Back to Journals » Journal of Pain Research » Volume 16
Effectiveness and Safety of Radiofrequency Thermocoagulation Treatment Guided by Computed Tomography for Infraorbital Neuralgia Following Failed Conservative Treatment: A Retrospective Study
Authors Sun Z, Liu L, Liu H, Luo F ![]()
Received 29 October 2022
Accepted for publication 7 March 2023
Published 21 March 2023 Volume 2023:16 Pages 1005—1015
DOI https://doi.org/10.2147/JPR.S395420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Krishnan Chakravarthy
Zhe Sun,1,* Lu Liu,1,* Hongbing Liu,2 Fang Luo1,2
1Department of Day Surgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China; 2Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Luo, Department of Pain Management, Beijing Tiantan Hospital, Capital Medical University, No. 119 West Road, South 4th Ring Road, Fengtai District, Beijing, 100070, People’s Republic of China, Tel +86 010 59976664, Fax +86 010 67050177, Email [email protected]
Purpose: To evaluate the effectiveness and safety of CT-guided radiofrequency thermocoagulation (RFT) for the treatment of infraorbital neuralgia following the failure of conservative management.
Patients and Methods: This was a single center, retrospective study which included 196 patients between the ages of 37 to 90 years, who suffered from infraorbital neuralgia, and had undergone CT-guided RFT treatment. The medical records of these patients were retrieved between January 7, 2015 and February 5, 2020, and the patients were followed up for 2 years. Follow-up outcomes included Numerical Rating Scale (NRS) scores, dosage of carbamazepine, time to take effect, status of recurrence and side effects. The effective rate was defined as the percentage of patients with postoperative NRS score reduction of > 50%.
Results: The effective rates were 92.9%, 100%, 100%, 100%, 93.4% and 85.7% on the same day, week 1, month 1, month 6, year 1 and year 2 after RFT, respectively. After RFT, the postoperative NRS scores and dosage of carbamazepine were significantly reduced than those preoperatively (P < 0.05). The median time to take effect was zero day. Twenty-eight patients with recurrence underwent RFT again and achieved complete pain relief. All patients experienced numbness in the infraorbital nerve innervation area and the numbness scores gradually decreased over time.
Conclusion: CT-guided RFT treatment may be an effective and safe technique for pain relief in patients with infraorbital neuralgia following failed results from conservative treatment.
Keywords: infraorbital neuralgia, radiofrequency thermocoagulation, effectiveness, safety, retrospective study
Introduction
Infraorbital nerve is the terminal branch of maxillary nerve, and the largest terminal branch of trigeminal nerve. It enters the orbit via the infraorbital fissure, passes through the infraorbital groove and then through the infraorbital canal. It reaches the face from the infraorbital foramen and innervates the skin and mucosa of the lower eyelid, nasal wing and upper lip.1 Infraorbital neuralgia is an unbearable facial pain, characterized by sudden, severe, paroxysmal, electric shock-like pain in the area of infraorbital nerve distribution.2,3 Infraorbital neuralgia is usually induced or aggravated by basic daily activities such as brushing teeth, washing face and chewing food, and even causes disability in severe cases.4 Currently, there are no reports available on the morbidity of infraorbital neuralgia. Herpes zoster, maxillary sinusitis and trauma have been reported as common factors inducing infraorbital neuralgia,5–7 however, it may also be of idiopathic origin.2 As one of the most excruciating diseases, this severe chronic pain can lead to various psychological disorders such as anxiety and depression, which seriously affects patients’ quality of life.5
Due to lack of relevant researches, there are no systematic guidelines currently available for the treatment of infraorbital neuralgia.4,7–9 Similar to trigeminal neuralgia, the first line of treatment for infraorbital neuralgia is oral drug therapy, which generally includes antiepileptics, analgesics or antidepressants.4 However, in many patients, infraorbital neuralgia cannot be completely relieved by drug therapy alone. These drugs may also have severe side effects such as dizziness and drowsiness in many cases. Patients who respond poorly to oral drug therapy can be supplemented with nerve block, which is another conservative treatment.7 Nerve block using a local anesthetic is the essential diagnostic criteria for infraorbital neuralgia, which can be administered with or without glucocorticoids as an initial interventional treatment option.4,7,9 However, due to the unsatisfactory results from single injection, repeated injections are generally required, which are accompanied by disadvantages such as complications caused by repeated puncture and drug-related risks. Neurodestructive techniques can be utilized for patients with unbearable infraorbital neuralgia, who failed to benefit from conservative treatments.10 Trescot reported that nerve cryoneurablation (intraoral or extraoral) can also be used in these cases.11 However, nerve ablation results in numbness of the innervated area of the infraorbital nerve, causes discomfort and affects the quality of life. Moreover, the short-term remission rate from this technique is high, the duration of pain relief is short and recurrence is also more likely. Furthermore, the injection of neurolytic agents could lead to nerve necrosis, tissue fibrosis, formation of neuroma and other side effects.12 Conventional open procedures such as infraorbital nerve decompression, neurectomy and avulsion are also beneficial.5,6,10,12–15 Although traditional open surgeries are beneficial in patients with failed conservative treatments, they are now rarely performed in clinical practice due to their highly invasive nature.
