Back to Journals » Journal of Inflammation Research » Volume 17
Development and Validation of Nomograms for Predicting Pneumonia in Patients with COVID-19 and Lung Cancer
Authors Xu Y ![]() , Li H, Wang X, Li B, Gao A, Zhao Q, Yang L, Qin W, Wang L
, Li H, Wang X, Li B, Gao A, Zhao Q, Yang L, Qin W, Wang L ![]()
Received 25 January 2024
Accepted for publication 29 May 2024
Published 7 June 2024 Volume 2024:17 Pages 3671—3683
DOI https://doi.org/10.2147/JIR.S456206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yiyue Xu,1,* Haoqian Li,1,* Xiaoqing Wang,2 Butuo Li,1 Aiqin Gao,1 Qian Zhao,1 Linlin Yang,1 Wenru Qin,1 Linlin Wang1
1Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, People’s Republic of China; 2Department of Portal Hypertension, Shandong Public Health Clinical Center, Shandong University, Jinan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Linlin Wang, Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, 440 JiYan Road, Jinan, 250117, People’s Republic of China, Tel +86-13793187739, Email [email protected]
Background: COVID-19 has spread worldwide, becoming a global threat to public health and can lead to complications, especially pneumonia, which can be life-threatening. However, in lung cancer patients, the prediction of pneumonia and severe pneumonia has not been studied. We aimed to develop effective models to assess pneumonia after SARS-CoV-2 infection in lung cancer patients to guide COVID-19 management.
Methods: We retrospectively recruited 621 lung cancer patients diagnosed with COVID-19 via SARS-CoV-2 RT-PCR analysis in two medical centers and divided into training and validation group, respectively. Univariate and multivariate logistic regression analysis were used to identify independent risk factors of all-grade pneumonia and ≥ grade 2 pneumonia in the training group. Nomograms were established based on independent predictors and verified in the validation group. C-index, ROC curves, calibration curve, and DCA were used to evaluate the nomograms. Subgroup analyses in immunotherapy or thoracic radiotherapy patients were then conducted.
Results: Among 621 lung cancer patients infected with SARS-CoV-2, 203 (32.7%) developed pneumonia, and 66 (10.6%) were ≥ grade 2. Multivariate logistic regression analysis showed that diabetes, thoracic radiotherapy, low platelet and low albumin at diagnosis of COVID-19 were significantly associated with all-grade pneumonia. The C-indices of the prediction nomograms in the training group and validation group were 0.702 and 0.673, respectively. Independent predictors of ≥ grade 2 pneumonia were age, KPS, thoracic radiotherapy, platelet and albumin at COVID 19 diagnosis, with C-indices of 0.811 and 0.799 in the training and validation groups. In the thoracic radiotherapy subgroup, 40.8% and 11% patients developed all-grade and ≥grade 2 pneumonia, respectively. The rates in the immunotherapy subgroup were 31.3% and 6.6%, respectively.
Conclusion: We developed nomograms predicting the probability of pneumonia in lung cancer patients infected with SARS-CoV-2. The models showed good performance and can be used in the clinical management of COVID-19 in lung cancer patients. Higher-risk patients should be managed with enhanced protective measures and appropriate intervention.
Keywords: COVID-19, pneumonia, lung cancer, risk factor, nomogram
Introduction
In December 2019, the novel Coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome Coronavirus 2 (SARS-CoV-2) spread rapidly throughout the world,1 causing a global public health problem.2 As the pandemic progressed and vaccination advanced, herd immunity enhanced and the proportion of severe cases and mortality gradually decreased over time, and the majority of infected individuals had relatively mild disease without signs of pneumonia. However, patients with underlying disease are still at elevated risk of complications, especially pneumonia.3
According to the updated global cancer report, lung cancer is ranked the second place in terms of incidence and first in cancer-related mortality rate.4 Based on the characteristics of pulmonary neoplasms and treatment-related toxicity, it is therefore highly important to focus on advancing the management of COVID-19 pneumonia in lung cancer patients, especially those who received immunotherapy or thoracic radiotherapy (TRT). Immunotherapy represented by immune checkpoint inhibitors (ICIs) impacts the risk of developing pneumonia due to its regulation of immune cells and pro-inflammatory factors,5,6 immunotherapy against lung cancer decrease COVID-19 severity and incidence of pneumonia to some extent.7 Radiation may injure normal lung tissue and radiotherapy enhances the rate of pneumonia after SARS-CoV-2 infection.8,9 At present, there is still a lack of safe and effective therapeutic drugs for COVID-19 in the clinic. Once lung cancer patients develop COVID-19 pneumonia, the poor response to conventional therapy will make condition difficult to control and threaten patients’ life. Thus, it is urgently needed to identify the risk factors that aid in predicting COVID-19 pneumonia, provide better protection and strict surveillance to high-risk patients to decrease pneumonia occurrence, avoid delay in anti-neoplastic treatment, and reduce mortality. Building a reliable prediction model is currently important for clinical management of lung cancer patients with COVID-19.
