")
Back to Journals » International Journal of General Medicine » Volume 16
The Role of Acupuncture and Its Related Mechanism in Treating Chronic Prostatitis/Chronic Pelvic Pain Syndrome
Authors Wang H , Zhang J, Ma D, Zhao Z
Received 16 May 2023
Accepted for publication 28 July 2023
Published 6 September 2023 Volume 2023:16 Pages 4039—4050
DOI https://doi.org/10.2147/IJGM.S417066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Hao Wang, Jiwei Zhang, Dongyue Ma, Ziwei Zhao
Department of Andrology, Xiyuan Hospital of China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Jiwei Zhang, Department of Andrology, Xiyuan Hospital of China Academy of Chinese Medical Sciences, Beijing, 100091, Email [email protected]
Abstract: Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is one of the most common diseases in urology, and its prevalence has been increasing, causing serious urogenital problems in men. Several targeted oral drug therapies exist to treat the pelvic pain experienced in this disease. However, these therapies may have potential adverse effects, and due to the unique location of the prostate, delivery of medications to the target lesion is difficult. Consequently, many patients seek alternative therapies. Acupuncture is a well-established treatment method in traditional Chinese medicine that can improve CP/CPPS symptoms and reduce pain. However, previous systematic reviews overlooked the significance of the characteristics and mechanisms of acupuncture therapy. This study aimed to summarize the characteristics and benefits of acupuncture therapy for CP/CPPS based on relevant literature and predict and analyze its related mechanisms.
Keywords: acupuncture, chronic prostatitis, chronic pelvic pain syndrome, mechanism, traditional Chinese medicine, pain
Introduction
Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) refers to urologic pain or discomfort in the pelvic region, as defined by the National Institutes of Health (NIH). It primarily presents no urinary tract infection for at least 3 months in a 6-month period.1 CP/CPPS affects approximately 2–15% of adult men of all ages, particularly those in their middle age, and the chronic symptoms usually last up to 6 months or longer.2–4 Chronic pain, the most common symptom of CP/CPPS, is difficult to treat and often affects patients’ daily lives, leading to negative emotions and sexual dysfunction.5,6 Considering the complexity of CP/CPPS, mental issues, stress and previous prostatic infections may be its etiology and risk factors.7,8
The primary goal of CP/CPPS treatment is to alleviate pain and reduce urination symptoms to improve patients’ quality of life.9 However, no unified treatment strategy has been developed.10 Several treatments are available for CP/CPPS, but due to the unique anatomical functional structure of the prostate tissue, many drugs are unable to cross the blood–prostate barrier. The current treatment strategy mainly aims to alleviate clinical symptoms, but its efficacy is not very satisfactory.11 Antibiotics, nonsteroidal anti-inflammatory drugs (NSAIDs), neurotransmitter antagonists, allopurinol, and botanicals can alleviate clinical symptoms and lower the NIH-chronic prostatitis symptom index (NIH-CPSI) score and its associated pain subscore.12 However, these drugs must be taken for an extended period of time and have several adverse effects and a high recurrence rate.13,14 Considering that no established treatment is valid for all patients, the role of acupuncture could enrich the multidisciplinary approach of this condition.
Acupuncture is also a non-oral drug therapy, which is a critical component of traditional Chinese medicine (TCM). And it has been extensively used to treat various pain-related and urological diseases,15,16 with the majority of studies focusing on CP/CPPS.17 Unlike other systematic reviews,18–20 we reviewed previous clinical evidence to analyze factors, such as acupoint selection, needle retention time, and duration of acupuncture therapy, and discussed the characteristics and mechanisms of acupuncture therapy to provide a reference for future treatment of CP/CPPS using acupuncture.
Materials and Methods
Search Strategy
The PubMed, Embase, and Cochrane Library databases were searched for relevant studies (up to October 2022). We also reviewed the reference lists of the studies identified via our search strategy and selected those that seemed relevant based on our keywords. The search was conducted in English. The following search terms were used: acupuncture, acupuncture treatment, electroacupuncture, acupuncture therapy, fire needling, scalp acupuncture, ear acupuncture, prostatitis, chronic pelvic pain syndrome, nonbacterial prostatitis, chronic prostatitis, clinical trial, clinical article, clinical study, controlled study, and randomized controlled trial (Table 1).
 |
Table 1 PubMed Search Strategy |
Inclusion Criteria
- Study types: Clinical trials involving acupuncture for CP/CPPS were included, and the qualified papers were limited to the English language.
- Participants: Patients with CP/CPPS (as defined by the NIH) were included, regardless of their ethnicity, country, and course.
- Intervention types: Common acupuncture (including electroacupuncture, fire needling, scalp acupuncture, and ear acupuncture) alone without other pharmacotherapies and external treatments in the treatment group, regardless of acupoint position, treatment frequency, and course. The establishment of a control group was not required.
- Comparison types: The control group received conventional treatment, medication, placebo acupuncture, sham acupuncture, or no treatment. Or there were no control groups.
- Outcome types: Changes in the total NIH-CPSI score and NIH-CPSI pain domain subscore were recorded as outcomes.
Data Collection and Analysis
Selection of Studies
According to the search strategy, two authors searched for relevant articles and summarized the results. Duplicate studies were eliminated. Some studies were excluded after analyzing the title and abstract. Furthermore, studies that did not meet the inclusion criteria were eliminated after analyzing the full text. Dissenting opinions were submitted to another author for adjudication throughout the whole process (Figure 1).