Previous studies have demonstrated that pulsed radiofrequency (PRF), a percutaneous minimally invasive treatment, is an alternative for patients experiencing ineffective conservative therapy with infraorbital neuralgia.8,16,17 We previously reported that the postoperative effective rates of PRF treatment for infraorbital neuralgia were 69% and 50% at one month and two years, respectively.8 Properly increasing the voltage could further improve short-term efficacy of PRF treatment; however, the effectiveness of treatment remains limited and there was still a significant long-term recurrence rate.16 Jia et al suggested that the postoperative effective rates of 42°C PRF combined with 60°C continuous radiofrequency (CRF) treatment were 95.5% and 72.7% at one month and two years, respectively.17 Although there are no significant adverse effects of PRF treatment for infraorbital neuralgia, their effective rates still need improvement.
Unlike PRF, radiofrequency thermocoagulation (RFT) is a neurodestructive technique. The thermal effect of RFT can result in degeneration and conduction blockade of the targeted nerve, which has been proved to be effective in the treatment of trigeminal neuralgia and other painful diseases.18–21 Moreover, some studies have reported that the efficacy of PRF is less than that of RFT in the treatment of trigeminal neuralgia.22,23 Ren et al suggested that RFT provided long-term pain relief when compared to PRF for neuralgia of supraorbital nerve, which is also a branch of the trigeminal nerve.17 However, there is little literature available on the treatment of infraorbital neuralgia by RFT. This study aims to evaluate the effectiveness and safety of CT-guided RFT in patients with infraorbital neuralgia, following failed conservative management.
Materials and Methods
This retrospective study was approved by the Medical Ethics Committee of Beijing Tiantan Hospital affiliated to Capital Medical University. This study was conducted in compliance with the Declaration of Helsinki. Data included in analysis were all de-identified. This retrospective study involved no more than minimal risk to subjects, and the waiver of consent did not adversely affect the subjects’ welfare and rights. The application for waiver of informed consent for this study was also approved by the Medical Ethics Committee of the study center. Patient informed consent was not required due to the retrospective nature of this study. The medical records of patients with infraorbital neuralgia, who had undergone CT-guided RFT after failed conservative treatment, were reviewed between January 2015 and February 2020.
Study Design and Participants
This was a single center, retrospective study, without a control group, conducted at Beijing Tiantan Hospital, Capital Medical University. Patients who met the following criteria were eligible for study: (1) Age >18 years; (2) Met the diagnostic criteria of 8B 82.0 in the international classification of diseases 11th revision (ICD-11);24 (3) Showed positive response to diagnostic block (1 mL of 2% lidocaine) before RFT treatment;2,7 (4) Failed to achieve pain relief from conservative treatment and previous RFT treatment. The exclusion criteria were as follows: (1) Patients with incomplete medical records; (2) Patients with secondary neuralgia by intra- and extra-cranial lesions, herpes zoster and trauma; (3) Patients with history of invasive treatment such as decompression, neurectomy and avulsion of the infraorbital nerve. A total of 217 patients with infraorbital neuralgia who had failed conservative treatment were reviewed, and the medical records of 196 patients were collected and analyzed based on the inclusion and exclusion criteria.
Procedures
All RFT treatments were conducted by experienced pain physicians. Patients were made to lie down in supine position on the computed tomography (CT) scanner bed. Electrocardiogram (ECG), heart rate (HR), blood pressure (BP), oxygen saturation and respiratory rate (RR) were continuously monitored. Negative plate of Pain Management Generator (PMG-230, Baylis Medical, Inc., Canada) was placed on the back of the patients.
Puncture point was the surface projection point of infraorbital foramen on the affected side, which is located at the intersection of the connecting line between external canthus and midpoint of upper lip and vertical line of pupil. RFT was performed after skin disinfection and local anesthesia with 1% lidocaine at the puncture site. A 10-cm-long insulated RF trocar needle with a 5-mm bare needle tip (PMF-21-100-5, Baylis Medical Inc.) was inserted upward, backward and outward in the direction of the infraorbital foramen, under the guidance of thin-layer CT (2 mm/layer, medical x-ray CT machine, model SOMATOM, SIEMENS Company, Germany). The needle was readjusted until the trocar reached the infraorbital foramen (Figure 1).8 After negative aspiration for blood or air was confirmed, the RF treatment electrode (PMK-21-100, Baylis Medical, Inc.) was inserted into the trocar after the stylet was removed. Parameters of RFT were set in proper order as 60°C, 75s; 65°C, 75s; 70°C, 75s; 75°C, 75s; and 80°C, 75s.25,26 After the effect of infraorbital nerve block disappeared, hypoalgesia of infraorbital nerve indicated that the nerve had been ablated.