The present studies found that lung cancer patients infected with SARS-CoV-2 have higher rates of severe disease and death than the general population.10 The comparison of lung cancer patients’ performance status before and after COVID-19 period showed a statistically significant worse score in the COVID-19 period.11 Increased age, comorbidities, and advanced disease were associated with increased risk of death in lung cancer patients, while race and pathologic type were unrelated.12–14 Studies in the overall population have found that hematological parameters such as lactate dehydrogenase, platelets, and albumin were reported as independent risk factors of severe COVID-19.15 In solid tumor patients, age and anti-tumor therapy were predictors for COVID-19 death.16 However, there are no studies predicting of COVID-19 pneumonia in patients with lung cancer.
A nomogram is a user-friendly graphical prediction model that can quantify an individual’s risk by integrating multiple risk factors.17 In this study, we aimed to develop easy-to-use and effective models to assess the risk of pneumonia and moderate-severe pneumonia after SARS-CoV-2 infection in lung cancer patients to stratify patients. These models can be used to assist clinicians in identifying high-risk patients and selecting appropriate treatment strategies.
Materials and Methods
Study Population
This retrospective study evaluated patients visiting Shandong Cancer Hospital and Shandong University Qilu Hospital between December 2022 and January 2023. The enrolled criteria for patient are list as follows: 1) Patients with histologically or cytologically confirmed lung cancer (tumor stage and pathologic types were not restricted); 2) Confirmed COVID-19 detecting via SARS-COV-2 nucleic acid in nasopharyngeal and oropharyngeal swab; 3) Age > 18 years. The exclusion criteria are as follows: 1) Patients with a history of other primary malignant tumors; 2) Patients with active pneumonia at baseline; 3) It was assessed as non-COVID-19 pneumonia; 4) It was not possible to ascertain the presence of pneumonia. This study was approved by the Ethics Committee of Shandong Cancer Hospital and complies with the Declaration of Helsinki.
Data Collection
Baseline demographic (age, sex, BMI, Karnofsky Performance Scale score, smoking index, and comorbidities), clinicopathological (histology, stage, anti-cancer therapy, and hematological data) and follow-up data were collected in detail from the electronic medical records according to a unified form. Baseline was defined as 2 to 4 weeks prior to COVID-19. Hematological data (lymphocyte, platelet, white blood cell, red blood cell, hemoglobin, neutrophil, monocyte, albumin, lactate dehydrogenase, and carcinoembryonic antigen) within a week after COVID-19 diagnosis were also collected, and changes in hematological data were calculated (diagnostic value minus baseline value). Pneumonia and moderate-severe pneumonia (≥ grade 2) were diagnosed and distinguished mainly based on computerized tomography (CT) images, chest X-ray, clinical symptoms, medical history, and laboratory tests according to the World Health Organization (WHO) criteria.18 The CT scan was performed by using 64-slice spiral CT (Siemens Medical Systems, Germany). To minimize sampling bias, two authors collected the data independently and cross-checked the data with medical personnel.
Model Training and Validation
Patients from Shandong Cancer Hospital were regarded as the training group and patients from Shandong University Qilu Hospital as the validation group. Nomograms of pneumonia and moderate-severe (≥ grade 2) pneumonia were established in the training group and verified in the validation group. We also performed subgroup analysis for the subset who had undergone immunotherapy or thoracic radiotherapy.
Statistical Analysis
Continuous variables are expressed as mean and standard deviation (SD), and categorical variables are expressed in frequency and percentage. In statistical analysis, simple deletion method is adopted to deal with missing data. In the training group, univariate logistic regression analysis was used to access potential risk factors, and variables with p-values less than 0.05 were incorporated into multivariate logistic regression analysis after excluding those with a Pearson correlation coefficient more than 0.4. Factors with p-values less than 0.1 were considered to be important predictors of COVID-19 pneumonia and included to establish the nomogram model. The concordance index (C-index), calibration curve, the area under the receiver operation curve (AUC), and decision curve analysis (DCA) were applied to evaluate the discrimination and clinical efficacy of the model. Roc curve and correction curve are used to evaluate nomogram correction graphically. In the validation group, C-index was used to verify the accuracy of the model. All analyses were performed using the STATA/MP 17.0 and R 4.2.1.
Results
The Demographic and Clinicopathological Features of Patients
Visits were routinely test for COVID-19 nucleic acid detection between December 2022 and January 2023. We retrospectively analyzed 716 lung cancer patients who were diagnosed with COVID-19 during this time period. As shown is Figure 1, patients were selected according to strict inclusion and exclusion criteria: 58 patients due to lack of baseline data; 2 due to age younger than 18 years; 2 due to no clear pathological findings; 24 due to other primary tumor; and 9 patients had pneumonia due to other causes. Ultimately, a total of 621 patients were enrolled for analysis, including 556 patients from Shandong Cancer Hospital, who were divided into the training group, and 65 patients from Shandong University Qilu Hospital, who were divided into the external validation group.