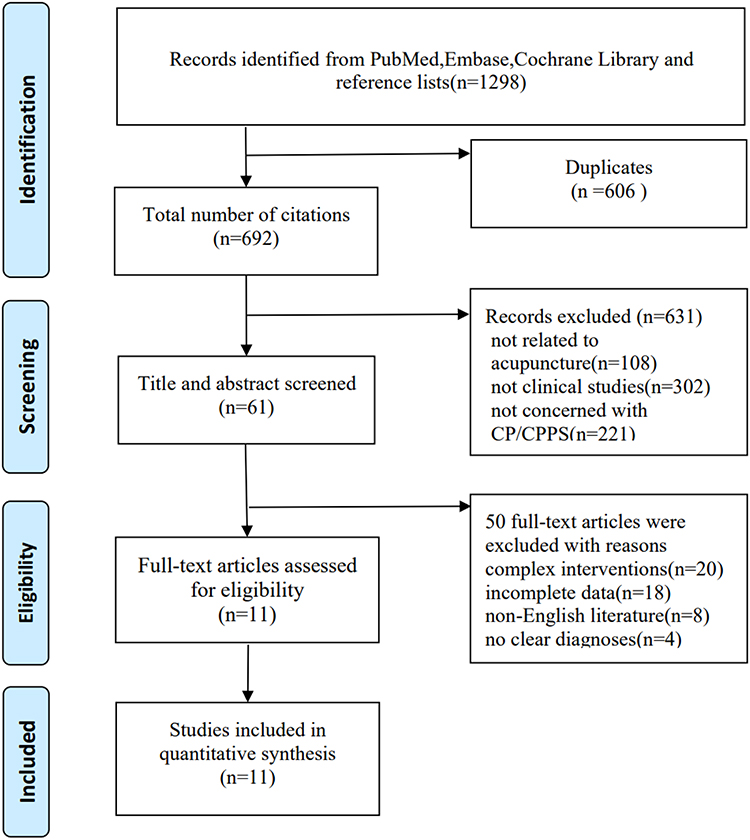 |
Figure 1 Flow chart of the study search. |
Data Extraction
Two authors independently extracted data in a standard format. These data included the author, publication date, number of participants treated with acupuncture or EA, acupuncture points, acupuncture therapy types, session duration, and reported outcomes (Table 2). The two authors checked the extracted data for accuracy and completeness. Another author participated in discussions and helped resolve any disagreements.
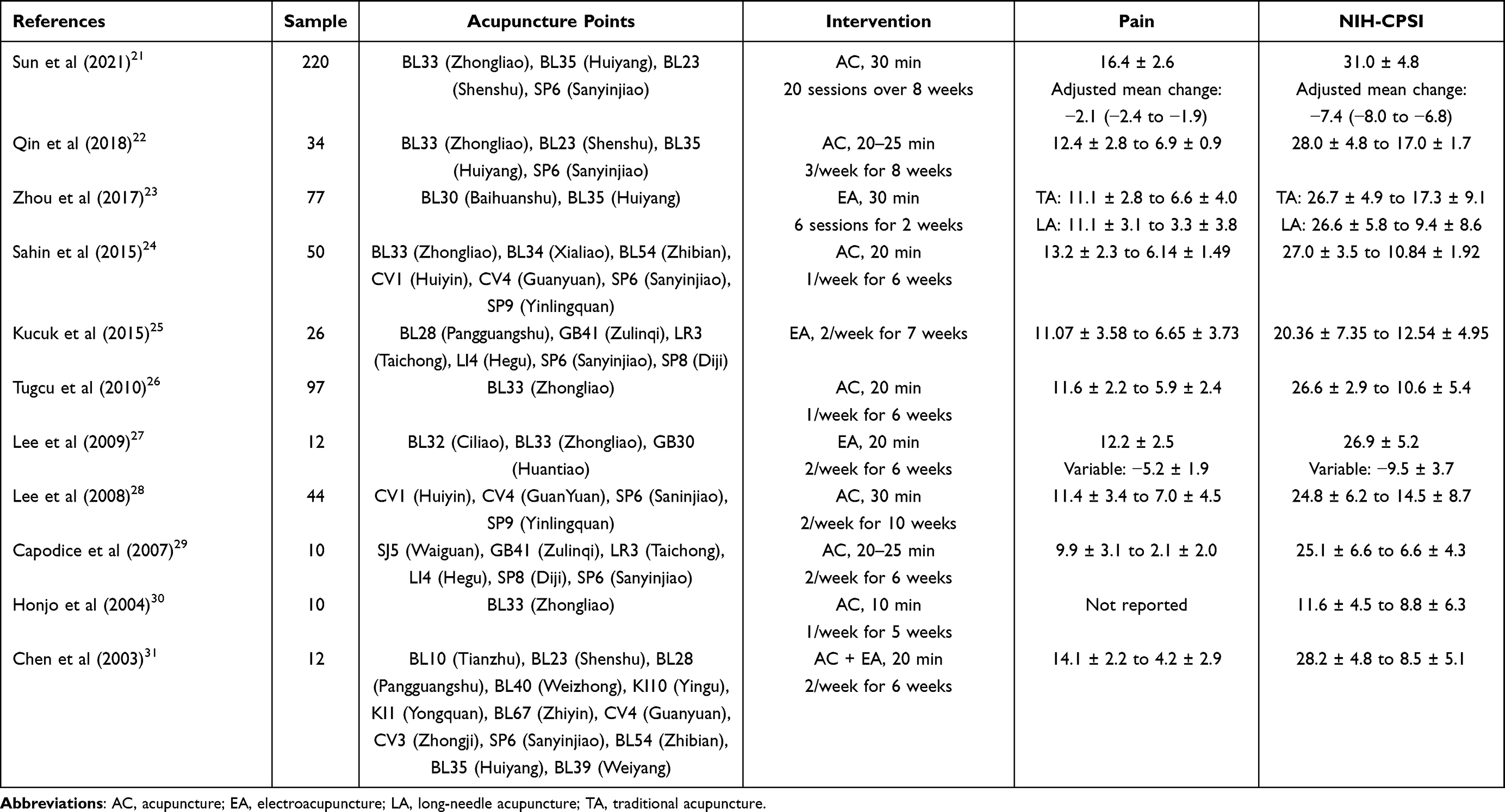 |
Table 2 Summary of the Included Studies |
Results
After duplicates were removed, only 692 of the 1298 searched studies were included in the assessment as shown in the selection flowchart (Figure 1). Following a review of the topics and abstracts, 631 studies were excluded because they were not clinical trials or were unrelated to acupuncture or CP/CPPS. Furthermore, 50 studies were excluded after reading the full text due to complex interventions, incomplete data, non-English language, and unclear diagnosis. Finally, we included 11 English clinical studies involving 570 patients who received acupuncture or EA. Of the 11 studies included, 7 were randomized controlled trials (RCTs)21–25,27,28 and four were before-and-after studies in the same patient.26,29–31
Various acupoint selection methods have been applied in the treatment of CP/CPPS, involving 25 different acupoints and 8 meridians, which include bladder meridian of foot-taiyang, ren meridian, kidney meridian of foot-shaoyin, gallbladder meridian of foot-shaoyang, spleen meridian of foot-taiyin, liver meridian of foot-jueyin, large intestinal meridian of hand-yangming, and triple energizer meridian of hand-shaoyang. Some similarities were observed among acupoint selection studies. Statistical analysis was used to examine the frequency of acupuncture points used in each study (Figure 2). The lumbosacral and lower extremities are the primary targets of acupuncture points. The acupoint meridians were primarily the bladder meridian of foot-taiyang (12/25), ren meridian (3/25), and spleen meridian of foot-taiyin (3/25). SP6 (Sanyinjiao) was the most frequently used acupoint (seven times), followed by BL33 (Zhongliao; six times), BL35 (Huiyang; four times), and BL23 (Shenshu; three times).
