Back to Journals » International Journal of Women's Health » Volume 18
Effect of Acupuncture for Diminished Ovarian Reserve: A Randomized Sham-Controlled Trial
Authors Wang X ![]() , Du P, Yang L, Li J, Hang T, Qi L
, Du P, Yang L, Li J, Hang T, Qi L ![]() , Su C, Liu X, Li W, Zhu Y, Lu G, Xu H, Fang Y
, Su C, Liu X, Li W, Zhu Y, Lu G, Xu H, Fang Y
Received 11 November 2025
Accepted for publication 12 February 2026
Published 8 April 2026 Volume 2026:18 580821
DOI https://doi.org/10.2147/IJWH.S580821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Xiaoyan Wang,1 Pengfei Du,1 Li Yang,1,2 Jiashan Li,1,2 Tian Hang,1,2 Lingyu Qi,1,2 Chenchen Su,1 Xin Liu,1 Weixin Li,1 Yaoyao Zhu,1 Ge Lu,1 Huanfang Xu,1,2 Yigong Fang1,2
1Institute of Acupuncture and Moxibustion, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 2Acupuncture and Moxibustion Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Huanfang Xu, Email [email protected] Yigong Fang, Email [email protected]
Objective: Acupuncture is a potential intervention for diminished ovarian reserve (DOR); however, the evidence remains limited. This single-center, randomized, sham-acupuncture controlled trial was conducted to evaluate the efficacy and safety of acupuncture in treating DOR.
Methods: A total of 120 DOR patients aged 18– 40 years were randomized to receive acupuncture or sham acupuncture. The treatment lasted 12 weeks, with 20-minute sessions three times weekly, followed by a 12-week follow-up. The primary outcome was the change in antral follicle count (AFC) from baseline to week 12. Secondary outcomes included serum levels of anti-Müllerian hormone (AMH), follicle-stimulating hormone (FSH), luteinizing hormone (LH), estradiol (E2), menstrual cycle length, and self-rating anxiety scale (SAS) scores.
Results: Of the participants, 108 completed the study. Both acupuncture and sham acupuncture interventions exhibited statistically significant increases in AFC at weeks 12 and 24 versus baseline. The acupuncture group had significantly higher AFC values compared to sham controls at both evaluation timepoints. At week 12, the acupuncture group showed a significantly greater increase in AFC (median [IQR], 2.00 [0 to 4.00]) compared to the sham group (0 [0 to 0.25]), with a between-group pseudo-median difference of 1.00 (95% CI, 0 to 2.00; p=0.003). By week 24, although improvements in AFC persisted, between-group differences became non-significant. Both groups demonstrated increases in AMH and decreases in FSH at weeks 12 and 24 compared to baseline, though between group comparisons revealed no statistically significant differences. There were no significant differences between groups in E2, LH, and menstrual cycle length. A statistically significant between-group difference in SAS was noted exclusively at week 24. Treatment related adverse events were mild and infrequent.
Conclusion: A 12-week of acupuncture significantly improved AFC in women with DOR compared to sham acupuncture. Further large-scale studies are warranted to confirm these findings and assess long-term outcomes.
Keywords: acupuncture, diminished ovarian reserve, randomized controlled trial, sham acupuncture, antral follicle count
Introduction
The function of the ovary is intricately linked to the number and quality of oocytes, both of which decline with age and do not regenerate in number. The concept of ovarian reserve (OR), which encompasses both the quality and quantity of available primordial follicles, has traditionally been used to describe a woman’s reproductive potential.1 However, according to a recent committee opinion by American Society for Reproductive Medicine,2 the focus of OR has shifted primarily to the quantity of oocytes. This shift is due to the limited utility of commonly used OR markers in predicting oocyte quality, specifically the potential of a fertilized oocyte to result in a live birth.2 Diminished ovarian reserve (DOR) refers to women of reproductive age who exhibit abnormal OR test results, such as elevated-but-not-menopausal basal follicle stimulating hormone (FSH) levels, low anti-Müllerian hormone (AMH) levels and reduced antral follicle count (AFC).3 Approximately 10% of the general female population may experience DOR, leading to fertility decline in their mid-30s and early menopause by age 45.4 The prevalence of DOR increases with age, exceeding 50% in women over 40.5 Contemporary women are increasingly delaying pregnancy until later or even advanced ages for various reasons, making DOR a significant global reproductive challenge.
Multiple factors contribute to the development of DOR, including advanced age, genetic predisposition, endocrine disturbances, metabolic alterations, iatrogenic causes such as ovarian surgery, autoimmune or inflammatory conditions, certain medical treatments, environmental exposures, and psychological stress.6,7 Nevertheless, the exact pathogenesis of DOR remains incompletely understood, and there is currently no established therapy to effectively restore ovarian reserve. Women with DOR are often advised to undergo controlled ovarian hyperstimulation (COH) or in vitro fertilization (IVF)-embryo transfer (ET) based on their individual conditions to achieve pregnancy. However, they often respond poorly to ovarian stimulation or fecundity compared with women of comparable age,4 with clinical pregnancy rates generally below 40%.8 Extensive evidence indicates that DOR is associated with lower rates of euploid blastocyst, pregnancy and live birth,9,10 as well as higher rates of cycle cancellation and poor ovarian response,11 despite significant advancements in IVF technology. Improving OR remains acritical unmet need in reproductive medicine.