 |
Figure 1 Operative procedure of puncturing the infraorbital foramen. (A) Localization for puncture. (B) The tip of the trocar entering the ipsilateral infraorbital foramen as shown in axial CT scan of maxillary sinus.(C) The needle entering the ipsilateral infraorbital foramen as shown in sagittal CT scan of maxillary sinus. (D) The needle entering the ipsilateral infraorbital foramen as shown in 3-D reconstruction of spiral CT. White marks indicate the needle in the infraorbital foramen. |
Data Collection
Preoperative demographic data, intraoperative data and postoperative follow-up data were retrieved from HIS medical record system and routine postoperative follow-up database, which was established to improve the quality of clinical treatment. Preoperative demographic data included gender, age and body mass index (BMI) of patients, affected side, duration of disease, numerical rating scale (NRS) score of pain, history of treatment such as PRF, etc., the preoperative dosage of carbamazepine (milligrams per day) along with comorbidities such as hypertension, diabetes mellitus, coronary heart disease and stroke. The intraoperative data included operation time, vital signs, NRS score immediately after RFT treatment and intraoperative complications or side effects. Routine follow up were performed on the same day (after the effect of local anesthetics gradually subsided before leaving the hospital), week 1, month 1, month 6, year 1, and year 2, postoperatively. Follow-up outcomes were NRS scores, the dosage of carbamazepine and the time of recurrence. The effective rate was defined as the percentage of patients with NRS score reduction of >50% postoperatively, and the effective rate at each follow-up time points were calculated. Time to take effect was defined as the time from RFT treatment to NRS score reduction of >50%. Recurrence was defined as NRS score greater than 50% of that before RFT treatment, without any oral medications. In addition, postoperative side effects such as facial swelling, facial numbness, ecchymosis, hematoma at puncture site, eye injury, blindness or infection were also recorded. The degree of facial numbness was scored as follows:27 0: no numbness; 1: mild numbness (with no significant impact on life); 2: moderate numbness (with some impact on life); and 3: severe numbness (intolerable).
Statistical Analysis
Statistical analyses were performed by IBM SPSS Statistics software (version 26, IBM, Inc., USA). Normally distributed continuous data were expressed as means ± standard deviations (SDs), and non-normally distributed continuous data were expressed as medians and interquartile ranges (IQRs). NRS scores and dosage of carbamazepine at different time points were analyzed by Wilcoxon signed-rank tests. Categorical data were described as frequency and percentage, and were analyzed by Friedman test. Bonferroni correction was used to correct multiple comparisons. P value <0.05 was considered statistically significant.
Results
A total of 217 patients with infraorbital neuralgia who had failed conservative treatment and underwent CT-guided RFT treatment were reviewed between January 2015 and February 2020. Twenty-one patients were excluded based on the exclusion criteria and the medical records of 196 patients were collected and analyzed.
Baseline Characteristic
Preoperative baseline and intraoperative characteristics are summarized in Table 1. Of all the 196 patients, 104 patients (53.1%) were male. The average age was 64.4 ± 10.4 years, and the maximum and the minimum age were 90 and 37 years, respectively. The median course of disease was 4.6 years (IQR, 3.7–5.6 years; range from 2.2 years to 8.5 years), and the mean operation time was 29.1±6.7 minutes. All the patients with infraorbital neuralgia were affected unilaterally, of whom 102 cases (52.0%) were affected on the left-side. All patients had failed to achieve pain relief from conservative management, such as oral drug therapy, nerve block with local anesthetics with or without glucocorticoids, before CT-guided RFT treatment. Sixty-one patients (31.1%) had experienced PRF treatment; however, the therapeutic effect was not ideal or had relapsed. All patients suffered from severe pain, and the median preoperative NRS score was 8 points (IQR, 8–9 points; range from 7 points to 10 points). The median preoperative carbamazepine dosage was 800 mg per day (IQR, 600–800 mg/day; range from 200 mg/day to 1000 mg/day).
 |
Table 1 Patient Characteristics |
NRS Score
The NRS scores of all the patients were 0 immediately after RFT treatment due to the effect of local anesthetics. All patients were tested for hypoalgesia, after the effect of local anesthetics had subsided in the infraorbital innervation area of the affected side, before being discharged. The NRS scores of 182 patients (92.9%) were reduced by more than 50% after RFT treatment compared to the preoperative NRS score on the same day. Postoperative NRS scores did not decrease significantly or decreased by less than 50% of the preoperative score in 12 patients (6.1%), and there were 2 patients (1.0%) with increased NRS scores on the same day after treatment. However, the NRS scores of all patients decreased within one week after treatment. The postoperative NRS scores at each follow-up time points were significantly lower in 168 patients than those preoperatively (P < 0.05) (Figure 2).
 |
Figure 2 Postoperative NRS scores at each follow-up time point. Notes: The postoperative NRS scores of 168 patients who completed the 2-year follow-up were included. *P < 0.05 was considered as statistically significant compared with baseline. |
Dosage of Carbamazepine
Discontinuation cases (rates) of carbamazepine were 20 (10.2%), 71 (36.2%), 119 (60.7%), 193 (98.5%), 181 (98.9%) (after excluding 13 patients with recurrence) and 167 (99.4%) (after excluding 28 patients with recurrence) on the same day, week 1, month 1, month 6, year 1, and year 2 after the RFT treatment, respectively. The postoperative dosage of carbamazepine were significantly reduced than the preoperative dosage in 168 patients (P < 0.05) (Figure 3).