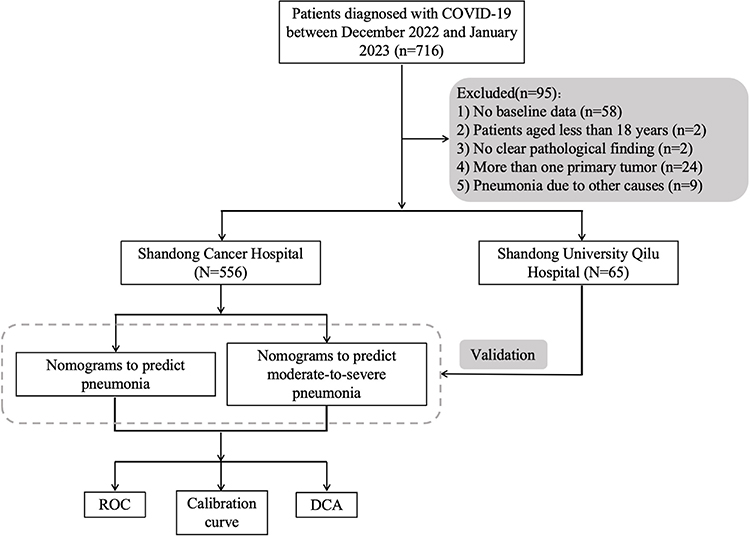 |
Figure 1 Flow diagram. |
A total of 203 (32.7%) patients developed COVID-19 pneumonia. Among them, 140 patients did not have pneumonia at baseline and developed pneumonia after SARS-CoV-2 infection. Sixty-three patients had old lesions in the lungs at baseline, and pneumonia was significantly aggravated after SARS-CoV-2 infection. According to the CT images, chest X-ray, clinical course, and hematological findings, 2 radiologists and clinicians with over 20 years’ experience jointly determined that 203 patients developed COVID-19 pneumonia. The World Health Organization’s (WHO) grading criteria are used to grade pneumonia. Sixty-six patients were graded as moderate-severe pneumonia.
A 5-month follow-up of 203 patients with pneumonia showed that 99 patients recovered completely and 78 patients had pulmonary sequelae, including pulmonary fibrosis and chronic pneumonia. Thirteen patients died because of pneumonia and 13 patients were lost to follow-up.
Independent Risk Factors for Pneumonia and Moderate-Severe Pneumonia
To investigate factors independently affecting COVID19 pneumonia, multivariate logistic regression analysis was performed on all parameters that were statistically significant on univariate analysis in the training group, as shown in Table 1. The results showed that diabetes (OR = 4.259, p < 0.001), thoracic radiotherapy (OR = 2.799, p < 0.001), platelet at baseline (OR = 0.997, p = 0.055), and albumin (OR = 0.921, p = 0.006) at diagnosis of COVID-19 were independent risk factors for pneumonia.