Acupuncture, an external therapy rooted in traditional Chinese medicine (TCM), has been used for centuries in China to treat menstrual disorders and infertility. In recent years, it has garnered increasing attention worldwide for its potential to improve IVF outcomes, particularly through its effects on improving OR. Acupuncture may improve ovarian reserve through a multi-targeted approach that involves: regulating the hypothalamic-pituitary-ovarian axis;12 mitigating oxidative stress and inflammatory responses in ovarian tissue;13 and influencing the balance of apoptosis-related proteins (eg, Bcl-2/Bax) to reduce follicular degeneration.14 A scoping review highlighted that studies focusing on DOR patients using acupuncture were few and generally of low quality.15 A recently published systematic review, which included only 13 randomized controlled trials (RCTs) with high heterogeneity, concluded that acupuncture may potentially improve sex hormones and increase AFC in DOR patients.16 The review also emphasized the need for more rigorous and well-designed trials globally. Therefore, this single-center, randomized, sham controlled trial was conducted to evaluate the efficacy and safety of acupuncture in treating DOR.
Methods
Study Design
This single center, randomized, sham controlled trial was approved by the ethics committees of the Institute of Acupuncture and Moxibustion of China Academy of Chinese Medical Sciences (SC2017-12-22-1-1). The protocol was registered in Chinese Clinical Trial Registry (No. ChiCTR1800014988) and published previously.17 The trial adhered to the guidelines of the Declaration of Helsinki. The study was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent after receiving a comprehensive briefing on the detailed trial information.
Participants
Women with DOR were recruited via hospital posters, WeChat, or online advertisements. Women aged 18–40 years, having low OR indicators defined as a serum level of AMH < 1.1 ng/mL, AFC < 5–7 and a basal serum level of FSH between 10 and 20 IU/L, and willing to undergo acupuncture were invited to participate in the study.
Participants were excluded if they had any of the following conditions: polycystic ovary syndrome, hyperprolactinemia, hyperandrogenemia, hypothyroidism, and other endocrine diseases affecting ovulation; iatrogenic DOR caused by pelvic surgeries, radiotherapy, chemotherapy, uterine artery embolization, immunosuppressants, etc; hormone therapy within the past three months, including estrogen, contraceptives, glucocorticoids, etc; severe anxiety with a score of self-rating anxiety scale (SAS) >70; or severe cardiovascular, cerebral, liver or kidney diseases, cancer, or psychiatric disease.
Randomization and Blinding
Eligible participants were randomly assigned to receive either acupuncture or sham acupuncture in a 1:1 ratio. The randomization sequence was computer-generated by an independent statistician using a blocked randomization design with concealed block sizes. This sequence was implemented via a central randomization system to ensure allocation concealment. Due to the nature of the intervention, the acupuncturists administering the treatment were not blinded to the group assignment. However, participants, outcome assessors, and data statisticians were blinded throughout the trial. To assess the success of blinding, participants were asked to guess their group assignment (acupuncture, sham acupuncture, or uncertain) at the end of the treatment period (Week 12) using a standardized questionnaire.
Interventions
In this trial, the intervention was administered by three acupuncturists, each having over 5 years of clinical practice in treating gynecological diseases using acupuncture. Prior to the trial, a comprehensive training session on acupuncture protocols and standard operating procedures was conducted.
The acupuncture group utilized disposable sterile acupuncture needles (Hwato brand, Suzhou Medical Appliance, Jiangsu, China), including sizes 0.25×25 mm, size 0.25×40 mm, and size 0.30×75 mm. The treatment protocol involved two distinct sets of acupoints, which were used alternately across sessions. Specifically, one set was applied with the patient in a supine position (Group 1), and the other set was applied in a prone position (Group 2). The two sets were alternated session by session throughout the 12-week intervention period. Group 1 acupoints encompassed GV20 (Baihui), GV24 (Shenting), GB13 (Benshen), CV12 (Zhongwan), ST25 (Tianshu), CV4 (Guanyuan), KI12 (Dahe), EX-CA1 (Zigong), SP6 (Sanyinjiao), and LR3 (Taichong). Acupoints of group 2 consisted of BL23 (Shenshu), BL33 (Zhongliao), and KI3 (Taixi). All acupoints were located based on the WHO Standard Acupuncture Point Locations in the Western Pacific Region.18 GV20, GV24, and GB13 were needled transversely to a depth of 10–20 mm. LR3 was needled towards KI1 (yongquan) for 10–20 mm. BL33 was needled obliquely downward into the third posterior sacral foramina for 50–60 mm. The remaining acupoints were perpendicularly needled for 30–40 mm. Following needle insertion, small and even lifting, thrusting, and twisting manipulations were performed to achieve deqi (a composite sensation of soreness, numbness, distension, heaviness, etc), which is considered crucial for ensuring the therapeutic effectiveness of acupuncture. For group 2 acupoints, electroacupuncture (EA) was applied to ipsilateral BL23 and BL33 acupoints using a dense-disperse wave with current intensity adjusted to a tolerable range of 1–5 mA adjusted to patient comfort. Acupuncture was delivered for 20 minutes per session, three times weekly for 12 weeks, followed by a 12-week follow-up period.