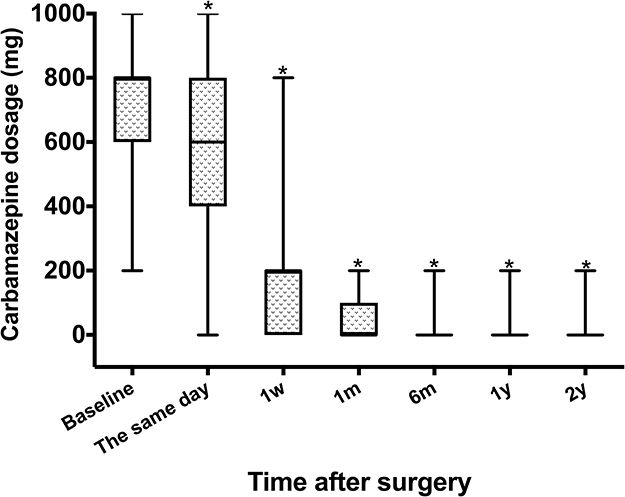 |
Figure 3 Postoperative dosage of carbamazepine at each follow-up time point. Notes: The postoperative dosage of carbamazepine of 168 patients who completed the 2-year follow-up were included. *P < 0.05 was considered as statistically significant compared with baseline. |
Effective Rate
The median time to take effect was 0 day (IQR, 0–1 day; range from 0 day to 7 days) after treatment. The effective cases (rate) were 182 (92.9%), 196 (100%), 196 (100%), 196 (100%), 183 (93.4%) and 168 (85.7%) on the same day, week 1, month 1, month 6, year 1 and year 2 after the RFT treatment, respectively.
A total of 28 patients (14.3%) experienced pain recurrence during the 2-year follow-up, and recurrence time was at 7.8, 8, 9, 9, 9, 10, 10, 10, 11, 11, 11, 12, 13, 13, 15, 15, 16, 16, 17, 17, 18, 19, 20, 20, 21, 22 and 22 months after treatment. Twenty-eight patients with recurrence underwent RFT treatment for the second time, and complete pain relief was achieved in all patients, with no recurrence during the follow-up period.
Side Effects
Vital signs were stable during the operation, and there were no obvious perioperative complications or side effects such as eye injury, blindness and infection. Facial swelling occurred in 20 patients (10.2%). Twelve patients (6.1%) suffered from facial ecchymosis, whereas hematoma at puncture site occurred in 6 patients (3.1%) (Figure 4). These short-term postoperative complications were completely relieved within 2 to 3 weeks.
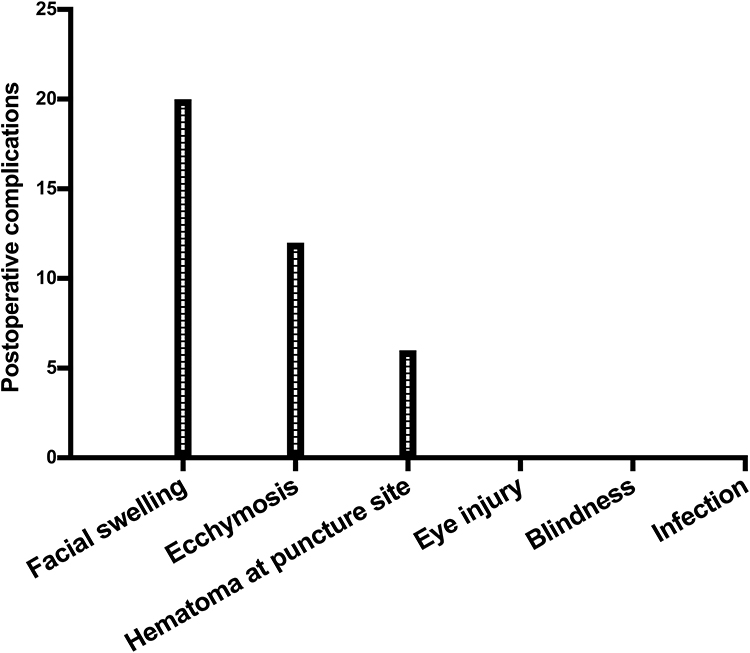 |
Figure 4 Postoperative complications. |
All patients experienced numbness in the infraorbital nerve innervation area after RFT treatment. For facial numbness score, 183 patients completed a one year follow-up (after excluding 13 patients with recurrence), and 168 patients completed a two years follow-up (after excluding 28 patients with recurrence). The numbness scores are shown in Figure 5. Of all the 196 patients, the proportion of patients who had a facial numbness score of 2 or 3 points was 81.6% on the same day after treatment. Numbness scores gradually decreased over time. However, of the 168 patients who completed the 2-year follow-up, only 18 (10.7%) patients complained of facial numbness with scores of 2 or 3 points. Facial numbness score of 168 patients were included in the Friedman test. There were no significant differences in facial numbness scores on the same day, week 1 and month 1 after treatment, respectively. The numbness scores on the aforementioned time points were significantly different from those at month 6, year 1 and year 2 after treatment. Based on the Friedman test, the numbness scores at month 6, year 1 and year 2 after treatment were significantly different.