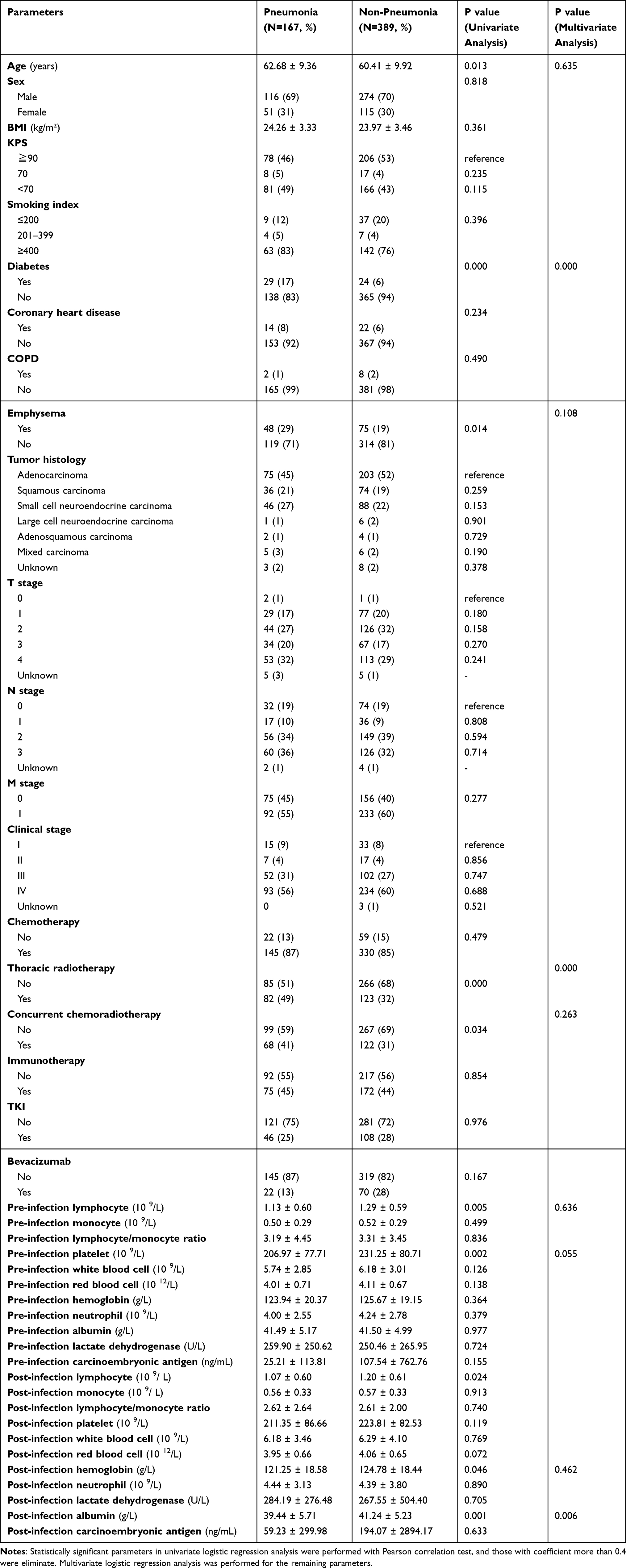 |
Table 1 Logistic Regression Analysis of Risk Factors for Pneumonia in the Training Group |
Table 2 shows the analysis of moderate-severe pneumonia, with age (OR = 1.058, p = 0.034), Karnofsky Performance Scale score (KPS) (KPS ≤ 70 vs ≥90, OR = 8.504, p = 0.002), thoracic radiotherapy (OR = 2.569, p = 0.010), platelet (OR = 0.994, p=0.031) and albumin (OR = 0.892, p = 0.058) at diagnosis of COVID-19 as independent risk factors for moderate-severe pneumonia.
 |
Table 2 Logistic Regression Analysis of Risk Factors for Moderate-Severe Pneumonia in the Training Group |
Construction and Validation of Discrimination Nomograms
Based on the predictors of pneumonia, the C-index of the constructed nomogram was 0.702 (0.648–0.757). The calibration curve showed that the predicted results were in good agreement with the observed results, and the DCA showed that the model had a good net benefit (Figure 2). The C-index for the validation group was 0.673 (0.532–0.814), demonstrating the stability of the model.
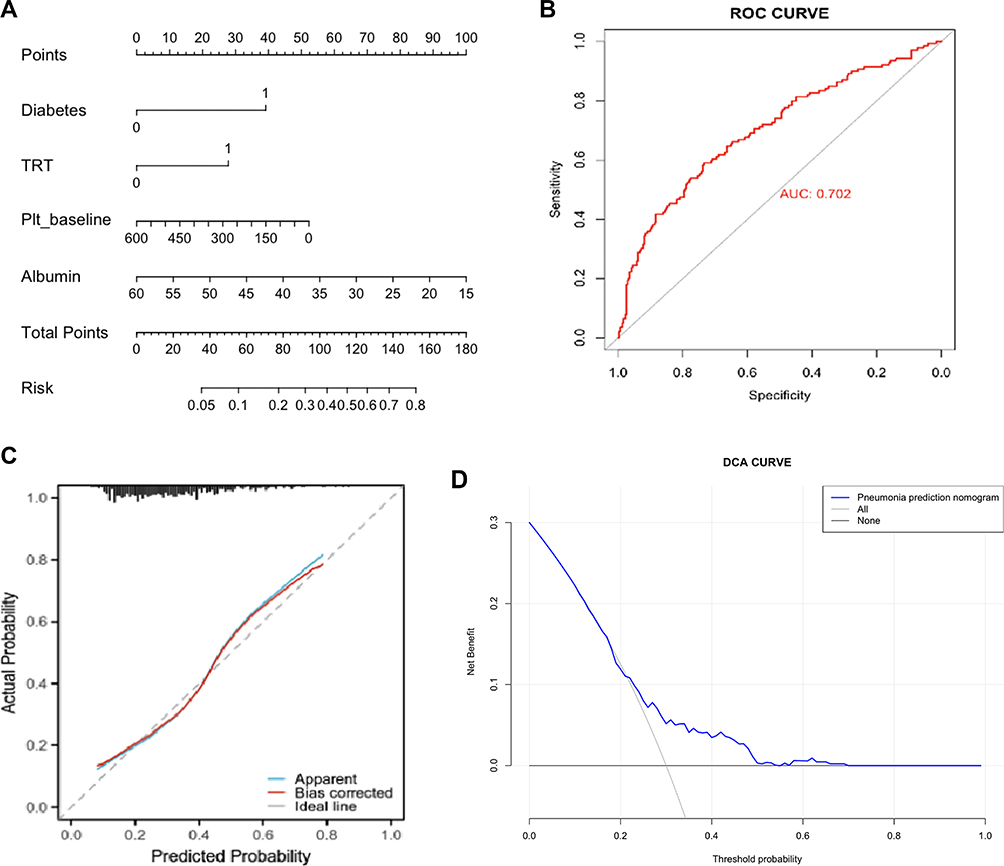 |
Figure 2 Nomogram (A), ROC (B), calibration curve (C), and DCA (D) of training group for pneumonia prediction. |
As shown in Figure 3, a nomogram was also constructed on the basis of independent predictors of moderate-severe pneumonia, and the C-index was 0.811 (0.738–0.884). Calibration curve and DCA show that the nomogram had good discrimination and achieved preferable prediction accuracy than pneumonia. The external verification performance was also satisfactory, with a C-index of 0.799 (0.677–0.921).