In the sham acupuncture group, the same two sets of acupoints were superficially needled to a depth of 1–3 mm without any needle manipulation or induction of deqi sensation. EA was applied to the same acupoints using an identical waveform configuration, but with a substantially reduced current intensity (<0.5 mA) that failed to elicit visible muscular fasciculations around the needles. The duration and frequency of the sham acupuncture were consistent with those of the true acupuncture sessions.
Outcome Measures
The primary outcome was the change from baseline in AFC at week 12. AFC is defined as the number of follicles measuring 2–10 mm in diameter in both ovaries, assessed by a single sonographer via transvaginal ultrasound on days 2–5 of the menstrual cycle.
Secondary outcomes included changes from baseline in AFC at week 24, basal serum levels of FSH, luteinizing hormone (LH) and estradiol (E2) measured on days 2–4 of the menstrual cycle, serum AMH level, menstrual cycle length and SAS scores at weeks 12 and 24.
Adverse events (AEs) were documented throughout the trial. Based on their potential association with the acupuncture needling procedure, AEs were categorized by acupuncturists and related specialists as treatment-related or non-treatment-related within 24 hours of occurrence.
Statistical Analysis
This study aimed to demonstrate the difference between acupuncture and sham acupuncture in improving AFC. Based on our previous pilot study,19 a 12-week acupuncture increased AFC by 2.25 follicles from baseline, while patients on the waiting list showed an increase of only 0.30 follicles from baseline. There is a lack of data on AFC changes with superficial needling for DOR. In this study, it was estimated that sham acupuncture would increase AFC by 0.80 follicles from baseline. A sample size of 50 participants per group was calculated to achieve 90% power at a two-sided significance level of 5%, assuming a standard deviation of 2.22. Considering a dropout rate of 20%, a total of 120 participants (60 per group) were required.
The statistical analysis was based on the modified intention-to-treat principle, with all randomized subjects who received at least one treatment included in the analysis. Missing data was imputed using multiple imputation. Continuous variables were presented as means and standard deviations or medians with interquartile ranges, as appropriate. The Mann–Whitney U-test was used to assess differences between groups, while the sign test was used to assess the change from baseline to weeks 12 or 24 within each group. Categorical variables were presented as frequencies and percentages and compared using either the chi-square test or Fisher’s exact test. A P value of <0.05 was considered statistically significant. All analyses were performed by a statistician blinded to group assignment using IBM SPSS statistics 27.
Results
Patient Characteristics
From March 5, 2018, to December 18, 2022, a total of 347 women with DOR were screened for eligibility. Of these, 120 women were enrolled in the study, and 108 completed the trial (Figure 1). Specifically, five women in the acupuncture group and seven in the sham acupuncture group withdrew from the study. Two women assigned to sham acupuncture did not receive treatment. Consequently, 60 women in the acupuncture group and 58 women in the sham acupuncture group were included in the statistical analysis. Baseline characteristics such as age, body mass index (BMI), age at menarche, menstrual cycle length, obstetric history, AFC, serum levels of AMH, FSH, LH and E2, and SAS scores were comparable between groups (Table 1).