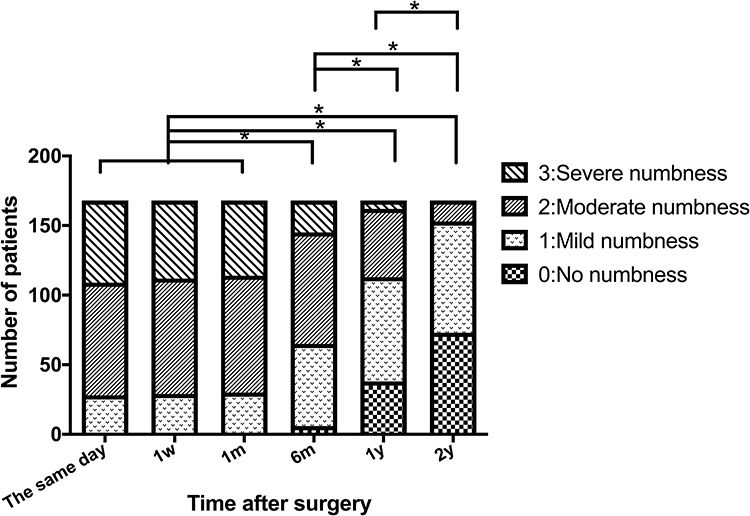 |
Figure 5 Facial numbness score at each follow-up time point. Notes: The facial numbness score of 168 patients who completed the 2-year follow-up were included in the Friedman test. Bonferroni correction was used to correct multiple comparisons. *P < 0.05/15 was considered as statistically significant. |
Discussion
Our study reports the effectiveness and safety of CT-guided RFT treatment in patients with infraorbital neuralgia with failed conservative management, and the results reveal that RFT treatment provides significant pain relief without serious complications. The effective rate was 92.9% on the same day, 100% at week 1, and 85.7% at year 2 after treatment. As a nerve damaging procedure, our study reports a higher effective rate than previous studies, with effective rates of 69% and 50% at month 1 and year 2, respectively, after standard parameter PRF therapy, which is a neuromodulatory procedure for infraorbital neuralgia.8 Similarly, the effective rate of this study is also higher than our previous research about the application of PRF combined with 60°C CRF treatment for infraorbital neuralgia,17 which was 95.5% and 72.7% at month 1 and year 2. Our results are consistent with Wang et al’s study,28 which demonstrates that, once the site of treatment is accurate, RFT provides a higher initial effective rate and long-term pain relief due to its therapeutic mechanism of blocking pain transmission.
In this study, we identified the pain source in advance with diagnostic blockade on all patients at the time of diagnosis. In this study, pain disappeared immediately following RFT procedure due to the effects of local anesthetics in all patients with infraorbital neuralgia, which proves that the accuracy of diagnosis of pain source and the puncture site was correct. Furthermore, all punctures were performed under the guidance of CT in our study, which also ensured the accuracy of puncture. The median time to take effect was 0 day, which was shorter than that in previous studies on neuromodulatory PRF treatments for infraorbital neuralgia,16,17 but was consistent with other studies that had rapid onset after RFT treatment.18,29
However, not all patients had NRS pain scores immediately reduced to zero on the day of the procedure. We found that except for the vast majority of patients (92.9%) who experienced an immediate pain relief with decreased NRS scores, a minority of patients (6.1%) suffered no obvious pain relief for one week after the RFT treatment. Few patients (1.0%) suffered even more severe pain within the first week after the procedure. Some patients had delayed pain relief after surgery, which might be related to direct puncture injury or heat damage to the surrounding tissue. Since all patients in this study had daycare surgeries, our data also provided some clarification to clinicians regarding the postoperative management of such patients after being discharged. Patients who had temporarily inadequate pain relief after operation needed to continue taking the same preoperative oral drug dosage, and had to wait for the RFT effect to take place gradually. However, for very few patients with aggravated postoperative pain, increasing the preoperative oral drug dosage and even incorporating nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids was necessary to achieve adequate analgesic effect.
Along with the decrease in postoperative NRS scores, the dosage of carbamazepine reduced gradually after RFT treatment. However, our results were inconsistent with Jia et al’s study,6 who reported of a one week requirement for drug reduction after combined PRF and 60°C CRF treatment for infraorbital neuralgia, which was longer than that in our study. Our study reports a rapid median onset time of standard RFT treatment. The discontinuation rate of carbamazepine was only 36.2% with an effective rate of 100% at week 1 after treatment, and 60.7% with the median NRS score of 0 point at month 1 after treatment, which might be due to patients’ concern about pain recurrence.
A total of 28 patients (14.3%) experienced pain recurrence within 2 years and all of these patients were willing to receive a second RFT treatment, indicating that the patients were highly satisfied with the operation. Moreover, no patients experienced resistance to second treatment, which was consistent with Gunduz et al’s study, which reported that the repeatability of this intervention was a distinct advantage.30 Xue et al demonstrated that the recurrence was mainly caused by nerve regeneration after RFT treatment.29 Nerve fibers disassemble rapidly in the early stages and neuropathological changes such as axonal regeneration may occur in the nerve. Further studies are needed to explore the ways to reduce the recurrence rate of infraorbital neuralgia following RFT treatment.
The proportion of patients reporting satisfactory pain relief was 92.9% on the same day of RFT treatment, which should be related to the therapeutic mechanism of RFT. As a neuroselective and disruptive technology, RFT treatment plays an important role in ion oscillation in tissue through high-frequency current generated by radiofrequency instrument, which results in local rise in temperature. Conductive tactile neurofibrils (Aα and Aβ-type) can tolerate higher temperatures; therefore, gradual heating can preserve the tactile fibers relatively, and selectively destroy conductive pain neurofibrils (Aδ and C-type).29 Pain relief can be achieved by cutting off the sensory pathway and the sense of touch can be partially or completely preserved.31–33 However, the optimal temperature of RFT treatment has not been confirmed yet.34 The temperature range is between 50°C and 95°C in previous studies.35–38 The higher the temperature within a certain range, the better the treatment effect and the higher the risk of adverse reactions from the RFT treatment.39 In the future, ideal therapeutic parameters of RFT for different painful diseases should be further explored to improve efficacy and reduce side effects.