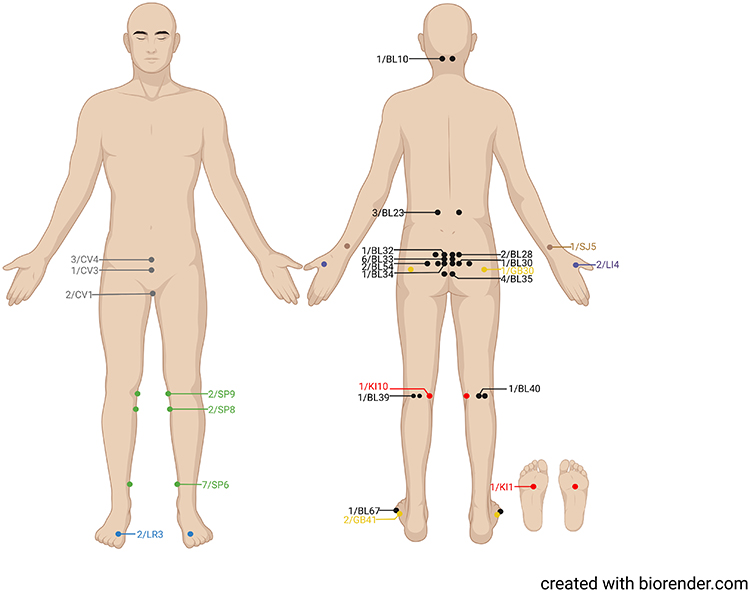 |
Figure 2 The location and distribution of the acupoints. Created with BioRender.com. Notes: The black, gray, red, yellow, green, blue, purple, and brown circles or lines represent the frequency/acupoint of bladder meridian of foot-taiyang, ren meridian, kidney meridian of foot-shaoyin, gallbladder meridian of foot-shaoyang, spleen meridian of foot-taiyin, liver meridian of foot-jueyin, large intestinal meridian of hand-yangming, and triple energizer meridian of hand-shaoyang, respectively. |
Acupuncture was used in seven studies,21,22,24,26,28–30 EA in three studies,23,25,27 and EA combined with acupuncture in one study.31 Except in Kucuk et al’s study,25 which did not specify the duration of each treatment, the duration of each acupuncture session was 10–30 min for 2–10 weeks. Each acupuncture session lasted 20 min in four studies,24,26,27,31 30 min in two studies,23,28 and 20–25 min in another two studies.22,29 Honjo et al30 treated CP/CPPS by giving acupuncture for 10 min per session. The sessions were repeated for 6 weeks in most studies24,26,27,29,31 and for more than 7 weeks in four studies.21,22,25,28 The frequency of the session was two or three times a week in eight studies21–23,25,27–29,31 and once a week in the remaining studies.24,26,30
All studies showed varying degrees of improvement in the NIH-CPSI score and its primarily associated pain subscore. The urinary subscore and quality-of-life subscore are also included in the NIH-CPSI scale. After acupuncture treatment, differences in the changes in NIH-CPSI scores and pain scores were noted across studies (Table 2). Notably, in the same study, the improvement in patients’ NIH-CPSI scores and pain subscores varied at different time points and was represented in four studies. Sun et al21 reported that the adjusted mean change in NIH-CPSI scores was −4.8 (−5.4 to −4.3) at week 4 and that in the pain subscore was −1.6 (−1.8 to −1.3). Qin et al22 reported that the adjusted mean pain subscore was 8.9 (8.2–9.7) at week 4 and the NIH-CPSI total scores at week 4 were also higher than those at week 8. Lee et al27 also assessed the efficacy of acupuncture for CP/CPPS at week 3, and the results showed that the adjusted mean change in NIH-CPSI scores was −7.0 ± 5.1 and that in the pain subscore was −3.7 ± 2.6. Furthermore, according to the findings of Lee et al,28 the mean NIH-CPSI score at week 5 was higher than that at week 10.
We also analyzed the situation in the period after the completion of the treatments. From Sun et al21 and Qin et al,22 the efficacy of acupuncture in reducing NIH-CPSI and pain subscore may persist until week 32. A 22-week follow-up from Zhou et al23 also indicated both traditional acupuncture and long-needle acupuncture can significantly reduce NIH-CPSI and pain subscore (P < 0.05). At week 24 of following-up, success in acupuncture group was 74% in the study of Sahin et al.24 Also, the effect of decreasing NIH-CPSI and pain subscore were also lasting at week 24 in another study.26 These follow-up results all indicated a sustained effect of acupuncture.
Discussion
Characteristics of TCM and Its Use in Treatment
Shoskes et al32 proposed and formulated UPOINT, which is a significant research project following the NIH-CPSI. It classifies prostatitis into six clinical phenotypes: urinary symptoms, psychosocial, organ-specific, infection, neurological/systemic, and skeletal muscle tenderness. Personalized treatment based on UPOINT consists of several steps. In addition to health education, health consultation, reasonable exercise, anxiety reduction, and diet modification, conventional drugs, such as antibiotics and α-blockers, are used to treat CP/CPPS.33 Similar to UPOINT, TCM emphasizes on the holistic concept and syndrome differentiation. Acupuncture, as an important component of TCM, is widely practiced and is recognized and accepted in many countries. The purpose of acupuncture is to alleviate symptoms through a holistic approach. Numerous studies have already shown that acupuncture can effectively improve UPOINT symptoms with few adverse effects. Furthermore, 11 studies in this review reported no serious adverse effects.