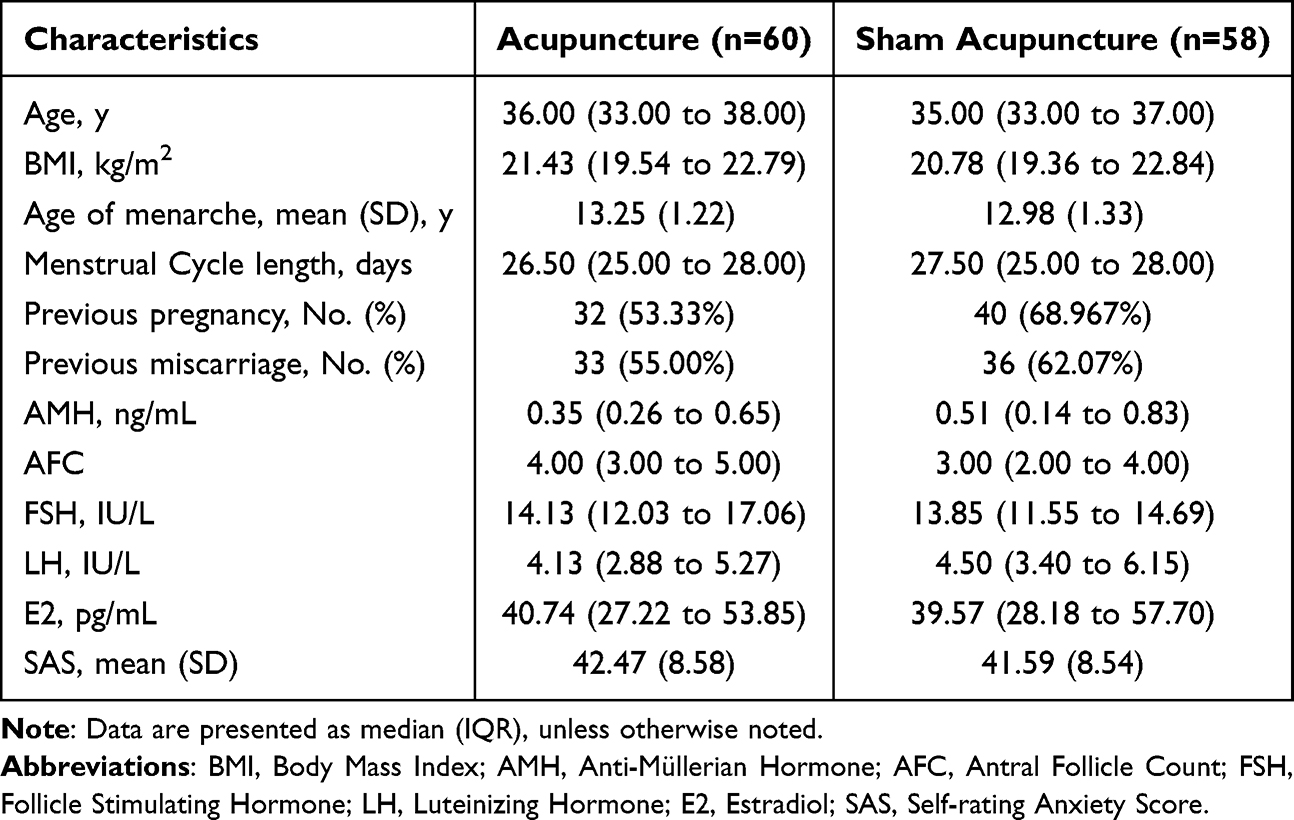 |
Table 1 Baseline Characteristics |
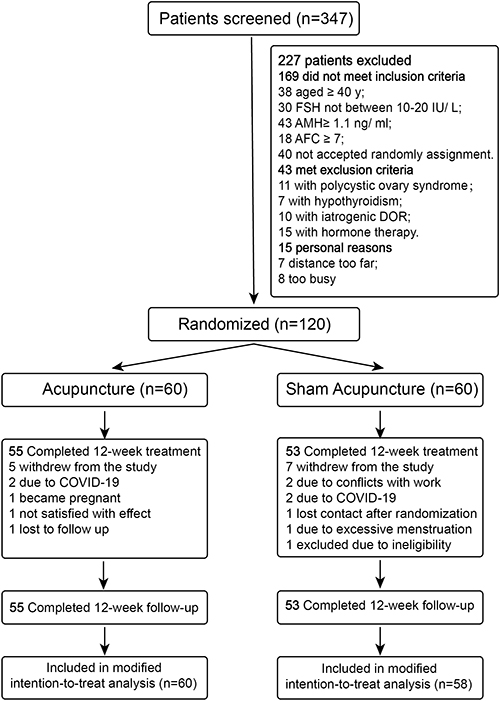 |
Figure 1 Study flow chart. |
Change of AFC
The acupuncture group showed median (interquartile range, IQR) AFC of 4.00 (3.00–5.00) at baseline, 6.00 (4.00–8.00) at week 12, and 5.00 (4.00–7.75) at week 24. Corresponding values in the sham acupuncture group were 3.00 (2.00–4.00), 4.00 (2.75–5.25), and 4.00 (3.00–6.00) at these time points. Both acupuncture and sham acupuncture interventions exhibited statistically significant increases in AFC compared to baseline at weeks 12 and 24. The acupuncture group exhibited superior efficacy, with significantly higher AFC values than the sham acupuncture group at both time points. Notably, from baseline to week 12, the acupuncture group demonstrated a greater increase in AFC (2 [0 to 4.00]) compared to the sham acupuncture group (0 [0 to 0.25]), with a between group pseudo-median difference of 1.00 (95% CI, 0 to 2.00; p=0.003). However, the increases of AFC from baseline to week 24 were comparable between groups (Table 2).