There were no puncture-related serious adverse effects in our study, precisely because our procedures were performed under CT guidance. Mild swelling and ecchymosis were observed after the procedure, which resolved in a short time. Hematoma at puncture site occurred in some patients due to injury to facial blood vessels during puncture, and recovered spontaneously without treatment. Therefore, the application of RFT is safe in the treatment of infraorbital neuralgia. However, RFT treatment was a destructive procedure and caused numbness, which is consistent with previous studies on RFT treatment for trigeminal neuralgia, supraorbital neuralgia and other painful diseases.18,36,37 Postoperative numbness might be caused by the disconnection of infraorbital nerve. Although the patients suffered from varying degrees of facial numbness, most patients claimed that they would prefer numbness over pain.37,40 We speculated that the reason why facial numbness score decreased over time was because patient’s adaptation to numbness or potential nerve repair. However, a considerable number of patients still suffered from numbness one year after RFT treatment, and the ideal therapeutic parameters for reducing numbness should be further explored in the future.
There were several limitations to our study. First, this was a single-center retrospective study with a relatively small sample size. Multicentric, randomized, controlled studies with a larger sample size must be conducted. Second, our study had a follow-up period of 2 years; long-term effectiveness and safety of CT-guided RFT treatment for patients must be explored. Third, the optimal parameters of RFT treatment such as temperature and duration need to be further studied. Fourth, due to lack of a control group, the conclusion of our study must be acknowledged with caution.
Conclusions
The current study provides preliminary evidence that CT-guided RFT treatment may be an effective and safe pain relief technique for patients with infraorbital neuralgia who failed to achieve pain relief from conservative treatment.
Abbreviations
NRS, numeric rating scales; PRF, pulsed radiofrequency; CRF, continuous radiofrequency; RFT, radiofrequency thermocoagulation; CT, computed tomography; ECG, electrocardiogram; HR, heart rate; BP, blood pressure; RR, respiratory rate; BMI, body mass index; SDs, standard deviations; IQRs, interquartile ranges; NSAIDs, nonsteroidal anti-inflammatory drugs.
Data Sharing Statement
Patient data will not be available because this was not a concern when the study was conducted and the patients were not informed.
Ethics Approval and Informed Consent
Ethics approval was obtained from the Ethics Committee of Beijing Tiantan Hospital, Capital Medical University. The application for a waiver of informed consent for this study was approved.
Consent for Publication
All the authors confirm that the details of any images, videos, recordings, etc. can be published, and the consent has been shown for the article contents to be published. Authors are prepared to provide copies of signed consent forms to the journal editorial office, if requested.
Acknowledgment
We thank the patients who enrolled in this study.
Funding
This research was supported by the Capital’s Funds for Health Improvement and Research (No. 2020-2-2046), the Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (No. XMLX201707) and the Foundation for the Excellent Medical Staff of Beijing (No. 2014-3-035). The funders had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript. The corresponding author had complete access to all the data in the study; all the co-authors were responsible for making the final decision to submit for publication.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kazkayasi M, Ergin A, Ersoy M, Tekdemir I, Elhan A. Microscopic anatomy of the infraorbital canal, nerve, and foramen. Otolaryngol Head Neck Surg. 2003;129:692–697. doi:10.1016/S0194-59980301575-4
2. Lopez Mesonero L, Pedraza Hueso MI, Herrero Velazquez S, Guerrero Peral AL. Infraorbital neuralgia: a diagnostic possibility in patients with zygomatic arch pain. Neurologia. 2014;29:381–382. doi:10.1016/j.nrl.2013.01.003
3. International Association for the Study of Pain. Classification of Chronic Pain. International Association for the Study of Pain; 1994.
4. Min HJ, Kim KS. Infraorbital neuralgia attributed to a foreign body. Headache. 2016;56(3):564–566. doi:10.1111/head.12777
5. Beigi B, Beigi M, Niyadurupola N, Saldana M, El-Hindy N, Gupta D. Infraorbital nerve decompression for infraorbital neuralgia/causalgia following blowout orbital fractures: a case series. Craniomaxillofac Trauma Reconstr. 2017;10(1):22–28. doi:10.1055/s-0036-1592095
6. Agrawal SM, Kambalimath DH. Trigeminal neuralgia involving supraorbital and infraorbital nerves. Natl J Maxillofac Surg. 2010;1:179–182. doi:10.4103/0975-5950.79226
7. de Vries N, Smelt WL. Local anaesthetic block therapy of posttraumatic neuralgia of the infraorbital nerve. Rhinology. 1990;28:103–106.
8. Luo F, Lu J, Shen Y, Meng L, Wang T, Ji N. Effectiveness and safety of pulsed radiofrequency treatment guided by computed tomography for refractory neuralgia of infraorbital nerve: a pilot study. Pain Physician. 2015;18:E795–804.
