese Medicine in Henan Province (grant number 2017JDZX030, 2018JDZX035, 2018JDZX115, 2019JDZX2001), training Program of leading talents in Clinical disciplines of traditional Chinese Medicine in Henan Province (2100202). The sponsors have no role in the design of the trial; collection, management, analysis, and interpretation of data; writing of the report, or the decision to submit the report for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lespasio MJ, Piuzzi NS, Husni ME, Muschler GF, Guarino A, Mont MA. Knee osteoarthritis: a primer. Perm J. 2017;21:16–183. doi:10.7812/TPP/16-183
2. Driban JB, Harkey MS, Barbe MF, et al. Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review. BMC Musculoskelet Disord. 2020;21(1):332. doi:10.1186/s12891-020-03367-2
3. Sánchez Romero EA, Meléndez Oliva E, Alonso Pérez JL, et al. Relationship between the gut microbiome and osteoarthritis pain: review of the literature. Nutrients. 2021;13(3):3. doi:10.3390/nu13030716
4. Ji RR, Berta T, Nedergaard M. Glia and pain: is chronic pain a gliopathy? J Pain. 2013;154 Suppl 1(1):S10–S28. doi:10.1016/j.pain.2013.06.022
5. Mossey JM, Gallagher RM. The longitudinal occurrence and impact of comorbid chronic pain and chronic depression over two years in continuing care retirement community residents. Pain Med. 2004;5(4):335–348. doi:10.1111/j.1526-4637.2004.04041.x
6. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–1602. doi:10.1016/S0140-6736(16)31678-6
7. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
8. Siddiq M, Clegg D, Jansen TL, et al. Emerging and new treatment options for knee osteoarthritis. Curr Rheumatol Rev. 2021. doi:10.2174/1573397117666211116111738
9. Khachian A, Seyedoshohadaei M, Haghani H, et al. Effect of self-management program on outcome of adult knee osteoarthritis. Int J Orthop Trauma Nurs. 2020;39:100797. doi:10.1016/j.ijotn.2020.100797
10. Sánchez Romero EA, Fernández-Carnero J, Calvo-Lobo C, et al. Is a combination of exercise and dry needling effective for knee OA? Pain Med. 2020;21(2):349–363. doi:10.1093/pm/pnz036
11. Kan HS, Chan PK, Chiu KY, et al. Non-surgical treatment of knee osteoarthritis. Hong Kong Med J. 2019;25(2):127–133. doi:10.12809/hkmj187600
12. Quinn RH, Murray JN, Pezold R, et al. Surgical management of osteoarthritis of the knee. J Am Acad Orthop Surg. 2018;26(9):e191–e193. doi:10.5435/JAAOS-D-17-00424
13. Fuggle NR, Cooper C, Oreffo R, et al. Alternative and complementary therapies in osteoarthritis and cartilage repair. Aging Clin Exp Res. 2020;32(4):547–560. doi:10.1007/s40520-020-01515-1
14. Chen J, Liu A, Zhou Q, et al. Acupuncture for the treatment of knee osteoarthritis: an overview of systematic reviews. Int J Gen Med. 2021;14:8481–8494. doi:10.2147/IJGM.S342435
15. Liu W, Fan Y, Wu Y, et al. Efficacy of acupuncture-related therapy in the treatment of knee osteoarthritis: a network meta-analysis of randomized controlled trials. J Pain Res. 2021;14:2209–2228. doi:10.2147/JPR.S315956
16. Hochman JR, Davis AM, Elkayam J, et al. Neuropathic pain symptoms on the modified painDETECT correlate with signs of central sensitization in knee osteoarthritis. Osteoarthr Cartil. 2013;21(9):1236–1242. doi:10.1016/j.joca.2013.06.023
17. Jiang Y, Oathes D, Hush J, et al. Perturbed connectivity of the amygdala and its subregions with the central executive and default mode networks in chronic pain. Pain. 2016;157(9):1970–1978. doi:10.1097/j.pain.0000000000000606
18. Tajerian M, Leu D, Zou Y, et al. Brain neuroplastic changes accompany anxiety and memory deficits in a model of complex regional pain syndrome. Anesthesiology. 2014;121(4):852–865. doi:10.1097/ALN.0000000000000403
19. Chen S, Li X. Functional magnetic resonance imaging for imaging neural activity in the human brain: the annual progress. Comput Math Methods Med. 2012;2012:613465. doi:10.1155/2012/613465