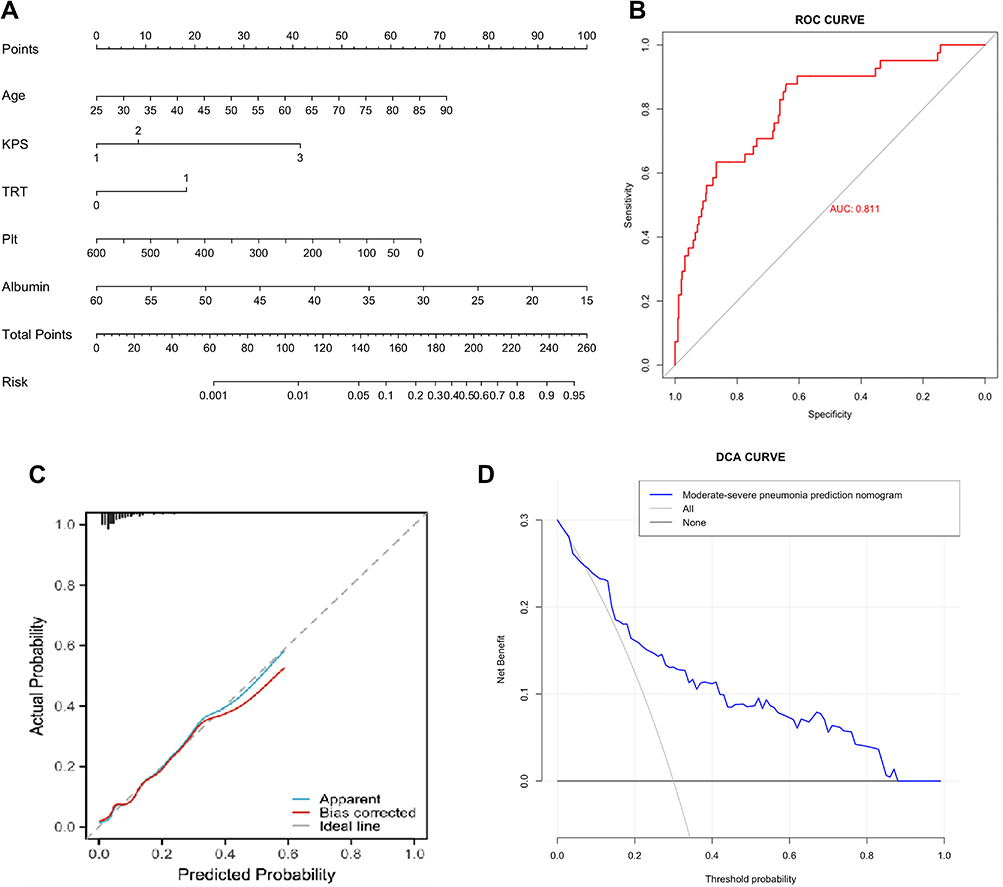 |
Figure 3 Nomogram (A), ROC (B), calibration curve (C), and DCA (D) of training group for moderate-severe pneumonia prediction. |
Subgroup Analysis
Both thoracic radiotherapy and immunotherapy may affect the occurrence of pneumonia, and thoracic radiotherapy is an independent risk factor for pneumonia. Therefore, subgroup analyses were performed in patients who had previously received thoracic radiotherapy or immunotherapy separately. Among 218 patients who had previously received thoracic radiotherapy, 89 (40.8%) developed pneumonia, and 24 (11.0%) developed moderate-severe pneumonia, which were higher than the general population. Patients with emphysema were more likely to develop all-grade pneumonia (OR = 1.945, p = 0.036). The risk of moderate-severe pneumonia increases with higher single doses (>2Gy vs ≤2Gy, OR = 4.575, p = 0.002). Two hundred and seventy-two had received immunotherapy, including programmed cell death 1 (PD-1) and programmed death ligand 1 (PD-L1) inhibitors. Twenty-six patients had received more than one line of immunotherapy. The median number of immunotherapy cycle was 4. Pneumonia occurred in 85 patients (31.3%) and 18 (6.6%) developed moderate-severe pneumonia. Patients who received more immunotherapy cycles had a lower risk of pneumonia (OR = 0.923, p = 0.020). Patients with low lymphocytes (OR = 0.247, p = 0.033) and high neutrophils (OR = 1.167, p = 0.006) at diagnosis of COVID-19 were more likely to develop moderate-severe pneumonia. Patients with a low lymphocyte/monocyte ratio at baseline (OR = 0.546, p = 0.037) or diagnosis of COVID-19 (OR = 0.448, p = 0.015) were more likely to develop moderate-severe pneumonia.