9. Cok OY, Deniz S, Eker HE, Oguzkurt L, Aribogan A. Management of isolated infraorbital neuralgia by ultrasound-guided infraorbital nerve block with combination of steroid and local anesthetic. J Clin Anesth. 2017;37:146–148. doi:10.1016/j.jclinane.2016.12.007
10. Wilkinson HA. Trigeminal nerve peripheral branch phenol/glycerol injections for tic douloureux. J Neurosurg. 1999;90:828–832. doi:10.3171/jns.1999.90.5.0828
11. Trescot AM. Headache management in an interventional pain practice. Pain Physician. 2000;3(2):197–200. doi:10.36076/ppj.2000/3/197
12. Marcinkowski M, Lewandowski L. Perception of gustatory sensation after treatment of the third branch trigeminal nerve and lingual nerve by peripheral alcohol injection. Ann Acad Med Stetin. 2006;52:65–68.
13. Ali FM, Prasant M, Pai D, Aher VA, Kar S, Safiya T. Peripheral neurectomies: a treatment option for trigeminal neuralgia in rural practice. J Neurosci Rural Pract. 2012;3:152–157. doi:10.4103/0976-3147.98218
14. Cerovic R, Juretic M, Gobic MB. Neurectomy of the trigeminal nerve branches: clinical evaluation of an “obsolete” treatment. J Craniomaxillofac Surg. 2009;37:388–391. doi:10.1016/j.jcms.2009.02.001
15. Shah SA, Khan MN, Shah SF, Ghafoor A, Khattak A. Is peripheral alcohol injection of value in the treatment of trigeminal neuralgia? An analysis of 100 cases. Int J Oral Maxillofac Surg. 2011;40:388–392. doi:10.1016/j.ijom.2010.11.010
16. Luo F, Wang T, Shen Y, Meng L, Lu JJ, Ji N. High voltage pulsed radiofrequency for the treatment of refractory neuralgia of the infraorbital nerve: a prospective double-blinded randomized controlled study. Pain Physician. 2017;20:271–279.
17. Jia YT, Chen Z, Ren H, Luo F. The effectiveness and safety of 42°C pulsed radiofrequency combined with 60°C continuous radiofrequency for refractory infraorbital neuralgia: a prospective study. Pain Physician. 2019;22(3):E171–E179.
18. Ren H, Shen Y, Luo F. Treatment of supraorbital neuralgia using ultrasound-guided radiofrequency thermocoagulation of the supraorbital nerve: a retrospective study. J Pain Res. 2020;13:251–259. doi:10.2147/JPR.S228720
19. Kanpolat Y, Savas A, Bekar A, Berk C. Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25-year experience with 1600 patients. Neurosurgery. 2001;48(3):524–532. doi:10.1097/00006123-200103000-00013
20. Lin B, Lu X, Zhai XL, Cai Z. Use of sensory and motor action potentials to identify the position of trigeminal nerve divisions for radiofrequency thermocoagulation. J Neurosurg. 2014;121:1497–1503. doi:10.3171/2014.8.JNS132484
21. Scrivani SJ, Keith DA, Mathews ES, Kaban LB. Percutaneous stereotactic differential radiofrequency thermal rhizotomy for the treatment of trigeminal neuralgia. J Oral Maxillofac Surg. 1999;57:104–112. doi:10.1016/S0278-2391(99)90218-5
22. Erdine S, Ozyalcin NS, Cimen A, Celik M, Talu GK, Disci R. Comparison of pulsed radiofrequency with conventional radiofrequency in the treatment of idiopathic trigeminal neuralgia. Eur J Pain. 2007;11:309–313. doi:10.1016/j.ejpain.2006.04.001
23. Luo F, Shen Y, Wang T, Meng L, Yu XT, Ji N. 3D CT-guided pulsed radiofrequency treatment for trigeminal neuralgia. Pain Pract. 2014;14:16–21. doi:10.1111/papr.12041
24. World Health Organization. International Statistical Classification of Diseases and Related Health Problems. World Health Organization; 2018.
25. Yao P, Hong T, Wang ZB, et al. Treatment of bilateral idiopathic trigeminal neuralgia by radiofrequency thermocoagulation at different temperatures. Medicine. 2016;95(29):e4274. doi:10.1097/MD.0000000000004274
26. Nie FC, Su D, Shi Y, et al. A prospective study of X-ray imaging combined with skin stimulation potential-guided percutaneous radiofrequency thermocoagulation of the Gasserian ganglion for treatment of trigeminal neuralgia. Pain Med. 2014;15(9):1464–1469. doi:10.1111/pme.12359
27. Huang Q, Liu X, Chen J, et al. The effectiveness and safety of thermocoagulation radiofrequency treatment of the ophthalmic division (v1) and/or maxillary (v2) and mandibular (v3) division in idiopathic trigeminal neuralgia: an observational study. Pain Physician. 2016;19:E1041–1047.
28. Wang ZM, Wang ZJ, Li K, Su X, Du C, Tian Y. Radiofrequency thermocoagulation for the treatment of trigeminal neuralgia. Exp Ther Med. 2022;23:17. doi:10.3892/etm.2021.10939
29. Xue TQ, Zhang QX, Bian H, et al. Radiofrequency thermocoagulation through foramen rotundum versus foramen ovale for the treatment of V2 trigeminal neuralgia. Pain Physician. 2019;22:E609–E614.