Acupoint Location
Meridian and acupoint selection in TCM includes proximal and distal acupoint selection.34 Proximal acupoint selection is a common acupoint selection method, and proximal acupoints include BL30 (Baihuanshu), BL32 (Ciliao), BL33 (Zhongliao), BL34 (Xialiao), BL35 (Huiyang), and BL54 (Zhibian). These acupoints are concentrated in the lumbosacral region and are the most commonly used acupoints in this review (Figure 2). Acupuncture at BL32 (Ciliao) and BL33 (Zhongliao), which are located in the second and third posterior sacral foramina, respectively, and BL34 (Xialiao) and BL54 (Zhibian), which are located in the third and fourth posterior sacral foramen, respectively, can stimulate the sacral nerve segments and relieve pain via direct inhibition at the spinal cord level.24 In particular, transsphenoidal sacral nerve stimulation has a beneficial effect on chronic refractory pelvic pain.27 BL30 (Baihuanshu) and BL35 (Huiyang) are located near the pudendal nerve, which is the main sensory and motor nerve of the perineum, providing genital sensation as well as controlling the urethral sphincter and anal sphincter. In patients with CP/CPPS, acupuncture at these two acupoints stimulates the pudendal nerve, inhibits local sensory transmission to the central nervous system, and reduces pain symptoms.23 In distal acupoint selection, acupoints far from the lesion site are selected. This selection method reflects the meridian theory of TCM. In this review, BL10 (Tianzhu), BL39 (Weiyang), BL40 (Weizhong), and BL67 (Zhiyin) were all on the bladder meridian of foot-taiyang, whereas SP8 (Diji), SP9 (Yinlingquan), and SP6 (Sanyinjiao), which are distributed below the knee joint, were all on the spleen meridian of foot-taiyin. Based on the meridian theory of TCM, the circulation of the bladder meridian of foot-taiyang and the spleen meridian of foot-taiyin passes through the lower abdomen or lumbar spine.
Retention Time
Each treatment in our study lasted for 10–30 min. The acupuncture effect is divided into three stages: the best induction period, half-life period, and residual effect period. A prolonged retention time is unfavorable, and the best induction period should be used.35 Acupuncture analgesia has different optimal times for different diseases, and the analgesic effect of acupuncture gradually reaches saturation as the acupuncture analgesia time extends.36 Acupuncture analgesia requires a 20- to 30-min induction period, after which the analgesic effect of acupuncture gradually weakens, leading to a “tolerance effect”.37 CP/CPPS is characterized by localized pelvic pain.38 Liu et al39 observed that needling the Shiqizhui acupoint for 30 min was more effective than holding the needle for 20 min for relieving pain in patients with primary dysmenorrhea. However, due to the lack of research, the precise duration of needle retention for pain relief remains unknown. To achieve the best therapeutic effect of CP/CPPS, we need to comprehensively analyze the patient’s personal condition, including pain severity, age, physical condition, and post-treatment response, to determine the best retention time of acupuncture.40
Course of Treatment
Currently, the dose–response relationship between acupuncture sessions and CP/CPPS outcomes remains unclear, and clinical guidelines for acupuncture do not specify minimum sessions in clinical practice. Four studies21,22,27,28 found that the longer the acupuncture session, the more effective it is in lowering NIH-CPSI scores and pain subscores. Zhang et al41 searched for RCTs that compared the efficacy of acupuncture with that of sham acupuncture or standard medication on CP/CPPS and determined the optimal acupuncture session to achieve clinical efficacy. In the included experiment, the results revealed a dose–response relationship between acupuncture frequency and the therapeutic effect in the case of 6–28 sessions of acupuncture. The overall trend showed that the more acupuncture treatments received, the lower the NIH-CPSI score. According to Zhang et al,41 four sessions are the minimum “dose” required to achieve clinical efficacy. Therefore, short-term acupuncture treatment may be adequate and effective in some cases, particularly for acute pain. Zhang et al41 also suggested that acupuncture treatment sessions be extended in cases of refractory CP/CPPS to achieve the best results. Another study by Qin et al42 included 10 studies involving 329 participants and found a J-shaped dose–response relationship between acupuncture sessions and the NIH-CPSI score. The NIH-CPSI score decreased from 26.1 (95% CI: 25.3–27.0) to 18.5 (95% CI: 11.6–25.4) after six acupuncture sessions, with a between-session difference of −7.6 (95% CI: −14.6 to −0.7). Considering the 95% CI, both robust-error meta-regression modeling (MD: −8.3 [95% CI: −10.4 to −6.3]) and sensitivity analysis without case series studies (MD: −8.1 [95% CI: −9.5 to −6.7]) demonstrated that the NIH-CPSI score clinically improved after 18 sessions.
Needing Depth
The clinical effect is primarily influenced by the depth of the acupuncture needle. Zhou et al23 investigated the therapeutic effect of LA on CP/CPPS. In the LA group, the long needle (0.4 × 100 mm) was inserted perpendicularly at BL30 (Baihuanshu) and BL35 (Huiyang) at a depth of 75–90 mm (3–3.5 cun). In the TA group, the same acupoints as those in the LA group were used and a traditional needle (0.3 × 40 mm) was inserted at a depth of 25–35 mm. Both LA and TA reduced the NIH-CPSI scores and pain subscores, but LA had a higher clinical efficacy score. Despite the fact that both shallow and deep punctures are effective in most pain cases, comparative studies on the relationship between acupuncture depth and effect in chronic pelvic pain are lacking. Some studies with large sample sizes have also tentatively shown that the efficacy of deep puncture is similar to that of shallow puncture, although their disease focus was not CP/CPPS.43,44 The CP/CPPS acupoints are mostly concentrated in the lumbosacral and buttocks regions (Figure 2). Zhou et al23 also selected acupoints from these areas. However, it is yet to be determined whether these muscle mass areas are better for treating CP/CPPS.
Evaluation of the Efficacy of TCM
Patients with CP/CPPS not only experience localized pain symptoms, discomfort, and lower-urinary-tract symptoms but also psychological symptoms, insomnia, fatigue, poor appetite, low back pain, and other manifestations, all of which can interfere with recovery. Evaluating the curative effect solely on the basis of the NIH-CPSI score, international prostate symptom score, and other western evaluation standards may be insufficient. In China and other countries, where acupuncture is popular, researchers are evaluating the efficacy of acupuncture based on the improvement of other concomitant symptoms in patients with CP/CPPS patients, except the pain, to prove the efficacy of acupuncture.