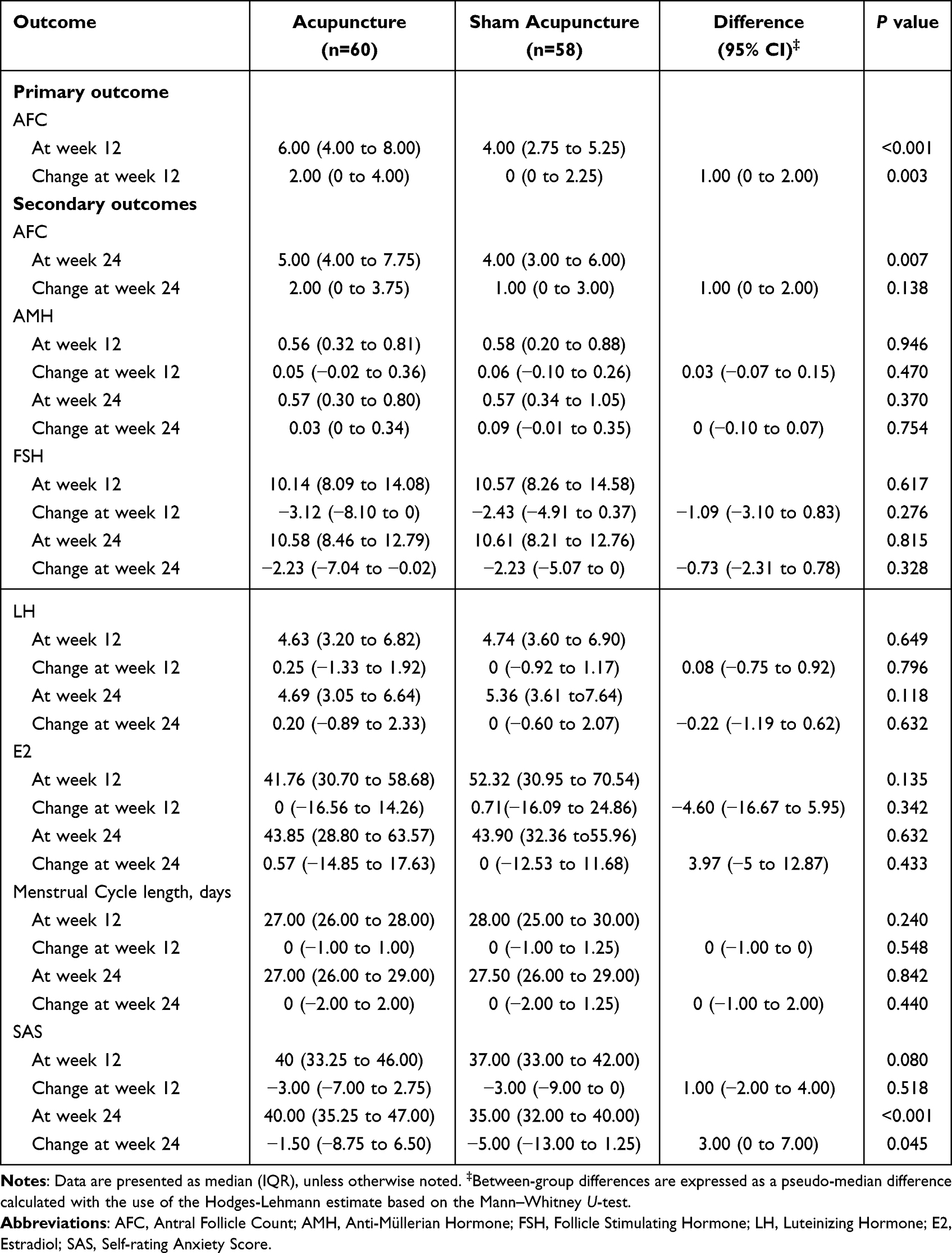 |
Table 2 Primary and Secondary Outcomes |
Secondary Outcomes
Both groups demonstrated increases in AMH and decreases in FSH at weeks 12 and 24 compared to baseline, though between-group differences were non-significant. E2 levels showed no statistically significant intra- or intergroup variations across all time points (Table 2). LH levels followed a similar pattern to E2, with non-significant changes observed in the acupuncture group at weeks 12 and 24, and in the sham acupuncture group at week 12. While sham acupuncture exhibited a statistically significant intra-group change in LH levels at week 24, between-group comparisons showed no significant differences (Table 2). Significant reductions in SAS scores were observed at week 12 in both groups and at week 24 in the sham acupuncture group compared to baseline. However, a statistically significant between-group difference was observed only at week 24 (Table 2).
Safety
Throughout the trial, no serious adverse event (AE) was reported. There were two reports of subcutaneous hemorrhage and two of needling pain in the acupuncture group, and one report of subcutaneous hemorrhage in the sham acupuncture group. All AEs were mild and recovered naturally without special medical intervention (Table 3).