Discussion
COVID-19 is an acute infectious disease caused by the novel coronavirus (SARS-CoV-2) that spreads rapidly, imposing a significant burden on human health and healthcare systems.19 Previous studies have reported the hospitalization mortality of 1.4–4.3%.20 Lung cancer patients infected with SARS-CoV-2 experience more severe conditions, with a mortality rate ranging from 25% to 36%.13,21,22 Identifying high-risk groups and implementing specific preventive measures for them holds significant importance.23,24 To our knowledge, this study is the first to construct a visual predictive model for lung cancer patients progressing to pneumonia, particularly moderate-severe pneumonia, after SARS-CoV-2 infection. The nomograms established in this study can effectively predict the risk of all-grade pneumonia and moderate-severe pneumonia, thereby identifying high-risk individuals for COVID-19 pneumonia, which holds significant clinical application potential.
In our study, diabetes at baseline was identified as an independent risk factor for pneumonia and it is speculated that SARS-CoV-2 infection might lead to severe fluctuations in blood glucose levels among diabetic patients, creating a vicious cycle, possibly associated with the lowered immunity in these individuals. Previous research has indicated higher probabilities of complications and mortality among diabetic patients,25–27 with some studies considering diabetes as a prognostic risk factor for COVID-19.28 Keynote-001 clinical trial found that patients with a history of thoracic radiotherapy have a higher overall frequency of treatment-related pulmonary toxicity, possibly linked to radiation-induced damage to normal lung tissues and changes in the immune microenvironment.29 This study found that patients previously treated with thoracic radiotherapy were more prone to developing COVID-19 pneumonia. Thrombocytopenia emerged as another independent risk factor, likely associated with thrombocytopenia-related critical illnesses, commonly seen in COVID-19 patients with organ dysfunction or compromised physiological functions.30 Hypoalbuminemia represents poor nutritional status in patients, thus understanding the heightened risk of pneumonia among this subgroup.
Advanced age, low KPS, history of thoracic radiotherapy, platelet and albumin at diagnosis of COVID-19 were identified as independent risk factors for patients developing moderate-severe pneumonia. Advanced age and low KPS both signify poor physical condition. Some studies have found that elderly patients are more prone to complications,20 and advanced age is an independent risk factor for severe illness.31
The incidence of pneumonia increases among patients with a history of thoracic radiotherapy, and the occurrence of moderate-severe pneumonia rises with the increase in the single radiation dose, suggesting clinicians should use high-dose radiotherapy cautiously. While smoking is not a risk factor, patients with emphysema, which is one of the consequences of smoking, were more prone to developing COVID-19 pneumonia after receiving thoracic radiotherapy.32
In our study, the incidence of pneumonia in the subgroup undergoing immunotherapy was slightly lower than the general population, with the treatment cycle being a protective factor, potentially linked to enhanced antiviral T-cell immune response. Another study also indicated that immunotherapy did not increase the risk of severe infections or cytokine storms.7 Patients receiving immunotherapy had a lower mortality rate than the general population.33,34 Lymphocytes and neutrophils, respectively, act as risk and protective factors. Some studies have shown that lymphocyte count affects the prognosis of COVID-19 patients.35 The specific mechanism might involve the effect of SARS-CoV-2 on T lymphocytes, where T lymphocyte damage becomes a crucial factor leading to patient deterioration.36 Analysis of patient lymphocyte spectra showed decreased lymphocytes and increased neutrophils.37 Neutrophils are important inflammatory cells that often exhibit immune cell response dysregulation and subsequent immune abnormalities in severe viral diseases. Moreover, due to compromised immune function, severely viral infected patients are more prone to concurrent bacterial infections, potentially explaining the elevated neutrophil counts observed in our study. Qin et al found that neutrophil counts might be higher in severe COVID-19 cases.38
We acknowledge the limitations of our study. Firstly, the retrospective nature of the analysis might introduce potential biases and confounding factors. Secondly, it did not distinguish the possible differences between variants of SARS-CoV-2. Finally, this study only included clinical parameters and could not analyze specific mechanisms. Further research is needed for a deeper understanding of the pathogenesis of COVID-19 pneumonia.