Possible Mechanisms
Acupuncture may reduce pain symptoms by modulating the associated neurotransmitters. The final stage of CP/CPPS may be a neuropathic pain syndrome characterized by chronic pain, recurrent inflammation, voiding disorders, and sexual dysfunction. The pain syndrome can be neurogenically mediated by upregulating the local pelvic/perineal afferent sensory neuronal system and winding it up within the spinal cord and central nervous system, including endogenous opioid system regulation and gating control theories.45 The pain-relieving efficacy of acupuncture can be attributed to a complex phenomenon involving numerous neuropeptides and neurotransmitters.46 Activation of primary sensory neurons induces the release of inflammatory neuropeptides, such as substance P (SP), which can exacerbate inflammatory cell accumulation. Meanwhile, inflammation and enhanced oxidative stress may activate cyclooxygenase-2 (COX-2), which induces the production of prostaglandin E2 (PGE2) and inhibits the release of β-endorphin (β-EP) secreted by immune cells, resulting in and maintaining CP/CPPS pain symptoms. To alleviate CP/CPPS pain, it is necessary to inhibit PGE2 release while promoting EP accumulation. Acupuncture increases the concentration of β-EP in the cerebrospinal fluid, even in patients with CP/CPPS, as reported by Lee et al47 Ma et al48 also found that acupuncture burial therapy was better than oral tamsulosin hydrochloride in raising plasma β-EP levels and lowering SP levels in patients with CPPS. Furthermore, acupuncture points in the lumbosacral region and below the umbilicus, such as BL33 (Zhongliao), CV4 (Guanyuan), and CV3 (Zhongji), may cause minor damage to local tissues, allowing endorphins, such as β-EP, and their receptors to accumulate locally for a certain period of time. This phenomenon explains the possible peripheral opioid analgesic effect induced by acupuncture treatment. According to the neurotransmitter theory, acupuncture may also stimulate the release of neurotransmitters, such as serotonin and norepinephrine, as well as regulate dopamine and 5-hydroxytryptamine. However, these mechanisms overlap in some ways, and more experimental data are required to confirm the mechanisms of their roles in the acupuncture treatment of CP/CPPS.47,49
Acupuncture may regulate the effects of inflammatory factors in patients or models with CP/CPPS. COX-2, a key mediator of inflammation, can contribute to the inflammatory response by producing PGE2, which causes local pain and vasodilation. Men with symptomatic CP/CPPS have higher PGE2 concentrations in the prostatic fluid than asymptomatic controls,50 implying that the pain in CP/CPPS may be caused by increased prostaglandin production. Hence, methods that lower prostaglandin PGE2 or COX-2 levels within the prostate would be beneficial to men with CP/CPPS. EA therapy is said to be anti-inflammatory because it regulates the expression of proinflammatory cytokines and COX-2 in peripheral and central nociceptive sites.51,52 Lee et al27 collected postmassage urine samples and found that the PGE2 levels in the EA group decreased significantly. Furthermore, Jiang et al53 used a rat model of neuropathic pain to investigate the role of PGE2 in EA analgesia. After 7 days of intervention, the expression level of the spinal PGE2 was significantly higher in the model group than in the control group, but it was reversed by EA (P < 0.01 and P < 0.05). Therefore, EA on neuropathic pain might alleviate the hyperalgesia state by inhibiting the local secretion of PGE2. Furthermore, interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α) are two important proinflammatory cytokines that may play a role in the development of CP/CPPS.54 Alexander et al55 observed increased levels of TNF-α and IL-1β in the seminal plasma of patients with CP. Nadler et al56 also reported that TNF-α and IL-1β levels were significantly higher in the prostatic fluid of patients with CP/CPPS than in the prostatic fluid of healthy controls and that a correlation existed between these cytokines. Furthermore, acupuncture has been shown to have an effect on inflammatory mediators in patients with CP/CPPS, with TNF-α and IL-1β expression levels being significantly reduced.50,57
Acupuncture may modulate immune responses in patients or models with CP/CPPS. Immune mechanisms, particularly autoreactive T lymphocytes, may play a role in the development of CP/CPPS.58,59 T lymphocytes are divided into subsets; CD4+ T cells are helper T lymphocytes that help B lymphocytes produce antibodies and help other T lymphocyte subsets, whereas CD8+ T cells are suppressor and killer T lymphocytes that inhibit lymphocytes from producing antibodies and suppress other lymphocytes.60 Natural killer (NK) cells secrete cytokines essential for mediating immune responses; thus, high levels of NK cells may be required in preventing CP/CPPS and other chronic inflammatory conditions.61,62 It may also exert positive effects through the production of helper T cell factors associated with disease remission. Quick et al63 reported that CD4+ T cells play a role in the development of pelvic pain in mice. Ye et al64 compared serum immunoglobulin G (IgG) and CD8+ levels in 23 patients with CP/CPPS and 26 healthy people and found that patients with CP/CPPS had lower serum CD8+ levels and higher serum IgG levels than healthy people. Liu et al65 investigated the effect of EA on the cellular immune function of rats with chronic nonbacterial prostatitis; results showed that the EA group had significantly higher CD4+ plasma levels and a higher CD4+/CD8+ ratio (P < 0.01 and P < 0.05), but the difference in CD8+ plasma levels was not statistically significant (P > 0.05). Yu et al66 demonstrated that 30 min of EA stimulation in ST36 (Zusanli) once a day for 3 days significantly increased splenic NK cell activity in mice. In a clinical study, Lee et al67 compared the effects of acupuncture and sham acupuncture on cellular immunity in 12 patients with CP/CPPS. The results showed that 8 (67%) of the participants (four in each group) were classified as treatment responders, and the NK cell level increased by 5% in the acupuncture group compared with that in the sham group (−13%; P = 0.03).
Limitations
In strict accordance with the search strategy of our review, we included 11 English language studies. Because of language barriers, some studies in other languages were excluded. Our study is also limited by a small sample size and poor evidence quality. The purpose of this review was to analyze the usefulness of acupuncture in patients with CP/CPPS from TCM and western medicine perspectives as well as discuss the mechanisms involved. Although the 11 studies mentioned above have consistently demonstrated that acupuncture is effective in lowering NIH-CPSI scores and relieving local pain in patients with CP/CPPS, the underlying mechanisms remain unclear.