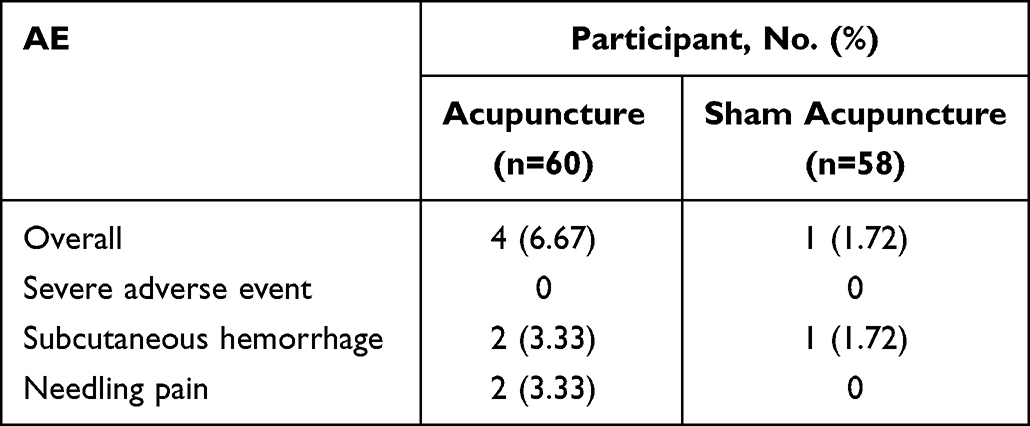 |
Table 3 Adverse Events |
Discussion
This single-center, sham controlled, randomized study indicated that a 12-week acupuncture treatment significantly increased AFC in women with DOR. Although AMH and FSH did not differ significantly between groups, both groups showed statistically significant improvements from baseline.
It is noteworthy that there is no ideal single measure of OR. Commonly used indicators include AMH, AFC, FSH and age. Age is considered the best surrogate marker for oocyte quality. Younger women with DOR may still have normal oocyte quality despite reduced oocyte numbers, whereas older women with DOR typically exhibit an age-appropriate decline in oocyte quality, even if their oocyte number is normal. AFC and AMH reliably reflect the quantity of the remaining follicles, whereas basal FSH is less reliable due to variability between reproductive cycles. These three tests are closely associated with the ovarian response during controlled ovarian stimulation, but not predictive of failure to conceive.
In this trial, AFC served as primary outcome, and a pseudo-median difference of 1.00 (0 to 2.00) follicle was observed between groups. The improvement of AFC in this trial was consistent with results of the systematic review13 and a previous transcutaneous electrical acupoint stimulation (TEAS) study,19 which reported that after over 3 menstrual cycles of TEAS treatment, the mean AFC increased by 1.5 (SD 0.87) follicles. Additionally, our follow-up results indicated that the improvement in AFC from baseline persisted throughout the 12-week follow-up period, although the between group differences were no longer significant.
In our study, the improvement in AMH and FSH from baseline has not yet demonstrated a between-group difference, similar to the effect of EA at acupoints of liver meridian.20 The previous TEAS study reported a more notable improvement in AMH, yet with considerable variation.21 Taking into account the results of this study, previous literature, and our clinical experience, there is still a lack of compelling evidence that acupuncture can improve AMH level. Serum FSH levels seemed to drop by about 3 IU/L from baseline after acupuncture, as observed in both our study and previous studies.20,21 An observational study of EA reported a larger drop in FSH from 19.33 at baseline to 10.58 at week 12 and 11.25 at week 24.22 However, although these differences maybe statistically significant, the minimal clinically important difference (MCID) for these OR indicators remains unknown, limiting the accurate interpretation of the study results.
Consistent with previous studies,23 our investigation into the effects of acupuncture on E2 and LH levels revealed no significant differences either before and after treatment or between groups. Notably, the menstrual cycle length was within normal ranges for most DOR patients, as reflected in our data, which accounts for the negative findings regarding menstrual cycle length in this study. These results challenge the routine use of E2, LH levels, and menstrual cycle length as outcome measures in clinical studies of DOR. SAS is widely employed to assess anxiety in DOR patients, yet studies have yielded conflicting findings. Our study detected no statistically significant group differences in SAS scores between acupuncture and sham acupuncture interventions, while a more substantial SAS reduction was documented with acupuncture when compared to medication therapy.20
There are limited acupuncture studies specifically targeting the DOR population. A scoping review revealed that the majority of acupuncture studies on DOR had been conducted in China, comprising 98% of the studies published between 2010 and 2022.12 Overall, research on acupuncture for DOR remains in its early stages. From initial observational studies to more recent RCTs, the methodologies used in clinical research on acupuncture for DOR have progressively improved in terms of acupuncture protocols, control methods, outcome settings and interpretations. This study represents the first comparison of acupuncture versus sham acupuncture in treating DOR. The acupuncture protocol used in this study is grounded in our team’s extensive clinical experience spanning over a decade. According to TCM principles regarding the pathogenesis of DOR, the selected acupoints aim to tonify the kidney, regulate the Chong and Ren meridians, and calm the mind. Additionally, the nerve segmental effect plays a critical role in influencing the effect of acupoints. In this study, most of the acupoints in the abdomen and lumbosacral region are located within the same or similar nerve segments as those innervating the ovaries. The most typical example is the deep needling at BL23 into the third posterior sacral foramina for stimulating the related sacral nerves. Our results validated the benefit of acupuncture on AFC and add to the clinical evidence that acupuncture is a potential treatment for DOR.