20. Riederer F, Marti M, Luechinger R, et al. Grey matter changes associated with medication-overuse headache: correlations with disease related disability and anxiety. World J Biol Psychiatry. 2012;13(7):517–525. doi:10.3109/15622975.2012.665175
21. Ikeda E, Li T, Kobinata H, et al. Anterior insular volume decrease is associated with dysfunction of the reward system in patients with chronic pain. Eur J Pain. 2018;22(6):1170–1179. doi:10.1002/ejp.1205
22. Cottam WJ, Condon L, Alshuft H, et al. Associations of limbic-affective brain activity and severity of ongoing chronic arthritis pain are explained by trait anxiety. Neuroimage Clin. 2016;12:269–276. doi:10.1016/j.nicl.2016.06.022
23. Li Z, Liu M, Lan L, et al. Altered periaqueductal gray resting state functional connectivity in migraine and the modulation effect of treatment. Sci Rep. 2016;6(1):20298. doi:10.1038/srep20298
24. Hafsi K, McKay J, Li J, et al. Nutritional, metabolic and genetic considerations to optimise regenerative medicine outcome for knee osteoarthritis. J Clin Orthop Trauma. 2019;10(1):2–8. doi:10.1016/j.jcot.2018.10.004
25. Zhang Z, Huang C, Jiang Q, et al. Guidelines for the diagnosis and treatment of osteoarthritis in China (2019 edition). Ann Transl Med. 2020;8(19):1213.
26. Berman BM, Lao L, Langenberg P, et al. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2004;141(12):901–910. doi:10.7326/0003-4819-141-12-200412210-00006
27. Qiu K, Jing M, Sun R, et al. The status of the quality control in Acupuncture-Neuroimaging Studies. Evid Based Complement Alternat Med. 2016;2016:3685785. doi:10.1155/2016/3685785
28. Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15(12):1833–1840.
29. Roos EM, Roos HP, Lohmander LS, et al. Knee Injury and Osteoarthritis Outcome Score (KOOS)–development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28(2):88–96. doi:10.2519/jospt.1998.28.2.88
30. Guillemin F, Coste J, Pouchot J, et al; French Quality of Life in Rheumatology Group. The AIMS2-SF: a short form of the arthritis impact measurement scales 2. Arthritis Rheum. 1997;40(7):1267–1274. doi:10.1002/1529-0131(199707)40:7<1267::AID-ART11>3.0.CO;2-L
31. Beck AT, Epstein N, Brown G, et al. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037//0022-006x.56.6.893
32. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4(6):561–571. doi:10.1001/archpsyc.1961.01710120031004
33. Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990;13(4):227–236. doi:10.1002/nur.4770130405
34. Kong J, Gollub R, Huang T, et al. Acupuncture de qi, from qualitative history to quantitative measurement. J Altern Complement Med. 2007;13(10):1059–1070. doi:10.1089/acm.2007.0524
35. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
36. Zhang Y, Bao F, Wang Y, et al. Influence of acupuncture in treatment of knee osteoarthritis and cartilage repairing. Am J Transl Res. 2016;8(9):3995–4002.
37. Chen N, Wang J, Mucelli A, et al. Electro-acupuncture is beneficial for knee osteoarthritis: the evidence from meta-analysis of randomized controlled trials. Am J Chin Med. 2017;45(5):965–985. doi:10.1142/S0192415X17500513
38. Zhang S, Ouyang L-Z, Wang X-Z, et al. Effect of acupuncture plus thunder-fire moxibustion on MMP-3, TIMP-1 and TGF-β1 in rats with knee osteoarthritis. J Acupunct Tuina Sci. 2017;15(5):322–327. doi:10.1007/s11726-017-1022-y
39. Mohammed N, Allam H, Elghoroury E, et al. Evaluation of serum beta-endorphin and substance P in knee osteoarthritis patients treated by laser acupuncture. J Complement Integr Med. 2018;15(2). doi:10.1515/jcim-2017-0010
40. Bao F, Sun H, Wu ZH, et al. Effect of acupuncture on expression of matrix metalloproteinase and tissue inhibitor in cartilage of rats with knee osteoarthritis. Zhongguo Zhen Jiu. 2011;31(3):241–246.