Conclusion
In this study, visual nomograms were constructed to predict COVID-19 pneumonia with satisfactory discrimination and calibration. It also demonstrated good discriminatory ability in predicting moderate-severe pneumonia. Rigorously validated by external validation groups, the efficacy of nomograms was promising, potentially serving as a convenient, intuitive and individual clinical tool for assessing the risk of pneumonia in lung cancer patients with SARS-CoV-2 infection, aiding in individualized management and treatment adjustments of COVID-19 patients.
Data Sharing Statement
Research data are stored in an institutional repository and will be shared upon request to the corresponding author.
Ethics Approval and Consent to Participate
This research is conducted according to the World Medical Association Declaration of Helsinki.
Acknowledgment
Informed consent was obtained from all study participants prior to the commencement of the study.
Funding
This research was supported by National Natural Science Foundation of China (Grant number 82172865), Start-up fund of Shandong Cancer Hospital (Grant number 2020-B14), Clinical Research Special Fund of Wu Jieping Medical Foundation (Grant number 320.6750.2021-02-51 and 320.6750.2021-17-13).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574. doi:10.1016/S0140-6736(20)30251-8
2. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
3. Ganti AK, Fillmore NR, Bihn J, et al. Risk factors of SARS-CoV-2 infection and complications from COVID-19 in lung cancer patients. Int J Clin Oncol. 2023;28(4):531–542. doi:10.1007/s10147-023-02311-3
4. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Mi Z, Zhang Y, Feng Z, et al. Treatment-related adverse events of PD-1/PD-L1 inhibitors combined with CTLA-4 inhibitors in clinical trials: a meta-analysis. Artif Cells Nanomed Biotechnol. 2022;50(1):301–309. doi:10.1080/21691401.2022.2131354
6. Yin J, Wu Y, Yang X, Gan L, Xue J. Checkpoint Inhibitor Pneumonitis Induced by Anti-PD-1/PD-L1 Therapy in Non-Small-Cell Lung Cancer. Front Immunol. 2022;13:830631.
7. Bakouny Z, Labaki C, Grover P, et al. Interplay of Immunosuppression and Immunotherapy Among Patients With Cancer and COVID-19. JAMA Oncol. 2023;9(1):128–134.
8. Minami-Shimmyo Y, Ohe Y, Yamamoto S, et al. Risk factors for treatment-related death associated with chemotherapy and thoracic radiotherapy for lung cancer. J Thorac Oncol. 2012;7(1):177–182. doi:10.1097/JTO.0b013e31823c4c07
9. Fornacon-Wood I, Banfill K, Ahmad S, et al. Impact of the COVID-19 Pandemic on Outcomes for Patients with Lung Cancer Receiving Curative-intent Radiotherapy in the UK. Clin Oncol. 2023;35(10):e593–e600. doi:10.1016/j.clon.2023.07.005
10. Rogado J, Pangua C, Serrano-Montero G, et al. Covid-19 and lung cancer: a greater fatality rate? Lung Cancer. 2020;146:19–22. doi:10.1016/j.lungcan.2020.05.034
11. Mojsak D, Dębczyński M, Kuklińska B, et al. Impact of COVID-19 in Patients with Lung Cancer: a Descriptive Analysis. Int J Environ Res Public Health. 2023;20(2):1583. doi:10.3390/ijerph20021583
12. Kuderer NM, Choueiri TK, Shah DP, et al. Clinical impact of COVID-19 on patients with cancer (CCC19): a cohort study. Lancet. 2020;395(10241):1907–1918. doi:10.1016/S0140-6736(20)31187-9
13. Garassino MC, Whisenant JG, Huang L-C, et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): first results of an international, registry-based, cohort study. Lancet Oncol. 2020;21(7):914–922. doi:10.1016/S1470-2045(20)30314-4
14. Provencio M, Mazarico Gallego JM, Calles A, et al. Lung cancer patients with COVID-19 in Spain: GRAVID study. Lung Cancer. 2021;157:109–115. doi:10.1016/j.lungcan.2021.05.014
15. Tang F, Zhang X, Zhang B, et al. A nomogram prediction of outcome in patients with COVID-19 based on individual characteristics incorporating immune response-related indicators. J Med Virol. 2022;94(1):131–140. doi:10.1002/jmv.27275
16. Liu C, Li L, Song K, et al. A nomogram for predicting mortality in patients with COVID-19 and solid tumors: a multicenter retrospective cohort study. J Immunother Cancer. 2020;8(2):e001314. doi:10.1136/jitc-2020-001314
17. Iasonos A, Schrag D, Raj GV, et al. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
18. World Health Organization. Guidelines Approved by the Guidelines Review Committee, in Clinical Management of COVID-19: Living Guideline. Geneva: 2022, World Health Organization © World Health Organization; 2021.