Conclusion
This review provides potential evidence and trends for future research to assist clinicians in treating patients with CP/CPPS through acupuncture. According to TCM, the location, retention time, treatment duration, and needling depth affect the efficacy of acupuncture. Based on our findings, we believe that acupoints in the lumbosacral region and bilateral lower extremities are more suitable for the treatment of CP/CPPS during clinical operation, and the locations of these acupoints are mostly located in the bladder meridian of foot-taiyang, ren meridian, and spleen meridian of foot-taiyin, such as those of BL33 (Zhongliao), CV4 (Guanyuan), and SP6 (Sanyinjiao). We also recommend setting the duration of acupuncture treatment for this condition at 20–30 minutes for each session, with at least four sessions. The mechanism of acupuncture for CP/CPPS is mostly attributed to neuromodulatory, immunomodulatory, and anti-inflammatory functions. We suggest that future studies should focus on the application of acupoints, as well as a more standard design in terms of the course, retention time, and frequency. And ultimately, a clinical protocol for the treatment of CP/CPPS with acupuncture will be developed. On this basis, the further validation of the mechanism in acupuncture for CP/CPPS is still necessary.
Data Sharing Statement
Data supporting this article are all in this article.
Acknowledgments
The authors would like to thank Xulu Lei, Ming Zhao, Qinghe Gao and Jun Guo for their contribution of grammatical guidance, revision and background information regarding. Also, the authors would like to thank https://www.biorender.com to assist us in creating our Figure 2.
Funding
This work was financed by Beijing Traditional Chinese Medicine Science and Technology Development Fund (QN-2020-07) and Qihuang Scholars Support Project of National Traditional Chinese Medicine Inheritance and Innovation (020450008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rees J, Abrahams M, Doble A, Cooper A. Diagnosis and treatment of chronic bacterial prostatitis and chronic prostatitis/chronic pelvic pain syndrome: a consensus guideline. BJU Int. 2015;116(4):509–525. doi:10.1111/bju.13101
2. Suskind AM, Berry SH, Ewing BA, Elliott MN, Suttorp MJ, Clemens JQ. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: results of the RAND Interstitial Cystitis Epidemiology male study. J Urol. 2013;189(1):141–145. doi:10.1016/j.juro.2012.08.088
3. Krieger JN, Riley DE, Cheah PY, Liong ML, Yuen KH. Epidemiology of prostatitis: new evidence for a world-wide problem. World J Urol. 2003;21(2):70–74. doi:10.1007/s00345-003-0329-0
4. Liang CZ, Li HJ, Wang ZP, et al. The prevalence of prostatitis-like symptoms in China. J Urol. 2009;182(2):558–563. doi:10.1016/j.juro.2009.04.011
5. Ge S, Hu Q, Guo Y, Xu K, Xia G, Sun C. Potential alterations of functional connectivity analysis in the patients with chronic prostatitis/chronic pelvic pain syndrome. Neural Plast. 2021;2021:6690414. doi:10.1155/2021/6690414
6. Evans-Durán B, Tripp DA, Campbell J, Doiron RC, Nickel JC. Chronic prostatitis/chronic pelvic pain syndrome-related pain symptoms and their impact on sexual functioning. Can Urol Assoc J. 2022;16(6):222–227. doi:10.5489/cuaj.7607
7. Crocetto F, Barone B, De Luca L, Creta M. Granulomatous prostatitis: a challenging differential diagnosis to take into consideration. Future Oncol. 2020;16(13):805–806. doi:10.2217/fon-2020-0185
8. Barone B, De Luca L, Napolitano L, et al. Lower urinary tract symptoms and mental health during COVID-19 pandemic. Arch Ital Urol Androl. 2022;94(1):46–50. doi:10.4081/aiua.2022.1.46
9. Mändar R, Korrovits P, Rahu K, et al. Dramatically deteriorated quality of life in men with prostatitis-like symptoms. Andrology. 2020;8(1):101–109. doi:10.1111/andr.12647
10. Pirola GM, Verdacchi T, Rosadi S, Annino F, De Angelis M. Chronic prostatitis: current treatment options. Res Rep Urol. 2019;11:165–174. doi:10.2147/RRU.S194679
11. Khattak AS, Raison N, Hawazie A, Khan A, Brunckhorst O, Ahmed K. Contemporary management of chronic prostatitis. Cureus. 2021;13(12):e20243. doi:10.7759/cureus.20243
12. Hu M, Wazir J, Ullah R, et al. Phytotherapy and physical therapy in the management of chronic prostatitis-chronic pelvic pain syndrome. Int Urol Nephrol. 2019;51(7):1081–1088. doi:10.1007/s11255-019-02161-x
13. Yellepeddi VK, Radhakrishnan J, Radhakrishnan R. Penetration and pharmacokinetics of non-steroidal anti-inflammatory drugs in rat prostate tissue. Prostate. 2018;78(2):80–85. doi:10.1002/pros.23447
14. Gaspar A, Silva J, Silva G, et al. Nonablative transurethral erbium: YAG laser treatment for chronic prostatitis/chronic pelvic pain syndrome: a prospective comparative study. Neurourol Urodyn. 2021;40(1):278–285. doi:10.1002/nau.24551
15. Wang H, Zhao M, Zhang J, Yan B, Gao Q, Guo J. Traditional Chinese medicine regulates inflammatory factors in chronic prostatitis/chronic pelvic pain syndrome: a review. Integr Med Nephrol Androl. 2023;10:e00001. doi:10.1097/IMNA-D-22-00001
16. Wang H, Lei X. Acupuncture for women with overactive bladder: perspective of traditional Chinese medicine and related mechanism. Int J Gen Med. 2023;16:1137–1148. doi:10.2147/IJGM.S406194
17. Wazir J, Ullah R, Li S, et al. Efficacy of acupuncture in the treatment of chronic prostatitis-chronic pelvic pain syndrome: a review of the literature. Int Urol Nephrol. 2019;51(12):2093–2106. doi:10.1007/s11255-019-02267-2
18. Chang SC, Hsu CH, Hsu CK, Yang SS, Chang SJ. The efficacy of acupuncture in managing patients with chronic prostatitis/chronic pelvic pain syndrome: a systemic review and meta-analysis. Neurourol Urodyn. 2017;36(2):474–481. doi:10.1002/nau.22958
19. Posadzki P, Zhang J, Lee MS, Ernst E. Acupuncture for chronic nonbacterial prostatitis/chronic pelvic pain syndrome: a systematic review. J Androl. 2012;33(1):15–21. doi:10.2164/jandrol.111.013235
20. Li J, Dong L, Yan X, et al. Is acupuncture another good choice for physicians in the treatment of chronic prostatitis/chronic pelvic pain syndrome? Review of the Latest Literature. Pain Res Manag. 2020;2020:5921038.