41. Otti A, Noll-Hussong M. Acupuncture-induced pain relief and the human brain’s default mode network - an extended view of central effects of acupuncture analgesia. Forsch Komplementmed. 2012;19(4):197–201. doi:10.1159/000341928
42. Cao J, Tu Y, Orr SP, et al. Analgesic effects evoked by real and imagined acupuncture: a Neuroimaging Study. Cereb Cortex. 2019;29(8):3220–3231. doi:10.1093/cercor/bhy190
43. Colombo B, Rocca MA, Messina R, et al. Resting-state fMRI functional connectivity: a new perspective to evaluate pain modulation in migraine? Neurol Sci. 2015;36(Suppl 1):41–45. doi:10.1007/s10072-015-2145-x
44. Cai RL, Shen GM, Wang H, et al. Brain functional connectivity network studies of acupuncture: a systematic review on resting-state fMRI. J Integr Med. 2018;16(1):26–33. doi:10.1016/j.joim.2017.12.002
45. Zou Y, Tang W, Li X, et al. Acupuncture reversible effects on altered default mode network of chronic migraine accompanied with clinical symptom relief. Neural Plast. 2019;2019:5047463. doi:10.1155/2019/5047463
46. Zhao L, Liu J, Zhang F, et al. Effects of long-term acupuncture treatment on resting-state brain activity in migraine patients: a randomized controlled trial on active acupoints and inactive acupoints. PLoS One. 2014;9(6):e99538. doi:10.1371/journal.pone.0099538
47. Zou Q, Yuan BK, Gu H, et al. Detecting static and dynamic differences between eyes-closed and eyes-open resting states using ASL and BOLD fMRI. PLoS One. 2015;10(3):e0121757. doi:10.1371/journal.pone.0121757
48. Yin S, Chen Y, Lei D, et al. Cerebral mechanism of puncturing at He-Mu point combination for functional dyspepsia: study protocol for a randomized controlled parallel trial. Neural Regen Res. 2017;12(5):831–840. doi:10.4103/1673-5374.206655
49. Chen X, Spaeth RB, Freeman SG, et al. The modulation effect of longitudinal acupuncture on resting state functional connectivity in knee osteoarthritis patients. Mol Pain. 2015;11:67. doi:10.1186/s12990-015-0071-9
50. Vaishnavi SN, Vlassenko AG, Rundle MM, et al. Regional aerobic glycolysis in the human brain. Proc Nat Acad Sci. 2010;107(41):17757–17762. doi:10.1073/pnas.1010459107
51. Han L. The rule of acupoints’ selection in acupuncture and moxibustion for knee osteoarthritis in clinic using data mining analysis. Modernization Trad Chin Med Materia Medica. 2016;18(8):1233–1240.
52. Tsukayama H, Yamashita H, Kimura T, et al. Factors that influence the applicability of sham needle in acupuncture trials: two randomized, single-blind, crossover trials with acupuncture-experienced subjects. Clin J Pain. 2006;22(4):346–349. doi:10.1097/01.ajp.0000176359.94644.mL
53. Lund I, Näslund J, Lundeberg T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: a physiologist’s perspective. Chin Med. 2009;4:1. doi:10.1186/1749-8546-4-1
54. Dincer F, Linde K. Sham interventions in randomized clinical trials of acupuncture–a review. Complement Ther Med. 2003;11(4):235–242. doi:10.1016/s0965-2299(03)00124-9
55. SPIRIT. SPIRIT statement, publications and downloads. Available from: https://www.spirit-statement.org/publications-downloads/.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
Effect of Traditional Chinese Non-Pharmacological Therapies on Knee Osteoarthritis: A Narrative Review of Clinical Application and Mechanism
Liu ZF, Zhang Y, Liu J, Wang YY, Chen M, Liu EY, Guo JM, Wang YH, Weng ZW, Liu CX, Yu CH, Wang XY
Orthopedic Research and Reviews 2024, 16:21-33
Published Date: 26 January 2024
Exploring the Analgesic Effect of Acupuncture on Knee Osteoarthritis Based on MLT/cAMP/PKA/CREB Signaling Pathway
Zhang C, Yu M, Zhang L, Zhou X, Han J, Fu B, Xue H, Zhang C
Journal of Inflammation Research 2025, 18:237-249
Published Date: 7 January 2025
Therapeutic Potential of Acupuncture in Knee Osteoarthritis: Clinical Efficacy and Mechanistic Insights
Yao K, Shamim MF, Xia J, Liu TT, Guo Y, Lin X
Journal of Inflammation Research 2025, 18:12169-12190
Published Date: 5 September 2025
Evaluating the Effect of Electroacupuncture in Knee Osteoarthritis: Protocol for a Multicenter Randomized Controlled Trial
Chen Y, Xie H, Ye M, Zhang L, Yuan A
Journal of Pain Research 2026, 19:606479
Published Date: 16 April 2026