19. Zhu F, Cao Y, Xu S, et al. Co-infection of SARS-CoV-2 and HIV in a patient in Wuhan city, China. J Med Virol. 2020;92(6):529–530. doi:10.1002/jmv.25732
20. Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
21. Trivanović D, Peršurić Ž, Agaj A, et al. The Interplay of Lung Cancer, COVID-19, and Vaccines. Int J Mol Sci. 2022;23(23):15067. doi:10.3390/ijms232315067
22. Mariniello DF, Aronne L, Vitale M, et al. Current challenges and perspectives in lung cancer care during COVID-19 waves. Curr Opin Pulm Med. 2023;29(4):239–247. doi:10.1097/MCP.0000000000000967
23. Passaro A, Bestvina C, Velez Velez M, et al. Severity of COVID-19 in patients with lung cancer: evidence and challenges. J Immunother Cancer. 2021;9(3):e002266. doi:10.1136/jitc-2020-002266
24. Lamontagne F, Stegemann M, Agarwal A, et al. A living WHO guideline on drugs to prevent covid-19. BMJ. 2021;372:n526. doi:10.1136/bmj.n526
25. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
26. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
27. Bhargava A, Fukushima EA, Levine M, et al. Predictors for Severe COVID-19 Infection. Clin Infect Dis. 2020;71(8):1962–1968. doi:10.1093/cid/ciaa674
28. Guo W, Li M, Dong Y, et al. Diabetes is a risk factor for the progression and prognosis of COVID −19. Diabetes Metab Res Rev. 2020;36(7):e3319. doi:10.1002/dmrr.3319
29. Shaverdian N, Lisberg AE, Bornazyan K, et al. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: a secondary analysis of the KEYNOTE-001 Phase 1 trial. Lancet Oncol. 2017;18(7):895–903. doi:10.1016/S1470-2045(17)30380-7
30. Lippi G, Plebani M, Henry BM. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: a meta-analysis. Clin Chim Acta. 2020;506:145–148. doi:10.1016/j.cca.2020.03.022
31. Liang W, Liang H, Ou L, et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern Med. 2020;180(8):1081–1089. doi:10.1001/jamainternmed.2020.2033
32. Vij N, Chandramani-Shivalingappa P, Van Westphal C, et al. Cigarette smoke-induced autophagy impairment accelerates lung aging, COPD-emphysema exacerbations and pathogenesis. Am J Physiol Cell Physiol. 2018;314(1):C73–c87. doi:10.1152/ajpcell.00110.2016
33. Trama A, Proto C, Whisenant JG, et al. Supporting Clinical Decision-Making during the SARS-CoV-2 Pandemic through a Global Research Commitment: the TERAVOLT Experience. Cancer Cell. 2020;38(5):602–604. doi:10.1016/j.ccell.2020.10.002
34. Várnai C, Palles C, Arnold R, et al. Mortality Among Adults With Cancer Undergoing Chemotherapy or Immunotherapy and Infected With COVID-19. JAMA Network Open. 2022;5(2):e220130. doi:10.1001/jamanetworkopen.2022.0130
35. Dong YM, Sun J, Li Y-X, et al. Development and Validation of a Nomogram for Assessing Survival in Patients With COVID-19 Pneumonia. Clin Infect Dis. 2021;72(4):652–660. doi:10.1093/cid/ciaa963
36. Liu J, Liu Y, Xiang P, et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J Transl Med. 2020;18(1):206. doi:10.1186/s12967-020-02374-0
37. Liu J, Li S, Liu J, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020;55:102763. doi:10.1016/j.ebiom.2020.102763
38. Qin C, Zhou L, Hu Z, et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762–768. doi:10.1093/cid/ciaa248
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
The m7G Modification Level and Immune Infiltration Characteristics in Patients with COVID-19
Lu L, Zheng J, Liu B, Wu H, Huang J, Wu L, Li D
Journal of Multidisciplinary Healthcare 2022, 15:2461-2472
Published Date: 26 October 2022
Preoperative Systemic Inflammatory Markers as a Significant Prognostic Factor After TURBT in Patients with Non-Muscle-Invasive Bladder Cancer
Ding L, Deng X, Wang K, Xia W, Zhang Y, Zhang Y, Shao X, Wang J
Journal of Inflammation Research 2023, 16:283-296
Published Date: 21 January 2023
Risk Factor for Superimposed Nosocomial Bloodstream Infections in Hospitalized Patients with COVID-19
Sathaporn N, Khwannimit B
Infection and Drug Resistance 2023, 16:3751-3759
Published Date: 13 June 2023
Increased Incidence and Risk Factors of Infections by Extended-Spectrum β-Lactamase-Producing Enterobacterales During the COVID-19 Pandemic: A Retrospective Case-Control Study
Geng Y, Li F, Chen C, Liu Z, Ma X, Su X, Meng H, Lu W, Wang X, Pan D, Liang P
Infection and Drug Resistance 2023, 16:4707-4716
Published Date: 20 July 2023