This study has some limitations. Methodologically, acupuncturists were not blinded, and the success of subject blinding was not formally assessed, though the use of superficial needling in this trial likely better preserves blinding compared to non-penetrating placebo acupuncture. Regarding outcome measures, the absence of established MCIDs for ovarian reserve outcomes introduced some ambiguity in interpreting the results, while the lack of pregnancy outcomes, due to the short follow-up period and inability to offer IVF support, may limit the clinical significance of this study. Finally, the generalizability of our results may be restricted by the single-center design and the technical expertise required for the deep needling technique at BL33.
Conclusion
Among women with DOR, a 12-week acupuncture treatment compared with sham acupuncture resulted in significant improvement in AFC. Further large-scale studies are needed to validate the efficacy of acupuncture on ovarian reserve and to determine its impact on pregnancy outcomes among women with DOR undergoing IVF.
Data Sharing Statement
Deidentified individual participant data from this study will be made publicly available. The shared dataset includes demographic characteristics, outcome measures, and adverse event records. Researchers wishing to access the data may contact the corresponding authors by Email at [email protected] or [email protected] with a justified request.
Acknowledgment
The authors would like to thank all the participants involved in this study.
Funding
This study was supported by grants from CACMS Innovation Fund (CI2021A03504) and the National Natural Science Foundation of China (NO. 81674087).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril. 2015;103(3):e9–9. doi:10.1016/j.fertnstert.2014.12.093
2. Penzias A, Azziz R, Bendikson K; Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril. 2020;114(6):1151–1157. doi:10.1016/j.fertnstert.2020.09.134
3. Pastore LM, Christianson MS, Stelling J, Kearns WG, Segars JH. Reproductive ovarian testing and the alphabet soup of diagnoses: DOR, POI, POF, POR, and FOR. J Assist Reprod Genet. 2018;35(1):17–23. doi:10.1007/s10815-017-1058-4
4. Tal R, Seifer DB. Ovarian reserve testing: a user’s guide. Am J Obstet Gynecol. 2017;217(2):129–140. doi:10.1016/j.ajog.2017.02.027
5. Dogan S, Cicek O, Demir M, Yalcinkaya L, Sertel E. The effect of growth hormone adjuvant therapy on assisted reproductive technologies outcomes in patients with diminished ovarian reserve or poor ovarian response. J Gynecol Obstet Hum Reprod. 2021;50(2):101982. doi:10.1016/j.jogoh.2020.101982
6. Osman NA, Morgham AE. Update on Assessment of Ovarian Reserve Testing. Obstet Gynecol Surv. 2024;79(7):429–435. doi:10.1097/OGX.0000000000001284
7. Zhu Q, Li Y, Ma J, Ma H, Liang X. Potential factors result in diminished ovarian reserve: a comprehensive review. J Ovarian Res. 2023;16(1):208. doi:10.1186/s13048-023-01296-x
8. Yu R, Jin H, Huang X, Lin J, Wang P. Comparison of modified agonist, mild-stimulation and antagonist protocols for in vitro fertilization in patients with diminished ovarian reserve. J Int Med Res. 2018;46(6):2327–2337. doi:10.1177/0300060518770346
9. Zhu S, Jiang W, Liao X, Sun Y, Chen X, Zheng B. Effect of diminished ovarian reserve on the outcome of fresh embryo transfer in IVF/ICSI cycles among young women: a retrospective cohort study. BMC Womens Health. 2024;24(1):230. doi:10.1186/s12905-024-03039-6
10. Jaswa EG, McCulloch CE, Simbulan R, Cedars MI, Rosen MP. Diminished ovarian reserve is associated with reduced euploid rates via preimplantation genetic testing for aneuploidy independently from age: evidence for concomitant reduction in oocyte quality with quantity. Fertil Steril. 2021;115(4):966–973. doi:10.1016/j.fertnstert.2020.10.051
11. Kawwass JF, Hipp HS, Session DR, Kissin DM, Jamieson DJ; National ART Surveillance System Group. Severity of diminished ovarian reserve and chance of success with assisted reproductive technology. J Reprod Med. 2017;62(3–4):153–160.