21. Sun Y, Liu Y, Liu B, et al. Efficacy of acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a randomized trial. Ann Intern Med. 2021;174(10):1357–1366. doi:10.7326/M21-1814
22. Qin Z, Zang Z, Zhou K, et al. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a randomized, sham acupuncture controlled trial. J Urol. 2018;200(4):815–822. doi:10.1016/j.juro.2018.05.001
23. Zhou M, Yang M, Chen L, et al. The effectiveness of long-needle acupuncture at acupoints BL30 and BL35 for CP/CPPS: a randomized controlled pilot study. BMC Complement Altern Med. 2017;17(1):263. doi:10.1186/s12906-017-1768-2
24. Sahin S, Bicer M, Eren GA, et al. Acupuncture relieves symptoms in chronic prostatitis/chronic pelvic pain syndrome: a randomized, sham-controlled trial. Prostate Cancer Prostatic Dis. 2015;18(3):249–254. doi:10.1038/pcan.2015.13
25. Küçük EV, Suçeken FY, Bindayı A, Boylu U, Onol FF, Gümüş E. Effectiveness of acupuncture on chronic prostatitis-chronic pelvic pain syndrome category IIIB patients: a prospective, randomized, nonblinded, clinical trial. Urology. 2015;85(3):636–640. doi:10.1016/j.urology.2014.11.004
26. Tugcu V, Tas S, Eren G, Bedirhan B, Karadag S, Tasci A. Effectiveness of acupuncture in patients with category IIIB chronic pelvic pain syndrome: a report of 97 patients. Pain Med. 2010;11(4):518–523. doi:10.1111/j.1526-4637.2009.00794.x
27. Lee SH, Lee BC. Electroacupuncture relieves pain in men with chronic prostatitis/chronic pelvic pain syndrome: three-arm randomized trial. Urology. 2009;73(5):1036–1041. doi:10.1016/j.urology.2008.10.047
28. Lee SW, Liong ML, Yuen KH, et al. Acupuncture versus sham acupuncture for chronic prostatitis/chronic pelvic pain. Am J Med. 2008;121(1):79.e71–77. doi:10.1016/j.amjmed.2007.07.033
29. Capodice JL, Jin Z, Bemis DL, et al. A pilot study on acupuncture for lower urinary tract symptoms related to chronic prostatitis/chronic pelvic pain. Chin Med. 2007;2(1):1. doi:10.1186/1749-8546-2-1
30. Honjo H, Kamoi K, Naya Y, et al. Effects of acupuncture for chronic pelvic pain syndrome with intrapelvic venous congestion: preliminary results. Int J Urol. 2004;11(8):607–612. doi:10.1111/j.1442-2042.2004.00868.x
31. Chen R, Nickel JC. Acupuncture ameliorates symptoms in men with chronic prostatitis/chronic pelvic pain syndrome. Urology. 2003;61(6):1156–1159; discussion 1159. doi:10.1016/S0090-4295(03)00141-9
32. Shoskes DA, Nickel JC, Rackley RR, Pontari MA. Clinical phenotyping in chronic prostatitis/chronic pelvic pain syndrome and interstitial cystitis: a management strategy for urologic chronic pelvic pain syndromes. Prostate Cancer Prostatic Dis. 2009;12(2):177–183. doi:10.1038/pcan.2008.42
33. Naveed M, Changxing L, Ihsan AU, et al. Therapeutic interventions to urologic chronic pelvic pain syndrome and UPOINT system for clinical phenotyping: how far are we? Urologia. 2022;89(3):315–328. doi:10.1177/03915603211065301
34. Wang GJ, Ayati MH, Zhang WB. Meridian studies in China: a systematic review. J Acupunct Meridian Stud. 2010;3(1):1–9. doi:10.1016/S2005-2901(10)60001-5
35. Han MJ, Zhao H, Jing XH, et al. Literature analysis of influence of different needle-retaining duration on acupuncture efficacy. Zhong yi za zhi. 2017;58(4):334–339.
36. Wang C, Xiang AF, Chen MY, Liu S. Research progress on the immediate effect of acupuncture analgesia and related influencing factors. Shanghai J Acupunct Moxibustion. 2022;41(2):203–207.
37. Lin LL, Wang LQ, Yang JW, et al. 针刺时效关系研究进展 [Researches status on time-effect of acupuncture]. Zhongguo Zhen Jiu. 2019;39(5):565–570. Chinese. doi:10.13703/j.0255-2930.2019.05.029
38. Chen L, Zhang M, Liang C. Chronic prostatitis and pelvic pain syndrome: another autoimmune disease? Arch Immunol Ther Exp. 2021;69(1):24. doi:10.1007/s00005-021-00628-3
39. Liu C, Ma Y, Guo Z, Gong C. Real-time analgesic effect of acupuncture at Shiqizhui (EX-B8) for primary dysmenorrhea with different needle-retaining time. Shanghai J Acupunct Moxibustion. 2014;33(10):901–902.
40. Huang XY, Li J, Gu K, et al. 留针时间初探 [Discussion on the duration of needle retention]. Zhongguo Zhen Jiu. 2019;39(4):445–450. Chinese. doi:10.13703/j.0255-2930.2019.04.027
41. Zhang W, Fang Y, Shi M, Zhang M, Chen Y, Zhou T. Optimal acupoint and session of acupuncture for patients with chronic prostatitis/chronic pelvic pain syndrome: a meta-analysis. Transl Androl Urol. 2021;10(1):143–153. doi:10.21037/tau-20-913
42. Qin Z, Wu J, Xu C, et al. Long-term effects of acupuncture for chronic prostatitis/chronic pelvic pain syndrome: systematic review and single-arm meta-analyses. Ann Transl Med. 2019;7(6):113. doi:10.21037/atm.2018.06.44
43. Diener H-C, Kronfeld K, Boewing G, et al. Efficacy of acupuncture for the prophylaxis of migraine: a multicentre randomised controlled clinical trial. Lancet Neurol. 2006;5(4):310–316. doi:10.1016/S1474-4422(06)70382-9
44. Linde K, Streng A, Jürgens S, et al. Acupuncture for patients with migraine: a randomized controlled trial. JAMA. 2005;293(17):2118–2125. doi:10.1001/jama.293.17.2118
45. Chen RC, Nickel JC. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome. Curr Urol Rep. 2004;5(4):305–308. doi:10.1007/s11934-004-0057-z
46. Cabýoglu MT, Ergene N, Tan U. The mechanism of acupuncture and clinical applications. Int J Neurosci. 2006;116(2):115–125. doi:10.1080/00207450500341472
47. Lee SW, Liong ML, Yuen KH, Leong WS, Khan NK, Krieger JN. Validation of a sham acupuncture procedure in a randomised, controlled clinical trial of chronic pelvic pain treatment. Acupunct Med. 2011;29(1):40–46. doi:10.1136/aim.2010.003137
48. Ma Y, Li X, Li F, Yu W, Wang Z. 穴位埋线治疗男性慢性盆腔疼痛综合征临床研究 [Clinical research of chronic pelvic cavity pain syndrome treated with acupoint catgut embedding therapy]. Zhongguo Zhen Jiu. 2015;35(6):561–566. Chinese.