30. Gunduz HB, Cevik OM, Asilturk M, et al. Percutaneous radiofrequency thermocoagulation in trigeminal neuralgia: analysis of early and late outcomes of 156 cases and 209 interventions. J Korean Neurosurg Soc. 2021;64:827–836. doi:10.3340/jkns.2020.0333
31. Zhou XC, Liu YQ, Yue ZY, Luan DH, Zhang H, Han J. Comparison of nerve combing and percutaneous radiofrequency thermocoagulation in the treatment for idiopathic trigeminal neuralgia. Braz J Otorhinolaryngol. 2016;82:574–579. doi:10.1016/j.bjorl.2015.11.006
32. Mittal B, Thomas DG. Controlled thermocoagulation in trigeminal neuralgia. J Neurol Neurosurg Psychiatry. 1986;49:932–936. doi:10.1136/jnnp.49.8.932
33. Letcher FS, Goldring S. The effect of radiofrequency current and heat on peripheral nerve action potential in the cat. J Neurosurg. 1968;29:42–47. doi:10.3171/jns.1968.29.1.0042
34. Elawamy A, Abdalla EEM, Shehata GA. Effects of pulsed versus conventional versus combined radiofrequency for the treatment of trigeminal neuralgia: a prospective study. Pain Physician. 2017;20:E873–E881.
35. Wan Q, Zhang DY, Cao XT, Zhang Y, Zhu MY, Zuo W. CT-guided selective percutaneous radiofrequency thermocoagulation via the foramen rotundum for isolated maxillary nerve idiopathic trigeminal neuralgia. J Neurosurg. 2018;128:211–214. doi:10.3171/2016.9.JNS152520
36. Ding YY, Li HX, Hong T, Yao P. Comparison of efficacy and safety of CT-guided radiofrequency thermocoagulation through foramen rotundum versus foramen ovale for V2 primary trigeminal neuralgia. Pain Physician. 2021;24:587–596.
37. Wang TT, Xu SJ, He QL, et al. Efficacy and safety of radiofrequency thermocoagulation with different puncture methods for treatment of V1 trigeminal neuralgia: a prospective study. Pain Physician. 2021;24:145–152.
38. Lin HD, Cao G, Jin GJ, et al. Extracranial non-gasserian ganglion application of radiofrequency thermocoagulation on the mandibular branch of the trigeminal through the foramen ovale for trigeminal neuralgia. Pain Physician. 2021;24:E425–E432.
39. Bogduk N, Macintosh J, Marsland A. Technical limitations to the efficacy of radiofrequency neurotomy for spinal pain. Neurosurgery. 1987;20:529–535. doi:10.1227/00006123-198704000-00004
40. Chen Z, Jia YT, Jia ZP, Wang T, Luo F. The long-term outcome of 3-dimensional CT-guided percutaneous radiofrequency thermocoagulation for tumor-related trigeminal neuralgia. Pain Physician. 2019;22:E467–E475.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Lurasidone 80 mg in Patients with Schizophrenia: Results of an Open-Label, 12-Week Extension Study
Miura I, Watabe K, Sakaguchi R, Okamoto K, Maruyama H
Neuropsychiatric Disease and Treatment 2022, 18:2627-2637
Published Date: 9 November 2022
Effectiveness and Safety of a Fixed-Dose Combination of Valsartan and Rosuvastatin (Rovatitan® Tablet) in Patients with Concomitant Hypertension and Hyperlipidemia: An Observational Study
Lee KJ, Ryu JK, Cho YH, Shin WY, Kim JS, Yoon YW, Jang JY, Kim WH, Beom JW, Kang SM
Drug Design, Development and Therapy 2023, 17:1047-1062
Published Date: 6 April 2023
Real-World Safety and Effectiveness of Omalizumab in Moderate to Severe Allergic Asthma Patients in China: A Post-Authorization Study
Su N, Zhi L, Liu F, Wang Y, Zhang Q, Liu X, Wang X, Hao G, Zhang X, Hu Q, Ligueros-Saylan M, Uddin A, Yang J, Liang T, Ding L, Li R, Wang C
Journal of Asthma and Allergy 2023, 16:625-636
Published Date: 19 June 2023
Effectiveness and Safety of Anlotinib Combined with PD-1 Blockades in Patients with Previously Immunotherapy Treated Advanced Non-Small Cell Lung Cancer: A Retrospective Exploratory Study
Dou XJ, Ma RY, Ren DW, Liu Q, Yan P
Lung Cancer: Targets and Therapy 2024, 15:29-40
Published Date: 25 March 2024
Effectiveness and Safety of Adalimumab Biosimilars in Pediatric Psoriasis: A Multi-Center International Experience
Bertoli C, Torres T, Romita P, Stingeni L, Hansel K, Mastorino L, Ortoncelli M, Panzone M, Cruz MJ, Bianchi L, Zangrilli A, Musumeci ML, Micali G, Gerbino C, Simonetti O, De Simoni E, Longo C, Mahé E, Di Lernia V
Psoriasis: Targets and Therapy 2025, 15:233-241
Published Date: 28 June 2025