12. Zhu Y, Yin Y, Xu H, et al. Effects of acupuncture on the hypothalamic-pituitary-ovarian axis and FSH/cAMP signaling pathway in aged rats. Zhongguo Zhen Jiu. 2025;45(2):200–208. doi:10.13703/j.0255-2930.20240819-k0004
13. Li D, Bai P, Wu JY, et al. Effect of acupuncture on ovary morphology and function in DHEA-induced polycystic ovary syndrome model rats. Chin J Integr Med. 2021;27(3):220–224. doi:10.1007/s11655-021-3290-0
14. Ren J, Chang BY, Cui MJ, Gao Z, Cao YX, Wang HJ. Effect of penetrative needling of “Zhibian” (BL54) through “Shuidao” (ST28) on expression of internal and external apoptosis-related factors in ovarian of mice with poor ovarian response. Zhen Ci Yan Jiu. 2025;50(2):123–130. doi:10.13702/j.1000-0607.20231108
15. Xie Y, Shi W, Tan Y, et al. Acupuncture and moxibustion for diminished ovarian reserve: a scoping review. Complement Ther Med. 2023;77:102973. doi:10.1016/j.ctim.2023.102973
16. Lin G, Liu X, Cong C, Chen S, Xu L. Clinical efficacy of acupuncture for diminished ovarian reserve: a systematic review and meta-analysis of randomized controlled trials. Front Endocrinol. 2023;14:1136121. doi:10.3389/fendo.2023.1136121
17. Xu H, Hao M, Zheng C, et al. Effect of acupuncture for diminished ovarian reserve: study protocol for a randomized controlled trial. Trials. 2021;22(1):720. doi:10.1186/s13063-021-05684-w
18. Lim S. WHO standard acupuncture point locations. Evid Based Complement Alternat Med. 2010;7(2):167–168. doi:10.1093/ecam/nep006
19. Li X, Xu H, Liu B, Yang H, Shang J, Fang Y. “Tiaojing Cuyun” acupuncture therapy in diminished ovarian reserve: a randomized controlled trial. China J Trad Chin Med Pharm. 2018;5:1736–1739.
20. Luo Q, Yang Z, Jin L, et al. Electroacupuncture at acupoints of liver Meridian for diminished ovarian reserve of liver depression: a randomized controlled trial. Zhongguo Zhen Jiu. 2024;44(11):1261–1266. doi:10.13703/j.0255-2930.20230905-k0005
21. Zheng Y, Feng X, Mi H, et al. Effects of transcutaneous electrical acupoint stimulation on ovarian reserve of patients with diminished ovarian reserve in in vitro fertilization and embryo transfer cycles. J Obstet Gynaecol Res. 2015;41(12):1905–1911. doi:10.1111/jog.12810
22. Wang Y, Li Y, Chen R, Cui X, Yu J, Liu Z. Electroacupuncture for reproductive hormone levels in patients with diminished ovarian reserve: a prospective observational study. Acupunct Med. 2016;34(5):386–391. doi:10.1136/acupmed-2015-011014
23. Bai Y, Chen Z, Gong A, et al. Effect of Tiaojing Cuyun acupuncture therapy on pregnancy outcomes in women with diminished ovarian reserve undergoing IVF-ET: a cohort study. Zhongguo Zhen Jiu. 2024;44(6):653–658. doi:10.13703/j.0255-2930.20230716-k0002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Acupuncture on the Cognitive Control Network of Patients with Knee Osteoarthritis: Study Protocol for a Randomized Controlled Trial

Yin S, Zhang ZH, Chang YN, Huang J, Wu ML, Li Q, Qiu JQ, Feng XD, Wu N
Journal of Pain Research 2022, 15:1443-1455
Published Date: 18 May 2022
Evaluating the Efficacy and Underlying Mechanisms of Acupuncture for Chronic Subjective Tinnitus Using Functional Near-Infrared Spectroscopy: Study Protocol for a Randomized Controlled Trial
Hu H, Lin X, Fang L, Li Y, Gao H
Journal of Pain Research 2023, 16:3367-3378
Published Date: 4 October 2023
Clinical Efficacy and Safety of a Modified Moxibustion Therapy for Low Back Pain in Lumbar Disc Herniation: A Two-Center, Randomized, Controlled, Non-Inferiority Trial
Xue K, Wang X, Xiao C, Zhang N, Liu M, Fu J, Cui J
Journal of Pain Research 2024, 17:1853-1865
Published Date: 23 May 2024
A Pilot Study for Effectiveness and Safety of Adjunctive Pharmacopuncture to Acupuncture Treatment for Rotator Cuff Diseases: A Pragmatic Randomized Controlled Trial
Cha HJ, Han CH, Jeon JH, Jeong JK, Jung IC, Yang C, Kang BK, Kim MJ, Choi YE, Kim YI
Journal of Pain Research 2024, 17:2203-2221
Published Date: 24 June 2024
Efficacy of Acupuncture for Pain in Parkinson’s Disease: Study Protocol for a Randomized Controlled Trial
Wu Y, Zhang F, Xiao L, Wang Y, Lin S, Wu S, Liu X, Zhuang L
Journal of Pain Research 2026, 19:622950
Published Date: 29 June 2026