49. Wu X, Cheng K, Xu C, et al. Mechanism of acupuncture and moxibustion on chronic prostatitis/chronic pelvic pain syndrome: a narrative review of animal studies. Pain Res Manag. 2021;2021:2678242. doi:10.1155/2021/2678242
50. Shahed AR, Shoskes DA. Correlation of beta-endorphin and prostaglandin E2 levels in prostatic fluid of patients with chronic prostatitis with diagnosis and treatment response. J Urol. 2001;166(5):1738–1741. doi:10.1016/S0022-5347(05)65664-9
51. Moon PD, Jeong HJ, Kim SJ, et al. Use of electroacupuncture at ST36 to inhibit anaphylactic and inflammatory reaction in mice. Neuroimmunomodulation. 2007;14(1):24–31. doi:10.1159/000107285
52. Lee JH, Jang KJ, Lee YT, Choi YH, Choi BT. Electroacupuncture inhibits inflammatory edema and hyperalgesia through regulation of cyclooxygenase synthesis in both peripheral and central nociceptive sites. Am J Chin Med. 2006;34(6):981–988. doi:10.1142/S0192415X06004454
53. Jiang H, Yu X, Ren X, Tu Y. Electroacupuncture alters pain-related behaviors and expression of spinal prostaglandin E2 in a rat model of neuropathic pain. J Tradit Chin Med. 2016;36(1):85–91. doi:10.1016/S0254-6272(16)30013-9
54. Pontari MA, Ruggieri MR. Mechanisms in prostatitis/chronic pelvic pain syndrome. J Urol. 2008;179(5 Suppl):S61–S67. doi:10.1016/j.juro.2008.03.139
55. Alexander RB, Ponniah S, Hasday J, Hebel JR. Elevated levels of proinflammatory cytokines in the semen of patients with chronic prostatitis/chronic pelvic pain syndrome. Urology. 1998;52(5):744–749. doi:10.1016/S0090-4295(98)00390-2
56. Nadler RB, Koch AE, Calhoun EA, et al. IL-1beta and TNF-alpha in prostatic secretions are indicators in the evaluation of men with chronic prostatitis. J Urol. 2000;164(1):214–218. doi:10.1016/S0022-5347(05)67497-6
57. Yao M, Wang Q, Pan HL, Xu ZM, Song AQ. 针刺治疗卵巢早衰及对患者细胞因子 [Effect of acupuncture on the expressions of TNF-α and IFN-γ in patients with premature ovarian failure]. Zhongguo Zhen Jiu. 2019;39(11):1181–1184. Chinese. doi:10.13703/j.0255-2930.2019.11.012
58. Öztekin İ, Akdere H, Can N, Aktoz T, Arda E, Turan FN. Therapeutic effects of oligonol, acupuncture, and quantum light therapy in chronic nonbacterial prostatitis. Evid Based Complement Alternat Med. 2015;2015:687196. doi:10.1155/2015/687196
59. Murphy SF, Schaeffer AJ, Thumbikat P. Immune mediators of chronic pelvic pain syndrome. Nat Rev Urol. 2014;11(5):259–269. doi:10.1038/nrurol.2014.63
60. Gadi D, Griffith A, Tyekucheva S, et al. A T cell inflammatory phenotype is associated with autoimmune toxicity of the PI3K inhibitor duvelisib in chronic lymphocytic leukemia. Leukemia. 2022;36(3):723–732. doi:10.1038/s41375-021-01441-9
61. John H, Maake C, Barghorn A, Zbinden R, Hauri D, Joller-Jemelka HI. Immunological alterations in the ejaculate of chronic prostatitis patients: clues for autoimmunity. Andrologia. 2003;35(5):294–299. doi:10.1111/j.1439-0272.2003.tb00860.x
62. Bohn AB, Nederby L, Harbo T, et al. The effect of IgG levels on the number of natural killer cells and their Fc receptors in chronic inflammatory demyelinating polyradiculoneuropathy. Eur J Neurol. 2011;18(6):919–924. doi:10.1111/j.1468-1331.2010.03333.x
63. Quick ML, Wong L, Mukherjee S, Done JD, Schaeffer AJ, Thumbikat P. Th1-Th17 cells contribute to the development of uropathogenic Escherichia coli-induced chronic pelvic pain. PLoS One. 2013;8(4):e60987. doi:10.1371/journal.pone.0060987
64. Ye C, Xiao G, Xu J, et al. Differential expression of immune factor between patients with chronic prostatitis/chronic pelvic pain syndrome and the healthy volunteers. Int Urol Nephrol. 2018;50(3):395–399. doi:10.1007/s11255-017-1763-z
65. Liu AG, Li HZ, Yan XK, et al. 电针“三阴”穴对慢性非细菌性前列腺炎大鼠细胞免疫功能的影响 [Effect of electroacupuncture at “Sanyin” acupoints on cellular immune function in rats with chronic abacterial prostatitis]. Zhen Ci Yan Jiu. 2013;38(3):192–197. Chinese.
66. Yu Y, Kasahara T, Sato T, et al. Role of endogenous interferon-gamma on the enhancement of splenic NK cell activity by electroacupuncture stimulation in mice. J Neuroimmunol. 1998;90(2):176–186. doi:10.1016/S0165-5728(98)00143-X
67. Lee SW, Liong ML, Yuen KH, Krieger JN. Acupuncture and immune function in chronic prostatitis/chronic pelvic pain syndrome: a randomized, controlled study. Complement Ther Med. 2014;22(6):965–969. doi:10.1016/j.ctim.2014.10.010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.